1 LifeBridge Physician Network Care Path Chronic Obstructive Pulmonary Disease (COPD) August 9, 2016 LBPN Care Path Aim: To develop and implement standard protocols, based on the best evidence, that provide a consistent clinical experience for LifeBridge Health patients and allow us to quantitatively demonstrate to payers the high-value care we provide. WHY? Rationale for COPD Focus i • In 2011, 12.7 million U.S. adults were estimated to have COPD. However, close to 24 million U.S. adults have evidence of impaired lung function, indicating an under diagnosis of COPD. • COPD is the third leading cause of death in America, claiming the lives of 134,676 Americans in 2010. • COPD was reported for an estimated 715,000 hospital discharges in 2010; a discharge rate of 23.2 per 100,000 population. • COPD ranks as the third most frequent cause for readmission to hospitals within 30 days. ii • A Lung Association survey revealed that half of all COPD patients (51%) say their condition limits their ability to work. It also limits them in normal physical exertion (70%), household chores (56%), social activities (53%), sleeping (50%) and family activities (46%). WHAT? Evidence-Based Recommendations Key Points: COPD is an umbrella term used to describe progressive lung diseases including emphysema, chronic bronchitis, refractory (non-reversible) asthma, and some forms of bronchiectasis. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) classifications are used to determine the severity of the disease, these classifications can help guide appropriate treatments to relieve symptoms and reduce risk. Appropriate therapies should be designed to help patients avoid exacerbations, hospitalizations, and death. The GOLD COPD guidelines recommend that all people with COPD receive an influenza vaccine every year. CDC Immunization Guidelines recommend that everyone with COPD receive the pneumococcal vaccine. COPD patients should be considered ideal candidates for Transitional Care Management (TCM) and Chronic Care Management (CCM) outreach. Providers can receive additional reimbursements for both TCM and CCM services.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
LifeBridge Physician Network Care Path Chronic Obstructive Pulmonary Disease (COPD)
August 9, 2016
LBPN Care Path Aim: To develop and implement standard protocols, based on the best evidence, that provide a consistent clinical experience for LifeBridge Health patients and allow us to quantitatively demonstrate to payers the high-value care we provide.
WHY? Rationale for COPD Focusi • In 2011, 12.7 million U.S. adults were estimated to have COPD. However, close to 24 million
U.S. adults have evidence of impaired lung function, indicating an under diagnosis of COPD. • COPD is the third leading cause of death in America, claiming the lives of 134,676 Americans
in 2010. • COPD was reported for an estimated 715,000 hospital discharges in 2010; a discharge rate
of 23.2 per 100,000 population. • COPD ranks as the third most frequent cause for readmission to hospitals within 30 days.ii • A Lung Association survey revealed that half of all COPD patients (51%) say their condition
limits their ability to work. It also limits them in normal physical exertion (70%), household chores (56%), social activities (53%), sleeping (50%) and family activities (46%).
WHAT? Evidence-Based Recommendations
Key Points: COPD is an umbrella term used to describe progressive lung diseases including
emphysema, chronic bronchitis, refractory (non-reversible) asthma, and some forms of bronchiectasis.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) classifications are used to determine the severity of the disease, these classifications can help guide appropriate treatments to relieve symptoms and reduce risk.
Appropriate therapies should be designed to help patients avoid exacerbations, hospitalizations, and death.
The GOLD COPD guidelines recommend that all people with COPD receive an influenza vaccine every year.
CDC Immunization Guidelines recommend that everyone with COPD receive the pneumococcal vaccine.
COPD patients should be considered ideal candidates for Transitional Care Management (TCM) and Chronic Care Management (CCM) outreach. Providers can receive additional reimbursements for both TCM and CCM services.

2
I. Risk Factors and Screeningiii: • Patients younger than 35 years rarely get COPD because susceptible individuals
develop the disease only after inhalational exposure to causative agents of sufficient intensity and duration. An estimated 80% to 90% of COPD is due to cigarette smoking.
• Other risk factors may include second-hand smoke and occupational or other exposure to dust, vapors, irritants, and fumes. α1-antitrypsin deficiency is the best-described genetic risk factor to consider, especially when patients develop COPD before age 50 years.
• Screening for COPD in the asymptomatic general population is not recommended. • The updated 2009 GOLD guidelines suggest that clinicians perform spirometry to look
for COPD in patients with symptoms, such as chronic cough and sputum production or shortness of breath.
II. Diagnosisiv: • Clinicians should suspect COPD in patients with a smoking history or substantial
exposure to inhaled irritants who have chronic cough, sputum, or dyspnea. • Peak Expiratory Flow (PEF) measurement can assist with the case-finding of COPD
before confirmation with spirometry.v A PEF rate of less than 80% has been shown to detect more than 90% of people with COPD in the community, including all of those with moderate or severe disease.vi
• Confirm the diagnosis by spirometry with a FEV1–FVC ratio < 0.70 measured after administration of a bronchodilator.
• Use the FEV1 and clinical data to determine disease severity and to exclude other disorders. The FEV1 percentage predicted is used to determine the GOLD classification and categorize COPD as:
o Mild (>80%) o Moderate (50%-80%) o Severe (30%-50%) o Very Severe (<30%)
• Consider measuring the α1-antrypsin level in patients who present with early-onset COPD or in those with a compatible family history.
III. Treatment Strategyvii: • All patients with COPD who smoke should be urged to stop and to enter a smoking
cessation program. • Patients who have symptoms, such as dyspnea, can be treated with inhaled β-agonists
or anticholinergic agents alone or in combination.
3
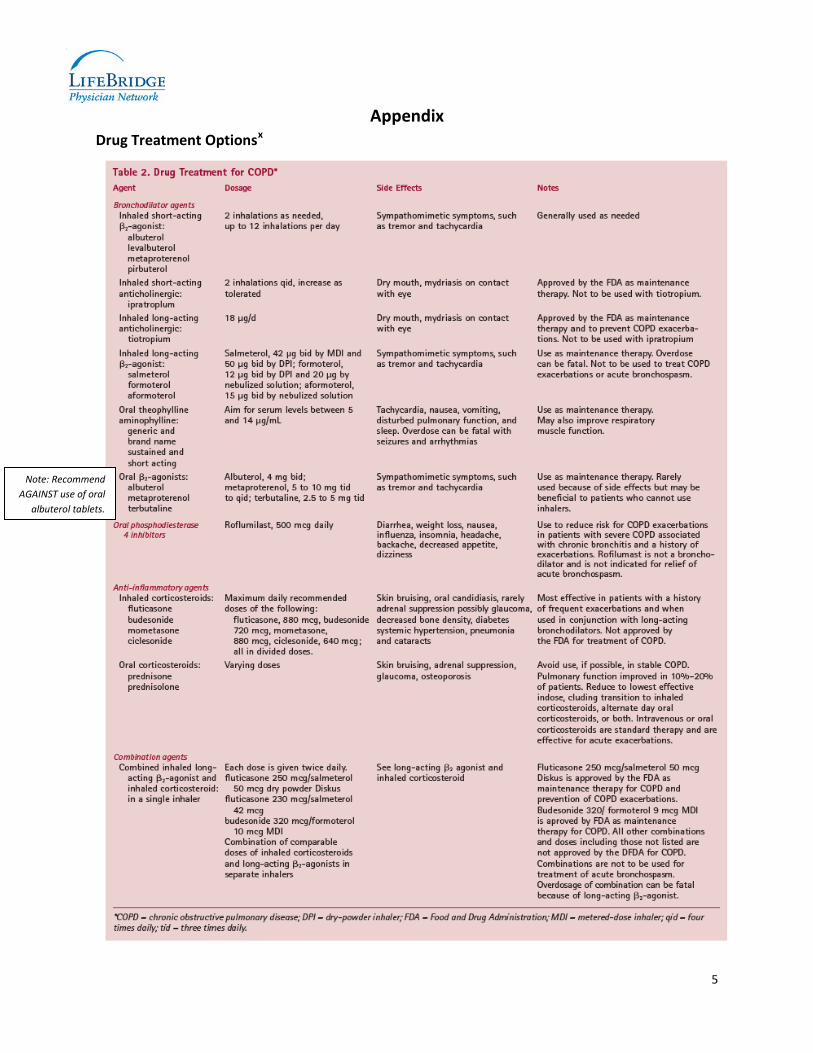
• The greatest benefit from treatment with long-acting bronchodilators is achieved in patients with an FEV1 < 60% of predicted, and benefits include improved health status and reduced COPD exacerbations. These benefits may be enhanced with the addition of an inhaled corticosteroid (See appendix for guidelines regarding drug treatment options). NOTE – long-acting beta2-agonists should not be used without concomitant use of corticosteroids for patients with asthma or asthma/COPD overlap.viii
• Acute exacerbations should be treated by optimizing bronchodilator therapy and adding antibiotics when clinically indicated.
• All patients should be encouraged to exercise. Pulmonary rehabilitation should be offered to patients with moderate-to severe COPD to improve dyspnea and health status.
• Continuous long-term oxygen therapy is recommended for patients with hypoxemia. • Eligible patients should be evaluated for lung-volume reduction surgery or lung
transplantation. • Comorbidities are common for people with COPD because organ systems work
differently when they do not receive enough oxygen. Common comorbidities include heart disease, osteoporosis, diabetes, and lung infections (e.g., pneumonia)ix. Chronic Care Management (CCM) outreach can be an effective practice for monitoring and controlling patients with COPD and comorbidities.
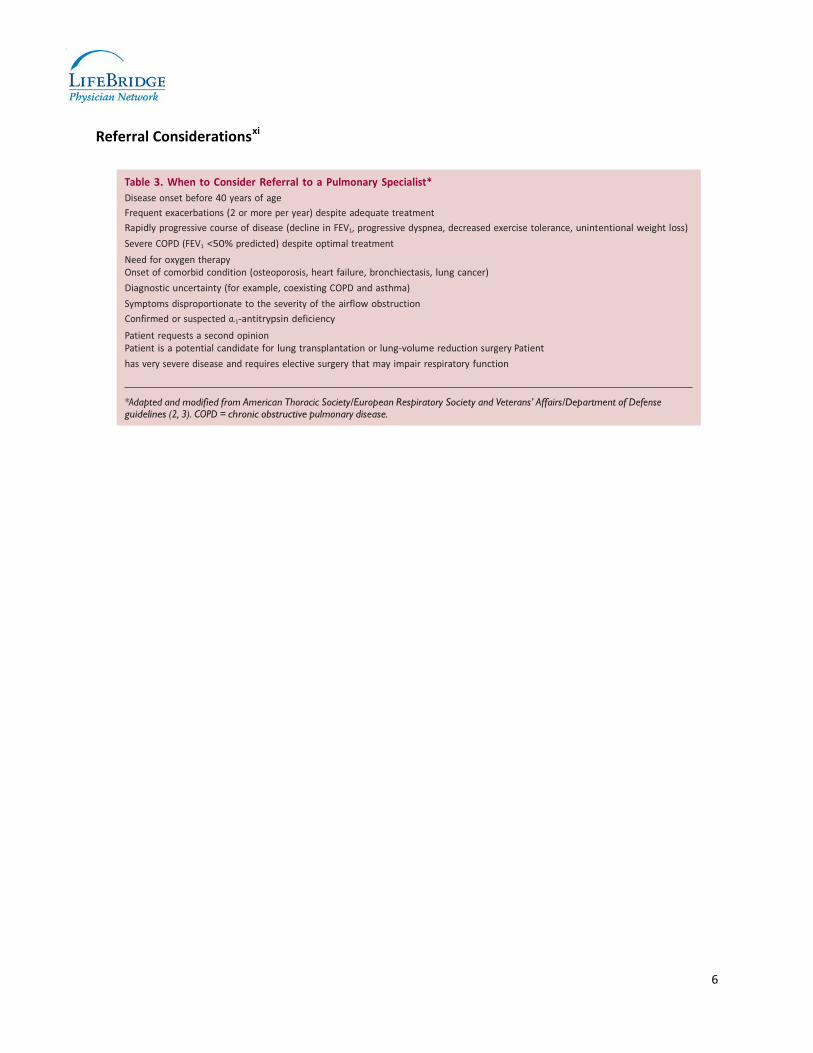
• Refer patients to a pulmonary specialist when appropriate (See appendix for pulmonary specialist referral guidelines).
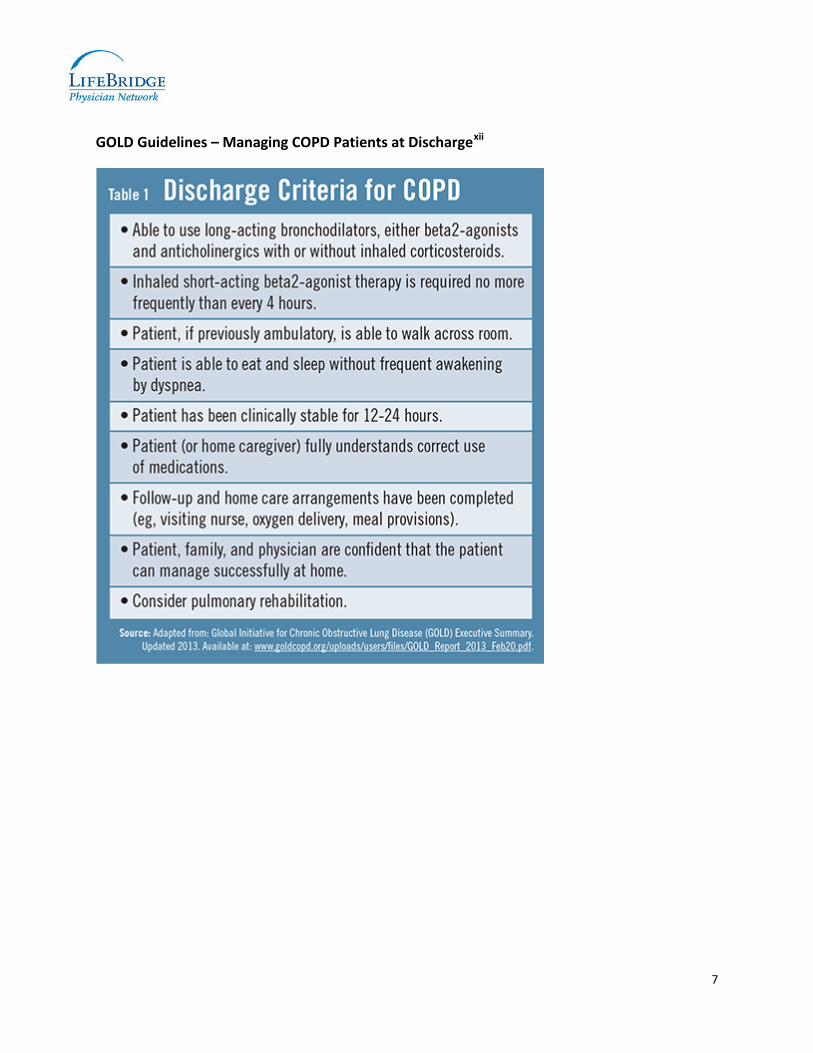
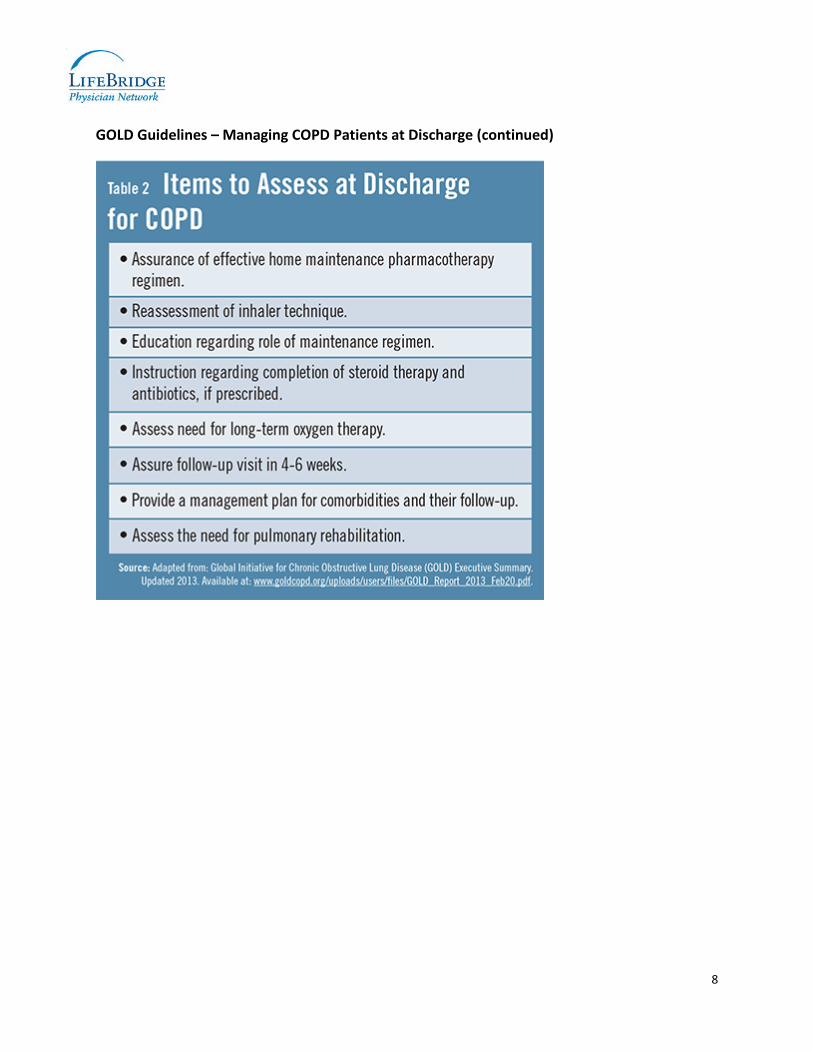
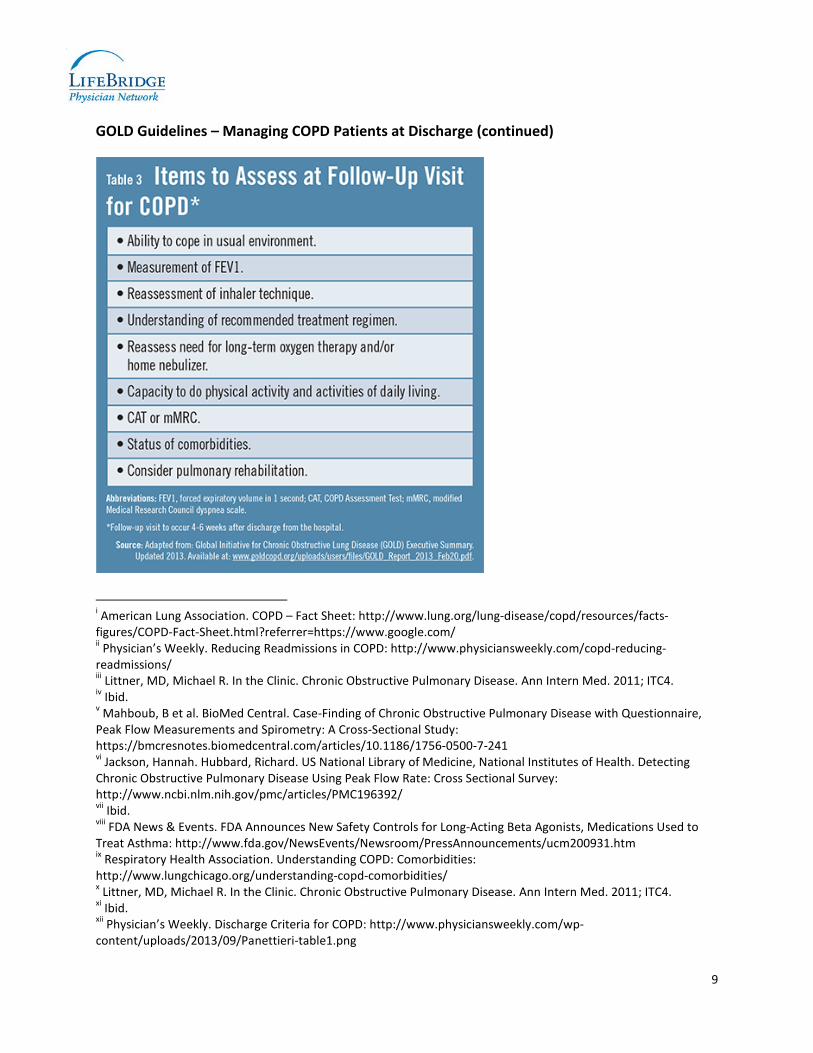
• Following an inpatient admission for COPD, physicians should refer to the GOLD guidelines for COPD patient discharge and follow-up (see appendix for GOLD discharge information/tables). In addition to the GOLD guidelines, Transitional Care Management (TCM) is recommended as a best practice. TCM requires an interactive patient contact within two business days post-discharge and an office visit within 7 to 14 days post-discharge. The TCM timeline is designed to better accommodate the patient’s transition needs and prevent 30-day readmission.
Measures of Performance (aligned with CMS’ ACO/PQRS/Meaningful Use CQM measures) 1. Tobacco Use: Screening and Cessation Intervention (ACO #17; NQF #28; PQRS #226)
Percentage of patients aged 18 years and older who were screened for tobacco use one or more times within 24 months AND who received cessation counseling intervention if identified as a tobacco user. Domain: Population/Public Health Numerator: Patients who were screened for tobacco use at least once within 24 months AND who received
tobacco cessation counseling intervention if identified as a tobacco user. Denominator: All patients aged 18 years and older.

4
2. Preventive Care and Screening: Influenza Immunization (ACO #14; NQF #41; PQRS #110) Percentage of patients aged 6 months and older seen for a visit between October 1 and March 31 who received an influenza immunization OR who reported previous receipt of an influenza immunization Domain: Population/Public Health Numerator: Patients who received an influenza immunization OR who reported previous receipt of an
influenza immunization. Denominator: All patients aged 6 months and older seen for a visit between October 1 and March 31.
3. Pneumonia Vaccination Status for Older Adults (ACO #15; NQF #43; PQRS #111) Percentage of patients 65 years of age and older who have ever received a pneumococcal vaccine. Domain: Clinical Process/Effectiveness Numerator: Patients who have ever received a pneumococcal vaccination. Denominator: Patients 65 years of age and older with a visit during the measurement period.
Tools and Resources • American Lung Association – COPD
http://www.lung.org/lung-disease/copd/?referrer=https://www.google.com/
• Centers for Disease Control – COPD http://www.cdc.gov/copd/index.html
• Global Initiative for Chronic Obstructive Lung Disease (GOLD) – Updated 2014 http://www.goldcopd.org/uploads/users/files/GOLD_Report_2014_Jan23.pdf
• COPD Foundation http://www.copdfoundation.org/
LBPN Contributing Experts/Team • Dr. William Han • Dr. Jaime Barnes • Dr. Joseph Carrington • LBPN Quality Committee
Questions? If you have questions about this Care Path or would like to connect with a specialist to discuss further, please contact either Dr. Charles Albrecht at 410-601-6340, or David Baker at 410-601-6666.
Key References Littner, MD, Michael R. In the Clinic. Chronic Obstructive Pulmonary Disease. Ann Intern Med. 2011; ITC4.
5
Appendix Drug Treatment Optionsx
Note: Recommend AGAINST use of oral
albuterol tablets.
6
Referral Considerationsxi
Diagnostic coexisting
lung-volume
that function
Defense
7
GOLD Guidelines – Managing COPD Patients at Dischargexii
8
GOLD Guidelines – Managing COPD Patients at Discharge (continued)
9
GOLD Guidelines – Managing COPD Patients at Discharge (continued)
i American Lung Association. COPD – Fact Sheet: http://www.lung.org/lung-disease/copd/resources/facts-figures/COPD-Fact-Sheet.html?referrer=https://www.google.com/ ii Physician’s Weekly. Reducing Readmissions in COPD: http://www.physiciansweekly.com/copd-reducing-readmissions/ iii Littner, MD, Michael R. In the Clinic. Chronic Obstructive Pulmonary Disease. Ann Intern Med. 2011; ITC4. iv Ibid. v Mahboub, B et al. BioMed Central. Case-Finding of Chronic Obstructive Pulmonary Disease with Questionnaire, Peak Flow Measurements and Spirometry: A Cross-Sectional Study: https://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-7-241 vi Jackson, Hannah. Hubbard, Richard. US National Library of Medicine, National Institutes of Health. Detecting Chronic Obstructive Pulmonary Disease Using Peak Flow Rate: Cross Sectional Survey: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC196392/ vii Ibid. viii FDA News & Events. FDA Announces New Safety Controls for Long-Acting Beta Agonists, Medications Used to Treat Asthma: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm200931.htm ix Respiratory Health Association. Understanding COPD: Comorbidities: http://www.lungchicago.org/understanding-copd-comorbidities/ x Littner, MD, Michael R. In the Clinic. Chronic Obstructive Pulmonary Disease. Ann Intern Med. 2011; ITC4. xi Ibid. xii Physician’s Weekly. Discharge Criteria for COPD: http://www.physiciansweekly.com/wp-content/uploads/2013/09/Panettieri-table1.png
Related Documents











