Amir H. Bakhtiary PhD, PT Associate Professor Physiotherapy Department Rehabilitation faculty Semnan University of Medical Sciences Knee Joint Kinesiology

Knee Joint Kinesiology
Jan 03, 2016
Knee Joint Kinesiology. Amir H. Bakhtiary PhD, PT Associate Professor. Physiotherapy Department Rehabilitation faculty Semnan University of Medical Sciences. Knee Extensors Muscles. Gluteus Max and Soleus may help knee Ext in Closed Kinematic Chain (Movements. Quadriceps. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Amir H. BakhtiaryPhD, PT
Associate Professor
Physiotherapy DepartmentRehabilitation faculty
Semnan University of Medical Sciences
Knee Joint Kinesiology

Knee Extensors Muscles

Gluteus Max and Soleus may help knee Ext in Closed Kinematic Chain (Movements

Quadricepsعضله چهارسر رانی
تنها بخش دومفصلی آن رکتوس فموریس است•جهت نیروی کشش آن نسبت به تنه فمور •
درجه به جلو5 تا 3 درجه به داخل و 7-10• درجه بطرف خارجVL 35جهت کشش • موازی با تنه فمورVIجهت کشش • VMجهت کشش •
درجه بطرف داخل18 – 15الیاف فوقانی − درجه بطرف داخل55-50الیاف تحتانی یا مایل −
زانو فعال می شودExt درانتهای دامنه VMبخش •


Compress force

نقش پاتال بر عملکرد عضله چهار سررانی را تعریف کنید؟
قرار گرفتن پاتال در داخل تاندون عضله چهار سررانیافزایش گشتاور نیروی عضله چهارسررانی از طریق•
تاندون چهار سررانیMAافزایش •افزایش فاصله تاندون کوادریسپس و پاتال از محور حرکت زانو•
تغییر جهت خط کشش عضله کوادریسپس•افزایش زاویه کشش تاندون•کاهش اصطکاک بین تاندون و سطح فمور•نقشی بیشتر از یک قرقره ساده بازی کرده•
هم تغییر جهت نیرو•هم تغییر اندازه نیرو•
% 49برداشتن پاتال موجب کاهش نیروی کوادریسپس تا •MAبدلیل کاهش

The role Of patella in improving Quadriceps Torque

Anterior Translation Force of Quadriceps
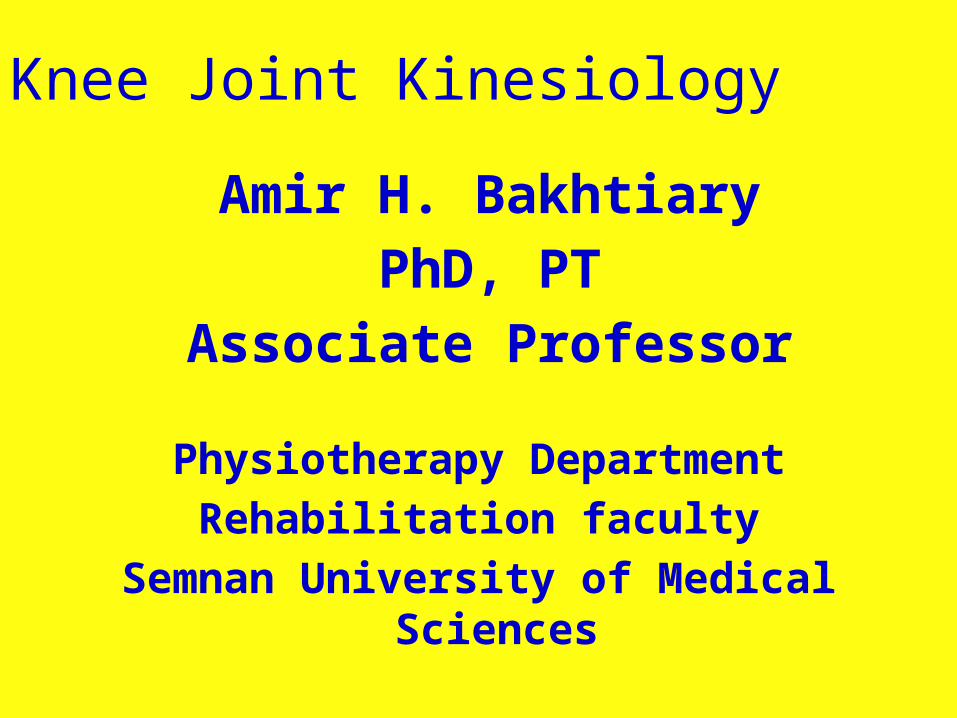
Increase the muscle force by Knee Ext in OKC
Cause More tension on the ACL

Decease the muscle force by Knee Ext in OKC
Cause Less tension on the ACL

Quadriceps Weakness

Patellofemoral Jointنقش پاتال در مفصل پاتلوفمورال مانند قرقره
( 2( تغییر جهت نیرو، 1اکسنتریک آناتومی شامل ( کاهش اصطکاک بین سطوح3افزایش اثر نیرو و
بستگی به قابلیت تحرک چهار گانه آن دارد••Patellar Flexion/Extension)تحرک اصلی( •Patellar Tilt اجازه تطبیق پاتال با کندیلهای نامتقارن(
فمور(•Med Tilt بین( درجه 100 الی 30-0 Flex)•Lat Tilt بین( درجه 100 الی 20 Flex)
•Med & Lat Rotation چرخش زاویه تحتانی پاتال به( تبعیت از تیبیا(
درجه به خارج می چرخد7-6 پاتال Flex درجه 100 الی 25بین ••Medio-lateral Translation یا Patellar Shift
•Active در انتهای :EXT 7/5 10 تا mmجابجایی خارجی •Passive:
− Full Ext :جابجایی داخلی( 9.6 mm :5.4، جابجایی خارجی mm )(mm 10، جابجایی خارجی: mm 9.4 )جابجایی داخلی: Flexدرجه 35در −

Patella Movement During Knee Flexion
Open kinematics Chain

Patella Movement During Knee Flexion
Closed kinematics Chain

Patellar Tilting

Medial and Lateral rotation
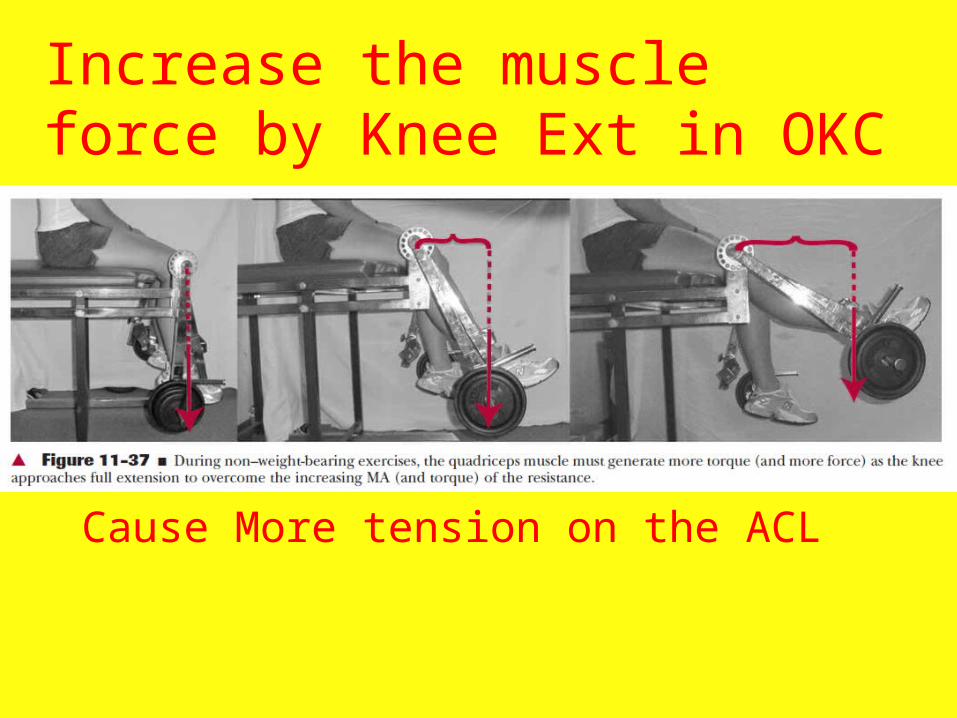
Medial and Lateral Shift

سطح مفصلی پاتلوفمورالناسازگارترین سطوح مفصلی بدن•
سطح مفصلی پاتال بسیار کوچکتر از فمور•خصوصیات غضروفی ان از یک نقطه به نقطه •
دیگر متفاوت استسطح مفصلی پاتال توسط غضروف ضخیمی •
پوشیده شدهتوسط یک ستیغ مرکزی به دو بخش داخلی و •
خارجی تقسیم شدههر دو بخش صاف تا کمی محدب )در دو صفحه •
ساژیتال و فرونتال( Odd% موارد فاست داخلی تری به نام 30در •
Facet سطح مفصلی فمور با یک شیار به دو بخش •
داخلی و خارجی در فرونتال مقعر و در ساژیتال محدب )فاست •
خارجی محدب تر( بین 151 تا ° 116 )از 138زاویه بین دو فاست °•
افراد مختلف متغییر(
Patellofemoral Joint Surface

Patellar Joint Surface

Patellofemoral Joint Surfaces
سطح تماس پاتال با فمور وجود نداردFull extهیچ تماسی در • تماس سطوح افزایش یافته )از Flexبا افزایش •
پایین به باال( اولین تماس با سطح تحتانی Flex درجه 20 تا 10در •
پاتال نیمه میانی پاتال وارد تماس شدهflex درجه 45در • تمام قسمتهای پاتال وارد تماس شدهflex درجه 90 در • درجه پاتال وارد شیار بین کندیلی 90 بیش از flexبا •
در تماس قرار گرفتهOdd facetشده و Odd تماس فقط در فاست خارجی و flex درجه 135در •
Facet odd Facetفاست داخلی بیشترین تماس و •
کمترین تماس را تجربهعدم تعادل در نیروهای وارده بر غضروف مفصلی منجر •
به تغییرات دژنراتیو در این فاستها می گردد
Patellofemoral Contact Surface

نیروهای وارده روی مفصل پاتلو فمورال نیروهای کوادریسپس و پاتال یکدیگر را Full extدر •
خنثی کردهپاتال در حالت تعادل در مقابل فمور قرار دارد•
برآیند این دو نیرو موجب فشرده Flexبا افزایش •شدن پاتال روی فمور
این نیرو افزایش یافتهFlexبا افزایش •موجب نیروی عکس العمل روی سطوح مفصلی گردیده •
که میزان آن تحت تاثیر•Knee Flexion•Quadriceps Force•Elastic Passive Force
اندازه نیروی عکس العمل •% وزن بدن50 زانو( Flex درجه 15 تا 10راه رفتن عادی )• برابر 3.5 زانو( Flex درجه 90 تا 60باال و پائین رفتن از پله )•
وزن بدن برابر 8( تا Flex درجه 135 شدید زانو )Flexفعالیتهای همراه با •
وزن بدن
Reaction Force on the Patellofemoral Joint

Reaction force on the patellofemoral surface

Medial shift of Patella during Flexion

Mechanism of Lateral force on the patella

What is the Compensatory Mechanisms for Compressive Force Distribution in patelofemoral joint?
• Contact area with knee flexion• Medial facet contact from 30-70
• Thickest hyaline cartilage in body
• Largest QF MA 30-70• QF torque as MA decreases
• QF tendon contacts condyles 70-90

What are the Medial and Lateral Stability factors of Patellofemoral Joint?
تحت تاثیر متقابل دو PFثبات طرفی مفصل مکانیسم قرار دارد
مکانیسم عرضی )رتیناکولوم اکستانسوری)•مکانیسم طولی )تاندونهای پاتال و کوادریسپس)•تعادل بین این دو مکانیسم منجر به حرکت صحیح •
Patellarپاتال هنگام حرکات زانو میشود یا Tracking
در صورت بر هم خوردن تعادل بین عوامل فوق •حرکت پاتال روی فمور دچار اختالل می گردد

Normal Patella Tracking
Maintains maximum congruence
Passive restraints Active restraints

Abnormal Patella Tracking
↓ congruence Stretches capsule & retinacula ↓ contact area
Lateral Medial

Causes of Abnormal Tracking
Skeletal abnormalities Strength imbalance in QF Strength imbalance in fibrous tissues Compensatory movements in knee due to
abnormal foot movement

Causes of Abnormal Tracking
Skeletal abnormalities Strength imbalance in QF Strength imbalance in fibrous tissues Compensatory movements in knee due to
abnormal foot movement

Skeletal Abnormalities: Q-angle
15 تا °10مقدار طبیعی = کاهش یافتهFlexبا
عوامل موثر بر افزایش آنپهنتر بودن لگن1. فمورanteversionافزایش 2. زانوValgusافزایش 3.
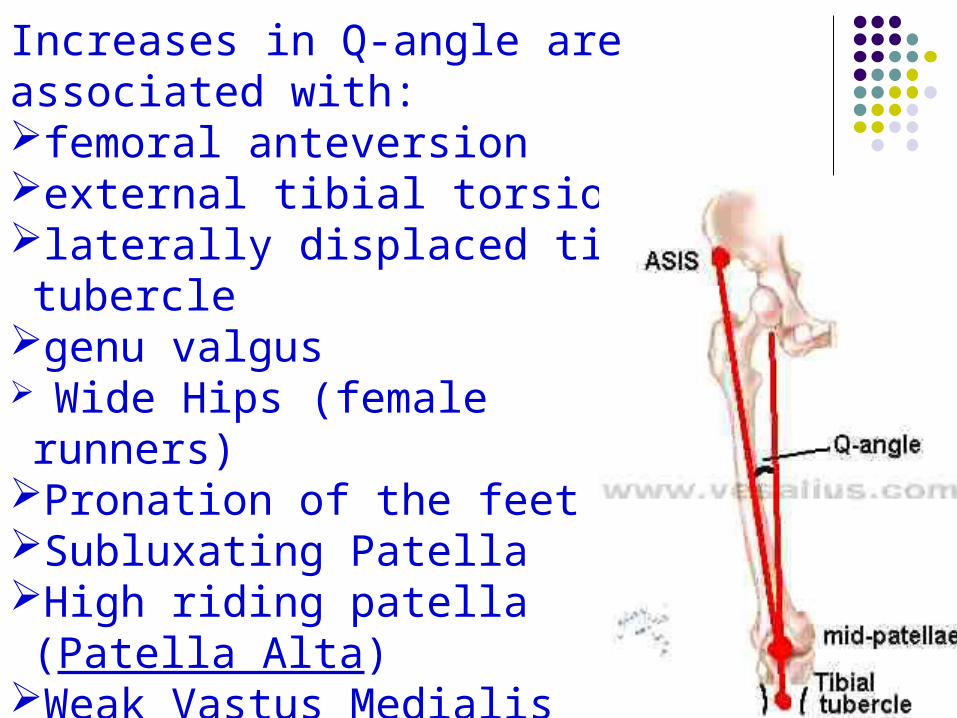
Increases in Q-angle are associated with: femoral anteversion external tibial torsion laterally displaced tibial tubercle genu valgus Wide Hips (female runners)Pronation of the feetSubluxating PatellaHigh riding patella (Patella Alta)Weak Vastus Medialis

Q Angle and contact pressure

Skeletal Abnormalities: Genu Varum & Genu Valgum
Q angle w/ age Varum common in
very young children Valgum seen in
growing children Menisectomy effects

Skeletal Abnormalities: Patella Alta & Patella Baja
Index of Insall & Salviti LP/LT Normal = 1.0 Patella alta = 0.8 Patella baja = 1.2 Women ratio

Skeletal Abnormalities: Patella Surface Lateral Border
Appositional forces ↓ in full extension
Prominence of lateral border prevents lateral displacement
Underdevelopment common in children as growing

Skeletal Abnormalities: Femoral & Tibial Torsion
Lateral tracking

Causes of Abnormal Tracking
Skeletal abnormalities Strength imbalance in QF Strength imbalance in fibrous tissues Compensatory movements in knee due to
abnormal foot movement

QF Strength Imbalance
Causes of Abnormal Tracking
Skeletal abnormalities Strength imbalance in QF Strength imbalance in fibrous tissues Compensatory movements in knee due to
abnormal foot movement

Fibrous Tissue Strength Imbalance
IT

Causes of Abnormal Tracking
Skeletal abnormalities Strength imbalance in QF Strength imbalance in fibrous tissues Compensatory movements in knee due to
abnormal foot movement

Compensatory Movement
Pronation of foot accompanied by medial rotation of tibia medial rotation & medial translation of patella
Pronation coupled w/ forceful quadriceps femoris leads to anterior tilt
EX: jumping, landing, running
Knee pathology

Meniscal lesion

Meniscal lesion can also occur through a collision and is thought deep knee bends can also be a cause.
A transverse tear of the lateral meniscus
A transverse tear of the lateral meniscus
A longitudinal tear of the lateral cartilage meniscus

Damage to the medial meniscus at it's attachment to the ligament. Also shown a longitudinal tear in the lateral meniscus.The cartilage gets squeezed between the bones with most of your bodyweight on top!

McMurray's click test for the integrity of the meniscus. This test is done to "pinch" the menisci against the femur. Internal rotation of the tibia on the femur stresses the posterior medial and the anterior lateral menisci

McMurray's click test for the integrity of the meniscus. This test is done to "pinch" the menisci against the femur. External rotation stresses the anterior medial menisci and the posterior horn of the lateral menisci.

Osteocartilage degenerative changes

History of Injury
• Acceleration Mechanisms • (lower leg slipping forwards(
• Deceleration Mechanisms • (lower leg stops suddenly(
• Hyper Extension Mechanisms • (Bad Tackle(
• Torque ('twisting'( Mechanisms (jumping while twisting, when the foot lands and grips the ground surface, while the body continues the twisting motion with the full weight of the person behind it.

ACL & PCL injury

Anterior Drawer Sign
The ACL ligament is injured through twisting the knee or through an impact to the side of the knee - often the outside.

Posterior Drawer SignThe posterior Cruciate ligament is injured through hyperextension of the knee or bending it backwards.

Jumpers Knee(Patellar tendinopathy - sometimes called Patellar tendinitis(
Under extreme stresses such as those involved in jumping a partial rupture can occur. This can often lead to inflammation and
degeneration of the tissue. Inflammation can also result from overuse.

Patella AltaPatella alta – the patella rides so high it loses the passive stabilisation of the lateral condylar ridge.

Side to Side Unstability

Collateral Ligaments Injury

If the force from the injury is great enough, other ligaments may also be torn. The most common
combination is a tear of the MCL and a tear of the anterior cruciate ligament (ACL(.
Related Documents