Leukemia (1997) 11, 1367–1393 1997 Stockton Press All rights reserved 0887-6924/97 $12.00 CORRESPONDENCE CASE REPORT Isochromosome 7q: the primary cytogenetic abnormality in hepatosplenic gd T cell lymphoma ELC Alonsozana 1 , J Stamberg 2 , D Kumar 1 , ES Jaffe 3 , LJ Medeiros 4 , C Frantz 5 , CA Schiffer 6,7 , BA O’Connell 6,7 , S Kerman 8 , SA Stass 1,7 and LV Abruzzo 1,7 1 Department of Pathology, Laboratories of Pathology, 2 Division of Human Genetics, 5 Department of Pediatrics, 6 Department of Medicine, and 7 Marlene and Stewart Greenebaum Cancer Center, University of Maryland, Baltimore, MD; 3 Hematopathology Section, Laboratory of Pathology, National Cancer Institute, National Institutes of Health, Bethesda, MD; 4 Division of Pathology, City of Hope National Medical Center, Duarte, CA; and 8 American Medical Laboratories, Chantilly, VA, USA Malignant lymphomas often have complex, nonrandom Because of its unique clinical and histopathologic features, chromosomal abnormalities. Hepatosplenic gd T cell lym- hepatosplenic gdTCL has been proposed as a distinct clinico- phoma (gdTCL) is an unusual post-thymic T cell lymphoma that pathologic entity. 4 Recently isochromosome 7q [i(7q)] was primarily involves liver and spleen, often in young adult males. reported in seven cases of hepatosplenic gdTCL. 6,7 We have Few cases have had cytogenetic analysis. We report a consist- previously reported three additional cases of hepatosplenic ent isochromosome 7q [i(7q)] abnormality in three cases of hepatosplenic gdTCL, one with i(7q) as the sole abnormality gdTCL with cytogenetic analysis in abstract form. 8 All three at presentation. Three patients, 15-, 37- and 65-year-old males, cases exhibited a common structural cytogenetic abnormality, presented with hepatosplenomegaly and fevers. Histopatho- i(7q). In one case, i(7q) was the sole abnormality identified on logic, immunophenotypic, and molecular genetic studies sup- the initial diagnostic study. The second case had three ported the diagnosis. Spleen, liver, and bone marrow contained additional abnormalities, and the third case had a complex sinusoidal infiltrates of atypical lymphoid cells of T cell immun- karyotype with multiple numerical and structural abnormali- ophenotype. PCR performed on two cases demonstrated clonal T cell receptor g gene rearrangements. Cytogenetic analysis of ties in addition to the i(7q). These cases represent the ninth to bone marrow showed i(7q) as the sole abnormality at presen- 11th cases of i(7q) reported in hepatosplenic gdTCL, and only tation in one case. The second case showed i(7q) in addition the second case with i(7q) as the sole abnormality. These to two normal chromosomes 7, and other structural and results support the proposal that hepatosplenic gdTCL is a dis- numerical abnormalities. The third case showed i(7q) and a tinct clinicopathologic entity. Furthermore, they implicate deletion in the long arm of chromosome 11. These findings i(7q) as the defining cytogenetic abnormality. support the proposal that i(7q) represents the primary nonran- dom cytogenetic abnormality in hepatosplenic gdTCL, and plays a role in its pathogenesis. Keywords: T cell lymphoma; hepatosplenic lymphoma; isochromo- Materials and methods some; chromosome 7 All cases were collected from the files of the University of Maryland Medical Center and the Hematopathology Section Introduction in the Laboratory of Pathology of the National Cancer Insti- tute. Two cases (cases 1 and 2) were seen in consultation by The T cell receptor (TcR) normally consists of either an ab or one of us (ESJ); the clinical and pathologic features of these gd heterodimer associated with a CD3 complex of proteins cases have been reported recently. 5 Two patients (1 and 3) on the cell surface. Most mature T cells express the ab hetero- were referred to the University of Maryland from outside hos- dimer. A minority of mature T cells express the gd hetero- pitals for evaluation and treatment. Hematoxylin and eosin dimer. These cells are found primarily in the splenic red pulp (H&E)-stained histologic sections were prepared at the submit- and intestinal epithelium. 1 Like most normal T cells, most lym- ting institutions. Additional sections were prepared from the phomas of T cell lineage express the ab heterodimer. 2 Hepa- submitted paraffin blocks of formalin-fixed tissue. In all cases, tosplenic gdT cell lymphoma (gdTCL) is an unusual peripheral spleen and bone marrow specimens were studied. Additional T cell lymphoma that expresses the gd TcR. 3–5 Cytologically, tissue from liver was available in case 1, and transbronchial the neoplastic cells are uniform, medium-sized lymphoid cells biopsy tissue was examined in case 3. with dispersed chromatin, small nucleoli, and a moderate amount of pale cytoplasm. The cells preferentially involve the sinusoids of spleen, liver, and bone marrow. As a result, Immunophenotypic analysis patients often present with hepatosplenomegaly, although per- ipheral blood involvement is unusual early in the course of Immunophenotypic studies were performed on fixed, paraffin- the disease. This lymphoma has a marked predilection for embedded sections and fresh tissue. Fixed, paraffin-embedded young men. The prognosis is poor, and most patients die sections were analyzed by the avidin-biotin-peroxidase (ABC) within 2 years of diagnosis despite aggressive chemotherapy. technique, as described previously 9 using a panel of anti- bodies to CD3, CD20 (L26), CD43 (Leu22), CD45RO (UCHL- 1, A6) and CD74 (LN-2). Immunophenotypic studies were Correspondence: LV Abruzzo, Department of Pathology, University performed on fresh tissue using one of two methods. For cases of Maryland, 22 S Greene St, Baltimore, MD 21201, USA Received 7 February 1997; accepted 17 April 1997 1 and 3, cell suspensions were analyzed by flow cytometry

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Leukemia (1997) 11, 1367–1393 1997 Stockton Press All rights reserved 0887-6924/97 $12.00
CORRESPONDENCE
CASE REPORT
Isochromosome 7q: the primary cytogenetic abnormality in hepatosplenic gd T celllymphomaELC Alonsozana1, J Stamberg2, D Kumar1, ES Jaffe3, LJ Medeiros4, C Frantz5, CA Schiffer6,7, BA O’Connell6,7, S Kerman8,SA Stass1,7 and LV Abruzzo1,7
1Department of Pathology, Laboratories of Pathology, 2Division of Human Genetics, 5Department of Pediatrics, 6Department of Medicine,and 7Marlene and Stewart Greenebaum Cancer Center, University of Maryland, Baltimore, MD; 3Hematopathology Section, Laboratory ofPathology, National Cancer Institute, National Institutes of Health, Bethesda, MD; 4Division of Pathology, City of Hope National MedicalCenter, Duarte, CA; and 8American Medical Laboratories, Chantilly, VA, USA
Malignant lymphomas often have complex, nonrandom Because of its unique clinical and histopathologic features,chromosomal abnormalities. Hepatosplenic gd T cell lym- hepatosplenic gdTCL has been proposed as a distinct clinico-phoma ( gdTCL) is an unusual post-thymic T cell lymphoma that pathologic entity.4 Recently isochromosome 7q [i(7q)] wasprimarily involves liver and spleen, often in young adult males.
reported in seven cases of hepatosplenic gdTCL.6,7 We haveFew cases have had cytogenetic analysis. We report a consist-previously reported three additional cases of hepatosplenicent isochromosome 7q [i(7q)] abnormality in three cases of
hepatosplenic gdTCL, one with i(7q) as the sole abnormality gdTCL with cytogenetic analysis in abstract form.8 All threeat presentation. Three patients, 15-, 37- and 65-year-old males, cases exhibited a common structural cytogenetic abnormality,presented with hepatosplenomegaly and fevers. Histopatho- i(7q). In one case, i(7q) was the sole abnormality identified onlogic, immunophenotypic, and molecular genetic studies sup- the initial diagnostic study. The second case had threeported the diagnosis. Spleen, liver, and bone marrow contained
additional abnormalities, and the third case had a complexsinusoidal infiltrates of atypical lymphoid cells of T cell immun-karyotype with multiple numerical and structural abnormali-ophenotype. PCR performed on two cases demonstrated clonal
T cell receptor g gene rearrangements. Cytogenetic analysis of ties in addition to the i(7q). These cases represent the ninth tobone marrow showed i(7q) as the sole abnormality at presen- 11th cases of i(7q) reported in hepatosplenic gdTCL, and onlytation in one case. The second case showed i(7q) in addition the second case with i(7q) as the sole abnormality. Theseto two normal chromosomes 7, and other structural and results support the proposal that hepatosplenic gdTCL is a dis-numerical abnormalities. The third case showed i(7q) and a
tinct clinicopathologic entity. Furthermore, they implicatedeletion in the long arm of chromosome 11. These findingsi(7q) as the defining cytogenetic abnormality.support the proposal that i(7q) represents the primary nonran-
dom cytogenetic abnormality in hepatosplenic gdTCL, andplays a role in its pathogenesis.Keywords: T cell lymphoma; hepatosplenic lymphoma; isochromo- Materials and methodssome; chromosome 7
All cases were collected from the files of the University ofMaryland Medical Center and the Hematopathology Section
Introduction in the Laboratory of Pathology of the National Cancer Insti-tute. Two cases (cases 1 and 2) were seen in consultation by
The T cell receptor (TcR) normally consists of either an ab or one of us (ESJ); the clinical and pathologic features of thesegd heterodimer associated with a CD3 complex of proteins cases have been reported recently.5 Two patients (1 and 3)on the cell surface. Most mature T cells express the ab hetero- were referred to the University of Maryland from outside hos-dimer. A minority of mature T cells express the gd hetero- pitals for evaluation and treatment. Hematoxylin and eosindimer. These cells are found primarily in the splenic red pulp (H&E)-stained histologic sections were prepared at the submit-and intestinal epithelium.1 Like most normal T cells, most lym- ting institutions. Additional sections were prepared from thephomas of T cell lineage express the ab heterodimer.2 Hepa- submitted paraffin blocks of formalin-fixed tissue. In all cases,tosplenic gdT cell lymphoma (gdTCL) is an unusual peripheral spleen and bone marrow specimens were studied. AdditionalT cell lymphoma that expresses the gd TcR.3–5 Cytologically, tissue from liver was available in case 1, and transbronchialthe neoplastic cells are uniform, medium-sized lymphoid cells biopsy tissue was examined in case 3.with dispersed chromatin, small nucleoli, and a moderateamount of pale cytoplasm. The cells preferentially involve thesinusoids of spleen, liver, and bone marrow. As a result, Immunophenotypic analysispatients often present with hepatosplenomegaly, although per-ipheral blood involvement is unusual early in the course of Immunophenotypic studies were performed on fixed, paraffin-the disease. This lymphoma has a marked predilection for embedded sections and fresh tissue. Fixed, paraffin-embeddedyoung men. The prognosis is poor, and most patients die sections were analyzed by the avidin-biotin-peroxidase (ABC)within 2 years of diagnosis despite aggressive chemotherapy. technique, as described previously9 using a panel of anti-
bodies to CD3, CD20 (L26), CD43 (Leu22), CD45RO (UCHL-1, A6) and CD74 (LN-2). Immunophenotypic studies wereCorrespondence: LV Abruzzo, Department of Pathology, Universityperformed on fresh tissue using one of two methods. For casesof Maryland, 22 S Greene St, Baltimore, MD 21201, USA
Received 7 February 1997; accepted 17 April 1997 1 and 3, cell suspensions were analyzed by flow cytometry

Correspondence
1368as described previously.5 In cases 1 and 2, frozen sectionswere analyzed by the ABC technique.9,10 The panel of anti-bodies included antibodies to CD1a, CD2, CD3, CD4, CD5,CD7, CD8, CD10, CD11c, CD14, CD16, CD19, CD20,CD21, CD22, CD25, CD56, CD57, TcRb and TcRd. For case2, flow cytometry was performed at an outside laboratory andresults reported.
Cytogenetic analysis
Cytogenetic studies in cases 1 and 3 were performed at theUniversity of Maryland on direct preparations of bone marrowand peripheral blood using standard techniques.11 The divid-ing cells were analyzed by Giemsa–trypsin banding. A seriesof six bone marrow specimens was examined over a 19 monthperiod in case 1. A single bone marrow and a peripheralblood specimen were examined in case 3. A minimum of 25(range 25–50) cells were analyzed for each sample, with theexception of the peripheral blood in case 3, in which only 12cells were available for analysis. In case 2, cytogenetic studieswere performed at an outside laboratory, and were availablefor review. For this case, bone marrow was examined with 20cells analyzed, using similar techniques.
Molecular diagnostic studies
In all cases, analysis for rearrangement of the TcRg chain genewas performed by polymerase chain reaction (PCR) on DNAextracted from formalin-fixed, paraffin-embedded tissue asdescribed previously.12,13 Southern blot analysis was also per-formed in case 3 on DNA isolated from bone marrow.Hybridizations with probes to the TcRb chain gene (Jb/III), theimmunoglobulin heavy chain gene (JH), and the immunoglob-ulin kappa light chain gene (JK) were performed using a com-mercially available kit according to the manufacturer’sinstructions (B/T Blue Gene Rearrangement Test System;Oncor, Gaithersburg, MD, USA).
Results
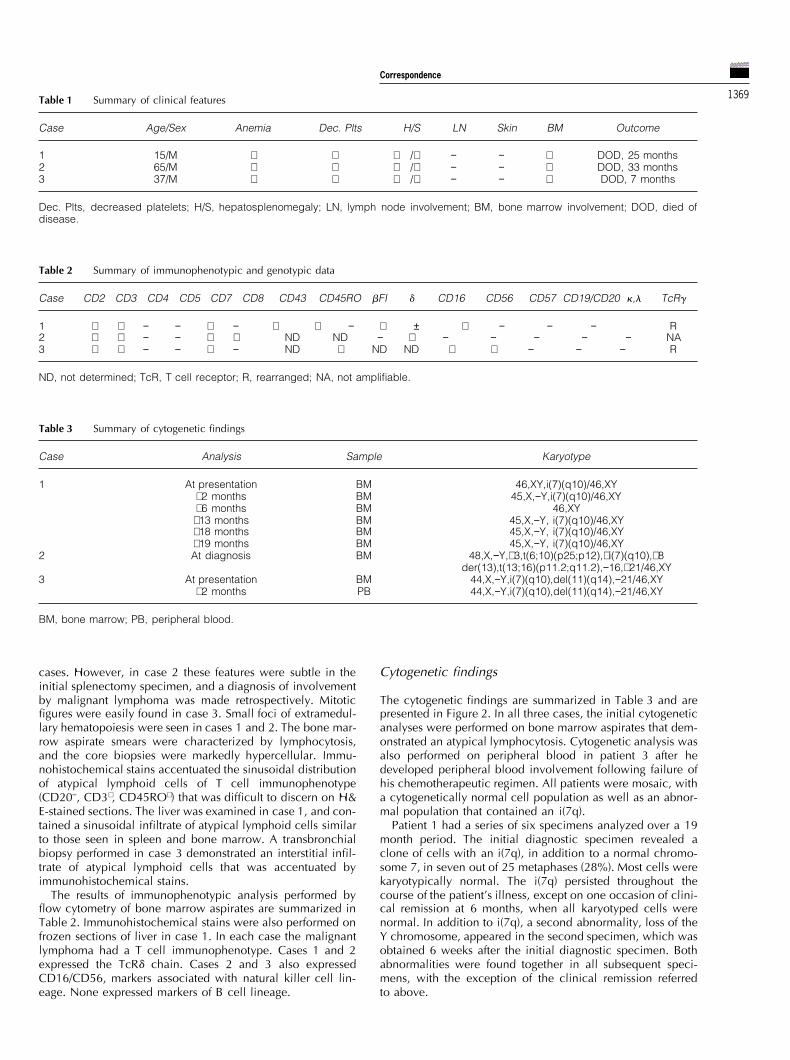
Figure 1 Representative photomicrographs illustrate the histologicClinical featuresand immunophenotypic features. (a) Bone marrow and (b) spleen frompatient 3 contain infiltrates of medium-sized lymphoid cells with
The clinical features are summarized in Table 1. All patients irregular nuclear contours and a moderate amount of cytoplasm,with a predilection for sinusoidal involvement (H&E).were males, aged 15, 65 and 37 years at the time of diagnosis.(c) Immunoperoxidase stain for CD3 performed on spleen shows a TPatient 1 presented with asymptomatic hepatosplenomegaly,cell immunophenotype (hematoxylin counterstain).followed by fevers, nausea and vomiting, and a petechial rash
on his head and neck. His past medical history was unremark-able. Patient 2 presented with splenomegaly and thrombocy- Histologic and immunophenotypic findingstopenia, and underwent splenectomy 5 months later for pre-sumed idiopathic thrombocytopenic purpura (ITP). After an The histologic and immunophenotypic features in all cases
were similar. Spleen, bone marrow aspirate smears and coreinterval of 26 months he was re-evaluated for recurring feversand thrombocytopenia. Patient 3 presented with fever and biopsies were available for review in all cases. All patients
underwent splenectomy. The spleens were enlarged (patientchills, and was found to have hepatosplenomegaly and lym-phadenopathy. His past medical history was unremarkable. 1, 2264 g; patient 2, 705 g; patient 3, 2050 g) with homo-
geneous, dark red parenchyma. Representative sections ofAll patients received aggressive multiagent chemotherapy.Although patient 1 achieved an initial clinical remission, the bone marrow and spleen from case 3 are presented in
Figure 1. The neoplastic cells were medium-sized lymphoiddisease recurred and he died 25 months after diagnosis.Patient 2 died 2 months after the diagnosis of gdTCL, and 33 cells with round to irregular nuclear contours, dispersed
chromatin, occasional small nucleoli, and a moderate amountmonths after his initial presentation. The lymphoma in patient3 was refractory to therapy, and he died 7 months after of pale cytoplasm. The splenic red pulp was expanded and
sinusoids were dilated by atypical lymphoid cells in all threediagnosis.
Correspondence
1369Table 1 Summary of clinical features
Case Age/Sex Anemia Dec. Plts H/S LN Skin BM Outcome
1 15/M + + +/+ − − + DOD, 25 months2 65/M + + +/+ − − + DOD, 33 months3 37/M + + +/+ − − + DOD, 7 months
Dec. Plts, decreased platelets; H/S, hepatosplenomegaly; LN, lymph node involvement; BM, bone marrow involvement; DOD, died ofdisease.
Table 2 Summary of immunophenotypic and genotypic data
Case CD2 CD3 CD4 CD5 CD7 CD8 CD43 CD45RO bFI d CD16 CD56 CD57 CD19/CD20 k,l TcRg
1 + + − − + − + + − + ± + − − − R2 + + − − + + ND ND − + − − − − − NA3 + + − − + − ND + ND ND + + − − − R
ND, not determined; TcR, T cell receptor; R, rearranged; NA, not amplifiable.
Table 3 Summary of cytogenetic findings
Case Analysis Sample Karyotype
1 At presentation BM 46,XY,i(7)(q10)/46,XY+2 months BM 45,X,−Y,i(7)(q10)/46,XY+6 months BM 46,XY
+13 months BM 45,X,−Y, i(7)(q10)/46,XY+18 months BM 45,X,−Y, i(7)(q10)/46,XY+19 months BM 45,X,−Y, i(7)(q10)/46,XY
2 At diagnosis BM 48,X,−Y,+3,t(6;10)(p25;p12),+i(7)(q10),+8der(13),t(13;16)(p11.2;q11.2),−16,+21/46,XY
3 At presentation BM 44,X,−Y,i(7)(q10),del(11)(q14),−21/46,XY+2 months PB 44,X,−Y,i(7)(q10),del(11)(q14),−21/46,XY
BM, bone marrow; PB, peripheral blood.
cases. However, in case 2 these features were subtle in the Cytogenetic findingsinitial splenectomy specimen, and a diagnosis of involvementby malignant lymphoma was made retrospectively. Mitotic The cytogenetic findings are summarized in Table 3 and are
presented in Figure 2. In all three cases, the initial cytogeneticfigures were easily found in case 3. Small foci of extramedul-lary hematopoiesis were seen in cases 1 and 2. The bone mar- analyses were performed on bone marrow aspirates that dem-
onstrated an atypical lymphocytosis. Cytogenetic analysis wasrow aspirate smears were characterized by lymphocytosis,and the core biopsies were markedly hypercellular. Immu- also performed on peripheral blood in patient 3 after he
developed peripheral blood involvement following failure ofnohistochemical stains accentuated the sinusoidal distributionof atypical lymphoid cells of T cell immunophenotype his chemotherapeutic regimen. All patients were mosaic, with
a cytogenetically normal cell population as well as an abnor-(CD20−, CD3+, CD45RO+) that was difficult to discern on H&E-stained sections. The liver was examined in case 1, and con- mal population that contained an i(7q).
Patient 1 had a series of six specimens analyzed over a 19tained a sinusoidal infiltrate of atypical lymphoid cells similarto those seen in spleen and bone marrow. A transbronchial month period. The initial diagnostic specimen revealed a
clone of cells with an i(7q), in addition to a normal chromo-biopsy performed in case 3 demonstrated an interstitial infil-trate of atypical lymphoid cells that was accentuated by some 7, in seven out of 25 metaphases (28%). Most cells were
karyotypically normal. The i(7q) persisted throughout theimmunohistochemical stains.The results of immunophenotypic analysis performed by course of the patient’s illness, except on one occasion of clini-
cal remission at 6 months, when all karyotyped cells wereflow cytometry of bone marrow aspirates are summarized inTable 2. Immunohistochemical stains were also performed on normal. In addition to i(7q), a second abnormality, loss of the
Y chromosome, appeared in the second specimen, which wasfrozen sections of liver in case 1. In each case the malignantlymphoma had a T cell immunophenotype. Cases 1 and 2 obtained 6 weeks after the initial diagnostic specimen. Both
abnormalities were found together in all subsequent speci-expressed the TcRd chain. Cases 2 and 3 also expressedCD16/CD56, markers associated with natural killer cell lin- mens, with the exception of the clinical remission referred
to above.eage. None expressed markers of B cell lineage.
Correspondence
1370Patient 2 had cytogenetic analysis performed on bone mar-
row approximately 3 years after he had undergone splen-ectomy. The karyotype of the majority of cells (18/20 or 90%)exhibited multiple structural and numerical abnormalities,including i(7q) and two normal chromosomes 7. In this patientthe i(7q) did not replace a normal chromosome 7, butoccurred in addition to two apparently normal 7s. The Y chro-mosome was also missing in these cells. A minor cell popu-lation (2/20 or 10%) exhibited a normal male karyotype.
Cytogenetic analysis performed on bone marrow of patient3 at the time of diagnosis also showed two cell populations.A minority of the cells (6/40 or 15%) contained i(7q) inaddition to other abnormalities, including loss of the Y chro-mosome. The remaining cells had a normal male karyotype.The analysis performed on peripheral blood 2 months laterwas similar.
Molecular diagnostic studies
Analysis of the TcRg chain was performed by PCR on DNAextracted from formalin-fixed, paraffin-embedded sections ofinvolved tissue.12 Cases 1 and 3 contained clonal TcRg re-arrangements (Table 2). Case 1 showed a single band with theV2 primer, and case 3 showed a single band with V11 primer;DNA from case 2 was not amplifiable (data not shown).Southern blot analysis performed on DNA extracted frominvolved bone marrow in case 3 demonstrated that the IgHgene, the IgK gene, and the TcRb gene were in the germlineconfiguration (data not shown).
Discussion
Hepatosplenic gdTCL is a recently described, rare lymphomaof post-thymic T cell origin. Few cases have been reported inthe literature,2,3,6,7,14–19 several only in abstract form.20,21 Only11 cases have had cytogenetic analysis,6,7,14,17–19, includingthree cases recently reported by Wang and co-workers.6 Intheir study all three cases had i(7q) and trisomy 8; one casehad two copies of the i(7q) as well as additional, unidentifiedmaterial on the long arm of chromosome 6. They proposedthat i(7q) plays a key role in the pathogenesis of hepatosplenicgdTCL, and that trisomy 8 is a secondary abnormality. Anotherfour cases with i(7q) and trisomy 8 have been reportedrecently by Jonveaux and coworkers.7 They proposed thati(7q) and trisomy 8 are the primary, nonrandom abnormalities.In this paper, we report three cases of hepatosplenic gdTCLwith i(7q). Significantly, one patient had i(7q) as the solechromosomal abnormality at diagnosis. Two patients had i(7q)and other numerical and structural abnormalities, includingtrisomy 8 in one patient. In all three of our patients the malig-nant clone also lost the Y chromosome, either at diagnosis orduring evolution of the disease. Our data bring the number ofpatients with hepatosplenic gdTCL and i(7q) to eleven,6,7,14
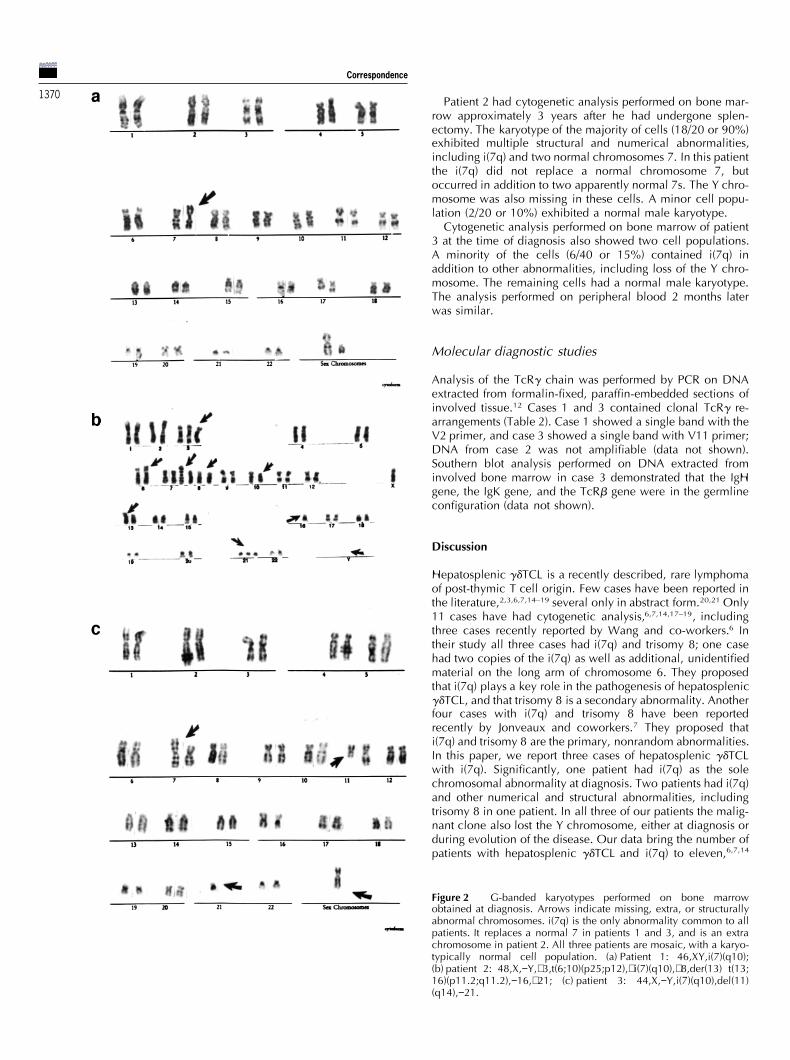
Figure 2 G-banded karyotypes performed on bone marrowobtained at diagnosis. Arrows indicate missing, extra, or structurallyabnormal chromosomes. i(7q) is the only abnormality common to allpatients. It replaces a normal 7 in patients 1 and 3, and is an extrachromosome in patient 2. All three patients are mosaic, with a karyo-typically normal cell population. (a) Patient 1: 46,XY,i(7)(q10);(b) patient 2: 48,X,−Y,+3,t(6;10)(p25;p12),+i(7)(q10),+8,der(13) t(13;16)(p11.2;q11.2),−16,+21; (c) patient 3: 44,X,−Y,i(7)(q10),del(11)(q14),−21.

Correspondence
1371two patients with i(7q) as the sole abnormality.8,14 Thus, it 124 cases of predominantly hematopoietic neoplasms, most
often associated with other chromosomal abnormalities. It wasappears likely that i(7q) is the primary cytogenetic abnormalityin hepatosplenic gdTCL. Frequent secondary abnormalities detected as the sole abnormality in four cases of acute
myeloid leukemia, three cases of myelodysplastic syndrome,acquired during disease evolution are loss of the Y chromo-some and gain of a chromosome 8. three cases of ALL, and one case of Wilm’s tumor, rep-
resenting a small minority of these tumor types. Cases of ALLCytogenetic analysis failed to demonstrate i(7q) in three pre-viously reported cases of hepatosplenic gdTCL.17–19 In one with i(7q) are usually of B cell lineage, and have other cyto-
genetic abnormalities, particularly t(4;11) or der(19), that arecase, reported by Ross and coworkers,18 the lymphoma arosein the setting of organ transplantation and had the karyotype believed to represent the primary abnormalities.23,25 Loss of
the short arm of chromosome 7, either due to monosomy ort(7;9)(p15;q13)t(13q;14q). Thus, the malignant cells had a bal-anced translocation between chromosomes 7 and 9, as well partial deletion, is a relatively common sole abnormality in
ALL.23,26 It has been proposed, therefore, that in ALL with i(7q)as a Robertsonian translocation of chromosomes 13 and 14.Chromosome 7 was broken at band 7p15, with no apparent it is the loss of genetic material from the short arm, rather than
gain of material from the long arm of the chromosome, thatgain or loss of genetic material. However, a break within ornear a coding region can cause dysregulation or loss of gene is important in its pathogenesis.
Isochromosome 7q has been reported in several cases offunction. In the second case, reported by Wong and cowork-ers,19 cytogenetic studies demonstrated a karyotype of hepatosplenic lymphomas that may represent hepatosplenic
gdTCL. Colwill and coauthors14 described a 20-year-old man44,X,−Y,−11,−22,+mar. However, the relative size or shape ofthe marker was not described, nor was it characterized by who presented with massive splenomegaly due to involve-
ment by T cell lymphoma. Although the malignant cells wereadditional banding methods, such as fluorescent in situhybridization with whole-chromosome libraries. In the third not studied for expression of the ab or the gd TcR, they had
clonal TcRd gene rearrangements, and the i(7q) was the solecase, reported by Mastovich and coworkers,17 analysis perfor-med on involved bone marrow demonstrated a normal female chromosomal abnormality. Thus, we believe that this case is
most likely an hepatosplenic gdTCL. A recent report of naturalkaryotype. However, the only cytogenetic study reported wasperformed at presentation, when the infiltrate was described killer (NK)-like T cell lymphoma of large granular lymphocyte
derivation contained three cases with i(7q) in addition to otheras ‘subtle’. Thus, the karyotype obtained may represent thenormal rather than the neoplastic cell population. This structural and numerical chromosome abnormalities.27 The
clinical and immunophenotypic features of these cases arepatient’s lymphoma underwent histologic progression 2 yearsafter presentation. Had cytogenetic studies been done at this consistent with the diagnosis of hepatosplenic gd T cell lym-
phoma, although the neoplastic cells in one case containedtime, they might have shown a different picture. In fact, thepatient reported by Ross and coworkers,18 and one of the prominent azurophilic granules and neither case was studied
for expression of TcRd. Because of the considerable clinicalpatients reported by Wang and coworkers,6 had normal chro-mosome results at presentation. However, cytogenetic studies and morphologic overlap between hepatosplenic gdTCL, NK
leukemia/lymphoma, and NK-like T cell lymphoma, theseperformed 9 weeks and 2.5 months later, respectively,revealed clonal chromosomal abnormalities. It is conceivable, cases may be difficult to distinguish by routine histopathologic
and immunophenotypic analysis. Evaluation of cases that falltherefore, that for the patients described by Mastovich andWong, further cytogenetic studies might have been informa- within this spectrum for expression of the ab and gd TcR, as
well as cytogenetic analysis, may help to define furthertive, and might have demonstrated i(7q) or other rearrange-ments. these entities.
Isochromosomes are found frequently as acquired abnor-malities in neoplastic cells, and result in both loss and gain
Referencesof genetic material. Recent studies indicate that, at least inconstitutionally occurring isochromosomes, there are usually
1 Bucy RP, Chen CL, Cooper MD. Tissue localization and CD8two centromeres present, separated by a very small amount accessory molecule expression of T g/d cells in humans. J Immunolof the apparently missing chromosome arm.22 There is little 1989; 142: 3045–3049.information on the structure of isochromosomes in malignant 2 Gaulard P, Bourquelot P, Kanavaros P, Haioun C, Le Coudeic JP,
Divine M, Goossens M, Zafrani ES, Farcet JP, Reyes F. Expressioncells. Their structure, as well as their mode of formation, areof the alpha/beta and gamma/delta T-cell receptors in 57 cases ofsubjects of interest to cytogeneticists, and will be discussedperipheral T-cell lymphomas: identification of a subset of g/d T-elsewhere (Stamberg and Abruzzo, manuscript incell lymphomas. Am J Pathol 1990; 137: 617–628.preparation). The simplest explanation for the role of isochro- 3 Farcet JP, Gaulard P, Marolleau JP, Le Coudeic JP, Henni T, Gour-
mosomes in neoplasia is that isochromosome formation din MF, Divine M, Haioun C, Zafrani C, Gossens M, Hercend T,results either in the loss of a tumor suppressor gene, the acti- Reyes F. Hepatosplenic T-cell lymphoma: sinusal/sinusoidal local-
ization of malignant cells expressing the T-cell receptor gd. Bloodvation of an oncogene, or both. However, isochromosomes1990; 75: 2213–2219.are rarely the sole cytogenetic abnormality detected, and are
4 Harris NL, Jaffe ES, Stein H, Banks PM, Chan JKC, Cleary ML,believed in most cases to represent secondary changes asso-Delsol G, Wolf-Peters CD, Falini B, Gatter KC, Grogan TM, Issac-ciated with tumor progression.23 An exception may be iso- son PG, Knowles DM, Mason DY, Muller-Hermelink HK, Pileri
chromosome 21q, recently described as a significant finding SA, Piris MA, Ralfkiaer E, Warnke RA. A revised European–Amer-in acute lymphoblastic leukemia (ALL) by Martineau and ican classification of lymphoid neoplasms: a proposal from the
International Lymphoma Study Group. Blood 1994; 84: 1361–coworkers.24 They suggest that in a subgroup of ALL patients,1392.i(21q) is an early, although rarely the sole, chromosome
5 Cooke CB, Krenacs L, Stetler-Stevenson M, Greiner TC, Raffeld M,abnormality.Kingma DW, Abruzzo L, Frantz C, Kaviani M, Jaffe ES. Hepatos-Mertens and coworkers23 reviewed the cytogenetic data plenic T cell lymphoma: a distinct clinicopathologic entity of
from more than 20 000 chromosomally abnormal tumors, and cytotoxic gd T cell origin. Blood 1996; 88: 4265–4274.showed that i(7q) is one of the more commonly occurring 6 Wang CC, Tien HF, Lin MT, Su IJ, Wang CH, Chuang SM, Shen
MC, Liu CH. Consistent presence of isochromosome 7q in hepa-isochromosomes. It was found as a recurrent abnormality in

Correspondence
1372 tosplenic T g/d lymphoma: a new cytogenetic-clinicopathologic 17 Mastovich S, Ratech H, Ware RE, Moore JO, Borowitz MJ. Hepa-entity. Genes Chromosom Cancer 1995; 12: 161–164. tosplenic T-cell lymphoma: an unusual case of a gd T-cell lym-
7 Jonveaux P, Daniel MT, Martel V, Maarek O, Berger R. Isochromo- phoma with a blast-like terminal transformation. Hum Patholsome 7q and trisomy 8 are consistent primary non-random 1994; 25: 102–108.chromosomal abnormalities associated with hepatosplenic T g/d 18 Ross CW, Schnitzer B, Sheldon S, Braun DK, Hanson CA.lymphoma. Leukemia 1996; 10: 1453–1455. Gamma/delta T-cell posttransplantation lymphoproliferative dis-
8 Alonsozana ELC, Stamberg J, Kumar D, Jaffe ES, Medeiros LJ, order primarily in the spleen. Am J Clin Pathol 1994; 102: 310–Frantz C, Schiffer C, O’Connell B, Kurman S, Stass SA, Cohen MM, 315.Abruzzo LV. Isochromosome 7q: the primary rearrangement in 19 Wong KF, Chan JKC, Matutes E, McCarthy K, Ng CS, Chan CH, Mahepatosplenic gd T-cell lymphoma. Am J Hum Genet 1996; 59: SK. Hepatosplenic gd T-cell lymphoma: a distinctive aggressive315A. lymphoma type. Am J Surg Pathol 1995; 19: 718–726.
9 Hsu SM, Jaffe ES. Leu M1 and peanut agglutinin stain the neoplas- 20 Krishnan J, Goodman Z, Frizzera G. Primary hepatic sinusoidaltic cells of Hodgkin’s disease. Am J Clin Pathol 1984; 82: 29–32. presentation of malignant T cell lymphoma. Mod Pathol 1992;
10 Gonzalez CL, Medeiros LJ, Braziel RM, Jaffe ES. T-cell lymphoma 25: 81A.involving subcutaneous tissue: a clinicopathologic entity com- 21 Salhany K, Kahn M, Kamoun M, Kant J, Glick A, Loh E. Hepato-monly associated with hemophagocytic syndrome. Am J Surg splenic gd T-cell lymphoma: an aggressive cytolytic peripheral T-Pathol 1991; 15: 17–27. cell lymphoma presenting with severe neutropenia. Mod Pathol11 Le Beau MM. Cytogenetic analysis of hematological malignant
1994; 7: 119A.diseases. In: Barch MJ (ed). The ACT Cytogenetics Laboratory22 Wolff DJ, Miller AP, Van Dyke DL, Schwartz S, Willard HF. Mol-Manual, 2nd edn. Raven Press: New York, 1991, pp 395–449.
ecular definition of breakpoints associated with human Xq iso-12 Greiner TC, Raffeld M, Lutz C, Dick F, Jaffe ES. Analysis of T cellchromosomes: implications for mechanisms of formation. Am Jreceptor-gamma gene rearrangements by denaturing gradient gelHum Genet 1996; 58: 154–160.electrophoresis of GC-clamped polymerase chain reaction pro-
23 Mertens F, Johansson B, Mitelman F. Isochromosomes in neo-ducts. Correlation with tumor-specific sequences. Am J Patholplasia. Genes Chromosom Cancer 1994; 10: 221–230.1995; 146: 46–55.
24 Martineau M, Clark R, Farrell DM, Hawkins JM, Moorman AV,13 Bourguin A, Tung R, Galili N, Sklar J. Rapid non-radioactive detec-Secker-Walker LM. Isochromosomes in acute lymphoblastic leu-tion of clonal T-cell receptor gene rearrangements in lymphoidkemia: i(21q) is a significant finding. Genes Chromosom Cancerneoplasms. Proc Natl Acad Sci USA 1990; 87: 8536–8540.1996; 17: 21–30.14 Colwill R, Dube I, Scott JG, Bailey D, Deharven E, Carstairs K,
25 Pui CH, Carroll AJ, Raimondi SC, Schell MJ, Head DR, Shuster JJ,Pantalony D. Isochromosome 7q as the sole abnormality in anCrist WM, Borowitz MJ, Link MP, Behm FG, Steuber CP, Land VJ.unusual case of T-cell lineage malignancy. Hematol Pathol 1990;
4: 53–58. Isochromosomes in childhood acute lymphoblastic leukemia: a15 Dommann-Scherrer CC, Kurer SB, Zimmermann DR, Odermatt collaborative study of 83 cases. Blood 1992; 79: 2384–2391.
BF, Dours-Zimmermann MT, Briner J, Heitz PU. Occult hepato- 26 Johansson B, Mertens F, Mitelman F. Cytogenetic deletion mapssplenic T-gd lymphoma: value of genotypic analysis in the differ- of hematologic neoplasms: circumstantial evidence for tumor sup-ential diagnosis. Virchows Arch 1995; 426: 629–634. pressor loci. Genes Chromosom Cancer 1993; 8: 205–218.
16 Garcia-Sanchez F, Menarguez J, Cristobal E, Cantalejo A, Ghil J, 27 Macon WR, Williams ME, Greer JP, Hammer RD, Glick AD, Col-Algara P, Vicario JL. Hepatosplenic gamma-delta T-cell malignant lins RD, Cousar JB. Natural killer-like T-cell lymphomas: aggress-lymphoma: report of the first case in childhood, including molecu- ive lymphomas of T-large granular lymphocytes. Blood 1996; 87:lar minimal residual disease follow-up. Br J Haematol 1995; 90: 1474–1483.943–946.
Related Documents










![Case Report Primary cutaneous γδ-T-cell lymphoma … cutaneous γδ-T-cell lymphoma (CGD-TCL) ... TCL [3]. Some other study reports that allogenic ... we reported a case of CGD-TCL](https://static.cupdf.com/doc/110x72/5ae360cf7f8b9a495c8d272b/case-report-primary-cutaneous-t-cell-lymphoma-cutaneous-t-cell-lymphoma.jpg)
