Introduction Research Risk Need Treatment Conclusion Lessons Learned from the PA DOC’s Recidivism Reduction Efforts: Practical Experiences in Implementing Evidence-Based Assessment & Treatment Practices Jeffrey A. Beard, Ph.D. Secretary of Corrections Pennsylvania Department of Corrections Presentation for : ASCA All Directors Training Program November 14, 2008 San Diego, CA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Introduction
Research
Risk
Need
Treatment
Conclusion
Lessons Learned from the PA DOC’s Recidivism Reduction Efforts:
Practical Experiences in Implementing Evidence-Based Assessment & Treatment Practices
Jeffrey A. Beard, Ph.D.Secretary of Corrections
Pennsylvania Department of Corrections
Presentation for : ASCA All Directors Training Program
November 14, 2008San Diego, CA
Introduction
Research
Risk
Need
Treatment
Conclusion
Why Follow Evidence-Based Practice (EBP)?
Population growth is unrelenting…
Fiscal impact is tremendous…
Most importantly, public safety is our responsibility…
Failed response – confinement has not been sufficient…
costly, ineffective as long-term solution to criminal behavior, & creates “roadblocks to re-entry”
recidivism - 68% arrested for new crime within 3 yrs of release (BJS)
Treatment works - addressing crime-producing needs is longer-term solution
recidivism rates reduced 10–30% with quality program
some programs are more effective than others
effective programs embrace the “Principles of Effective Intervention”
Introduction
Research
Risk
Need
Treatment
Conclusion
Principles of Effective Correctional Intervention
Risk Principle
Need Principle
Treatment Principle
Responsivity Principle
Dosage Principle
Relapse Principle
Community Integration Principle
Staffing Principle
Fidelity Principle
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 1: The Risk Principle
• Definition of risk probability of re-offense not to be confused with seriousness, dangerousness,
public objection, or political sensitivity
• Risk principle high risk likely to re-offend if not treated low risk unlikely to re-offend, even if untreated treatment of low risk may increase risk level

Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 2: The Need Principle
• Definitions dynamic risk factors (changeable) – can be addressed criminogenic needs – related to re-offending (Handout #1)
• Need Principle - target criminogenic needs: Anti-social attitudes, values, beliefs, cognitions Anti-social associates & pro-social isolation Temperamental & personality factors
weak socialization, egocentrism impulsivity, risk taking aggressive energy, hostility, anger weak decision-making, problem-solving, coping skills
Low levels of educational, vocational, financial achievement Familial factors (e.g., marital/spouse) – poor quality personal relationships,
lack of mutual caring/respect/interest/accountability; anti-criminal expectations or neutral expectations with regard to criminal behavior
Substance abuse• Do not target non-criminogenic needs (self-esteem, anxiety, depression, etc)
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 3: The Treatment Principle
• Most effective approach = Cognitive Behavioral Integrates three theories:
• Behaviorism/Learning Theory Operant conditioning, reinf & punishment (Handout #2) Action-oriented Direct training – role play, practice, graduated rehearsal
• Social Learning Theory Observational learning Modeling, imitation, feedback
• Cognitive Theory Targets thoughts influencing behavior Two basic models:
Cognitive Restructuring - attempt to alter thought content (beliefs, values, attitudes)
Cognitive Skills - attempt to alter and improve thought processes (structure & form of reasoning)
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 3: The Treatment Principle, continued…
Ineffective Theoretical Models• Psychodynamic (traditional “Freudian” theory, psychoanalysis, Gestalt, Rogerian
non-directive, and other client-centered approaches)• Biological (diet, pharmacological treatments, etc.)• Deterrence (“offenders lack discipline”, “punishing-smarter” strategies, etc.)
Questionable Approaches & Programs (see Handout #3 for more examples)• Drama Therapy• Handwriting Formation Therapy• Physical Strength Training for Substance Abusers• Yoga, Meditation, Sweat Lodges• Bibliotherapy• Drug Education• Shaming Offenders• Gardening• Famous Ineffective Programs – Scared Straight, DARE, Wilderness Camps
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 4: The Responsivity Principle
• Definition of responsivity Individual factors influencing potential for results/change
• Types of responsivity factors (Handout #4) Personality (anxiety, depression, etc.) Motivation (readiness, amenability, compliance, etc.) Cognitive (learning style, IQ, attention deficits, etc.) Demographic (age, gender, race, etc.) Other (offender typology, etc.)
• Application of responsivity principle = Matching Offender to program
(e.g., anxious offender/Encounter group) Offender to staff
(e.g., low cognitive level offender/high conceptual level staff)
Staff to program (e.g., staff prefers structure/contingency management program)
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 5: The Dosage Principle
• Dosage defined: total hours of treatment exposure (duration & intensity) high dosage – exceeds 100 contact hours low dosage – little evidence low dosage programs are effective by
themselves • Duration
defined: length of service/program last for 3-9 months
• Intensity defined: how “compact” program is delivered (dense)
• Recommendations for Duration & Intensity: ideal program has both high intensity and longer duration no “watering down” - give dosage over shorter, rather than longer period Match dosage to individual risk/need profile
higher risk require greater dosage (more intensive, longer duration)

Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 6: The Relapse Principle
• Purpose: maintain treatment gains
• Provide booster sessions
• Deliver aftercare in prison and community settings
• Teach relapse prevention strategies & techniques: identify triggers avoid high risk individuals, settings, situations practice low-risk alternative responses reward improved competencies train family & friends in supportive roles
• Intervene as soon as possible when circumstances deteriorate

Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 7: The Community Integration Principle
continuity of care – integrate with community-based services for seamless transition
advocacy & brokerage – refer offenders to programs with quality & relevant services
public education – transfer knowledge of research & EBP to community stakeholders
collaboration – communicate, cooperate, & form relationships with key stakeholders
address obstacles – identify, then minimize or eliminate obstacles to re-entry
external monitoring – regularly evaluate the quality of service delivery by providers
delivery setting – provide services in community to greatest extent possible

Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 8: The Staffing Principle
Who should deliver the programming/formal treatment intervention?
• Staff should have appropriate: levels of education experience training personal qualities, skills, & characteristics (Handout #5)
Who is responsible for targeting changes in offender behavior? …When should efforts toward rehabilitation be made? ALWAYS – develop an environment/culture supportive of
rehabilitation through all frontline staff, not just treatment staff Every social interaction with an offender in prison/center is
opportunity to reinforce appropriate behavior (Handout #6)
Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 9: The Fidelity Principle
Internal Methods for Promoting Quality Assurance
Implementation - pilot minimum 1 month (formal start & end dates), literature review, develop & utilize treatment manual
Post-assessment of offenders• actuarial reassessment of offenders on target areas• observation – pro-social speech, no excuses, demonstrate skills• institutional conduct
Feedback• inmate/client satisfaction surveys• staff questionnaires & other input mechanisms• formal advisory board
Monitoring & Supervision• file reviews• regular observation of direct service delivery (Handout #7)• clinically-specific performance evaluations• adherence to program/treatment manual• involvement by leadership (e.g., regular service delivery)

Introduction
Research
Risk
Need
Treatment
Conclusion
Principle 9: The Fidelity Principle, continued…
External Evaluation
Audits, Inspections, Site Visits – licensure, accreditation, etc.
Process evaluations - measure extent to which program is operating as intended, “black box” (Handout #8)
• Correctional Program Checklist (CPC) examines 5 areas: Program Leadership & Development Staff Characteristics Offender Assessment Treatment Characteristics Quality Assurance
Outcome evaluations – measures extent program achieves intended results• recidivism (collect follow-up data at 3, 6, 12, 18 months)• drug abstinence• misconducts• escapes
Introduction
Research
Risk
Need
Treatment
Conclusion
Who should we focus on? Which needs must we address?
Needs are Diverse & Significant…
65% serious alcohol, drug problem (another 6% w/lower level need)
68% hostility, anger, violence, aggression
59% antisocial attitudes, criminal thinking
43% no HS/GED & 80% unemployed 6 months+ before prison
7% sex offender issues
Introduction
Research
Risk
Need
Treatment
Conclusion
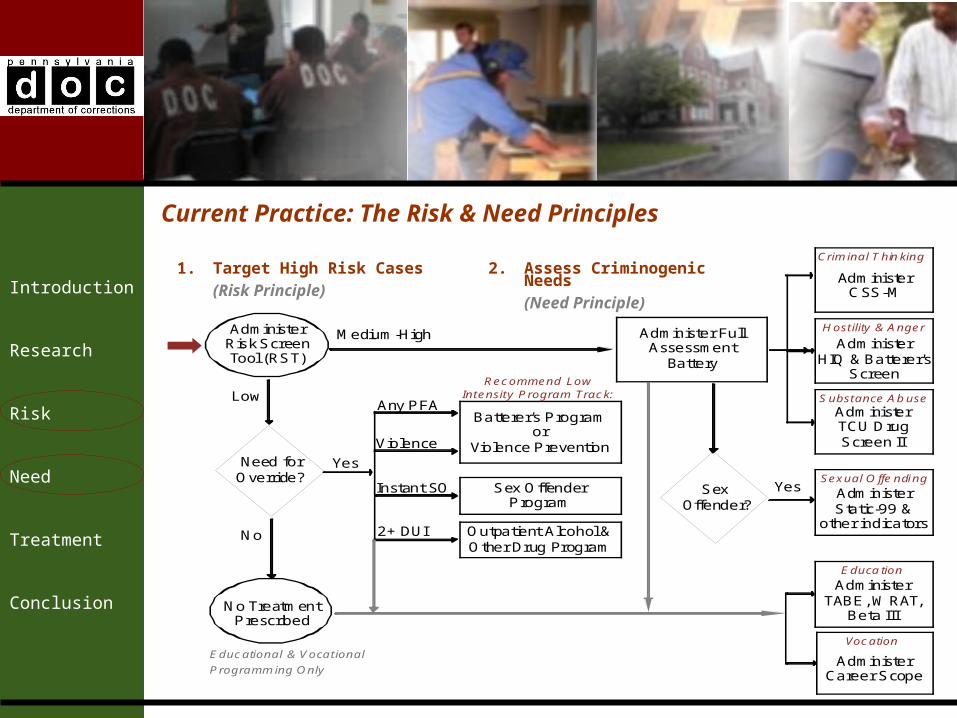
Current Practice: The Risk & Need Principles
1. Target High Risk Cases
(Risk Principle)
2. Assess Criminogenic Needs
(Need Principle)
AdministerRisk ScreenTool (RST)
Need forOverride?
No
Medium-High
Low
Yes
No TreatmentPrescribed
Administer FullAssessment
Battery
Educational & Vocat ional
Programm ing Only
Sexual O ffe ndi ng
H ost ility & Anger
Educa tion
Crim inal T hin king
Substance Ab use
Vocation
AdministerCSS-M
AdministerHIQ & Batterer's
Screen
AdministerTCU DrugScreen II
AdministerStatic-99 &
other indicators
AdministerTABE, W RAT,
Beta III
AdministerCareer Scope
SexOffender?
Yes
Batterer's Programor
Violence Prevention
Sex OffenderProgram
Outpatient Alcohol &Other Drug Program
Any PFA
2+ DUI
Instant SO
Violence
Recommend LowIntensity Program Track:
Introduction
Research
Risk
Need
Treatment
Conclusion
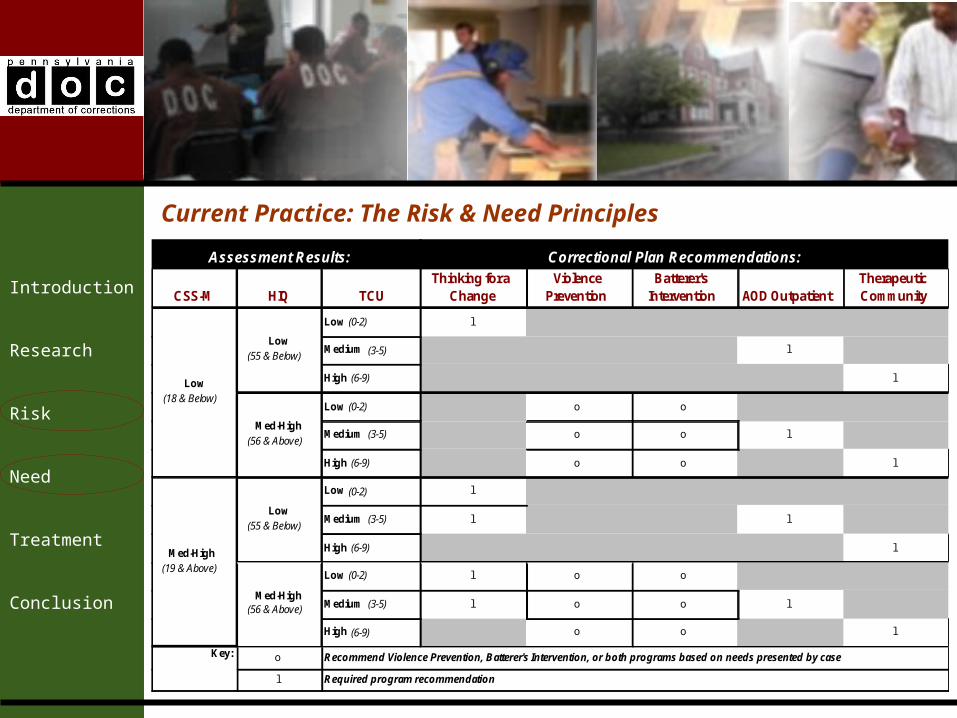
Current Practice: The Risk & Need Principles
CSS-M HIQ TCUThinking for a
ChangeViolence
PreventionBatterer's
Intervention AOD OutpatientTherapeutic Community
Low (0-2) l
Medium (3-5) l
High (6-9) l
Low (0-2) o o
Medium (3-5) o o l
High (6-9) o o l
Low (0-2) l
Medium (3-5) l l
High (6-9) l
Low (0-2) l o o
Medium (3-5) l o o l
High (6-9) o o l
o
l
Assessment Results:
Recommend Violence Prevention, Batterer's Intervention, or both programs based on needs presented by case
Required program recommendation
Key:
Correctional Plan Recommendations:
Low (18 & Below)
Low (55 & Below)
Med-High (56 & Above)
Med-High (19 & Above)
Low (55 & Below)
Med-High (56 & Above)
Introduction
Research
Risk
Need
Treatment
Conclusion
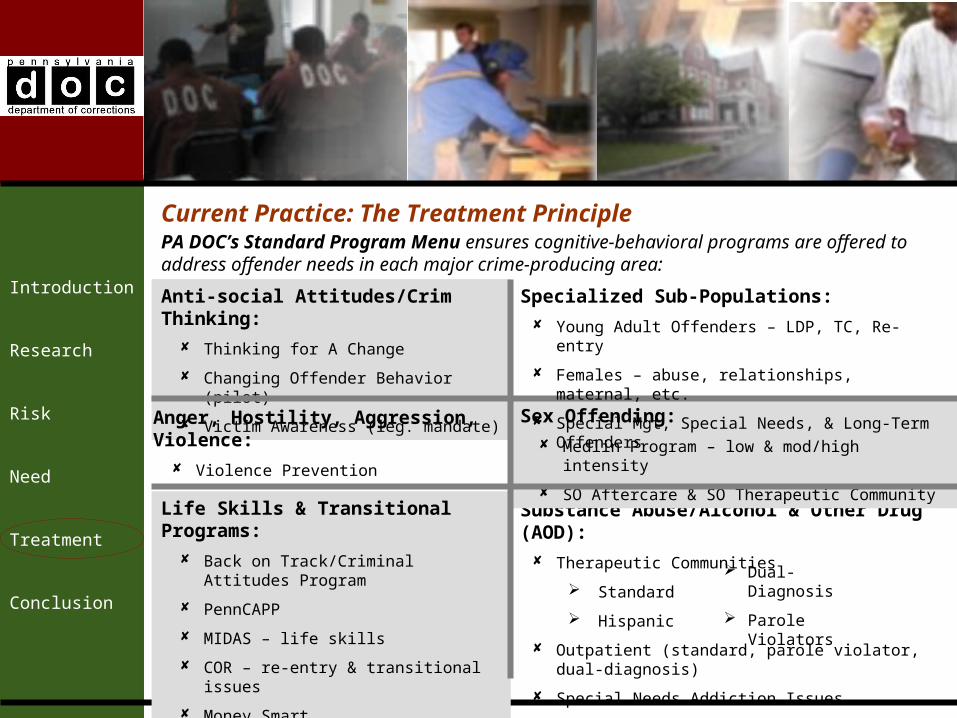
Current Practice: The Treatment Principle
Anti-social Attitudes/Crim Thinking:
Thinking for A Change
Changing Offender Behavior (pilot)
Victim Awareness (leg. mandate)
Anger, Hostility, Aggression, Violence:
Violence Prevention
Batterer’s Intervention
Substance Abuse/Alcohol & Other Drug (AOD):
Therapeutic Communities
Standard
Hispanic
Outpatient (standard, parole violator, dual-diagnosis)
Special Needs Addiction Issues
Sex Offending:
Medlin Program – low & mod/high intensity
SO Aftercare & SO Therapeutic Community
Life Skills & Transitional Programs:
Back on Track/Criminal Attitudes Program
PennCAPP
MIDAS – life skills
COR – re-entry & transitional issues
Money Smart
Parenting
Specialized Sub-Populations:
Young Adult Offenders – LDP, TC, Re-entry
Females – abuse, relationships, maternal, etc.
Special Mgt, Special Needs, & Long-Term Offenders
Dual-Diagnosis
Parole Violators
PA DOC’s Standard Program Menu ensures cognitive-behavioral programs are offered to address offender needs in each major crime-producing area:
Introduction
Research
Risk
Need
Treatment
Conclusion
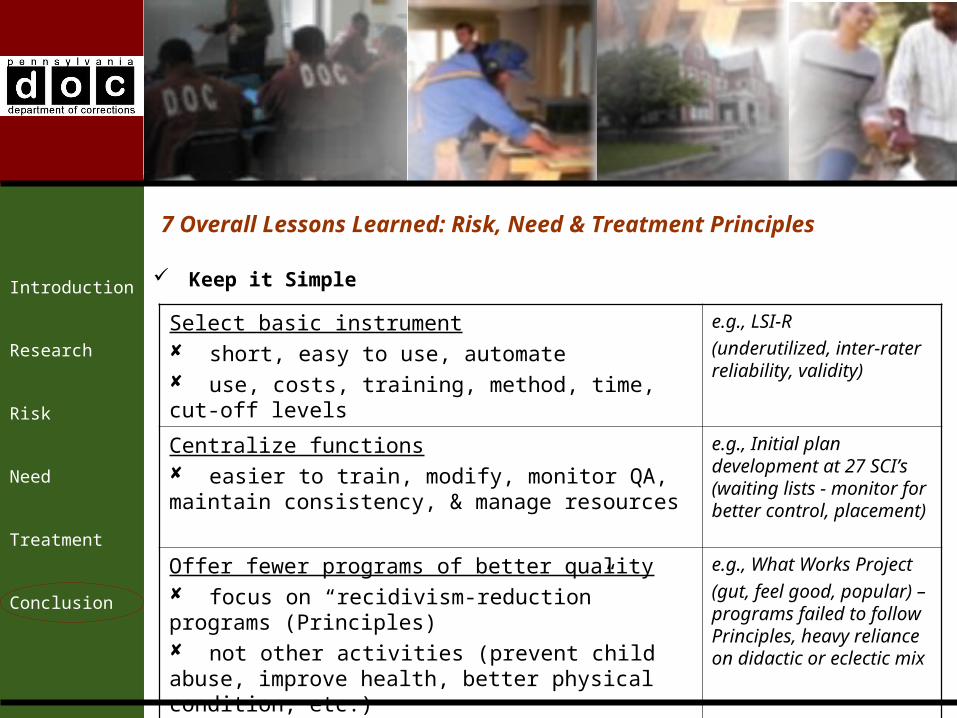
7 Overall Lessons Learned: Risk, Need & Treatment Principles
Keep it Simple
Select basic instrument short, easy to use, automate use, costs, training, method, time, cut-off levels
e.g., LSI-R
(underutilized, inter-rater reliability, validity)
Centralize functions easier to train, modify, monitor QA, maintain consistency, & manage resources
e.g., Initial plan development at 27 SCI’s (waiting lists - monitor for better control, placement)
Offer fewer programs of better quality focus on “recidivism-reduction” programs (Principles) not other activities (prevent child abuse, improve health, better physical condition, etc.)
e.g., What Works Project
(gut, feel good, popular) – programs failed to follow Principles, heavy reliance on didactic or eclectic mix
Introduction
Research
Risk
Need
Treatment
Conclusion
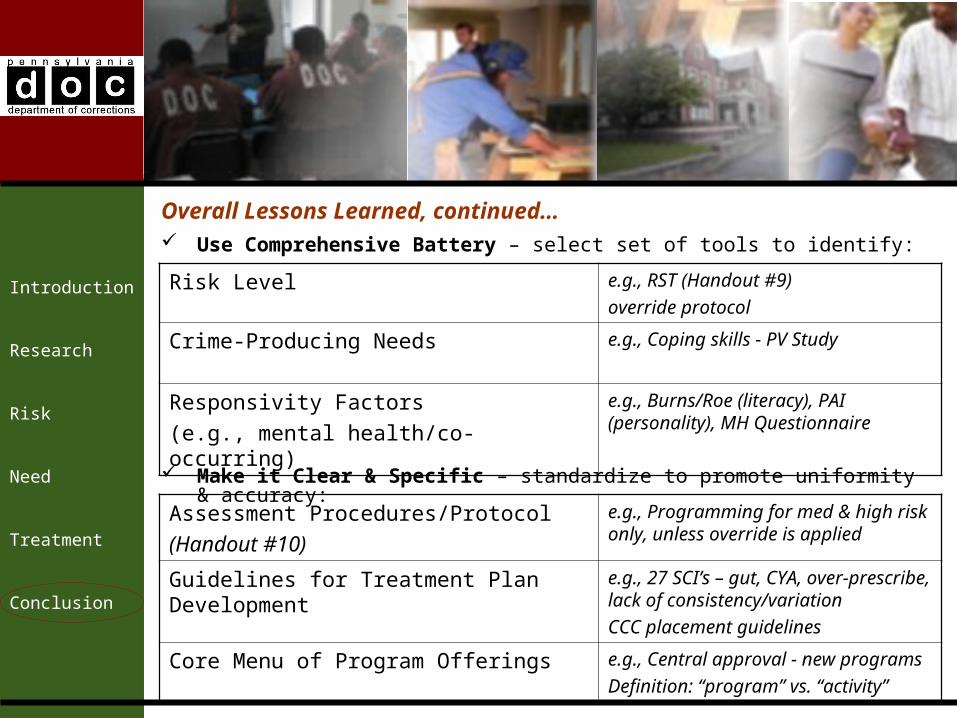
Use Comprehensive Battery – select set of tools to identify:
Risk Level e.g., RST (Handout #9)
override protocol
Crime-Producing Needs e.g., Coping skills - PV Study
Responsivity Factors
(e.g., mental health/co-occurring)
e.g., Burns/Roe (literacy), PAI (personality), MH Questionnaire
Overall Lessons Learned, continued…
Make it Clear & Specific – standardize to promote uniformity & accuracy:
Assessment Procedures/Protocol
(Handout #10)
e.g., Programming for med & high risk only, unless override is applied
Guidelines for Treatment Plan Development e.g., 27 SCI’s – gut, CYA, over-prescribe, lack of consistency/variation
CCC placement guidelines
Core Menu of Program Offerings e.g., Central approval - new programs
Definition: “program” vs. “activity”
Introduction
Research
Risk
Need
Treatment
Conclusion
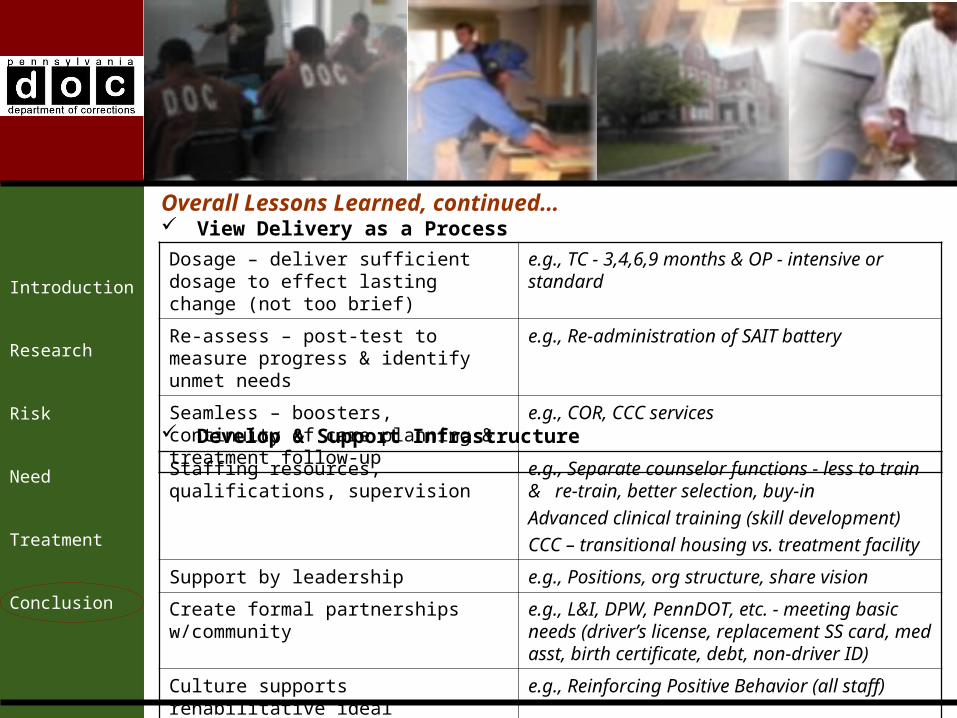
View Delivery as a Process
Dosage – deliver sufficient dosage to effect lasting change (not too brief)
e.g., TC - 3,4,6,9 months & OP - intensive or standard
Re-assess – post-test to measure progress & identify unmet needs
e.g., Re-administration of SAIT battery
Seamless – boosters, continuity of care planning & treatment follow-up
e.g., COR, CCC services
Develop & Support Infrastructure
Staffing resources, qualifications, supervision
e.g., Separate counselor functions - less to train & re-train, better selection, buy-in
Advanced clinical training (skill development)
CCC – transitional housing vs. treatment facility
Support by leadership e.g., Positions, org structure, share vision
Create formal partnerships w/community e.g., L&I, DPW, PennDOT, etc. - meeting basic needs (driver’s license, replacement SS card, med asst, birth certificate, debt, non-driver ID)
Culture supports rehabilitative ideal e.g., Reinforcing Positive Behavior (all staff)
Overall Lessons Learned, continued…
Introduction
Research
Risk
Need
Treatment
Conclusion
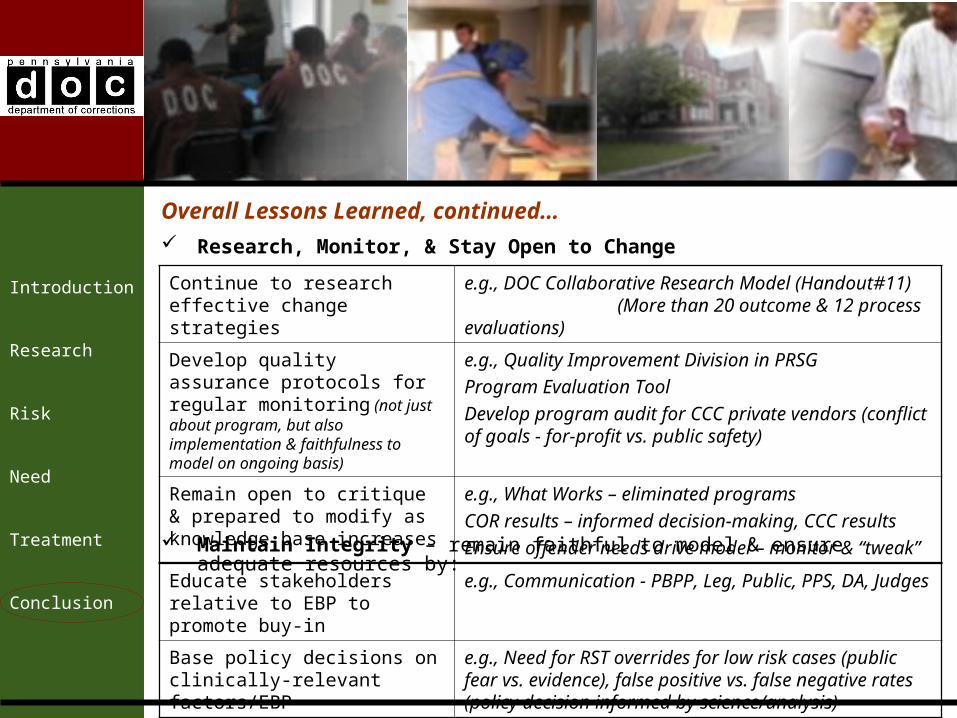
Research, Monitor, & Stay Open to Change
Continue to research effective change strategies
e.g., DOC Collaborative Research Model (Handout#11) (More than 20 outcome & 12 process evaluations)
Develop quality assurance protocols for regular monitoring (not just about program, but also implementation & faithfulness to model on ongoing basis)
e.g., Quality Improvement Division in PRSG
Program Evaluation Tool
Develop program audit for CCC private vendors (conflict of goals - for-profit vs. public safety)
Remain open to critique & prepared to modify as knowledge base increases
e.g., What Works – eliminated programs
COR results – informed decision-making, CCC results
Ensure offender needs drive model – monitor & “tweak” Maintain Integrity – remain faithful to model & ensure adequate resources by:
Educate stakeholders relative to EBP to promote buy-in
e.g., Communication - PBPP, Leg, Public, PPS, DA, Judges
Base policy decisions on clinically-relevant factors/EBP
e.g., Need for RST overrides for low risk cases (public fear vs. evidence), false positive vs. false negative rates (policy decision informed by science/analysis)
Overall Lessons Learned, continued…
Introduction
Research
Risk
Need
Treatment
Conclusion
Questions regarding this presentation may be addressed to:
Jeffrey A. Beard, Ph.D.Secretary of Corrections
Pennsylvania Department of CorrectionsP.O. Box 598
2520 Lisburn RoadCamp Hill, Pennsylvania 17001-0598
Phone: (717) 975-4918Fax: (717) 703-3621
Related Documents











