Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017 Dr Keith Holt Osteo-arthritis is a condition in which there is wear and tear of the smooth bearing surfaces of a joint. Initially this wear may not give rise to symptoms. Ultimately however, pain, stiffness, and even deformity may result. A range of treatments, from anti-inflammatory tablets through to replacement, are available to help in the various stages of this condition. What is Arthritis? The term 'Arthritis' literally means 'inflammation of a joint'. There are many causes of this but, the end result of all of these processes, is a joint where the smooth, low friction bearing surfaces on the ends of the bone become worn out. This special surface (made of hyaline cartilage) is the same shiny white surface that can be seen on the end of a lamb (or other animal) bone, and is responsible for the extremely low friction bearing surfaces of our major joints (about ten times less friction than the best man made bearing surface). Wear or damage to this is generally known as 'osteo-arthritis' and may be primary (where the surface just wears out prematurely - i.e. degenerative), or secondary (where the damage is caused by direct injury, inflammatory conditions such as rheumatoid arthritis, infections and so on). Arthritis secondary to injury A major joint injury, where the surface is directly damaged (as happens in at least 10% of anterior cruciate ligament injuries), is essentially a seed for the onset of osteo-arthritis proper. The damaged hyaline cartilage not only doesn't make any attempt to heal itself, but rather, the area of damage slowly deteriorates with time, gradually enlarging. In that initial injury, a piece of the lining tissue (hyaline cartilage) may be exploded out of the weight bearing surface creating a pot hole. That pot hole then, like all pot holes, gets gradually bigger because of the inevitable breakdown of the edges. Eventually, the weight bearing part of the joint becomes a large area of bare bone with no bearing surface at all and, this in turn, wears out its counterpart, the surface which it articulates with on the other side of the joint. This goes on to become advanced osteo-arthritis and, as might be expected, it is hastened by impact loading type activities such as running and jumping. Primary or Degenerative arthritis Degenerative osteo-arthritis, rather than anything else, has to do with inheriting a joint with a short 'use by' date. No one knows why some people's joints wear out early and why some do not, albeit that the pathologic changes that occur are somewhat understood. The thing about degenerative arthritis is that it is not caused by sport, exercise or physical jobs. Indeed, there is no evidence that marathon runners' knees wear out any quicker than couch potatoes'. In fact, Knee Arthritis A normal right knee Arthritis following knee injury The gap between the bone ends is not a gap, but rather, it is the thickness of the articular surface (hyaline cartilage) which cannot be seen on an x-ray This knee shows normal gaps No gap at all indicates bone on bone arthritis. That is, there is no remaining lining (bearing surface) Same Patient

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
Dr Keith Holt
Osteo-arthritis is a condition in which there is wear and tear of the smooth bearing surfaces of a joint. Initially this wear may not give rise to symptoms. Ultimately however, pain, stiffness, and even deformity may result. A range of treatments, from anti-inflammatory tablets through to replacement, are available to help in the various stages of this condition.
What is Arthritis?
The term 'Arthritis' literally means 'inflammation of a joint'.
There are many causes of this but, the end result of all of
these processes, is a joint where the smooth, low friction
bearing surfaces on the ends of the bone become worn out.
This special surface (made of hyaline cartilage) is the same
shiny white surface that can be seen on the end of a lamb
(or other animal) bone, and is responsible for the extremely
low friction bearing surfaces of our major joints (about ten
times less friction than the best man made bearing surface).
Wear or damage to this is generally known as 'osteo-arthritis'
and may be primary (where the surface just wears out
prematurely - i.e. degenerative), or secondary (where the
damage is caused by direct injury, inflammatory conditions
such as rheumatoid arthritis, infections and so on).
Arthritis secondary to injury
A major joint injury, where the surface is directly damaged
(as happens in at least 10% of anterior cruciate ligament
injuries), is essentially a seed for the onset of osteo-arthritis
proper. The damaged hyaline cartilage not only doesn't make
any attempt to heal itself, but rather, the area of damage
slowly deteriorates with time, gradually enlarging.
In that initial injury, a piece of the lining tissue (hyaline
cartilage) may be exploded out of the weight bearing surface
creating a pot hole. That pot hole then, like all pot holes,
gets gradually bigger because of the inevitable breakdown
of the edges. Eventually, the weight bearing part of the joint
becomes a large area of bare bone with no bearing surface
at all and, this in turn, wears out its counterpart, the surface
which it articulates with on the other side of the joint. This
goes on to become advanced osteo-arthritis and, as might
be expected, it is hastened by impact loading type activities
such as running and jumping.
Primary or Degenerative arthritis
Degenerative osteo-arthritis, rather than anything else, has
to do with inheriting a joint with a short 'use by' date. No
one knows why some people's joints wear out early and why
some do not, albeit that the pathologic changes that occur
are somewhat understood. The thing about degenerative
arthritis is that it is not caused by sport, exercise or physical
jobs. Indeed, there is no evidence that marathon runners'
knees wear out any quicker than couch potatoes'. In fact,
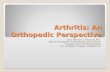
Knee Arthritis
A normal right knee Arthritis following knee injury
The gap between the bone ends is not a gap, but rather, it is the
thickness of the articular surface (hyaline cartilage) which cannot
be seen on an x-ray
This knee shows normal gaps
No gap at all indicates bone on bone arthritis. That is, there is no remaining lining (bearing surface)
Sam
e Pa
tient

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
the only evidence for these factors is just the opposite, with
obesity being a proven cause of premature arthritis of the
weight bearing joints. Having said the above however, it is
clear that once a joint is damaged, or is starting to wear, then
the more it is used, the more rapidly it will wear.
Diagnosing arthritis?
Despite all the available tests, the diagnosis of osteoarthritis
can be difficult to make in its early phases, and it can be
missed. Plain x-ray, despite its simplicity, is still one of the
best methods of diagnosing this: especially when special
views are obtained.
Plain x-ray imaging remains the mainstay of initial diagnosis.
It is the cheapest of the investigations and, once the wear
starts to progress, it is the easiest to assess. It is not because
the lining tissue becomes visible on X-rays, but rather, as the
lining tissues start to wear, the gap between the bones becomes
visibly narrower. As the area of most wear usually involves
those areas which are in contact whilst weight bearing with
the knee 20º bent (20º of flexion), the most sensitive x-ray
is one taken from behind the knee when weight bearing in
that position. This view is very important, not only for primary
diagnosis, but also when trying to assess severity.
Another feature which may be seen is small bone spurs
(osteophytes) which protrude from the side of the joint. It is
thought that these develop as a consequence of increased
stresses on the underlying bone, and they do get bigger as
the osteo-arthritis progresses. Whilst easily visible on an x-ray
however, they do not in themselves cause too many problems,
and removing them is rarely worthwhile.
Eventually, other changes also start to appear: such as cysts in
the bone and bone build up (sclerosis), all of which indicate
progressive osteo-arthritis. Cysts are particularly characteristic
of advanced wear, representing joint fluid that is being pushed
into the unprotected underlying bone. They represent a failure
of that underlying bone to cope with the increased stresses
being imposed upon it and, usually, imply that treatments such
as an arthroscopic clean up (chondroplasty) will probably not
help. Indeed, such treatment often aggravates the situation
and can make the symptoms worse.
MRI is good in that it can not only see the joint lining, it can
also see if there is swelling in the underlying bone. Thus, it
can detect stress reactions and stress fractures, additional
problems that sometimes occur under an area of wear.
CT arthrogram, where a radio-opaque dye is put into the
knee and the area is CT scanned, is perhaps the best method
of determining the thickness of the articular surface, and it is
very sensitive to defects in that lining. Unfortunately however,
it does not see the underling bone and cannot detect swelling
or stress injury to the bone; factors that maybe very important
in trying to determine the best treatment option.
X-ray - moderate arthritis
MRI - arthritis with stress fracture
X-ray - very advanced arthritis
Bone on bone wear (no
remaining lining)Normal gap
(lining thickness)
End stage wear
Right Knee
Bone translocation
Cysts
Spurs
Thin lining (light grey on bone end)
Stress fracture (dark area)
Stress fracture (dark area)
Underlying swelling in the bone (white area)
Normal lining(light grey)

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
Arthroscopy, where the joint surfaces can be inspected,
can be normal early on. When the arthritis presents as pot
holes in the joint surface, arthroscopy provides a very good
assessment. Sometimes however, the lining can by intact
and look smooth, but it is actually thin. In this instance,
arthroscopy is not so helpful.
Clearly, no one test is optimal and sometimes more than one
test is necessary to work out the exact pathology.
What is the cause?
The cause in the degenerative joint remains unknown. We
know that the chondrocytes, the hyaline cartilage cells which
lie on the deep surface of the cartilage layer, start to produce
less of the osmotic molecules (proteoglycans) which hold
fluid in the lining layer. It is this fluid that is responsible for
the sponginess of the lining, and therefore, is responsible
for the forgiving nature of that layer during impact loading.
In addition to this however, the majority of this layer is
made up of collagen arcades which look like arches under
a microscope. These are responsible for the strength that
the hyaline lining has, hence, when the chondrocytes fail to
maintain this structure (the extra-cellular matrix - the tissue
outside the cell), the surface is susceptible to wear and
degradation. That is - osteo-arthritis.
When looking at the microscopic structure of the hyaline
cartilage, it is important to note that the cartilage cells
(chondrocytes) are few and far between, and they are deep
in the tissue, near the bone. These cells, in themselves, are
not the structural element of the lining tissue but rather,
they manufacture and maintain the matrix of that tissue (the
collagen arcades, proteoglycans etc.), which is the structural
element. They only divide, at most, once in a persons' lifetime,
and hence, they have little or no capacity to heal any damage.
Once they start to fail or die, they are not replaced: the matrix
fails and osteo-arthritis (wear) ensues.
The evidence would suggest that, with age, the chondrocytes
become less able to maintain the extra-cellular matrix. Hence,
the hyaline cartilage layer becomes more brittle and becomes
more susceptible to stress related injury and wear as one gets
older. In some however, that wear develops prematurely
and, whilst the cause of that is unknown, genetic factors are
known to play a role.
The cause in the injured joint is clearer. When a traumatic
injury to the joint has caused significant injury to the articular
layer, it will not recover. If this injury involves a defect, where
a piece of lining tissue has been exploded out of the joint
surface, then this is a permanent injury. This sort of injury
usually occurs with a twisting injury when the joint under
load. It is a shearing compression injury, which is not all that
uncommon in twisting turning sports, but particularly rugby.
A near normal knee
More advanced osteo-arthritis
Mild wear
Moderately advanced wear
Mild wear
Some meniscal
loss
Mild osteo-arthritis
Right medial femoral condyle
Right medial tibial plateau
Right medial meniscus

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
and they do cause increased pressure to be applied to part
of the joint, leading to premature wear. A straight legged
person places 60% of their weight on the inside (medial
compartment) of their leg, and 40% on the lateral. That is
what the joint is designed to take. A bow legged (varus) person
places more than 60% of his weight on the inside half of the
joint, whereas a knock kneed (valgus) person places more
on the outside half of the joint. In each instance, one side of
the joint becomes overloaded and the other side becomes
unloaded or even unused. This means that the stresses on
the overloaded side of the joint are higher than normal, and
hence, premature wear may occur in that half of the joint.
This, in association with loss of meniscal function, can be
devastating for the joint in the longer term.
A common scenario is that there is degenerative breakdown
of the meniscal cartilage, presenting as a painful knee, often
of sudden onset. Degenerative tears of the menisci can be
very painful, they do not heal by themselves and, for the
most part, cannot be successfully repaired. Treatment, by
removal of the torn parts of that cartilage (partial or total
menisectomy), usually relieves the pain but, it also leads to
increased pressure on the articular or lining cartilage because
the stress is now focused on a smaller area, hence, wear of
the lining surface or osteo-arthritis may occur.
Without any deformity this increased pressure on the ends
of the bone may not be all that significant but, if there is also
Other causes of wear stem from overload of the hyaline
cartilage lining, rather than from direct injury. Such abnormal
forces are commonly seen after menisectomy, where a
meniscal cartilage is removed for a tear. Particularly important
with this, is the effect of any mal-alignment of the leg, which
can also change the forces within the joint.
Meniscal cartilage loss
The menisci (meniscal cartilages - sometimes known as 'the cartilages') function as fillers to spread the load between the surfaces of the femur and tibia. The ends of these bones are not the same shape, and thus, the menisci are needed to make up for that incongruity. They primarily function somewhat like shock absorbers but they also have a secondary role to enhance lubrication and nutrition of the articular or lining cartilage.
Loss of a meniscus (particularly the lateral one) leads to a poor spread of weight across the joint surface. This means that loads are taken over smaller areas of the joint, and hence, pressures are higher, causing increased rates of wear of the lining surface (the hyaline cartilage). It also follows, that the more meniscus that is lost, the faster that wear occurs.
Mal-alignment of the leg
Another cause of increased wear is a mal-aligned (crooked)
leg, such as a knock knee deformity (valgus) or a bow leg
(varus) deformity. These are not uncommon in the community
After loss of a meniscus, it can be seen that the lateral (outside) part of the knee has higher contact pressures because of the convex on convex structure of that part of the joint. Hence, wear in the lateral (outside) compartment of the knee develops more rapidly than it does in the medial (inside) compartment of the knee, where the joint is convex on concave. This wear (osteo-arthrits) ultimately leads to the end of impact loading type sports, including all running. Ultimately, it may also lead to knee replacement.
In the normal knee, the meniscus is a mobile structure that makes the joint spaces congruous and spreads the load over a wide area of the joint lining (articular surface). By increasing the area of distribution of the contact force, the local pressures are reduced and wear is prevented.
Loss of meniscus causes high pressures to be experienced at the point of contact of the femur and tibia. This pressure, especially at the time when impact loading is occurring, can exceed the breakdown strength of the lining of the joint (hyaline cartilage). This causes breakdown (wear) of that lining which, in essence, is osteo-arthritis, and which, once begun, will become progressive with time.
Meniscus filling in the gaps between the bone ends
Meniscus removed leading to point loading within the joint

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
Valgus (knock kneed) knees, which have gone on to lateral compartment osteo-arthritis. As the lateral side wears out, the bones on that side get closer togerther and hence the valgus deformity gets worse. This increases the load on that side of the knee even further and increases the rate of wear.
The 2 lines crossing the centre of the knee are the line from the centre of the hip and the line to the centre of the ankle. These should be in line. The angle between them is the angle of deformity.
an underlying deformity, then this extra increase in pressure
may become very significant. The combination of a varus leg
(bowed) and a resected or non-functioning (torn) medial
meniscus will always lead to arthritis on the inside part of the
knee (medial compartment arthritis). The time scale for this
depends on the amount of remaining meniscal function, the
degree of bowing of the leg, and the activity of the person.
Loss of the outside meniscus, associated with a valgus (knock
kneed) leg, leads to progressive osteo-arthritis of the outside
of the knee (lateral compartment arthritis) and, in general, this
progresses more rapidly than its medial counterpart because
of the relatively more important role of the lateral meniscus
compared to the medial. It is to be noted in passing that,
the commonest cause of retirement from elite sport in the
world today, is a lateral meniscal tear that requires resection,
leading to premature osteo-arthritis.
In the above cases, the arthritis that develops in a mal-
aligned leg following meniscectomy (or meniscal failure), is
likely to progress to the extent that, it will be visible on plain
X-rays within 10 years from the time of the original surgery.
Depending on the above factors however, this can be as
quick as a few months.
Progression of disease occurs as the wear increases, because
the deformity increases. As the wear causes the lining on the
ends of the bone to become thinner, so the bones on that
side of the knee become closer together. This then causes an
increase in the deformity which, in turn, causes increased
force to be exerted on that side of the knee, and hence, an
increased rate of wear. Essentially therefore, the problem
spirals. The worse it gets, the more rapid the progression.
When this progression becomes apparent, if the other side of
the knee is normal, and the patient is young, the treatment of
choice may be to re-align the leg: to put the weight through
the other side of the knee, thus sparing the worn side (rotating
tyres if you will). This is called osteotomy (cutting the bone).
What are the symptoms of arthritis?
Initially there may be no symptoms at all. Eventually however,
pain and swelling do become a feature. Sometimes this just
occurs gradually with no particular starting event. Other
times however, an injury may activate the arthritis, such
that a damaged or worn out joint which previously gave
little or no trouble, may suddenly start to be painful and
give considerable trouble. Frequently, the accident or injury
that initiates this is relatively minor and causes very little
new damage to the joint itself. For some reason however,
an arthritic joint becomes intolerant of injury and can be
rendered symptomatic through even a small event.
As the arthritis becomes more and more progressive, the
joint tightens up and the range of motion frequently starts
to become restricted. Initially there may be just a slight
inability to straighten the knee. With time however motion
is lost at both ends of the range, with both an inability to
fully straighten (extend) the knee, and an inability to fully
bend (flex) the knee, becoming apparent. In addition to
this, uneven wear may occur as described above, causing
the knee to become progressively valgus (knock kneed) or
progressively varus (bow legged).
Frequent symptoms of arthritis, are pain and stiffness after rest.
First thing in the morning therefore, the knee may not want to
work too well, but it warms up with use. It is also helped by
local heat, such as when in the shower. In contradistinction,
it is worse in cold wet weather. As the arthritis progresses,
the periods of flare up get worse, and closer together, until
it starts to hurt all the time, frequently disrupting sleep. In
addition, function starts to deteriorate such that walking
distance gradually reduces, ultimately to 100m or less.
Why does arthritis hurt?
Nobody really understands exactly why arthritis hurts. There
are some nerves in the ends of the bone and, potentially, these
may hurt. If this is the main cause of the pain however, then
Centre of knee
To centre of hip
To centre of ankle
This line from the centre of the hip
to the centre of the ankle should pass through the centre of the knee. This is the centre of weight
bearing

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
of reactive swelling in the joint and, if taken with breakfast,
they may give more mileage on the joint during the day.
They decrease stiffness both after sitting, and first thing in
the morning. By the time of replacement therefore, the joint
may be a bit more worn out compared to someone not taking
medication, but the time to replacement is usually longer. The
fact that the joint may be a bit more worn out at the time of
replacement, is usually of little consequence in terms of the
eventual success of that procedure.
Standard anti-inflammatory agents seem to work best for most
people. These do have some potential for causing ulcers or
erosions in the stomach if used for extended periods, however,
if taken with food, and in soluble form (spreading the area
of absorption), this risk can be greatly reduced. Similarly
suppositories can be used at night when not eating and these
are very helpful in decreasing morning stiffness. Drugs such
as ibuprofen and diclofenac, which are freely available over
the counter, are just half strength anti-inflammatory tablets.
These drugs work well, particularly noting that diclofenac
will last twice as long as ibuprofen.
If necessary, a drug that reduces acid production in the
stomach, will also decrease the risk of ulcer formation. Some
of the older style ones such as ranitidine, are available over the
counter. More modern ones like nexium require a script. On
balance however, the newer ones are not much better than
the old ones, and they may actually have fewer side effects.
Cox-2 inhibitors are newer anti-inflammatory drugs which
were introduced with the hope that they would have less of
the gastric side effects than the conventional ones (NSAIDs
- Non-Steroidal Anti-Inflammatory Drugs). These do work
but they are not as reliably effective as the older style anti-
inflammatories mentioned above. In addition, they are not as
free from gastric side effects as was initially thought. In this
group are Celebrex (which contains a sulphur moiety and to
which some people will therefore react), and Mobic. Some
others in this group (e.g. Vioxx) have been withdrawn from
the market because of an increased risk of cardiac events.
It now turns out that this group all interfere with a cardiac
protective enzyme, and hence, are probably not suitable
for long term use.
Cortisone injection is a mainstay of treatment. Cortisone is
a strong anti-inflammatory agent and, by injection, it can be
delivered directly into the site of the problem. Although the
actual drug may only last 6 or 7 days, the anti-inflammatory
effect may be such that prolonged relief is provided for
months. Side effects are uncommon and generally transient.
Long term reviews also suggest that detrimental effects to
the joint are minimal, albeit that some types of cortisone are
perhaps better for the joint than others.
When an arthritic joint has been stirred up or aggravated,
it does not explain why so many arthritic joints do not hurt.
Another theory says that it is the lining of the joint, the capsule
(the synovium) that hurts. Every joint has a capsule, which is
a glad bag type of wrapping around it, and which keeps in
the joint fluid. This capsule is lined by a special layer called
the synovium which is very sensitive. In the normal joint this
layer is not irritated. If the articular lining cartilage starts to
fragment however, some of those fragments can float free in
the joint, and these can become extremely irritating to the
synovium. This irritation then causes pain and it also causes
those synovial cells to increase their fluid production and
hence to make the joint swell. Unfortunately however, simple
lavage of those particles does not often help the pain or the
swelling. Hence, this is not the sole explanation for the cause
of pain in these joints.
What is the treatment?
A good reference for this, is a summary of the world literature
that was made for the American Academy of Orthopaedic
Surgeons. It is listed below. Within this, there is also a further
link to more detailed information, if required.
http://www.drrmarx.com/pdf/JBJS-AAOS-clinical%20
Practice.pdf
Initially the treatment may be very simple and may include,
modification of activities to avoid impact loading type sports,
anti-inflammatory tablets or regular paracetamol, and weight
loss. In addition, physiotherapy and guided exercise regimes
may help. Being fitter makes the arthritis hurt less, so an
appropriate exercise regime, avoiding aggravating activities,
will help. The object of conservative care is to decrease the
rate of wear and to make the arthritic joint hurt less, covering
it up with medication if needs be. Nothing known can stop or
reverse the progression of the wear. Along those lines, there
is no evidence for glucosamine, chondroitin, fish oil, Krill oil,
etc., although some people claim some pain relief with these.
Weight loss is paramount among the treatments that are
available. Premature arthritis has been strongly associated
with obesity, and reduction to more normal weight (BMI)
is associated with a decrease in the rate of wear, a slowing
down of the wear process and a reduction in symptoms. It
should be strongly considered if BMI is high and, if unable
to be controlled by correction of diet and introduction of
exercise, then consideration of bariatric surgery should be
contemplated.
Anti-inflammatory agents are very useful. They are designed to
cover up the problem somewhat but, given that the problem
is in effect incurable, this may effectively delay definitive
treatment (such as replacement surgery) and considerably
improve lifestyle for some years. They decrease the amount

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
is more likely to aggravate than to help.
Although the results are not always as good as one would hope
for, the fact that the procedure is relatively minor makes it
attractive. Despite being minor to undergo however, recovery
can be prolonged, and it has to be remembered that a good
number of these joints will ultimately require replacement
to get the best long term result.
One last reason to consider arthroscopy is that it is a useful
procedure for determining what the rest of the joint is like. As
such, it may help when trying to determine if a re-alignment
procedure (osteotomy) would be worthwhile considering.
Not only can the good side of the joint be inspected, but
the patella and its tracking can also be visualised. This then
helps determine how the patella might be treated at the
time of osteotomy.
Chondroplasty is essentially an arthroscopic clean up of the
damaged areas, smoothing them out and removing loose
pieces of articular lining. In an acute injury, this can induce
a healing response but, this is limited and the joint does
not produce hyaline cartilage again. What is produced is
fibro-cartilage or scar tissue, the same as would be seen if
a piece of skin were to be lost or irreparably damaged (e.g.
burned). The resulting fibro-cartilage is not a low friction
bearing surface, and hence, does not tolerate motion over
a long period of time. Nevertheless, it is better than having a
pot hole or defect in the lining on the end of the bone, and
it may seal up the edges of the pot hole so as to decrease
the rate of expansion of that hole. In addition, if reasonable
filling of the pot hole can be achieved, then reasonable pain
relief may be obtained.
Micro fracture and burring are essentially techniques which
cause increased bleeding from a defect that is down to
bone. They are designed to encourage scar formation and,
by exposing the marrow of the bone itself, the theory is that
bone marrow cells (which are stem cells), will exude into
the defect and help in the healing process. Unfortunately,
whilst the theory is good, the reality is that you still just get
scar tissue in the defect and it does not heal. Micro fracture,
where a small spike is pushed across the end plate of the
bone repeatedly therefore, has turned out to be no better
than burring or roughening the end of the bone.
If a defect is large, recent in origin, and on just one surface,
the option of choice initially, is to make the bony base of the
defect bleed by one of the above techniques - to encourage
this scar formation. To maximise scar fill of the defect, it
is then best to have 6 - 8 weeks, non-weight bearing, on
crutches. The scar which forms, hopefully, will be thicker,
and will fill the defect better, thereby improving the overall
result, leading to prolonged improvement in joint function.
an injection may return it to its previous quiescent state. If it
does not, then other treatments may be indicated but, all of
these other treatments may have consequences greater than
any perceived problems caused by cortisone.
Synvisc and related products were introduced in Canada
more than a decade ago. This group of compounds contain
normal joint fluids with their proteoglycan molecules. The
idea is to replace the damaged proteoglycans in an arthritic
joint with more normal ones. These substances only lasts a
few weeks before being fully degraded, but long term relief is
occasionally noted. The problems with this range of products
are many. They are very expensive ($500 per injection per
joint, for which there is no rebate available), they are animal
products and hence, very occasionally, the joint may react
to them, and they do not actually change the amount of
wear in the joint. On the plus side however, they do not
burn any bridges and, if they fail, the joint can still be treated
successfully. In addition, if they help, they can be repeated.
Therapy etc. There is no doubt that exercise and being
generally fit makes the arthritis feel better. Note however
that it does not make the actual arthritis (wear) better, and
indeed, using the joint a lot will actually increase the wear
rate, particularly if the exercise is impact loading (such as
jogging). The rate of wear depends on use, and can best be
slowed down by modifying that use.
Often people describe building the muscles up around the
joint as a treatment. Unfortunately, whilst it sounds good,
it is myth. It helps to be fit, but it does not have to be the
knee that does all the exercise. Think of it as putting a bigger
engine into a car with worn out tyres. It sounds better, it may
even go better, but the tyres are still worn: and, if you drive
the car harder, the tyres will wear quicker.
Arthroscopy may be considered if there are mechanical
problems or if there are symptomatic meniscal tears present.
Simply cleaning up an arthritic joint, like cleaning up a pot
hole on the road, does not fix the problem. There is now quite
good literature evidence to suggest this, and therefore, unless
there is something in the joint that can be fixed, arthroscopy
is not recommended.
Where there is a meniscal tear, the chance of improvement
by arthroscopy is better but, of course, it is not a cure for
the arthritis. For most people however, when the joint first
gets bad, it is usually the degenerating meniscus that hurts
rather than the arthritis. Unfortunately, the only way to
find this out, is to deal with the meniscal tear and see if it
helps. If this is done, figures would suggest that about 70%
will show some improvement, 20% will be unchanged or
minimally improved, and 10% somewhat worse. As the
arthritis becomes more advanced of course, these figures will
deteriorate, ultimately reaching the stage where arthroscopy

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
Lower Femoral Osteotomy
For lateral
compartment osteo-arthritis in a valgus left
knee
High Tibial Osteotomy
For medial compartment osteo-arthritis in a varus left
knee.
These techniques work best when used in acute injuries to
the articular surface, and in the young. They do not work
well for established arthritis, where the area of wear is large,
or where both sides of the joint are involved. They also do
not work well where there is a significant mal-alignment. In
these settings, other treatments are better.
Osteotomy is a time honoured, well proven, procedure, in
which the limb alignment is changed to unload the bad side
of the joint, and to load up the good side. In order for it to
work, the good side has to be fairly much normal. If it is not,
then transferring weight to that side will merely transfer the
problem to that side.
In the young, where replacement is not a viable option, and
where there is an alignment problem, osteotomy remains
the procedure of choice. A varus (bow legged) knee with
arthritis on the medial side (inside) is made valgus (knock
kneed), and vice versa. In order to do this, one of the leg
bones will need to be cut and the angle changed. It turns
out that, in varus knees, the deformity is usually in the tibia,
so this is the bone in which the correction will take place. In
a valgus knee, the deformity is usually in the femur and not
the tibia. The usual reason given for this, is that, in a valgus
knee, the lateral femoral condyle is small (underdeveloped -
hypoplastic). In this deformity therefore, the correction must
be in the femur. In either instance, it is important to correct
the deformity in the appropriate bone, so that the joint line
stays horizontal. If the joint becomes sloped, then it can be
subject to shearing forces, which may, in turn, contribute
to further wear.
It is to be noted that, in order to change the forces at the
joint level, the correction has to be in the bone. It cannot
be achieved by the use of orthotics or similar devices: these
merely rotate the bone and do not actually adjust the varus/
valgus angle. Unloading braces do similar, but these are bulky,
uncomfortable and not suitable for long term use. Hence,
these are regarded as devices designed to test, whether or
not, an unloading procedure will help. They are not a therapy
in their own right.
Osteotomy is not a last resort procedure, even though it
is a moderate sized procedure to do. Essentially, if there is
wear and an associated deformity, it should be done sooner
rather than later. For most people this means within the next
6 - 12 months, but it does depend on the extend of the wear,
the symptoms and so on. It also depends on age. If you are
approaching 60 and the knee is not too symptomatic, the
best option may be to do nothing and wait until the pain is
bad enough to go straight to knee replacement. If you are
in your twenties, then this maybe the only way of delaying
replacement for a significant length of time.
The results of osteotomy are good. Indeed, the likelihood of
delaying replacement 5 years is 85%, and the likelihood of
delaying replacement 10 years is 75% (though even better
in some series). Having got to 10 years, many will indeed get
15 - 20 years out of this procedure. The reason this happens
is that, by unloading the bad side of the knee, the pain either
completely, or mostly, disappears. For those in whom this
does not happen, early replacement remains an option but,
as judged by the above figures, this is a small number overall.
In order to achieve this level of result, the leg needs to be
some 3 - 5 degrees over corrected, placing the majority of
the weight on the good side of the joint, and significantly
unloading the worn side. Nowadays, this correction can be
done with the aid of 'in theatre' computer navigation, which
helps get the alignment corrected more accurately than was
previously possible.
The advantage of an osteotomy is that it remains your knee.
This means that, it still bends as far as it used to, and it does
not have the restrictions of a replaced knee. In addition,
whilst running is not advocated (even if there is no residual
pain), activity can certainly be moderately vigorous. Again
therefore, this is the procedure of choice in the younger
patient; always remembering that a good osteotomy is like
Arrows indicate the size of the inserted
wedge.
Arthritic side
Arthritic side

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
having a normal knee, whereas a good knee replacement
never is. It is always to be remembered therefore, that, a
poor result from an osteotomy can be dealt with by knee
replacement but, a poor result from a replacement, may be
un-fixable.
The concept of osteotomy is reasonably simple in that, the
bone in question, has to be cut across, then opened as a
wedge until the desired correction is achieved. The bone
is then fixed with a strong plate, and the wedge shaped
defect, thus created, is filled to encourage healing. Various
fillings are possible, including bone graft from one's own hip.
Whilst the latter encourages more rapid healing, and is the
graft of choice in those over 55, where union may be slow,
there are now many bone substitutes, some of which have
growth factors in them to help healing. Accordingly, because
of the problems associated with bone harvest from the hip,
this method is only used when clearly indicated. For the
majority, the newer bone substitutes, with growth factors in
them, seem to work very well: hence, these are considered
the standard for this procedure at present.
Recovery from osteotomy is similar to recovery from a
broken leg (which is essentially the same thing). The bone
will take about 6 weeks to begin healing, and it will hopefully
go on to full union over the next several months. As the plate
is strong however, immediate weight bearing is possible.
This does not mean that one should walk directly on this,
but standing is certainly possible. Mostly, crutches are used
for a few weeks so as not to overload the leg. By about six
weeks however, they can generally be totally discarded. As
the bone becomes better united, it will feel better, and more
normal activity will be possible. Most people know when it
definitively joins.
Overall, it may take 9 - 12 months to gain maximum benefit
from this procedure, bearing in mind that the worn area of
the knee remains worn. This part however is unloaded so,
given time, it gradually loses pain and feels more normal. If
the recovery of the joint is thought to be slower than expected
however, and particularly if it is still swollen, it can be injected
with cortisone. This can be done at any time in the recovery
period because the cortisone goes into the joint and not into
the bone: hence it does not interfere with healing.
In the first 3 months, anti-inflammatories (including nurofen
etc.) should not to be taken. This is because they slow down
or prevent bone healing, which subsequently may be difficult
to treat. Similarly, smoking should be ceased, as this is a major
cause of bone non-union.
Knee replacement is the treatment of choice if the arthritis
is advanced, if it involves all of the knee (so that there are
no good bits left to transfer the load to), if there is a marked
tightening of the joint with loss of full extension, or if the
patient is over 60 years of age, where union of the bone
can be an issue. Similarly, when osteotomy eventually fails,
or if it does not give the desired pain relief early on, knee
replacement can be performed.
Stem Cell therapy
The hope of the modern world is that we will be able to
reverse and cure osteo-arthritis by using either stem cell
therapy or genetic engineering. If we could just re-grow a
knee like the lizard re-grows it's tail, we would not have to
do replacement surgery any more.
This is certainly the dream but, as yet, that is still what it is.
Whilst an enormous amount of research is being done in this
area, to date, there has been little, if any, documented long
term success for these therapies. This may be because, just
being able to grow these cells, is not enough. Targeting them
to the right areas and getting them to form normal looking
hyaline cartilage (with its very special matrix of collagen
arcades), still eludes us: and, after all, it is the extracellular
matrix that is the mainstay of this tissue. The cells are few
in number, deep in the tissue, and non-structural. They are
merely the maintainers of that matrix.
Knee Replacementfor end stage osteo-arthritis

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2017
Chondral grafting has been our biggest foray into stem cell
type therapies. It involved sending some normal articular
(hyaline) cartilage to the laboratory, growing this by forcing
the cells to divide, and then re-implanting those cells some
5 - 6 weeks later. The cells are taken from normal parts of
the joint that are not used too much (so that minimal harm
is done). The harvest is done via the arthroscope as a day
case procedure, and the cells are sent away to the laboratory
for culture.
The cells are grown with the aid of tissue growth factors and
other advanced tissue engineering techniques. When ready,
they are placed onto a membrane and implanted directly
into the defect. The membrane is glued in with an absorbable
glue, and the cells transfer across from the membrane to
the bone end, where they grow. The joint then needs to be
protected for some weeks until the area is stable enough to
allow weight bearing. The cells continue to grow over 1 - 2
years, usually filling, or partly filling, the defect.
For some years we did this procedure and, in the short term,
some people did seem to do well. Unfortunately, over 5 years,
the results were less good, and many of these cases ended
up coming to knee replacement. Given the time it took to
go through this and to fully recover, these results did not
really justify continuing use of this technology. Similarly, the
figures were such that ,the government has now withdrawn
all medicare rebates for such procedures.
Whilst there may still be a place for this type of procedure
therefore, it is likely that it will need better technology.
Unfortunately, with current technology, the cells often
degenerate to fibro-cartilage (scar) rather than staying as
hyaline cartilage, a result that could have been obtained by
making the bony defect bleed and then not weight bearing
on it for 6 - 8 weeks. Also, these cells do not form the normal
matrix which constitutes the majority of the lining tissue,
and hence, the new tissue does not survive the stresses of
everyday use. To achieve the latter will need better tissue
engineering techniques or better technologies altogether.
Injectable stem cells are the big thing on the internet at the
moment. They come with hope and hype, and some miracles
are touted. Unfortunately, there is no evidence for any of this
at the present time. Because it is simple to do, comes without
major surgery, and the procedure contains the buzz words
'stem cell', it seems very enticing. It would be fabulous if it
worked but, currently, it is looking like 21st century snake oil.
Because of all of the above factors however, it has enormous
placebo effect, so sorting out the real results from placebo
ones will take time.
The evidence so far is that, for a stem cell to work, it has
to be an appropriate cell: and we know for instance, that
bone marrow is a better source than fat or muscle tissue. We
also know that the cells have to be targeted. They cannot
just be injected into a joint, be expected to find the defect
and then start to fill it. Similarly, they cannot be expected
to convert damaged hyaline cartilage cells into cells which
will then start dividing, make new matrix and heal a defect.
All this needs to happen in a controlled fashion and, even if
that is occurring, we may still have to deal with alignment
issues, meniscal deficiency and so forth. It is very complex
and we are not there yet. The next coupe of decades could
be interesting however.
Questions and concernsPlease contact Dr Holt’s office
Phone: +61 8 92124200Fax: +61 8 94815724Email: [email protected]
Further information can also be obtained on this and other related topics, such as:OsteotomyKnee replacementRehab after knee replacement
at: www.keithholt.com.au
Links of Interest:to the AAOS (American Academy of Orthopaedic Surgeons) guidelines on arthritis treatment
http://www.drrmarx.com/pdf/JBJS-AAOS-clinical%20Practice.pdf
http://www.aaos.org/research/guidelines/OAKSummaryofRecommendations.pdf
Related Documents