Kebijakan Strategis untuk mengurangi ketidak adilan dalam mencapai Universal Health Coverage Laksono Trisnantoro Universitas Gadjah Mada InaHEA 2nd National Meeting, Jakarta, 9th April 2015 1 Strategic Policy for narrowing inequity in Universal Health Coverage programs

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

KebijakanStrategis untuk
mengurangiketidak adilan
dalam mencapaiUniversal Health
Coverage
Laksono Trisnantoro Universitas Gadjah Mada
InaHEA 2nd National Meeting, Jakarta, 9th April 2015
1
Strategic Policy for narrowing
inequity in Universal Health
Coverage programs

What Happened in 2014• JKN dimulai 1 Januari
2014• Situasi supply-side dalam
keadaan tidak seimbang.- SDM dokter dan kesehatan
tidak merata- Pelayanan kesehatan tidak
merata• Di awal tahun 2015,
berbagai sumbermenyatakan bahwa BPJS kekurangan 2 – 5 Triliun
• JKN started in January 2014
• Supply side is extremely not well distributed across Indonesia- Human resources- Health facilities
- In 2015 some report shows that BPJS is shortage of 2-4 Triliun
2
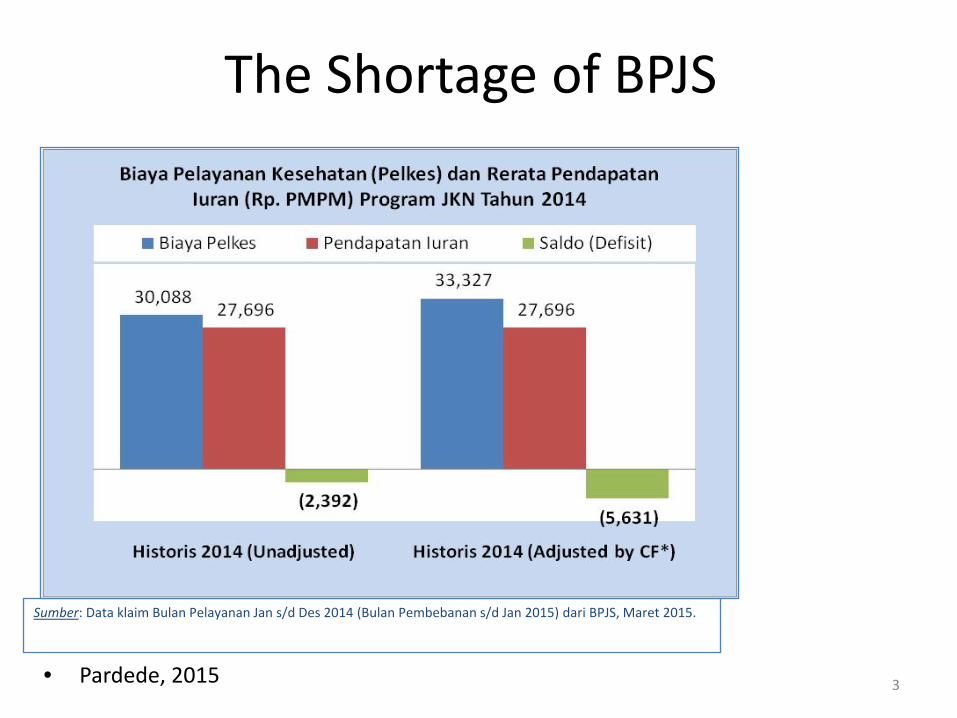
The Shortage of BPJS
• Pardede, 2015 3
Sumber: Data klaim Bulan Pelayanan Jan s/d Des 2014 (Bulan Pembebanan s/d Jan 2015) dari BPJS, Maret 2015.

Who Gets What in 2014?
• Siapa yang mendapatkan danaBPJS?
• Apakah masyarakatyang membutuhkan?Ataukahjustru masyarakatmenengah ke atas di kota-kota besar?
• Who get what from BPJS expenditure?
• Whether the poor or the better of community?
• Whether people in the remote area or in the big cities
4
In more specific, which member group?
• Kelompok masyarakatmiskin yang dibayarmelalui PBI?
• Kelompok Non-PBI eks PT Askes Indonesia dan PT Jamsostek?
• Kelompok Non-PBI Mandiri (Pekerja BukanPenerima Upah)?
Bagaimana isu Ketidakadilan?
• Poor community paid by central government budget (PBI)?
• The ex PT Askes and PT Jamsostek members and formal sector?
• The Non-PBI Mandiri?
How is equity issue is managed?
5

The Analysis
• Revenue Collection• Pooling• Purchasing
6
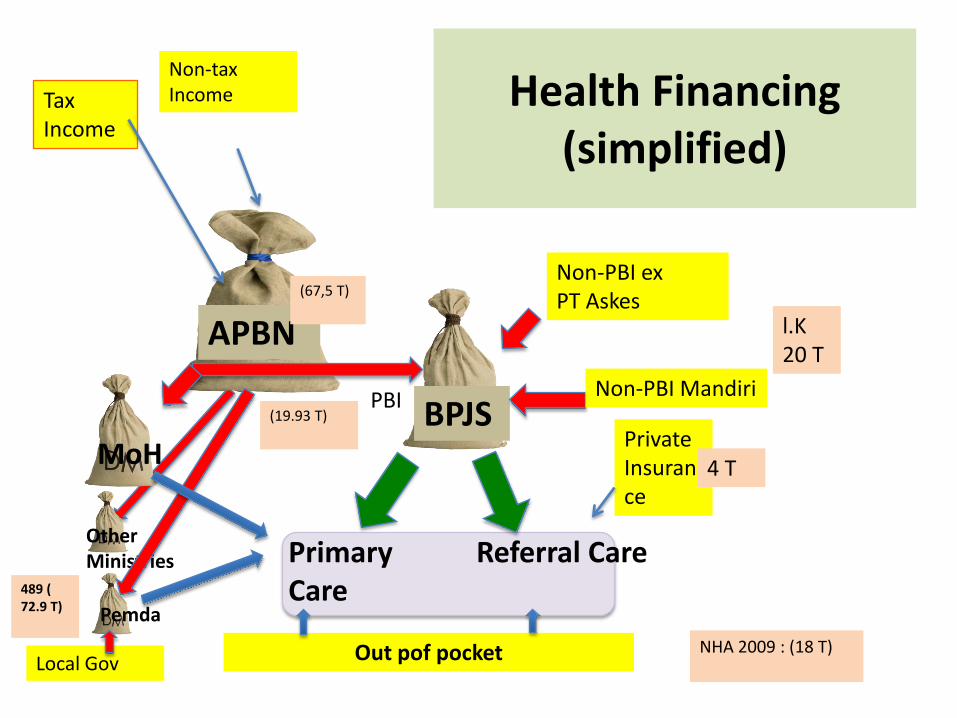
Health Financing (simplified)
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
7Local Gov
Private Insurance
(19.93 T)
NHA 2009 : (18 T)
489 ( 72.9 T)
l.K20 T
4 T
(67,5 T)

Revenue Colelection
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
8Local Gov
Private Insurance
(67,5 T)
NHA 2009 : (18 T)
489 ( 72.9 T)
4 T(19.93 T)
+-20 T
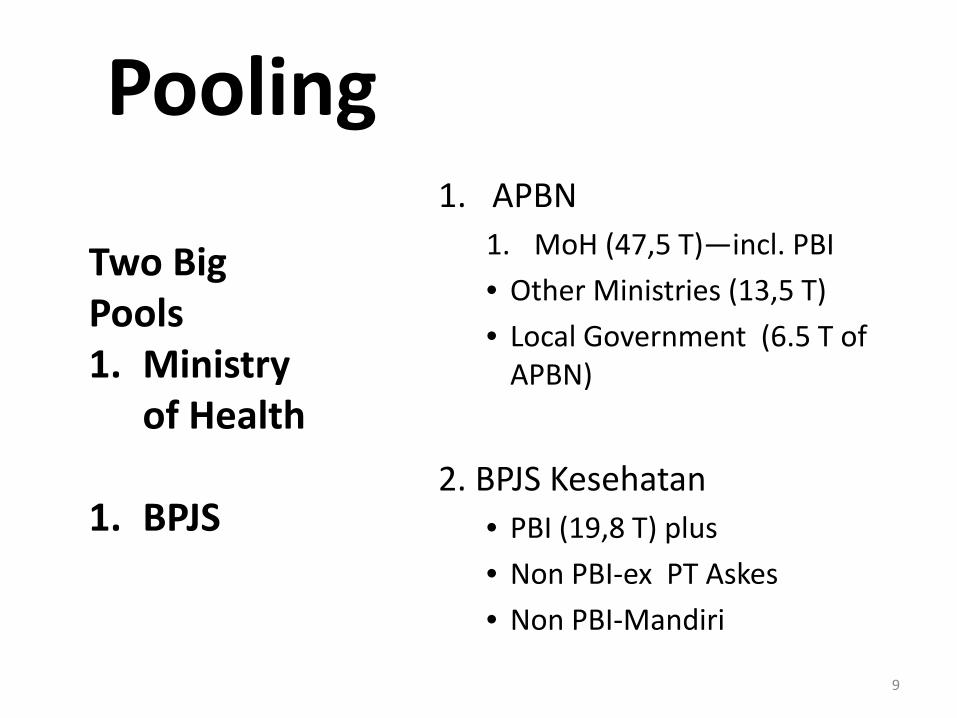
Pooling
9
1. APBN1. MoH (47,5 T)—incl. PBI• Other Ministries (13,5 T)• Local Government (6.5 T of
APBN)
2. BPJS Kesehatan• PBI (19,8 T) plus• Non PBI-ex PT Askes• Non PBI-Mandiri
Two Big Pools1. Ministry
of Health
1. BPJS
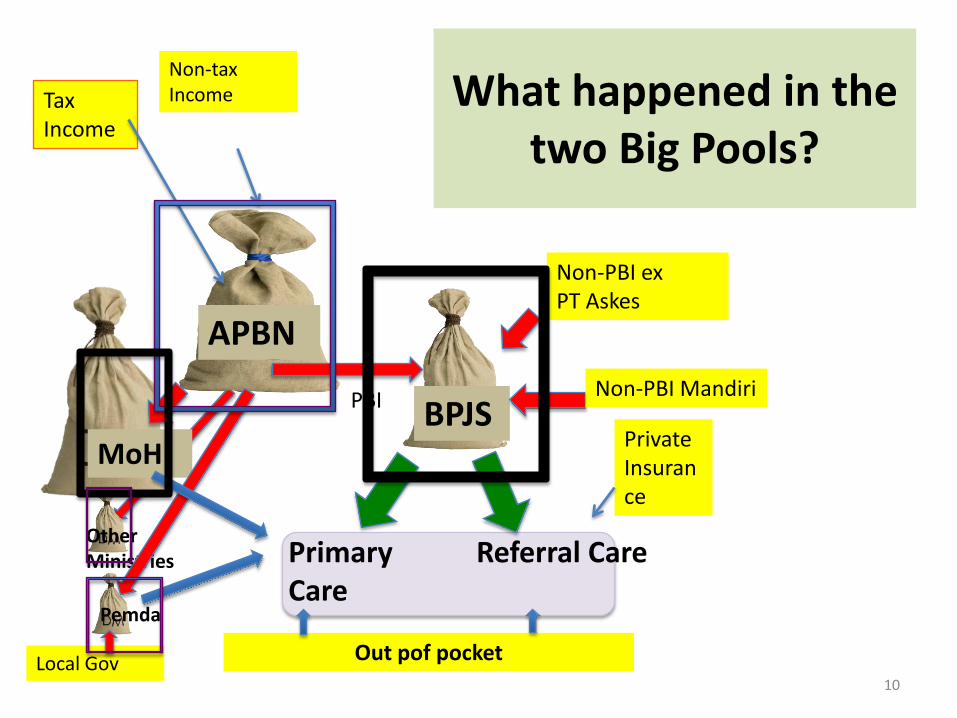
What happened in the two Big Pools?
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
10Local Gov
Private Insurance

Ministry of Health
In 2014:• Small Budget for
Hospital Investment • Human Resources
budget stagnant
Pada tahun 2014• Dana investasi kecil
untuk penambahanpelayanan kesehatandan sumber dayakesehatan
11
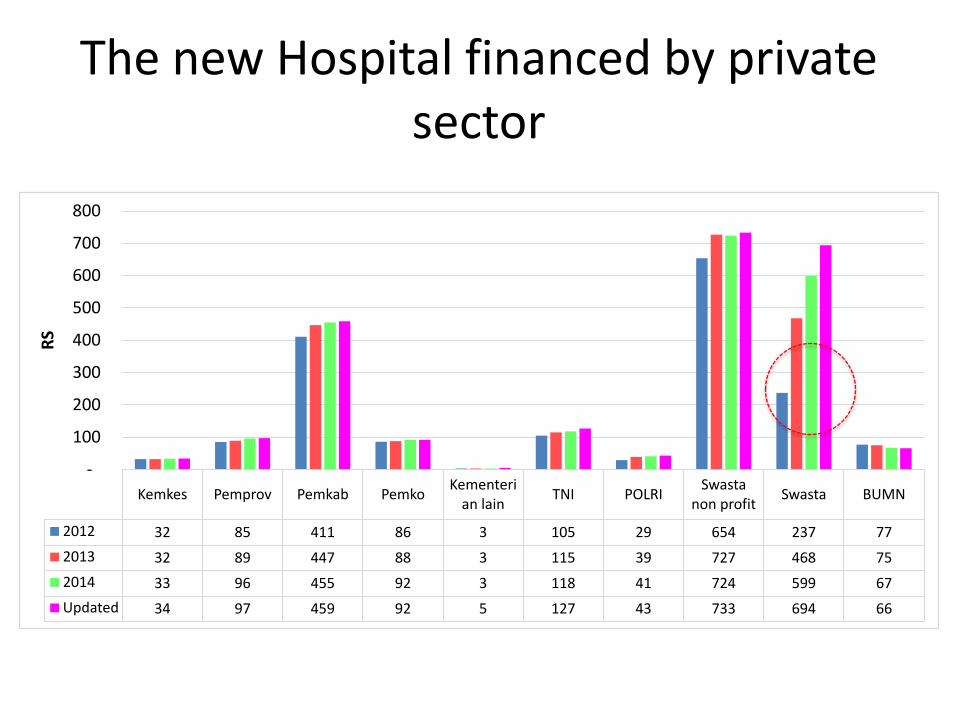
Kemkes Pemprov Pemkab Pemko Kementerian lain TNI POLRI Swasta
non profit Swasta BUMN
2012 32 85 411 86 3 105 29 654 237 77 2013 32 89 447 88 3 115 39 727 468 75 2014 33 96 455 92 3 118 41 724 599 67 Updated 34 97 459 92 5 127 43 733 694 66
-
100
200
300
400
500
600
700
800
RSThe new Hospital financed by private
sector

Specialists Distribution
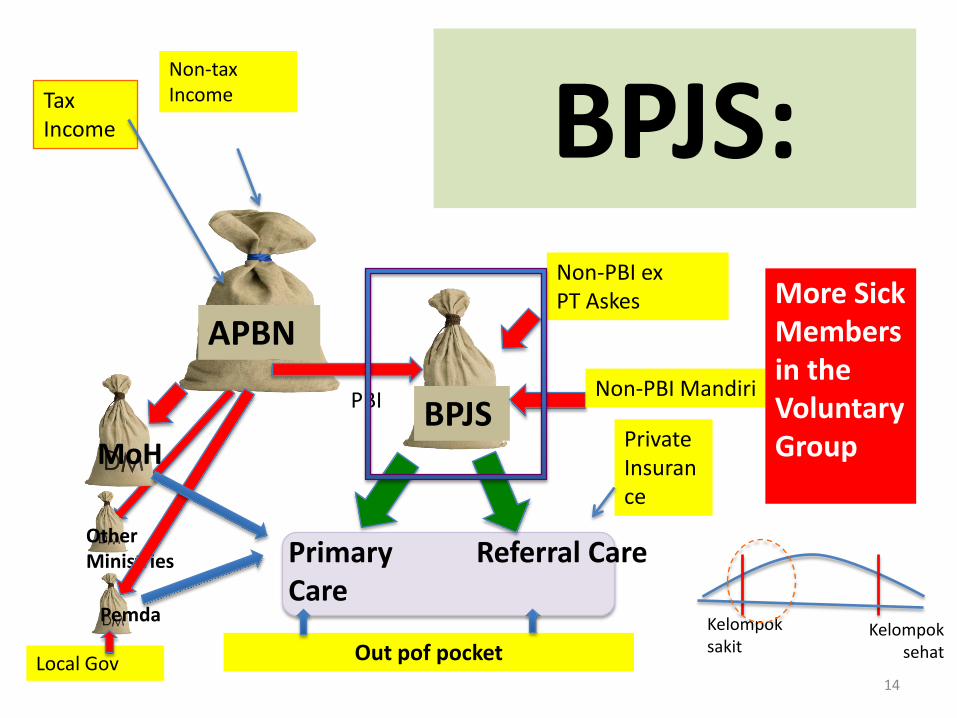
BPJS:
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
14Local Gov
Private Insurance
More Sick Members in the Voluntary Group
Kelompoksakit
Kelompoksehat

Adverse Selection problems in Non-PBI
Mandiri
APBN
BPJS
PajakPendapatanNegara bukan Pajak
Non-PBI Mandiri
PelayananPrimer:
PelayananRujukan
Non-PBiPNS, Jamsostekdll dll
Kemenkes
Dana dari Masyarakat langsung
Kementerianlain
PBI
Pemda
15PendapatanAsli Daerah
Kelompoksakit
Kelompoksehat
AskesSwasta

The health risk in BPJS pool
• Non-PBI-Mandiri(Voluntary Group)Not poor, some rich .
• PBI members (poor member)
• Non-PBI (ex PT Askes )More Healthy members
Kelompoksakit
Kelompoksehat
Kelompoksakit
Kelompoksehat
Kelompoksakit
Kelompoksehat
16
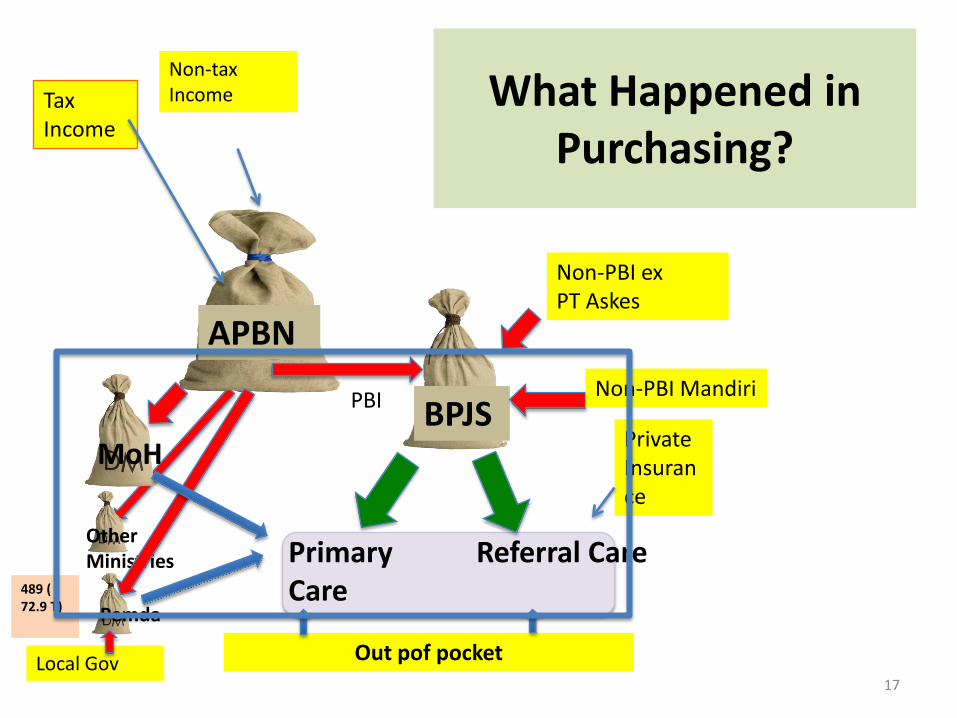
What Happened in Purchasing?
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
17Local Gov
Private Insurance
489 ( 72.9 T)

BPJS, Purchasing and Payment Mechanism
• Kapitasi untuk pelayanan kesehatan primer, dan
• Klaim untuk pelayanan kesehatan rujukan berbasis INA-CBG.
• Capitation for Primary Care
• Claim, based on INA-CBG (DRG) type of payment
18

The facts in 2014• Kapitasi tidak terkait kinerja
FKTP• Tidak ada batas atas
(plafond) di RS dalam melakukan klaim.
• Sistem Pencegahan danPenindakan Fraud belumberjalan
• Daerah dengan SDM lengkap, RS banyak, teknologi tinggiakan menyerap dana BPJS banyak
• Capitation is not linked with performance indicators
• There is no upper limit for hospital in claiming the services
• Fraud Prevention, Detection, deterrence, and prosecution system is not yet established
• Regions which have many doctors, health services, and high technology equipment get the fund more
19

The Risk of this current condition of financing
• Health facilities in remote areas become more lagged behind
• The distribution of human resources for health will suffer
• Not efficient primary care• Fraud will be uncontrollable
and make the use of resources become less efficient
• Adverse selection problems • PBI budget is used by the
middle and higher income group
• Pembangunan RS dan faskes di daerah terpencil tidak dapatmengejar ketinggalan
• SDM kesehatan semakin tidakmerata
• FKTP tidak efisien• Klaim INA-CBGs tidak dijamin
efisiensinya karena fraud tidakterkendali
• Problem Adverse Selection semakin meningkat
• PBI (APBN) disinyalirmenanggung biaya pelayanankesehatan Non PBI (mandiri)
20

Who get the most from BPJS
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
21Local Gov
Private Insurance
In Nov 2014:Claim Ratio is around 1300%
Claim RatioLess than 90% (Nov 2014)

The possibility:PBI Budget is used by Non-PBI
Mandiri (Pekerja BukanPenerima Upah)
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
22Local Gov
Private Insurance
In Nov 2014:Claim Ratio is around 1300%
Claim RatioLess than 90%

• Wheter UHC can be achieved in 2019?
23

Scenario 1: OptimisticScenario 2: Pessimistic.

UHC pessimistic scenario
2014 2015 2016 2017 2018 2019
DIY
NTT
Zero
JKN increases geographical inequity,and also socio-economic inequity
Proposed Strategic Policy to reduce inequity
1. Using more reform approach in JKN; Not only Financing;
2. Short term recommendation in Financing Policy (Revenue Collection, Pooling and Purchasing).
26
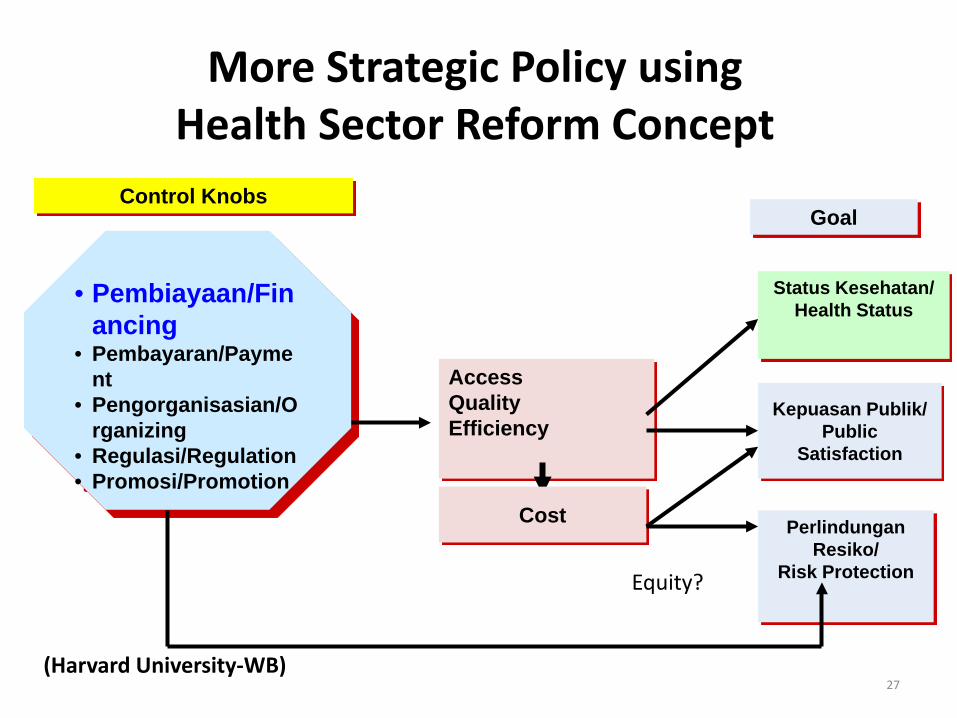
More Strategic Policy using Health Sector Reform Concept
AccessQualityEfficiency
• Pembiayaan/Financing
• Pembayaran/Payment
• Pengorganisasian/Organizing
• Regulasi/Regulation• Promosi/Promotion
Status Kesehatan/Health Status
Kepuasan Publik/Public
Satisfaction
PerlindunganResiko/
Risk Protection
Cost
GoalControl Knobs
27
Equity?
(Harvard University-WB)

Proposed Strategic Policies in Financing to reduce in-equity
28
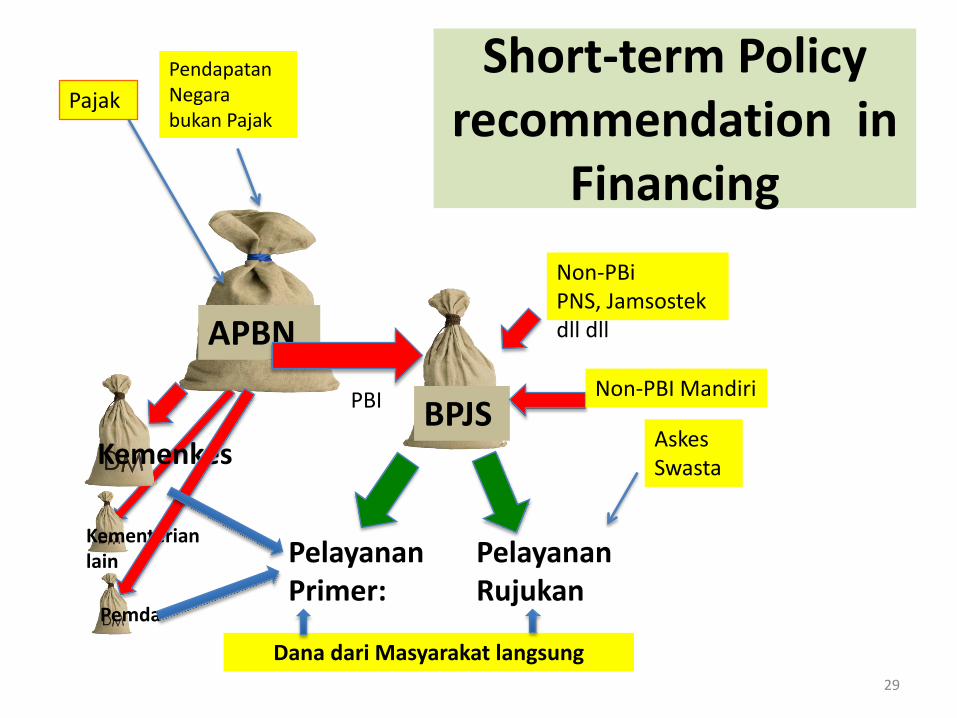
Short-term Policy recommendation in
Financing
APBN
BPJS
PajakPendapatanNegara bukan Pajak
Non-PBI Mandiri
PelayananPrimer:
PelayananRujukan
Non-PBiPNS, Jamsostekdll dll
Kemenkes
Dana dari Masyarakat langsung
Kementerianlain
PBI
Pemda
29
AskesSwasta
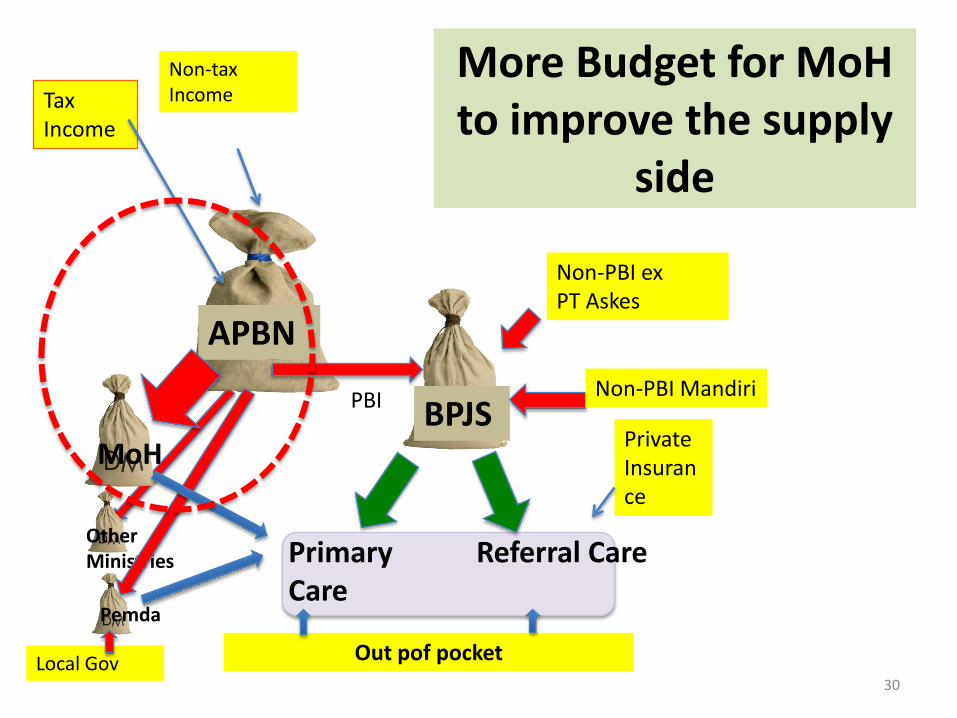
More Budget for MoHto improve the supply
side
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
30Local Gov
Private Insurance

Kemkes Pemprov Pemkab Pemko Kementerian lain TNI POLRI Swasta
non profit Swasta BUMN
2012 32 85 411 86 3 105 29 654 237 77 2013 32 89 447 88 3 115 39 727 468 75 2014 33 96 455 92 3 118 41 724 599 67 Updated 34 97 459 92 5 127 43 733 694 66
-
100
200
300
400
500
600
700
800
RSMore MoH and local government budget to finance
new health services and hospitals

More MoH budget for redistribution of Specialist

Do not increase the premium for PBI
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
33Local Gov
Private Insurance

Increase the premium for the middle and rich
members
APBN
BPJS
Tax Income
Non-tax Income
Non-PBI Mandiri
Primary Care
Referral Care
Non-PBI exPT Askes
MoH
Out pof pocket
Other Ministries
PBI
Pemda
34Local Gov
Private Insurance
Aim:To reduce Claim Ratio

To reduce in-equity: there should be fundamental
change in BPJS
35

Needs compartment in BPJS
• In BPJS there should be compartment based on source of income and expenditure
Aim:• To prevent the budget
from PBI to be used by Non-PBI-mandiri members
(State budget for the poor should be used by the poor)
36

Compartment in BPJS
APBNBPJS
PajakPendapatanNegara bukan Pajak
Non-PBI Mandiri
PelayananPrimer:
PelayananRujukan
Non-PBiPNS, Jamsostekdll dll
Kemenkes
Dana dari Masyarakat langsung
Kementerianlain
PBI
Pemda
37
RpRp
Rp
PendapatanAsli Daerah
AskesSwasta
Thank-you
38
Related Documents











