1 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014 SH CP 32 Isolation for In-patient Areas (Source & Protective) Procedure (Infection Prevention and Control Policy: Appendix 9) This Appendix must be read in conjunction with the Infection Prevention and Control Policy Version: 2 Summary: Provides evidence based guidelines on the management of the infectious service user requiring source isolation. Protective isolation of service users who are significantly vulnerable to infection is also covered Keywords (minimum of 5): (To assist policy search engine) Source isolation, protective isolation, notification, cleaning, personal protective clothing, airborne, contact, faecal oral, blood and body fluids Target Audience: All staff of all disciplines, Non-Executive Directors, Volunteers, Governors and Contractors Next Review Date: August 2018 Approved & Ratified by: IP&C Committee Date of meeting: 5 th August 2014 Date issued: August 2014 Author: Jacky Hunt Infection Prevention & Control Nurse Sponsor: Della Warren Chief Operating Officer and Director of Infection Prevention and Control

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
SH CP 32
Isolation for In-patient Areas (Source &
Protective) Procedure
(Infection Prevention and Control Policy: Appendix 9)
This Appendix must be read in conjunction with the
Infection Prevention and Control Policy
Version: 2
Summary:
Provides evidence based guidelines on the management of the infectious service user requiring source isolation. Protective isolation of service users who are significantly vulnerable to infection is also covered
Keywords (minimum of 5): (To assist policy search engine)
Source isolation, protective isolation, notification, cleaning, personal protective clothing, airborne, contact, faecal oral, blood and body fluids
Target Audience:
All staff of all disciplines, Non-Executive Directors, Volunteers, Governors and Contractors
Next Review Date: August 2018
Approved & Ratified by:
IP&C Committee Date of meeting: 5th August 2014
Date issued:
August 2014
Author:
Jacky Hunt Infection Prevention & Control Nurse
Sponsor:
Della Warren Chief Operating Officer and Director of Infection Prevention and Control

2 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Version Control
Change Record
Date Author Version Page Reason for Change
June2014 Jacky Hunt 1 Review date due
22.10.14 Jacky Hunt 2 8,11,33 Technical Amendment due to change of infected linen bag outer cover from red to white
13.3.17 Jacky Hunt 2 20,31,36 Technical Amendment due to change in source isolation requirements for influenza and mumps (appendix 9.3). Appendix 9.5 terminal clean of isolation room has been strengthened to include advice on radiator cleaning and separate instruction is now available for microfibre and mop and bucket cleaning.
7.3.18 Review date extended from July to August 2018
Reviewers/contributors
Name Position Version Reviewed & Date
IP&C Team
Alistair Rumsey Contract Manager – OCS LNFH
Helen Chesterfield Consultant Microbiologist PHT
Stella Gardner
MH/LD&SS Area Lead Nurses and Modern Matrons
ICS Area and Modern Matrons
IP&C Committee
3 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
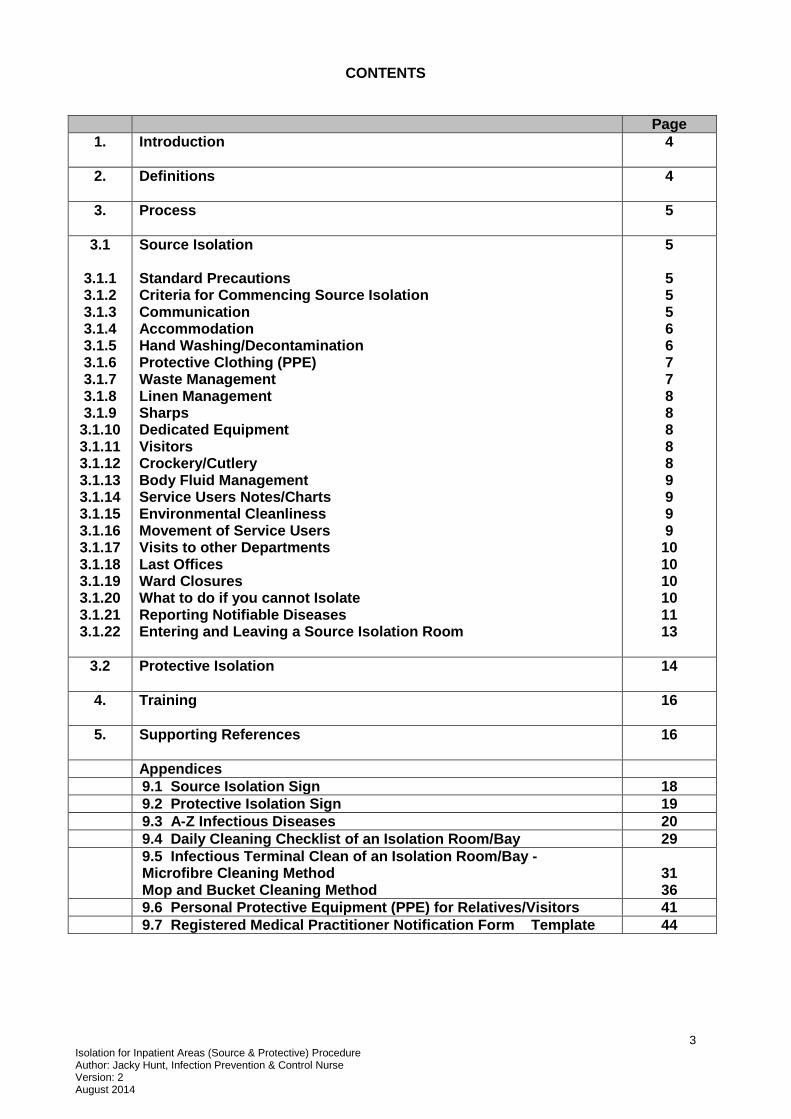
CONTENTS
Page
1. Introduction
4
2. Definitions
4
3. Process
5
3.1
3.1.1 3.1.2 3.1.3 3.1.4 3.1.5 3.1.6 3.1.7 3.1.8 3.1.9
3.1.10 3.1.11 3.1.12 3.1.13 3.1.14 3.1.15 3.1.16 3.1.17 3.1.18 3.1.19 3.1.20 3.1.21 3.1.22
Source Isolation Standard Precautions Criteria for Commencing Source Isolation Communication Accommodation Hand Washing/Decontamination Protective Clothing (PPE) Waste Management Linen Management Sharps Dedicated Equipment Visitors Crockery/Cutlery Body Fluid Management Service Users Notes/Charts Environmental Cleanliness Movement of Service Users Visits to other Departments Last Offices Ward Closures What to do if you cannot Isolate Reporting Notifiable Diseases Entering and Leaving a Source Isolation Room
5
5 5 5 6 6 7 7 8 8 8 8 8 9 9 9 9 10 10 10 10 11 13
3.2 Protective Isolation
14
4. Training
16
5. Supporting References
16
Appendices
9.1 Source Isolation Sign 18
9.2 Protective Isolation Sign 19
9.3 A-Z Infectious Diseases 20
9.4 Daily Cleaning Checklist of an Isolation Room/Bay 29
9.5 Infectious Terminal Clean of an Isolation Room/Bay - Microfibre Cleaning Method Mop and Bucket Cleaning Method
31 36
9.6 Personal Protective Equipment (PPE) for Relatives/Visitors 41
9.7 Registered Medical Practitioner Notification Form Template 44

4 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Isolation for In-patient Areas (Source & Protective) Procedure 1. Introduction
The purpose of this appendix is to:
Control, confine and minimize the spread of infection.
To protect service users, visitors and staff from the risk of infection.
Provide clarity and consistency of what is expected from all staff when caring for service users in isolation in a health care setting.
Provide a minimum standard for services commissioned by Southern Health NHS Foundation
For information and isolation measures required for specific infectious disease please refer to the A-Z list in Appendix 9.3 on page 21. 2. Definitions 2.1 Protective isolation – Minimising the risk of spread of infection between service users
by the physical isolation of service users at increased risk of infection 2.2 Source Isolation - Minimising the risk of spread of infection between service users by
the physical isolation of those service users who pose an infection risk to others.
Physical separation of service user from other service users can be achieved by the following means:
Isolation in dedicated side rooms.
Segregation of a group of service users with a disease or infection from service users who do not harbour the disease or the infection (cohort nursing in open ward / clinic areas).
Use of positive and negative pressure ventilation rooms – this type of isolation is not available within our Trust) but can be found in some Acute Trusts.
High Security Infectious Disease Unit (HSIDU) accommodation. In the rare event that this is required e.g. if viral haemorrhagic fever is suspected, contact: Consultant Microbiologist, Royal Free London Foundation Trust, Coppetts Wood Hospital, +44 (0)20 7794 0500 (Royal Free switchboard, ask for infectious diseases doctor on call).
There are 6 main ways that infections can be spread:
2.3 Airborne - Air borne droplet nuclei (particles ≤ 5m) or dust particles contain the
infectious agent. These particles can remain suspended in the air and travel long distances. If the particles are inhaled, a susceptible person may develop infection eg TB, chickenpox, SARS.
2.4 Droplet Route - Droplets are larger than droplet nuclei and do not remain suspended in
the air, or travel long distances. They are produced when the infected person talks, coughs, or sneezes, and during some procedures (e.g. suctioning and bronchoscopy). A susceptible person may become infected if the infectious droplets land on the mucosal surfaces on the nose, mouth, or eye. e.g. mumps, respiratory syncytal virus (RSV).
2.5 Direct Contact – Infections may be spread directly from the infected person by skin to
skin contact e.g. impetigo, syphilis or indirectly via contaminated equipment.

5 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
2.6 Indirect contact – cross infection that occurs when there is no direct human-to-human contact. Infection spreads from contaminated surfaces or objects, or to vectors such as mosquitoes, flies, mites, fleas, ticks, rodents or dogs.
2.7 Ingestion-(faecal oral) - Food or water becomes contaminated with faeces from an infected person this is then ingested by another person (e.g. they do not wash their hands after going to the toilet and then prepare food for others) e.g. Salmonella, Norovirus.
2.8 Blood and body fluids - Body fluids containing an infectious agent e.g. HIV, enters
another person’s body via contact with the mucous membranes (eyes, mouth, vaginal, anal passage), inoculation or through broken skin.
3. Process
3.1 SOURCE ISOLATION
3.1.1 Standard Precautions - Since every service user is a potential infection risk, it is
essential that standard precautions are applied to all service users at all times. (Refer to the Standard Precautions and PPE Appendix 5 of the Trust Infection Prevention and Control Policy). In addition to standard precautions, isolation precautions are also required if certain infections are known or suspected (refer to Appendix 9.3 of this document to table A-Z of Infectious Diseases).
3.1.2 Criteria for Commencing Source Isolation Before deciding to isolate a service user, careful consideration must be given to the following:
Service users clinical condition e.g. mental health, risk of falls Mode of transmission of the infection e.g. air-borne, faecal-oral route etc Degree of antibiotic resistance The availability of facilities The susceptibility of others to infection Dispersal characteristics of the service user
After consideration of the above, make a risk assessment. Document your decision and reasons for your decision. Advice on the implementation of source isolation and this risk assessment can be obtained from your Infection Control Team or refer to Appendix 9.3 of this document to table A-Z of Infectious Diseases.
3.1.3 Communication
Explain the rationale for isolation to the service user and, where possible, the duration of isolation anticipated. Where available provide a service user information leaflet.
Place a Source Isolation notice on the door of the room -DOH 2011 (refer to Appendix 9.1 of this document).
Record in the service user's notes that isolation has been commenced and the reason why.
Revise the nursing care plan accounting for infection control precautions to be maintained by staff, service user and visitors.
Inform the Infection Control Team that there is a service user in isolation.
Check whether the service user has a ‘Notifiable Disease’ and if the so follow 3.1.21 of this document.

6 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Consider whether people entering the room should be immune to the service user's disease (important for rubella, chicken pox and tuberculosis).
Inform the Housekeeping Department (Facilities) and request isolation room cleaning (see Appendix 9.4 of this document)
3.1.4 Accommodation
The most effective form of isolation is a single room with a self-contained toilet and its own hand basin. This should always be the first choice for placement of an infected service user (DOH 2011)
Where a single room is not available service users with the same infection or colonised with the same micro-organisms may be nursed in an identified designated area (Cohort nursing). This is provided that they are not infected with other potentially transmissible micro-organisms and the possibility of re-infection with the same organisms is minimal. When cohorting service users with similar infections ensure physical separation from other non-infected service users and where possible that care for cohorted service users is by designated staff that are not caring for other non-infected service users (DOH 2011)
Ensure that appropriate equipment is available
Inside the room / cohort area: Outside the room / cohort area
Hand washing sink stocked with liquid soap & paper towels
Orange plastic waste bag in a foot-operated metal bin
Service users dedicated commode if no en suite facilities
Ensure that mattresses and pillows in hospital /clinics have wipeable covers.
Where possible equipment should be dedicated to that service user and remain in the room, e.g. stethoscopes, sphygmomanometer , tourniquet
Alcohol gel/rub is available
Water soluble (alginate-stitched) bags (for linen)
Sharps Bin (if safe to leave within room)
Ensure doors are kept closed (as appropriate) It is recognised that some situations eg with confused or clinically unstable service users this may not be possible (DOH 2011)
Remove non-essential equipment
Avoid fans
Source Isolation notice on door (refer to Appendix 1A)
Disposable aprons (yellow)
Non-sterile disposable gloves
Service user's charts
Alginate bags for infected linen (for double-bagging linen)
Alcohol gel/rub
Dedicated colour coded bucket and mop handle (often kept in housekeeping cupboard)
NB The mental health of the service user may dictate that it is unsafe to store some of this equipment within or outside the room. In this case staff should store such equipment in a locked cupboard and collect it before entering the isolation room/area. Always undertake a risk assessment.
3.1.5 Hand washing/decontamination
Hand decontamination (with alcohol gel or soap and water), must always be practised before entering and on leaving the isolation room/ area. In addition to this wash hands thoroughly with liquid soap and running water after removal of disposable gloves/apron, before leaving the isolation room/area (DOH 2011).

7 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
In areas where soap and water are not available within the room eg certain adult mental health wards, use alcohol hand gel to decontaminate hands in place of soap and water.
Staff and visitors must pay close attention to good hand hygiene at all times. Ensure the service user is informed about the importance of hand hygiene and provide assistance if the service user cannot manage their own hand hygiene.
For further information and indications for hand hygiene, not directly related to isolation, please refer to the Hand Hygiene Appendix 6 of the overarching Trust Infection Prevention and Control Policy
3.1.6 Protective Clothing
Ensure arms are ‘bare below the elbows’. If ties are worn they should be tucked in or removed. If contact with blood or body fluids is likely, personal protective clothing must be worn as part of standard precautions (refer Standard Precautions and PPE Appendix 5 of Trust Infection Control Policy). In addition to this, when in the isolation room /area:
Staff must wear disposable plastic yellow aprons when in direct contact with the service users, their immediate environment or equipment. Aprons should be put on before entering the room/area and removed before leaving the room/area.
Non-sterile, disposable gloves are needed when there is likely to be contact with the
service user or their immediate environment or equipment. Gloves must be put on before entering the isolation room/area and removed before leaving the isolation
room/area
After removing gloves and aprons, wash hands thoroughly with soap and water before leaving the room as hands often become contaminated in the process of removing gloves (EPIC 2014). In areas where soap and water are not available within the room eg certain adult mental health wards, use alcohol hand gel to decontaminate hands in place of soap and water.
Goggles/visors/fluid repellent face masks will be required if splashing with body fluids or generation of aerosols is likely (refer to Standard Precautions & PPE Appendix 5 of Trust Infection Prevention and Control Policy). A filtering face piece is required for a minority of infections e.g. suspected, influenza, SARS or drug resistant tuberculosis, meningococcal meningitis (Refer to Appendix 9.3 in this document Table of A-Z of Infectious Diseases, or contact the Infection Control Team for advice) .
Protective clothing should be worn for the intended purpose and then removed inside the room/isolation area (remove gloves before apron). It should never be worn when visiting another ward / area e.g. linen cupboard - except when disposing of a bed pan (refer to Body Fluid Management section in this appendix see 3.1.13). First remove gloves, then apron and finally face/eye protection if worn.
3.1.7 Waste Management
Discard all waste from isolation room/area into orange hazardous waste bag (DOH 2013).
Double bagging not required.
Ensure bags are securely tied (using swan neck tie), labelled and disposed of when ¾ full.
Bins MUST be lidded, foot operated, wipeable and in good working order and fire-retardant.

8 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
3.1.8 Linen Management
Used linen should be handled with a minimum of agitation, never hugged to your body or left on the floor.
Treat all used linen in the isolation area as infected. (i.e.) place in a water soluble (alginate) bag inside a white outer laundry bag (DOH 2011)
Secure laundry bags when ¾ full using a ‘swan neck’ tie.
Service users’ clothing which is washed on site should be washed separately on the hottest wash the material can withstand.
3.1.9 Sharps
If it is not safe to store a sharps bin in the isolation room, staff must take sharps bins into the rooms when required, for disposal of sharps at the point of use.
3.1.10 Dedicated Equipment
Keep equipment to a minimum/essential items only to reduce the risk of cross-infection.
Whenever possible use disposable items or items that are non-porous and easily decontaminated.
If dedicated equipment cannot be used decontaminate equipment appropriately as indicated by the manufacturer before use on other service users.
Staff should not use their own personal equipment in isolation rooms e.g. stethoscopes.
3.1.11 Visitors
Visitors should report to nursing staff before entering isolation rooms if they have not received advice about preventing spread of infection. In some instances visitors will be discouraged.
Visitors need to be advised to wash their hands before entering and leaving the service users room.
Protective clothing is generally not necessary (see Appendix 9.6: Personal Protective Equipment (PPE) for Relatives & Visitors).
In some instances (e.g.) chicken pox/shingles/TB visitors may need to be restricted – contact the Infection Control Team for further advice.
If they are visiting more than one service user in the hospital, they should visit non infected service users first, refer to the Infection Control Team for advice.
Where possible, visitors should be restricted to a minimum whilst isolation is in progress.
Discourage visiting by the very young, elderly or infirm, where possible. 3.1.12 Crockery/Cutlery
Disposable crockery/cutlery is not required unless advised by Infection Control Team in exceptional circumstances.
Crockery/cutlery must be washed in hot water in the usual manner in central washing up facilities. The combination of hot water and detergents used in hospital dishwashers is sufficient to decontaminate dishes, glasses, cups and eating utensils.
When collecting water jugs and glasses from an isolation cohort it is advisable to use a “buddy system”. The nurse working within the bay collects up the dirty jugs in the bay and then hands out them out to the housekeeper outside the bay, who is waiting with a trolley. The dirty jugs can then be transported to the kitchen before they are placed in the dish washer. Conversely clean jugs and glasses can then be passed from a trolley outside the bay entrance to the nurse working in the closed bay. This avoids the housekeeper having to don personal protective clothing. The housekeeper should wash hands immediately after handling used jugs/

9 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
glasses/crockery and cutlery and wipe down the trolley with detergent and hot water or a sanitizing wipe.
3.1.13 Body Fluid Management
Ideally a toilet should be dedicated for the service users’ sole use. If this is not available a separate bedpan/urinal/commode should be labelled and left in the service user’s room.
Gloves/aprons must be worn when handling body fluids (e.g.) urine, excreta, secretions and blood (refer to Standard Precautions and PPE Appendix).
No hand sluicing/chemical decontamination of bed pans or urinals is recommended, they should be placed directly into the washer disinfector or macerator.
If the macerator or bedpan washer breaks down, use pulp products only and empty them down the toilet whilst wearing protective clothing. Place used pulp products into an orange bag and inform Facilities staff that more frequent waste collections are required.
Bedpans / vomit bowls / urinals must always be covered before leaving the room and the nurse must wear a disposable yellow plastic apron and disposable gloves. The bedpan / vomit bowl / urinal must be disposed of immediately in the macerator/washer. When this is done the nurse can remove protective clothing and dispose of as hazardous waste and decontaminate hands.
Spillage of blood and blood stained body fluid must be promptly decontaminated (refer to Standard Precautions & PPE Appendix 5 of Trust Infection Prevention and Control Policy).
3.1.14 Service Users Notes/Charts
Keep notes/charts outside the isolation room that are usually kept by the bedside to prevent unnecessary entries into the isolation room/area
3.1.15 Environmental Cleanliness
Daily cleaning
Daily cleaning is essential to reduce dust and prevent the accumulation and growth of micro-organisms. Dust particles are mainly skin scales, respired droplets and fibres from clothing.
Cloths must be single use and discarded after each use
Yellow colour coded bucket, mop handle and cloths to be used in isolation room/area.
See Appendix 9.4: Cleaning of an Isolation Room/Area for more detailed instructions for daily cleaning of isolation rooms.
Final (Terminal) Cleaning
Cleaning is essential when the service user no longer requires isolation nursing. The room, bed and other fixtures and fittings must be thoroughly cleaned after discharge of an infectious service user or if the service user no longer needs isolation precautions.
See Appendix 9.5: Final (Terminal) Clean of an Isolation Room/Bedspace for more detailed instructions for terminally cleaning isolation rooms and the documentation that must be signed by both Housekeeping staff and nursing staff when the final isolation room/bed space cleaning has been completed. It is the responsibility of the nurse in charge to ensure that the standard of final cleaning is checked.
3.1.16 Movement of Service users
Limiting service user movement to other wards and departments reduces the risk for further transmission (refer to Outbreak of Infection and Major Outbreak Appendix 8 of the Trust Infection Prevention Policy).

10 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Inform person in charge of the receiving department of infection and precautions required.
Cover any infectious lesions.
Protective clothing is not generally necessary when transporting service users with infections on their bed, trolley or wheelchair unless you have direct contact with the patient.
Disposable gloves and yellow aprons should be worn if the porter has direct contact with the service user eg when helping them in or out of the wheel chair. Gloves and aprons must be disposed of as hazardous waste into an orange bag, when direct contact with the service user has finished.
Clean your hands after touching the service user or their linen.
Wheelchairs/trolleys must be wiped down with a Clinell wipe before use on another service user.
3.1.17 Visits to Other Departments
Check appendix 3.1.21 of this appendix– Avoid visits to other Departments for infections marked as ‘High Priority for side room’ unless the visit is essential.
Service users in isolation should be seen at the end of the working session whenever possible if clinically safe to do so.
Staff coming into direct contact with the service user should wear disposable gloves/aprons. Discard as hazardous waste after use and wash hands.
Minimise equipment and staff contact with the service user as much as possible. Isolated service users should be taken directly to and from isolation and not left in waiting areas.
Any linen used for the service user must be treated as infected i.e. place in an alginate bag and then inside a white laundry bag.
Clean surfaces, with which the service user has had direct contact, with detergent wipe e.g. Clinell sanitising wipe (for decontamination of a body fluid refer to Standard Precautions & PPE Appendix 5 of Trust Infection Prevention and Control Policy)
3.1.18 Last Offices
In the event of death observe the same infection control precautions taken while the service user was alive.
Requirements of body bag depends on the infection – refer to the Care of the Deceased in Relation to Infection Control Appendix 19 of Trust Infection Prevention Policy for precautions after death. (Lymington Hospital uses a thin body bag in place of a sheet for last offices. This does not replace the heavy duty body bag required for high risk infections).
Inform the Senior Mortuary technician to ensure the body is handled correctly. 3.1.19 Ward Closure – Refer to Ward Closure Appendix 11 of the Trust Infection Prevention
Policy 3.1.20 What to do if you Can Not Isolate
If a service user cannot be isolated ( e.g. no isolation room available, their clinical care would be compromised or their mental health condition makes isolation unsafe or very difficult) please document the reason for failure to isolate in the service users notes and contact the Infection Prevention Team for advice on how best to limit the risk. MRSA positive service users - if clinically unsafe to isolate the service user inform the Infection Control Team, document your risk assessment and continue isolation precautions in the bay. Do not close the rest of the bay but do seek advice from the infection control team/manager on call if considering service users for admission to the bay with indwelling medical devices or wounds.

11 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Clostridium difficile toxin (CDT) positive service users – isolation of these service users is a high priority. If unable to isolate service user with CDT diarrhoea in a side room, inform the infection control team, document your risk assessment and continue isolation precautions in the bay. Close the bay to admissions
3.1.21 Reporting Notifiable Diseases
There are 30 diseases which are statutory notifiable under the revised Public Health (Control of Disease) Act 1984 and the Health Protection (notification) Regulations 2010.
Responsibility for Notification Doctors in England and Wales have a statutory duty to notify a ‘Proper Officer’ of the Local Authority (usually Consultant in Communicable Disease Control-CCDC at local Health Protection Team) of suspected cases of certain infectious disease. The responsibility of notification rests with the attending Registered Medical Practitioner looking after the service user.
When As soon as possible after confirmed or suspected diagnosis of a notifiable disease so that Public Health action can be taken immediately. If the clinical diagnosis is subsequently disproved then the notification can be de-notified by informing the Health Protection Team How to Notify
Complete the Registered Medical Practitioners Notification Form (refer to Appendix 9.7).
Record notification in the service user’s notes.
Notification should be sent/faxed immediately to: Contact details of Wessex Health Protection Team are: Unit 8, Fulcrum 2, Solent Way, Fareham, Hampshire, PO15 7FN Tel: 0845 055 2022 Out of hour’s advice For health professionals: To contact a public health professional in an emergency out of hours; in the evenings, at weekends or during bank holidays, please phone: 0844 9670082
Email: [email protected]
Notifications sent to the Health Protection Unit must be made in a secure manner. This may be by telephone, letter, encrypted email or to a secure fax machine.
Reason for Notification The purpose of notification is to ensure epidemiological investigations, contact tracing, treatment of contacts (when necessary) and preventative measures can be instituted as soon as possible. Extra measures may be required according to the service user’s occupation as in the case of health care workers, food handlers and teachers. Notification also provides data for national surveillance of infectious diseases.

12 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Diseases Notifiable to the Proper Officers under Health Protection (Notification)
Regulations 2010
Acute encephalitis Acute infectious hepatitis Acute meningitis Acute poliomyelitis Anthrax Botulism Brucellosis Cholera Diphtheria Enteric fever (typhoid or
paratyphoid fever) Food poisoning Haemolytic uraemic syndrome
(HUS) Infectious bloody diarrhoea Invasive group A streptococcal
disease Legionnaires’ Disease
Leprosy Malaria Measles Meningococcal septicaemia Mumps Plague Rabies Rubella SARS Scarlet fever Smallpox Tetanus Tuberculosis Typhus Viral haemorrhagic fever (VHF) Whooping cough Yellow fever
As of April 2010, it is no longer a requirement to notify the following diseases: Dysentery, Leptospirosis, Ophthalmia neonatorum, Relapsing fever and Viral hepatitis. These and other diseases that may present significant risk to human health may be reported under Other significant disease category
HIV/AIDS is not a notifiable disease, but doctors are urged to report in a voluntary confidential scheme. Advice about the reporting of cases may be obtained locally from the CCDC or Consultant in Genito-Urinary Medicine.
HIV/AIDS cases should be reported on a special HIV/AIDS form in strict medical confidence to the Director, PHLS Communicable Disease Surveillance Centre, 61 Colindale Avenue, London NW9 5EQ, Tel: 0208 3277406.

13 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
3.1.22 Checklist for Entering and Leaving the Room
Before entering the source isolation room/areas
Remove white coats, jackets or outside clothing
Collect all equipment needed to avoid entering and leaving the infected area unnecessarily.
Ensure arms are bare below the elbows to facilitate hand hygiene.
Clean hands with alcohol rub/gel.
Put on yellow disposable plastic apron and disposable gloves (if airborne infection, refer to Appendix 9.3: A-Z Infectious Diseases and check whether a filtering face piece (face mask) is required).
If body fluid contact likely wear personal protective clothing in accordance with the Standard Precautions & PPE Appendix 5.
Inside the source isolation room/area
Perform service user task (change disposable gloves, and wash hands if they become contaminated during a procedure).
Do not sit on the bed.
Do not touch the service user or anything else in the room unnecessarily.
Before leaving the source isolation room/area
Remove all protective clothing and discard into orange hazardous waste bin (remove gloves first, followed by apron, and followed by eye/face protection if used.
Wash hands with soap and water (alcohol gel if no hand washing facilities in room).
Outside the room If a facemask has been worn to protect from airborne infection e.g. pandemic flu, remove mask outside the room and discard into an orange waste bag for hazardous waste. Wash hands.
Clean hands with alcohol rub to remove pathogenic organisms acquired from such items as the door handle.

14 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
3.2 PROTECTIVE ISOLATION
3.2.1 Criteria For Commencing Protective Isolation – Protective isolation is required to
protect service users with reduced natural immunity and/or neutropaenia (blood neutrophils of less than 0.5 x109/l)
3.2.2 Getting Started
Explain the need for isolation to the service user.
Remove any unnecessary equipment from the room.
Contact the Housekeeping Department to ensure the room has been thoroughly cleaned with detergent and hot water, and no visible dust has gathered.
Place a blue ‘protective isolation sign’ on the door (see Appendix 9.2).
Document your reason for starting protective isolation, date started. 3.2.3 Outside the Room
Protective isolation notice
Blue (service user care) single use plastic aprons
Service user charts
Alcohol rub
Disposable gloves 3.2.4 Inside the Room
Lidded, foot operated sack holder for waste containing an orange bag for hazardous waste
Sterile gloves ( for aseptic procedures and touching susceptible sites)
Non sterile disposable gloves
Alcohol hand rub
A sink with soap and water and paper towels 3.2.5 Hand Hygiene - Staff and visitors must pay close attention to good hand hygiene at all
times. Ensure the service user is informed about the importance of hand hygiene and provide assistance if the service user cannot manage their own hand hygiene.
3.2.6 Staff Health - Staff with any kind of infection must be excluded from caring for this
service user. Staff who are nursing service users with infections i.e. source isolation should avoid nursing service users in protective isolation during the same shift
3.2.7 The Room - Service users should be nursed in a single bedded room containing only
essential furniture. The door should remain closed except for entry and exits. Fittings should include a hand wash basin and ideally en-suite facilities and a foot operated bin. Side rooms must be cleaned before the service user is admitted including clean mop head.
3.2.8 Protective clothing – Plastic single use aprons should be worn by staff to protect the
patient from the many microorganisms being transferred from their uniforms. If doctors wear white coats these should be removed before entering.
Non-sterile gloves must be worn by staff for contact with body fluids as per standard infection control precautions. Sterile gloves must be used when handling invasive devices e.g. Hickman lines or aseptic technique procedures. No masks required. After use remove protective clothing outside the room, discard the room and wash hands.
3.2.9 Service user hygiene – The service user’s personal hygiene needs to be scrupulous to
minimize the risk of infection. The service user may require encouragement and assistance to maintain this, as they may feel fatigued. Bottles of shower gel or soap

15 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
should be used, avoid bars of soap. Dental hygiene must be performed at least twice a day. When shaving an electric razor should be used to minimize the risk of cuts. This should be the service user’s own shaver and not a communal one. Day and nightwear should be changed daily and when soiled. This is to prevent the transfer of organisms
3.2.10 Linen - No special precautions. Change bed linen daily and when soiled to prevent
transfer of organisms. 3.2.11 Crockery - No special precautions. Wash all cutlery and crockery in dish washer only.
3.2.12 Food/drink – food is a potential source of infection and good food hygiene practice is essential. A clean diet must be provided. This includes thoroughly cooked foods, and canned foods/drinks. Professional catering using a cook chill service is acceptable but avoid any reheating of food at ward level in a microwave oven. Avoid foods that are known to have high bacterial counts e.g. fresh cream, shellfish, ice, cold meat, raw or lightly cooked eggs, soft cheeses, pâté, raw vegetables, salads and unpeeled fruit. Infection from ice can also occur from contamination within the ice maker or from staff, service users or visitors. Water should be pre-boiled or sterile from pharmacy (not bottled water)
3.2.13 Waste - No special precautions. Ensure waste bags are not allowed to accumulate. 3.2.14 Equipment - Use disposable wherever possible. All re-usable equipment for use in the
room must be cleaned in accordance with the Decontamination of Medical Devices Appendix.
3.2.15 Visitors - Visitors with infections must be excluded. All visitors must wash hands on
entering and leaving the room. There is no need for visitors to wear single use gloves and aprons when visiting unless directly involved in care giving activities. Visitors must leave outer coat outside the room. By limiting visitors to a few key visitors, exposure to potential pathogens can be reduced. Similarly children (unless close family members) should avoid visiting.
3.2.16 Flowers - Flowers and plants have not been directly linked to infection in
immunocompromised service users, however they could potentially be a reservoir for gram negative bacteria or fungal spores. Therefore pot plants are inappropriate. If fresh flowers are to be kept in the room the water must be changed daily - not in the cubicle wash basin
3.2.17 Cleaning - All protective isolation rooms must be cleaned before other areas to prevent cross infection. Equipment and supplies (including cleaning equipment) to be kept for the sole use of the service user in protective isolation. Surfaces and furniture must be damp dusted daily using detergent and water then dried using disposable cloths and paper towels. Mop floor daily using detergent and water. Launder mop head after each use. Clean and dry mop handle and bucket after each use.
3.2.18 Estates - Notify the Infection Prevention and Control Team if building works are planned for any area in the vicinity of the isolation room.

16 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Entering and leaving protective isolation
Before entering the protective isolation room/
Remove white coats, jackets or outside clothing (ideally hang them on a hook outside the room). Ensure hands are bare below the elbow.
Collect all equipment needed, to avoid entering and leaving the area unnecessarily. Ensure all equipment is clean before visiting the protective isolation room.
Consider if you have any symptoms of infection, do not enter the room if you could be infectious.
Ensure arms are bare below the elbows to facilitate hand hygiene.
Put on white or blue (general service user care) disposable plastic apron to protect organisms being transferred from clothing.
No face mask required (other than as part of standard precautions).
Wash hands with soap and water or clean hands with alcohol rub/gel if visibly clean.
Inside the protective isolation room/area
Put on sterile disposable gloves if you are performing an aseptic clinical procedure or touching a medical device. Non sterile gloves may be required as part of standard precautions if body fluid contact likely.
Change disposable gloves, and wash hands if they become contaminated during a procedure.
Do not sit on the bed.
Do not touch the service user or anything else in the room unnecessarily.
Limit the number of people entering the room eg Doctors rounds
On leaving the protective isolation room/area
Remove all protective clothing and discard into orange hazardous waste bin outside the room
Wash hands with soap and water or alcohol gel
Ensure the door is closed.
Adapted from Mallet and Dougherty 2011
4. Training
Refer to the Trust Training Needs Analysis (TNA) in IP&C Policy.
5. References
Public Health (Control of Diseases) Act 1984 available on http://www.opsi.gov.uk/RevisedStatutes/Acts/ukpga/1984/cukpga_19840022_en_1
Health Protection (Notification) Regulations 2010 (SI2010/659) http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/NotificationsOfInfectiousDiseases/ReportingProcedures/

17 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Department of Health (2009) The Health and Social Care Act 2008: Code of Practice for the Prevention and Control of Healthcare Associated Infections. London: DH. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_110288
Department of Health (2011) Isolating service users with healthcare associated infection A summary of best practice , London DH http://hcai.dh.gov.uk/files/2011/03/Document_Isolation_Best_Practice_FINAL_100917.pdf Mallet, J and Dougherty, L (2011) The Royal Marsden, Manual of Clinical Nursing Procedures, 8th Edition, Blackwell Science, Oxford HSE (2005) Controlling the Risks of Infection at Work from Human Remains: London HSE available on http://www.hse.gov.uk/pubns/web01.pdf
Department of Health (2013) Health Technical Memorandum 07-01: Safe management of healthcare waste available on https://www.gov.uk/government/publications/guidance-on-the-safe-management-of- healthcare-waste

18 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.1: Isolation in Progress– Source Isolation
Appendix 1a: Isolation in progress– source isolation
Appendix 1b: Isolation in progress notice – protective isolation
ALERT
INFECTION CONTROL PRECAUTIONS
ALL STAFF MUST
Remove white coats, arms bare from elbows down
Decontaminate hands before entering and leaving the
room
Wear single-use apron and gloves when dealing with
blood / body fluids and / or direct service user contact
Discard protective clothing in room in an orange bag
Wash hands after removing gloves
Unless advised, masks are not required
VISITORS
Speak to the nurse in charge before entering room
Use alcohol hand rub before entering and wash hands
with soap and water before leaving the room
The use of gloves, aprons and masks is not routinely
necessary
PLEASE ENSURE THE DOOR REMAINS
CLOSED AT ALL TIMES (if safe to do so)
Contact IPCT for further advice
protecting service users, staff and visitors

19 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
ALERT
INFECTION CONTROL PRECAUTIONS
DO NOT ENTER this room if you are unwell or have an infection or you have been in contact with someone who has an infection
ALL STAFF MUST
Remove white coats, arms bare from elbows down
Decontaminate hands before entering and leaving the
room
Wear single-use apron and gloves when having direct
service user contact
Discard protective clothing and clean hands on leaving
the room (outside the room)
Unless advised, masks are not required
VISITORS
Speak to the nurse in charge before entering room
Visitors should be restricted to close relatives and friends
Wash hands or use alcohol hand rub before entering and
leaving the room
The use of gloves, aprons and masks is not routinely
necessary
PLEASE ENSURE THE DOOR REMAINS CLOSED AT ALL
TIMES
protecting service users, staff and visitors
Appendix 9.2: Isolation in Progress– Protective isolation

20 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.3: A-Z of Infectious Diseases
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
Adenovirus Airborne Direct contact
Medium Source isolate resolution of symptoms
No No
Anthrax: Pulmonary
Inhalation of spores High Source isolate. Needs transfer to a negative pressure room or Infectious Disease Hospital Urgently
Yes Shoe covering, single use gown and Mask Face Respirator class FFP3 Laboratories must handle specimens in CL3 if anthrax is suspected so contact local lab, mark specimen as ‘high risk’, wear gloves when sampling Rare and Imported Pathogens Laboratory (RIPL) at HPAPorton (Tel: 01980 612100)
Anthrax : Cutaneous Direct contact with wound
No No Yes Gloves and aprons as part of standard precautions for direct contact with wound. Mark any specimens as ‘high risk’ and contact your local laboratory.
Bronchiolitis Droplet and direct contact with secretions
Medium Source isolate while symptomatic. No No (use surgical mask for sputum inducing procedures)
Campylobacter
Ingestion food or faeces
Medium Source isolate until 48 hours after cessation of symptoms.
Yes No
Carbapenemase-producing Enterobacteriaceae (CPE)
Direct and contact with a CPE carrier or their immediate environment
High Who to Screen/Assess on Admission 1.Patients admitted to a physical health community hospital with a known positive history of CPE. 2. Patients admitted to a physical
No No
1317140378646 Toolkit for Early Detection ACUTE 2013.pdf

21 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
health community hospital who are known to be a contact (ie spent time in an open ward or bay) of a patient with a positive result for CPE. 3.Patients admitted to a physical health community hospital directly from an overseas healthcare facility. Action Confirmed cases: Patients transferring into a physical health community hospital who are known to have a positive diagnosis of CPE will be placed in source isolation and managed as per A3 of PHE toolkit. Contacts: Patients admitted to a physical health community hospital who are known to be a contact (ie spent time in an open ward or bay) of a patient with a positive result for CPE will be managed as per A4 of the toolkit Suspected cases from overseas: Patients admitted to a physical health community hospital directly from an overseas health facility will be immediately placed in isolation and managed as per A2 and A3 of the toolkit.
Cellulitis Direct contact High Source isolate if caused by Group A Strep or drug resistant organism
No No

22 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
and indirect contact
eg MRSA (see relevant sections)
Chickenpox
Contact with vesicular fluid Airborne.
High Source isolate until lesions are dry and scabbed.
No Exclude staff non immune to chicken pox from caring for this patient. Inform Infection Prevention Team No
Clostridium difficile Contact faecal –oral Indirect contact from contaminated environment
High if symptomatic
Source isolate until 48 hours after cessation of symptoms. Negative stool samples are not required.
No No
Conjunctivitis
Direct and indirect contact with discharges from an infected eye
Medium Isolation is not required unless viral eg Adenovirus (see above).
No Gloves and aprons as part of standard precautions for direct contact
Cryptosporidiosis
Faecal-oral spread. Yes Source isolate until 48 hours after symptoms have resolved.
Yes No
Cytomegalovirus
Transplacental Direct contact with infected body fluids Sexual Transplant/blood transfusion
- Isolation is not required except if in neonatal area
No No
Diarrhoea and or vomiting (undiagnosed)
Various-usually faecal oral
High Source isolate until 48 hours after symptoms have resolved. If viral gastroenteritis is suspected in a bay setting, cohort all of the service users in the bay together to prevent spread.
- No
E.coli 0157 Faecal-oral spread and via
High Source isolate until 48 hours after symptoms have resolved
Yes No

23 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
contaminated food/water.
Extended Spectrum Betal-Lactamases ESBLs
Contact High if incontinent or in leaking wounds Medium otherwise
Source isolate until discharged. No need to keep taking clearance samples.
No No
Enteric Fever see Typhoid fever German Measles See Rubella Glandular Fever
Close contact with saliva
- Not required No No
Glycopeptides resistant enterococci (GRE)
Direct and Indirect Contact
High Source isolate until no longer colonised/discharged
No, Part of National surveillance
No
Hand foot & mouth Coxsackievirus
Droplet from an infected person
Medium Source isolate until resolution of fever
No No
Hepatitis A Food or water contaminated with faeces from infected person. Direct spread from infected person.
High Source isolate until 1 week after onset of jaundice or 10 days after onset of first symptoms.
No No
Hepatitis B & C Close physical contact with the blood or body fluids of an infected person
Low Not required unless actively bleeding.
Yes Standard precautions only
Herpes simplex
Direct contact with lesion, exudates or
- Not usually , only required if extensive lesions or
No
No

24 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
Cold Sores Genital herpes Neonatal herpes
saliva. Sexually transmitted. During pregnancy or at delivery.
neonatal/chemotherapy service users nearby
No No No
Human fleas (very uncommon)
Contact with infected bedding and clothing
High Until service user bedding and clothes have been treated
No Recommend limiting visitors to those who have already had contact until treated. Wear disposable gown , plastic aprons and disposable gloves for all contact and for cleaning until treated. NB No isolation required for animal fleas instead treat animals and infected environment.
Human Immunodeficiency virus (HIV)
Close physical contact with the blood or blood stained body fluids of an infected person
- No need to isolate. No, but part of national surveillance.
Standard precautions only
Impetigo Direct contact with secretions from an infection wound Indirect contact with contaminated environment/items eg fabric towels
High Source Isolate until 24 hours after treatment with antibiotics has started or until sores are healed
No No
Influenza (including A and Airborne High Source isolation until asymptomatic Yes Non-pandemic influenzae- surgical

25 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
B) and 5 days minimum from onset of symptoms. If febrile assume infectious
mask ,immunised staff to care for service user Pandemic influenzae – use eye protection, disposable gown and FFP3 mask if performing sputum producing procedure- otherwise wear surgical mask and risk asses need for eye protection if working within 1 m of the service user. See Pandemic Influenza Policy
Lice (body) .
Contact Source isolation until service user is washed and clean clothes put on. Clothes should be washed separate from others at 600C.
No All persons entering room should wear disposable gloves and aprons until service user bedding and clothing is treated.
Lice (Head) Contact (head to head and via shared combs, head wear)
- No but infectious until successfully treated
No Gloves and aprons for direct service user contact
Lice (pubic) Contact (usually sexual)
- No No Gloves and aprons as part of standard precautions
Malaria Vector Transmitted by mosquito bite
- No need to isolate. Yes No
Measles Coughing and sneezing. Also direct contact with the nose/throat secretions of an infected person
High
Source isolate until 4 days after onset of rash
Yes Only immune staff to care for service user
Meningococcal meningitis/septicaemia
Direct contact with respiratory droplets or secretions.
Medium
Source isolate until 24 hours of effective antibiotics have been administered.
Yes Surgical face mask until 24 hours of appropriate antibiotic therapy has been given.
26 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
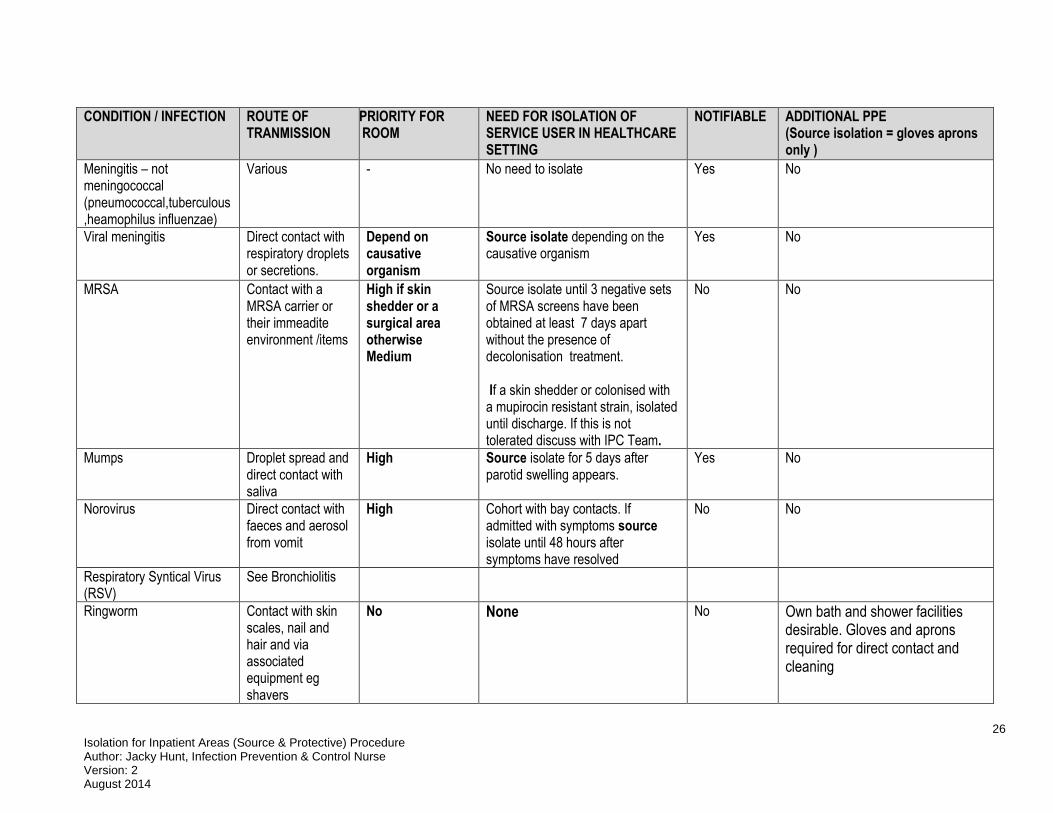
Meningitis – not meningococcal (pneumococcal,tuberculous,heamophilus influenzae)
Various - No need to isolate Yes No
Viral meningitis Direct contact with respiratory droplets or secretions.
Depend on causative organism
Source isolate depending on the causative organism
Yes No
MRSA Contact with a MRSA carrier or their immeadite environment /items
High if skin shedder or a surgical area otherwise Medium
Source isolate until 3 negative sets of MRSA screens have been obtained at least 7 days apart without the presence of decolonisation treatment. If a skin shedder or colonised with a mupirocin resistant strain, isolated until discharge. If this is not tolerated discuss with IPC Team.
No No
Mumps Droplet spread and direct contact with saliva
High Source isolate for 5 days after parotid swelling appears.
Yes No
Norovirus Direct contact with faeces and aerosol from vomit
High Cohort with bay contacts. If admitted with symptoms source isolate until 48 hours after symptoms have resolved
No No
Respiratory Syntical Virus (RSV)
See Bronchiolitis
Ringworm Contact with skin scales, nail and hair and via associated equipment eg shavers
No None No Own bath and shower facilities desirable. Gloves and aprons required for direct contact and cleaning

27 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
Salmonella Faecal oral and consuming infected food/water
High Source isolate until 48 hours after the resolution of symptoms.
Yes No
Scabies
Prolonged direct skin contact with the infected person, and sharing sheets and clothes.
Low unless Norwegian Scabies which is high
Source isolation depending on setting, isolate until first treatment with scabicide is complete. Treat again in 7 days with scabicide. Service Users with Norwegian Scabies must be isolated in own room for duration of stay in in-patient areas
No Report clusters to the CCDC
Gloves and aprons/gowns for all direct contact until successfully treated.
Shingles Caused by reactivation of latent VZV. Vesicle fluid . If individual is not immune to varicella zoster virus they can get chickenpox (varicella) from touching the fluid in a shingles (zoster) vesicle
Medium Source isolation until lesions dry and scabbed.
No Gloves and aprons for direct contact until lesions are dry. Exclude staff non immune to chickenpox
Shigella
Faecal oral High
Source isolate until 48 hours after the resolution of symptoms
Yes No
Group A streptococci infection
Direct and indirect contact. Droplet
Medium
Source isolate until 24 hours after effective antibiotic treatment has started. If isolation is not achievable due to the service users health condition, commence enhanced
No No

28 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
CONDITION / INFECTION ROUTE OF TRANMISSION
PRIORITY FOR SIDE ROOM
NEED FOR ISOLATION OF SERVICE USER IN HEALTHCARE SETTING
NOTIFIABLE ADDITIONAL PPE (Source isolation = gloves aprons only )
cleaning of the ward with chlorine based disinfectant even on one case of Gp A Strep
Toxoplasmosis
Direct and indirect contact
- Isolation is not required. No
Tuberculosis open (smear positive)
Droplets and airborne spread.
High Source isolation required until 14 days of effective antibiotic treatment.
Yes No (if doing sputum inducing procedures use standard precautions- and put on fluid impermeable face/eye protection)
Typhoid and Paratyphoid Faecal oral High Source isolation required with ensuite facilities until 48 hours after the resolution of symptoms
Yes No
Multi Drug Resistant TB Droplets and airborne spread.
High Source isolate until smear negative Multidrug-resistant TB service users should be nursed in an Isolation Unit with negative pressure.
Yes Mask face respirator class FFP3
Whooping cough (pertussis)
Droplet. High Source isolate with respiratory precautions for 5 days after antibiotics have started. If antibiotics are not given isolate for 3 weeks after the onset of symptoms
Yes No Exclude non immune staff and visitors

29 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.4: Cleaning of Source Isolation Room
Daily Cleaning Procedure for a Single Isolation Room/Bed Space
1. Report to the nurse in charge before starting work to receive any special instructions
2. Collect all materials and equipment required for cleaning inside the room, including hand towels, soap, disposable cloths, clean mop head, chlorine releasing disinfectants eg Actichlor Plus tablets, damp dusting bucket, large mop bucket, yellow mop handle and mop head (and bucket for cleaning en-suite if applicable)
3. Before entering the isolation room, fill buckets with water. For each litre of cold water use one tablet.
Ensure tablets are dissolved before using. ONLY USE COLD WATER. Warm water results in the production of toxic chlorine gas.
When preparing the solution wear disposable gloves and apron and ensure good ventilation. All equipment (including buckets) is usually carried to the room on a trolley.
Chlorine based products will bleach fabrics Only personnel trained in the use of chlorine releasing agent e.g. Actichlor Plus should
use this product
4. Park the trolley just outside the room, do not take it inside the room
5. Decontaminate hands outside the room
6. Put on disposable yellow apron over uniform & disposable gloves before entering the room then enter room
7. Open window
8. Pick up any large items of rubbish & place in orange bag, including locker bag
9. Once detergent and chlorine containing agent eg Actichlor Plus tablets have dissolved in damp dusting bucket, use a yellow cloth to damp dust all surfaces e.g. bed locker, bed
frames, table tops, chairs, window ledges and bed lamp. The chlorine releasing solutions must be changed when it becomes visibly dirty. The solution should be freshly made for use for each room, and thrown away, down the
sluice after each cleaning session
10. Clean all window ledges and skirting boards
11. Wipe down all doors and handles, paying particular attention to vents. Discard yellow cloth into orange bag. Dry all surfaces using disposable paper and discard after use into orange bag.
12. Clean sink, splash backs, mirror and all fixtures and fittings with clean yellow cloth and detergent and chlorine containing agent e.g. Actichlor Plus solution
13. If en-suite present, using your bucket for en-suite cleaning to thoroughly clean shower cubicle with yellow cloth and chlorine releasing solution eg Actichlor Plus, paying attention to shower head, tiles and shower tray
14. Wipe and replenish paper towel, soap and toilet paper dispenser (if appropriate)
15. Using a yellow disposable cloth, thoroughly clean toilet using clean to dirty method. Ensure
you rinse your yellow cloth regularly 16. Discard used cloths into orange waste bag.

30 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
17. Dry mop the floor working from the furthest point towards the door. Alternatively an (exhaust filtered) vacuum cleaner can be used. Wipe the casing of the vacuum cleaner with a Clinell sanitising wipe, after vacuuming before moving to another room
18. If floor not carpeted wet mop the floor working from the furthest point towards the door. Display floor signs.
19. Leave room and shut door
20. Go directly (whilst still wearing your aprons and gloves) to the sluice area.
21. Empty floor buckets, damp dusting bucket and en-suite bucket in sluice /cleaning cupboard
sink (never use a hand washing sink or a sink in the isolation room)
22. Wash the bucket with detergent and water and rinse and dry the bucket whilst in the sluice/or if applicable decontaminate in a ward washer disinfector
23. Remove mop heads and send for laundry in a plastic bag
24. Store mop handle and buckets in the cleaning cupboard or isolation room
25. Remove disposable gloves and apron whilst still in the sluice and thoroughly wash hands using soap and water, in the hand washing sink
.
.
.
.
.

31 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.5: Infectious Terminal Clean of Isolation Room/Bay
Microfibre cleaning method Site: …………………………….. Ward/Dept: ……………………………………. Room number/name: ………………………………………………………………. Date requested: …………………………… Time requested:…………………… Requested by: ………………………………………………………………………. Requirement to remove radiator covers prior to terminal cleaning Remove if:-
Ward closure due to infection (e.g. D&V, MRSA, FLU outbreak) Single case of Clostridium difficile and C.diff carrier case if advised by IPCT On request of IPCT as part of management of a resistant organism
Removal not required if:- Bay closures due to infection e.g. D&V Single case of resistant organism e.g. MRSA or ESBL
Actions Y N Signature
Radiator cleaning if covers removed:- Estates department to be contacted in advance of infectious terminal cleaning by the nurse in charge to remove radiator covers. Estates helpline telephone number: 0300 300 3636 (Mon - Fri 08:30 – 5pm) Arrange the date and time to coincide with terminal cleaning. Estates department to replace radiator covers when infectious terminal cleaning process completed.
Cleaning of radiators: Outside & Inside (if required) Facility staff to clean using a damp disposable cloth soaked in detergent and chlorine containing solution (e.g. Actichlor Plus).
Nursing staff Responsibility (ideally nursing tasks to be completed prior to housekeeping tasks)
Actions Y N Signature
The patient must have vacated the bed space before cleaning commences.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area.
Ensure good ventilation.
The room or area should be cleared of miscellaneous items (e.g. discard magazines, used toiletries into an orange hazardous waste bag).
Remove all linen from bed and place in an alginate bag, followed by infectious outer laundry bag, and tie securely.
All disposable fittings and single use medical devices should be disposed of into an orange hazardous waste bag, e.g. oxygen tubing, suction tubing & suction drainage bags.
All reusable medical equipment must be decontaminated according to

32 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
manufacturer’s instructions. Following decontamination, remove the equipment from the area.
Cleaning: Use a detergent and chlorine containing solution eg Actichlor Plus, 1000ppm. Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actichlor Plus BS Solution Only Southern Health NHS V1.pdf
Actichlor Plus GE Southern Health NHS V1.pdf
If commode or raised toilet seat present, thoroughly clean all areas with a detergent and chlorine solution, rinse and then dry.
Thoroughly wipe the mattress, upper bed frame, bed head, bed rails, and plastic pillow cover with detergent and chlorine solution eg Actichlor Plus and dry with disposable paper towels. Discard paper towels into orange hazardous waste bag. Ensure good ventilation whilst cleaning within the room.
Clean the patient wash bowl if non-disposable with detergent and chlorine solution e.g. Actichlor Plus and dry with disposable paper towels. If bedside entertainment system present, remove headset earpiece covers and discard into orange hazardous waste bag. Arrange for cleaning and replacement earpieces.
Name of nurse (print): Date completed: Time:
Signature:
Housekeeping Staff Responsibility (Ideally nursing tasks should be completed prior to housekeeping tasks)
Housekeeping Team to use detergent and chlorine containing agent eg Actichlor Plus 1000ppm for all cleaning tasks during this procedure.
Actions Y N Signature
Before starting: report to clinical staff to receive any specific instructions.
Make up Chlorine based disinfectant solution: In the cleaning room, prepare all equipment needed.
Wearing gloves and aprons make up a chlorine solution by adding one tablet of Chlorine releasing agent e.g. Actichlor Plus to one litre of cold water.
When the tablet has fully dissolved, dose cloths and mops as per microfibre set up on trolley in yellow buckets.
NB: Only personnel trained in use of Chlorine releasing agent e.g. Actichlor Plus, should use this product.
Collect all materials and equipment: e.g. hand towels, toilet rolls, soap, pre-dosed yellow microfibre cloths or disposables & pre-dosed yellow microfibre mops, high dusting tool.

33 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Park cleaning trolley outside: Within reach of the door. Do not take the trolley inside the room.
Clean hands before entering the isolation area.
PPE: Put on single use gloves and yellow apron before entering the isolation area (discuss with nursing staff if any additional PPE is required).
Ensure good ventilation e.g. open a window
Remove dirty curtains: Place into an alginate bag, then outer infectious linen stream bag.
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique. Clean all horizontal surfaces from:- High to low Clean to dirty Top to bottom Far end of room to the door
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique.
High Dust - Damp dust all areas to hand height level regularly rinsing cloth, allow to air dry.
Bedside Lamp - Extend the lamp, damp dust all areas, return to original position, allow to air dry.
Hand held ‘nurse call’ device, careful to clean around idented button, allow to air dry.
Bedside Locker - Thoroughly clean all areas inside and outside, and allow to air dry.
Bedside Table - Thoroughly clean all areas of table top, underside & stand, allow to air dry.
Bedside Chair - Thoroughly clean all wipeable areas of chair seat, back, top, underside and legs, allow to air dry.
Bed Frame (below top frame) - Raise bed and thoroughly clean all areas of underside and stand areas working from the top to the bottom, allow to air dry.
Window Ledges - Damp dust all areas, and allow to air dry.
All Doors, Door Handles & Door Vents - Thoroughly clean all areas paying attention to hand contact surfaces, allow to air dry.
Skirting Boards - Damp dust all areas, allow to air dry.
Clinical Hand Wash Sink, Taps & Splash Back Use two cloths one for taps and dispensers the other for the Basin.
Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016).
Tiles -Thoroughly clean the area working from the outside inwards, Allow to air dry.
Mirrors - Thoroughly clean the area then dry and buff with a second cloth/disposable paper towel to remove any smears.
Bathroom facilities/ En Suite: Using a fresh cloth, clean the basin and shower cubicle paying attention to taps, shower heads, tiles and shower tray.
34 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
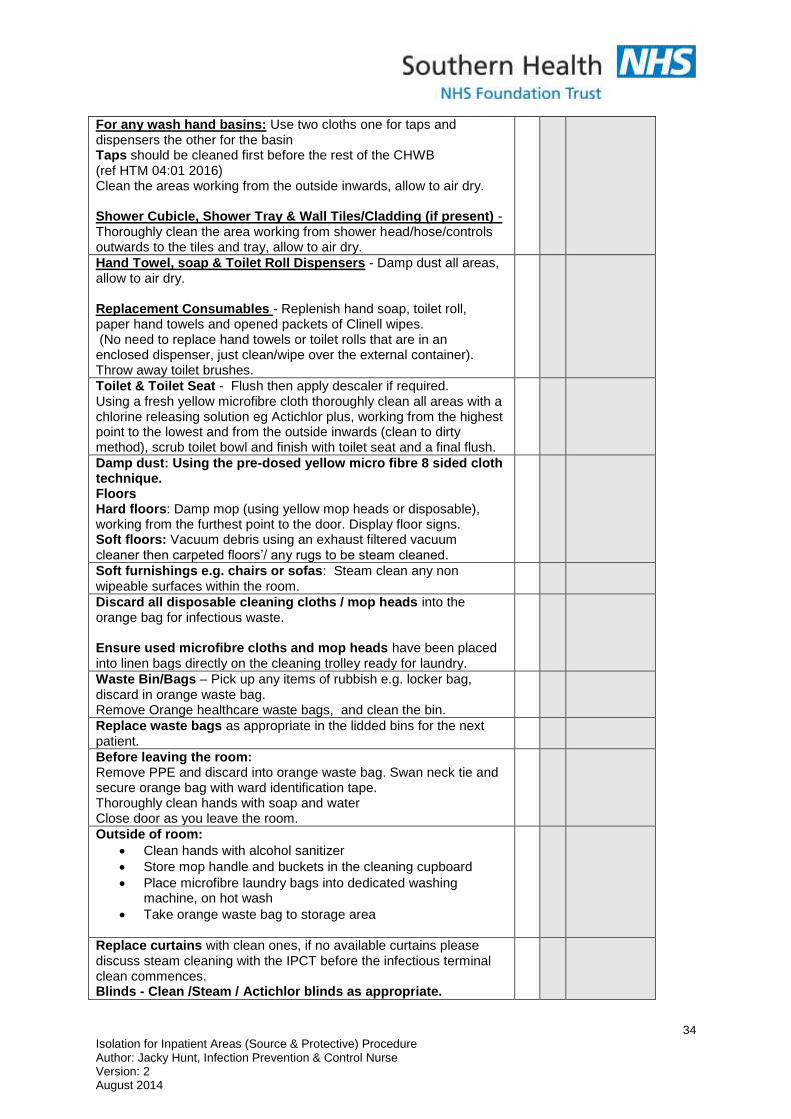
For any wash hand basins: Use two cloths one for taps and dispensers the other for the basin Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016) Clean the areas working from the outside inwards, allow to air dry. Shower Cubicle, Shower Tray & Wall Tiles/Cladding (if present) - Thoroughly clean the area working from shower head/hose/controls outwards to the tiles and tray, allow to air dry.
Hand Towel, soap & Toilet Roll Dispensers - Damp dust all areas, allow to air dry. Replacement Consumables - Replenish hand soap, toilet roll, paper hand towels and opened packets of Clinell wipes. (No need to replace hand towels or toilet rolls that are in an enclosed dispenser, just clean/wipe over the external container). Throw away toilet brushes.
Toilet & Toilet Seat - Flush then apply descaler if required. Using a fresh yellow microfibre cloth thoroughly clean all areas with a chlorine releasing solution eg Actichlor plus, working from the highest point to the lowest and from the outside inwards (clean to dirty method), scrub toilet bowl and finish with toilet seat and a final flush.
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique. Floors Hard floors: Damp mop (using yellow mop heads or disposable), working from the furthest point to the door. Display floor signs. Soft floors: Vacuum debris using an exhaust filtered vacuum cleaner then carpeted floors’/ any rugs to be steam cleaned.
Soft furnishings e.g. chairs or sofas: Steam clean any non wipeable surfaces within the room.
Discard all disposable cleaning cloths / mop heads into the orange bag for infectious waste. Ensure used microfibre cloths and mop heads have been placed into linen bags directly on the cleaning trolley ready for laundry.
Waste Bin/Bags – Pick up any items of rubbish e.g. locker bag, discard in orange waste bag. Remove Orange healthcare waste bags, and clean the bin.
Replace waste bags as appropriate in the lidded bins for the next patient.
Before leaving the room: Remove PPE and discard into orange waste bag. Swan neck tie and secure orange bag with ward identification tape. Thoroughly clean hands with soap and water Close door as you leave the room.
Outside of room:
Clean hands with alcohol sanitizer
Store mop handle and buckets in the cleaning cupboard
Place microfibre laundry bags into dedicated washing machine, on hot wash
Take orange waste bag to storage area
Replace curtains with clean ones, if no available curtains please discuss steam cleaning with the IPCT before the infectious terminal clean commences. Blinds - Clean /Steam / Actichlor blinds as appropriate.

35 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Comments from housekeeping staff
Comments from nursing staff
On completion of the Terminal Clean please sign the box below confirming that you are satisfied with the standard of cleanliness.
Ward Manager/shift leader Name: (print) Date completed: Time:
Housekeeping supervisor Name: (print) Date completed: Time:
Signature:
Signature:
Retain copies of this form:- 1. The person requesting final isolation clean must ensure that a copy is to be retained on the ward 2. One copy to be retained by Housekeeping

36 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.5: Infectious Terminal Clean of Isolation Room/Bay
Mop and Bucket cleaning method Site: …………………………….. Ward/Dept: ……………………………………. Room number/name: ………………………………………………………………. Date requested: …………………………… Time requested:…………………… Requested by: ………………………………………………………………………. Requirement to remove radiator covers prior to terminal cleaning Remove if:-
Ward closure due to infection (e.g. D&V, MRSA, FLU outbreak) Single case of Clostridium difficile and C. diff carrier case if advised by IPCT On request of IPCT as part of management of a resistant organism
Removal not required if:-
Bay closures due to infection e.g. D&V Single case of resistant organism e.g. MRSA or ESBL
Actions Y N Signature
Radiator cleaning if covers removed:- Estates department to be contacted in advance of infectious terminal cleaning by the nurse in charge to remove radiator covers. Estates helpline telephone number: 0300 300 3636 (Mon - Fri 08:30 – 5pm) Arrange the date and time to coincide with terminal cleaning. Estates department to replace radiator covers when infectious terminal cleaning process completed.
Cleaning of radiators: Outside and inside (if required) Facility staff to clean using a damp disposable cloth soaked in detergent and chlorine containing solution (e.g. Actichlor Plus).
Nursing staff Responsibility (ideally nursing tasks to be completed prior to housekeeping tasks)
Actions Y N Signature
The patient must have vacated the bed space before cleaning commences.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area.
Ensure good ventilation e.g. open a window
The room or area should be cleared of miscellaneous items (e.g. discard magazines, used toiletries into an orange hazardous waste bag).
Remove all linen from bed and place in an alginate bag, followed by infectious outer laundry bag, and tie securely.
All disposable fittings and single use medical devices must be disposed of into an orange hazardous waste bag, e.g. oxygen tubing, suction tubing & suction drainage bags.
All reusable medical equipment must be decontaminated according to manufacturer’s instructions. Following decontamination, remove the equipment from the area.

37 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Actions Y N Signature
Cleaning: Use a detergent and chlorine containing solution eg Actichlor Plus 1000ppm, Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actichlor Plus BS Solution Only Southern Health NHS V1.pdf
Actichlor Plus GE Southern Health NHS V1.pdf
If commode or raised toilet seat present, thoroughly clean all areas with a detergent and chlorine solution, rinse and then dry.
Thoroughly wipe the mattress, upper bed frame, bed head, bed rails, and plastic pillow cover with detergent and chlorine solution eg Actichlor Plus and dry with disposable paper towels. Discard paper towels into orange hazardous waste bag. Ensure good ventilation whilst cleaning within the room.
Clean the patient wash bowl if non-disposable with detergent and chlorine solution e.g. Actichlor Plus and dry with disposable paper towels. If bedside entertainment system present, remove headset earpiece covers and discard into orange hazardous waste bag. Arrange for cleaning and replacement earpieces.
Name of nurse (print): Date completed: Time:
Signature:
Housekeeping Staff Responsibility (ideally nursing tasks should be completed prior to housekeeping tasks)
Housekeeping Team to use detergent and chlorine containing agent eg Actichlor Plus 1000ppm for all cleaning tasks during this procedure. Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actions Y N Signature
Prepare all equipment needed. Park cleaning trolley outside infection room/bay.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area (discuss with nursing staff if any additional PPE is required).
Ensure good ventilation.
Whilst the chlorine containing tablets are dissolving, remove dirty curtains, place into alginate then outer infectious laundry bag.

38 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Actions Y N Signature
Use a detergent and chlorine containing solution eg Actichlor Plus, clean the following using a yellow disposable cloth and damp dusting bucket:
High Dust - Damp dust all areas to hand height level regularly rinsing cloth, allow to air dry.
Bedside Lamp - Extend the lamp, damp dust all areas, return to original position, allow to air dry.
Hand held ‘nurse call’ device, be careful to clean around idented button.
Bedside Locker - Thoroughly clean all areas inside and outside, and allow to air dry.
Bedside Table - Thoroughly clean all areas of table top, underside and stand area regularly rinsing cloth, allow to air dry.
Bedside Chair - Thoroughly clean all wipeable areas of chair seat, back top, underside and legs, allow to air dry.
Bed Frame (below top frame) - Raise bed and thoroughly clean all areas of underside and stand areas working from the top to the bottom, regularly rinsing cloth, allow to air dry.
Window Ledges - Damp dust all areas, and allow to air dry.
All Doors, Door Handles & Door Vents - Thoroughly clean all areas paying attention to hand contact surfaces, regularly rinsing cloth, allow to air dry.
Skirting Boards - Damp dust all areas, allow to air dry.
Clinical Hand Wash Sink, Taps & Splash Back Use two cloths one for taps and dispensers the other for the basin. Taps should be cleaned first before the rest of the CHWB
(ref HTM 04:01 2016)
Tiles -Thoroughly clean the area working from the outside inwards, allow to air dry.
Mirrors - Thoroughly clean the area then dry and buff with a second cloth/disposable paper towel to remove any smears.
Bathroom facilities/ En Suite, use detergent and chlorine releasing solution contained in the ‘Ensuite Cleaning Bucket’ and disposable yellow cloths and clean taps & splash back tiles thoroughly. Clean the area working from the outside inwards, regularly rinsing cloth, allow to air dry.
For any wash hand basins: Use two cloths one for taps and dispensers the other for the basin. Clean the areas working from the outside inwards, allow to air dry.
Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016)
Shower Cubicle, Shower Tray & Wall Tiles/Cladding (if present) - Thoroughly clean the area working from shower head/hose/controls outwards to the tiles and tray, allow to air dry.
Hand Towel & Toilet Roll Dispensers:
Damp dust all areas, allow to air dry. (No need to replace hand towels or towel rolls that are in an enclosed dispenser, just clean/wipe over the external container).
Throw away toilet brushes into infectious waste stream bag.

39 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Actions Y N Signature
Toilet & Toilet Seat - Flush then apply descaler if required, thoroughly clean all areas using a yellow cloth and chlorine releasing solution eg Actichlor plus, working from the highest point to the lowest and from the outside inwards, scrub toilet bowl and finish with toilet seat and a final flush.
Floors – Remove debris using an exhaust filtered vacuum cleaner OR dry mop. Follow this with, wet mopping using a yellow handled mop and chlorine releasing agent eg Actichlor plus from the yellow mop bucket (dispose/launder mop heads after use). If areas are carpeted, steam clean carpet and launder any rugs.
Soft furnishings e.g. chairs or sofas: Steam clean any non wipeable surfaces within the room.
Waste: Discard all disposable cleaning cloths in the orange bag for infectious waste. Pick up any items of rubbish e.g. locker bags, discard into orange waste bag Remove orange waste bag to clean the bin. Replace waste bags as appropriate in the lidded bin for the next patient.
Replacement Consumables - Replenish hand soap, toilet roll, hand towels and opened packets of Clinell wipes. (No need to replace hand towels or toilet rolls that are in an enclosed dispenser, just clean/wipe over the external container). Throw away toilet brushes.
Before leaving the room: Remove PPE and discard into the orange waste bag. Swan neck tie and secure with ward identification tag / tape. Thoroughly clean hands with soap and water. Close door as you leave the room.
Outside the room: Clean hands with alcohol sanitiser Store cleaned and dry cleaning trolley, mop handle and bucket in the cleaning cupboard. Take orange bag waste to storage area.
Replace curtains with clean ones, if no available curtains please discuss steam cleaning with the IPCT before the Infectious terminal cleaning process.. Blinds – Clean / Steam / Actichlor blinds as appropriate.
Comments from housekeeping staff
Comments from nursing staff

40 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
On completion of the Terminal Clean please sign the box below confirming that you are satisfied with the standard of cleanliness.
Ward Manager/shift leader Name: (print) Date completed: Time:
Housekeeping supervisor Name: (print) Date completed: Time:
Signature:
Signature:
Retain copies of this form:- 1. The person requesting final isolation clean must ensure that a copy is to be retained on the ward 2. One copy to be retained by Housekeeping
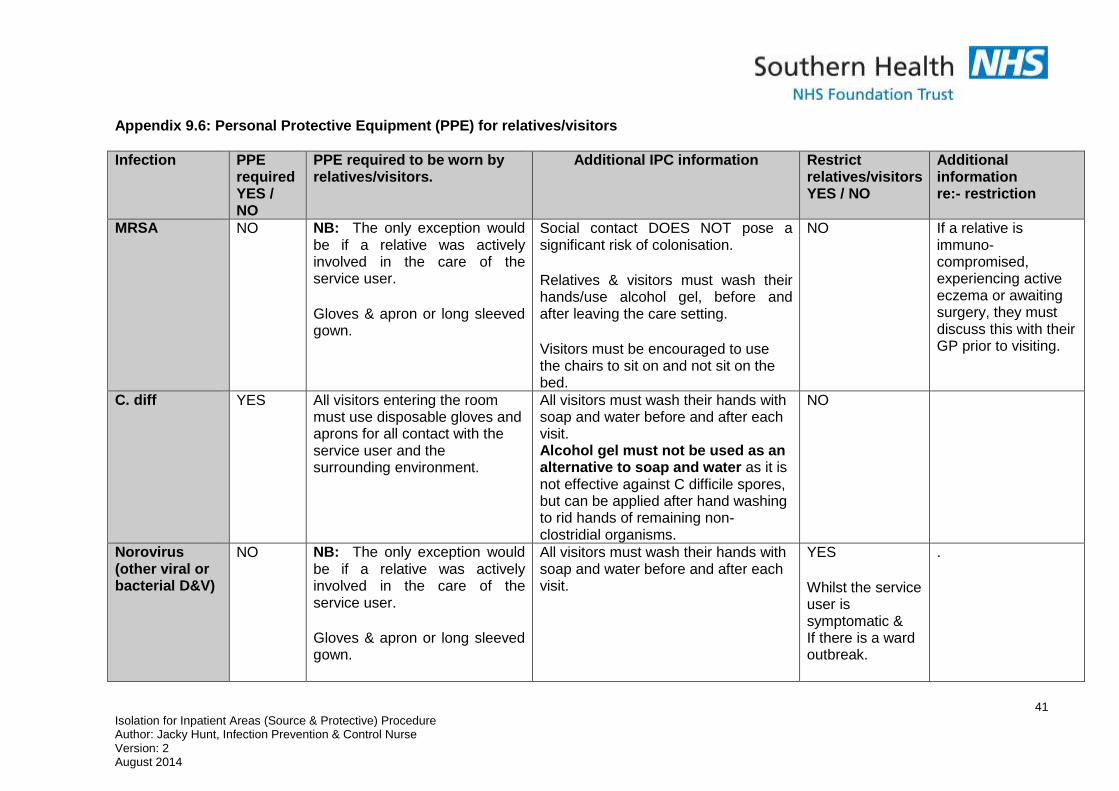
41 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.6: Personal Protective Equipment (PPE) for relatives/visitors
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
MRSA
NO
NB: The only exception would be if a relative was actively involved in the care of the service user. Gloves & apron or long sleeved gown.
Social contact DOES NOT pose a significant risk of colonisation. Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting. Visitors must be encouraged to use the chairs to sit on and not sit on the bed.
NO If a relative is immuno-compromised, experiencing active eczema or awaiting surgery, they must discuss this with their GP prior to visiting.
C. diff
YES All visitors entering the room must use disposable gloves and aprons for all contact with the service user and the surrounding environment.
All visitors must wash their hands with soap and water before and after each visit. Alcohol gel must not be used as an alternative to soap and water as it is not effective against C difficile spores, but can be applied after hand washing to rid hands of remaining non-clostridial organisms.
NO
Norovirus (other viral or bacterial D&V)
NO
NB: The only exception would be if a relative was actively involved in the care of the service user. Gloves & apron or long sleeved gown.
All visitors must wash their hands with soap and water before and after each visit.
YES Whilst the service user is symptomatic & If there is a ward outbreak.
.

42 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
ESBL
NO NB: The only exception would be if a relative was actively involved in the care of the service user. Gloves & apron or long sleeved gown.
Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting. Visitors must be encouraged to use the chairs to sit on and not sit on the bed.
NO
TB (open, smear positive)
NO NB: The exceptions are:- ● If MDR TB is suspected ● If aerosol-generating procedures are being performed e.g. cough/sputum inducing procedures, intubation etc Relatives/visitors are not to be present in the room.
Who is susceptible to TB:- Those with immune systems
weakened by HIV infection or other medical problems
The very young and the elderly, as their immune systems are less robust
Those with chronic poor health and nutrition
YES Household contacts only to visit
Following 2 weeks of effective treatment showing clinical improvement, visitors can be extended beyond the immediate household contacts.
Multi drug resistant TB
YES NB: If multi drug resistant TB. Face mask respirator class FFP2 Or FFP3
Source isolate until smear negative. Multi drug resistant TB service users’ should be nursed in an isolation unit with negative air pressure e.g. at SUHT in the isolation unit. This is a notifiable disease.
YES
INFLUENZA (or suspected influenza)
YES Surgical face mask Gloves & aprons.
Hand hygiene, Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting. Respiratory precautions
YES
Chickenpox & NO NB: The only exception would Relatives & visitors must wash their NO Restrict visitors if

43 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
Shingles
be if a relative was actively involved in the care of the service user. Gloves & apron
hands/use alcohol gel, before and after leaving the care setting.
they have no previous history of chicken pox
Scabies
NO NB: Unless likely prolonged skin to skin contact e.g. hand holding for 5 -10 mins. OR Norweign scabies has been diagnosed. Visitors should cover exposed skin on hands and arms when participating in direct service user care. Disposable gloves & aprons or long sleeved disposable gowns should be worn.
A quick handshake or hug is unlikely to
Transfer the mite. There is very little chance of transfer of mites from clothing and bedding in classic scabies as the mites do not survive away from their host, they quickly become dehydrated and die in the environment. Mites survive longer away from the hosts body in Norweigan scabies e.g. on bed linen, towels and clothing.
NO Restrict non-urgent visitors until the first treatment has been applied?
Blood borne viruses
NO NB: If visitors are likely to be in contact with blood or bodily fluids to wear PPE. Gloves & aprons as a minimum.
Risk if from blood and bodily fluids. NO
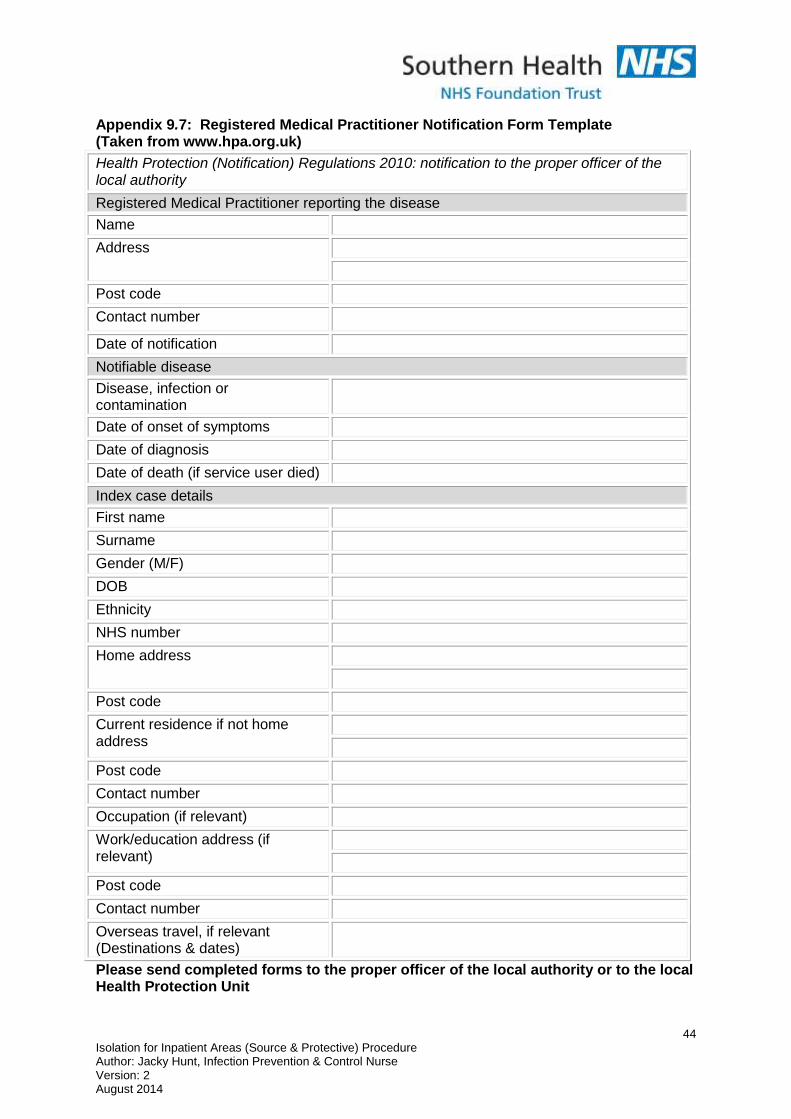
44 Isolation for Inpatient Areas (Source & Protective) Procedure Author: Jacky Hunt, Infection Prevention & Control Nurse Version: 2 August 2014
Appendix 9.7: Registered Medical Practitioner Notification Form Template (Taken from www.hpa.org.uk)
Health Protection (Notification) Regulations 2010: notification to the proper officer of the local authority
Registered Medical Practitioner reporting the disease
Name
Address
Post code
Contact number
Date of notification
Notifiable disease
Disease, infection or contamination
Date of onset of symptoms
Date of diagnosis
Date of death (if service user died)
Index case details
First name
Surname
Gender (M/F)
DOB
Ethnicity
NHS number
Home address
Post code
Current residence if not home address
Post code
Contact number
Occupation (if relevant)
Work/education address (if relevant)
Post code
Contact number
Overseas travel, if relevant (Destinations & dates)
Please send completed forms to the proper officer of the local authority or to the local Health Protection Unit
Related Documents











