Lambert-Eaton Myasthenic Syndrome: A Review Hideyuki Matsumoto, MD, PhD 1 and Yoshikazu Ugawa, MD, PhD 2 1 Department of Neurology, Japanese Red Cross Medical Center, Tokyo, Japan 2 Department of Neurology, School of Medicine, Fukushima Medical University, Fukushima, Japan Lambert-Eaton myasthenic syndrome (LEMS) is an auto-immune disorder caused by neuromuscular transmission failure, and is a representative pre-neuromuscular junctional disorder. The auto-immune antibody is anti-P/Q-type voltage-gated calcium channel (P/Q-type VGCC) antibody detected in approximately 80 to 90% of LEMS patients. Approximately 60% of LEMS patients have small cell lung cancer (SCLC), approximately 10% of patients have other malignant tumors, and the remaining 30% have no malignancy. Thus, the therapeutic strategy for LEMS depends on the presence of a malignant tumor. LEMS with a malignant tumor is also considered to be a representative paraneoplastic neurological syndrome. Recently, new chemotherapeutic drugs for malignant tumors including SCLC have been developed. In cases with no malignancy, several new immune-mediated therapies have become available. Therefore, we can expect improved therapeutic responses for this disorder. Keywords: Lambert-Eaton myasthenic syndrome (LEMS), anti-P/Q-type voltage-gated calcium channel (P/Q-type VGCC) antibody, small cell lung cancer (SCLC), paraneoplastic neurological syndrome, repetitive nerve stimulation test 1. Introduction Lambert-Eaton myasthenic syndrome (LEMS) is an auto-immune disorder caused by neuromuscular trans- mission failure, and is a representative pre-neuro- muscular junctional disorder. 1–3 The auto-immune antibody is anti-P/Q-type voltage-gated calcium chan- nel (P/Q-type VGCC), which is speculated to target P/Q-type VGCC in nerve terminals (pre-neuromuscu- lar junctions). The antibody is detected in approx- imately 80 to 90% of LEMS patients. This disorder is very rare and the exact prevalence rate is unknown but speculated to be approximately 1 per 1,000,000 people. The gender is male dominant (male : female = 3 : 1). As shown in Table 1, the main clinical symptoms are leg-dominant muscular weakness of the proximal limbs and trunk with easy fatigability. 4 Autonomic dysfunc- tions such as dry mouth, mydriasis, dysuria, and constipation are also observed. Cranial nerve involve- ments, i.e., diplopia, ptosis, dysarthria, and dysphagia, are often associated. Tendon reflex is diminished. However, tendon reflex is normalized by the strong contraction of the muscles relating to the tendon reflex (post-tetanic potentiation), which is a finding specific to LEMS. Corresponding author: Hideyuki Matsumoto, MD, PhD Department of Neurology, Japanese Red Cross Medical Center, 4-1-22 Hiroo, Shibuya-ku, Tokyo 150-8935, Japan E-Mail: hideyukimatsumoto.jp@gmail.com Received for publication 23 December 2014 and accepted in revised form 7 May 2015 © 2016 Japan Primary Care Association Journal of General and Family Medicine 2016, vol. 17, no. 2, p. 138–143. Review Articles — 138 —

Lambert-Eaton Myasthenic Syndrome: A Review
Nov 07, 2022
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Lambert-Eaton Myasthenic Syndrome: A ReviewHideyuki Matsumoto, MD, PhD1 and Yoshikazu Ugawa, MD, PhD2
1 Department of Neurology, Japanese Red Cross Medical Center, Tokyo, Japan 2 Department of Neurology, School of Medicine, Fukushima Medical University, Fukushima, Japan
Lambert-Eaton myasthenic syndrome (LEMS) is an auto-immune disorder caused by neuromuscular transmission
failure, and is a representative pre-neuromuscular junctional disorder. The auto-immune antibody is anti-P/Q-type
voltage-gated calcium channel (P/Q-type VGCC) antibody detected in approximately 80 to 90% of LEMS patients.
Approximately 60% of LEMS patients have small cell lung cancer (SCLC), approximately 10% of patients have other
malignant tumors, and the remaining 30% have no malignancy. Thus, the therapeutic strategy for LEMS depends on the
presence of a malignant tumor. LEMS with a malignant tumor is also considered to be a representative paraneoplastic
neurological syndrome. Recently, new chemotherapeutic drugs for malignant tumors including SCLC have been
developed. In cases with no malignancy, several new immune-mediated therapies have become available. Therefore, we
can expect improved therapeutic responses for this disorder.
Keywords: Lambert-Eaton myasthenic syndrome (LEMS), anti-P/Q-type voltage-gated calcium channel (P/Q-type
VGCC) antibody, small cell lung cancer (SCLC), paraneoplastic neurological syndrome, repetitive nerve stimulation
test
mission failure, and is a representative pre-neuro-
muscular junctional disorder.1–3 The auto-immune
antibody is anti-P/Q-type voltage-gated calcium chan-
nel (P/Q-type VGCC), which is speculated to target
P/Q-type VGCC in nerve terminals (pre-neuromuscu-
lar junctions). The antibody is detected in approx-
imately 80 to 90% of LEMS patients. This disorder is
very rare and the exact prevalence rate is unknown but
speculated to be approximately 1 per 1,000,000 people.
The gender is male dominant (male : female = 3 : 1).
As shown in Table 1, the main clinical symptoms are
leg-dominant muscular weakness of the proximal limbs
and trunk with easy fatigability.4 Autonomic dysfunc-
tions such as dry mouth, mydriasis, dysuria, and
constipation are also observed. Cranial nerve involve-
ments, i.e., diplopia, ptosis, dysarthria, and dysphagia,
are often associated. Tendon reflex is diminished.
However, tendon reflex is normalized by the strong
contraction of the muscles relating to the tendon reflex
(post-tetanic potentiation), which is a finding specific to
LEMS.
Department of Neurology, Japanese Red Cross Medical Center, 4-1-22 Hiroo, Shibuya-ku, Tokyo 150-8935, Japan
E-Mail: [email protected]
Received for publication 23 December 2014 and accepted in revised form 7 May 2015
© 2016 Japan Primary Care Association
Journal of General and Family Medicine 2016, vol. 17, no. 2, p. 138–143.
Review Articles
The clinical symptoms in LEMS patients are improved
by the treatment of the tumor. Therefore, LEMS with a
malignant tumor is also considered to be a representa-
tive paraneoplastic neurological syndrome. In partic-
ular, small cell lung cancer (SCLC) is frequent
(Figure 1). Approximately 60% of LEMS patients
have SCLC, approximately 10% of patients other
malignant tumors, and the remaining 30% had no
malignancy (Table 2).3 LEMS without any malignant
tumors also often has other concomitant auto-immune
disorders, e.g., type 1 diabetes mellitus, thyroid
dysfunction, and rheumatoid arthritis.
type VGCC antibody in LEMS. Next, we summarize
the examinations, diagnosis, and therapies for LEMS.
2. Anti-P/Q-type VGCC Antibody
P/Q-type VGCC, the following pathophysiology is
speculated: the antibody made from the P/Q-type
VGCC in SCLC has an influence on the P/Q-type
VGCC in nerve terminals. In the case of LEMS without
anti-P/Q-type VGCC antibody, patients are considered
to have seronegative LEMS, in which unknown
antibodies are speculated to relate to the pathophysi-
ology. Ten percent of LEMS patients present with
cerebellar ataxia.5 In these patients, the following
mechanisms are speculated: anti-P/Q-type VGCC
antibody has an influence on the antigen expressed
in the cerebellum, i.e., P/Q-type VGCC. These are,
however, assumptions, and it is unknown whether anti-
P/Q-type VGCC antibody really causes LEMS or not,
because animal models for LEMS have not yet been
developed. To determine the pathophysiology of
LEMS in more detail, further basic research on the
significance of anti-P/Q-type VGCC antibody in
LEMS is required.
Male : Female (%) 76 : 24
Muscular weakness of upper limbs 80%
Muscular weakness of lower limbs 97%
Decreased tendon reflex 85%
Abnormal oculomotor movement 5%
Anti-P/Q-type VGCC antibody 85%
(Modified from reference 4)
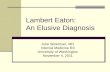
Figure 1. Small cell lung cancer (SCLC). Chest computed tomography (CT) shows a low density tumor without enhancement of contrast media at the posterior mediastinum (arrowhead). LEMS patients often have SCLC, suggesting a paraneoplastic neurological syndrome.
Table 2. Malignant tumors in LEMS
Lung cancer (90% small cell lung cancer: SCLC)
Malignant lymphoma
— 139 —
clinical symptoms, the positive anti-P/Q-type antibody,
and the specific findings in repetitive nerve stimulation
test. The most important differential diagnosis is
myasthenia gravis (MG), which is an auto-immune
disorder caused by neuromuscular transmission failure,
and a representative “post”-neuromuscular junctional
disorder (see our review article on MG).6 In general,
the clinical symptoms in LEMS do not appear only
in the ocular muscles, in contrast to MG. However,
similar to MG, 3% of LEMS patients present with
myasthenic crisis. The most specific findings in LEMS
may be the normalized tendon reflex after strong
muscular contraction (post-tetanic potentiation). Since
the leg symptoms are prominent in LEMS patients,
patellar tendon reflex is usually checked. During
relaxation, patellar tendon reflex is absent. On the
other hand, immediately after the contraction of
quadriceps muscle (knee extension), patellar tendon
reflex is normally elicited.
Compound muscle action potentials (CMAPs) are
usually recorded from the abductor digiti minimi,
abductor pollicis brevis, trapezius, and nasalis muscles.
As shown in Figure 2A, 3Hz repetitive electrical
stimulation of peripheral nerves shows gradual ampli-
tude reduction of CMAPs (waning). The waning is
detectable even in muscles without weakness in LEMS
patients. The exercise test is useful to sensitively detect
the waning. In the exercise test, the target muscle is
strongly contracted before electrical stimulation and the
CMAPs to repetitive electrical stimulation are recorded
every minute after the muscular contraction (from
one to three minutes). One or two minutes after the
contraction, the waning exaggerates. Here, we must
caution that waning is also observed in MG. However,
LEMS patients have the following specific findings:
(i) the CMAP amplitude is markedly small compared to
the muscle force, and (ii) immediately after the exercise
test, the CMAP amplitude is markedly enlarged. These
findings are observed even in single-pulse nerve
stimulation (Figure 2B and 2C), and the significances
are almost the same as those of the gradual amplitude
increment of CMAPs in 20 to 50Hz repetitive nerve
stimulation test (waxing). Recently, high-frequency
repetitive electrical stimulation has not been conducted
due to the severe pain it induces.
3-2. Tensilon test
tration of 10mg of edrophonium chloride (Antirexµ), a
cholinesterase inhibitor that transiently blocks the
action of acetylcholinesterase. It is of note that this
test can be false positive because of the placebo effect.7
To precisely determine the effects of edrophonium
chloride, a comparison of the effects between edro-
phonium chloride and placebo is helpful. First, saline
is gradually injected as a placebo test. Next, 2mg of
edrophonium chloride is gradually injected, and side
effects such as bradycardia, dyspnea, and abdominal
Figure 2. Repetitive nerve stimulation test. Three hertz repetitive nerve stimulation test for the abductor pollicis brevis muscle is performed during relaxation (A). The fourth amplitude of the com- pound muscle action potentials (CMAPs) is 23% smaller than that of the first CMAP, suggesting waning (waning is defined as a more than 10% CMAP amplitude reduction). Single-pulse nerve stimulation is performed during relaxation and immediately after exercise. During relaxation (B), the CMAP amplitude is very small (1.1mV). Immediately after exercise (C), however, the CMAP amplitude is increased to 3.9mV (the CMAP incre- ment is 255%). In LEMS patients, the release of acetylcholine from nerve terminals is disturbed, leading to neuromuscular transmission failure. Im- mediately after exercise, abundant acetylcholine is released. Therefore, the CMAP amplitude is enlarged due to the improvement in neuromuscular trans- mission failure. These findings, the small CMAPs during relaxation, and the enlargement immediately after exercise, are specific to LEMS.
Journal of General and Family Medicine 2016, vol. 17, no. 2
— 140 —
pain are monitored for. If no side effects appear, the
remaining 8mg of edrophonium chloride is gradually
injected. If severe side effects appear, atropine sulface
hydrate (atropine sulfate injectionµ), an anticholinergic
drug, is injected. In order to handle potential side
effects, emergency carts should always be prepared for
this test. Clinical symptoms are transiently improved
in LEMS, but not always. If this test is positive
(effective), a cholinesterase inhibitor should be con-
sidered as a symptomatic therapy. Due to the side
effects of edrophonium chloride, this test is not always
required.
The therapeutic strategy for LEMS depends on the
presence of a malignant tumor. If a LEMS patient has a
malignant tumor such as SCLC, the primary therapy
is treatment for the malignant tumor, i.e., surgery,
chemotherapy, radiotherapy, etc. In parallel with the
remission of the malignant tumor, the clinical symp-
toms of LEMS improve. Anti-P/Q-type VGCC anti-
body is considered to play a role in suppressing the
growth of malignant tumors. Therefore, immunother-
apy for LEMS with a malignant tumor should be
considered only if severe symptoms remain despite
both the treatment for a malignant tumor and the
symptomatic therapy for LEMS. A malignant tumor is
often found after a diagnosis of LEMS. Therefore, it is
proposed that a malignant tumor should be searched for
at least two years after the diagnosis of LEMS and
before immunotherapy.8 In the case of no malignancy,
immunotherapy should be conducted for the treatment
of LEMS. Previously, guanidinium chloride was used
as a symptomatic therapy, although this medicine is not
currently used due to the side effects on the central
nervous system, bone marrow, etc. The medicines
currently used as symptomatic therapies for LEMS are
3,4-Diaminopyridine (3, 4-DAP) and cholinesterase
inhibitor. The following immunotherapies are admin-
istered according to the therapeutic strategy for MG:
steroids and immunosuppressive drugs, plasmaphere-
sis, intravenous immunoglobulin (IVIg), and rituximab.
There are no large-scale studies on immunotherapy and
the efficacy of these medicines is reported in a small
number of LEMS patients.
4-1. Treatments for malignancy
lung cancer (SCLC), and approximately 10% of
patients have other malignant tumors such as malignant
lymphoma (Table 2).3 Radical treatments such as
surgery, chemotherapy, and radiotherapy for a malig-
nant tumor should be conducted as treatments for
LEMS with malignancy. Recently, new chemothera-
peutic drugs for malignant tumors including SCLC
have been developed. Therefore, an improved prog-
nosis of LEMS patients with malignancy is expected.
4-2. 3,4-Diaminopyridine (3, 4-DAP)
in Japan. This is the most common medicine world-
wide, and its efficacy has been shown in a randomized,
double-blind, placebo-controlled trial.9 This medicine
blocks potassium channels in nerve terminals, resulting
in an increase in acetylcholine release. This sympto-
matic therapy is effective not only for muscular
weakness but also for autonomic dysfunction. It should
be started at 5mg/day and gradually increased. The
maximal dosage is 100mg/day. The main side effects
are abdominal pain, diarrhea, insomnia, dysesthesia
around the mouth and limbs, epileptic seizures, and
long QT syndrome. Currently, in Japan, this is a
non-approved medicine, but obtainable as a reagent.
To administer this medicine, therapeutic application
should be approved by the ethics committee of each
institution and informed consent should be obtained
from each patient.
4-3. Cholinesterase inhibitor
terase enzyme from breaking down the acetylcholine
released from nerve terminals. This medicine increases
the concentration of acetylcholine at the synaptic cleft,
enhancing the muscular contraction. This is a sympto-
matic therapy for LEMS, although it is not highly
effective. This medicine is often used concomitantly
with 3, 4-DAP. Pyridostigmine bromide (Mestinonµ;
up to three tablets/day) or ambenoium chloride
(Mytelaseµ; 1.5 tablets/day) is often used. The half-
life of the former is shorter than that of the latter. In
terms of side effects, clinicians should be vigilant for
Lambert-Eaton Myasthenic Syndrome: A Review
— 141 —
cholinergic crisis.
4-4. Immunotherapy
4-4-1. Steroids
abnormal auto-immune antibodies from being made.
Prednisolone (Predonineµ) is often used as an oral
glucocorticosteroid therapy. This medicine is usually
administered on consecutive or alternate days. Predni-
solone is usually administered at an initial dosage of
1mg/kg/day, maintained at the same high dosage for a
certain period, and gradually reduced to the main-
tenance dosages needed to prevent the deterioration of
clinical symptoms. Clinicians should be aware of the
many side effects, including infection, gastric ulcer,
diabetes mellitus, insomnia, psychosis, and osteopo-
rosis. Preventive medicines for these major side effects
should be considered. To avoid the side effects of
high-dosage steroids, a low dosage of prednisolone is
also combined with immunosuppressive drugs.
Steroid pulse therapy (methylprednisolone,
Solumedrolµ, 1 g/day © 3 days) may also be used to
shorten the therapeutic period with the high-dosage
oral steroid therapy.
4-4-2. Immunosuppressive drugs
often used according to the therapeutic strategy for
MG. The usual dosage of tacrolimus is 3mg/day. The
trough level should be under 20 ng/ml. The dosage
(3mg) is markedly low compared to the dosage used in
organ transplantation. Side effects such as diabetes
mellitus and hyperkalemia should be monitored for.
The initial dosage of cyclosporine is 5mg/kg/day and
the maintenance dosage is 3mg/kg/day. As for side
effects, clinicians should watch for renal failure,
hypertension, and malignant tumors. The trough
level should be under 200 ng/ml during the initial
period and under 150 ng/ml during the maintenance
period. Immunosuppressive drugs are often used for
the reduction of steroids, but the efficacy of mono-
therapy has not yet been determined. As other
medicines, azathioprine (Imuranµ), cyclophosphamide
can be used.
rary (two or three weeks). Therefore, plasmapheresis is
mainly used for myasthenic crisis. It is also used for
shortening the duration of high-dosage steroid therapy
in LEMS. Plasma exchange (PE), double filtration
plasmapheresis (DFPP), and immunoadsorption ther-
apy (IAPP) are available. PE is effective for LEMS.
However, the efficacy of DFPP or IAPP is unknown.
4-4-4. Intravenous immunoglobulin (IVIg)
IVIg is mainly used for shortening the duration of high-
dosage steroid therapy and for steroid-resistant LEMS
in addition to myasthenic crisis. The temporal efficacy
of IVIg is considered to be almost the same as that of
PE. This infusion therapy is more convenient than
plasmapheresis.
body directed against the CD20 antigen. Efficacy has
been shown for LEMS patients.
5. Current Problems and Future Expectations
One clinical problem for LEMS, is measurement of
anti-P/Q-type VGCC antibody is not commercially
available. Another problem is that there are no
medicines with approvals for the treatment of LEMS.
As a research problem, animal models of LEMS have
not yet been developed. For this reason, it remains
unknown whether anti-P/Q-type VGCC antibody
causes LEMS or not. Although there are many issues
to solve in the future, new chemotherapeutic drugs for
malignant tumors including SCLC have been devel-
oped and new immune-mediated therapies are avail-
able. Currently, therefore, we can expect improved
therapeutic responses for this disorder.
Conflicts of interest
to this article.
ments for neurological disorders—knowledge essential
Journal of General and Family Medicine 2016, vol. 17, no. 2
— 142 —
Myasthenia. Nihon Naika Gakkai Zasshi. 2013; 102:
1994–2000.
of autoimmune neuromuscular junction diseases.
Rinsho Shinkeigaku. 2011; 51: 872–876.
3 Motomura M, Fukuda T: Lambert-Eaton myas-
thenic syndrome. Brain Nerve. 2011; 63: 745–754.
4 Nakao YK, Motomura M, Fukudome T, et al:
Seronegative Lambert-Eaton myasthenic syndrome:
1773–1775.
5 Seki N, Mitsui J, Hoshino M, et al: A case of small
cell carcinoma of the lung associated with paraneo-
plastic cerebellar degeneration and Lambert-Eaton
myasthenic syndrome. No To Shinkei. 2006; 58:
68–73.
7 Matsumoto H, Shimizu T, Igeta Y, Hashida H:
Psychogenic unilateral ptosis with ipsilateral muscle
spasm of orbicular oculi. Acta Med Indones. 2012; 44:
243–245.
Sci. 1998; 841: 817–822.
9 Oh SJ, Claussen GG, Hatanaka Y, Morgan MB:
3,4-Diaminopyridine is more effective than placebo in
a randomized, double-blind, cross-over drug study in
LEMS. Muscle Nerve. 2009; 40: 795–800.
Lambert-Eaton Myasthenic Syndrome: A Review
— 143 —
1 Department of Neurology, Japanese Red Cross Medical Center, Tokyo, Japan 2 Department of Neurology, School of Medicine, Fukushima Medical University, Fukushima, Japan
Lambert-Eaton myasthenic syndrome (LEMS) is an auto-immune disorder caused by neuromuscular transmission
failure, and is a representative pre-neuromuscular junctional disorder. The auto-immune antibody is anti-P/Q-type
voltage-gated calcium channel (P/Q-type VGCC) antibody detected in approximately 80 to 90% of LEMS patients.
Approximately 60% of LEMS patients have small cell lung cancer (SCLC), approximately 10% of patients have other
malignant tumors, and the remaining 30% have no malignancy. Thus, the therapeutic strategy for LEMS depends on the
presence of a malignant tumor. LEMS with a malignant tumor is also considered to be a representative paraneoplastic
neurological syndrome. Recently, new chemotherapeutic drugs for malignant tumors including SCLC have been
developed. In cases with no malignancy, several new immune-mediated therapies have become available. Therefore, we
can expect improved therapeutic responses for this disorder.
Keywords: Lambert-Eaton myasthenic syndrome (LEMS), anti-P/Q-type voltage-gated calcium channel (P/Q-type
VGCC) antibody, small cell lung cancer (SCLC), paraneoplastic neurological syndrome, repetitive nerve stimulation
test
mission failure, and is a representative pre-neuro-
muscular junctional disorder.1–3 The auto-immune
antibody is anti-P/Q-type voltage-gated calcium chan-
nel (P/Q-type VGCC), which is speculated to target
P/Q-type VGCC in nerve terminals (pre-neuromuscu-
lar junctions). The antibody is detected in approx-
imately 80 to 90% of LEMS patients. This disorder is
very rare and the exact prevalence rate is unknown but
speculated to be approximately 1 per 1,000,000 people.
The gender is male dominant (male : female = 3 : 1).
As shown in Table 1, the main clinical symptoms are
leg-dominant muscular weakness of the proximal limbs
and trunk with easy fatigability.4 Autonomic dysfunc-
tions such as dry mouth, mydriasis, dysuria, and
constipation are also observed. Cranial nerve involve-
ments, i.e., diplopia, ptosis, dysarthria, and dysphagia,
are often associated. Tendon reflex is diminished.
However, tendon reflex is normalized by the strong
contraction of the muscles relating to the tendon reflex
(post-tetanic potentiation), which is a finding specific to
LEMS.
Department of Neurology, Japanese Red Cross Medical Center, 4-1-22 Hiroo, Shibuya-ku, Tokyo 150-8935, Japan
E-Mail: [email protected]
Received for publication 23 December 2014 and accepted in revised form 7 May 2015
© 2016 Japan Primary Care Association
Journal of General and Family Medicine 2016, vol. 17, no. 2, p. 138–143.
Review Articles
The clinical symptoms in LEMS patients are improved
by the treatment of the tumor. Therefore, LEMS with a
malignant tumor is also considered to be a representa-
tive paraneoplastic neurological syndrome. In partic-
ular, small cell lung cancer (SCLC) is frequent
(Figure 1). Approximately 60% of LEMS patients
have SCLC, approximately 10% of patients other
malignant tumors, and the remaining 30% had no
malignancy (Table 2).3 LEMS without any malignant
tumors also often has other concomitant auto-immune
disorders, e.g., type 1 diabetes mellitus, thyroid
dysfunction, and rheumatoid arthritis.
type VGCC antibody in LEMS. Next, we summarize
the examinations, diagnosis, and therapies for LEMS.
2. Anti-P/Q-type VGCC Antibody
P/Q-type VGCC, the following pathophysiology is
speculated: the antibody made from the P/Q-type
VGCC in SCLC has an influence on the P/Q-type
VGCC in nerve terminals. In the case of LEMS without
anti-P/Q-type VGCC antibody, patients are considered
to have seronegative LEMS, in which unknown
antibodies are speculated to relate to the pathophysi-
ology. Ten percent of LEMS patients present with
cerebellar ataxia.5 In these patients, the following
mechanisms are speculated: anti-P/Q-type VGCC
antibody has an influence on the antigen expressed
in the cerebellum, i.e., P/Q-type VGCC. These are,
however, assumptions, and it is unknown whether anti-
P/Q-type VGCC antibody really causes LEMS or not,
because animal models for LEMS have not yet been
developed. To determine the pathophysiology of
LEMS in more detail, further basic research on the
significance of anti-P/Q-type VGCC antibody in
LEMS is required.
Male : Female (%) 76 : 24
Muscular weakness of upper limbs 80%
Muscular weakness of lower limbs 97%
Decreased tendon reflex 85%
Abnormal oculomotor movement 5%
Anti-P/Q-type VGCC antibody 85%
(Modified from reference 4)
Figure 1. Small cell lung cancer (SCLC). Chest computed tomography (CT) shows a low density tumor without enhancement of contrast media at the posterior mediastinum (arrowhead). LEMS patients often have SCLC, suggesting a paraneoplastic neurological syndrome.
Table 2. Malignant tumors in LEMS
Lung cancer (90% small cell lung cancer: SCLC)
Malignant lymphoma
— 139 —
clinical symptoms, the positive anti-P/Q-type antibody,
and the specific findings in repetitive nerve stimulation
test. The most important differential diagnosis is
myasthenia gravis (MG), which is an auto-immune
disorder caused by neuromuscular transmission failure,
and a representative “post”-neuromuscular junctional
disorder (see our review article on MG).6 In general,
the clinical symptoms in LEMS do not appear only
in the ocular muscles, in contrast to MG. However,
similar to MG, 3% of LEMS patients present with
myasthenic crisis. The most specific findings in LEMS
may be the normalized tendon reflex after strong
muscular contraction (post-tetanic potentiation). Since
the leg symptoms are prominent in LEMS patients,
patellar tendon reflex is usually checked. During
relaxation, patellar tendon reflex is absent. On the
other hand, immediately after the contraction of
quadriceps muscle (knee extension), patellar tendon
reflex is normally elicited.
Compound muscle action potentials (CMAPs) are
usually recorded from the abductor digiti minimi,
abductor pollicis brevis, trapezius, and nasalis muscles.
As shown in Figure 2A, 3Hz repetitive electrical
stimulation of peripheral nerves shows gradual ampli-
tude reduction of CMAPs (waning). The waning is
detectable even in muscles without weakness in LEMS
patients. The exercise test is useful to sensitively detect
the waning. In the exercise test, the target muscle is
strongly contracted before electrical stimulation and the
CMAPs to repetitive electrical stimulation are recorded
every minute after the muscular contraction (from
one to three minutes). One or two minutes after the
contraction, the waning exaggerates. Here, we must
caution that waning is also observed in MG. However,
LEMS patients have the following specific findings:
(i) the CMAP amplitude is markedly small compared to
the muscle force, and (ii) immediately after the exercise
test, the CMAP amplitude is markedly enlarged. These
findings are observed even in single-pulse nerve
stimulation (Figure 2B and 2C), and the significances
are almost the same as those of the gradual amplitude
increment of CMAPs in 20 to 50Hz repetitive nerve
stimulation test (waxing). Recently, high-frequency
repetitive electrical stimulation has not been conducted
due to the severe pain it induces.
3-2. Tensilon test
tration of 10mg of edrophonium chloride (Antirexµ), a
cholinesterase inhibitor that transiently blocks the
action of acetylcholinesterase. It is of note that this
test can be false positive because of the placebo effect.7
To precisely determine the effects of edrophonium
chloride, a comparison of the effects between edro-
phonium chloride and placebo is helpful. First, saline
is gradually injected as a placebo test. Next, 2mg of
edrophonium chloride is gradually injected, and side
effects such as bradycardia, dyspnea, and abdominal
Figure 2. Repetitive nerve stimulation test. Three hertz repetitive nerve stimulation test for the abductor pollicis brevis muscle is performed during relaxation (A). The fourth amplitude of the com- pound muscle action potentials (CMAPs) is 23% smaller than that of the first CMAP, suggesting waning (waning is defined as a more than 10% CMAP amplitude reduction). Single-pulse nerve stimulation is performed during relaxation and immediately after exercise. During relaxation (B), the CMAP amplitude is very small (1.1mV). Immediately after exercise (C), however, the CMAP amplitude is increased to 3.9mV (the CMAP incre- ment is 255%). In LEMS patients, the release of acetylcholine from nerve terminals is disturbed, leading to neuromuscular transmission failure. Im- mediately after exercise, abundant acetylcholine is released. Therefore, the CMAP amplitude is enlarged due to the improvement in neuromuscular trans- mission failure. These findings, the small CMAPs during relaxation, and the enlargement immediately after exercise, are specific to LEMS.
Journal of General and Family Medicine 2016, vol. 17, no. 2
— 140 —
pain are monitored for. If no side effects appear, the
remaining 8mg of edrophonium chloride is gradually
injected. If severe side effects appear, atropine sulface
hydrate (atropine sulfate injectionµ), an anticholinergic
drug, is injected. In order to handle potential side
effects, emergency carts should always be prepared for
this test. Clinical symptoms are transiently improved
in LEMS, but not always. If this test is positive
(effective), a cholinesterase inhibitor should be con-
sidered as a symptomatic therapy. Due to the side
effects of edrophonium chloride, this test is not always
required.
The therapeutic strategy for LEMS depends on the
presence of a malignant tumor. If a LEMS patient has a
malignant tumor such as SCLC, the primary therapy
is treatment for the malignant tumor, i.e., surgery,
chemotherapy, radiotherapy, etc. In parallel with the
remission of the malignant tumor, the clinical symp-
toms of LEMS improve. Anti-P/Q-type VGCC anti-
body is considered to play a role in suppressing the
growth of malignant tumors. Therefore, immunother-
apy for LEMS with a malignant tumor should be
considered only if severe symptoms remain despite
both the treatment for a malignant tumor and the
symptomatic therapy for LEMS. A malignant tumor is
often found after a diagnosis of LEMS. Therefore, it is
proposed that a malignant tumor should be searched for
at least two years after the diagnosis of LEMS and
before immunotherapy.8 In the case of no malignancy,
immunotherapy should be conducted for the treatment
of LEMS. Previously, guanidinium chloride was used
as a symptomatic therapy, although this medicine is not
currently used due to the side effects on the central
nervous system, bone marrow, etc. The medicines
currently used as symptomatic therapies for LEMS are
3,4-Diaminopyridine (3, 4-DAP) and cholinesterase
inhibitor. The following immunotherapies are admin-
istered according to the therapeutic strategy for MG:
steroids and immunosuppressive drugs, plasmaphere-
sis, intravenous immunoglobulin (IVIg), and rituximab.
There are no large-scale studies on immunotherapy and
the efficacy of these medicines is reported in a small
number of LEMS patients.
4-1. Treatments for malignancy
lung cancer (SCLC), and approximately 10% of
patients have other malignant tumors such as malignant
lymphoma (Table 2).3 Radical treatments such as
surgery, chemotherapy, and radiotherapy for a malig-
nant tumor should be conducted as treatments for
LEMS with malignancy. Recently, new chemothera-
peutic drugs for malignant tumors including SCLC
have been developed. Therefore, an improved prog-
nosis of LEMS patients with malignancy is expected.
4-2. 3,4-Diaminopyridine (3, 4-DAP)
in Japan. This is the most common medicine world-
wide, and its efficacy has been shown in a randomized,
double-blind, placebo-controlled trial.9 This medicine
blocks potassium channels in nerve terminals, resulting
in an increase in acetylcholine release. This sympto-
matic therapy is effective not only for muscular
weakness but also for autonomic dysfunction. It should
be started at 5mg/day and gradually increased. The
maximal dosage is 100mg/day. The main side effects
are abdominal pain, diarrhea, insomnia, dysesthesia
around the mouth and limbs, epileptic seizures, and
long QT syndrome. Currently, in Japan, this is a
non-approved medicine, but obtainable as a reagent.
To administer this medicine, therapeutic application
should be approved by the ethics committee of each
institution and informed consent should be obtained
from each patient.
4-3. Cholinesterase inhibitor
terase enzyme from breaking down the acetylcholine
released from nerve terminals. This medicine increases
the concentration of acetylcholine at the synaptic cleft,
enhancing the muscular contraction. This is a sympto-
matic therapy for LEMS, although it is not highly
effective. This medicine is often used concomitantly
with 3, 4-DAP. Pyridostigmine bromide (Mestinonµ;
up to three tablets/day) or ambenoium chloride
(Mytelaseµ; 1.5 tablets/day) is often used. The half-
life of the former is shorter than that of the latter. In
terms of side effects, clinicians should be vigilant for
Lambert-Eaton Myasthenic Syndrome: A Review
— 141 —
cholinergic crisis.
4-4. Immunotherapy
4-4-1. Steroids
abnormal auto-immune antibodies from being made.
Prednisolone (Predonineµ) is often used as an oral
glucocorticosteroid therapy. This medicine is usually
administered on consecutive or alternate days. Predni-
solone is usually administered at an initial dosage of
1mg/kg/day, maintained at the same high dosage for a
certain period, and gradually reduced to the main-
tenance dosages needed to prevent the deterioration of
clinical symptoms. Clinicians should be aware of the
many side effects, including infection, gastric ulcer,
diabetes mellitus, insomnia, psychosis, and osteopo-
rosis. Preventive medicines for these major side effects
should be considered. To avoid the side effects of
high-dosage steroids, a low dosage of prednisolone is
also combined with immunosuppressive drugs.
Steroid pulse therapy (methylprednisolone,
Solumedrolµ, 1 g/day © 3 days) may also be used to
shorten the therapeutic period with the high-dosage
oral steroid therapy.
4-4-2. Immunosuppressive drugs
often used according to the therapeutic strategy for
MG. The usual dosage of tacrolimus is 3mg/day. The
trough level should be under 20 ng/ml. The dosage
(3mg) is markedly low compared to the dosage used in
organ transplantation. Side effects such as diabetes
mellitus and hyperkalemia should be monitored for.
The initial dosage of cyclosporine is 5mg/kg/day and
the maintenance dosage is 3mg/kg/day. As for side
effects, clinicians should watch for renal failure,
hypertension, and malignant tumors. The trough
level should be under 200 ng/ml during the initial
period and under 150 ng/ml during the maintenance
period. Immunosuppressive drugs are often used for
the reduction of steroids, but the efficacy of mono-
therapy has not yet been determined. As other
medicines, azathioprine (Imuranµ), cyclophosphamide
can be used.
rary (two or three weeks). Therefore, plasmapheresis is
mainly used for myasthenic crisis. It is also used for
shortening the duration of high-dosage steroid therapy
in LEMS. Plasma exchange (PE), double filtration
plasmapheresis (DFPP), and immunoadsorption ther-
apy (IAPP) are available. PE is effective for LEMS.
However, the efficacy of DFPP or IAPP is unknown.
4-4-4. Intravenous immunoglobulin (IVIg)
IVIg is mainly used for shortening the duration of high-
dosage steroid therapy and for steroid-resistant LEMS
in addition to myasthenic crisis. The temporal efficacy
of IVIg is considered to be almost the same as that of
PE. This infusion therapy is more convenient than
plasmapheresis.
body directed against the CD20 antigen. Efficacy has
been shown for LEMS patients.
5. Current Problems and Future Expectations
One clinical problem for LEMS, is measurement of
anti-P/Q-type VGCC antibody is not commercially
available. Another problem is that there are no
medicines with approvals for the treatment of LEMS.
As a research problem, animal models of LEMS have
not yet been developed. For this reason, it remains
unknown whether anti-P/Q-type VGCC antibody
causes LEMS or not. Although there are many issues
to solve in the future, new chemotherapeutic drugs for
malignant tumors including SCLC have been devel-
oped and new immune-mediated therapies are avail-
able. Currently, therefore, we can expect improved
therapeutic responses for this disorder.
Conflicts of interest
to this article.
ments for neurological disorders—knowledge essential
Journal of General and Family Medicine 2016, vol. 17, no. 2
— 142 —
Myasthenia. Nihon Naika Gakkai Zasshi. 2013; 102:
1994–2000.
of autoimmune neuromuscular junction diseases.
Rinsho Shinkeigaku. 2011; 51: 872–876.
3 Motomura M, Fukuda T: Lambert-Eaton myas-
thenic syndrome. Brain Nerve. 2011; 63: 745–754.
4 Nakao YK, Motomura M, Fukudome T, et al:
Seronegative Lambert-Eaton myasthenic syndrome:
1773–1775.
5 Seki N, Mitsui J, Hoshino M, et al: A case of small
cell carcinoma of the lung associated with paraneo-
plastic cerebellar degeneration and Lambert-Eaton
myasthenic syndrome. No To Shinkei. 2006; 58:
68–73.
7 Matsumoto H, Shimizu T, Igeta Y, Hashida H:
Psychogenic unilateral ptosis with ipsilateral muscle
spasm of orbicular oculi. Acta Med Indones. 2012; 44:
243–245.
Sci. 1998; 841: 817–822.
9 Oh SJ, Claussen GG, Hatanaka Y, Morgan MB:
3,4-Diaminopyridine is more effective than placebo in
a randomized, double-blind, cross-over drug study in
LEMS. Muscle Nerve. 2009; 40: 795–800.
Lambert-Eaton Myasthenic Syndrome: A Review
— 143 —
Related Documents