Advancing community health across the continuum of care: A health systems perspective Sara Bennett PhD Presentation to Core Group, Global Health Practitioner Conference - 14 April 2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Advancing community health across the continuum of care: A health systems
perspective
Sara Bennett PhD Presentation to Core Group, Global Health Practitioner
Conference - 14 April 2015

2
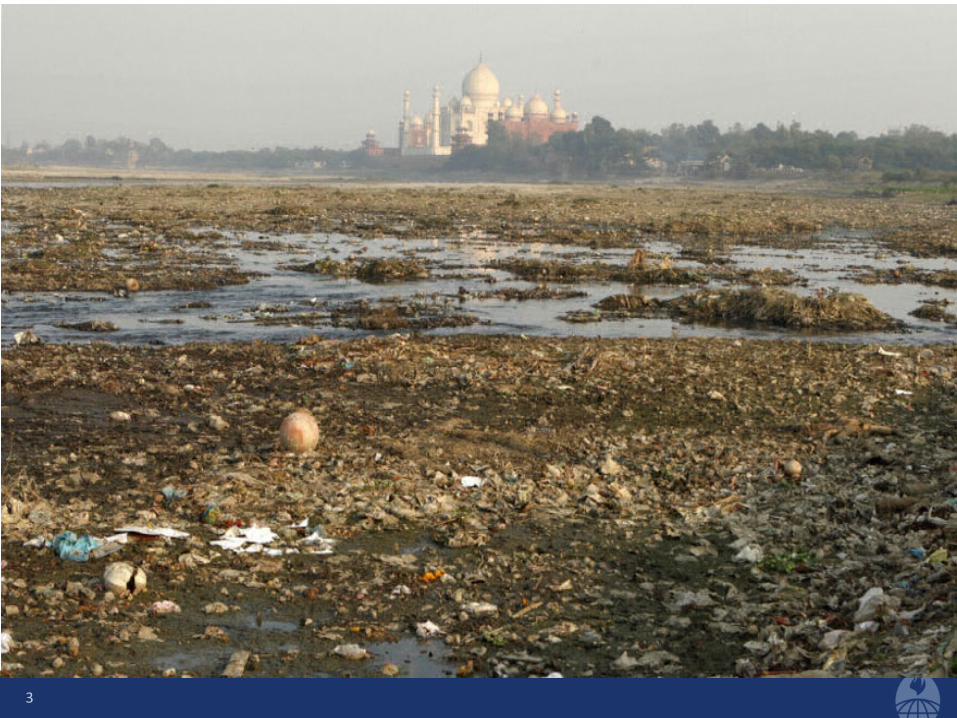
3
Top-down approaches to health systems?
4

5
Where is the community?
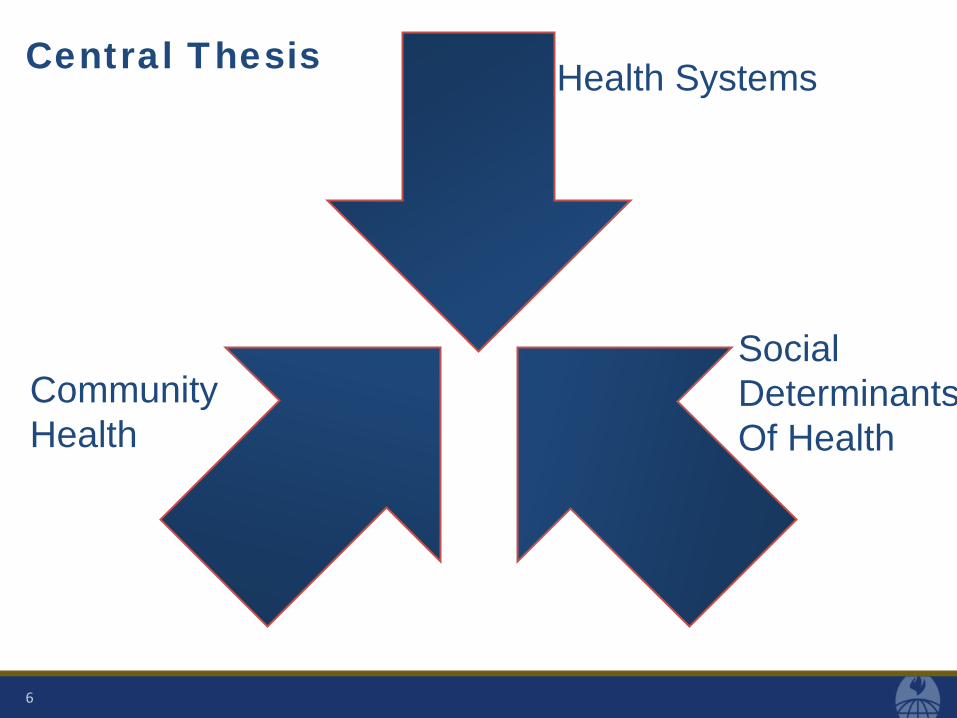
Central Thesis
6
Health Systems
Community Health
Social Determinants Of Health

Objectives
1. Describe the global trends that are inspiring integration – People-centered & integrated services delivered across a continuum
of care
2. Identify key, broad strategies to support more people-centered and continuous health services
3. Provide some concrete examples of how we need to approach things differently
7
Person centered
• An approach to care that consciously adopts individuals’, families’, and communities’ perspectives as participants in and beneficiaries of trusted health systems. This perspective can be characterized around dimensions such as respect for patients’ values, preferences and expressed needs in regard to co-ordination and integration of care, information, communication and education, physical comfort, emotional support and alleviation of fear and anxiety, involvement of family and friends, transition and continuity
8
Integrated care
• "The management and delivery of health services such that people receive a continuum of health promotion, disease prevention, diagnosis, treatment, disease-management, rehabilitation and palliative care services, through the different levels and sites of care within the health system, and according to their needs throughout the life course.”
PAHO
9

CHALLENGES DRIVING PERSON-CENTERED, AND INTEGRATED SERVICES ACROSS THE CONTINUUM OF CARE
10

11
Intersectoral challenges
Medicalization & De-personalization
Accountabilty
Challenges driving person-centered and integrated services

1. Intersectoralism
12
Increasingly the really sticky
challenges in global health are
intersectoral
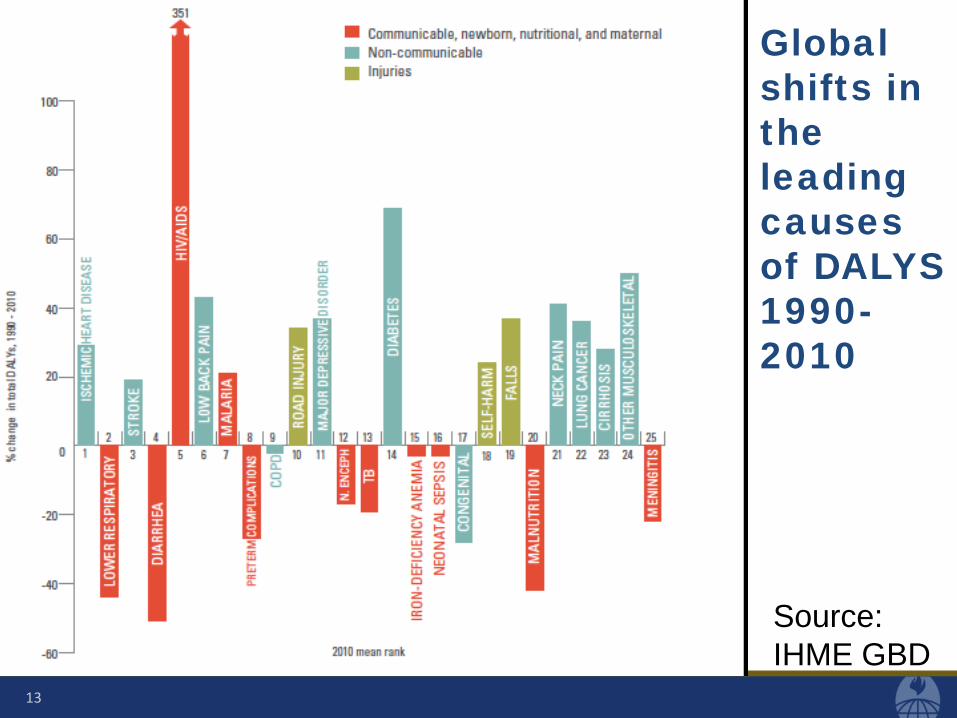
Global shifts in the leading causes of DALYS 1990- 2010
13
Source: IHME GBD
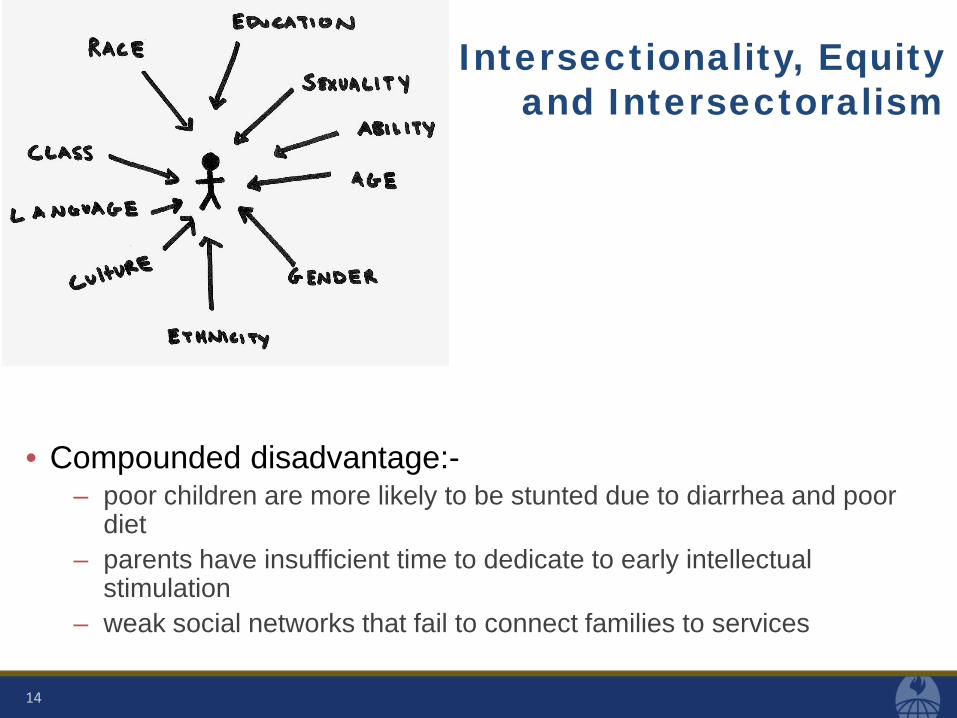
Intersectionality, Equity and Intersectoralism
• Compounded disadvantage:- – poor children are more likely to be stunted due to diarrhea and poor
diet – parents have insufficient time to dedicate to early intellectual
stimulation – weak social networks that fail to connect families to services
14
What are the implications of intersectorality? • Shift from atomized individuals to social networks,
communities & community assets • Increasing focus on local capacities
– Central government can set rules but cannot build the relationships, capacities & commitment for implementation
– Need local level partnerships – across sectors and across public/private actors
• Shift from biomedical models of health systems: simply treating illness approaches that recognize complex & interrelated needs:-
– health, housing, safety, education etc
15

2. Medicalization & De-personalization
• Increasing reflection on the over-medicalization of services
16
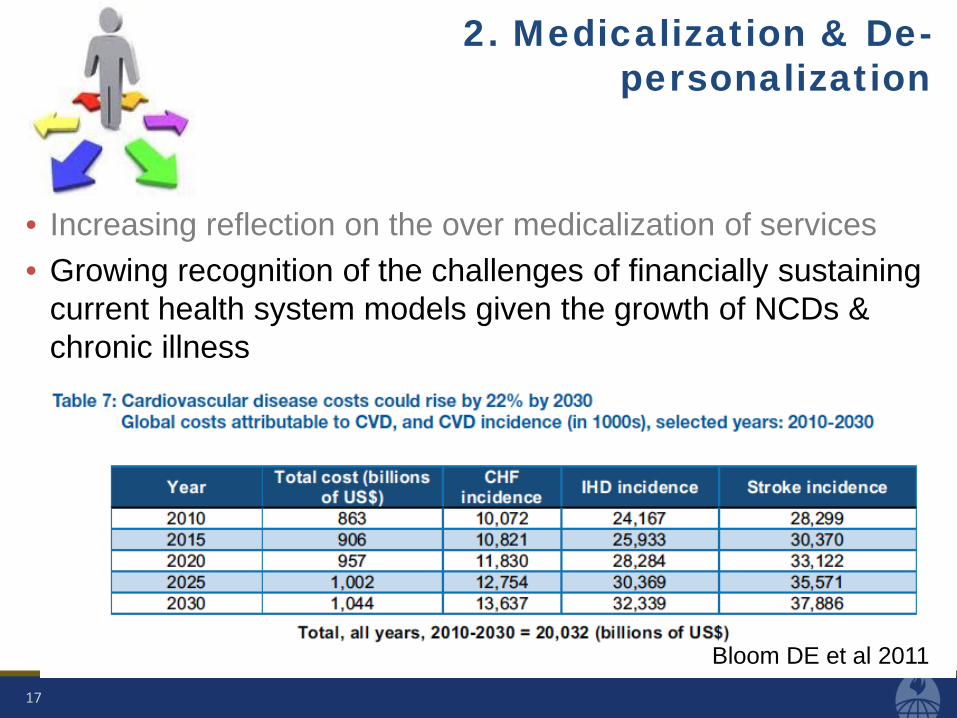
2. Medicalization & De-personalization
• Increasing reflection on the over medicalization of services • Growing recognition of the challenges of financially sustaining
current health system models given the growth of NCDs & chronic illness
17
Bloom DE et al 2011

2. Medicalization & De-personalization
• Increasing reflection on the over medicalization of services • Growing recognition of the challenges of financially sustaining
current health system models given the growth of NCDs • Health systems frequently fail to treat patients with due
respect and courtesy – often with negative implications for health
18

Maternal Disrespect in Tanzania
19
Neglect “When the community goes to the center, to go and deliver there, they may find that there is no nurse. The family can go to the nurse’ s home and say, “ We have brought a laboring woman” but the nurse will delay. She stays in her home until it reaches a very late stage and by the time the nurse comes, that woman has delivered by herself.” CHW
Abuse “They give you a bad face. They take a look at you and when your clothes are like this and this they chase you away.” Woman
McMahon et al 2014
3. Accountability
20

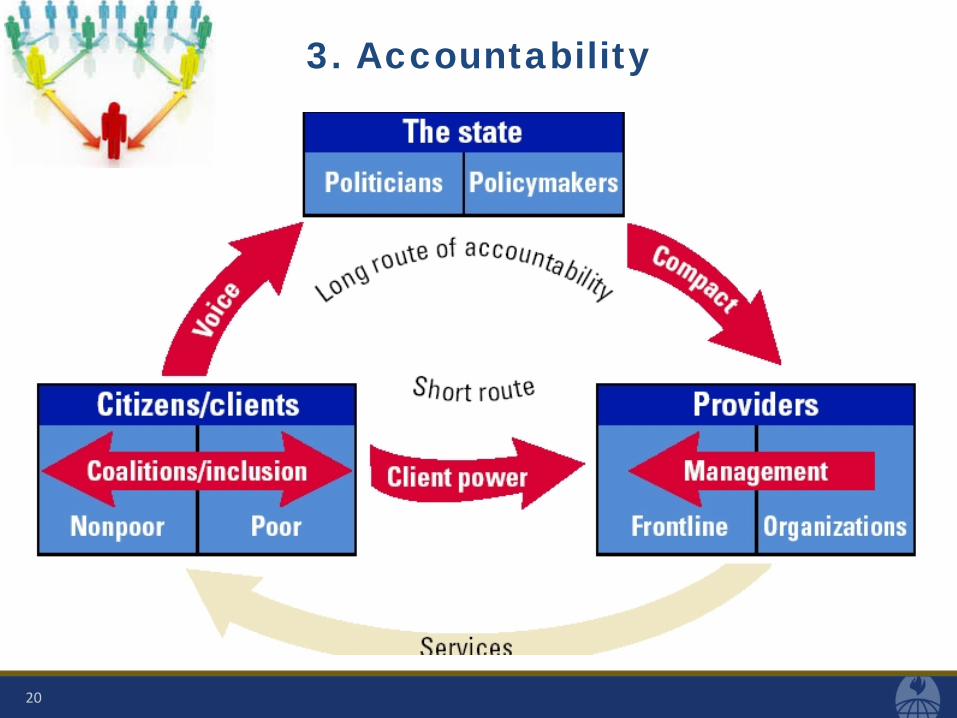
3. Accountability
• RCT interventions to promote provider accountability can have
significant positive effects on health outcomes – Eg. 35% reduction in child mortality
• Real world studies of processes to promote voice and accountability (eg. Village health committees) more mixed
• Challenges – Community structures may not be inclusive – Community accountability mechanisms may not function in a
sustainable and institutionalized fashion
21
• Sou

HOW TO MAKE HEALTH SERVICES MORE PERSON-CENTERED & INTEGRATED?
22

Moving the policy and practice agenda forward
23
Innovate Learn by Doing Manage politics

Innovation needed!
• Menu of options for developing person-centered and integrated services
– M-health/e-health - disruptive technologies that change the way health system actors relate and empower people
– Social accountability – Citizen voice & action eg. Community scorecards (CARE), verbal autopsies (WRA), community defined quality (SCF) (Hoffman 2014)
– Unlocking community capabilities – expert patients; women’s group that strengthen social networks to facilitate access to health
• Evidence about the effectiveness of these strategies is not always strong
• Strategies will work differently in different contexts 24

Learning by doing
• Need to learn from the experimentation and innovation • Pursue learning action cycles
• Engage communities in these processes in a participatory way: mapping, ranking, photovoice (Loewenson et al 2014)
25

Managing politics
• Community-oriented, people-centered services imply a paradigm shift:
– redistributing power from the medical establishment to communities and frontline health workers
• Strategies to manage resistance – develop strong leaders at the community level and beyond – create alliances between like-minded groups – reorient health workers, empowering them to work better with
communities and other sectors
26

BRINGING IT TOGETHER…SOME
EXAMPLES 1. EARLY CHILDHOOD
DEVELOPMENT 2. LEARNING FROM EBOLA
3. COMMUNITY CASE MANAGEMENT
27

Early Childhood Development
28
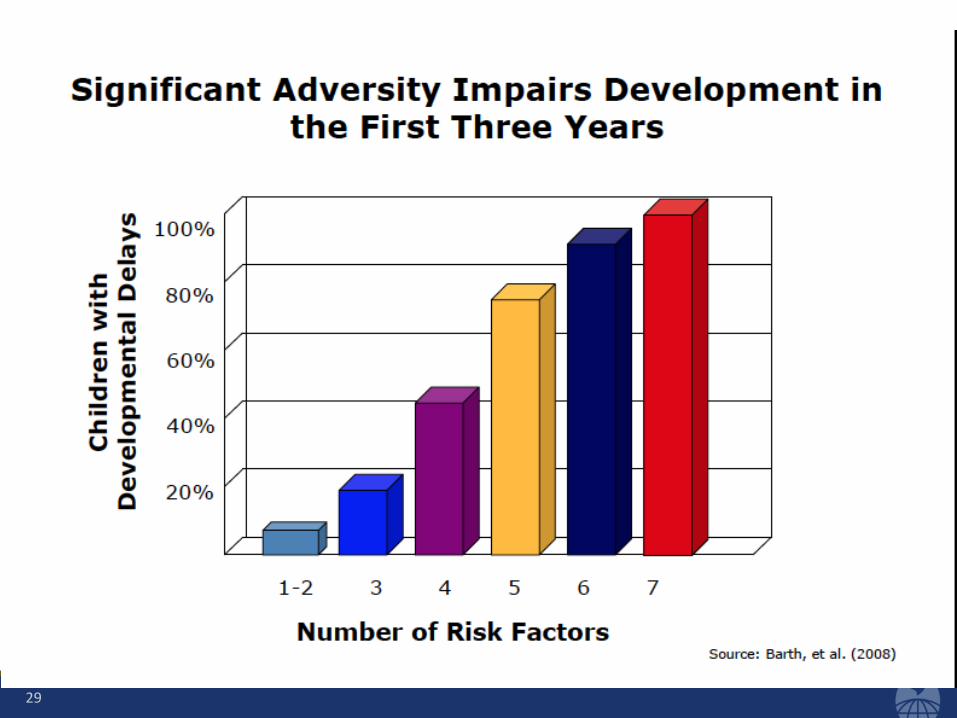
• Increasing awareness of the malleability of young children’s neurological and biological development and how it is affected by the environment • Early childhood disadvantages tend to compound each other
29

Early Childhood Development
30
• Increasing awareness of the malleabiity of young children’s neurological and biological development and how it is affected by the environment • Early childhood disadvantages tend to compound each other • Equity key to the ECD agenda • Innovative programs emerging to promote early childhood
development • These tend to be multifaceted
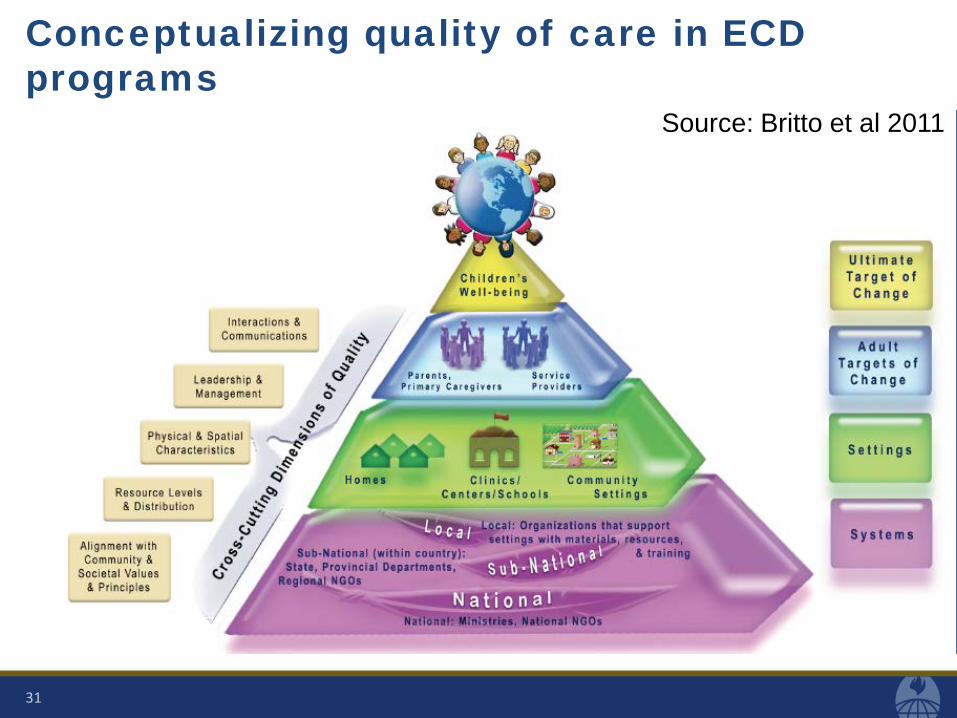
Conceptualizing quality of care in ECD programs
31
Source: Britto et al 2011
LEARNING FROM AND PREPARING FOR EBOLA
32

Liberia R_t and Ebola Treatment Unit Timeline
33
First isolation unit (March)
Quarantine in 4 counties and West Point (Aug 11)
Foya treatment center opens (23 beds)
Elwa treatment center opens (6 beds)
Elwa expands to 40 beds
Elwa expands to 125 beds, Foya to 80 beds
US announces plans for 17 ETUs & 1700 beds
Island clinic opens 120 beds, fills with 200 patients
772 beds at 9 ETUs
DART airlifts 135 tons of medical supplies
2 ETUs, 3 CCCs open 1st US, Swedish funded sites, Cuban doctors arrive UNMEER starts

What turned around the epidemic in Liberia? Probably NOT:
• ETUs and hospital beds – Few available early when most needed, most beds built in November-
December after the R_t <1 and were not used
• Better hospital treatment – most cases never made it to hospital
• UNMEER – R_t was already <1, and curve reversed in mid-August when Liberian
Incident Management System (IMS) was re-organized
• Forced population quarantine (August) – heightened distrust and resistance, sparked a riot – BUT also prompted government to change tactics to increase
community engagement and communications strategies
34
Source: D.H. Peters, personal communication

What turned around the epidemic in Liberia?
• Engaged communities – own & participate rather than deny & resist
• Behavior change -- Which behaviors mattered most? – Isolating sick cases at home and at clinics – General hygiene (hand washing and no touching) – Safer care for ill at home (and hygiene after they leave home) – Identifying cases and deaths (community dependent)
• Safe burial – Burial teams & safe funerals
• Strong national and local leadership – >90% of workforce was local
35
Source: D.H. Peters, personal communication

STRENGTHENING INTEGRATED COMMUNITY CASE MANAGEMENT
36
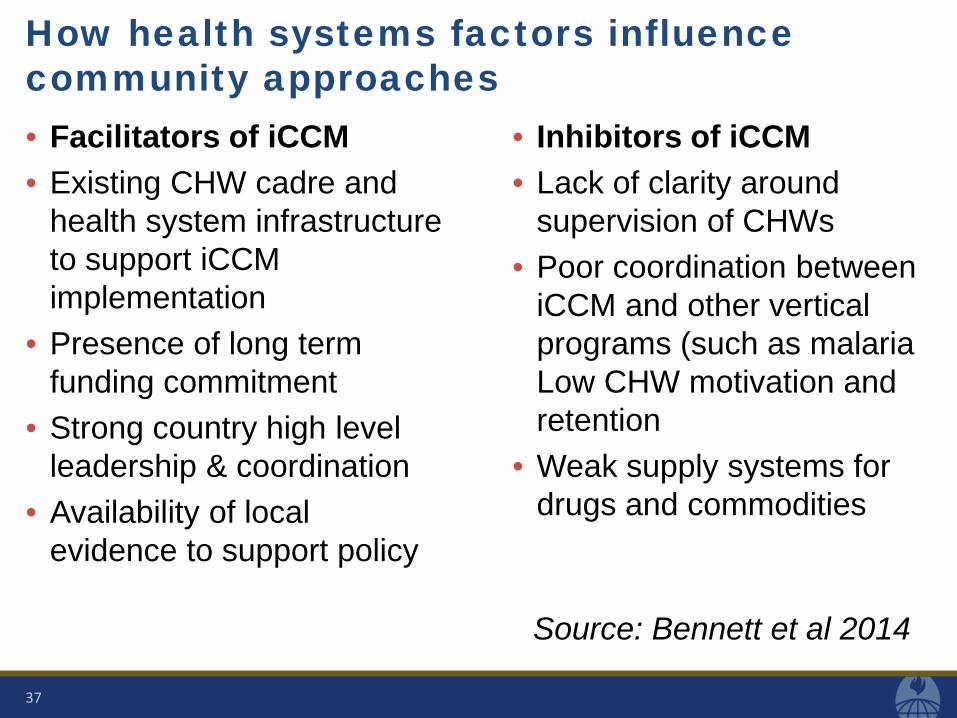
How health systems factors influence community approaches • Facilitators of iCCM • Existing CHW cadre and
health system infrastructure to support iCCM implementation
• Presence of long term funding commitment
• Strong country high level leadership & coordination
• Availability of local evidence to support policy
• Inhibitors of iCCM • Lack of clarity around
supervision of CHWs • Poor coordination between
iCCM and other vertical programs (such as malaria Low CHW motivation and retention
• Weak supply systems for drugs and commodities
37
Source: Bennett et al 2014

CONCLUSIONS
38
Conclusions
Engender trust &
social capital
Challenge inequity
Be resilient & adaptive
Respond to root causes
of illness
Coordinate across sectors
39
Health systems in the future will need to:-
Related Documents











