KERATOPLASTY UPDATE 2016 PK, DALK, DSEK,DMEK,PDEK INDOREDRISHTI.WORDPRESS.COM

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

KERATOPLASTYUPDATE 2016
PK, DALK, DSEK,DMEK,PDEK
INDOREDRISHTI.WORDPRESS.COM

DR DINESH MITTAL DR SONALEE MITTAL
DRISHTI EYE HOSP VIJAYNAGAR INDORE

From the first documented successful corneal transplant performed by Eduard Konrad Zirm in 1906 to contemporary femtosecond laser assisted surgery, theevolution of keratoplasty has been nothing short of remarkable

THE CORNEA•The cornea is the refractive surface of the eye and, with the sclera, forms the outermost coating of the eyeball. It constitutes up to one-sixth of the entire eyeball. The corneal epithelium is
derived from surface ectoderm, and the mesoderm gives rise to Bowman’s layer, the stroma, Descemet’s membrane, and the endothelium.

THE CORNEA•The average diameter of the cornea varies from 11 to 12 mm horizontally and 9 to 11 mm vertically. The cornea is responsible for 48 diopters of the total power. The posterior surface of the cornea is more spherical than the anterior surface, and the central cornea is thinner (520 μm compared with the peripheral cornea 650 μm or more).

Precorneal Tear Film•The tear film is 7 μm thick and has a volume of 6.5 ± 0.3 μL. The tear film is made up of an outer lipid layer (0.1 μm), middle aqueous layer (7 μm), and innermost mucin layer (0.02 to 0.05 μm).The tear film keeps the corneal surface moist and prevents the adherence of microbes. More than 98% of the volume of tears is water. The tear film has many essential substances, such as electrolytes, glucose, immunoglobulins, lactoferrin, lysozyme, albumin, and oxygen.

Anatomy of the Cornea•The cornea has 5 layers: •THE EPITHELIUM,•BOWMAN’S LAYER, •THE STROMA, •DESCEMET’S MEMBRANE,• ENDOTHELIUM

Normal corneal layers

Epithelium•The corneal epithelium has a thickness of 50 to 90 μm and comprises 5 to 7 layers of stratified,squamous, and nonkeratinized cells . The epithelium forms approximately 10% of the total corneal thickness. cells of corneal epithelium may be divided into 3 types: •squamous cells • middle wing cells •and deeper basal cells .

Epithelium•Superficial Layer of Squamous Cells•The superficial layer, which consists of squamous cells, forms the outermost 1 to 2 layers of the corneal epithelium. The oldest epithelial cells disintegrate and shed into the tear film by process of desquamation. These superficial cells are composed of microscopic projections in the form of microvilli, reticulations, or microplicae .

Epithelium. •The fibrillar glycocalyx is present on these ramifications, which interacts with the mucinous tear film. •The epithelial cells are replaced every 7 to 14 days. superficial cells adhere to each other by presence of desmosomes and junctional complexes. These complexes consist of tight junctions that circumvent entire cell & resist flow of fluid through epithelial surface.

Epithelium• . The epithelial cells are replaced every 7 to 14 days. The superficial cells adhere to each other by the presence of desmosomes and junctional complexes. •Middle Layer of Wing Cells•The middle layer of the corneal epithelium consists of wing cells, which have lateral, thin, wing-like projections protruding from a more rounded cell body.
The wing cells are connected to each other by desmosomal junctions and gap junctions.

Epithelium
•Deep Layer of Basal Cells•The deep layer of the corneal epithelium consists of basal cells, which are cuboidal to columnar in shape and have a diameter of 8 to 10 μm. Posteriorly, the cells are flat and have a basal lamina to which they anchor with the help of hemidesmosomes. The basal cells are metabolically active
and are responsible for division, and they form the wing and the superficial cells.

Epithelium
•The corneal epithelium acts as a tough protective shield against microorganisms and foreign bodies;
•however, it is partially permeable to small molecules such as glucose, sodium oxygen, and carbon dioxide

Basement Membrane•The basal cells of corneal epithelium are anchored with help of hemidesmosomes to
basement membrane, which is located between corneal epithelium and Bowman’s membrane. It is primarily made up of type IV and VII collagen and glycoproteins and has 2 parts: the superficial lamina lucida layer and the deeper lamina densa layer

Bowman’s Layer•Bowman’s layer is acellular membrane-like zone with a thickness of 8 to 14 μm. It has numerous pores for the passage of corneal nerves into corneal epithelium. •On examination with electron microscopy, it is made up of a fine meshwork of uniform type I and III
collagen fibrils

Corneal Stroma•The corneal stroma, with a thickness of approximately 500 μm, is responsible for 90% of the thickness of the cornea. It is located between Bowman’s layer and Descemet’s membrane . It is composed of lamellae, which are formed from flattened bundles of collagen, stromal keratocytes, and ground substances like keratan sulphate. The major structural component of the corneal stroma is collagen

Corneal Stroma•There are 200 to 250 bundles of collagen fibrils, and each bundle has a fibril 2 μm thick and 9 to 260 μm wide. The collagen fibers are arranged in a regular manner, parallel to the corneal surface. Such a uniform arrangement and equal spacing of collagen fibers creates a lattice or 3-dimensional diffraction grating, which is responsible for the ability of the cornea to scatter 98% of incoming light rays.

Corneal Stroma• lamellae in posterior part of stroma have an orthogonal layering ( the bundles are at right angles to each other). In anterior one-third of the stroma, the lamellae have a more oblique layering. arrangement of ant. and post. lamellar stromal fibers is different. fibers are more compact anteriorly so that their compactness and their oblique arrangement make lamellar dissection more difficult anteriorly. On the other hand, the arrangement of the fibers is less oblique and loose posteriorly .

Corneal Stroma•On other hand, arrangement of fibers is less oblique and loose posteriorly so that manual dissection is simpler in the posterior part.•The primary glycosaminoglycans of the stroma are keratin sulfate and chondroitin sulfate, which occur at a ratio of 3:1. The lamellar stroma is secreted and maintained by stromal fibroblasts called keratocytes, which occupy 3% to 5% of the stromal volume. They are responsible for the maintenance of stromal components .

Descemet’s Membrane•Descemet’s membrane is basement membrane of corneal endothelium and is synthesized by endothelium. At birth, the human Descemet’s membrane is 3 μm wide, but in adulthood,• the width increases to 12 μm . There are 2 distinct regions in Descemet’s membrane:• the anterior one-half to one-third, which is banded; and posterior two-thirds, which are nonbanded. Recently, another layer of the cornea, called Dua’s layer, has been described.

Descemet’s Membrane•Recently, another layer of the cornea, called Dua’s layer, has been described. This is a novel, well-defined, acellular, strong layer in pre-Descemet’s cornea. It separates along
the last row of keratocytes in most cases with big bubble technique . Its recognition will have a considerable impact on posterior corneal surgery and understanding of corneal biomechanics and posterior corneal pathology, such as acute hydrops, descemetocele, and•pre-Descemet’s dystrophies .

Endothelium• endothelium is a single-layered, low cuboidal endothelium. It has 400,000 cells and a thickness of 4 to 6 μm. endothelial cells have a hexagonal shape and are 20 μm wide. They prevent seepage of the aqueous humor into the stroma..The number of endothelial cells decreases with age at the rate of 0.3% to 0.6% per year.

Endothelium•Unlike the corneal epithelium, endothelial cells cannot undergo mitosis after birth. At birth, cell densities range from 3500 to 4000 cells/mm2, whereas an adult’s cell densities range from 1400 to 2500 cells/mm2. As cells decrease in number, they become thinner and attenuated. The cornea loses it clarity when the endothelial cell densities reach 400 to 700 cells/mm2, below which corneal edema occurs .

Endothelium•The endothelial cells are linked to each other by junctional complexes and gap junctions, but no desmosomes are present. The endothelial cells do not replicate in human beings. They decrease in density with increasing age, raised IOP , & inflammation & after intraocular surgery. The endothelium plays a major role in maintaining stromal hydration (normally 78%) through the sodium potassium–activated adenosine triphosphotase (ATPase) present in basolateral borders of cells.

Endothelium•Endothelial cell loss varies from 2% to 7% after anterior lamellar keratoplasty and from 20% to 30% after posterior lamellar keratoplasty depending on the surgeon’s skill. In cases of Descemet’s membrane endothelial keratoplasty (DMEK), endothelial cell loss is higher due to difficulty in performing this technique. However, in hands of an experienced Surgeon , endothelial cell loss after Descemet’s stripping endothelial keratoplasty and DMEK may be similar.

PKP
DALK
ALK
DSEK
DMEK

Penetrating Keratoplasty• PKP is the most common & successful human transplantation procedure. •Over 30 000 corneal transplantations are performed in the United States each year. •Optical results have improved greatly as a consequence of advances in tissue selection and preservation, trephines, & management of postoperative astigmatism .

Preoperative evaluation and diagnostic approach•PKP may be used to provide tectonic support (such as in corneal thinning and perforation), & to improve visual outcome (such as in the replacement of a scarred cornea). Indications for PK include: keratoconus, previous graft failure or rejection, full-thickness or deep corneal scars, Fuchs’ endothelial dystrophy, pseudophakic or
aphakic bullous keratopathy, chemical burns, corneal ulcers, corneal dystrophies .

Preoperative evaluation and diagnostic approach•Conditions with primarily posterior pathology, such as Fuchs’ endothelial dystrophy and pseudophakic or aphakic bullous keratopathy, are now commonly treated with endothelial
keratoplasty. The rate of success of PK is often excellent, but the chance of graft rejection increases significantly with active or recurrent infection, inflammation, corneal vascularization, or previous graft rejection.

Preoperative evaluation and diagnostic approach
• It is important to perform a careful preop evaluation & thoroughly discuss with patient surgery, visual expectation, possible
complications, and, in particular, the long process of postoperative care. The recipient must be prepared for lifelong management of the eye. In general, important considerations for preoperative evaluation for PK are as follows

Preoperative evaluation and diagnostic approach
•Evaluation of visual potential.• Ocular surface disease – must be recognized and treated prior to PK.• Includes rosacea, dry eyes, blepharitis, trichiasis, exposure keratopathy, ectropion, and entropion.• IOP must be controlled prior to surgery.•Ocular inflammation – must be recognized and treated.

Preoperative evaluation and diagnostic approach
• Prior corneal diseases and vascularization – a history of herpetic keratitis significantly reduces the chance of graft success due to several factors, including recurrent disease in the graft, vascularization, trabeculitis with increased IOP, and persistent inflammation that may induce rejection.• Peripheral corneal thinning/melting (such as that associated with rheumatoid arthritis) – may significantly affect surgical outcome .

INDICATIONS

Optical:•A healthy, clear donor cornea is used to replace an opaque, cloudy, or distorted cornea in an attempt to improve vision and hence quality of life• Pseudophakic bullous keratopathy•Keratoconus , Regraft secondary to rejection• Keratoglobus , Degenerations , Dystrophies , Scar• Aphakic bullous keratopathy , Congenital opacities,
Chemical injuries .

Tectonic•A donor cornea is used to restore the recipient corneal anatomy and globe integrity
•Descemetocele•Corneal stromal thinning• Corneal perforation

Therapeutic•Surgical intervention is performed when therapeutic measures have failed and infection continues to progress.• Infection may be due to bacteria, virus, parasites, or other cause.

Cosmetic•Corneal transplantation is performed to improve the appearance of the patient and has no bearing on the visual outcome. This could also be done in a nonseeing eye. An opaque cornea with a white or blue-gray hue may be disturbing to the patient, who may request PK.

Surgical techniques• decompression of globe is ensured prior to PK, as excessive preop IOP may increase risk of expulsive choroidal hemorrhage. Intravenous mannitol or mechanical ocular decompression should be considered. Miotics are placed preoperatively to protect the lens during surgery. Scleral supporting rings may be used principally in aphakic eyes or in young patients. Care is needed when suturing the scleral fixation rings, as inadvertent misalignment of the rings may result in irregular trephination

Graft Size Determination
•Before handling the donor cornea, the recipient graft size should be decided and both donor and recipient trephine blades should be examined under the operative microscope to ascertain the indicated correct size and quality of the blades.•Graft size determination is based on three main factors: the size of the recipient cornea, the targeted disease, and the known increased risk of rejection with increasing graft size.

Graft Size Determination
•Most adult corneas measure slightly greater in horizontal meridian compared with vertical meridian because superior limbus descends slightly superiorly. White-to-white measurements for an adult cornea in the horizontal meridian are on average 12.5 mm. A normal-sized cornea with endothelial disease such as Fuchs' endothelial dystrophy, iridocorneal endothelial syndrome, or pseudophakic bullous keratopathy would typically be trephinated with a 7.5-mm trephine .

Graft Size Determination
•Although a larger recipient size trephination would supply a larger quantity of healthy endothelial cells, larger donor corneal size (> 8 to 8.5 mm) is associated with a higher risk of rejection . Ectatic corneal pathologic processes, including keratoconus and PMD , require prior recipient donor size measurements at the slit lamp because the area of corneal thinning is often larger than that seen under the operating microscope. It is paramount that the area of thinning be encompassed in the trephinated tissue to avoid tissue disparity and wound mismatch .

Graft Size Determination•Most surgeons use a 0.25-mm oversize in the donor button to counteract the 0.2-mm difference in size produced by endothelial trephination of the donor cornea. This essentially counteracts the disparity to give an equivalent donor and recipient trephination


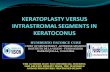
TREPHINES USED IN KERATOPLASTY
Hanna trephine leftBaron hessburg trephine middleOpen disposable trephine right

Surgical techniques• It is customary first to trephinate the donor cornea before the recipient trephination, thereby avoiding any error in sizing and an incomplete or aborted donor cornea trephination. error in donor cornea trephination precludes continuing with procedure The AC is maintained when possible by injection of balanced salt solution throughout the procedure, and wound integrity is verified with a Weck cell sponge at the end of the procedure. All wound leaks should then be corrected.

Surgical techniques•The size of the graft is determined based on location of pathology and clinical judgment. The donor tissue is typically sized 0.25 mm larger in diameter than the recipient tissue. In certain circumstances, a larger (0.5 mm) donor may be considered in an aphakic eye to induce myopia, or a same size donor button, such as in a recipient with keratoconus, may be chosen to reduce myopia.

Surgical techniques•The visual axis of the recipient cornea is marked with a marking pen. An inked radial keratotomy marker may be used to mark the peripheral cornea. If a sclerally-fixated IOL is planned, the scleral flaps are made prior to trephination, and the IOL is prepared before the eye is opened. A donor corneal button is punched. Today most commonly used trephine is the Barron Donor Cornea Punch . donor is cut from endothelium to epithelium.

Surgical techniques• donor is cut from endothelium to epithelium. The donor also may be cut from epithelium to endothelium using an artificial anterior chamber, and then a manual trephine as above, or more recently, the femtosecond laser may be used.This has the theoretical advantage that both the donor and recipient are cut in the same fashion with the same blade, which reduces donor–recipient disparity and potentially reduces astigmatism.

Surgical techniques•The recipient cornea may be cut using a variety of trephines, such as the Hessburg–Barron suction trephine , Hanna trephine, Castroviejo trephine, and now with a femtosecond laser. The Hessburg– Barron suction trephine consists of a circular blade assembly that has a vacuum chamber attached to a spring-loaded syringe. Excision of host corneal button may be performed via a partial-thickness trephination followed by a controlled entry into anterior chamber.

Surgical techniques•Excision of host corneal button may be performed via a partial-thickness trephination followed by a controlled entry into anterior chamber using a No. 75 Beaver blade, or via a continued trephination that is stopped as soon as aqueous egress shows anterior chamber has been entered. recipient button is then excised using forceps and corneal scissors . edge of recipient bed is made perpendicular for optimal graft–host apposition.

Surgical techniques•Pilocarpine 2% to 4% is typically applied three times at 5-minute intervals, 1 hour before surgery. This ensures a constricted lens-iris diaphragm, therefore reducing potential damage to the lens, IOL, lens capsule, and vitreous face.•Mydriatic agents for pupillary dilation include 1% tropicamide, 2.5% phenylephrine, and 1% cyclopentolate. These agents are used when prior phacoemulsification, open-sky cataract extraction, or posterior lens repositioning is planned.

Surgical techniques• If patient requires concurrent cataract extraction, IOL explantation, anterior vitrectomy, or the placement of a new IOL, this may be done prior to trephination, if visualization allows. Since in many cases the diseased cornea precludes adequate visualization, an “open sky” technique is utilized after trephination Viscoelastic may be placed in anterior chamber of recipient and donor button then is placed over recipient bed and sutured in place with four cardinal sutures .

Surgical techniques•Care is taken in placement of the cardinal sutures, as proper tissue distribution is paramount. depth of suture is 90% of corneal thickness. remaining sutures may be a combination of interrupted and running sutures or solely interrupted sutures . The author’s choice is often 8 interrupted sutures with an additional single 10-0 nylon running suture that encompasses 360 degrees of
corneal wound. If there is corneal neovascularization, then interrupted sutures.

Surgical techniques• Interrupted sutures are suited for vascularized or thinned cornea, as subsequent selective removal may be necessary to prevent advancement of vessels or to control astigmatism.•Running sutures have the advantage of speedy placement intraoperatively and better tension distribution and healing. Prior to placement of final sutures, the viscoelastic material in the anterior chamber is removed.

Surgical techniques•The running sutures may be adjusted intraoperatively by using a keratoscope.
•When the suturing is complete, all sutures are rotated such that the knots are buried within the stroma, and the security of the wound is tested.
















Four cardinal sutures in place

12 interrupted sutures in place

Running suture

Sutures in Knots buried



TYPE OF SUTURING•Four categories of suturing techniques employed in keratoplasty will be addressed in subsequent sections:•1 Interrupted sutures (IS)•2 Combined continuous and interrupted sutures (CCIS)•3 Single continuous suture (SCS)•4 Double continuous suture (DCS)

Cardinal suturesThe second suture is 180 degrees from the first suture so that the donor tissue and wound are divided equally into nasal and temporal halves .The third and the fourth sutures also divide the donor tissue and wound evenly









Suture Patterns and Suture Materials
•The suture material of choice for PK is nylon. corneal suturing techniques ranges from a combination of interrupted sutures with a single running suture, to all interrupted
sutures, to double-running sutures. Although for the most part 10-0 nylon sutures are used, with double-running sutures, first running suture may be 10-0, followed by an 11-0 or10-0 nylon suture for second running suture.

Suture Patterns and Suture Materials
•The initial step with all grafting techniques is the fixation of the graft to the donor cornea with 4 cardinal sutures at the 12-, 6-, 3-, and 9-o’clock positions. The first suture is placed at the 12-o’clock position. The donor corneal disc may be held with a double-prong forceps, such as a Polack forceps (Rumex Inc), for better donor disc stabilization, and the needle is passed between the two prongs of the forceps.

Suture Patterns and Suture Materials
•For all subsequent sutures, a 0.12 forceps may be used. •The second corneal suture is the most important suture because it determines the proper seating of the donor graft. This suture is placed at the 6-o’clock position, and the graft should have equal corneal tissue on either side of this suture .

Suture Patterns and Suture Materials
• last two cardinal sutures are placed at 3- and 9-o’clock positions, and this provides initial fixation of donor graft to recipient corneal bed. Whereas the interrupted sutures are placed deep within corneal stroma of donor and recipient corneas, the running sutures are somewhat more superficial. Avoid sutures passing through the full thickness of the donor graft. All suture knots are buried within the cornea to provide patient comfort.

Suture Patterns and Suture Materials
•Knots may be buried within donor cornea or the recipient cornea. •However, some are of the opinion that knots buried within the host cornea may be more prone to corneal neovascularization. Use of intraoperative keratoscopy can provide optimal suture tension and astigmatism control.

Five important points regarding suture adjustment should be emphasized
• 1 Corneal astigmatism is multifactorial and suture adjustment or removal can only correct astigmatism that is due to uneven suture tension in a approximated wound. If wound is unevenly approximated, adjustment of suture tension does little to reduce astigmatism.• If uniform tension in a regular wound is present and vector forces are even across the wound, continuous sutures work well.

Five important points regarding suture adjustment should be emphasized
•However, continuous sutures do not protect a wound from locally applied forces and they are poorly suited for irregularly shaped wounds that require vastly different amounts of tension at different sites in wound. Interrupted sutures better serve such irregularly shaped wounds. astigmatism with all sutures out postop may reflect poor donor trephination, uneven use of corneal scissors, and/or improper placement of the initial interrupted cardinal sutures.

Five important points regarding suture adjustment should be emphasized•2 Once the suture has been adjusted or removed to achieve suitable topography, remaining sutures should be left in place until they have to be removed. Patients should be advised that sutures can be left in place until there is an indication for removal. Some fibrosis can be expected around the suture track, but usually this is not an indication for removal. most common indication for removal of single continuous suture is breakage.

Five important points regarding suture adjustment should be emphasized•3 After several years, continuous sutures may be easier to remove than interrupted sutures. As the suture degrades, knots can become more difficult to remove. Continuous sutures may therefore cause less inflammation and less likelihood of residual buried remnants than interrupted sutures.

Five important points regarding suture adjustment should be emphasized•4 Wound healing can be variable from patient to patient, and postoperative use of topical and systemic corticosteroids varies among surgeons. The decision on when sufficient wound integrity exists to safely remove a corneal suture must be made carefully with these variables in mind, weighing risks and benefits. timings for suture removal given are only guidelines & every patient & wound must be addressed on an individual basis.

Five important points regarding suture adjustment should be emphasized•5 The ultimate decision regarding suture technique comes down to surgeon preference and individual patient characteristics.
• All suture techniques can provide excellent optical results with appropriate surgeon experience and skill.

DALK

Deep Anterior LamellarKeratoplasty DALK
•Historically, corneal transplantation has been performed through full-thickness grafting, also known as penetrating keratoplasty (PK). Lamellar keratoplasty (LK) is a more recent approach to allow for preservation of unaffected tissue, and specialized procedures allow for preservation
of either the anterior or posterior corneal layers. The main determining factor in whether to use an anterior or posterior approach is health of the corneal endothelium. The first LK was performed more than 150 years ago

Deep Anterior LamellarKeratoplasty DALK• first LK was performed more than 150 years ago, although historically use of anterior LK was limited by worse visual outcomes compared with PK, as well as technical difficulty of the procedure.In second half of 20th century, PK was largely favored. However, in 1970s, there was an increased interest in lamellar procedures. With advances in technical approach to deep anterior lamellar keratoplasty (DALK), which involves removal of the central corneal stroma with preservation of Descemet’s membrane and corneal endothelium, there has been a resurgence in interest in this technique.

Deep Anterior Lamellar Keratoplasty
•DALK has become an alternative to PK for a variety of indications . Studies have demonstrated equivalent best corrected visual outcomes and superior preservation of endothelial cell density with DALK compared with PK. Interest in DALK has been piqued by its advantages, including enhanced structural integrity, decreased recovery time, and lower incidence of rejection and infection.

Surgical Technique•Depending on patient’s corneal diameter and disease, the DALK bed is typically measured
with a diameter of 7 to 8.5 mm . A trephine is used to cut through anterior stromal layer without entering anterior chamber. depth of trephination depends on surgeon preference and depth of disease in stroma. most surgeons now favoring a Descemet’s–baring procedure using the big-bubble technique .

Big-Bubble Technique
•1. Trephination•2. Air injection•3. Partial keratectomy•4. Incision into the anterior wall of big bubble•5. Severing the stroma with an iris spatula

Big-Bubble Technique6. Formation of 2 slits into the anterior wall of the collapsed bubble7. Lifting deep stroma and excision with scissors8. Moistening Descemet’s membrane9. Suturing the donor corneal tissue10. Special situations and complications• Failure to form big bubble• Perforation of Descemet’s membrane

Combination Big-Bubble/Viscoelastic Technique
•We use a combination of steps from the big-bubble and viscoelastic techniques to produce successful anatomic and visual results with the DALK procedure. The steps of our procedure are as follows :•1. Trephination is performed using Hessburg-Barron trephine to 80% depth (approximately
300 μm) with 4 to 5 quarter turns of handle (each quarter turn cuts approximately 60 μm).

Combination Big-Bubble/Viscoelastic Technique
2. paracentesis incision is made to decrease IOP , and 4 to 6 small air bubbles are injected into the anterior chamber.3. A bent 27-gauge needle on an air-filled syringe is used to advance the bevel down into the deep periphery of the trephined cornea at the level of the deepest trephination toward the corneal center;

Combination Big-Bubble/Viscoelastic Technique
this is followed by the Tan cannula on an air-filled syringe to inject the air with the goal of dissecting Descemet’s membrane off the central cornea.4. Partial keratectomy is performed with a crescent blade to dissect off the superior lamellar tissue.

Combination Big-Bubble/Viscoelastic Technique
5. Viscoelastic dissection of Descemet’s membrane is performed with Healon on a 27-gauge needle inserted into the corneal center to dissect off Descemet’s membrane all the way past the trephine border.6. The stroma is severed with an iris spatula.7. Two slits are formed in corneal stroma in a cruciate pattern with a blade (the viscoelastic helps protect the underlying Descemet’s membrane from traumatic damage and performation).

Combination Big-Bubble/Viscoelastic Technique
8. deep stroma is lifted and 4 quadrants are excised, then Tan DALK scissors are usedto excise these 4 quadrants of tissue and trim off peripheral rim of the corneal tissue.9. The donor tissue is cut to the same size.10. The donor Descemet’s membrane is stained with trypan blue and subsequently stripped and removed using a Weck-Cel sponge and/or smooth tying forceps.•11. The donor corneal tissue is sutured.


DALK TECHNIQUE

DALK TECHNIQUE•A POCKET IS CREATED FOR A CANNULA TO INJECT PRE-DESCEMET’S AIR . THIS POCKET DOES NOT HAVE TO COMPLETELY REACH DESCEMET’S IN ORDER FOR AN AIR INJECTION TO CREATE A CLEVAGE PLANE.

•Big bubble formation is characterized by a semi-opaque disk with a near circular outline. Air separates the central Descemet's membrane from the stroma by forming a large
air bubble

DALK TECHNIQUE•AIR HAS BEEN INJECTED TO SEPARATE DESCEMET MEMBRANE FROM STROMA . THE SUCCESS OF THAT MANEUVER CANNOT BE DETERMINED AT THIS POINT

DALK TECHNIQUE•AN ANTERIOR CAP OF STROMA IS DISSECTED AND REMOVED

DALK TECHNIQUE• REMOVAL OF NATERIOR CAP DISCLOSES A DARK AREA RESULTING FROM INJECTED AIR .REMOVAL OF SOME AQUEOUS HUMOR BY PARACENTESIS ALLOW SMALL AIR BUBBLE TO EXPAND .AIR IS THEN INJECTED IN ANTERIOR CHAMBER TO SEE IF SMALL BUBLE DISPLACES TI TO PERIPHERY

DALK TECHNIQUE• A BLUNT 25 CANNULA WITH A PORT ON POSTERIOR SURFACE IS USED TO GAIN ACCESS TO SPACE BETWEEN STROMA AND DESCEMET MEMBRANE BY MEANS OF BLUNT DISSECTION AND INJECTION OF SODIUM HYALURONATE .SUCCESS IS SUGGESTED BY A BILOBED AIR BUBBLE IN ANTERIOR CHAMBER

DALK TECHNIQUE
•STROMA IS BEING REMOVED

DALK TECHNIQUE• SMALL AMOUNT OF PERIPHERAL STROMA REMAINS . A LARGE AMOUNT OF CENTRAL CLEAR DESCMET’S MEMBRANE IS PRESENT . IT IS BEST NOT TO RISK PERFORATION TRYING TO REMOVE ALL STROMA .

DALK TECHNIQUE•DESCEMET’S MEMBRANE WITH ENDOTHELIUM IS STRIPPED FROM DONOR

DALK TECHNIQUE•DONOR IS SUTURED WITH EIGHT CARDINALS AND A RUNNING SUTURE .


DALK VS PK• American Academy of Ophthalmology DALK/PK studies found visual acuity results between the 2 procedures to be equivalent,
although there was a trend toward worse visual outcomes if more than 10% of the recipient stromal bed was retained. Rates of both early and late endothelial cell loss are lower in DALK than in PK, and graft survival has been shown to be longer in eyes undergoing DALK with big bubble technique compared with PK. perience.

DALK VS PK• In the same study, better visual acuity results were achieved with the big bubble technique compared with manual-dissection DALK.• A recent study focused on outcomes of DALK vs PK from the patient perspective. Among 20 patients who had undergone PK in one eye and DALK in other, there was no significant difference in objective findings, including visual acuity and refractive outcomes. However, patientsreported preferring the PK procedure, although there was no further detail available on which aspects of experience were different between 2 procedures.


Conclusion DALK offers an option for corneal transplantation in eyes with a healthy corneal endothelium and is becoming more accessible to corneal surgeons. This technique is generally less traumatic, avoids rejection, provides tectonic support in cases of trauma, and has advantage of being a largely extraocular procedure. Although perforation of Descemet’s membrane may necessitate conversion to PK, this complication is increasingly rare.

Conclusion•DALK should especially be considered in patients with a high rejection or infection risk who require corneal transplantation with a healthier endothelium due to the shorter course of topical steroids required with this technique compared with PK .

EK TECHNIQUES•Melles eliminated the challenging recipient stromal dissection and excision steps by peeling the Descemet’s membrane & dysfunctional endothelium from the recipient cornea before implanting the donor tissue. This EK modification became known as Descemet’s stripping with endothelial keratoplasty (DSEK).

EK TECHNIQUES•Use of a microkeratome was introduced to facilitate the donor lamellar dissection, and this technique variation was called either DSEK or Descemet’s stripping automated endothelial keratoplasty (DSAEK). In 2005, eye banks began performing the donor lamellar dissection with a microkeratome and providing ‘pre-cut’ tissue to surgeons .

DSEK•Even though DSEK provides 20/40 or better vision more reliably than PK, fewer patients than expected achieve 20/20 vision and variations in the donor stromal thickness increase the higher order aberrations of the posterior corneal surface. Addressing these concerns, Melles developed a technique for peeling Descemet’s membrane and healthy endothelium from a donor cornea.

DMEK•Melles developed Descemet’s membrane endothelial keratoplasty (DMEK). The extremely thin DMEK graft is more challenging to handle than a thicker DSEK graft, leading to the development of hybrid techniques that have a narrow rim of donor stromal tissue ringing a central area of bare endothelium without stroma . The hybrid techniques, known as DMEK-S and DMAEK, combine excellent visual outcomes with easier handling.

DMEK• In 2006, Tappin first performed the true endothelial cell transplantation of Descemet’s membrane using a carrier device. Later, Melles reported the first clinical results of transplanting isolated Descemet’s membranes in human eyes and called the procedure Descemet’s membrane endothelial keratoplasty (DMEK). Existence of a distinct pre-Descemet’s layer (Dua’s layer) of tissue.

PDEK• evidence of a distinct pre-Descemet’s layer (Dua’s layer) of tissue was presented by Dua in 2007. Addition of a 10-μm pre-Descemet’s layer to the endothelial allow easier handling and insertion of the tissue because it does not tend to scroll as much as Descemet’s membrane, with the pre-Descemet’s layer splinting Descemet’s membrane. Pre-Descemet’s endothelial keratoplasty (PDEK) is term given to this technique in which additional pre-Descemet’s layer is transplanted.

DSEAKTISSUE PREPARATION

DSEAK TISSUE PREPARATION•THE CORNEO SCLERAL RIM IS PLACED OVER THE ARTIFICIAL ANTERIOR CHAMBER

DSEAK TISSUE PREPARATION•AN ALIGNMENT MARK IS MADE ON THE CORNEA

DSEAK TISSUE PREPARATION•THE CORNEO SCLERAL RIM IS PRESSURISED . THE ALIGNMENT MARK 1 IS SEEN .

DSEAK TISSUE PREPARATION•THE MICRO KERATOME HEAD IS ENGAGED AND CORNEAL CUT IS INITIATED

DSEAK TISSUE PREPARATION
ANTERIOR STROMAL CAP 2 IS CUT

DSEAK TISSUE PREPARATION• ANT. STROMAL CAP IS REMOVED AND THICKNESS OF POST. CORNEA CAN BE MEASURED .A S SHAPED MARK IS PLACED OVER POSTERIOR STROMA TO HELP WITH INTRAOCULAR ORIENTATION

DSEAK TISSUE PREPARATION•ANTERIOR STROMAL CAP IS REPLACED AND ALIGNMENT MARK 3 IS REAPPROXIMATED . THE S SHAPED MARK 4 ON POSTERIOR STROMA IS VISIBLE

DSEAK TISSUE PREPARATION

DSEK PROCEDURE

DSEK PROCEDURE•PREOPERATIVE APPEARANCE IN A PATIENT WITH PSEUDOPHAKIC BULLOUS KERATOPATHY

DSEK PROCEDURE•SURGEON’S VIEW FROM TEMPORAL LIMBUS . THE DESCEMET’S MEMBRAE IS
BEING STRIPPED AND FOLDED BACK UPON ITSELF

DSEK PROCEDURE•THE ENDOTHELIUM DONOR DISC 1 IS LOADED IN ENDOSERTER . THE DONOR STROMA 2 IS DISCARDED

DSEK PROCEDURE•THE DONOR TISSUE IS RETRACTED INTO ENDOSERTER

DSEK PROCEDURE•THE ENDOSERTER IS ROTATED 180 DEGREES AND THE DONOR DISC 1 IS BEING DELIVERED IN ANTERIOR CHAMBER .

DSEK PROCEDURE•AIR IS INJECTED INTO ANTERIOR CHAMBER THROUGH A NEEDLE

DSEK PROCEDURE•TRANSCORNEAL VENTING INCISIONS ARE MADE WITH A MYRINGOTOMY BLADE TO REMOVE THE INTERFACE FLUID

DSEK PROCEDURE•POST OPERATIVE DAY 1 •CORNEA IS GETTING CLEAR


INDICATIONS•EK is an excellent option for any type of endothelial dysfunction. If anterior stromal scarring from long-standing corneal edema is significant, replacement of the full corneal thickness with a PK may provide better visual acuity. However, in many cases, patients who have tolerated long-standing corneal edema also have other visual limitations (e.g., retinal problems).In such cases, EK is an attractive alternative because it quickly restores vision .
resolves the corneal edema and bullae while maintaining much of the structural integrity of the eye.

Donor Tissue Preparation and Insertion•Donor tissue preparation involves three steps:• dissection,• sizing to the appropriate diameter with a trephine (usually 8–9 mm), •and insertionPreparing the donor tissue before opening the patient’s eye allows the surgeon to ensure that the tissue will be suitable for transplantation

DSEK•The lamellar dissection is usually done with a microkeratome either at the eye bank or at the time of surgery . A donor corneal/ scleral shell is mounted on an artificial anterior chamber designed to accompany the microkeratome being used. The artificial anterior chamber can be filled with viscoelastic material, balanced salt solution,
or tissue storage solution.

DSEK•The donor thickness is measured, and a microkeratome head of appropriate depth is selected to provide a posterior donor button of approximately 0.08−0.20 mm thickness, according to surgeon preference.

DSEK•The donor tissue is carefully transferred from the artificial anterior chamber and placed endothelial side up on a standard punch trephine block, where it is punched to an diameter, taking into consideration the horizontal white-to-white dimensions of the recipient cornea and the anterior chamber depth. donor tissue is covered with tissue storage solution while the recipient eye is prepared.

Insertion techniques•A variety of insertion techniques are available, including forceps, glides and inserters. When using forceps, the posterior donor button is folded over on itself like a “taco” with approximately 60% anterior and 40% posterior, and the folded tissue is gently grasped at the leading edge with forceps that only compress at the tip as the tissue is guided into the eye. A disadvantage of this method is that it can be difficult to unfold the donor correctly in the eye.

Insertion techniques•A disadvantage of this method is that it can be difficult to unfold the donor correctly in the eye, especially for surgeons early in the learning curve. Another method is to fixate the edge of the donor with a suture, thread the suture across the anterior chamber & out through a stab incision nasally, and pull the tissue into the eye .

Insertion techniques•A third method is to place tissue on a glide or insertion cartridge, insert retina /vitreal intraocular forceps through a nasal stab incision, reach across the eye and grasp the tip of donor through the 5 mm temporal incision, and pull the tissue into the eye •Use of a funnel glide or insertion cartridge helps the donor tissue curl with endothelium inward for protection as it is inserted. The tissue can also be inserted with a single-use cartridge inserter .

Operative steps•Once donor tissue is in eye & unfolded stromal side up, anterior chamber is filled with air to press donor button up against
recipient cornea . Several small incisions can be made in peripheral recipient cornea down to graft interface to help drain any fluid . trapped between donor and recipient tissue After 8–10 minutes, many surgeons remove most of the air to prevent pupillary block, and leave anterior chamber one-third full

Operative steps•Some surgeons then have the patients lay face up with a partial air bubble for 30–60 minutes. Other surgeons leave anterior chamber completely filled for 1–2 hours.• At completion of surgery, antibiotics, corticosteroids, dilating drops, and NSAIDs are applied to the treated eye.

DMEK•The donor tissue dissection consists of gently peeling off Descemet’s membrane (DM) and endothelium First, DM periphery is scored all the way around. The tissue is stained with trypan blue to enhance visualization. The peripheral edge is lifted all the way around using a microfinger or hockey stick-shaped instrument.

DMEK DONOR PREPARATION
•MICRODISSECTOR IS USED TO ELEVATE THE SCORED EDGE OF DESCEMET’S MEMBRANE .

DMEK•With the tissue submerged in tissue storage solution, an edge of membrane is grasped with forceps and peeled about halfway to center, quadrant-by-quadrant, with replacement of each section on stromal base . The tissue is partially trephined, cutting through DM but not completely through the stroma. An edge is grasped with nontoothed forceps and the central DM is gently peeled from the underlying stroma and replaced in tissue storage solution.

DMEK DONOR PREPARATION•TUBAGEN FORCEPS ARE USED TO PEEL THE FINAL GRAFT FROM THE DONOR RIM AFTER CENTRAL TREPHINATION

DMEK• Immediately before insertion , DM is stained again with trypan blue to improve visualization and is placed in a glass pipette or inserter, such as an intraocular lens inserter, for placement in the recipient eye. The donor DM is gently unfolded in the correct orientation with a combination of balanced salt solution and air injections.•Then air is injected beneath the donor tissue to completely fill the anterior chamber and press the graft up against the host cornea

DMAEK and DMEK-S• In the hybrid techniques, the donor preparation consists of four steps: lamellar dissection, injection of air to create a big bubble and separate DM from the central stroma, excision of the stromal tissue from the central 6–7 mm of the donor graft, and cutting the tissue to the desired diameter with a trephine. Although this sequence of donor preparation steps is more complex than that required with DMEK, the resulting 1 mm rim of attached stromal tissue allows the surgeon to easily insert the hybrid grafts using standard DSEK techniques, as described above.

OUTCOMES• EK provides more rapid and predictable visual recovery than PK,
allowing patients to return to work and daily activities sooner. In large PK series, the rate of 20/40 or better vision has ranged from 47% to 65% in Fuchs’ dystrophy patients & from 20% to 40% in patients with pseudophakic or aphakic bullous keratopathy. Unfortunately, PK can result in significant corneal distortion, so 10–15% of PK eyes generally require use of a hard contact lens for best vision, and in some cases vision can be limited to counting fingers or worse. DSEK is performed through a small incision and causes little to no corneal distortion. A mean corrected distance visual acuity (CDVA) of 20/40 is generally achieved within 3–6 months of DSEK, and over 90% of patients without ocular co-morbidities achieve 20/40 or better vision.

OUTCOMES• A small percentage of DSEK patients reach less than 20/40
vision because of irregularities resulting from the lamellar dissection or from folds that form in the donor tissue as it conforms to the back of the recipient cornea. With DMEK and the hybrid techniques, the visual recovery is even more impressive than it is with DSEK. Over 70% of DMEK patients without ocular co-morbidities achieve 20/25 or better vision within 3 months. Overall the visual acuity achieved with DMEK is comparable to that in normal eyes, and significantly better than that achieved with DSEK or PK. One reason for this is that DMEK achieves a more normal posterior corneal surface with fewer higher-order aberrations than DSEK or PK.

Refractive Changes• In contrast to PK, EK causes little to no change in corneal topography, resulting in far less change in spherical equivalent or cylinder. Whereas PK induces 4–5 D of refractive cylinder on average and may exceed 8 D, DSEK and DMEK cause no significant increase in mean refractive cylinder. DSEK generally induces 0.5–2.0 D of hyperopia, while DMEK causes a smaller mean hyperopic shift of about 0.25–0.50 D. The expected hyperopic shift should be factored into intraocular lens calculations when cataract surgery is staged before, or combined with, EK.

Graft Survival• it is not unusual for surgeons who are newly learning EK to initially have a higher rate of primary graft failure due to surgical trauma. However, with experience, the primary graft failure rate should drop to the low levels seen with PK.• In an initial consecutive DSEK series, the 5-year graft survival rate was similar to that reported for PK in the large multicenter Cornea Donor Study

Graft Survival• In an initial consecutive DSEK series, the 5-year graft survival rate was similar to that reported for PK in the large multicenter Cornea Donor Study (95% vs 93% for Fuchs’ dystrophy & 76% vs 73% for pseudophakic or aphakic corneal edema). Whereas PK regrafts generally have a poor 5-year survival rate of 53% or less, 4-year survival rate for DSEK under failed PK was 74% in an initial consecutive series.

ComplicationsGraft detachment
•Lack of complete adherence between the donor tissue and host cornea is the most frequently reported complication with EK. ranged from 0 to 82%. An EK graft is secured into position with an air bubble initially, rather than with sutures, so detachment is addressed by re-injecting air into eye. Keys to minimizing the risk of graft detachment are meticulous wound construction to preclude postoperative wound leaks ..

ComplicationsGraft detachment
•Keys to minimizing the risk of graft detachment are meticulous wound construction to preclude postoperative wound leaks, complete removal of fluid from donor/ host interface, achieving a firm air tamponade, and cautioning patient not to rub eye in the early postoperative period. Partially detached DSEK grafts can be watched as they frequently will seal down spontaneously over time. With DMEK and hybrid techniques, partial detachments are more common and less likely to seal down spontaneously.

COMPLICATIONS OF DMEK

Pre-Descemet’sEndothelial Keratoplasty PDEK

PDEK•Addition of a 10-μm pre-Descemet’s layer to the endothelial graft can generate tissue for endothelial transplant, allowing easier handling and insertion of tissue because it does not tend to scroll as much as Descemet’s membrane, with pre-Descemet’s layer splinting Descemet’s membrane. Pre-Descemet’s endothelial keratoplasty (PDEK) is the term given to this technique .

Surgical Technique Donor Preparation
•A corneoscleral disc with an 2-mm scleral rim is dissected from whole globe or obtained from an eye bank. A 30-gauge needle attached to a syringe is inserted from limbus into midperipheral stroma . Air is slowly injected into donor stroma until a type 1 big bubble is formed, which is a well-circumscribed, central domeshaped elevation measuring 7 to 8.5 mm in diameter .

Surgical Technique Donor Preparation
• It starts in center and enlarges centrifugally, retaining a circular configuration. Trephination of donor graft is performed along the margin of big bubble . The bubble wall is penetrated at the extreme periphery, and trypan blue is injected into the bubble to stain the graft, which is then cut all around the trephine mark with corneoscleral scissors and covered with the tissue culture medium. graft is loaded into an injector when ready for insertion.

PDEK donor graft preparation
•A 30 gauge needle is inserted at limbus on endothelial side .

PDEK donor graft preparation
•Needle is advanced into stroma

PDEK donor graft preparation
•Intra stromal air injection is performed

PDEK donor graft preparation
•Central dome shaped big bubble is formed

PDEK donor graft preparation
•Trephination of endothelial graft is performed

PDEK donor graft preparation
•Stained with tryptan blue and cut with corneo scleral scissors


Recipient Bed Preparation•After administering peribulbar anesthesia, the recipient corneal epithelium is debrided (if grossly edematous) for better visualization . A trephine mark is made on the recipient cornea respective to the diameter of Descemet’s membrane to be scored on endothelial side . A 2.8-mm tunnel incision is made at 10-o’clock position near limbus. The anterior chamber is formed and maintained with saline injection or infusion.

Recipient Bed Preparation•margin of Descemet’s membrane to be removed is scored initially from endothelial side with a reverse Sinskey hook . Once an adequate edge is lifted, a nontoothed forceps is used to gently grab Descemet’s membrane at its edge, and the graft is separated from the underlying stroma in a capsulorrhexis-like circumferential manner. The peeled Descemet’s membrane is then removed from the eye.


Donor Lenticule Implantation•The donor lenticule (endothelium–Descemet’s membrane–pre-Descemet’s layer) roll is inserted in the custom-made injector and slowly pushed up the lumen of the nozzle. The injector is improvised from an intraocular lens implant injector by removing the sponge tire and spring and reattaching the sponge tire to prevent any back suction and inadvertent damage to the donor graft.

Donor Lenticule Implantation•Using the injector, the graft roll is injected in a controlled fashion into the anterior chamber. The donor graft is oriented endothelial side down and positioned on the recipient posterior stroma by careful, indirect manipulation of the tissue with air and fluid . •Once the lenticule is unrolled, an air bubble is injected underneath the donor graft lenticule to lift it toward the recipient posterior stroma.

Donor Lenticule Implantation•The anterior chamber is completely filled with air for next 30 minutes, followed by an air-liquid exchange to pressurize the eye . •The eye speculum is removed and the anterior chamber is examined for air position. •The patient is advised to lie in a strictly supine position for the next 3 hours

Discussion•Although DMEK provides a significantly higher rate of 20/20 and 20/25 vision, with comparable endothelial cell loss compared with DSAEK procedure; a 63% air reinjection rate for partial detachments and 8% rate of graft failure, which requires a repeat DMEK or DSAEK, have been reported. It has failed to gain widespread acceptance mainly because of difficulty in donor preparation resulting in a significant loss of donor tissue .

Discussion• It has failed to gain widespread acceptance mainly because of difficulty in donor preparation resulting in a significant loss of donor tissue, loss of endothelial cells after Descemet’s membrane removal, and difficulty in positioning the donor tissue within the eye. In PDEK, the pre-Descemet’s layer serves as a splint, which facilitates easy manipulation of the entire graft.

Discussion•Because the endothelium–Descemet’s membrane complex remains adherent to the underlying pre-Descemet’s layer, tight rolling of the thin, delicate tissue is prevented. The splinting effect provided by the additional layer reduces inadvertent tears or endothelial damage during tissue harvesting and intraoperative maneuvers. PDEK donor membrane complex is thicker than DMEK donor graft and reduces the likelihood of upside-down transplantation .


THANK YOU
DR DINESHDR SONALEE
Related Documents