Fever in Children Blok 26 Agustus 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Fever in Children
Blok 26 Agustus 2014
-
Case 1 v 4-month-old well-appearing girl admitted for croup and
respiratory distress. Develops fever to 39.1oC v What additional evaluation would you do at this point?
-
Case 2 v 10-year old boy with ALL, in induction, admitted for
febrile neutropenia. He had just received his first dose of ceftazidime when he developed another fever to 38.5oC, chills, and new dizziness shortly after receiving the antibiotics. v What would be the next steps in this patients
management?
-
Objectives v To know about fever: definition, classification,
etiology and patophysiology
v To assess patient with fever.
v To determine which patients are at high risk of developing serious bacterial infection.
v To initiate empiric therapy.
-
Objectives v To know about fever: definition, classification,
etiology and patophysiology
v To assess patient with fever.
v To determine which patients are at high risk of developing serious bacterial infection.
v To initiate empiric therapy.
-
Definition of Fever
v Fever: an abnormal elevation of body temperature that occurs as part of a specific biologic response that is mediated and controlled by the central nervous system
v 0 to 28 to 30 days of age: rectal temperature 38.0C
v Healthy one- to three-month-old: rectal temperature 38.0
v Children 3 to 36 months: rectal temperatures 38.0
v Older children and adults: oral temperatures 37.8
-
Classification of Fever v Duration of fever: v Acute ( 14 days ), v Acute recurrent or periodic (episodic
fever separated by afebrile periods) v Chronic (> 14 days), which is more
commonly referred to as fever of unknown origin (FUO)
-
Fever
Fever with localizing
signs
Fever without
localizing signs
Fever of unknown
origin
Classification of Fever
-
Classification Definition Most frequent etiology
Duration of
fever
Fever with localizing signs
Acute febrile illness with focus infection which could be diagnosed by anamnesis & physical examination
Upper respiratory tract infection (URTI)
< 1 week
Fever without localizing signs
Acute febrile illness without focus infection diagnosed after anamnesis & physical examination
Viral infection, urinary tract infection (UTI)
< 1 week
Fever of unknown origin
Fever occured minimal 3 weeks, no established diagnosis yet after 1 week investigation at hospital
Infection, juvenile idiopathic arthritis
> 1 week
Classification of Fever
-
Organ system Diseases Upper airway infections Viral URTI, otitis media, tonsillitis, laryngitis,
herpetic stomatitis Pulmonary Bronkhiolitis, pneumonia Gastrointestinal Gastroenteritis, hepatitis, appendicitis CNS Meningitis, encephalitis Exanthems Campak, chicken pox Collagen Rheumathoid arthritis, Kawasaki disease Neoplasma Leukemia, lymphoma Tropics Kala azar, cickle cell anemia
Fever with Localized Signs Common Causes
Acute febrile illness with focus of infection, which can be diagnosed after history & physical examination
-
Fever without localizing signs
Serious infections occured in 1% cases: serious bacteriemic infections (SBIs)
Children 3-24 months have the highest incidence (3-4%),
aged 7-12 months demonstrating twice incidence association with high fever >39.50C
About 20% all febrile episodes demonstrate no localizing signs
Most common cause is a viral infection Most occuring during the first few years of life
-
Etiology Causes Diagnostic tools
Infections Bacteremia/sepsis Most virus (HH-6) UTI Malaria
Ill looking, high CRP, leukocytosis Well appearing, nomal CRP, WBC Urine dipsticks In malarial area
FUO Juvenile idiopathic arthritis
Pre-articular, rash, splenomegaly, high antinuclear factor, CRP
Post vaccination
DTwP, measles Time of fever onset in relation to the time of vaccination
Drug fever Most drug History of drug intake, diagnosis of exclusion
Fever without localized signs Common causes
-
What etiologies cause fever?
v Infectious
v Inflammatory
v Oncologic
v Other: CNS dysfunction, drug fever
v Life-threatening conditions
-
Infectious v Systemic
v Bacteremia, sepsis, meningitis, endocarditis
v Respiratory v URI, sinusitis, otitis media, pharyngitis, pneumonia,
bronchiolitis
v Abdominal v Urinary tract infection, abscess (liver, kidney, pelvis)
v Bone/joint infection
v Hardware infection v Central line, VP shunt, G-tube
-
Inflammatory v Kawasaki disease
v Juvenile inflammatory arthritis
v Lupus
v Inflammatory bowel disease
v Henoch-Schonlein purpura
-
Others v CNS dysfunction
v Drug fever
-
Pathophysiology of Fever
-
Objectives v To know about fever: definition, classification,
etiology and patophysiology
v To assess patient with fever.
v To determine which patients are at high risk of developing serious bacterial infection.
v To initiate empiric therapy.
-
EVALUATION - History v History of present illness
v degree and duration of fever, method of measurement, and the dose and frequency of antipyretics (if any).
v Important associated symptoms that suggest serious illness include poor appetite, irritability, lethargy, and change in crying (eg, duration, character).
v Associated symptoms that may suggest the cause: vomiting, diarrhea (including presence of blood or mucus), cough, difficulty breathing, favoring of an extremity or joint, and strong or foul-smelling urine.
v Drug history should be reviewed for indications of drug-induced fever.
-
EVALUATION - History v Factors that predispose to infection are identified.
v In neonates: v prematurity, prolonged rupture of membranes, maternal
fever, and positive prenatal tests (usually for group B streptococcal infections, cytomegalovirus infections, or sexuallytransmitted diseases).
v For all children: v recent exposures to infection (including family and
caregiver infection), indwelling medical devices (eg, catheters, ventriculoperitoneal shunts), recent surgery, travel and environmental exposures (eg, to endemic areas, to ticks, mosquitoes, cats, farm animals, or reptiles), and known or suspected immune deficiencies.
-
EVALUATION - History v Review of systems:
v symptoms suggesting possible causes, including
v runny nose and congestion (viral URI),
v headache (sinusitis, Lyme disease, meningitis),
v ear pain or waking in the night with signs of discomfort (otitis media),
v cough or wheezing (pneumonia, bronchiolitis),
v abdominal pain (pneumonia, strep pharyngitis, gastroenteritis, UTI, abdominal abscess),
v back pain (pyelonephritis), and
v any history of joint swelling or redness (Lyme disease, osteomyelitis).
-
EVALUATION - History v A history of repeated infections (immunodeficiency) or
symptoms that suggest a chronic illness, such as poor weight gain or weight loss (TB, cancer), is identified.
v Certain symptoms can help direct the evaluation toward noninfectious causes; they include
v heart palpitations, sweating, and heat intolerance (hyperthyroidism) and
v recurrent or cyclic symptoms (a rheumatoid, inflammatory, or hereditary disorder).
-
EVALUATION - History v Past medical history should note
v previous fevers or infections and known conditions predisposing to infection (eg, congenital heart disease, sickle cell anemia, cancer, immunodeficiency).
v A family history of an autoimmune disorder or other hereditary conditions (eg, familial dysautonomia, familial Mediterranean fever) is sought.
v Vaccination history is reviewed to identify patients at risk of infections that can be prevented by a vaccine.
-
EVALUATION Physical Examination
v Vital signs: v abnormalities in temperature and respiratory rate.
v In ill-appearing children, BP should also be measured.
v Temperature should be measured rectally in infants for accuracy.
v Any child with cough, tachypnea, or labored breathing requires pulse oximetry.
-
EVALUATION Physical Examination
v Child's overall appearance and response to the examination are important. v A febrile child who is overly compliant or listless is of more
concern than one who is uncooperative.
v An irritable infant or child who is inconsolable is also of concern.
v The febrile child who looks quite ill, especially when the temperature has come down, is of great concern and requires in-depth evaluation and continued observation.
v Children who appear more comfortable after antipyretic therapy do not always have a benign disorder.
-
Age is important v >10 % of well-appearing young infants with a
temperature >38C has a serious bacterial infection or meningitis
v Only 39C (manifest bacteremia}
-
Serious Bacterial Infec1on (SBI) Syndromes Pneumonia Meningi,s Bacteremia Osteomyeli,s Urinary tract infec,on Bacterial Gastroenteri,s Sepsis
Allen C: Fever without a source in children 3 to 36 months of age.UpToDate CDROM 18.2,2010 Smitherman HF,Macias CG : Evaluation and management of fever in the neonate and young infant (< 3mo of age),UpToDate
CDROM 18.2,2010 Tolan RW :Fever Without a Focus , http://www.medscape.com, 2009
-
ETIOLOGY Serious Bacterial Infection (SBI)
Common Bacterial Etiology of SBI Streptococcus pneumoniae Streptococcus agalactiae Neisseria meningitidis Haemophilus influenzae type b Listeria monocytogenes Eschericia coli
Allen C: Fever without a source in children 3 to 36 months of age.UpToDate CDROM 18.2,2010 Smitherman HF,Macias CG : Evaluation and management of fever in the neonate and young infant (< 3mo of age),UpToDate
CDROM 18.2,2010 Tolan RW :Fever Without a Focus , http://www.medscape.com, 2009
-
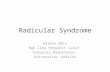
Source: Jornal de Pediatrica - Vol. 85, No. 5, 2009
-
Yale Observa1on Scale (YOS) degree of Illness Indica,ons Assessment of febrile child ages 3-36 months
Predicts serious infec,on (Occult Bacteremia) Quan,fies "Toxic Appearance" in children
Observa1on Items 1 (Normal) 3 (Moderate Impairment)
5 (Severe Impairment)
Quality of cry Strong with normal tone or contentment without crying
Whimpering or sobbing Weak cry, moaning, or high-pitched cry
Reac1on to parent s1mula1on
Brief crying that stops or contentment without crying
IntermiJent crying Con1nual crying or limited response
Color Pink Acrocyano1c or pale extremi1es
Pale or cyano1c or moJled or ashen
State varia1on If awake, stays awake; if asleep, wakes up quickly upon s1mula1on
Eyes closed briefly while awake or awake with prolonged s1mula1on
Falls asleep or will not arouse
Hydra1on Skin normal, eyes normal, and mucous membranes moist
Skin and eyes normal and mouth slightly dry
Skin doughy or tented, dry mucous membranes, and/or sunken eyes
Response (eg, talk, smile) to social overtures
Smiling or alert (
-
Yale Observa1on Scale (YOS) degree of Illness Indica,ons Assessment of febrile child ages 3-36 months
Predicts serious infec,on (Occult Bacteremia) Quan,fies "Toxic Appearance" in children
-
A total score of less than 11 signifies a less than 3% probability of serious illness.
A total score 11-15 signifies a 26% probability serious illness
A total score of greater than 15 signifies 92 % probability of serious illness
-
Laboratory evaluation v What would you do if the patient has device (VP
shunt, tracheostomy, gastrostomy tube) or central line? v CBC with differential
v Blood culture
v CSF (tap VP shunt)
-
Laboratory evaluation v What would you do if the patient has a high risk for
sepsis? v Immunocompromised v Transplant recipient v Oncology patient
v CBC with differential v Blood culture v Urinalysis and urine culture
-
Laboratory evaluation v What would you do for an infant 2 months of age?
v CBC with differential
v Blood culture
v Urinalysis and urine culture
v Lumbar puncture
-
Laboratory evaluation v Who needs a urinalysis and urine culture?
v Circumcised males < 6 months
v Uncircumcised males < 1 year
v Females < 2 years
v Immunocompromised patients
v Patients with history of UTI/pyelonephritis
-
Laboratory evaluation v Who needs a lumbar puncture?
v Neonates 2 months v Ill-appearing v Altered mental status
v What tests do you send? v Gram stain and culture v Cell count and differential v Protein and glucose v Extra tube for additional studies
v Enteroviral PCR, HSV PCR, CA encephalitis project
-
Laboratory evaluation v Consider CRP, ESR
v Consider PT/PTT, fibrinogen
v Consider chest x-ray
v Consider nasopharyngeal DFA
v For immunosuppressed patients consider: v Viral PCR studies (ie CMV, EBV, HHV6)
v Additional imaging (ie ultrasound, CT scan)
-
Objectives v To know about fever: definition, classification,
etiology and patophysiology
v To assess patient with fever.
v To determine which patients are at high risk of developing serious bacterial infection.
v To initiate empiric therapy.
-
Which patients are high-risk for serious bacterial infection?
v Neonates
v Transplant recipients v Bone marrow
v Solid organ
v Oncology patients v Undergoing therapy, mucositis, central line
v Most chemotherapy: nadir ~ 10 days after rx
v Asplenic patients, including sickle cell
-
Objectives v To know about fever: definition, classification,
etiology and patophysiology
v To assess patient with fever.
v To determine which patients are at high risk of developing serious bacterial infection.
v To initiate empiric therapy.
-
Treatment for non-high risk patients
v May not need empiric antibiotics
v Consider the following issues: v Is patient clinically stable?
v Are the screening laboratory studies suggestive of infection?
-
Yale Observation Scale
A total score of less than 11 signifies a less than 3% probability of serious illness.
A total score 11-15 signifies a 26% probability serious illness
A total score of greater than 15 signifies 92 % probability of serious illness
-
Treatment for patients with central lines
v Ceftriaxone
v Vancomycin
-
Treatment for neonates 2 months
v If < 28 days old v Ampicillin AND cefotaxime OR v Ampicillin AND gentamicin
v Consider acyclovir
v If 29-60 days old v Ceftriaxone Ampicillin OR Vancomycin
v Until CSF results are known (cell count, protein, glucose), initiate therapy with meningitic dosing regimen
-
Treatment for febrile neutropenia v Broad-spectrum antibiotics with Pseudomonas
coverage v Ex: use ceftazidime or piperacillin-tazobactam
v Consider double coverage for possible resistant Pseudomonas v Ex: add amikacin or tobramycin
v Consider gram-positive coverage (central line, skin infections) v Ex: add vancomycin
v Consider anaerobic coverage (mucositis, typhlitis) v Ex: use piperacillin-tazobactam or add clindamycin
-
Take home points v Infections are the most common cause of
fever in children
v During assessment of a child with fever, pay close attention to vital sign changes, overall appearance, and potential sites of infection
v Closely monitor for clinical decompensation after antibiotic administration, particularly in patients at high-risk of developing sepsis
-
References v Baraff LJ. Management of fever without source in infants and
children. Ann Emerg Med. 2000. 36:602-14.
v Meckler G, Lindemulder S. Fever and neutropenia in pediatric patients with cancer. Emerg Med Clin N Am. 2009. 27:525-44.
v Palazzi EL. Approach to the child with fever of unknown origin. UpToDate. 2011
v Palazzi DL. Etiologies of fever of unknown origin. UpToDate. 2011.
v Tolan R. Fever of unknown origin: A diagnostic approach to this vexing problem. Clin Pediatr. 2010;49:207-13.
Related Documents