130 Am J Clin Pathol 2008;129:130-142 130 DOI: 10.1309/WYACYWF6NGM3WBRT © American Society for Clinical Pathology Anatomic Pathology / LEUKEMIA CUTIS Leukemia Cutis Jeong Hee Cho-Vega, MD, PhD, 1 L. Jeffrey Medeiros, MD, 2 Victor G. Prieto, MD, PhD, 3 and Francisco Vega, MD, PhD 2 Key Words: Leukemia cutis; Histology; Immunophenotype; Molecular genetic pathogenesis DOI: 10.1309/WYACYWF6NGM3WBRT Abstract Leukemia cutis (LC) is a nonspecific term used for cutaneous manifestations of any type of leukemia. LC has a wide range of cutaneous manifestations, which can make it difficult to clinically distinguish LC from other skin lesions. Patients with LC usually have concomitant systemic leukemia, but occasionally skin involvement precedes the involvement of the bone marrow or peripheral blood. Thus, a skin biopsy can be the first indication of the presence of leukemia in a subset of patients. The immunophenotyping of routinely processed skin biopsy specimens is very useful in establishing the diagnosis of LC. Although the molecular mechanisms explaining the pathogenesis of LC are not well defined, chemokine receptors and adhesion molecules may have an important role in skin tropism. We review the literature and recent advances pertaining to LC, with special emphasis on the immunohistochemical assessment and possible mechanisms involved in skin tropism by leukemic cells. Leukemia cutis is defined as cutaneous infiltration by neo- plastic leukocytes (myeloid or lymphoid), resulting in clinical- ly identifiable cutaneous lesions. 1 When composed of neoplas- tic granulocytic precursors, leukemia cutis has been designated as myeloid sarcoma, granulocytic sarcoma, primary extramedullary leukemia, or chloroma. 2 When composed of neoplastic monocytic precursors (monoblasts and promono- cytes), leukemia cutis also has been designated as monoblastic sarcoma. 2 The terms myeloid sarcoma and extramedullary myeloid cell tumor have also been used to include both granu- locytic and monocytic tumors. 3,4 Leukemia cutis has been described in patients with acute myeloid leukemia, chronic myeloproliferative disease, including chronic myelogenous leukemia (CML), myelodysplastic syn- dromes, and myelodysplastic/lymphoproliferative diseases ❚Table 1❚. 2 In patients with chronic diseases, skin involvement is associ- ated with transformation into a blastic phase and suggests disease progression. Leukemia cutis is used as the term for lymphocytic leukemias involving skin that are also designated by their specif- ic diagnosis, such as precursor B- or T-cell lymphoblastic leukemia/lymphoma and chronic lymphocytic leukemia. In this review article, we discuss the various types of leukemia most frequently represented in leukemia cutis as defined by the World Health Organization classification. 4 We focus on the immunophenotypic features of leukemia cutis and will discuss the possible molecular mechanisms responsi- ble for the migration of leukemic cells to the skin. Clinical Manifestations Frequency Overall, leukemia cutis occurs in 10% to 15% of patients with acute myeloid leukemia (AML) and less frequently in Downloaded from https://academic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 September 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

130 Am J Clin Pathol 2008;129:130-142130 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Anatomic Pathology / LEUKEMIA CUTIS
Leukemia Cutis
Jeong Hee Cho-Vega, MD, PhD,1 L. Jeffrey Medeiros, MD,2 Victor G. Prieto, MD, PhD,3
and Francisco Vega, MD, PhD2
Key Words: Leukemia cutis; Histology; Immunophenotype; Molecular genetic pathogenesis
DOI: 10.1309/WYACYWF6NGM3WBRT
A b s t r a c t
Leukemia cutis (LC) is a nonspecific term used forcutaneous manifestations of any type of leukemia. LChas a wide range of cutaneous manifestations, whichcan make it difficult to clinically distinguish LC fromother skin lesions. Patients with LC usually haveconcomitant systemic leukemia, but occasionally skininvolvement precedes the involvement of the bonemarrow or peripheral blood. Thus, a skin biopsy can bethe first indication of the presence of leukemia in asubset of patients. The immunophenotyping of routinelyprocessed skin biopsy specimens is very useful inestablishing the diagnosis of LC. Although themolecular mechanisms explaining the pathogenesis ofLC are not well defined, chemokine receptors andadhesion molecules may have an important role in skintropism. We review the literature and recent advancespertaining to LC, with special emphasis on theimmunohistochemical assessment and possiblemechanisms involved in skin tropism by leukemic cells.
Leukemia cutis is defined as cutaneous infiltration by neo-plastic leukocytes (myeloid or lymphoid), resulting in clinical-ly identifiable cutaneous lesions.1 When composed of neoplas-tic granulocytic precursors, leukemia cutis has been designatedas myeloid sarcoma, granulocytic sarcoma, primaryextramedullary leukemia, or chloroma.2 When composed ofneoplastic monocytic precursors (monoblasts and promono-cytes), leukemia cutis also has been designated as monoblasticsarcoma.2 The terms myeloid sarcoma and extramedullarymyeloid cell tumor have also been used to include both granu-locytic and monocytic tumors.3,4
Leukemia cutis has been described in patients with acutemyeloid leukemia, chronic myeloproliferative disease, includingchronic myelogenous leukemia (CML), myelodysplastic syn-dromes, and myelodysplastic/lymphoproliferative diseases ❚Table
1❚.2 In patients with chronic diseases, skin involvement is associ-ated with transformation into a blastic phase and suggests diseaseprogression. Leukemia cutis is used as the term for lymphocyticleukemias involving skin that are also designated by their specif-ic diagnosis, such as precursor B- or T-cell lymphoblasticleukemia/lymphoma and chronic lymphocytic leukemia.
In this review article, we discuss the various types ofleukemia most frequently represented in leukemia cutis asdefined by the World Health Organization classification.4 Wefocus on the immunophenotypic features of leukemia cutisand will discuss the possible molecular mechanisms responsi-ble for the migration of leukemic cells to the skin.
Clinical Manifestations
Frequency
Overall, leukemia cutis occurs in 10% to 15% of patientswith acute myeloid leukemia (AML) and less frequently in
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

Am J Clin Pathol 2008;129:130-142 131131 DOI: 10.1309/WYACYWF6NGM3WBRT 131
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
chronic myeloproliferative diseases.5 The frequency ofleukemia cutis differs widely for the various types of AML.Skin involvement can be seen up to 50% of patients withacute myelomonocytic (AMMoL) and monocytic (AMoL)types.6,7 Skin involvement can also be seen in patients withchronic myelomonocytic leukemia,8-11 while skin involve-ment in acute erythroid leukemia and erythroleukemia isexceptional.12-14
Regarding lymphocytic leukemias, skin involvement hasbeen described in 4% to 20% of chronic lymphocyticleukemia/small lymphocytic lymphoma (CLL/SLL) cases andin 20% to 70% of mature T-cell leukemias, including adult T-cell leukemia,15-17 T-cell prolymphocytic leukemia (T-PLL),18-20 and Sézary syndrome (SS). In contrast, leukemiacutis is unusual in patients with precursor B- or T-cell lym-phoblastic leukemia/lymphomas (1%)21-23 and plasma cellmyeloma.24-26
The frequency of leukemia cutis seems to be higheramong children than adults; as many as 25% to 30% of infantswith congenital leukemia develop skin involvement.27,28 Suchcases of congenital acute leukemia are most frequently AML(two thirds of cases). Acute lymphoblastic leukemia (ALL) isless frequent.
Clinical Presentation
Patients with leukemia cutis may have single or multipleskin lesions.29 The lesions are usually described as violaceous,red-brown, or hemorrhagic papules, nodules, and plaques ofvarying sizes.30 Erythematous papules and nodules are report-ed as the most common clinical presentation ❚Image 1A❚.29
Legs are involved most commonly, followed by arms, back,chest, scalp, and face.31 Leukemic infiltration tends to prefer-entially occur at sites of previous or concomitant inflamma-tion ❚Image 1B❚.31,32 A particular type of leukemia can pro-duce different skin lesions during the course of the disease,even in the same patient.29
Most cases of leukemia cutis occur after a diagnosis ofsystemic leukemia has been established. Concomitantinvolvement of skin and systemic leukemia have beenobserved in up to one third of the cases, and, occasionally(<10% of cases), skin infiltration can occur before bone mar-row or peripheral blood involvement and in the absence ofsystemic symptoms.33 The term “aleukemic leukemia cutis”or “primary extramedullary leukemia” has been used for thisuncommon event, which occurs predominantly in patientswith AML.33,34 Aleukemia cutis lesions are usually wide-spread and papulonodular.35
There are no consistent demographic and/or clinical dif-ferences between patients with leukemia with or withoutleukemia cutis regarding sex, age, WBC count, hemoglobinconcentration, platelet count, and fibrinogen level. Higherserum levels of lactate dehydrogenase and/or β2-microglobulin
have been reported in patients with leukemia cutis than inpatients without leukemia cutis.36,37
Up to 30% of children with congenital leukemia haveskin infiltration,28 and this is one of the causes of the “blue-berry muffin” appearance.28 Most pediatric patients withleukemia cutis have high leukemic tumor load andhepatosplenomegaly.38,39
Unusual clinical presentations of leukemia includemarked thickening of the gums and oral petechiae inAMoL,30 leonine faces in AMMoL, eczematous lesions,40
penile or scrotal ulcers,41 and panniculitis resembling erythe-ma nodosum.42 As many as 90% of patients with leukemiacutis also have involvement of other extramedullary sites,with involvement of the meninges particularly frequent (40%of the cases).34
Nonleukemic cutaneous manifestations of leukemia(also knows as leukemids) are more common than leukemiacutis; they occur in 40% or more of patients withleukemia.43 These cutaneous lesions are mostly a manifes-tation of cytopenias and drug reactions. These includepetechiae, purpura, ecchymoses, leukocytoclastic vasculitis,neutrophilic dermatoses (Sweet syndrome and pyodermagangrenosum), and opportunistic infections, particularlythrush, disseminated herpes zoster, or severe and atypicalpresentations of herpes simplex.43
Diagnostic Features
Histopathologic Findings
The diagnosis of leukemia cutis is based on the morpho-logic pattern of skin infiltration, cytologic features, and, mostimportant, the immunophenotype of the tumor cells.Correlation with clinical data and bone marrow and peripher-al blood findings is often helpful to confirm the diagnosis.
❚Table 1❚Subtypes of Leukemia Involving Skin
Myeloid/monocytic disordersAcute myeloid leukemiaAcute myelomonocytic leukemiaAcute monocytic leukemiaChronic myelogenous leukemiaChronic myelomonocytic leukemia (transformation)Myelodysplastic syndromes (transformation)
Lymphoproliferative disordersB-cell leukemias/lymphomas
Precursor B-cell acute lymphoblastic leukemiaChronic lymphocytic leukemia/small lymphocytic lymphoma
T-cell leukemias/lymphomasPrecursor T-cell acute lymphoblastic leukemiaAdult T-cell leukemia/lymphomaT-cell prolymphocytic leukemiaSézary syndrome
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

132 Am J Clin Pathol 2008;129:130-142132 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
A B
C D
E F
❚❚Image 1❚❚ A, Multiple variably sized red-brown papules on the upper extremity skin in a patient with granulocytic sarcoma. B,The leukemic infiltration of chronic lymphocytic leukemia occurred in a scar of previous herpes zoster infection. C, D, and E,At low-power magnification, most types of leukemic infiltrates in skin show superficial and deep perivascular and periadnexalpatterns of involvement (C, H&E, ×40; E, H&E, ×20) or a diffuse infiltrate involving the dermis and subcutis (D, H&E, ×40; inset,×40). The upper papillary dermis is usually spared (Grenz zone) (E, arrow). F, Rare cases can manifest as a subtle superficialinterstitial infiltrate of atypical leukemic cells (H&E, ×20; inset, ×40).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

Am J Clin Pathol 2008;129:130-142 133133 DOI: 10.1309/WYACYWF6NGM3WBRT 133
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
In general, at low-power magnification, most types ofleukemic skin infiltrates show a perivascular and/or periadnex-al pattern of involvement ❚Image 1C❚ and ❚Image 1E❚ or a densediffuse/interstitial ❚Image 1D❚ or nodular infiltrate involving thedermis and subcutis (Image 1D, inset) with sparing of theupper papillary dermis (Grenz zone) (Image 1E, arrow). Rarecases present as a subtle superficial interstitial infiltrate ❚Image
1F❚. Stromal fibrosis is often seen and is associated with anytype of leukemic infiltrates. Based on histologic findings alone,it is often impossible to assign lineage, which is essential forclassification (myeloid, monocytic, or precursor B- or T-cell).
Myeloid (Granulocytic) SarcomaThe infiltrate is nodular with a perivascular-periadnexal dis-
tribution or interstitial and diffuse ❚Image 2A❚ and ❚Image 2B❚.Epidermotropism is unusual. Myeloblasts and granulocytic pre-cursors are the predominant cell components. The neoplasticcells are usually large, with relatively abundant eosinophiliccytoplasm and large nuclei with blastic (finely dispersed) chro-matin and occasional small nucleoli. Mitotic figures are usuallyprominent. Scattered macrophages and mature granulocytes canbe frequently seen. Focal involvement with destruction ofnerves, sebaceous glands, and muscle bundles is not unusual.44
Myeloid (Monoblastic) SarcomaThe infiltrate can be nodular with a perivascular or peri-
adnexal distribution or interstitial and/or diffuse. Involvementof the subcutaneous tissue can be seen. Epidermotropism israrely seen. The skin infiltrates in AMoL ❚Image 2C❚ orAMMoL ❚Image 2D❚ cases are composed of cells with blasticchromatin and promonocytic features (large cleaved nuclei,small nucleoli, and amphophilic cytoplasm). Skin involve-ment of chronic myelomonocytic leukemia is common andshows histologic features similar to those found in AMMoL.
Precursor B- or T-Cell Acute Lymphoblastic Leukemia/Lymphoma
The most common clinical presentation is one or multiplecutaneous nodules. The cytomorphologic features of precursorB- and T-cell lymphoblastic leukemia/lymphoma are virtuallyidentical. Typically, the infiltrates are deep seated and lack epi-dermotropism. The pattern of infiltration can be perivascularand/or diffuse ❚Image 2E❚. Morphologically, the cells have usu-ally a monomorphous appearance, being intermediate in sizewith round nuclear contours and blastic chromatin (Image 2E,inset). Frequently, numerous mitotic and apoptotic figures arepresent.23 Stromal fibrosis is frequently seen.
Chronic Lymphocytic Leukemia/Small Lymphocytic LeukemiaLeukemia cutis has been reported in 4% to 20% of
patients with CLL/SLL. Three main architectural patterns arerecognized: (1) perivascular and periadnexal, (2) nodular and
diffuse ❚Image 2F❚, and (3) band-like.45 Cytologically, the infil-trates are characterized by a relatively monotonous populationof small lymphoid cells with round nuclear contours (Image 2F,inset). A distinctive characteristic feature of CLL/SLL, if thebiopsy specimen size and degree of infiltration are largeenough, is the presence of proliferation centers (aggregates ofprolymphocytes and paraimmunoblasts). In some cases, thelesions are confined to sites affected by previous inflammatoryor infectious conditions such as Borrelia burgdorferi, herpeszoster (Image 1B), and herpes simplex.32,46 In other cases,leukemic infiltrates are seen associated with primary cutaneousepithelial neoplasms.47,48 Compared with CLL/SLL, othermature B-cell lymphoid neoplasms rarely involve skin, often atthe time of end-stage disease.
T-Cell Lymphoproliferative DiseasesAdult T-cell leukemia/lymphoma (ATLL) is a neoplasm of
CD4+ mature T lymphocytes for which human T-cell lym-photropic virus type I (HTLV-1) is the proven etiologic agent.ATLL commonly involves the skin, peripheral blood, andlymph nodes. Cutaneous lesions of ATLL are polymorphousin appearance; skin lesions are frequently observed in all clin-ical subtypes (acute, chronic, lymphoma, and smoldering),and their incidence is reported to vary from 43% to 72%.49 Aprimarily cutaneous subtype of ALL has also been proposed.
It is often difficult to distinguish cutaneous lesions ofATLL from those of mycosis fungoides (MF) because onethird of cutaneous lesions of ATLL show a superficial band-like infiltrate with epidermotropism and Pautrier-likemicroabscesses. Unlike MF, epithelial necrosis and a deep-seated perivascular infiltrate ❚Image 2G❚, sometimes accom-panied by angioinvasion, can be seen in ATLL.50,51 The skininfiltrates can be heterogeneous with small, medium, large,mixed, or pleomorphic T cells (Image 2G, inset). Some caseshave shown prominent granulomatous inflammation.52 Insuspected cases of ATLL, serologic confirmation of HTLV-1infection is essential but circumstantial evidence of the roleof virus in pathogenesis; confirmation of monoclonal inte-gration of the HTLV-1 proviral genome is definitive proof ofcausation.
T-PLL is the most common type of mature T-cellleukemia and is characterized, in most cases, by a rapidly ris-ing peripheral blood lymphocyte count, bone marrow involve-ment, and splenomegaly. Skin involvement and serous effu-sions, especially pleural, are encountered fairly often in thesecases.19 The reported incidence of skin involvement rangesfrom 25% to 30%.53 The face is frequently involved, with orwithout associated swelling and relative infrequency of anerythrodermic cutaneous presentation, compared with otherforms of primary cutaneous T-cell lymphomas.18 Also charac-teristic is the petechial and/or purpuric quality of the lesionsdue to RBC extravasation.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

134 Am J Clin Pathol 2008;129:130-142134 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
The skin infiltrate usually involves the upper dermis with aperivascular and periadnexal distribution ❚Image 2H❚ and lessfrequently has a diffuse pattern.19,53 Other histologic featuresinclude variable degree of stromal edema surrounding bloodvessels, minimal endothelial damage (without fibrin deposi-tion), RBC extravasation and hemosiderin deposition, and fociof epidermotropism. Rarely, the tumor forms a subcutaneous
mass. The cytologic features of T-PLL in routinely stained tis-sue sections are heterogeneous. T-PLL cells are slightly largerthan normal lymphocytes, frequently having relatively roundnuclear contours (Image 2H, inset). Prominent nucleoli arecharacteristic but not always present; their presence is bestdetected under oil. Some cases demonstrate highly irregularnuclei (Sézary-like cells) without prominent nucleoli.54
A CB
FED
❚❚Image 2❚❚ A and B, Granulocytic sarcoma. The infiltrate shows perivascular and diffuse distribution with Grenz zone (A, H&E,×200; B, H&E, ×100). Myeloblasts and granulocytic precursors are large, with relatively abundant eosinophilic cytoplasm andlarge nuclei with blastic (finely dispersed) chromatin and occasional small nucleoli. Focal involvement with destruction of nervesis also noted. C and D, Monoblastic sarcoma. The skin infiltrates of the acute monocytic leukemia (C, H&E, ×200) or acutemyelomonocytic leukemia (D, H&E, ×400) are composed of a monomorphous population of monoblasts and promonocyteswith large cleaved nuclei with amphophilic cytoplasm. E, Pre-B acute lymphoblastic leukemia (ALL). The perivascular andperiadnexal leukemic infiltrates of pre-B ALL (H&E, ×40) are medium to small tumor cells with round contours, scant cytoplasm,and finely dispersed chromatin (inset, ×400). F, Chronic lymphocytic leukemia (CLL). This case involving the skin is characterizedby the interstitial infiltrates of small to medium-sized lymphocytes in the dermis (H&E, ×40; inset, ×400). Note the presence offocal pseudoepitheliomatous hyperplasia of the epidermis adjacent to the CLL infiltrates.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

Am J Clin Pathol 2008;129:130-142 135135 DOI: 10.1309/WYACYWF6NGM3WBRT 135
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
SS is a clonal T-cell lymphoproliferative disorder involvingthe blood, skin, and lymph nodes that manifests with erythroder-ma and circulating cerebriform lymphocytes. By convention, SSis regarded as a variant of MF because the cytologic andimmunophenotypic features of the neoplastic cells are identi-cal to those described in MF. In addition, patients with long-standing patches and plaques from MF may subsequentlyexhibit circulating neoplastic cells indistinguishable from pri-mary SS. However, differences in clinical outcomes have beennoted in that patients with primary SS typically experience amore aggressive disease course.55
Skin biopsy specimens show a perivascular dermal infil-trate and/or interstitial dermal infiltration. In most skin biopsyspecimens, the infiltrate is located in upper and mid dermis.Lichenoid infiltrates are present to some degree in 15% of thecases, and a dense band-like infiltrate is present in 5% ❚Image
2I❚.56 Although epidermotropism is part of the classical defini-tion of SS (Image 2I, arrow), a significant proportion of patientswith SS lack epidermotropism.56 The infiltrates are usuallycomposed of small or medium lymphoid cells, with variablenumbers of morphologically atypical hyperchromatic lympho-cytes with irregular nuclear contours (Image 2I, inset). Thepresence of atypical, larger perivascular lymphocytes is a usefuldiagnostic key to recognizing primary SS. Parakeratosis, acan-thosis, and spongiosis can be seen in most cases.
Immunophenotypic FindingsThe diagnosis of leukemia cutis alone is nonspecific, and
immunophenotyping is very important for generating a specific,clinically useful diagnosis. Most skin biopsy specimensinvolved by leukemia cutis are usually small punch biopsyspecimens that are routinely fixed and processed. Fortunately,many T-cell, B-cell, and myeloid markers can be used in theassessment of formalin-fixed sections, especially when anti-gen-retrieval techniques are used.57 Touch imprints of thebiopsy specimen for cytochemistry can also be very helpfulfor diagnosis.
A summary of the immunophenotypic profile of the dif-ferent types of leukemia cutis is shown in ❚Table 2❚. In addi-tion, a systematic approach useful for immunophenotypiccharacterization of leukemic infiltrates is given in ❚Figure 1❚.
Myeloid SarcomaMyeloperoxidase (MPO) and lysozyme are helpful in dis-
criminating between myeloid and nonmyeloid cells. MPO isstrongly positive in most neoplasms of granulocytic lineage,and it can be weakly positive in a subset of monocytic neo-plasms ❚Image 3A❚. Rarely, precursor B-cell lymphoblasticleukemia/lymphoma is MPO+. Lysozyme is a marker forgranulocytes, monocytes, and macrophages and is positive inmyeloid and monocytic neoplasms but negative in lymphoid
IHG
G, Adult T-cell leukemia/lymphoma. The leukemic infiltrate is superficial and deep perivascular (H&E,×20). The tumor cells areheterogeneous, ranging in size from small to large (inset, ×200). In this case, human T-cell lymphotropic virus type 1 infection wasconfirmed serologically. H, T-cell prolymphocytic leukemia (T-PLL). The skin infiltrate involves the upper and deep dermis with aperivascular and periadnexal distribution (H&E, ×20). T-PLL cells are slightly larger than normal lymphocytes with moderatelyabundant basophilic cytoplasm (inset, ×400). Note the presence of the characteristic extravasation of RBCs admixed with thetumor cells. I, A case of secondary Sézary syndrome involving the skin shows a band-like dermal infiltrate in upper dermisindistinguishable from the infiltrates of mycosis fungoides (H&E, ×40). Note the presence of a Pautrier microabscess (arrow). Sometumor cells have convoluted nuclei (inset, ×200). Hyperkeratosis, parakeratosis, and acanthosis are associated.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

136 Am J Clin Pathol 2008;129:130-142136 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
❚Table 2❚Immunophenotypic Profile of Leukemia Cutis
Leukemia/Lymphoma
Myeloid/Monocytoid LeukemiaB-Cell T-Cell
Granulocytic MonoblasticMarker Sarcoma Sarcoma Pre-B-ALL CLL/SLL Pre-T-ALL ATLL T-PLL SS
MPO + –/+ –/+ – –/+ – – –Lysozyme + + – – – – – –CD56 –/+ + – – – – – –CD68 (PG-M1) – + – – – – – –CD117 + –/+ – – –/+ – –/+ –TdT –/+ – + – + – – –CD34 + – + – + – – –CD10 – –/+ + – + – – –CD19 –/+ – + + –/+ – – –CD20 – – –/+ + – – – –CD23 – –/+ – + – – – –Pax5/BSAP – – + + – – – –CD138 – – – – – – – –CD79a – – + + – – – –CD3 – – – – + (cyto) + + +CD4 –/+ + – – + + + +CD5 – – – + + + + –/+CD7 –/+ –/+ – – + –/+ + –/+CD8 – – – – + – + –CD43 + + + + + + + +CD45 + + –/+ + + + + +TCL-1 – – – – – – + –
ALL, acute lymphoblastic leukemia; ATLL, adult T-cell leukemia/lymphoma; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; cyto, cytoplasmicexpression; MPO, myeloperoxidase; SS, Sézary syndrome; TCL-1, T-cell leukemia-1; TdT, terminal deoxynucleotidyl transferase; T-PLL, T-cell prolymphocytic leukemia.
Leukemia Cutis
Myeloid disordersMPO+Lysozyme+
CD56–/+CD68 (PGM1)–CD117+CD34+TdT–/+
PAX-5/BSAP+CD79a+
CD3 (cyto)+CD79a–CD1a+CD4+CD8+
CD3+CD4+CD8–CD7–/+CD25+CD45RO–/+CD45RA–/+
CD3+CD4+CD8–/+CD7+CD25–/+CD45RO+CD45RA–TCL–1+
CD3–/+CD4+CD8–/+CD7– (usually)CD25–/+CD45RO+CD45RA–
CD56+CD68 (PGM1)+CD117–/+CD34–TdT–
TdT+MPO– or –/+CD10+
TdT–MPO–
CD5+CD19+CD20+CD23+Cyclin D1–
MPO– or –/+Lysozyme–
Mature B-cell leukemia
Lymphoproliferative disorders
Mature T-cell leukemias
CLL
Myeloid
AML AMoL AMMoL ALL
ATLLT-PLL SS
B-cellALL
T-cellALL
CML
Monocytic
❚❚Figure 1❚❚ Systematic immunophenotypic assessment of leukemia cutis using a panel of CD markers. ALL, acute lymphoblasticleukemia; AMoL, acute monocytic leukemia; AMMoL, acute myelomonocytic leukemia; ATLL, adult T-cell leukemia/lymphoma;CLL, chronic lymphocytic leukemia; MPO, myeloperoxidase; SS, Sézary syndrome; TdT, terminal deoxynucleotidyl transferase; T-PLL, T-cell prolymphocytic leukemia.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

Am J Clin Pathol 2008;129:130-142 137137 DOI: 10.1309/WYACYWF6NGM3WBRT 137
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
CBA
FED
❚❚Image 3❚❚The tumor cells of granulocyticsarcoma are strongly positive formyeloperoxidase (A, ×10) and lysozyme(B, ×10). CD68 is frequently positive inmonoblastic sarcoma (C, ×400). CD117is usually positive in granulocyticsarcoma involving the dermis (D, ×100).The combined expression of PAX-5/BSAP (E, ×400) and TdT (F, ×400) isvery useful to diagnose precursor B-acute lymphoblastic leukemia. The tumorcells of adult T-cell leukemia/lymphomaare characteristically positive for CD4 (G,×10) and negative for CD8 (inset, ×10).The Sézary syndrome cells involving skinare also positive for CD4 (H, ×100).
HG
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

138 Am J Clin Pathol 2008;129:130-142138 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
neoplasms ❚Image 3B❚. CD56 is a neural cell adhesion mole-cule expressed by natural killer cells and a subset of T cellsand monocytes. Its expression is well recognized in a numberof neoplasms, including AML, especially with monocytic dif-ferentiation. In 1 study, however, CD56 expression was notassociated with the presence of leukemia cutis in patients withAML.58 CD68/KP-1 produces a cytoplasmic granular positiv-ity in most of the AMLs. However, the KP-1 antibody reactswith a lysosomal antigen and is less specific than the PG-M1antibody, which is more restricted to monocytic neoplasms❚Image 3C❚. CD117, a c-kit product, is positive in AML,including the myeloblastic component of AMMoL ❚Image
3D❚. However, the majority of AMoL cases are negative.CD117 is not specific, however, and other hematopoietictumors expressing CD117 include mast cell proliferations,plasma cell neoplasms, a subset of precursor T-lymphoblasticleukemia/lymphoma, and rare T-cell lymphomas.
Precursor B-Cell Lymphoblastic Leukemia/LymphomaPax-5/BSAP is a B cell–specific transcription factor that
is detectable at the pro–B-cell stage and subsequently in allfurther stages of B-cell development until the plasma cellstage, when it is down-regulated.59 The combination Pax-5/BSAP and terminal deoxynucleotidyl transferase (TdT) isvery useful to identify precursor B-cell lymphoblasticleukemia/lymphoma ❚Image 3E❚ and ❚Image 3F❚. However,Pax-5/BSAP is also expressed by AML associated witht(8;21).60 CD10, CD19, and CD79a are positive in most cases.CD45 expression may be absent.
Mature B-Cell NeoplasmsIn CLL/SLL, the neoplastic lymphocytes are positive for
CD5, CD20, CD23, and CD43 and negative for CD10.
Precursor T-Cell Lymphoblastic Leukemia/LymphomaThese neoplasms are positive for CD1a, CD3, CD10, and
TdT. CD3 in combination with TdT and/or CD1a is the mostspecific marker for the identification of precursor T-cell lym-phoblastic leukemia/lymphoma. Other useful T cell–associat-ed markers are CD2, CD4, CD5, and CD8. A subset of casesexpresses CD4 and CD8. CD99 is usually positive. It is alsoimportant to remember that CD99 can be expressed in non-hematopoietic tumors and should not be considered a markerof lymphoblastic leukemia/lymphoma.
Adult T-Cell Leukemia/LymphomaThe neoplastic cells express CD2, CD3, CD4 ❚Image 3G❚,
and CD5; a decrease in the expression of CD7 is often noted.There is increased expression of the interleukin-2α receptor,best evaluated by an antibody against CD25.61 There is noexpression of cytotoxic proteins TIA-1 and granzyme B.CD1a and TdT are negative.
T-Cell Prolymphocytic Leukemia
Most cases are positive for CD3, CD4, CD45RO, and T-cell leukemia-1 (TCL-1) and negative for CD1a, CD34, andTdT.20 CD4 and CD8 are coexpressed in 25% of the cases;rarely, CD4 and CD8 are both absent.62 The majority of T-PLLtumors show chromosomal rearrangement involving chromo-some 14 that transcriptionally activates the TCL-1 gene at14q32 through juxtaposition of the T-cell receptor enhancer/promoter sequence.
Sézary SyndromeThe immunophenotype of tumor cells in primary and sec-
ondary SS is similar.56 Most cases are positive for CD3, CD4❚Image 3H❚, CD25, and CD45RO.20,56 Diminished or loss ofexpression of CD7 and CD26 is usually seen. The larger atyp-ical cells may be CD5– and can express CD30.
Molecular Findings and Pathogenesis
A variety of chromosomal abnormalities have beenreported in patients with AML with leukemia cutis.5,34 Itseems likely reasonable to conclude that most of the molecu-lar abnormalities closely mirror those shown for AML in bonemarrow. Relatively few molecular data have been generatedfrom the assessment of leukemia cutis specimens directly. Itseems that abnormalities of chromosome 8 are significantlymore common in patients with AML with leukemia cutis thanin patients with AML without leukemia cutis.5,34,63 Agis et al5
showed that numerical abnormalities of chromosome 8 weresignificantly more common in patients with AML withleukemia cutis (5/14 cases [36%]) than in patients withoutleukemia cutis (10/355 [2.8%]). Sen et al64 demonstrated that7 of 11 patients with AMoL with leukemia cutis showed tri-somy 8 detected by fluorescence in situ hybridization. Thereare also isolated cases reported of tetrasomy 8 and pentasomy8.5,34,65-69 It is currently unknown what genes or epigeneticeffects are impacted by aneuploidy of chromosome 8 thatpotentially predispose to leukemia cutis in patients with AML.Molecular genetic studies in other subtypes of leukemiainvolving the skin are also very limited.
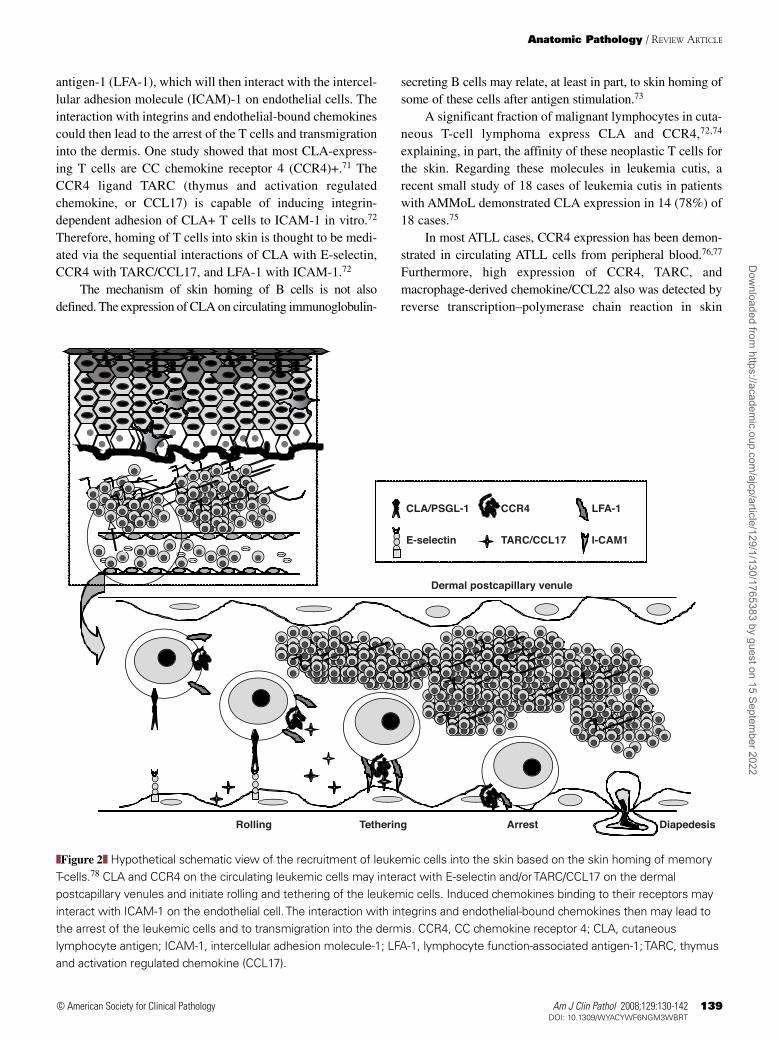
The underlying molecular basis responsible for themigration of leukemic cells to the skin is not defined.Homing to specific tissues is controlled by the combinedexpression of different chemokine receptors and specificadhesion molecule receptors. For example, homing to theskin of memory T cells is regulated by coexpression of cuta-neous lymphocyte antigen (CLA) with specific chemokinereceptors.70 CLA on the T cells interacts with E-selectin onthe dermal postcapillary venules and initiates rolling and teth-ering of T cells on the endothelial cells. Chemokine bindingto T-cell receptors activates lymphocyte function–associated
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022
Am J Clin Pathol 2008;129:130-142 139139 DOI: 10.1309/WYACYWF6NGM3WBRT 139
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
antigen-1 (LFA-1), which will then interact with the intercel-lular adhesion molecule (ICAM)-1 on endothelial cells. Theinteraction with integrins and endothelial-bound chemokinescould then lead to the arrest of the T cells and transmigrationinto the dermis. One study showed that most CLA-express-ing T cells are CC chemokine receptor 4 (CCR4)+.71 TheCCR4 ligand TARC (thymus and activation regulatedchemokine, or CCL17) is capable of inducing integrin-dependent adhesion of CLA+ T cells to ICAM-1 in vitro.72
Therefore, homing of T cells into skin is thought to be medi-ated via the sequential interactions of CLA with E-selectin,CCR4 with TARC/CCL17, and LFA-1 with ICAM-1.72
The mechanism of skin homing of B cells is not alsodefined. The expression of CLA on circulating immunoglobulin-
secreting B cells may relate, at least in part, to skin homing ofsome of these cells after antigen stimulation.73
A significant fraction of malignant lymphocytes in cuta-neous T-cell lymphoma express CLA and CCR4,72,74
explaining, in part, the affinity of these neoplastic T cells forthe skin. Regarding these molecules in leukemia cutis, arecent small study of 18 cases of leukemia cutis in patientswith AMMoL demonstrated CLA expression in 14 (78%) of18 cases.75
In most ATLL cases, CCR4 expression has been demon-strated in circulating ATLL cells from peripheral blood.76,77
Furthermore, high expression of CCR4, TARC, andmacrophage-derived chemokine/CCL22 also was detected byreverse transcription–polymerase chain reaction in skin
CLA/PSGL-1
Dermal postcapillary venule
Rolling Tethering Arrest Diapedesis
E-selectin
CCR4
TARC/CCL17
LFA-1
I-CAM1
❚❚Figure 2❚❚ Hypothetical schematic view of the recruitment of leukemic cells into the skin based on the skin homing of memory T-cells.78 CLA and CCR4 on the circulating leukemic cells may interact with E-selectin and/or TARC/CCL17 on the dermalpostcapillary venules and initiate rolling and tethering of the leukemic cells. Induced chemokines binding to their receptors mayinteract with ICAM-1 on the endothelial cell. The interaction with integrins and endothelial-bound chemokines then may lead tothe arrest of the leukemic cells and to transmigration into the dermis. CCR4, CC chemokine receptor 4; CLA, cutaneouslymphocyte antigen; ICAM-1, intercellular adhesion molecule-1; LFA-1, lymphocyte function-associated antigen-1; TARC, thymusand activation regulated chemokine (CCL17).
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

140 Am J Clin Pathol 2008;129:130-142140 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
lesions of patients with ATLL. Therefore, the presence of sim-ilar chemokine receptors and adhesion molecules in leukemiccells and normal memory T cells may explain the tropism ofsome of these leukemias to the skin ❚Figure 2❚.78
Avigdor et al79 reported 2 cases of plasma cell myelomawith extramedullary progression (1 case with skin involvement)despite a good response to thalidomide in bone marrow. Variouscell adhesion molecules expressed by plasma cell myelomacells also mediate homing of those cells to bone marrow anddisease progression.79,80 It has been suggested that thalidomide,by altering cell adhesion molecules involved in the homing ofplasma cells into the bone marrow, may facilitate plasma cellmobilization from the bone marrow into the circulation andtoward extramedullary sites. A similar hypothesis has beenmentioned in patients with AML treated with all-trans-retinoicacid in whom isolated extramedullary relapse developed.81
Treatment and Prognosis
Leukemia cutis is a local manifestation of an underlyingsystemic disease; therefore, the treatment should be aimed ateradicating the systemic disease by using systemic chemother-apy, as well as local therapy.
In general, the development of leukemia cutis portends apoor prognosis. Several studies indicate that, in the presenceof leukemia cutis in patients with AML or CML, the diseasewill follow a aggressive course and the survival is short.6 Su33
reported that 88% of patients with leukemia cutis die within 1year of the diagnosis. Patients with congenital leukemia seemto be an exception because leukemia cutis does not confer aworse prognosis in this clinical setting.27
From the Departments of 1Pathology, The Methodist Hospital;2Hematopathology and 3Dermatopathology, The University ofTexas M.D. Anderson Cancer Center, Houston.
Address reprint requests to Dr Vega: Dept ofHematopathology, The University of Texas M.D. Anderson CancerCenter, 1515 Holcombe Blvd, Houston, TX, 77030.
References1. Weedon D. Cutaneous infiltrates: lymphomatous and
leukemic. Skin Pathology. 2nd ed. New York, NY: ChurchillLivingstone; 2002:1118-1120.
2. Brunning RD, Matutes E, Flandria F, et al. In: Jaffe ES, HarrisNL, Stein H, et al, eds. World Health Organization Classificationof Tumors: Pathology and Genetics of Tumors of Haematopoieticand Lymphoid Tissues. Lyon, France: IARC Press; 2001:104-105.
3. Davey FR, Olson S, Kuree AS, et al. The immunophenotypingof extramedullary myeloid cell tumors in paraffin-embeddedtissue sections. Am J Surg Pathol. 1988;12:699-707.
4. Roth MJ, Medeiros LJ, Elenitoba-Johnson K, et al. Extramedullarymyeloid cell tumors: an immunohistochemical study of 29cases using routinely fixed and processed paraffin-embeddedtissue sections. Arch Pathol Lab Med. 1995;119:790-798.
5. Agis H, Weltermann A, Fonatsch C, et al. A comparativestudy on demographic, hematological, and cytogeneticfindings and prognosis in acute myeloid leukemia with and without leukemia cutis. Ann Hematol. 2002;81:90-95.
6. Kaddu S, Zenahlik P, Beham-Schmid C, et al. Specificcutaneous infiltrates in patients with myelogenous leukemia: a clinicopathologic study of 26 patients with assessment ofdiagnostic criteria. J Am Acad Dermatol. 1999;40:966-978.
7. Horlick HP, Silvers DN, Knobler EH, et al. Acutemyelomonocytic leukemia presenting as a benign-appearingcutaneous eruption. Arch Dermatol. 1990;126:653-656.
8. Dyachenko P, Rozenman D, Bennett M. Unusual skin andtesticular lesions in a patient with CMML. Eur J Intern Med.2006;17:290-291.
9. Copplestone JA, Oscier DG, Mufti GJ, et al. Monocytic skininfiltration in chronic myelomonocytic leukaemia. Clin LabHaematol. 1986;8:115-119.
10. Braga D, Manganoni AM, Boccaletti V, et al. Specific skininfiltration as first sign of chronic myelomonocytic leukemiawith an unusual phenotype. J Am Acad Dermatol.1996;35:804-807.
11. Elenitoba-Johnson K, Hodges GF, King TC, et al.Extramedullary myeloid cell tumors arising in the setting ofchronic myelomonocytic leukemia: a report of two cases. ArchPathol Lab Med. 1996;120:62-67.
12. Shaklai M, Nir M, Feuerman E, et al. Cutaneous involvementin erythroleukemia: report of a case. Dermatologica.1974;149:385-387.
13. Mizukoshi N, Sato K, Sano S. A case of erythroleukemia withskin involvement [in Japanese]. Nippon Hifuka Gakkai Zasshi.1985;95:585-590.
14. Janier M, Raynaud E, Blanche P, et al. Leukaemia cutis anderythroleukaemia. Br J Dermatol. 1999;141:372-373.
15. Siegel RS, Gartenhaus RB, Kuzel TM. Human T-celllymphotropic-I–associated leukemia/lymphoma. Curr TreatOptions Oncol. 2001;2:291-300.
16. Dosaka N, Tanaka T, Miyachi Y, et al. Examination of HTLV-Iintegration in the skin lesions of various types of adult T-cellleukemia (ATL): independence of cutaneous-type ATLconfirmed by Southern blot analysis. J Invest Dermatol.1991;96:196-200.
17. Hamada T, Setoyama M, Katahira Y, et al. Differences inHTLV-I integration patterns between skin lesions andperipheral blood lymphocytes of HTLV-I seropositive patientswith cutaneous lymphoproliferative disorders. J Dermatol Sci.1992;4:76-82.
18. Magro CM, Morrison CD, Heerema N, et al. T-cellprolymphocytic leukemia: an aggressive T cell malignancywith frequent cutaneous tropism. J Am Acad Dermatol.2006;55:467-477.
19. Valbuena JR, Herling M, Admirand JH, et al. T-cellprolymphocytic leukemia involving extramedullary sites. Am J Clin Pathol. 2005;123:456-464.
20. Herling M, Khoury JD, Washington LT, et al. A systematicapproach to diagnosis of mature T-cell leukemias revealsheterogeneity among WHO categories. Blood. 2004;104:328-335.
21. Yen A, Sanchez R, Oblender M, et al. Leukemia cutis: Darier’ssign in a neonate with acute lymphoblastic leukemia. J AmAcad Dermatol. 1996;34:375-378.
22. Sander CA, Medeiros LJ, Abruzzo LV, et al. Lymphoblasticlymphoma presenting in cutaneous sites: a clinicopathologicanalysis of six cases. J Am Acad Dermatol. 1991;25:1023-1031.
23. Ali R, Ozan U, Ozkalemkas F, et al. Leukaemia cutis in T-cellacute lymphoblastic leukaemia. Cytopathology. 2006;17:158-161.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022
Am J Clin Pathol 2008;129:130-142 141141 DOI: 10.1309/WYACYWF6NGM3WBRT 141
© American Society for Clinical Pathology
Anatomic Pathology / REVIEW ARTICLE
24. Alexandrescu DT, Koulova L, Wiernik PH. Unusual cutaneousinvolvement during plasma cell leukaemia phase in a multiplemyeloma patient after treatment with thalidomide: a case reportand review of the literature. Clin Exp Dermatol. 2005;30:391-394.
25. Bayer-Garner IB, Joseph L, Sanderson RD, et al. Expression ofsyndecan-1 is a sensitive marker for cutaneous plasmacytoma. J Cutan Pathol. 2003;30:18-22.
26. Tsutani H, Sugiyama T, Shimizu S, et al. Discordant LFA-1/ICAM-1 expression in a case of secondary plasma cellleukemia associated with subcutaneous plasmacytoma. Am J Hematol. 1993;42:299-304.
27. Zhang IH, Zane LT, Braun BS, et al. Congenital leukemia cutiswith subsequent development of leukemia. J Am AcadDermatol. 2006;54(2 suppl):S22-S27.
28. Resnik KS, Brod BB. Leukemia cutis in congenital leukemia:analysis and review of the world literature with report of anadditional case. Arch Dermatol. 1993;129:1301-1306.
29. Watson KM, Mufti G, Salisbury JR, et al. Spectrum of clinicalpresentation, treatment and prognosis in a series of eight patientswith leukaemia cutis. Clin Exp Dermatol. 2006;31:218-221.
30. Su WP, Buechner SA, Li CY. Clinicopathologic correlationsin leukemia cutis. J Am Acad Dermatol. 1984;11:121-128.
31. Paydas S, Zorludemir S. Leukaemia cutis and leukaemicvasculitis. Br J Dermatol. 2000;143:773-779.
32. Cerroni L, Zenahlik P, Kerl H. Specific cutaneous infiltrates of B-cell chronic lymphocytic leukemia arising at the site ofherpes zoster and herpes simplex scars. Cancer. 1995;76:26-31.
33. Su WP. Clinical, histopathologic, and immunohistochemicalcorrelations in leukemia cutis. Semin Dermatol. 1994;13:223-230.
34. Baer MR, Barcos M, Farrell H, et al. Acute myelogenousleukemia with leukemia cutis; eighteen cases seen between1969 and 1986. Cancer. 1989;63:2192-2200.
35. Tomasini C, Quaglino P, Novelli M, et al. “Aleukemic”granulomatous leukemia cutis. Am J Dermatopathol.1998;20:417-421.
36. Byrd JC, Edenfield WJ, Shields DJ, et al. Extramedullarymyeloid cell tumors in acute nonlymphocytic leukemia: aclinical review. J Clin Oncol. 1995;13:1800-1816.
37. Marti RM, Pujol RM, Servitje O, et al. Sézary syndrome andrelated variants of classic cutaneous T-cell lymphoma: adescriptive and prognostic clinicopathologic study of 29 cases.Leuk Lymphoma. 2003;44:59-69.
38. Bresters D, Reus AC, Veerman AJ, et al. Congenitalleukaemia: the Dutch experience and review of the literature.Br J Haematol. 2002;117:513-524.
39. Lampkin BC. The newborn infant with leukemia [editorial]. J Pediatr. 1997;131:176-177.
40. O’Connell DM, Fagan WA, Skinner SM, et al. Cutaneousinvolvement in chronic myelomonocytic leukemia. Int JDermatol. 1994;33:628-631.
41. Zax RH, Kulp-Shorten CL, Callen JP. Leukemia cutispresenting as a scrotal ulcer. J Am Acad Dermatol.1989;21:410-413.
42. Sumaya CV, Babu S, Reed RJ. Erythema nodosum–like lesionsof leukemia. Arch Dermatol. 1974;110:415-418.
43. Wong TY, Suster S, Bouffard D, et al. Histologic spectrum ofcutaneous involvement in patients with myelogenousleukemia including the neutrophilic dermatoses. Int JDermatol. 1995;34:323-329.
44. Elder DE, Lever WF, Elenitsas R. Cutaneous lymphoma andleukemias. In: Elder DE, Elenitsas R, Johnson BL, et al, eds.Histopathology of the Skin. 9th ed. Philadelphia, PA: Lippincott;2005:927.
45. Cerroni L, Zenahlik P, Hofler G, et al. Specific cutaneousinfiltrates of B-cell chronic lymphocytic leukemia: aclinicopathologic and prognostic study of 42 patients. Am J Surg Pathol. 1996;20:1000-1010.
46. Cerroni L, Hofler G, Back B, et al. Specific cutaneousinfiltrates of B-cell chronic lymphocytic leukemia (B-CLL) atsites typical for Borrelia burgdorferi infection. J Cutan Pathol.2002;29:142-147.
47. Robak E, Robak T. Skin lesions in chronic lymphocyticleukemia. Leuk Lymphoma. 2007;48:855-865
48. Agnew KL, Ruchlemer R, Catovsky D, et al. Cutaneousfindings in chronic lymphocytic leukaemia. Br J Dermatol.2004;150:1129-1135.
49. Buechner SA, Li CY, Su WP. Leukemia cutis: ahistopathologic study of 42 cases. Am J Dermatopathol.1985;7:109-119.
50. DiCaudo DJ, Perniciaro C, Worrell JT, et al. Clinical andhistologic spectrum of human T-cell lymphotropic virus typeI–associated lymphoma involving the skin. J Am AcadDermatol. 1996;34:69-76.
51. Yamaguchi T, Ohshima K, Karube K, et al.Clinicopathological features of cutaneous lesions of adult T-cell leukaemia/lymphoma. Br J Dermatol. 2005;152:76-81.
52. Higaki Y, Mizushima J, Kawashima M, et al. Cutaneousgranulomas associated with adult T-cell leukemia/lymphoma.Dermatology. 2003;206:157-160.
53. Mallett RB, Matutes E, Catovsky D, et al. Cutaneousinfiltration in T-cell prolymphocytic leukaemia. Br J Dermatol.1995;132:263-266.
54. Garand R, Goasguen J, Brizard A, et al. Indolent course as a relatively frequent presentation in T-prolymphocyticleukaemia. Groupe Francais d’Hematologie Cellulaire. Br J Haematol. 1998;103:488-494.
55. Vonderheid EC, Bernengo MG, Burg G, et al. Update onerythrodermic cutaneous T-cell lymphoma: report of theInternational Society for Cutaneous Lymphomas. J Am AcadDermatol. 2002;46:95-106.
56. Diwan AH, Prieto VG, Herling M, et al. Primary Sézarysyndrome commonly shows low-grade cytologic atypia and anabsence of epidermotropism. Am J Clin Pathol. 2005;123:510-515.
57. Pileri SA, Ascani S, Milani M, et al. Acute leukaemiaimmunophenotyping in bone-marrow routine sections. Br J Haematol. 1999;105:394-401.
58. Seymour JF, Pierce SA, Kantarjian HM, et al. Investigation ofkaryotypic, morphologic and clinical features in patients withacute myeloid leukemia blast cells expressing the neural celladhesion molecule (CD56). Leukemia. 1994;8:823-826.
59. Zhang Z, Espinoza CR, Yu Z, et al. Transcription factor Pax5(BSAP) transactivates the RAG-mediated V(H)-to-DJ(H)rearrangement of immunoglobulin genes. Nat Immunol.2006;7:616-624.
60. Valbuena JR, Medeiros LJ, Rassidakis GZ, et al. Expression ofB cell–specific activator protein/PAX5 in acute myeloidleukemia with t(8;21)(q22;q22). Am J Clin Pathol.2006;126:235-240.
61. Matsushita K, Arima N, Hidaka S, et al. CD8-positive adult T-cell leukemia cells with an integrated defective HTLV-Igenome show a paracrine growth to IL-2. Am J Hematol.1994;47:123-128.
62. Matutes E. T-cell prolymphocytic leukemia. Cancer Control.1998;5:19-24.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022

142 Am J Clin Pathol 2008;129:130-142142 DOI: 10.1309/WYACYWF6NGM3WBRT
© American Society for Clinical Pathology
Cho-Vega et al / LEUKEMIA CUTIS
63. Byrd JC, Lawrence D, Arthur DC, et al. Patients with isolatedtrisomy 8 in acute myeloid leukemia are not cured withcytarabine-based chemotherapy: results from Cancer andLeukemia Group B 8461. Clin Cancer Res. 1998;4:1235-1241.
64. Sen F, Zhang XX, Prieto VG, et al. Increased incidence oftrisomy 8 in acute myeloid leukemia with skin infiltration(leukemia cutis). Diagn Mol Pathol. 2000;9:190-194.
65. Ferrara F, Cancemi D, Friso P, et al. Tetrasomy 8 andt(1;11)(p32;q24) in acute myelo-monocytic leukemia withextensive leukemic cutaneous involvement. Leuk Lymphoma.1996;20:513-515.
66. Jani Sait SN, Raza A, Sandberg AA. Tetrasomy ofchromosome 8: an interesting and rare cytogeneticphenomenon in acute nonlymphocytic leukemia. CancerGenet Cytogenet. 1987;27:269-271.
67. La Starza R, Crescenzi B, Matteucci C, et al. Cytogenetic andFISH investigations on tetrasomy 8 in ANLL. Cancer GenetCytogenet. 1995;79:182-185.
68. Zhang XX, Robinson LJ, Stenzel TT, et al. Translocation(15;17)(q22;q21) as a secondary chromosomal abnormality ina case of acute monoblastic leukemia with tetrasomy 8. CancerGenet Cytogenet. 1999;113:9-13.
69. Gould J, Iqbal A, Heath M, et al. Pentasomy 8 in acutemonoblastic leukemia. Cancer Genet Cytogenet. 2000;117:146-148.
70. Fuhlbrigge RC, Kieffer JD, Armerding D, et al. Cutaneouslymphocyte antigen is a specialized form of PSGL-1 expressedon skin-homing T cells. Nature. 1997;389:978-981.
71. Campbell JJ, Haraldsen G, Pan J, et al. The chemokinereceptor CCR4 in vascular recognition by cutaneous but notintestinal memory T cells. Nature. 1999;400:776-780.
72. Ferenczi K, Fuhlbrigge RC, Pinkus J, et al. Increased CCR4expression in cutaneous T cell lymphoma. J Invest Dermatol.2002;119:1405-1410.
73. Kantele A, Savilahti E, Tiimonen H, et al. Cutaneouslymphocyte antigen expression on human effector B cellsdepends on the site and on the nature of antigen encounter.Eur J Immunol. 2003;33:3275-3283.
74. Picker LJ, Michie SA, Rott LS, et al. A unique phenotype ofskin-associated lymphocytes in humans: preferentialexpression of the HECA-452 epitope by benign and malignantT cells at cutaneous sites. Am J Pathol. 1990;136:1053-1068.
75. Petrella T, Meijer CJ, Dalac S, et al. TCL1 and CLAexpression in agranular CD4/CD56 hematodermic neoplasms(blastic NK-cell lymphomas) and leukemia cutis. Am J ClinPathol. 2004;122:307-313.
76. Yoshie O. Expression of CCR4 in adult T-cell leukemia. LeukLymphoma. 2005;46:185-190.
77. Yoshie O, Fujisawa R, Nakayama T, et al. Frequent expressionof CCR4 in adult T-cell leukemia and human T-cell leukemiavirus type 1–transformed T cells. Blood. 2002;99:1505-1511.
78. Wolf-Henning B. Lymphocyte Homing to the Skin. New York,NY: Informa Health Care; 2005:53-79.
79. Avigdor A, Raanani P, Levi I, et al. Extramedullary progressiondespite a good response in the bone marrow in patients treatedwith thalidomide for multiple myeloma. Leuk Lymphoma.2001;42:683-687.
80. Teoh G, Anderson KC. Interaction of tumor and host cellswith adhesion and extracellular matrix molecules in thedevelopment of multiple myeloma. Hematol Oncol Clin NorthAm. 1997;11:27-42.
81. Giralt S, O’Brien S, Weeks E, et al. Leukemia cutis in acutepromyelocytic leukemia: report of three cases after treatmentwith all-trans retinoic acid. Leuk Lymphoma. 1994;14:453-456.
Dow
nloaded from https://academ
ic.oup.com/ajcp/article/129/1/130/1765383 by guest on 15 Septem
ber 2022
Related Documents

![Case Report Metastatic Calcinosis Cutis: A Case in a Child ...downloads.hindawi.com/journals/crihem/2015/384821.pdf · phoblastic and myeloid acute leukemia []. Metastatic cal-cinosis](https://static.cupdf.com/doc/110x72/5f903fad69bb713af81a8e96/case-report-metastatic-calcinosis-cutis-a-case-in-a-child-phoblastic-and-myeloid.jpg)









