Universidade Federal do Rio Grande do Norte Centro de Ciências da Saúde Departamento de Fisioterapia Programa de Pós-graduação em Fisioterapia RELAÇÃO ENTRE HISTÓRIA REPRODUTIVA E PROLAPSO DE ÓRGÃOS PÉLVICOS SINTOMÁTICO COM FORÇA MUSCULAR RESPIRATÓRIA EM MULHERES DE MEIA-IDADE E IDOSAS RESIDENTES NA COMUNIDADE INGRID GUERRA AZEVEDO NATAL-RN 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-graduação em Fisioterapia
RELAÇÃO ENTRE HISTÓRIA REPRODUTIVA E PROLAPSO DE
ÓRGÃOS PÉLVICOS SINTOMÁTICO COM FORÇA MUSCULAR
RESPIRATÓRIA EM MULHERES DE MEIA-IDADE E IDOSAS
RESIDENTES NA COMUNIDADE
INGRID GUERRA AZEVEDO
NATAL-RN
2017
15
Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-graduação em Fisioterapia
RELAÇÃO ENTRE HISTÓRIA REPRODUTIVA E PROLAPSO DE
ÓRGÃOS PÉLVICOS SINTOMÁTICO COM FORÇA MUSCULAR
RESPIRATÓRIA EM MULHERES DE MEIA-IDADE E IDOSAS
RESIDENTES NA COMUNIDADE
INGRID GUERRA AZEVEDO
Tese apresentada ao Programa de Pós-Graduação em Fisioterapia da Universidade Federal do Rio Grande do Norte, como pré-requisito à obtenção do Grau de Doutor em Fisioterapia. Área de concentração: Avaliação e Intervenção em Fisioterapia Saúde da Mulher. Orientadora: Profa. Dra. Elizabel de Souza Ramalho Viana. Co-orientadora: Profa. Dra. Saionara Maria Aires da Câmara.
NATAL-RN
2017
16

17
Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-graduação em Fisioterapia
Coordenador do programa de Pós-graduação em Fisioterapia:
Prof. Dr. Álvaro Campos Cavalcanti Maciel
iii
18
Universidade Federal do Rio Grande do Norte
Centro de Ciências da Saúde
Departamento de Fisioterapia
Programa de Pós-graduação em Fisioterapia
RELAÇÃO ENTRE HISTÓRIA REPRODUTIVA E PROLAPSO DE
ÓRGÃOS PÉLVICOS SINTOMÁTICO COM FORÇA MUSCULAR
RESPIRATÓRIA EM MULHERES DE MEIA-IDADE E IDOSAS
RESIDENTES NA COMUNIDADE
BANCA EXAMINADORA:
Prof. Dr. Álvaro Campos Cavalcanti Maciel - UFRN
Profa. Dra. Lilian Lira Lisboa - UFRN
Profa. Dra. Ana Tereza do Nascimento Sales Figueiredo Fernandes - UEPB
Profa. Dra. Saionara Maria Aires da Câmara – Presidente da Banca – FACISA-
UFRN
Profa. Dra. Silvana Loana de Oliveira Sousa - Universidad Miguel de Hernández
iv

19
DEDICATÓRIA
À minha querida família, fonte de amor,
perseverança e honestidade,
em especial a Agostinho Nunes Guerra e
Francisca Campêlo Guerra.
v
20
AGRADECIMENTOS
Neste espaço destinado a agradecimentos, notei a necessidade de procurar a
origem das palavras que remetem a “agradecer”. Descobri, então, que “obrigado (a)”
origina-se do latim obligatus, particípio do verbo obligare, o qual significa ligar ou
amarrar. Quando ficamos devedores a alguém, tornamo-nos, mesmo que por um
breve espaço de tempo, ligados àquela pessoa ou situação, ou seja, criamos um elo,
mesmo que momentâneo. Já a palavra “gratidão” vem do latim gratia, que significa
graça, ou gratus, que se traduz como agradável. É uma emoção que envolve um
sentimento e, portanto, não há obrigações, ligações ou amarrações.
Gratidão é o sentimento maior que invade meu coração hoje. Sinto-me grata
ao meu passado, por ter me tornado a nova pessoa que sou e honrada pelas lições
que me impôs; dentre as pessoas que nele estiveram, algumas foram chamadas às
estrelas, mas permanecem me dando forças, e outras permanecem aqui, embora
seguindo em outros caminhos da mesma trilha a qual todos nós precisamos
caminhar. Todo meu maior agradecimento a cada uma delas. Elas foram
necessárias no meu caminho (e eu, certamente, no delas), e contribuíram
significativamente para minha evolução científica e pessoal.
Espreitando a plenitude do presente, hoje, saboreio este presente junto a
pessoas que, como um quebra-cabeça, se juntaram perfeitamente à minha história,
fazendo com que este dia chegasse. Obrigada aos professores da banca pelas suas
contribuições, que são todas bem-vindas. À professora Dra. Elizabel Viana, palavras
nunca seriam suficientes para expressar o quanto me sinto grata ao seu “sim”
naquela reunião em 14 abril de 2015. Senti como se sua coragem se parecesse com
a minha, pois para colocar minha pós-graduação em cheque naquela situação,
intimamente eu parecia ter a certeza que nada estava perdido, mas que haveria um
recomeço. E nos seus olhos, dias depois, quando nos encontramos, a confiança que
vi
21
me depositou, dizendo que sabia que tudo daria certo, me mostrou, mais uma vez,
que o caminho a ser percorrido teria que ser mudado. Muito obrigada seria pouco!
Desejo a você que essa coragem perdure por toda sua vida, e que sua honestidade
nunca se perca. Isso sim, acima de qualquer ciência, faz diferença na vida de outras
pessoas!
Meus agradecimentos ao professor Dr. Ricardo Guerra, por ter me acolhido
como um verdadeiro pai em março de 2015, e não como, naquele momento,
coordenador da pós-graduação. Pra mim, as maiores contribuições que o senhor
tem deixado desde a graduação não são somente suas aulas e artigos publicados,
mas sim, seu bom humor, sua leveza e seu comprometimento com tudo o que faz.
Obrigada pelo exemplo de profissional e de homem que és!
Sou grata ao professor Dr. Álvaro Campos pela confiança ao me sugerir um
caminho que se fez mais fácil de ser percorrido, pela objetividade quando minha
ansiedade precisava ser controlada, assim, colocando meus pés no chão, e por me
disponibilizar um grupo de mulheres batalhadoras e inteligentes para me ajudar. À
professora Dra. Saionara Aires, pela ajuda de sempre, pela paciência, pelas
oportunidades, pelos inúmeros ensinamentos, pelas orientações e também pelas
conversas quando eu achava que estava tudo fora do lugar e na verdade, ela me
mostrava que estava tudo onde realmente deveria estar. Além disso, agradeço à
amiga de longa data, que voltei a ter por perto numa situação delicada, me fazendo
ver que o que vale a pena nessa caminhada árdua de aquisição de um título não é o
título em si, mas o que nós conquistamos junto com ele.
À Mariana Vieira, Mayle Moreira, Rafaella Silva e Rafaela Andrade, muito
obrigada por terem deixado suas atividades em Natal e terem ido comigo até Santa
Cruz, fazendo com que esse sonho fosse passo-a-passo, construído. Sem vocês
seria tudo muito mais difícil. Em particular, à amiga Rafaela Andrade, por aguentar
vii
22
tanto choro e tanta reclamação e, mesmo assim, nunca mudar seu discurso em
dizer: “Amiga, já deu certo. Você vai conseguir!”. Ao grupo de acadêmicos de
iniciação científica (Bruno, Jailma, Letícia, Pedro, Edeildo, Natália, Maria Helena e
Luiz) e às mestrandas Luana Cortez e Sabrina Gabrielle, por todo apoio nas coletas.
Sozinha nada disso seria possível! Vocês foram essenciais para esta conquista! Às
professoras Silvana Loana e Catherine Pirkle, agradeço pela oportunidade de
trabalharmos juntas. Foi certamente um grande aprendizado. À Juliana Fernandes e
Cristiano Gomes, pelo companheirismo e por tanta ajuda com a famigerada
Estatística sempre que precisei.
À professora Dra. Silvana Alves, enquanto chefe do setor de pesquisa e
inovação tecnológica do HUAB, que gentilmente, desde o início, se dispôs a
contribuir com este projeto, disponibilizando, inclusive, recursos próprios sem nada
em troca, me fazendo questionar se aquilo realmente estava acontecendo ou o que
eu teria que fazer para pagar. Em especial, agora, à grande amiga, que se tornou
um dos meus exemplos de perseverança, inteligência e fonte de energias positivas
que quero ter sempre por perto. À eterna professora Dra. Lilian Lira, pelas infinitas
discussões e tantas conversas, pela ajuda de sempre, e por me lembrar que tenho
uma missão nesse caminho que resolvi trilhar.
Agradeço aos bioquímicos e técnicos do laboratório do HUAB, e em
particular, à Ana Cristina Fernandes, então chefe deste setor, que fez com que 208
exames de 5 tipos fossem realizados, me apoiando desde o início. Sem vocês este
projeto não seria concluído! À Lukandda Cury Castro, enquanto chefe do unidade
de reabilitação do HUAB, que fez com que minha escala fosse adequada às
necessidades das coletas de dados por 4 meses, e aos colegas do HUAB, pela
torcida constante. Obrigada pela compreensão de sempre! À enfermeira Amanda
Umbelino, que me ajudou recrutando tantas senhoras para que a amostra do estudo
viii

23
vfosse fechada e a Luiz Fernando, que tanto me ajudou com o AGHU, sistema
através do qual conseguimos os contatos das mulheres que haviam sido atendidas
no HUAB. Estendo agradecimentos aos agentes de saúde do município de Santa
Cruz, os quais se empenharam na divulgação do projeto.
Algumas pessoas, mesmo fisicamente distantes, me fizeram manter firme nos
meus propósitos, ao saber que para o que precisasse elas estariam ali. Gabriela
Raulino, grande amiga, incentivadora, e se tivesse uma plateia para aplaudir minhas
conquistas, tenho certeza que ela estaria na primeira fila. Quantas conversas
edificantes tivemos durante essa nossa jornada de doutorandas. Você falando de
Karl Marx e Christian Fuchs, no Rio ou em Londres, e eu, das mulheres santa-
cruzenses e do envelhecimento, mas na intenção sempre, de nos tornarmos
pessoas melhores. Obrigada por compartilhar desta vida comigo! Kalianny Queiroz e
Danielly Melo, corações amigos que, perto ou longe, estão comigo pro que der e
vier, há tanto tempo! Agradeço ainda, à Ana Kelly Almeida, por ser semanalmente
minha dose de equilíbrio e de força, me fazendo enxergar a vida além de um título.
Sou grata à cidade de Santa Cruz e aos tantos ensinamentos que um só lugar
me trouxe, em particular, às 208 mulheres que compuseram a amostra. Esta
pesquisa foi realizada por vocês e para vocês, e eu gostaria muito de oferecer os
benefícios desta ciência gradualmente construída como retorno à esta população,
mesmo que não às mesmas pessoas. Agradeço ainda aos funcionários da FACISA
e HUAB, que permitiram que a coleta de dados fosse possível.
À minha família, por chorarem meu choro e sorrirem meu sorriso, pelo apoio
de sempre e por serem meus exemplos de trabalho digno. Em especial, aos meus
avós Francisca Campelo e Agostinho Guerra, em nome de quem todas minhas
vitórias, desde sempre, serão destinadas. É por vocês que tento ser um ser humano
melhor a cada dia. Meus pais, Ilma Guerra e Francisco Azevedo, pelo dom da vida e
ix
24
por nunca deixarem de acreditar em mim, não medindo esforços para que eu tivesse
tudo o que vocês não tiveram. Ao meu irmão, Igor Guerra Azevedo, por me permitir
ter muito mais que um irmão de sangue, mas um irmão de alma, sendo, por vezes,
meu equilíbrio, minha razão e minha inspiração.
Por fim, agradeço imensamente à toda essa inteligência do universo, que
escreve nossa vida como ela realmente precisa ser. Todas as peças de tantos
questionamentos hoje se juntaram, e tantas respostas tenho de que teria que ser
realmente assim. E ao futuro, a confiança de que todo o porvir é justo e necessário.
Foi esta a minha maior lição, e será nisso que seguirei acreditando!
x

25
Sumário
Lista de figuras xii
Lista de tabelas xiii
Lista de abreviaturas xiv
Lista de apêndices xv
Resumo xvi
Abstract xviii
1. INTRODUÇÃO 21
2. JUSTIFICATIVA 30
3. OBJETIVOS 33
4. MATERIAS E METODOS 35
4.1. Caracterização da pesquisa 36
4.2. Local do estudo 36
4.3. Aspectos éticos 37
4.4 População e amostra 37
4.4. Critérios de elegibilidade 37
4.5. Variáveis do estudo 38
4.6. Instrumentos equipamentos e procedimentos 39
5. RESULTADOS E DISCUSSAO 47
6. CONCLUSÕES 102
7. CONSIDERAÇÕES FINAIS 104
8. REFERÊNCIAS 107
9. APÊNDICES 126
xi

26
Lista de Figuras
Figura 1: Mapa da localização do município de Santa Cruz
xii
27
Lista de tabelas
Tabela 1. Lista das variáveis independentes 38
Tabela 2. Lista das variáveis dependentes 39
Artigo 1
Tabela 1. Características das participantes de acordo com a categoria gestações 73
Tabela 2. Pressões Respiratórias Máximas de acordo com as características das
participantes 74
Tabela 3. Modelos de regressão linear para pressão inspiratória máxima 76
Tabela 4. Modelos de regressão linear para pressão expiratória máxima 77
Artigo 2
Tabela 1. Características das participantes de acordo com prolapso de órgãos
pélvicos 100
Tabela 2. Análise de regressão linear univariada e multivariada para variáveis
associadas à força muscular inspira 101
Tabela 3. Análise de regressão linear univariada e multivariada para variáveis
associadas à força muscular expiratória 101
xiii
28
Lista de abreviaturas e siglas
DIEESE Departamento Intersindical de Estatística e Estudos Econômicos
DMRA Diástase dos músculos retos abdominais
IBGE Instituto Brasileiro de Geografia e Estatística
FMR Força Muscular Respiratória
CVF Capacidade Vital Forçada
VEF1 Volume Expiratório Forçado no 1º Segundo
FEF Fluxo Expiratório Forçado
CRF Capacidade Residual Funcional
VRE Volume de Reserva Expiratório
PImáx Pressão Inspiratória Máxima
PEmáx Pressão Expiratória Máxima
POP Prolapso de Órgão Pélvico
VVM Ventilação Voluntária Máxima
IMC Índice de Massa Corpórea
FACISA Faculdade de Ciências da Saúde do Trairi
HUAB Hospital Universitário Ana Bezerra
TCLE Termo de Consentimento Livre e Esclarecido
Kg Kilograma
OMS Organização Mundial de Saúde
FPP Força de Preensão Palmar
cmH20 Centímetros de água
CPT Capacidade Pulmonar Total
VR Volume Residual
ANOVA Análise de Variância
xiv

29
Lista de Apêndices
Apêndice A Termo de Consentimento Livre e Esclarecido ............................127
Apêndice B Ficha de Avaliação ......................................................................130
xv
30
Resumo
Introdução: A história reprodutiva feminina e disfunções do assoalho pélvico tem
contribuído para as alterações físicas que aparecem no envelhecimento, como as
alterações precoces na capacidade funcional de mulheres. Desta forma, investigar a
história reprodutiva feminina e prolapso de órgãos pélvicos (POP) sintomático, e sua
relação coma força muscular respiratória se torna de grande necessidade para a
instituição de tratamento e acompanhamento adequado dessa musculatura.
Objetivo: Avaliar a relação da força muscular respiratória com variáveis da história
reprodutiva e POP sintomático, em mulheres de meia idade e idosas residentes na
comunidade. Métodos: Foram estudadas 208 mulheres entre 41-80 anos, nas
cidades de Santa Cruz - RN. Os sujeitos foram recrutados por conveniência e após
consentimento, a avaliação foi realizada. Foram coletados dados sociodemográficos,
medidas antropométricas, hábitos de vida, história reprodutiva, alterações de
assoalho pélvico (todas essas variáveis por questionário estruturado para esta
pesquisa), avaliação do desempenho físico (através do IPAQ – versão curta) e
avaliação da força muscular respiratória (manovacuometria), através das pressões
inspiratória máxima (PImáx) e expiratória máxima (PEmáx). Resultados: Mais de
noventa porcento (90,4%) das mulheres com com sete ou mais filhos tiveram menos
que escolaridade básica, enquanto 80,8% desse grupo recebiam menos que três
salários mínimos. Aproximadamente 44,1% da amostra tiveram três gestações ou
menos, 30,4% tiveram 4-6 gestações e 25,5% tiveram mais que sete gestações. As
mulheres com sete gestações ou mais são mais velhas que as mulheres do grupo
com três filhos ou menos gestações. Quanto à PImáx, aquelas que tiveram sete ou
mais gestações tinham mais de 12 cmH2O a menos quando comparadas a aquelas
que tiveram sete gestações ou mais (β=-12,29; p=0,233). Considerando a PEmáx,
aquelas que tiveram sete ou mais gestações tinham mais de 21 cmH2O a menos
xvi

31
quando comparadas a aquelas que tiveram sete gestações ou mais (β= -21,69;
p<0,001). Com relação ao POP, 14,7% das mulheres apresentaram prolapso de
órgão pélvico (POP) sintomático. O POP sintomático não foi associado à PImáx. As
variáveis idade, escolaridade, IMC, tabagismo e paridade foram associadas à PImáx
na análise univariada, mas apenas idade, IMC e tabagismo são determinantes de
PImáx no modelo multivariado. No modelo univariado, POP sintomático, idade,
escolaridde, IMC e paridade foram associados à PEmáx. As mulheres com POP
sintomático apresentaram PEmáx mais baixa quando comparadas às mulheres sem
esta condição (β = -14,78; p = 0,014). As mulheres com maior idade e maior número
de filhos (≥ 5 crianças) obtiveram piores valores de PEmáx, e aquelas com maior
IMC e mais anos de estudos (> 7 anos), valores mais elevados, na análise
univariada. No modelo multivariado, apenas idade, IMC e POP sintomático são
determinantes para a PEmáx. Conclusão: Este estudo traz evidências de que as
múltiplas gestações e POP sintomático influenciam a força muscular respiratória,
uma vez que mulheres com maior número de gestações e com POP sintomático têm
valores mais baixos de pressões respiratórias máximas. Ainda, outras variáveis,
como o IMC e o tabagismo possuem relação com a capacidade de gerar pressões
respiratórias.
Palavras-chave: História reprodutiva, prolapso de órgãos pélvicos, força muscular
respiratória, epidemiologia, envelhecimento.
xvii
32
Abstract
Background: Female reproductive history and pelvic floor dysfunction have
contributed to the physical changes that appear in aging, such as early changes in
the functional capacity of women. Thus, investigating the female reproductive history
and symptomatic pelvic organ prolapse (POP), and its relationship with respiratory
muscle strength, becomes a great necessity for the institution of treatment and
adequate monitoring of this musculature. Objective: To assess the relationship of
respiratory muscle strength with variables of reproductive history and pelvic floor
prolapse in middle-aged and elderly women living in the community. Methods: A
total of 208 women aged 41-80 years were studied in the cities of Santa Cruz - RN.
The subjects were recruited for convenience and after consentment, the evaluation
was performed. Socio-demographic data, anthropometric measures, life habits,
reproductive history, pelvic floor changes (all variables by structured questionnaire
for this research), physical performance evaluation (through IPAQ - short version)
and respiratory muscle strength (manovacuometry), through maximal inspiratory
pressure (MIP) and maximal expiratory pressure (MEP). Results: More than ninety
percent (90.4%) of the women with seven or more children had less than basic
education, while 80.8% of this group received less than three minimum wages.
Approximately 44.1% of the sample had three pregnancies or less, 30.4% had 4-6
pregnancies and 25.5% had more than seven pregnancies. Women with seven or
more pregnancies are older than women in the group with three children or fewer
pregnancies. As for MIP, those who had seven or more pregnancies had more than
12 cmH2O less when compared to those who had seven or more pregnancies (β = -
12.29; p = 0.233). Considering MEP, those who had seven or more pregnancies had
more than 21 cmH2O less when compared to those who had seven or more
xviii
xviii
33
pregnancies (β = -21.69, p <0.001). Regarding POP, 14.7% of the women presented
symptomatic POP, which was not associated with MIP. The variables age, schooling,
BMI, smoking and parity were associated with MIP in the univariate analysis, but only
age, BMI and smoking are determinants of MIP in the multivariate model. In the
univariate model, symptomatic POP, age, schooling, BMI and parity were associated
with MEP. Women with symptomatic POP presented lower MEP when compared to
women without this condition (β = -14.78; p = 0.014). Women with greater age and
greater number of children (≥ 5 children) had worse values of MEP, and those with
higher BMI and more years of studies (> 7 years), higher values, in the univariate
analysis. In the multivariate model, only age, BMI and symptomatic POP are
determinants for MEP. Conclusion: This study provides evidence that multiple
pregnancies and symptomatic POP influence the respiratory muscle strength, since
women with more gestations and with symptomatic POP have lower values of
maximum respiratory pressures. Still, other variables such as BMI and smoking are
related to the capacity to generate respiratory pressures.
Keywords: Maximal respiratory pressures; childbearing; pelvic organ prolapse;
aging; global health.
xix

34
1. INTRODUÇÃO
21
1.1 O Envelhecimento Populacional e a Feminização da população idosa
Segundo os dados do Instituto Brasileiro de Geografia e Estatística
(IBGE), 2013, no Brasil, o segmento populacional que mais cresce é o de
idosos, com taxas de crescimento de mais de 4% ao ano, no período de 2012
a 2022. A população com 60 anos ou mais de idade passa de 14,2 milhões
em 2000, para 19,6 milhões em 2010, devendo atingir 41,5 milhões em 2030,
e 73,5 milhões em 2060 (IBGE, 2013). Espera-se, para os próximos 10 anos,
um incremento médio de mais de 1,0 milhão de idosos anualmente (IBGE,
2013).
Essa situação de envelhecimento populacional é consequência,
primeiramente, da rápida e contínua queda da fecundidade no país, além de
ser também influenciada pela queda da mortalidade em todas as idades (WHO,
2015). Em 2000, a expectativa de vida aos 60 anos de idade era 18,9 anos
para ambos os sexos (IBGE, 2013). É estimado que em 2030 haja um
acréscimo de 25,6 anos, atingindo, em média, a idade de 85,6 anos. Se
homem, a sobrevida média aos 60 anos passará de 16,9 anos para 23,2 anos.
Se mulher, passará de 20,7 anos para 27,9 anos (IBGE, 2013).
O processo de envelhecimento é dinâmico e progressivo, influenciado
pela idade, por fatores fisiológicos, sociais e biológicos (SANTOS et al., 2011).
Entre 2000 e 2050, a proporção da população mundial acima de 60 anos vai
dobrar de cerca de 11% para 22% (WHO, 2015). Nesse período, é esperado
um aumento de 605 milhões para 2 bilhões de pessoas com 60 ou mais anos
(WHO, 2015).
Atrelado ao processo de envelhecimento, ocorre o aparecimento de
doenças e agravos crônicos, isolados ou associados (comorbidades). Tais

22
condições crônicas podem afetar a funcionalidade do idoso, dificultando o
desenvolvimento das atividades de vida diária (AVDs), de forma independente
e influenciando diretamente na sua qualidade de vida (INOUYE et al., 2007). A
possibilidade de incapacidade e dependência funcional está relacionada, entre
outros fatores, com a redução da massa muscular – denominada sarcopenia –
que acontece lenta e progressivamente durante o processo de envelhecimento
(JANSEN; ROSS, 2005; SILVA et al., 2006).
Como supracitado, o aumento da população idosa, no Brasil, se dá de
forma rápida e progressiva, sendo maior o número de idosas que de idosos
(IBGE, 2013). Já no cenário mundial, quando o sexo feminino constitui maioria
das pessoas idosas, mesmo que a velhice não seja universalmente feminina,
possui um forte componente desse gênero (CARVALHO; WONG, 2008).
Em 2000, para cada 100 mulheres idosas, havia 81 homens idosos no
Brasil (CARVALHO; WONG, 2008). Estima-se que, em 2050, essa relação será
de 100 idosas para 76 idosos do sexo masculino. Entre os mais idosos,
aqueles com 80 anos ou mais, essa diferença se torna mais evidente, uma vez
que para cada 100 mulheres, o número de homens deverá cair entre 2000 e
2050, de 71 para 61 (CARVALHO; WONG, 2008). Haveria, portanto, em
meados do século, quase duas mulheres para cada homem, entre os idosos
mais idosos (CARVALHO; WONG, 2008).
Apesar da população feminina apresentar maior expectativa de vida se
comparada à população masculina, ela vive mais tempo com situações
crônicas, o que limita sua capacidade física e, consequentemente, sua
qualidade de vida (SANTOS et al., 2011). Com o envelhecimento, o gênero
feminino é mais afetado que o masculino, tornando-se as mulheres mais
23
vulneráveis, não apenas aos problemas de saúde, mas ao isolamento social e
a transtornos emocionais, devido a aspectos como a aposentadoria, a viuvez e
às alterações fisiológicas (LIMA, 2009). Tal fato aponta que há peculiaridades
no envelhecimento feminino, as quais precisam de atenção por pesquisadores
e profissionais de saúde (LIMA, 2009).
Alguns fatores conseguem explicar as diferenças existentes no
envelhecimento entre os gêneros, como os diferentes hábitos de vida entre
homens e mulheres, os valores e comportamentos que contribuem para as
diferenças de nível de escolaridade e, consequentemente, de condição
socioeconômica, a diferença na prática de atividade física ao longo da vida, o
tabagismo e hábitos alimentares, que podem predispor as mulheres à
decadência física e incapacidade (GREGORY, 2013; GREGORY, 2011).
Além de uma pior qualidade de vida (SANTOS et al., 2011), a força e
massa muscular começam a apresentar certa debilidade, de maneira mais
precoce nas mulheres, quando comparadas aos homens (HANSEN et al.; et
al., 2011). É apontado que questões hormonais, em particular, os hormônios
sexuais, tem forte influência sobre a força muscular esquelética, o que poderia
explicar a diferença de gênero no declínio da força muscular periférica
(SOWERS et al., 2007). Sabendo-se que o envelhecimento feminino é
caracterizado por grandes alterações hormonias, torna-se de grande
importância, além da musculatura periférica, investigar a força muscular
respiratória e sua realação com fatores que podem influenciá-la. A FMR está
associada com a mobilidade (BUCHMAN et al., 2008) e a fatores adversos
realcionados à saúde no processo de envelhecimento (FRAGOSO; GILL,
2012). Portanto, necessita ser investigada a fim de se evidenciar maneiras de
24
intervir e melhorar sua associação com o envelhecimento.
1.2 Relações da força muscular respiratória com o envelhecimento
Dentre as várias alterações que o processo de envelhecimento ocasiona
no organismo, há mudanças consideráveis no sistema respiratório (OSKVIG,
1999), podendo levar ao declínio da capacidade vital forçada (CVF), volume
expiratório forçado no 1º segundo (VEF1) e fluxo expiratório forçado (FEF), bem
como aumento na capacidade residual funcional (CRF) e volume de reserva
expiratório (VRE). Estes parâmetros se relacionam com a redução no
recolhimento elástico pulmonar e com a diminuição da complacência da caixa
torácica (MATSUDO, 1992; JANSSENS, 1999; VAN GEEL et al., 2009).
Além das alterações supracitadas, em se tratando do sistema
musculoesquelético, há alterações na força muscular com hipotrofia da
musculatura esquelética, o que compromete, principalmente, as fibras tipo II
(fibras de força) (NAIR, 2005; TOLEP, 1995). Desta forma, seguindo o
processo de envelhecimento e atrelado a todas as demais alterações
volumétricas e torácicas que acontecem no idoso, a força muscular respiratória
também diminui (OFIR, 2008; SIMÕES, 2010; WATSFORD, 2005). Tolep e
colaboradores (1995) relataram, ainda, uma redução de até 25% na força
diafragmática de idosos, comparados com adultos jovens.
É conhecido que alguns fatores influenciam a FMR. Sabe-se que existe
diferença entre os gêneros, quando os homens apresentam valores superiores
de pressões respiratórias máximas (OFIR, 2008). Além disso, tais valores são
maiores em pessoas mais jovens e não obesas, evidenciando relação negativa
entre a idade e a FMR (ENRIGHT et al., 1994; JENSEN, 2009; NEDER et al.,
25
1999; OFIR, 2008), bem como com a obesidade (JENSEN, 2009). Ofir e
colaboradores, em 2008, avaliaram 73 sujeitos saudáveis, com idade entre 40-
80 anos, e observaram diferenças significativas nas forças musculares
expiratória e inspiratória entre homens e mulheres, separados em grupo de 40-
59 anos e 60-80 anos. As forças musculares respiratórias foram maiores no
gênero masculino (p< 0,0005) e no grupo de indivíduos mais jovens (p= 0,003).
Pesquisas tem mostrado que a redução nos níveis de estrógeno faz com
que as mulheres tenham um declínio acelerado da força, na época da
menopausa, sugerindo que os hormônios sexuais podem ser o ponto mais
importante para a diferença de gênero na força muscular periférica (SOWERS
et al., 2007). Corroborando com esta hipótese, evidências identificaram que há
uma influência positiva dos hormônios sexuais femininos sobre a função
pulmonar (LIEBERMAN et al., 1995; SHARMA; GOODWIN, 2006). Ainda
considerando questões hormonais, mulheres de baixa renda tendem a entrar
na menopausa mais precocemente, o que pode ser consequência da
desregulação do balanço hormonal reprodutivo da mulher promovida pelo
aumento da secreção de glicocorticoides, em resposta a agentes estressores
(VÉLEZ et al., 2010).
A gravidez, por exemplo, causa alterações à fisiologia da mulher e
aumenta as demandas metabólicas no corpo (KING, 2000). Adicionalmente, há
consequências fisiológicas e sociais relacionadas à história reprodutiva,
contribuindo para o aumento de agentes estressores a serem enfrentados ao
longo da vida pela mulher (VÉLEZ et al., 2010), o que reflete diretamente a
influência de variáveis da história reprodutiva sobre o organismo feminino.
Múltiplos partos ou uma gravidez ainda durante o período da adolescência,
26
alteram a fisiologia da mulher (PIRKLE et al., 2014). Isto pode levar a
alterações nas musculaturas das regiões abdominal e em torno dos quadris,
contribuindo para a maior dificuldade na realização de atividades funcionais e
geração de força muscular (WALL, 1999). Porém, a influência direta dessas
variáveis sobre a FMR ainda é desconhecida, o que requer, portanto,
investigação.
1.3 Impacto da história reprodutiva feminina no estado de saúde,
funcionalidade e força muscular respiratória
Evidências apontam que aspectos da história reprodutiva da mulher,
como a o número de filhos e a idade que a mulher teve seu primeiro parto,
apresentam impacto na saúde e capacidade funcional dessa população
(CÂMARA et al., 2015; PIRKLE et al., 2014). Câmara e col. (2015), em uma
população com 473 mulheres de meia-idade do município de Parnamirim, RN,
concluíram que aquelas cujo primeiro filho nasceu antes de seus 18 anos, ou
que tiveram mais de 3 filhos, apresentaram pior desempenho físico quando
comparadas com as demais.
Além de pior desempenho físico, um estudo prévio encontrou que
mulheres que tiveram seu primeiro filho precocemente (ainda na fase da
adolescência) apresentam maior risco de desenvolver doenças crônicas em
idades mais avançadas (PIRKLE et al., 2014). O estudo de PIRKLE et al.,
2014, que avaliou mulheres de localidades com diferentes condições
socioeconômicas (Canadá, Albânia, Colômbia e Brasil), evidenciou que
variáveis da história reprodutiva feminina aumenta o risco de desenvolver

27
doenças crônicas, incluindo doença pulmonar crônica, e evidencia maiores
limitações funcionais durante fases mais avançadas da vida.
Outras evidências apontam que a idade materna precoce com que se
tem o primeiro filho, e a quantidade de filhos que se tem, podem predispor o
organismo feminino a uma situação crônica de estresse, o que pode contribuir,
então, para o risco de doenças cardiovasculares e diabetes (MUELLER et al.,
2013; PARIKH et al., 2010). Alguns estudos observaram associações entre
eventos reprodutivos femininos, como idade materna precoce no primeiro
nascimento, com a função respiratória (HERENTTA, 2007; PIRKLE et al, 2014),
mas apenas relataram os resultados com poucas observações sobre os
possíveis motivos do observado nas associações.
A maioria dos estudos que investiga a relação da história reprodutiva
com a funcionalidade feminina leva em consideração o desempenho da
musculatura periférica (membros superiores e inferiores) (CÂMARA et al.,
2015; CHENG et al., 2009; PIRKLE et al., 2014; TSENG et al., 2012). Apenas
poucos estudos trazem a relação entre a história reprodutiva e variáveis
pulmonares, como as capacidades e volumes pulmonares (BEN SAAD et al.,
2006) e as doenças respiratórias (HENRETTA, 2007; KRZYZANOWSKI et al.,
1986).
BEN SAAD et al. (2006) estudaram mulheres tunisianas acima de 45
anos com o objetivo de analisar os fatores que influenciam a função pulmonar e
a força muscular inspiratória, em mulheres saudáveis e, em particular,
determinar o efeito da paridade sobre as variáveis respiratórias. Esses autores
concluíram que as variáveis da função pulmonar diminuem com o aumento da
paridade, e atribuem essa associação a muitas causas possíveis associadas a
28
gravidezes múltiplas. Dentre as possíveis causas, estão as alterações
hormonais cumulativas (por exemplo, o aumento do cortisol), modificações
anatômicas no tórax e nos músculos respiratórios, derivados do aumento
repetitivo do útero, sendo todas essas alterações resultantes de gestações
repetidas.
Sabe-se que, durante a gravidez, o aumento do volume uterino leva a
uma alteração na configuração do tórax e, consequentemente, há uma
alteração da biomecânica dos músculos respiratórios (GILORY et al., 1988). Os
efeitos destas alterações podem ser combinados com as repetidas gravidezes,
interferindo, pois, na função pulmonar e força muscular respiratória (BEN SAAD
et al., 2006). Além disso, mulheres que começam precocemente a ter filhos, e
que geram várias crianças, acumulam excesso de peso durante o curso da sua
vida, além do acúmulo de estresse, que leva a alterações fisiológicas, como
aumento de massa gorda, disfunção metabólica, resistência à insulina,
dislipidemia e inflamação (KAAJA; GREER, 2005), contribuindo para o
aumento da mortalidade em decorrência de doenças pulmonares (HENRETTA,
2007).
Dentre as várias condições de saúde às quais estão relacionadas, a
multiparidade e a obesidade estão associadas ao aparecimento de disfunções
do assoalho pélvico, como o prolapso de órgão pélvico (GIRI et al, 2017; WU et
al, 2014). Há uma maior prevalência deste transtorno com o aumento da
paridade (WU et al, 2014). Adicionalmente, mulheres com sobrepeso e
obesidade têm maior probabilidade de prolapso de órgãos pélvicos (GIRI et al,
2017).
29
Embora a causa do prolapso do órgão pélvico seja multifatorial, ela está
principalmente associada a episódios sustentados de aumento da pressão
intra-abdominal, o que acontece em repetidas gestações e em casos de
obesidade, além de tosse crônica e constipação (IGLESIA; SMITHLING, 2017).
Considerando que os músculos do assoalho pélvico são parte de um conjunto
de músculos chamado core (AKUTHOTA; NADLER, 2004) e que alterações em
qualquer um deles pode alterar a função um do outro (AKUTHOTA; NADLER,
2004), torna-se importante investigar a influência de distúrbios do assoalho
pélvico, como o prolapso de órgãos pélvicos sintomático, na força muscular
respiratória, sobre a qual o diafragma e os músculos abdominais, também parte
do core, tem participação primária (WEST, 2013).
Partindo do pressuposto que a história reprodutiva e queixas urinárias
estão associadas à capacidade funcional de mulheres de meia idade e idosas
(DA CÂMARA et al., 2015; PIRKLE et al., 2014; SANSES et al., 2016) e
sabendo-se que a FMR é um dos fatores que pode influenciar a funcionalidade
no processo de envelhecimento (BUCHMAN et al., 2008; SIMÕES et al., 2010),
torna-se importante investigar como esses fatores estão associados com a
capacidade de gerar pressões respiratórias mais tarde no curso da vida.

30
2. JUSTIFICATIVA
31
Sabe-se que o processo de envelhecimento ocasiona um declínio geral
na capacidade funcional e qualidade de vida dos indivíduos. O envelhecimento
feminino, em si, deve ser estudado de forma diferenciada, visto que esta
população é submetida a várias alterações fisiológicas com o fenômeno da
menopausa e de sua história reprodutiva. As mulheres são a maior parte da
população idosa mundial e, embora vivam por mais tempo, quando
comparadas ao gênero masculino, apresentam piores resultados de saúde e de
desempenho físico.
Desta forma, torna-se necessário conhecer fatores que possam interferir
especificamente no processo de envelhecimento feminino e, particularmente,
na força muscular respiratória, visto que muitas são as consequências
originadas de um quadro de fraqueza desse grupo específico de músculos.
No que diz respeito à musculatura periférica, já é bem estabelecido em
diferentes populações que há alterações na capacidade funcional feminina, em
associação com a história reprodutiva. Porém, no que se trata de musculatura
respiratória, poucos estudos trazem a associação de variáveis de força
muscular respiratória com variáveis da história reprodutiva, como o número de
gestações e a idade com que a mulher teve seu primeiro filho. Dessa forma,
estudar esse público, de forma a avaliar tais variáveis e, assim, evidenciar
associações com as pressões respiratórias, oferece à comunidade científica o
conhecimento de como abordar integral e especificamente as condições que
interferem no processo de envelhecimento, no que diz respeito não somente à
musculatura periférica, mas também, a respiratória.
Sendo assim, considerando que no Brasil e no mundo, a população
idosa é predominantemente feminina, que as mulheres compõem as principais
32
usuárias de serviços de saúde, gerando impactos consideráveis na sua
qualidade de vida, torna-se de extrema importância o estudo desses fatores,
objetivando traçar estratégias para prevenção e tratamento de condições
específicas direcionadas a esta população em particular.
Deste modo, pesquisas que abordem essas possíveis associações entre
o envelhecimento feminino e a força muscular respiratória devem ser
estimuladas e fomentadas, contribuindo assim, para o avanço dessa temática.
Diante da escassez de estudos que evidenciem essas relações, em mulheres,
tem-se a necessidade de estudar mais profundamente essa população e,
assim, evidenciar pontos ainda não esclarecidos, relacionados ao impacto da
história reprodutiva, disfunções do assoalho pélvico (prolapso de órgãos
pélvicos) e condição socioeconômica. Desta forma, espera-se obter evidências
que ajudem a embasar e estabelecer estratégias de intervenção voltadas para
esta população.

33
3. OBJETIVOS

34
3.1. Objetivo Geral
Avaliar a relação da força muscular respiratória com variáveis da história
reprodutiva e prolapso de órgãos pélvicos sintomático, em mulheres de meia
idade e idosas residentes na comunidade.
3.2. Objetivos Específicos
3.2.1. Comparar a força muscular respiratória de mulheres de meia idade e
idosas com diferentes números de gestações;
3.2.2. Avaliar a relação entre a força muscular respiratória e as variáveis
socioeconômicas, variáveis de saúde e hábitos de vida;
3.2.3. Verificar as relações entre a força muscular respiratória e prolapso de
órgãos pélvicos sintomático em mulheres de meia-idade e idosas;
3.2.4. Avaliar se a relação entre prolapso de órgãos pélvicos sintomático e
história reprodutiva com a força muscular respiratória se mantém após o
controle por variáveis de confundimento.

35
4. MATERIAIS E MÉTODOS
36
4.1 Caracterização da pesquisa
Esta pesquisa caracteriza-se por ser do tipo observacional analítica e
tem caráter transversal.
4.2 Local da pesquisa
A pesquisa foi desenvolvida na cidade de Santa Cruz/RN, localizada a
120km de Natal, capital do estado (figura 1). A coleta dos dados foi realizada
na Faculdade de Ciências da Saúde do Trairi (FACISA) e no Hospital
Universitário Ana Bezerra (HUAB), ambos localizados no município de Santa
Cruz/RN. A cidade de Santa Cruz possui uma população de cerca de 40,000
habitantes, segundo a projeção para 2017 (IBGE), apresentando
aproximadamente 624,356 km2 (IBGE).
Figura 1: Mapa da localização do município de Santa Cruz.
37
4.3 Aspectos Éticos
Esta pesquisa faz parte de um estudo observacional longitudinal
denominado “Influência do status menopausal e dos níveis hormonais na
funcionalidade, força muscular e composição corpórea: um estudo longitudinal”.
O presente estudo obteve aprovação no Comitê de Ética em Pesquisa, com
parecer n. 1.875.802, estando de acordo com a resolução 466/12 do Conselho
Nacional de Saúde. Todos os sujeitos receberam esclarecimentos sobre os
procedimentos da pesquisa e assinaram o termo de consentimento livre e
esclarecido (TCLE) (Apêndice A).
4.4 População e Amostra
A presente pesquisa se propôs a avaliar mulheres com idade entre 40 e
80 anos, residentes no município de Santa Cruz-RN. Para composição da
amostra, foi realizada divulgação do projeto nas unidades básicas de saúde,
no HUAB, bem como centros comunitários, convidando as mulheres a
participar. Após a avaliação dos critérios de elegibilidade descritos abaixo, 208
mulheres (sendo 104 mulheres de 41-60 anos e 104 mulheres de 61-80 anos)
foram selecionadas para fazerem parte do estudo.
4.5 Critérios de Elegibilidade
4.5.1 Critérios de Inclusão
Foram incluídas no estudo mulheres com idade entre 41-80 anos,
residentes no município de Santa Cruz/RN, com capacidade de se deslocar até
o local da avaliação.
38
4.5.2. Critérios de Exclusão
Foram considerados critérios de exclusão não completar todas as etapas
do processo de avaliação ou desistência, mulheres com alterações motoras
e/ou doenças degenerativas que impedissem a realização dos testes e com
alterações cognitivas identificadas por 4 erros ou mais na Prova Cognitiva de
Leganés (DE YEBENES et al., 2003).
4.6. Variáveis do estudo
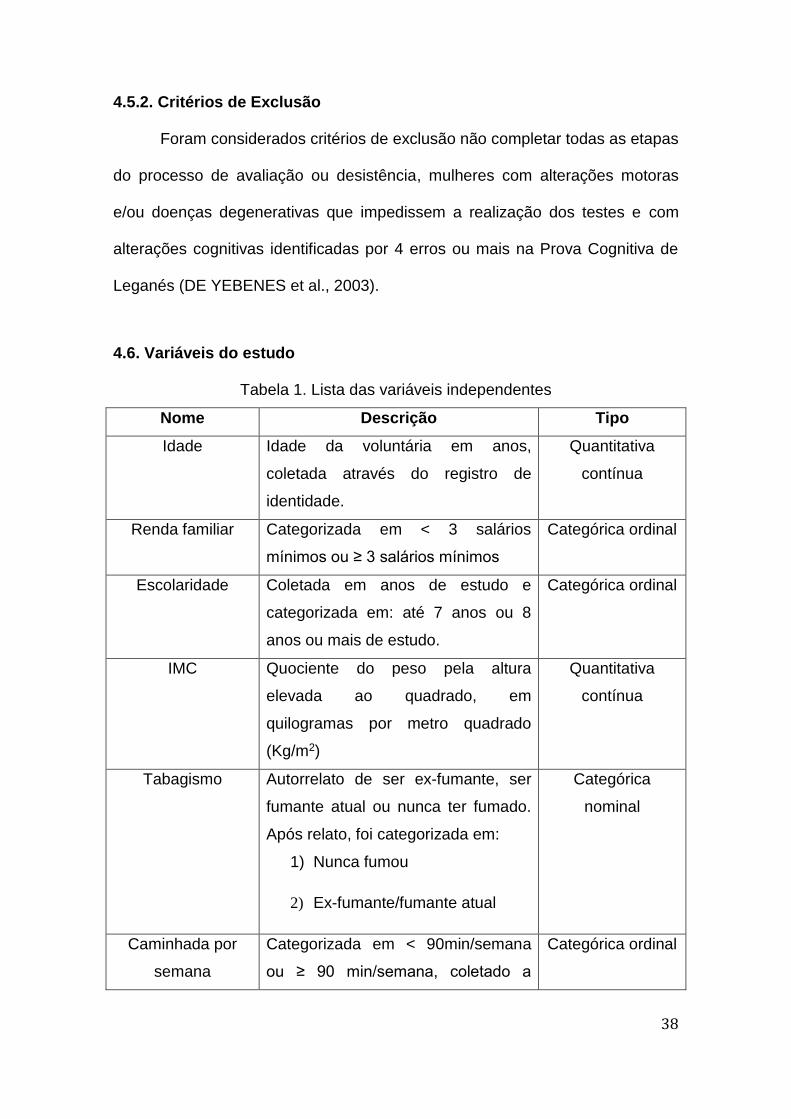
Tabela 1. Lista das variáveis independentes
Nome Descrição Tipo
Idade Idade da voluntária em anos,
coletada através do registro de
identidade.
Quantitativa
contínua
Renda familiar
Categorizada em < 3 salários
mínimos ou ≥ 3 salários mínimos
Categórica ordinal
Escolaridade Coletada em anos de estudo e
categorizada em: até 7 anos ou 8
anos ou mais de estudo.
Categórica ordinal
IMC Quociente do peso pela altura
elevada ao quadrado, em
quilogramas por metro quadrado
(Kg/m2)
Quantitativa
contínua
Tabagismo Autorrelato de ser ex-fumante, ser
fumante atual ou nunca ter fumado.
Após relato, foi categorizada em:
1) Nunca fumou
2) Ex-fumante/fumante atual
Categórica
nominal
Caminhada por
semana
Categorizada em < 90min/semana
ou ≥ 90 min/semana, coletado a
Categórica ordinal
39
partir do questionário IPAQ, versão
curta
Tempo sentada por
dia
Categorizado em até 4h/dia ou mais
de 4h/dia, a partir de coleta pela
versão curta do IPAQ
Categórica ordinal
Gestações Autorrelato da quantidade de filhos,
sendo categorizada em: ≤3
gestações; 4-6 gestações ou ≥7
gestações
Categórica ordinal
Idade materna ao
primeiro filho
Autorrelato da idade que tinha ao
parir o primeiro filho, sendo
categorizada em:
Nulípara; < 18 anos de idade; ≥18
anos de idade.
Categórica ordinal
Prolapso de órgão
pélvico
Autorrelato da sensação de peso na
vagina, categorizada em “sim” ou
“não”.
Categórica
nominal
Paridade Autorrelato da quantidade de filhos,
sendo categorizado em:
Menos que cinco filhos; cinco filhos
ou mais.
Categórica ordinal
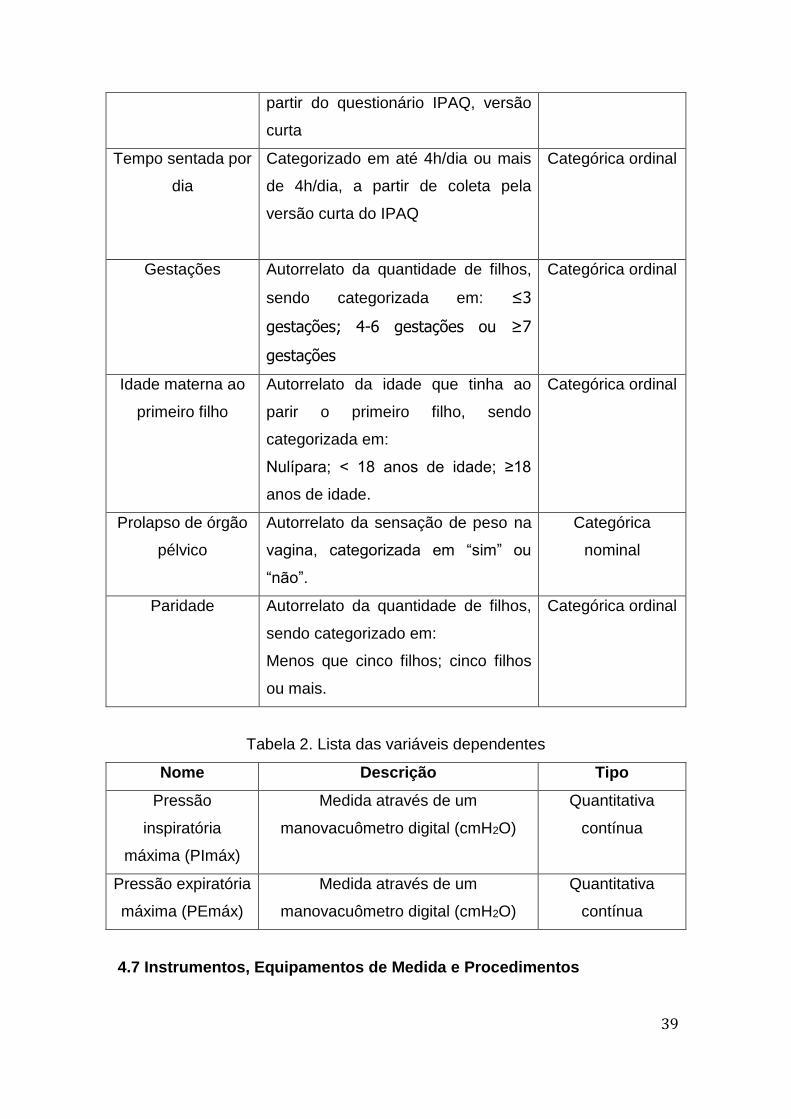
Tabela 2. Lista das variáveis dependentes
Nome Descrição Tipo
Pressão
inspiratória
máxima (PImáx)
Medida através de um
manovacuômetro digital (cmH2O)
Quantitativa
contínua
Pressão expiratória
máxima (PEmáx)
Medida através de um
manovacuômetro digital (cmH2O)
Quantitativa
contínua
4.7 Instrumentos, Equipamentos de Medida e Procedimentos
40
Antes de iniciar a coleta de dados, foi realizado treinamento com os
entrevistadores (estudantes de graduação e pós-graduação em Fisioterapia)
dos protocolos de avaliação, quando todos os questionários e procedimentos
foram uniformizados.
Posteriormente à etapa de treinamento, realizou-se a divulgação do
projeto no Hospital Universitário Ana Bezerra, nas Unidades Básicas de Saúde
do município de Santa Cruz e na Clínica Escola da FACISA. Após contato
inicial com as mulheres, elas foram instruídas quanto aos procedimentos a
serem executados e objetivos da pesquisa, além de convidadas a assinarem o
TCLE.
Uma vez concordando em participar do estudo, as voluntárias foram
avaliadas por meio de um questionário estruturado, desenvolvido para esta
pesquisa (APÊNDICE B), seguindo os procedimentos descritos a seguir.
4.7.1 Dados sociodemográficos e antropométricos
Inicialmente, as voluntárias foram avaliadas quanto aos dados
sociodemográficos como idade, escolaridade e renda familiar. A idade foi
autorrelatada, mas conferida através do documento de identificação. A
escolaridade, por sua vez, foi coletada em anos de estudo e categorizada em
até sete anos de estudo ou mais que sete anos de estudo, como forma de
dividir aquelas que tiveram menos que o ensino fundamental como
escolaridade das demais. Já a renda familiar foi coletada em valores brutos e
categorizada tomando como base o salário mínimo brasileiro do momento da
entrevista, valor assinalado na corrente moeda brasileira de R$ 880,00
(Oitocentos e oitenta reais). A partir disto, a renda familiar foi categorizada em

41
menos que três salários mínimos (SM) ou três salários mínimos ou mais. As
categorias para renda de menos de três SM ou três/mais SM se deu na
tentativa de separar aquelas mulheres que possuíam renda insuficiente para
atender as necessidades de uma família das demais. Segundo o DIEESE
(Departamento Intersindical de Estatística e Estudos Econômicos) o valor do
salário mínimo na época da entrevista deveria ser pelo menos quatro vezes
maior para poder atender as necessidades básicas de uma família no Brasil em
relação à alimentação, moradia, higiene e transporte (BRASIL, 2017).
Posteriormente, as voluntárias foram avaliadas quanto ao peso e altura.
Para a medida de peso (kg) foi utilizada uma balança digital, de fabricação
nacional, da marca Welmy®, Modelo W100H, e estadiômetro para registro da
altura (m), que foram utilizados para o cálculo do IMC (kg/m2).
4.7.2 Hábitos de vida
As mulheres foram questionadas sobre os seus hábitos de vida, como
tabagismo e prática de atividade física. As questões sobre tabagismo estão
presentes no questionário estruturado usado para esta pesquisa, como
anteriormente mencionado. Desta forma, as mulheres foram categorizadas e
dois grupos: ex-fumantes e/ou fumantes atuais ou nunca fumantes.
As voluntárias foram também questionadas sobre a realização de
caminhada e tempo gasto por dia na posição sentada, como forma de
caracterizar a atividade sedentária. Tais dados foram coletados seguindo as
orientações do questionário IPAQ versão curta (anexado à ficha de avaliação
do APÊNDICE B) (CRAIG et al., 2003; MATSUDO et al., 2001). Para a variável
caminhada por semana, as mulheres foram instruídas a relatar quantos dias, e

42
quanto tempo por dia, elas caminharam por mais de dez minutos sem parar,
durante a última semana, seja como forma de ir de um lugar a outro ou como
exercício físico. A partir das suas respostas, as voluntárias foram alocadas
dentro de uma das duas categorias: menos de 90 min/semana e 90
min/semana ou mais (CÂMARA et al., 2015). Para o tempo sentada por dia, as
mulheres foram solicitadas a informar quanto tempo, em um dia normal, elas
ficavam sentadas, seja em casa ou no trabalho, descansando, assistindo
televisão ou lendo, e a variável foi dicotomizada em 4 h/dia ou menos, e mais
do que 4 h/dia (CÂMARA et al., 2015; GÓMEZ-CABELLO et al., 2012). De
acordo com GÓMEZ-CABELLO et al., 2012, ficar sentado por mais de 4 horas
por dia aumenta o risco de sobrepeso, obesidade e obesidade central,
independente das horas caminhadas. As categorias de variáveis ‘tempo de
caminhada por semana’ e ‘tempo sentada por dia’ foram baseadas em achados
de uma amostra de mulheres entre 40-65 anos, realizado no município de
Parnamirim, no Rio Grande do Norte, do qual este estudo faz parte (CÂMARA
et al., 2015).
4.7.3 História reprodutiva
As variáveis ‘idade materna no primeiro parto’ e ‘número de gestações’
foram coletadas por autorrelato. O número de gestações foi categorizado como
≤3 gestações, 4-6 gestações ou ≥7 gestações. A categorização desta variável
foi baseada em estudos que avaliaram a paridade. As mulheres com 3 ou mais
filhos apresentam pior desempenho físico (CÂMARA et al., 2015) e maior
chance de desenvolver doenças crônicas (PIRKLE et al., 2014). Além disso,
existe uma associação positiva entre o número de gestações e o risco de

43
doença coronariana (PARIKH et al, 2010). Uma vez que 25% de nossa amostra
relatou ter tido mais de 7 gestações ao longo da vida (TOOHEY et al., 1995),
utilizamos esse ponto de corte para a criação da terceira categoria. Estudos
sugerem (RAYAMAJHI; THAPA; PANDE, 2006; ABU-HEIJA; CHALABI, 1998)
que mulheres com mais de 5 filhos (grande multíparas) apresentam um risco
ainda maior de resultados adversos para a saúde.
A fim de categorizar se a mulher teve seu primeiro filho quando
adolescente ou idade adulta, sua idade quando teve o primeiro filho foi dividida
como <18 anos ou ≥ 18 anos (CÂMARA et al., 2015), ou ainda, se não teve
filhos foi considerada como nulípara. A gravidez na adolescência está
relacionada a uma maior ocorrência de complicações obstétricas e pode causar
danos à vida da mulher, uma vez que ocorre em uma fase da vida em que elas
ainda podem não ter acumulado reservas fisiológicas suficientes para a
gravidez e parto saudáveis (ALLAL et al., 2004).
4.7.4 Força Muscular Respiratória
A força muscular respiratória pode ser diretamente medida usando
pressões estáticas máximas (pressão inspiratória máxima – PImáx e pressão
expiratória máxima – PEmáx) ou, ainda, pode ser inferida por manobras
dinâmicas, como a ventilação voluntária máxima (VVM) (BLACK E HYATT,
1969; RUPPEL, 1994). A determinação de PImáx e PEmáx trata-se de um
método simples, prático e eficaz para a avaliação da musculatura respiratória,
sendo uma ferramenta importante no cotidiano do fisioterapeuta
pneumofuncional (FREITAS, 2010).
44
PImáx e PEmáx são, respectivamente, a maior pressão que pode ser
gerada, durante uma inspiração e expiração máximas, contra uma via aérea
ocluída por meio de um clipe nasal (NEDER et al., 1999; SOUZA, 2002).
Ambas podem ser medidas por meio do manovacuômetro, instrumento clássico
para avaliar a força dos músculos respiratórios em nível da boca. Os valores de
PImáx e PEmáx são dependentes não apenas da força dos músculos
respiratórios, mas também do volume pulmonar em que são realizadas as
medidas e do correspondente valor da pressão de retração elástica do sistema
respiratório (SOUZA, 2002).
Nesta amostra, a força dos músculos respiratórios foi avaliada utilizando-
se um manovacuômetro digital, da marca GlobalMed, Porto Alegre, Rio Grande
do Sul, Brasil (MVD 300® -300 a +300 cmH20). Os testes foram realizados com
as voluntárias sentadas. Antes de cada teste, as participantes foram
detalhadamente orientadas sobre os procedimentos, e os resultados obtidos
foram avaliados nos seus valores absolutos. Para obtenção da força muscular
expiratória, foi solicitado que elas realizassem uma inspiração máxima (próximo
à capacidade pulmonar total - CPT) seguida de uma expiração máxima
(próxima ao volume residual - VR). Para obtenção da força muscular
inspiratória, foi solicitado que realizem uma expiração máxima (próximo à VR),
seguida de uma inspiração máxima (próximo a CPT) (ATS/ERS, 2002). Para
cada avaliação, foi considerado o valor máximo obtido em no máximo cinco
provas, desde que este valor não fosse superior a 10% entre as três melhores
provas (ATS/ERS, 2002).
4.7.5 Análise Estatística
45
A análise estatística deste estudo será dividida em artigo 1 e artigo 2,
uma vez que os principais resultados desta tese serão apresentados sob a
forma de dois artigos científicos:
Análise Estatística - Artigo 1
A análise dos dados foi desenvolvida através do software SPSS, versão
20.0 (SPSS, Chicago, IL, EUA). A normalidade dos dados foi verificada através
do teste de Kolmogorov-Smirnov. A estatística descritiva para todas as
variáveis foi apresentada de acordo com a variável “gestações” e analisada
com análise de variância (ANOVA) e post hoc de Tukey para variáveis
contínuas. Para as variáveis categóricas, utilizaram-se os testes de qui-
quadrado para comparação de proporções.
Para cada categoria de variáveis independentes, foram apresentados os
valores médios e desvios padrão de PImáx e PEmáx, e comparados através de
teste t de Student e ANOVA, com post hoc de Tukey.
Análises de regressão linear múltipla foram realizadas para modelar o
efeito da história reprodutiva sobre a PImáx e PEmáx, e ajustados para as
covariáveis que apresentaram associações com as pressões respiratórias, com
p <0,20 na análise bivariada (Idade, renda familiar mensal, escolaridade,
tabagismo, IMC, tempo sentada por dia e caminhada). As variáveis idade e
IMC foram centradas. A primeira foi centrada como idade do participante
menos a idade mínima na amostra, que foi de 41 anos, e a variável IMC foi
centrada como o IMC da participante menos o IMC médio da amostra,
equivalente a 29,06 Kg/m2. Os diagnósticos de regressão foram conduzidos
para todas as análises lineares, incluindo testes de colinearidade, e não foram
observados desvios.
46
Análise Estatística - Artigo 2
Foram apresentadas estatísticas descritivas para todas as variáveis de
acordo com a variável prolapso de órgão pélvico e analisadas utilizando teste t
independente. Para variáveis categóricas, foi utilizado teste de qui-quadrado
para comparação de proporções. Os modelos de regressão linear univariada
foram utilizados para determinar a associação entre as características dos
participantes, o prolapso de órgãos pélvicos e a força muscular respiratória. Foi
utilizado o método "backward" e variáveis com associações estatisticamente
significativas (p <0,05) com o prolapso de órgãos pélvicos e PImáx ou Pemáx
permaneceram no modelo multivariado.
Todas as análises foram realizadas usando o Statistical Package for the
Social Sciences (SPSS), versão 19.0, IBM SPSS, Chicago, IL, EUA.

47
5. RESULTADOS E DISCUSSÃO

48
Neste tópico serão apresentados os principais resultados analisados
neste estudo até o presente momento, sob a forma de dois artigos científicos
produzidos com os dados coletados, cujos títulos são:
Artigo 1: Multiple childbearing is associated with respiratory muscle
strength in Brazilian women: A cross-sectional community-based study.
Artigo 2: Relationship between symptomatic pelvic organ prolapse and
respiratory muscle strength in middle-aged and elderly women in Northeast
Brazil: A cross-sectional study.
O artigo 1 encontra-se submetido à revista BMC Pulmonary Medicine,
que possui fator de impacto 2.435, e é classificada como A1 pelo web-qualis da
área 21 da CAPES. O artigo 2, após devidos ajustes, será submetido à Revista
Brasileira de Fisioterapia, que possui fator de impacto 1.27, e é classificada
como A2 pelo web-qualis da área 21 da CAPES.
49
ARTIGO 1
Multiple childbearing is associated with respiratory muscle
strength in Brazilian women: A cross-sectional community-
based study
Ingrid Guerra Azevedo – PhD Student - Physiotherapy Department,
Universidade Federal do Rio Grande do Norte/ Empresa Brasileira de Serviços
Hospitalares - Hospital Universitário Ana Bezerra - Praça Tequinha Farias, 13
Santa Cruz- RN –Brasil. 59.200-000. Email: [email protected]
Saionara Maria Aires da Câmara - Faculdade de Ciências da Saúde do Trairi -
Universidade Federal do Rio Grande do Norte - R. Teodorico Bezerra, 2-122,
Santa Cruz - RN, 59200-000, Brasil. Email: [email protected]
Catherine McLean Pirkle – University of Hawaii at Manoa - Office of Public
Health Studies - 1960 East-West Road, BioMed D104-H Honolulu, HI 96822-
2319 - U.S.A. Email: [email protected]
Álvaro Campos Cavalcanti Maciel - Departamento de Fisioterapia. Centro de
Ciências da Saúde. Universidade Federal do Rio Grande do Norte – UFRN.
Av. Senador Salgado Filho, 3000. Caixa Postal 1524 - CEP: 59072-970. Email:
Elizabel de Souza Ramalho Viana - Departamento de Fisioterapia. Centro de
Ciências da Saúde. Universidade Federal do Rio Grande do Norte – UFRN. Av.
Senador Salgado Filho, 3000. Caixa Postal 1524 - CEP: 59072-970. Email:
Abstract
Background: Multiple childbearing is common in low-income settings and it is
related to chronic conditions among women. This study aimed to investigate
50
associations between the number of lifetime pregnancies and maximal
inspiratory/expiratory pressures (MIP and MEP). Methods: Women aged 41-80
years-old who were residents of the rural community of Santa Cruz – RN –
Brazil, composed the sample. They were recruited by advertisements in primary
care and community centers. Data regarding demographics, socioeconomic
characteristics, health behaviors, and reproductive history were collected with a
questionnaire. A digital manometer was used to take maximal respiratory
pressures (MRP); height and weight were also taken. Multiple linear regression
analyses were performed to model the effect of multiple childbearing on MRP,
adjusting for covariates. Results: 204 women comprised the study sample.
44.1% had ≤3 pregnancies, 30.4% had 4-6 pregnancies and 25.5% had >7
pregnancies. In the unadjusted analyses, MIP varied considerably according to
education, income, BMI, smoking, sitting time per day and childbearing, and for
MEP values, there were differences according to age, education, BMI and
childbearing. According to the multiple linear regression, the higher the number
of pregnancies, the lower MIP, but these values were non-significant when
adjusted for age, age at first birth, education, income, smoking, BMI, sitting time
per day and walking. For MEP values, associations remained statistically
significant after adjustment. Conclusion: Multiple childbearing appears to
influence respiratory muscle strength; women with a higher number of lifetime
pregnancies have lower values of MRP, especially expiratory muscular
strength. This association may be due to biomechanical changes in the
respiratory muscles promoted by multiple pregnancies.
Keywords: Maximal respiratory pressures; childbearing; aging; global health.
51
Background
Aging is a dynamic and progressive process, influenced by chronological
age, physiological, socioeconomic, and biological factors [1,2]. Among
physiological factors linked to aging, numerous alterations in the respiratory
system, negatively impact respiratory volumes and capacities [3] contributing to
morbidities commonly observed in the elderly, such as chronic obstructed
pulmonary disease (COPD). In fact, it is estimated that by 2020 COPD will rank
5th in terms of worldwide burden of disease [4]. In the United States, it is already
the 3rd leading cause of morbidity and mortality [5].
Aging-associated alterations in the respiratory system include pulmonary
volumetric and thoracic changes that can contribute to respiratory muscle
strength decline [6-8]. Also, it is known that aging is associated to a reduction in
muscle mass and strength [9,10], which can weaken peripheral (limbs) and
respiratory muscle systems. Reduction in peripheral muscle strength with
increasing chronological age is well documented in the literature [11-13].
Moreover, a reduction of up to 25% in the diaphragmatic strength of elderly
when compared to young adults has already been reported [10]. In elderly men
and women, some evidence points to an association between respiratory
muscle strength and physical function [14,15], as measured with lower limb
speed tests [16]. In addition, respiratory muscle strength is also associated with
mobility decline in older persons independent of lower extremity strength and
physical activity [15,17].
Studies about respiratory muscle strength according to gender or
socioeconomic status are largely lacking. There is a large body of evidence that
documents that female sex and socioeconomic adversity contribute to reduced

52
physical function in older adults [2,18,19]. Nevertheless, these associations
have usually been assessed only in peripheral muscles, such as in the legs.
Much less work explores associations between social risk factors and
respiratory function.
Based on previous robust evidence of associations between
socioeconomic measures and physical function assessed in the peripheral
muscles [2,18,19] and some very limited evidence of female-specific risks (e.g.
reproductive variables), we would expect associations between female
reproductive, socioeconomic and respiratory measures. Yet, this avenue of
investigation is all but absent in the literature. To our knowledge, only one study
investigated the association between the aforementioned factors and
respiratory outcomes, and found that multiparity was associated with a
decrease in respiratory muscle strength, mainly among women aged 60 years
and over [20]. However, these authors did not investigate maximal expiratory
pressure (MEP), but rather, only maximal inspiratory pressure (MIP). Through
MEP, it is possible to evaluate the expiratory muscles, which are responsible,
besides breathing, for helping the intestinal transit and also cleaning the airways
through cough [21].
Female reproductive history indicators such as age at first childbirth,
together with the effects of menopause, appear to contribute to the physical
alterations that coincide with aging, such as earlier declines in female functional
capacity, when compared to men at similar ages [22-24]. Studies indicate that
women with early childbearing and/or who had three or more childbirths present
worse physical performance, measured primarily through tests of the lower
53
limbs, when compared to others women who had children after 20 years of age
and fewer children [23-25].
A couple of studies have observed associations between female
reproductive events with respiratory function [23,26], like early maternal age at
first birth and chronic lung disease, but only reported the results as surprising
findings with little investigation of the potential reasons for the observed
associations. Thus, more research is need to corroborate (or not) these
findings. This research should be informed by considerations of socioeconomic
and lifestyle factors likely associated with both female reproductive histories and
respiratory function later in life.
This study aims to investigate whether there are associations between
female reproductive history indicators and respiratory muscle strength, in
addition to socioeconomic factors, such as income and educational levels, in
women from a rural community in Northeast Brazil.
Methods
Population and sample
The study sample is composed of women aged between 41-80 years old,
living in the rural community of Santa Cruz, located 120km from Natal, the
capital of the state of Rio Grande do Norte (RN), Brazil. This community has a
population of about 36,000 inhabitants, over a landmass of approximately
624,356 km2. This is a relatively homogeneous area, with most of the
population considered lower-middle class. Santa Cruz is ranked 3393 of 5565
Brazilian municipalities with Human Development Index (HDI) scores, which
works as a comparison index among different population, being an important
54
measure of progress, being a composite index of life expectancy, years of
schooling and income [27]. This means that Santa Cruz has an HDI of 0.635,
measured in 2010 [28], which is considered medium in the HDI classification
system [27]. According to the last census data from 2010, approximately 60% of
the population is considered vulnerable to poverty [28], which means “those
who are below or at risk of falling below a certain minimally acceptable
threshold of critical choices across several dimensions, such as health,
education, material resources, security” [27].
For this cross-sectional study, we aimed to sample around 50 women for
each group of 10 years (41-80 years old). Half of the sample was over 60 years
old and half was below. This was done so that there was a relatively equal
representation of participants across the age range of interest. Without
deliberate sampling of older age categories, the sample would have been
skewed to the younger categories, as it is easier for younger women to travel to
the evaluation site in central Santa Cruz.
We were able to recruit 208 women by advertisements in primary health
care units and community centers across the city, according to the following
inclusion criteria: aged between 41-80 years, living in Santa Cruz. We excluded
women with neurological impairments, degenerative diseases, or any chronic
condition that could compromise the respiratory muscle strength evaluation. We
also excluded women with severe cognitive impairment, defined as four or more
errors in the orientation scale of the Leganes Cognitive Test [29], as this is
considered indicative of being unable to complete the study protocols.
Nevertheless, we excluded four presumably eligible women since they could not
55
follow the instructions for developing a maximal respiratory pressure as
required. Thus, 204 women comprised our final sample.
Procedures & Measures
All participants were evaluated by trained interviewers at the Faculty of
Health Sciences of Trairi, which is a Campus of the Federal University of Rio
Grande do Norte located in the city of Santa Cruz.
Outcome
Maximal Respiratory Pressure:
Respiratory muscle strength was assessed using an electronic
manometer MVD 300® (-300 a +300 cmH20) (Globalmed®, Porto Alegre, Rio
Grande do Sul, Brazil), supervised by a trained interviewer. Individuals were
positioned in a sitting position and asked to perform a maximal expiration (near
to the residual volume) followed by a maximal inspiration (near to total lung
capacity) for the maximal inspiratory pressure (MIP) assessment. A maximal
inhalation (near to total lung capacity) followed by a forced expiration was
performed for the maximal expiratory pressure (MEP) assessment. The highest
value obtained in up to five maneuvers was chosen for MIP and MEP, since in
none of the participants did the values of the best three trials differ by more than
10% from each other [30].
Exposure
Reproductive History:
The variables maternal age at first childbirth and number of pregnancies
were self-reported. Lifetime childbearing was categorized as three pregnancies

56
or fewer, four to six children, or seven pregnancies or more. This variable was
created based on the literature related to lifetime parity. The first category was
based in previous studies indicating that women with three or more children
have a worse physical performance [24] and a greater chance of developing
chronic diseases [23]. Since 25% of our sample matched the definition of seven
or more childbearing [31]. Studies suggest that women with more than 5
children (large multiparous women) present an even greater risk of adverse
health outcomes [32, 33].
In order to categorize whether the woman had her first child as a
teenager or adult, her age at when she first gave birth was divided into less than
18 years-old and 18 years or more, or if she did not have children, she was
considered nulliparous [24]. Eighteen is the age of majority in Brazil.
Potential confounders
Age: age was considered a covariate in these analyses because it is
related to respiratory muscle strength [3] and to childbirth [20].
Body mass index (BMI): greater number of children is associated with
greater body weight [24, 34]. BMI was also already associated to both higher
[35] and lower respiratory muscle strength [36]. Measures of height (m) and
weight (kg) were taken using a scale with an estadiometer (WELMY®, W100H,
model R-110, Santa Bárbara d'Oeste, Brazil), and used to calculate the BMI
(kg/m2).
Socioeconomic position: family income and education were considered
as potential confounders as both are associated to reproductive history [23, 37]
and respiratory muscle strength [17]. Income and educational data were also

57
self-reported. Income was categorized using the Brazilian minimum monthly
wage (MW) as a reference, which is defined as the lowest remuneration that
workers can receive as payment for their jobs per month. The definition of
minimum wage states that it is an amount that should be able to supply the
normal basic needs for a family. At the time of the interview, the MW was equal
to R$ 880.00 (around 250.00 US dollars). Nevertheless, according to the
Statistics and Socioeconomic Studies Department of Brazil (DIEESE) [38], the
sufficient minimum salary to meet this is definition, at the time of data collection,
should be more than four times the value established by the Brazilian
government. In our study, family income was thus dichotomized as less than
3MW and 3MW or more, as a way to distinguish those who are under of this
proper amount [37]. Educational data were categorized into less than seven
years (less than basic education) or more than seven years (basic education of
more) [37].
Physical activity: physical activity measures are associated to both
reproductive history [18, 20] and respiratory measures [20]. To assess physical
activity, we asked the participants about how many days and how much time
per day they had walked for more than ten minutes, without stopping, during the
last week. This measure included walking as a way to go from one place to
another, or as physical exercise. Subsequently, participants were categorized
into one of two categories: less than 90 min/week and 90 min/week or more
[37]. To evaluate the time per day spent in sedentary activity, women were
asked to report how much time in a normal day they stay seated, and the
variable was dichotomized at 4 h/day or less, and more than 4 h/day [37, 39].
58
Smoking: women with high lifetime pregnancies are more likely to be
smokers [18], and also tobacco use is associated to respiratory muscle strength
[40, 41]. We asked the participants about their habits in relation to smoking
(current smoker, previous smoker or never smoker). Since only few women
reported being current smokers (N=13; 6.4%), we dichotomized the women into
two groups: ever smoked and never smoked.
Data Analysis
Data analyses were conducted using SPSS software, version 20.0
(SPSS, Chicago, IL, USA). Descriptive statistics for all variables were presented
according to the variable pregnancies and analyzed using analysis of variance
(ANOVA) and post hoc Tukey tests for continuous variables. For categorical
variables, Chi-square tests were used for comparison of proportions. Means
and standard deviations of MIP and MEP were presented for each category of
the independent variables and compared using t-tests and ANOVA.
Multiple linear regression analyses were performed to model the effect of
multiple childbearing on MIP and MEP adjusted for all potential confounders.
Three models were performed to evaluate the association of the variables of
respiratory muscle strength and lifetime pregnancy after controlling for each
group of covariates: in model 1, the associations between pregnancies and the
outcome variables were adjusted for age and age at first birth; in model 2, we
added the variables related to socioeconomic position (education and family
income); in model 3, the variables associated to lifestyle (smoking, sitting time
per day and walking) and BMI were included. We centered the variables age
(participant’s age minus the minimum age in the sample, 41) and BMI
59
(participant’s BMI minus the sample mean BMI, 29.06 Kg/m2). Regression
diagnostics were conducted for all linear analyses, including tests of collinearity,
and no major deviations were noted.
Ethics
All participants were informed of the objectives and procedures of the
research study at first contact and signed a consent form. The study protocol
received ethics approval by the Ethics and Research Committee of the Federal
University of Rio Grande do Norte (approval number 1.875.802).
Results
Sample characteristics are presented according to pregnancies category
(Table 1). There was a significant difference in mean age across pregnancy
groups: women who had more than seven pregnancies were older than the
women from the other groups, and also women who had between four to six
pregnancies were older than those who had less than three pregnancies.
Educational attainment and income differed significantly across pregnancy
categories. Greater proportions of women with lower levels of education and
income were observed for the groups with higher numbers of lifetime
childbearing. Compared to women who had three or fewer pregnancies, those
with seven children or more were marginally more likely to have ever smoked
(38% versus 54%, p= 0.09). In contrast, those reporting seven or more
pregnancies were significantly less sedentary than the lower pregnancy groups.
Finally, for the age at first birth variable, there was a gradient for the proportion
of women reporting early first childbirth (before 18 years-old) across pregnancy
60
categories; the proportion increased significantly with greater number of
pregnancies (from 11% to 54%).
---Insert table 1 here---
Unadjusted analyses for MIP and MEP values according to the study
covariates are shown in table 2. Mean MIP values differed significantly across
education, smoking, sitting time per day and pregnancy categories. The mean
MIP among those who had given birth to fewer than three children was
approximately 21 cmH2O greater than those who had given birth to seven
children or more. A similar difference was observed for those with greater levels
of education compared to lower educational attainment. When considering MEP
values, there were significant differences according to education and
pregnancies. As for MIP, those who had given birth to three or fewer children
had 20 cmH2O more on average than those who had delivered seven children
or more. The difference between educational groups was not as great as for
MIP (12 cmH2O), but in the same direction.
---Insert table 2 here---
Table 3 shows the multiple linear regression results for MIP outcome.
The reproductive history variables were not associated with MIP after controlling
for the covariates. Increasing age was significantly associated with lower mean
MIP values in models 1 and 2, but not in the 3rd model that included BMI and
health behaviors. In model 3, those who reported never smoking and limited
sedentary behavior had significantly higher mean MIP values. Table 4 shows
the results of the multiple linear regression for MEP. A significant relationship
between pregnancies and MEP was observed, even in the fully adjusted model.
Compared to those women who had three or fewer pregnancies, those who had
61
had four to six children and seven pregnancies or more had significantly lower
mean MEP values (-12.5 cmH2O and -17.8 cmH2O, respectively). No significant
relationship was observed between MEP and age at 1st childbirth. For both MIP
and MEP, greater mean BMI was associated with significantly greater values.
---Insert table 3 & 4 here---
Discussion
The results of this study suggest that childbearing is associated to
respiratory muscle strength, especially for the MEP, since the association was
maintained even after extensive adjustment for covariates in the linear
regression models. Briefly, women with a greater number of lifetime
pregnancies performed worse on the evaluation of respiratory pressures than
women reporting fewer children. The mean difference between the low and high
pregnancy group was around 18 cmH20 for MEP. It has already been reported
that increasing 1 unit in the respiratory muscle strength is enough to reduce
around 35% the rate of mobility decline associated to aging [17], which shows
the clinical relevance of the large differences observed between the different
parity categories.
To our knowledge, research investigating the relationship between
respiratory muscle strength and reproductive characteristics is almost entirely
absent from the literature. In a rare exception, researchers examining healthy
Tunisian women aged ≥45 observed an association between multiparity and
lung function, evaluated by spirometry, as well as inspiratory muscle strength
[20]. The authors concluded that lung function declines with increasing parity,
and they attribute this association to many possible causes associated to
multiple pregnancies, including cumulative hormonal changes (e.g. cortisol

62
secretion), and anatomical modifications in the thorax and respiratory muscles,
derived from the repetitive augmentation of the uterus.
According to our results, there is a clear and strong gradient of lower
expiratory muscle strength with higher lifetime pregnancies. Physiologically, this
association may be explained by alterations in abdominal muscle biomechanics
after bearing multiple children. During pregnancy, it is common that the two
sides of the recti abdominal muscle become distant from each other, known as
recti diastasis, which may reduce abdominal strength subsequent to pregnancy
[42]. Additionally, considering our findings, it is possible that the effect of
abdominal recti and the respiratory muscle strength is more evident with the
cumulative effect of many pregnancies on the muscles’ biomechanics, since the
association is strongest in the group with the highest number of children.
In addition to abdominal muscles alterations, the increased uterine
volume following pregnancy conduces a change in the configuration of the
chest and, then, of respiratory muscles [43]. These changes may accumulate
after repeated pregnancies [20], leading to a reduction in respiratory muscle
strength.
The associations observed between number of pregnancies and MIP
were not sustained after adjustments for the covariates in the linear regression
models. Possibly, the differences in MIP among the groups were not big enough
to be detected in a relatively small sample. Furthermore, in our results, women
with higher BMI present higher values for MIP. Some theories support
increased respiratory muscle strength in obese individuals, which have an
excess of adipose tissue in the thoracic cavity and abdomen, and can be
explained by an adaptation to chronic overload that is accompanied by obesity

63
[35]. It is possible that the increased volume of the abdominal area during
several pregnancies promotes a similar effect on the inspiratory muscles,
leading to a less expressive loss in MIP over the aging process. More studies
are necessary to clarify such associations.
An alternative explanation for our findings may have to do with hormonal
changes related to multiple pregnancies across the lifecourse. Multiple
pregnancies and multiparity may predispose the female organism to a chronic
stress situation [44], which is associated to higher levels of cortisol secretion
[45]. Considering that elevated levels of cortisol are associated to a reduction in
muscle strength [45], it is possible that this hormone is an intermediate factor in
the relationship between the number of pregnancies and respiratory muscle
strength.
The findings of this study point suggest that health professionals,
especially physiotherapists, should promote the safe exercise of respiratory
muscles, especially the abdominal ones, among parous women from the
prenatal to postpartum period. Weaker expiratory muscles are associated to
ineffective coughing [21], impaired intestinal transit [21], atelectasis [6] and
mobility decline [15, 17], which can lead to adverse health outcomes and poor
quality of life. This is even more significant considering among low-income
populations, since they are more likely to start childbearing earlier [23, 24], tend
to have multiple children [23], and also to have greater losses in muscle
function with aging [17, 46]. In this perspective, this study brings evidence of the
need to consider reproductive variables when assessing the respiratory system,
especially in aging populations.

64
This study has some limitations. The sample may not have been
sufficiently powered to detect small differences in MIP and MEP values across
covariates. It is possible that the difference in MIP values across groups of
number of pregnancies was not big enough to be detected with this relatively
small sample. Additionally, women from this sample were recruited through
convenience sampling, which may limit the external validity of the study.
However, this sample presents similar socioeconomic characteristics (family
income and education) to the population of women from Santa Cruz according
to the last census data [28]. Finally, some information was collected by self-
reporting and misclassification bias may occur for those with lower education.
Nonetheless, self-reported questionnaires are a typical method employed in
health literature [47]. Furthermore, we used objective and validated measures of
respiratory muscle strength and bias related to recall of the exposure and
covariates measures would most likely be non-differential, as it is unlikely that
reporting would differ systematically across MIP/MEP values.
Conclusion
This study provides evidence that multiple pregnancies influence
respiratory muscle strength, since women with a higher number of pregnancies
have lower mean values of maximal respiratory pressures. However, when
adjusted for confounding variables, this relation is only maintained for the
expiratory muscular strength. The relationship between MEP and this
reproductive variable may be explained by biomechanical changes in the
respiratory muscles promoted by multiple pregnancies. If corroborated by
others, our findings indicate a need to motivate pregnant women, from the
65
prenatal to postpartum period, to safely exercise their respiratory muscles,
particularly abdominal ones.
List of Abbreviations: MIP: Maximal Inspiratory Pressure; MEP: Maximal
Expiratory Pressures; MRP: Maximal Respiratory Pressure; COPD: Chronic
Obstructed Pulmonary Disease; BMI: Body Mass Index; HDI: Human
Development Index; RN: Rio Grande do Norte; MW: Monthly Wage; DIEESE:
Statistics and Socioeconomic Studies Department of Brazil; ANOVA: Analysis
of Variance.
Declarations
Ethics approval and consent to participate: The study protocol received
ethics approval by the Ethics and Research Committee of the Federal
University of Rio Grande do Norte (approval number 1.875.802). All participants
were informed of the objectives and procedures of the research study at first
contact and signed a consent form.
Consent to publish: Not applicable.
Availability of data and materials: The datasets used and/or analysed during
the current study are available from the corresponding author on reasonable
request.
Competing interests: The authors declare that they have no competing
interests.
Funding: Not applicable.
Authors’ contributions: IGA, SMAC, ESRV and ACCM contributed to the
conception and design of the present study and analysis plan. SMAC, CP and

66
IGA analyzed the data with feedback from all authors and wrote the manuscript.
IGA and SMAC contributed to the acquisition of data. All authors contributed to
the interpretation of the data and to critical review of the manuscript. All authors
read and approved the final manuscript.
Acknowledgements: The authors are grateful to the students from
FACISA/UFRN who contributed in the data collection process, to all participants
of this study for being part in this research, and also to the University Hospital
Ana Bezerra for contributing to the development of this research.
References
1. Santos CA, Dantas EEM, Moreira MHR. Correlation of physical aptitude;
functional capacity, corporal balance and quality of life (QoL) among elderly
women submitted to a post-menopausal physical activities program. Arch
Gerontol Geriatr. 2011; 53:344-9.
2. Sousa ACPDA, Guerra RO, Thanh Tu M, Phillips SP, Guralnik JM,
Zunzunegui MV. Lifecourse Adversity and Physical Performance across
Countries among Men and Women Aged 65-74. PloS One. 2014; 9, e102299.
3. De Melo Barcelar J, Aliverti A, Rattes C, et al. The expansion of the
pulmonary rib cage during breath stacking is influenced by age in obese
women. PLoS One. 2014; doi:10.1371/journal.pone.0110959.
4. Murray CJL, Lopez AD. Evidence-based health policy—lessons from the
Global Burden of Disease Study. Science. 1996;274:740–3.
5. National Center for Health Statistics. Health, United States 2015 with Special
Feature on Racial and Ethnic Health Disparities. Hyattsville, MD: US Dept.
67
Health and Human Services. 2017. http://www.cdc.gov/nchs/hus/. Accessed 12
June 2017.
6. Sanches VS, Santos FM, Fernandes JM, Santos ML, Müller PT, Christofoletti
G. Neurodegenerative disorders increase decline in respiratory muscle strength
in older adults. Respir Care. 2014; doi: 10.4187/respcare.03063.
7. Lowery EM, Brubaker AL, Kuhlmann E, Kovacs EJ. The aging lung.
Clin Interv Aging. 2013; doi:10.2147/CIA.S51152.
8. Lalley PM. The aging respiratory system—pulmonary structure, function and
neural control. Respir Physiol Neurobiol. 2013;
doi:10.1016/j.resp.2013.03.012.
9. Landi F, Liperoti R, Russo A, Giovannini S, Tosato M, Capoluongo E,
Bernabei R, Onder G . Sarcopenia as a risk factor for falls in elderly individuals:
results from the ilSIRENTE study. Clin Nutr. 2012; 31:652-8.
10. Tolep K, Higgins N, Muza S, Criner G, Kelsen SG. Comparison of
diaphragm strength between healthy adult elderly and young men. Am J Respir
Crit Care Med. 1995;152: 677-82.
11. Liu CK, Leng X, Hsu FC, Kritchevsky SB, Ding J, Earnest CP, et al. The
impact of sarcopenia on a physical activity intervention: the Lifestyle
Interventions and Independence for Elders Pilot Study (LIFE-P). J Nutr Health
Aging. 2014;18:59-64.
12. Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB,
Ferrucci L, Guralnik JM, Fragala MS, Kenny AM, et al. The FNIH sarcopenia
project: rationale, study description, conference recommendations, and final
estimates. J Gerontol A Biol Sci Med Sci. 2014;69:547–58.
68
13. Leenders M, Verdijk LB, van der Hoeven L, van Kranenburg J, Nilwik R, van
Loon LJ. Elderly men and women benefit equally from prolonged resistance-
type exercise training. J Gerontol A Biol Sci Med Sci. 2013;68:769-79.
14. Parentoni AN, Mendonça VA, Dos Santos KD, Sá LF, Ferreira FO, Gomes
Pereira DA, Lustosa LP. Gait Speed as a Predictor of Respiratory Muscle
Function, Strength, and Frailty Syndrome in Community-Dwelling Elderly
People. J Frailty Aging. 2015;4:64-8.
15. Giua R, Pedone C, Scarlata S, Carrozzo I, Rossi FF, Valiani V, Incalzi RA.
Relationship between respiratory muscle strength and physical performance in
elderly hospitalized patients. Rejuvenation Res. 2014;17:366-71.
16. Simões LA, Dias JMD, Marinho KC, Pinto CLLR, Britto RR. Relação da
função muscular respiratória e de membros inferiores de idosos comunitários
com a capacidade funcional avaliada por teste de caminhada. Rev. bras.
fisioter. 2010; 14: 24-30.
17. Buchman AS, Boyle PA, Wilson RS, Leurgans S, Shah RC, Bennett DA.
Respiratory Muscle Strength Predicts Decline in Mobility in Older Persons.
Neuroepidemiology. 2008; doi:10.1159/000154930.
18. Grundy E, Read S, Frans E, Carey J, Qiang L. Pathways from fertility
history to later life health : Results from analyses of the English Longitudinal
Study of Ageing Table of Contents. Demogr. Res. 2015;32:107–46.
19. Hajiahmadi M, Shafi H, Delavar MA. Impact of parity on obesity: a cross-
sectional study in Iranian women. Medical Principles and Practice. 2015; 24:
70–4.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Lustosa%20LP%5BAuthor%5D&cauthor=true&cauthor_uid=27032046
https://www.ncbi.nlm.nih.gov/pubmed/?term=Scarlata%20S%5BAuthor%5D&cauthor=true&cauthor_uid=24749768
69
20. Ben Saad H, Tfifha M, Harrabi I, Tabka Z, Guenard H, Hayot M, Zbidi A.
Facteurs influençant les variables ventilatoires des Tunisiennes âgées de
45 ans et plus. Revue des Maladies Respiratoires. 2006; 23:324-38.
21. West JB. Fisiologia Respiratória - Princípios Básicos – 9th ed. São Paulo:
Saraiva; 2013.
22. Cho GJ, Shin JH, Yi KW, Park HT, Kim T, Hur JY, Kim SH. Adolescent
pregnancy is associated with osteoporosis in postmenopausal women.
Menopause. 2012;19:456-60.
23. Pirkle C, Sousa ACPA, Alvarado B, Zunzunegui MV. Early maternal age at
first birth is associated with chronic diseases and poor physical performance in
older age: cross-sectional analysis from the International Mobility. BMC public
Health. 2014;14:293.
24. Da Câmara SM, Pirkle C, Moreira MA, Vieira MCA, Vafaei A, Maciel AC.
Early maternal age and multiparity are associated to poor physical performance
in middle-aged women from Northeast Brazil: a cross-sectional community
based study. BMC Womens Health. 2015;15:56.
25. WHO. Global database on Body Mass Index. 2016.
http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed 17 Dec
2016.
26. Henretta JC. Early childbearing, marital status, and women’s health and
mortality after age 50. J Health Soc Behav. 2007; 48:254–66.
27. United Nations Development Programme (UNDP). Human Development
Report 2014. Sustaining Human Progress: Reducing Vulnerabilities and
Building Resilience. 2017. http://hdr.undp.org/en/content/human-development-
report-2014. Accessed 17June 2017.
70
28. Atlas do desenvolvimento humano. 2017.
http://www.atlasbrasil.org.br/2013/en/perfil_m/santa-cruz_rn/. Accessed 11 May
2017.
29. De Yébenes MJ, Otero A, Zunzunegui MV, Rodríguez-Laso A, Sánchez-
Sánchez F, Del Ser T. Validation of a short cognitive tool for the screening of
dementia in elderly people with low educational level. Int J Geriatr
Psychiatry. 2003;18:925-36.
30. American Thoracic Society-ATS. European respiratory society-ERS.
Statement on respiratory muscle testing. American Journal of Respiratory
Critical Care Medicine. 2002; 166,518–624.
31. Toohey JS, Keegan KA Jr, Morgan MA, Francis J, Task S, de Veciana M.
The “dangerous multipara”: fact or fiction? Am J Obstet Gynecol. 1995;
172:683–6.
32. Abu-Heija, Chalabi HE. Great grand multiparity: is it a risk? J Obstet
Gynaecol. 1998;136-8.
33. Rayamajhi R, Thapa M, Pande S. The challenge of grandmultiparity in
obstetric practice. Kathmandu University Medical Journal. 2006; 4:70-74.
34. Umberson D, Liu H, Mirowsky J, Reczek C. Parenthood and Trajectories of
Change in Body Weight Over the Life Course. Social science & medicine.
2011;73:1323-31.
35. Santiago-Recuerda A, Gómez-Terreros FJ, Caballero P, Martin-Duce A,
Soleto MJ, Vesperinas G, et al. Relationship between the upper airway and
obstructive sleep apneahypopnea syndrome in morbidly obese women. Obes
Surg. 2007;17:689-97.

71
36. Mafort TT, Rufino R, Costa CH, Lopes AJ. Obesity: systemic and pulmonary
complications, biochemical abnormalities, and impairment of lung function.
Multidiscip Respir Med. 2016;12:11-28.
37. Da Câmara SM, Zunzunegui MV, Pirkle C, Moreita MA, Maciel AC.
Menopausal status and physical performance in middle aged women: a cross-
sectional community-based study in Northeast Brazil. PLoS One. 2015; doi:
10.1371/journal.pone.0119480.
38. Brasil. Salário mínimo nominal e necessário. 2014.
http://www.dieese.org.br/analisecestabasica/salarioMinimo.html. Accessed
17January 2017.
39. Gómez-Cabello A, Vicente-Rodríguez G, Pindado M, Vila S, Casajús JA, de
la Fuente PF, et al. Increased risk of obesity and central obesity in sedentary
postmenopausal women. Nutr Hosp. 2012;27:865–70.
40. Chen HI. Effects of chronic smoking on respiratory muscle function. Chin J
Physiol. 1988;31:53-62.
41. Freitas ERFS, Araujo ECLS, Alves KS. Influência do tabagismo na força
muscular respiratória em idosos. Fisioterapia e Pesquisa. 2012; 19, 326-31.
42. Axer H, Keyserling DG, Prescher A. Collagen fibers in linea alba and rectus
sheaths. I. General scheme and morphological aspects. The Journal of surgical
research. 2001b; 96,127–134.
43. Gilory RJ, Mangura BT, Lavietes MH. Rib cage and abdominal volume
displacements during breathing in pregnancy. Am Rev Respir Dis.1988 ;137:
668-72.

72
44. Parikh NI, Cnattingius S, Dickman PW, Mittleman MA, Ludvigsson JF,
Ingelsson E. Parity and risk of later-life maternal cardiovascular disease. Am
Heart J. 2010;159:215–21.
45. Peeters GM, van Schoor NM, van Rossum EF, Visser M, Lips P. The
relationship between cortisol, muscle mass and muscle strength in older
persons and the role of genetic variations in the glucocorticoid receptor. Clin
Endocrinol (Oxf). 2008;69:673-82.
46. Murray ET, Hardy R, Strand BH, Cooper R, Guralnik JM, Kuh D. Gender
and life course occupational social class differences in trajectories of functional
limitations in midlife: findings from the 1946 British birth cohort. J. Gerontol. A.
Biol. Sci. Med. Sci. 2011; 66:1350–9.
47. Leggett LE, Khadaroo RG, Holroyd-Leduc J, Lorenzetti DL, Hanson
H, Wagg A, et al. Measuring Resource Utilization: A Systematic Review of
Validated Self-Reported Questionnaires. Medicine. 2016; doi:
10.1097/MD.0000000000002759.

Table 1: Participant characteristics according to childbearing categories (N=204)
Childbearing
3 or fewer 4 to 6 7 or more p-value
N (%)/ Mean (SD)
Age (years) 55.6 (10.6) 59.6 (10.4) 68.7 (8.6) p<0.01a
Education
p<0.01b
Less than basic education (0-7 years)
22 (24.4%)
40 (64.5%)
47 (90.4%)
Basic education or more (≥ 8 years)
68 (75.6%) 22 (35.5%) 5 (9.6%)
Income
0.02b
<3MW 56 (62.2%)
49 (79.0%)
42 (80.8%)
≥3MW 34 (37.8%) 13 (21.0%) 10 (19.2%)
BMI (kg/m2) 29.60 (4.6) 29.43 (4.7) 27.57 (4.0) 0.02c
Smoking
0.09b
Ever 34 (37.8%)
22 (35.5%)
28 (53.8%)
Never 56 (62.2%) 40 (64.5%) 24 (46.2%)
Walking (min/week)
0.25b
<90 min
85 (94.4%)
54 (87.1%)
46 (88.5%)
≥90min 5 (5.6%) 8 (12.9%) 6 (11.5%)
Sitting time per day
p<0.01b
4h or less
54 (60.0%)
26 (41.9%)
37 (71.2%)
>4h
36 (40.0%) 36 (58.1%) 15 (28.8%)
Age at first child p<0.01b
Nulliparous 11 (12.2%) 0 (0.0%) 0 (0.0%)
< 18 years old 10 (11.1%) 19 (30.7%) 28 (53.8%)
≥ 18 years old 69 (76.7%) 43 (69.3%) 24 (46.2%)
Total 90 (44.1%) 62 (30.4%) 52 (25.5%)
MW: Minimum wage; BMI: Body Mass Index; Min: Minute; SD: standard deviation.
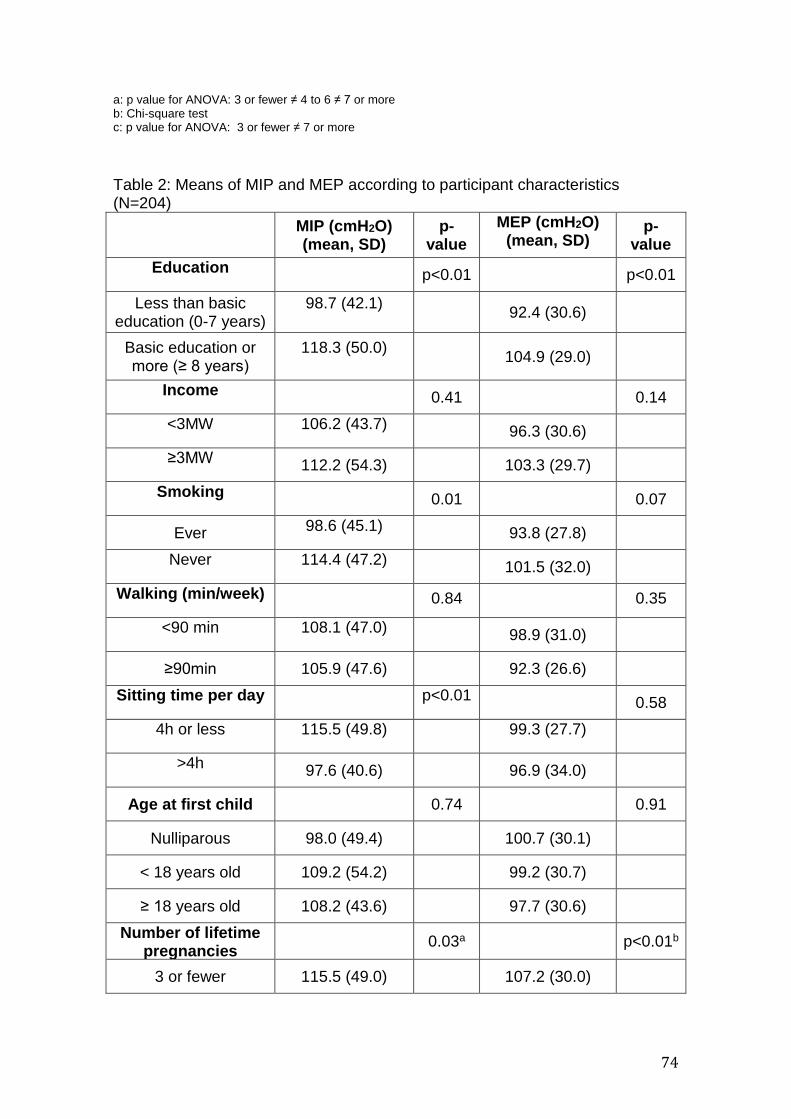
74
a: p value for ANOVA: 3 or fewer ≠ 4 to 6 ≠ 7 or more b: Chi-square test c: p value for ANOVA: 3 or fewer ≠ 7 or more
Table 2: Means of MIP and MEP according to participant characteristics (N=204)
MIP (cmH2O) (mean, SD)
p-value
MEP (cmH2O) (mean, SD)
(mean, SD)
p-value
Education
p<0.01
p<0.01
Less than basic education (0-7 years)
98.7 (42.1)
92.4 (30.6)
Basic education or more (≥ 8 years)
118.3 (50.0)
104.9 (29.0)
Income
0.41
0.14
<3MW
106.2 (43.7)
96.3 (30.6)
≥3MW
112.2 (54.3) 103.3 (29.7)
Smoking
0.01
0.07
Ever 98.6 (45.1)
93.8 (27.8)
Never
114.4 (47.2)
101.5 (32.0)
Walking (min/week)
0.84
0.35
<90 min
108.1 (47.0)
98.9 (31.0)
≥90min 105.9 (47.6) 92.3 (26.6)
Sitting time per day
p<0.01
0.58
4h or less 115.5 (49.8)
99.3 (27.7)
>4h
97.6 (40.6) 96.9 (34.0)
Age at first child 0.74 0.91
Nulliparous 98.0 (49.4) 100.7 (30.1)
< 18 years old 109.2 (54.2) 99.2 (30.7)
≥ 18 years old 108.2 (43.6) 97.7 (30.6)
Number of lifetime pregnancies
0.03a p<0.01b
3 or fewer 115.5 (49.0) 107.2 (30.0)

75
4 to 6 107.9 (43.0) 94.4 (28.8)
7 or more 94.5 (46.0) 87.0 (29.4)
MW: Minimum wage; BMI: Body Mass Index; MIP: Maximal Inspiratory Pressure; MEP: Maximal Expiratory Pressure. a: 3 or fewer > 7 or more b: 3 or fewer > 4 to 6 > 7 or more
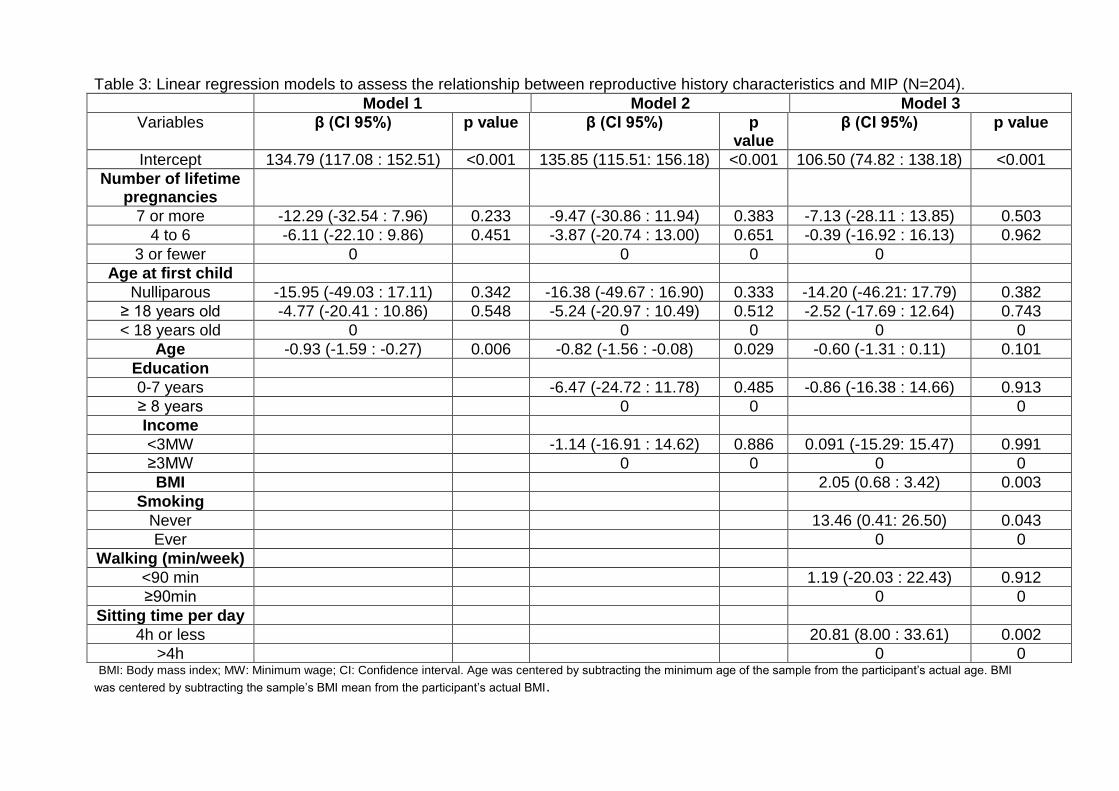
Table 3: Linear regression models to assess the relationship between reproductive history characteristics and MIP (N=204).
Model 1 Model 2 Model 3
Variables β (CI 95%) p value β (CI 95%) p value
β (CI 95%) p value
Intercept 134.79 (117.08 : 152.51) <0.001 135.85 (115.51: 156.18) <0.001 106.50 (74.82 : 138.18) <0.001
Number of lifetime pregnancies
7 or more -12.29 (-32.54 : 7.96) 0.233 -9.47 (-30.86 : 11.94) 0.383 -7.13 (-28.11 : 13.85) 0.503
4 to 6 -6.11 (-22.10 : 9.86) 0.451 -3.87 (-20.74 : 13.00) 0.651 -0.39 (-16.92 : 16.13) 0.962
3 or fewer 0 0 0 0
Age at first child
Nulliparous -15.95 (-49.03 : 17.11) 0.342 -16.38 (-49.67 : 16.90) 0.333 -14.20 (-46.21: 17.79) 0.382
≥ 18 years old -4.77 (-20.41 : 10.86) 0.548 -5.24 (-20.97 : 10.49) 0.512 -2.52 (-17.69 : 12.64) 0.743
< 18 years old 0 0 0 0 0
Age -0.93 (-1.59 : -0.27) 0.006 -0.82 (-1.56 : -0.08) 0.029 -0.60 (-1.31 : 0.11) 0.101
Education
0-7 years -6.47 (-24.72 : 11.78) 0.485 -0.86 (-16.38 : 14.66) 0.913
≥ 8 years 0 0 0
Income
<3MW -1.14 (-16.91 : 14.62) 0.886 0.091 (-15.29: 15.47) 0.991
≥3MW 0 0 0 0
BMI 2.05 (0.68 : 3.42) 0.003
Smoking
Never 13.46 (0.41: 26.50) 0.043
Ever 0 0
Walking (min/week)
<90 min 1.19 (-20.03 : 22.43) 0.912
≥90min 0 0
Sitting time per day
4h or less 20.81 (8.00 : 33.61) 0.002
>4h 0 0 BMI: Body mass index; MW: Minimum wage; CI: Confidence interval. Age was centered by subtracting the minimum age of the sample from the participant’s actual age. BMI
was centered by subtracting the sample’s BMI mean from the participant’s actual BMI.
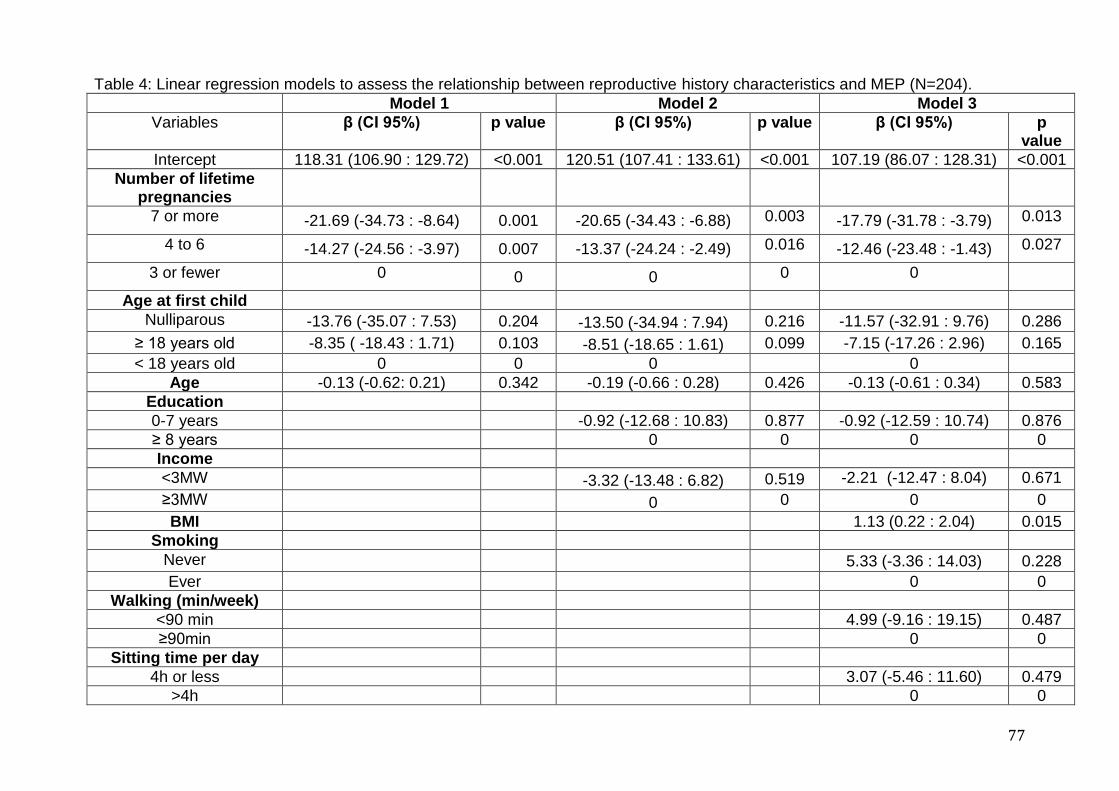
77
Table 4: Linear regression models to assess the relationship between reproductive history characteristics and MEP (N=204).
Model 1 Model 2 Model 3
Variables β (CI 95%) p value β (CI 95%) p value β (CI 95%) p value
Intercept 118.31 (106.90 : 129.72) <0.001 120.51 (107.41 : 133.61) <0.001 107.19 (86.07 : 128.31) <0.001
Number of lifetime pregnancies
7 or more -21.69 (-34.73 : -8.64) 0.001 -20.65 (-34.43 : -6.88) 0.003 -17.79 (-31.78 : -3.79) 0.013
4 to 6 -14.27 (-24.56 : -3.97) 0.007 -13.37 (-24.24 : -2.49) 0.016 -12.46 (-23.48 : -1.43) 0.027
3 or fewer 0 0 0 0 0
Age at first child
Nulliparous -13.76 (-35.07 : 7.53) 0.204 -13.50 (-34.94 : 7.94) 0.216 -11.57 (-32.91 : 9.76) 0.286
≥ 18 years old -8.35 ( -18.43 : 1.71) 0.103 -8.51 (-18.65 : 1.61) 0.099 -7.15 (-17.26 : 2.96) 0.165
< 18 years old 0 0 0 0
Age -0.13 (-0.62: 0.21) 0.342 -0.19 (-0.66 : 0.28) 0.426 -0.13 (-0.61 : 0.34) 0.583
Education
0-7 years -0.92 (-12.68 : 10.83) 0.877 -0.92 (-12.59 : 10.74) 0.876
≥ 8 years 0 0 0 0
Income
<3MW -3.32 (-13.48 : 6.82) 0.519 -2.21 (-12.47 : 8.04) 0.671
≥3MW 0 0 0 0
BMI 1.13 (0.22 : 2.04) 0.015
Smoking
Never 5.33 (-3.36 : 14.03) 0.228
Ever 0 0
Walking (min/week)
<90 min 4.99 (-9.16 : 19.15) 0.487
≥90min 0 0
Sitting time per day
4h or less 3.07 (-5.46 : 11.60) 0.479
>4h 0 0
78
BMI: Body mass index; MW: Minimum wage; CI: Confidence interval. Age was centered by subtracting the minimum age of the sample from the participant’s actual age. BMI
was centered by subtracting the sample’s BMI mean from the participant’s actual BMI.

ARTIGO 2
Relationship between symptomatic pelvic organ prolapse and
respiratory muscle strength in middle-aged and elderly women
in Northeast Brazil: A cross-sectional study
Ingrid Guerra Azevedo – PhD Student - Physiotherapy Department,
Universidade Federal do Rio Grande do Norte/ Empresa Brasileira de Serviços
Hospitalares - Hospital Universitário Ana Bezerra - Praça Tequinha Farias, 13
Santa Cruz- RN –Brasil. 59.200-000. Email: [email protected]
Silvana Loana de Oliveira Sousa - Universidad Miguel de Hernández
Facultad de Medicina - Departamento de Patología y Cirugía (Grado en
Fisioterapia) Crta. Nacional 332, s/n
Sant Joan D'Alacant – 03550 – Espanha. Email: [email protected]
Elizabel de Souza Ramalho Viana - Departamento de Fisioterapia. Centro de
Ciências da Saúde. Universidade Federal do Rio Grande do Norte – UFRN. Av.
Senador Salgado Filho, 3000. Caixa Postal 1524 - CEP: 59072-970. Email:
Diego de Sousa Dantas - Faculdade de Ciências da Saúde do Trairi -
Universidade Federal do Rio Grande do Norte - R. Teodorico Bezerra, 2-122,
Santa Cruz - RN, 59200-000, Brasil. Email: [email protected]
Álvaro Campos Cavalcanti Maciel - Departamento de Fisioterapia. Centro de
Ciências da Saúde. Universidade Federal do Rio Grande do Norte – UFRN.
Av. Senador Salgado Filho, 3000. Caixa Postal 1524 - CEP: 59072-970. Email:

80
Saionara Maria Aires da Câmara - Faculdade de Ciências da Saúde do Trairi -
Universidade Federal do Rio Grande do Norte - R. Teodorico Bezerra, 2-122,
Santa Cruz - RN, 59200-000, Brasil. Email: [email protected]
Abstract
Background: Pelvic organ prolapse (POP) is associated with conditions that
lead to an increase of intra-abdominal pressures. This study aims to investigate
whether there are associations between POP and respiratory muscle strength.
Methods: Women aged 41-80 years-old who were residents of the community
of Santa Cruz – RN – Brazil were included in the sample. Data regarding
demographics, socioeconomic characteristics, health behaviors, reproductive
history and symptomatic POP were collected through a structured
questionnaire, when women self-related this dysfunction. A digital manometer
was used to take maximal respiratory pressures (MRP); height and weight were
also taken. Multiple linear regression analyses were performed to model the
effect of POP on MRP, adjusting for covariates. Results: 204 women
comprised the study sample. For MEP values, associations remained
statistically significant after adjustment. Conclusion: Symptomatic POP
influences expiratory muscle strength. Our findings indicate a need to include
respiratory muscle training as part of the therapy for women with symptomatic
POP, particularly expiratory strengthening.
Keywords: Maximal respiratory pressures; Pelvic organ prolapse; global health.
81
Background
Pelvic organ prolapse (POP) is defined as the descent of one or more of
the anterior vaginal wall, posterior vaginal wall, uterus, or apex of the vagina
(ABRAMS et al., 2003) that is more common with aging (DIETZ, 2008;
BUREAU; CARLSON, 2017). Given the population aging, POP prevalence is
estimated to increase substantially between 2010 and 2050 in the US (from a
minimum of 46%, or 3.3 to 4.9 million women, up to 200% or 9.2 million
women), bringing important implications for public health (WU et al., 2009).
The main symptom of POP is the vaginal bulge (TAN et al., 2005), and
women with this condition usually suffer from physical and emotional distress
(LOWDER et al., 2011). They are more likely to feel isolated, less feminine and
less attractive, which greatly affect their professional and personal activities
(LOWDER et al., 2011). Functional limitations (especially in strength and body
mobility domains) are also highly prevalent in women with POP, particularly in
older ones (aged ≥ 65 years) (SANSES et al., 2016).
POP is a multifactorial event that involves failure of support and
suspension mechanisms of the pelvic organs, as well as alterations of
synergism between the abdomen and the pelvic floor (IGLESIA; SMITHLING,
2017). In this sense, it is associated with sustained episodes of increased intra-
abdominal pressure, such as multiple pregnancies, chronic cough, repeated
heavy lifting, obesity, constipation and other causes that result in less function
of the pelvic floor, as macrosomia and vaginal deliveries (RODRIGUES et al.,
2009; RESENDE et al, 2010; IGLESIA; SMITHLING, 2017).
82
Moreover, previous studies have showed an association between POP
and pulmonary ventilation function among pre and postmenopausal women
(STRINIC et al., 1997; STRINIC et. al., 2002), and, although not measuring
respiratory muscle strength, these authors have suggested a weakness of
respiratory muscles in women with this dysfunction (STRINIC et al., 1997).
However, to the best of our knowledge, the association between specific
measures of respiratory muscle strength and the pelvic organ prolapse has not
been examined previously.
Across the adult life span, there are reductions in several respiratory
variables, including respiratory muscle strength, which contributes to adverse
health outcomes among older people (FRAGOSO; GILL, 2012), and to
reduction in functional capacity (BUCHMANN et al., 2008). Understanding the
relationship between the pelvic organ prolapse and respiratory variables may
provide important information to help clinicians to handle both conditions among
women during their aging process.
Thus, this study aims to investigate whether there is an association
between symptomatic POP and respiratory muscle strength in middle-aged and
elderly women.
Methods
This is a cross-sectional study that took place in Santa Cruz, a city from
Northeast Brazil. Santa Cruz is located in the Rio Grande do Norte state and it
is 120km far from Natal (capital of the state). Its population is of about 36,000
inhabitants and most of them is considered lower-middle class, according to the
Brazilian Institute of Geography and Statistics.
83
Population and sample
The sample for this study was composed of women aged between 41-80
years old, living in the community of Santa Cruz, located 120 km far from the
capital of the state of Rio Grande do Norte, Natal. The sample consists of 208
women recruited through advertisements placed in the primary health care units
and community centers across the city. Exclusion criteria consisted of
neurological impairments, and degenerative diseases that could compromise
the respiratory muscle strength evaluation; and cognitive impairment defined as
four or more errors in the orientation scale of the Leganes Cognitive Test (DE
YÉBENES et al., 2003), considered indicative of being unable to complete the
study protocols (SOUSA et al., 2014). Additionally to these criteria, for the
present study we excluded four subjects that could not follow the instructions for
developing maximal respiratory pressures as required. Our final sample was
comprised of 204 women.
Procedures & Measures
All the sample assessment was conducted by trained interviewers at the
Faculty of Health Sciences of Trairi, which is a Campus of the Federal
University of Rio Grande do Norte, located in the city of Santa Cruz. The
standardized protocols are described below.
Outcomes
Maximal Respiratory Pressure:

84
An electronic manometer MVD 300® (-300 a +300 cmH20) (Globalmed®,
Porto Alegre, Rio Grande do Sul, Brazil) was used to assess respiratory muscle
pressures. The individuals were positioned in a sitting position and asked to
perform a maximal expiration (near to the residual volume) followed by a
maximal inspiration (near to total lung capacity) for the maximal inspiratory
pressure (MIP) assessment. A maximal inhalation (near to total lung capacity)
followed by a forced expiration was performed for the maximal expiratory
pressure (MEP) assessment. The highest value obtained in up to five
maneuvers was chosen for MIP and MEP, since in none of the participants the
values of the best three trials differed more than 10% from each other
(ATS/ERS, 2002).
Exposure
Symptomatic Pelvic Organ Prolapse:
Participants were asked: “Do you have a sensation that there is a bulge
in your vagina or that something is falling out from your vagina?” (ROGER,
2013). Those answering “yes” were considering as presenting symptomatic
pelvic organ prolapse. This question was derived of the Pelvic Organ Prolapse
Incontinence Sexual Questionnaire, International Urogynecological Association
-IUGA-revised (PISQ-IR), which was validated and specifically developed for
international use (ROGER et al., 2013; BARBER; EUBAUER; KLEIN-OLART,
2006). It has been reported that feeling a bulge or that something is falling
outside the vagina is 81% predictive of prolapse, and the absence of these
symptoms is 76% predictive of not having prolapse (TAN et al., 2005), showing
that this is a reliable tool for this evaluation.
Other independent variables
85
Age: age was considered a covariate in these analyses because pelvic
organ prolapse is more prevalent in older women (DIETZ, 2008), and because
there is a reduction in the respiratory muscle strength with aging (DE MELO
BARCELAR et al., 2014).
Socioeconomic status: Women with lower poverty status and women
higher educational levels had a lower incidence of pelvic organ prolapse
symptoms when compared to those women with lower or no degree of
education or with a worse economical position (WU et al, 2014; ELBISS;
OSMAN N; HAMMAD, 2015). Moreover, family income and education were also
already associated to respiratory muscle strength (BUCHMAN et al., 2008). To
categorize the family income variable, the Brazilian minimum monthly wage
(MW) was used as a reference. It is defined as the lowest remuneration that
workers can monthly receive as payment for their jobs. At the time of this
study’s interview, the MW in Brazil was equal to R$ 880.00 (around 250.00 US
dollars). Considering that according to the Statistics and Socioeconomic Studies
Department of Brazil (DIEESE, 2017), the sufficient minimum salary to meet the
definition of MW (the amount that should be able to supply the normal basic
needs for a family) should be more than four times the value established by the
Brazilian government, the family income in our sample was dichotomized as
less than 3MW and 3MW or more. Thus, this was a way to distinguish those
who are under of this proper amount (CÂMARA et al., 2015). Educational data
were categorized into less than basic education (less than seven years) or basic
education of more (more than seven years) (CÂMARA et al., 2015).
Body mass index (BMI): greater body weight is associated with pelvic
organ prolapse and respiratory muscle strength. Overweight and obese women
86
are more likely to have pelvic organ prolapse (GIRI et al., 2017; WU et al,
2014). Moreover, BMI was already associated to higher (SANTIAGO-
RECUERDA et al., 2007) and lower respiratory muscle strength (MAFORT et
al., 2016). A scale with a stadiometer (WELMY®, W100H, model R-110, Santa
Bárbara d'Oeste, Brazil) was used to measure height (m) and weight (kg), which
were used to calculate the BMI (kg/m2).
Walking per week: participants were questioned about how many days
and how much time per day they had walked for more than ten minutes in the
past week, and the subjects were categorized into the categories ‘less than 90
min/week’ and ‘90 min/week or more’ (CÂMARA et al., 2015). Physical activity
measures were associated to maximal respiratory pressures in previous studies
(NEDER, 1999; SANTOS et al., 2011). The association between physical
activity and pelvic organ prolapse remains under-studied and still needs more
longitudinal researches (NYGAARD et al., 2014; OUCHI et al., 2017), but we
hypothesized that this condition may limit mobility and, consequently, physical
activity levels.
Smoking: tobacco use was evaluated by self-report. It is associated to
respiratory muscle strength (CHEN, 1988; TANTISUWAT; THAVEERATITHAM,
2014) and to pelvic organ prolapse (RODRÍGUEZ-MIAS et al., 2015), although
some controversial results have been reported (ELBISS; OSMAN N; HAMMAD,
2015). According to smoking status, the sample was categorized in ‘never
smokers’ and ‘current or former smokers’.
Parity: Number of pregnancies is related to pelvic organ prolapse
(HENDRIX et al., 2002; WU et al, 2014) and to respiratory muscle strength
(BEN SAAD et al., 2006). Parity was dichotomized into ‘less than five births’ and
87
‘five births or more’. This cut-off was selected based on the definition of grand-
multipara (five children or more), which is associated to a greater risk of
adverse health outcomes (RAYAMAJHI; THAPA; PANDE, 2006).
For gathering all this information regarding the sample characteristics, as
physical and socioeconomic, physical activity, number of children and pelvic
floor data, volunteers were evaluated through a structured questionnaire
developed for this research.
Ethics
All participants were informed of the objectives and procedures of the
research study at first contact and signed a consent form. The study protocol
received ethics approval by the Ethics and Research Committee of the Federal
University of Rio Grande do Norte (approval number 1.875.802).
Data Analysis
Descriptive statistics for all variables were presented according to the
variable pelvic organ prolapse and analyzed using independent t-test. For
categorical variables, Chi-square tests were used for comparison of proportions.
Univariate linear regression models were used to determine the association
between the participants’ characteristics, pelvic organ prolapse and respiratory
muscle strength (MIP and MEP). For multivariate linear regression models, we
used the “backward” method and variables with statistically significant
contributions (p < 0.05) concerning both, pelvic organ prolapse and MIP or
MEP, remained in the model.
88
All analyses were performed using the Statistical Package for the Social
Sciences (SPSS) software program (SPSS version 19.0; IBM SPSS, Chicago,
IL, USA).
Results
Characteristics of participants are presented according to pelvic organ
prolapse (Table 1). In our sample, 14.7% of the women had symptomatic POP.
There were no significant difference in any of the demographics, socioeconomic
position, anthropometric, clinical and parity variables analyzed with respect to
the presence of pelvic organ prolapse (Table 1).
---Insert table 1 here---
The mean of respiratory pressures achieved by participants was -107,89
cmH2O (SD=46,87) for MIP and 98,31cmH2O (SD=30,47cmH2O) for MEP (data
no exposed). The table 2 shows the univariate and multivariate linear
regression results for MIP outcome. The symptomatic POP was not associated
with MIP. The variables age, education, body mass index (BMI), smoking status
and parity were associated with MIP in the univariate analysis, but only age,
BMI and smoking status are determinants for MIP in the multivariate model.
Older women and smokers or ex-smokers presented lower MIP values, while
those with higher BMI obtained higher MIP.
---Insert table 2 here---
The results of the univariate and multivariate analysis for MEP are
presented in table 3. In the univariate model, symptomatic POP, age, education,
BMI and parity were associated with MEP. Women with symptomatic POP had
lower maximal expiratory pressure (MEP) when compared to women without

89
this condition (β=-14,78; p=0,014). Similar to the results obtained with MIP,
those women with higher age and higher number of children (≥ 5 children)
achieved worse values of MEP, and those with higher BMI and more years of
studies (>7 years), higher values, in the univariate analysis. In the multivariate
model, only age, BMI and symptomatic POP are determinants for MEP.
---Insert table 3 here---
Discussion
In our study, we demonstrated that symptomatic POP is associated with
weaker expiratory muscle strength, despite being adjusted by relevant
confounders, such as age and BMI. For our knowledge, none study has
examined the association between this urogynecological disorder and
respiratory muscle strength, although some studies have suggested this
association to explain the relationship between POP and lower expiratory flows
(STRINIC et al., 1997; STRINIC et al., 2002). In our sample, women with
symptomatic POP presented a reduction of almost 15 cmH2O in the expiratory
muscle strength when compared to women without it. It has been already
reported that the respiratory muscle strength reduces around 0.8 to 2.4 cmH2O
per year in elderly (ENRIGHT et al., 1994). Thus, having POP has a similar
effect on expiratory muscle strength as being 19 years older, according to our
results.
Both abdominal and diaphragm muscles (among other respiratory
muscles) are part of a set of dynamic stabilizers of the spine, called core
(AKUTHOTA; NADLER, 2004), which also includes the pelvic floor and
multifidus muscles. It has been demonstrated that alterations in any of them
may influence each other’s functioning (AKUTHOTA; NADLER, 2004). Thus,

90
the pelvic floor weakness, evidenced in the occurrence of pelvic organ prolapse,
may contribute to abdominal weakness, and consequently to lower MEP.
In a previous study with healthy subjects, the contraction of the pelvic
floor muscles resulted in an increase in dynamic ventilatory maneuvers (PARK
et al., 2015). These results suggest that the contraction of these muscles leads
to an increase in the respiratory muscle recruitment, such as the abdominal
muscles, which is very important in maintaining dynamic breathing and capacity
during daily living activities (PARK et al., 2015).
The contraction of pelvic floor muscles is also associated to a contraction
in the abdominal muscles, such as transversus abdominis and obliquus internus
(NEUMANN; GILL, 2002). Moreover, when abdominal muscles are contracted,
the diaphragm moves upward and the pelvic floor muscles moves downward,
and the increased intra-abdominal pressure induces a contraction of the pelvic
floor muscles as well (CRESSWELL; GRUNDSTRÖM; THORSTENSSON,
1992). This is known as abdominal-pelvic synergy, which influences all core
muscles (NAGIB et al., 2005; NEUMANN; GILL, 2002).
Since the cross-sectional nature of these findings, it was not possible to
stablish causal inferences of this relationship. It is possible that the women with
POP avoid producing greater abdominal muscle contraction, because of the
fear of having the vaginal bulge sensation, and consequently producing lower
maximum expiratory pressures. Similarly, it is possible that a weakness in the
abdominal muscles, as found in those with lower MEP, direct overload the
pelvic floor muscles, due to the abdominal-pelvic synergy, leading to their
weakness over the long term. Longitudinal studies are necessary to elucidate
these hypotheses.
91
The first hypothesis can be refused for a previous study that showed that
during the Valsalva maneuver it occurs a contraction of transversus
abdominals, internal and external oblique muscles and co-contraction of the
pelvic floor muscle, moving cranially, parallel to the diaphragm, in order to resist
the increase of intra-abdominal pressure and to support continence and the
anatomical position of the pelvic organs (TALASZ et al., 2012). Thus, due to the
similarity of the maximal expiratory pressure maneuver with the Valsalva
maneuver (ATS/ERS, 2002), we suggest the first also does not provoke urine
leakage or pelvic organ descent, since they induce co-contraction of pelvic floor,
representing a protective effect on the pelvic floor against the increase of intra-
abdominal pressure (TALASZ et al., 2012).
In this study, only MEP was associated to POP, since the association
between MIP and this gynecological disorder was lost in the multivariate
analysis. Although the diaphragm muscle interferes in the abdominal-pelvic
synergy (PARK et al., 2015; AKUTHOTA; NADLER, 2004), the performance
during MIP evaluation reflects the strength mainly from muscles that are outside
the core group, as sternocleidomastoids and scalenes (YOKOBA, 2003), which
may explain our findings of non-relationship between MIP and POP. In addition,
some other studies evidenced that during the development of MIP maneuver,
there is a decrease of perineal pressure, as well as a reduction in the perineal
and abdominal electromyographic signals (MOREIRA, 2002; NAGIB, 2005).
The results of our study provide important aspects for practice. It is
possible that the pelvic floor muscle training, besides reducing the occurrence
and symptoms of POP (THUBERT; BAKKER; FRITEL, 2015), may also
contribute to a greater capacity of generate expiratory muscle strength. On the

92
other hand, it is also possible that women with POP can be benefited from an
expiratory muscle training program, developed, for example, through respiratory
devices. Additionally, in healthy subjects, voluntary contraction of the abdominal
muscles has come out with an increased pelvic floor muscle activity, showing
that abdominal muscle training can be used to rehabilitate those muscles
(SAPSFORD; HODGES, 2001).
Corroborating to this idea, one method that uses the contraction of
abdominal muscles and respiratory maneuvers for pelvic floor training is the
hypopressive exercise. This exercise involves three steps: first – a slow
diaphragmatic inspiration, followed by total expiration, and diaphragmatic
aspiration – a movement that brings the abdominal wall to the lumbar spine and
lastly, maintenance apnea for any seconds. Nevertheless, previously study did
not show additional benefits with hypopressive exercises when compared to
pelvic floor muscles training (RESENDE et al., 2012).
Limitations
This study has some limitations. It was not possible to perform clinical
evaluation to identify POP, which was evaluated by self-reporting. However, we
used a validated questionnaire for this and there is no reason to think that
people with lower MEP would under report this condition differently, leading to
bias towards no effect. Moreover, the questionnaire we used was able to
identify only symptomatic POP, which represents a more advanced degree of
pelvic floor disorder. Hence, more studies are needed to investigate the
association of lower grades of POP and respiratory muscle strength.

93
Conclusion
This study evidences that symptomatic pelvic organ prolapse influences
expiratory muscle strength, once women with this dysfunction showed lower
mean values of maximal expiratory pressure, in univariate analysis and after
adjusted for confounders, in the multivariate analysis. The relationship between
MEP and symptomatic pelvic organ prolapse may be explained by the
occurrence of an abdominal-pelvic synergy, shown, in this case, mainly
between the pelvic floor and the abdominal muscles. Our findings indicate a
need to include respiratory muscle training as part of the therapy for women
with symptomatic pelvic organ prolapse, particularly expiratory strengthening.
List of Abbreviations: MIP: Maximal Inspiratory Pressure; MEP: Maximal
Expiratory Pressures; MRP: Maximal Respiratory Pressure; POP: Pelvic Organ
Prolapse; BMI: Body Mass Index; MW: Monthly Wage; DIEESE: Statistics and
Socioeconomic Studies Department of Brazil; ANOVA: Analysis of Variance.
References
Abrams P, Cardozo L, Fall M, et al. The standardization of terminology in lower
urinary tract function: Report from the Standardization Subcommittee of the
International Continence Society. Urology 2003;61:37-49.
https://doi.org/10.1016/S0090-4295(02)02243-4
Akuthota V, Nadler SF. Core strengthening. Arch Phys Med Rehabil.
2004;85(3)(suppl 1):S86-S92.
94
American Thoracic Society-ATS. European respiratory society-ERS. Statement
on respiratory muscle testing. American Journal of Respiratory Critical Care
Medicine. 2002; 166,518–624.
Atlas do desenvolvimento humano. 2017.
http://www.atlasbrasil.org.br/2013/en/perfil_m/santa-cruz_rn/. Accessed 11 May
2017.
Barber MD, Neubauer NL, Klein-Olarte V. Can we screen for pelvic organ
prolapse without a physical examination in epidemiologic studies? Am J Obstet
Gynecol. 2006;195:942–8.
Ben Saad H, Tfifha M, Harrabi I, Tabka Z, Guenard H, Hayot M, Zbidi A.
Facteurs influençant les variables ventilatoires des Tunisiennes âgées de 45
ans et plus. Revue des Maladies Respiratoires. 2006; 23:324-38.
Brasil. Salário mínimo nominal e necessário. 2014.
http://www.dieese.org.br/analisecestabasica/salarioMinimo.html. Accessed
17January 2017.
Buchman AS, Boyle PA, Wilson RS, Leurgans S, Shah RC, Bennett DA.
Respiratory Muscle Strength Predicts Decline in Mobility in Older Persons.
Neuroepidemiology. 2008; doi:10.1159/000154930.
Bureau M; Carlson K. Pelvic organ prolapse: A primer for urologists. Can Urol
Assoc J 2017;11(6Suppl2):S125-30.
Chen HI. Effects of chronic smoking on respiratory muscle function. Chin J
Physiol. 1988;31:53-62.
Cresswell AG, Grundström H, Thorstensson A: Observations on intraabdominal
pressure and patterns of abdominal intra-muscular activity in man. Acta Physiol
Scand, 1992, 144: 409–418.
95
Da Câmara SM, Zunzunegui MV, Pirkle C, Moreita MA, Maciel AC. Menopausal
status and physical performance in middle aged women: a cross-sectional
community-based study in Northeast Brazil. PLoS One. 2015; doi:
10.1371/journal.pone.0119480.
De Melo Barcelar J, Aliverti A, Rattes C, et al. The expansion of the pulmonary
rib cage during breath stacking is influenced by age in obese women. PLoS
One. 2014; doi:10.1371/journal.pone.0110959.
De Yébenes MJ, Otero A, Zunzunegui MV, Rodríguez-Laso A, Sánchez-
Sánchez F, Del Ser T. Validation of a short cognitive tool for the screening of
dementia in elderly people with low educational level. Int J Geriatr Psychiatry.
2003;18:925-36.
Dietz HP. Prolapse worsens with age, doesn't it? Aust N Z J Obstet Gynaecol.
2008;48(6):587-91.
Elbiss HM, Osman N, Hammad FT. Prevalence, risk factors and severity of
symptoms of pelvic organ prolapse among Emirati women. BMC Urology.
2015;15:66. doi:10.1186/s12894-015-0062-1.
Enright PL, Kronmal RA, Manolio TA, Schenker MB, Hyatt RE. Respiratory
muscle strength in the elderly. Correlates and reference values. Cardiovascular
Health Study Research Group. Am J Respir Crit Care Med. 1994 Feb;149(2 Pt
1):430-8.
Fragoso CAV and Gill TM. Respiratory Impairment and the Aging Lung: A Novel
Paradigm for Assessing Pulmonary Function. J Gerontol A Biol Sci Med Sci.
2012 Mar; 67A(3): 264–275.doi: 10.1093/gerona/glr198
96
Giri A, Hartmann KE, Hellwege JN et al. Obesity and pelvic organ prolapse: a
systematic review and meta-analysis of observational studies. Am J Obstet
Gynecol. 2017;217(1):11-26.e3. doi: 10.1016/j.ajog.2017.01.039.
Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic
organ prolapse in the Women's Health Initiative: gravity and gravidity. Am J
Obstet Gynecol. 2002 Jun;186(6):1160-6.
Hodges PW, Sapsford R, Pengel LHM. Postural and Respiratory Functions of
the Pelvic Floor Muscles. Neurourology and Urodynamics 2007; 26:362–371.
Iglesia CB, Smithling KR. Pelvic Organ Prolapse. Am Fam Physician. 2017
;96(3):179-185.
Leggett LE, Khadaroo RG, Holroyd-Leduc J, Lorenzetti DL, Hanson H, Wagg A,
et al. Measuring Resource Utilization: A Systematic Review of Validated Self-
Reported Questionnaires. Medicine. 2016; doi:
10.1097/MD.0000000000002759.
Lowder JL, Ghetti C, Nikolajski C, Oliphant S, Zyczynski H. Body image
perceptions in women with pelvic organ prolapse: a qualitative study. Am J
Obstet Gynecol. 2011 May;204(5):441.e1-5. doi: 10.1016/j.ajog.2010.12.024.
Mafort TT, Rufino R, Costa CH, Lopes AJ. Obesity: systemic and pulmonary
complications, biochemical abnormalities, and impairment of lung function.
Multidiscip Respir Med. 2016;12:11-28.
Moreira ECH, Brunetto AF, Castanho MMJ, Nakagawa TH, Yamaguti WPS.
Estudo da ação sinérgica dos músculos respiratórios e do assoalho pélvico.
Rev Bras Fisioter. 2002;6(2):71-6.
Nagib ABL, Guirro ECO, Palauro VA, Guirro RRJ. Avaliação da sinergia da
musculatura abdomino-pélvica em nulíparas com eletromiografia e biofeedback
perineal. Rev. Bras. Ginecol. Obstet. [online]. 2005; 27, n(4), 210-15.

97
Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function
tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med
Biol Res. 1999;32(6):719-27.
Neumann P, Gill V: Pelvic floor and abdominal muscle interaction: EMG activity
and intra-abdominal pressure. Int Urogynecol J Pelvic Floor Dysfunct, 2002, 13:
125–132
Nygaard IE, Shaw JM, Bardsley T, Egger MJ. Lifetime physical activity and
pelvic organ prolapse in middle-aged women. Am J Obstet Gynecol. 2014; 210:
477.e1–477.12.
Ouchi M, Kato K, Gotoh M, Suzuki S. Physical activity and pelvic floor muscle
training in patients with pelvic organ prolapse: a pilot study. Int Urogynecol J.
2017 Jun 17. doi: 10.1007/s00192-017-3356-x.
Park H, Han D. The effect of the correlation between the contraction of the
pelvic floor muscles and diaphragmatic motion during breathing. J. Phys. Ther.
Sci. 2015; 27: 2113–2115.
Park H, Hwang B, Kim Y. The impact of the pelvic floor muscles on dynamic
dynamic ventilation maneuvers. J. Phys. Ther. Sci. v.27, p. 3155-3157, 2015.
Rayamajhi R, Thapa M, Pande S. The challenge of grandmultiparity in obstetric
practice. Kathmandu University Medical Journal. 2006; 4:70-74.
Resende AP, Stüpp L, Bernardes BT, Oliveira E, Castro RA, Girão MJ, Sartori
MG. Can hypopressive exercises provide additional benefits to pelvic floor
muscle training in women with pelvic organ prolapse? Neurourol Urodyn. 2012
Jan;31(1):121-5. doi: 10.1002/nau.21149. Epub 2011 Oct 28.
98
Resende APM, Stüpp L, Bernardes BT, Franco GR, Oliveira E, Girão MJBC,
Sartori MGF. Prolapso genital e reabilitação do assoalho pélvico. Femina. 2010;
38(2):101-104.
Rodrigues AM, Oliveira LM, Martins KF, Roy CA, Sartori MGF, Girão MJBC,
Castro RA. Fatores de risco para o prolapso genital em uma população
brasileira. Rev Bras Ginecol Obstet. 2009; 31(1):17-21.
Rodríguez-Mias NL, Martínez-Franco E, Aguado J, Sánchez E, Amat-Tardiu L.
Pelvic organ prolapse and stress urinary incontinence, do they share the same
risk factors? Eur J Obstet Gynecol Reprod Biol. 2015 Jul;190:52-7. doi:
10.1016/j.ejogrb.2015.04.015.
Rogers RG, Rockwood TH, Constantine M et al. A new measure of sexual
function in women with pelvic floor disorders (PFD); Pelvic Organ
Prolapse/Incontinence Sexual Questionnaire, IUGA-Revised (PISQ-IR). Int
Urogynecol J. 2013;24(7):1091-103.doi:10.1007/s00192- 012-2020-8.
SANSES TVD, SCHILTZ NK, COURI BM, et al. Functional Status in Older
Women Diagnosed with Pelvic Organ Prolapse. American journal of obstetrics
and gynecology. 2016;214(5):613.e1-613.e7. doi:10.1016/j.ajog.2015.11.038.
Santiago-Recuerda A, Gómez-Terreros FJ, Caballero P, Martin-Duce A, Soleto
MJ, Vesperinas G, et al. Relationship between the upper airway and obstructive
sleep apneahypopnea syndrome in morbidly obese women. Obes Surg.
2007;17:689-97.
Santos, TM; Travensolo, C. F. Comparação da força muscular respiratória entre
idosos sedentários e ativos: estudo transversal. Revista Kairós Gerontologia,
14(6). ISSN 2176-901X. São Paulo (SP), Brasil, dezembro 2011: 107-121.
Tantisuwat A, Thaveeratitham P. Effects of smoking on chest expansion, lung
99
function, and respiratory muscle strength of youths. J Phys Ther Sci. 2014
Feb;26(2):167-70. doi: 10.1589/jpts.26.167.
Sapsford RR, Hodges PW. Contraction of the pelvic floor muscles during
abdominal maneuvers. Arch Phys Med Rehabil. 2001 Aug;82(8):1081-8.
Sousa ACP de A, Guerra RO, Thanh Tu M, Phillips SP, Guralnik JM,
Zunzunegui M-V. Lifecourse Adversity and Physical Performance across
Countries among Men and Women Aged 65-74. PLoS ONE.
2014;9(8):e102299. doi:10.1371/journal.pone.0102299.
Strinic T, Eterovic D, Dujic Z, Markovlc V, Tocilj J. Spirometric disorders in
women with genital descensus. Acta Obster Gynecol Scand 1997; 16: 879-883.
Talasz H, Kremser C, Kofler M, Kalchschmid E, Lechleitner M, Rudisch A. Proof
of concept: differential effects of Valsalva and straining maneuvers on the pelvic
floor. Eur J Obstet Gynecol Reprod Biol. 2012 Oct;164(2):227-33. doi:
10.1016/j.ejogrb.2012.06.019.
Tan JS, Lukacz ES, Menefee SA, Powell CR, Nager CW. Predictive value of
prolapse symptoms: a large database study. Int Urogynecol J. 2005;16:203–9.
Thubert T, Bakker E, Fritel X. Pelvic floor muscle training and pelvic floor
disorders in women. Gynecol Obstet Fertil. 2015 May;43(5):389-94. doi:
10.1016/j.gyobfe.2015.03.026. Epub 2015 Apr 25.
United Nations Development Programme (UNDP). Human Development Report
2014. Sustaining Human Progress: Reducing Vulnerabilities and Building
Resilience. 2017. http://hdr.undp.org/en/content/human-development-report-
2014. Accessed 17June 2017.
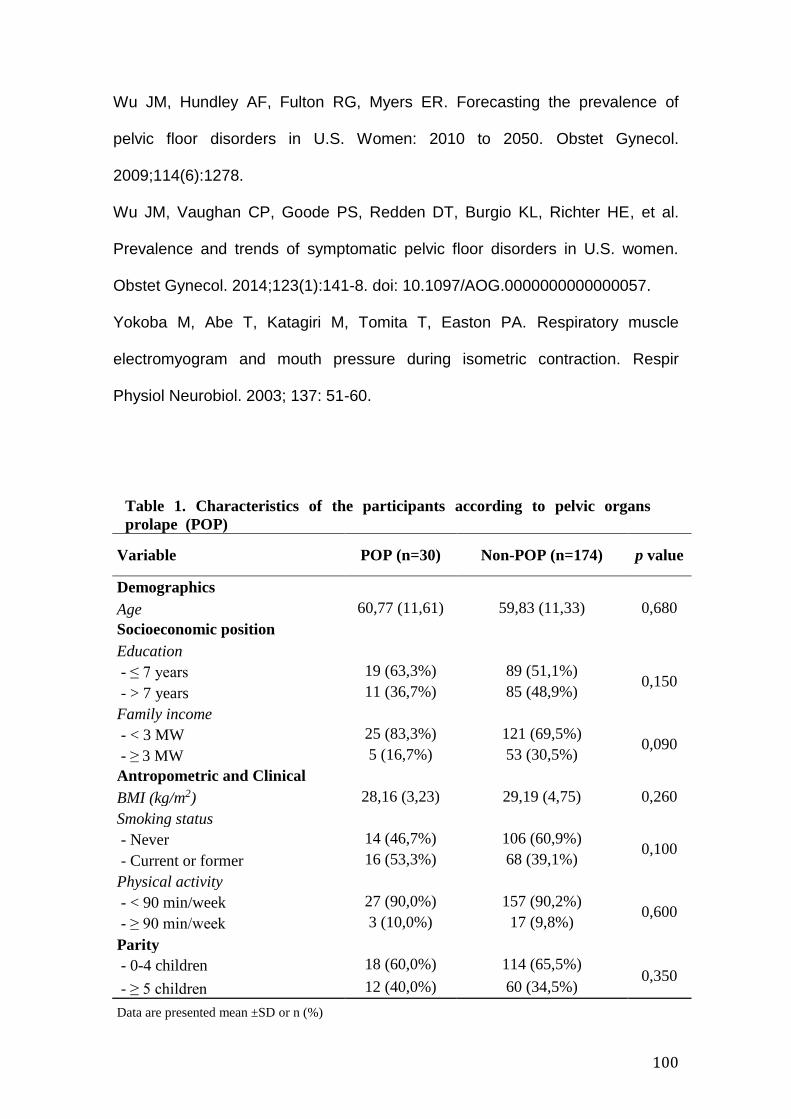
100
Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of
pelvic floor disorders in U.S. Women: 2010 to 2050. Obstet Gynecol.
2009;114(6):1278.
Wu JM, Vaughan CP, Goode PS, Redden DT, Burgio KL, Richter HE, et al.
Prevalence and trends of symptomatic pelvic floor disorders in U.S. women.
Obstet Gynecol. 2014;123(1):141-8. doi: 10.1097/AOG.0000000000000057.
Yokoba M, Abe T, Katagiri M, Tomita T, Easton PA. Respiratory muscle
electromyogram and mouth pressure during isometric contraction. Respir
Physiol Neurobiol. 2003; 137: 51-60.
Table 1. Characteristics of the participants according to pelvic organs
prolape (POP)
Variable POP (n=30) Non-POP (n=174) p value
Demographics
Age 60,77 (11,61) 59,83 (11,33) 0,680
Socioeconomic position
Education
- ≤ 7 years 19 (63,3%) 89 (51,1%) 0,150
- > 7 years 11 (36,7%) 85 (48,9%)
Family income
- < 3 MW 25 (83,3%) 121 (69,5%) 0,090
- ≥ 3 MW 5 (16,7%) 53 (30,5%)
Antropometric and Clinical
BMI (kg/m2) 28,16 (3,23) 29,19 (4,75) 0,260
Smoking status
- Never 14 (46,7%) 106 (60,9%) 0,100
- Current or former 16 (53,3%) 68 (39,1%)
Physical activity
- < 90 min/week 27 (90,0%) 157 (90,2%) 0,600
- ≥ 90 min/week 3 (10,0%) 17 (9,8%)
Parity
- 0-4 children 18 (60,0%) 114 (65,5%) 0,350
- ≥ 5 children 12 (40,0%) 60 (34,5%)
Data are presented mean ±SD or n (%)
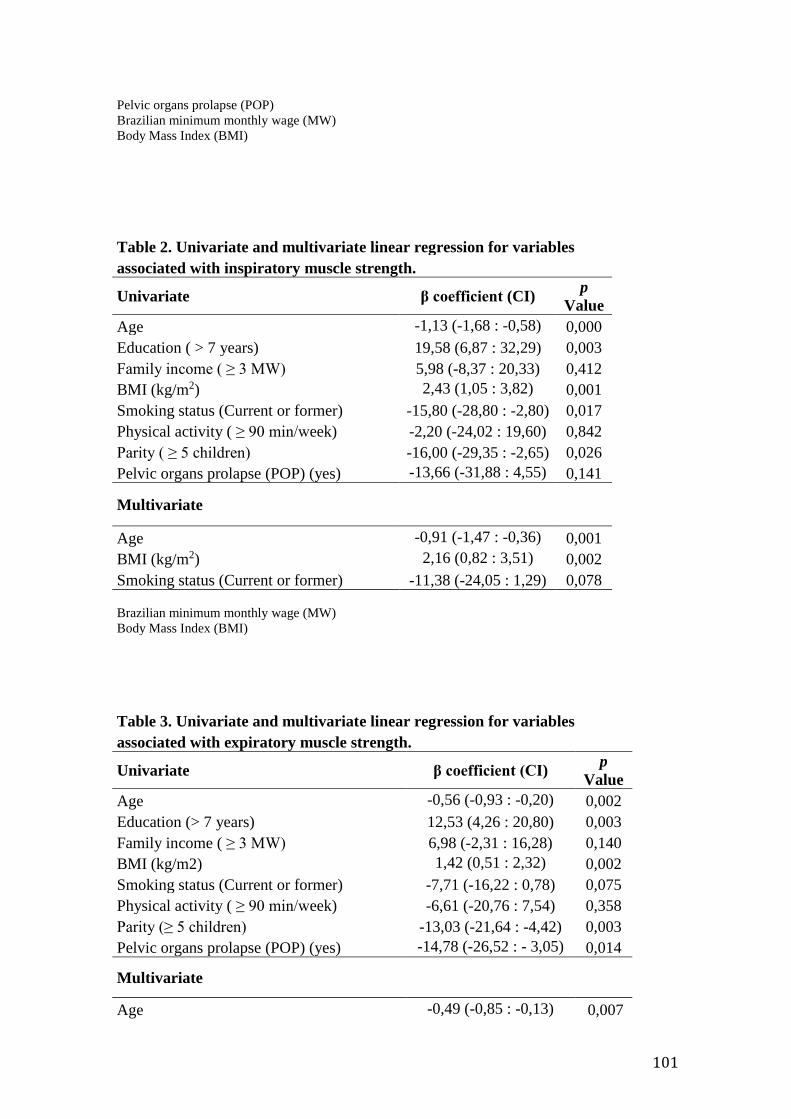
101
Pelvic organs prolapse (POP)
Brazilian minimum monthly wage (MW)
Body Mass Index (BMI)
Table 2. Univariate and multivariate linear regression for variables
associated with inspiratory muscle strength.
Univariate β coefficient (CI) p
Value
Age -1,13 (-1,68 : -0,58) 0,000
Education ( > 7 years) 19,58 (6,87 : 32,29) 0,003
Family income ( ≥ 3 MW) 5,98 (-8,37 : 20,33) 0,412
BMI (kg/m2) 2,43 (1,05 : 3,82) 0,001
Smoking status (Current or former) -15,80 (-28,80 : -2,80) 0,017
Physical activity ( ≥ 90 min/week) -2,20 (-24,02 : 19,60) 0,842
Parity ( ≥ 5 children) -16,00 (-29,35 : -2,65) 0,026
Pelvic organs prolapse (POP) (yes) -13,66 (-31,88 : 4,55) 0,141
Multivariate
Age -0,91 (-1,47 : -0,36) 0,001
BMI (kg/m2) 2,16 (0,82 : 3,51) 0,002
Smoking status (Current or former) -11,38 (-24,05 : 1,29) 0,078
Brazilian minimum monthly wage (MW)
Body Mass Index (BMI)
Table 3. Univariate and multivariate linear regression for variables
associated with expiratory muscle strength.
Univariate β coefficient (CI) p
Value
Age -0,56 (-0,93 : -0,20) 0,002
Education (> 7 years) 12,53 (4,26 : 20,80) 0,003
Family income ( ≥ 3 MW) 6,98 (-2,31 : 16,28) 0,140
BMI (kg/m2) 1,42 (0,51 : 2,32) 0,002
Smoking status (Current or former) -7,71 (-16,22 : 0,78) 0,075
Physical activity ( ≥ 90 min/week) -6,61 (-20,76 : 7,54) 0,358
Parity (≥ 5 children) -13,03 (-21,64 : -4,42) 0,003
Pelvic organs prolapse (POP) (yes) -14,78 (-26,52 : - 3,05) 0,014
Multivariate
Age -0,49 (-0,85 : -0,13) 0,007

102
BMI (kg/m2) 1,19 (0,29 : 2,08) 0,009
Pelvic organs prolapse (POP) (yes) -13,10 (-24,48 : -1,73) 0,024
Brazilian minimum monthly wage (MW)
Body Mass Index (BMI)

103
6. CONCLUSÕES
A partir dos achados do presente estudo, pode-se concluir que
mulheres com maiores números de gestações têm menores valores de
pressões respiratórias máximas, quando, após ajustadas por covaráveis,
apenas a pressão expiratória máxima se mantém associada ao número de
gestações. Além disso, mulheres com maiores níveis de escolaridade têm
maiores valores de pressões respiratórias máximas.
As mulheres que apresentam prolapso de órgãos pélvicos sintomático
aprensentam menores valores de pressão expiratória máxima, mas não há
associação entre pressão inspiratória máxima e a ocorrência de prolapso de
órgãos pélvicos sintomático, o que se mantém após ajustadas por covaráveis
Adicionalmente, o maior número de filhos é associado a menores valores de
pressões respiratórias máximas nas mulheres com POP sintomático.
Os achados deste estudo apontam para a necessidade de motivar as
mulheres grávidas, desde o período pré-natal até o pós-parto, a exercitar com
segurança seus músculos respiratórios, particularmente os abdominais. Além
disso, indica-se a importância em se incluir o treinamento muscular respiratório
como parte da terapia para mulheres com prolapso de órgãos pélvicos
sintomático, particularmente o fortalecimento expiratório.

104

105
7. CONSIDERAÇÕES FINAIS
Este estudo é parte de outro já realizado no município
de Parnamirim, com 500 mulheres, quando foram
evidenciadas associações entre as variáveis da história reprodutiva feminina e
a musculatura periférica. Os achados encontrados no presente estudo
evidenciam, por sua vez, a importância de se considerar a história reprodutiva
e alterações do assoalho pélvico como possíveis fatores que influenciam a
capacidade da mulher em gerar pressões respiratórias máximas.
A força muscular respiratória, estimada através das pressões
respiratórias máximas, está diretamente ligada à capacidade funcional e à
qualidade de vida de indivíduos, como já evidenciado na literatura. Portanto, é
de grande importância seu estudo e instituição de medidas para melhorá-las.
De acordo com as evidências encontradas na amostra estudada, o acréscimo
da avaliação, treinamento e acompanhamento de músculos respiratórios,
incluindo diafragma e abdominais, deve ser uma prática a ser considerada nos
serviços de Fisioterapia que tratam a saúde da mulher.
A construção da tese e dos artigos aqui incluídos me trouxeram
conhecimentos acerca da Epidemiologia e de uma área de Fisioterapia não
anteriormente explorada por mim: a da saúde da mulher. Desta forma,
encontrar associações entre a parte respiratória, a história reprodutiva e
prolapso de órgãos pélvicos nas participantes me mostraram a importância de
se avaliar o indivíduo como um todo, de maneira integral, considerando, além
de outros fatores, a sua história de vida e disfunções do assoalho pélvico. Além
disso, durante a escrita dos artigos, tive a colaboração de duas professoras de
diferentes centros internacionais (University of Hawaii at Manoa, nos Estados
106
Unidos, e Universidad Miguel de Hernández, na Espanha) e de áreas distintas,
me proporcionando um maior conhecimento científico, devido à diversidade da
atuação de ambas.
Neste período de doutoramento, tive a oportunidade de visitar um centro
de pesquisa em Saúde Pública nos Estados Unidos da América (Office of
Public Health Studies - University of Hawaii at Manoa), e trabalhar em dados de
um estudo multicêntrico, além de participar da construção de outro estudo
desenvolvido na cidade de Santa Cruz por nosso grupo de pesquisa, também
com população feminina, com participação de pesquisadores de vários centros.
Desta forma, acredito que neste processo contínuo de aprendizado,
chegar ao fim do Doutorado com essas vivências me proporcionaram um
grande conhecimento acerca da Epidemiologia e da Saúde Pública, o que será
de grande valia para execução de minha profissão e atuação no sistema
público de saúde brasileiro, contribuindo também, para uma melhor formação
de outros profissionais fisioterapeutas. Adicionalmente, considerando o período
de formação que me foi oferecido pelo sistema público brasileiro até hoje, sinto-
me agora, mais que nunca, na obrigação de devolver à sociedade o que em
mim foi investido durante esses anos até o título atualmente alcançado.

107
108
7. REFERÊNCIAS
ABRAMS, P.; CARDOZO, L.; FALL, M.; et al. The standardization of
terminology in lower urinary tract function: Report from the Standardization
Subcommittee of the International Continence Society. Urology. v.61, p.37-49,
2003. https://doi.org/10.1016/S0090-4295(02)02243-4
ABU-HEIJA, CHALABI HE. Great grand multiparity: is it a risk? J Obstet
Gynaecol. 1998;136-8.
AKUTHOTA, V.; NADLER, S.F. Core strengthening. Arch Phys Med Rehabil.
v.85, n.3, p.S86-S92, 2004.
ALLAL, N.; SEAR, R.; PRENTICE, A.M.; MACE, R. An evolutionary model of
stature, age at first birth and reproductive success in Gambian women. Proc.
Biol. Sci. 2004;271:465– 70.
AMERICAN THORACIC SOCIETY - ATS. European respiratory society ERS.
Statement on respiratory muscle testing. American Journal of Respiratory
Critical Care Medicine. v.166, n.4, p.518–624, 2002.
BARBER, M.D.; NEUBAUER, N.L.; KLEIN-OLARTE, V. Can we screen for
pelvic organ prolapse without a physical examination in epidemiologic studies?
Am J Obstet Gynecol. v.195, p.942-8, 2006.
BEN SAAD, H.; TFIFHA M.; HARRABI, I.; TABKA, Z.; GUENARD, H.; HAYOT,
M.; ZBIDI, A. Factors influencing pulmonary function in Tunisian women aged
45 years and more. Rev Mal Respir. 2006 Sep;23(4 Pt 1):324-38.
BLACK, L.F.; HYATT, R.E. Maximal respiratory pressures: normal values and
relationship to age and sex. Am Rev Respir Dis. v.99, n.5, p.696-702, 1969.

109
BOHANNON, R.W. Reference values for extremity muscle strength obtained by
hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med
Rehabil. v.78, n.1, p,26- 32,1997.
BOHANNON, R.W. Test-retest reliability of hand-held dynamometry during a
single session of strength assessment. Phys Ther. v.66, n.2, p.206-09, 1986.
BRASIL. MINISTÉRIO DA SAÚDE. Secretaria de Atenção à Saúde.
Departamento de Atenção Básica. Orientações para a coleta e análise de
dados antropométricos em serviços de saúde: Norma Técnica do Sistema de
Vigilância Alimentar e
Nutricional - SISVAN / Ministério da Saúde, Secretaria de Atenção à Saúde,
Departamento de Atenção Básica. – Brasília: Ministério da Saúde, 2011.
76 p.: il. – (Série G. Estatística e Informação em Saúde).
BRASIL. Salário mínimo nominal e necessário (julho). 2014. Disponível em:
http://www.dieese.org.br/analisecestabasica/salarioMinimo.html. Acesso em 19
de Janeiro de 2017.
BUCHMAN AS, Boyle PA, Wilson RS, Leurgans S, Shah RC, Bennett DA.
Respiratory Muscle Strength Predicts Decline in Mobility in Older Persons.
Neuroepidemiology. 2008;31(3):174-180. doi:10.1159/000154930.
BUREAU, M.; CARLSON, K. Pelvic organ prolapse: A primer for urologists. Can
Urol Assoc J. v.11, p.S125-30, 2017.
BURGER, H.G.; HALE, G.E.; ROBERTSON, D.M.; DENNERSTEIN, L. A review
of hormonal changes during the menopausal transition: focus on findings from
the Melbourne Women’s Midlife Health Project. Hum Reprod Update. v.13, n.6,
p.559–65, 2007.
110
BUTLER, L.; SANTORO, N. The reproductive endocrinology of the menopausal
transition. Steroids. v.76, n.7, p.627-35, 2011.
CARVALHO, J. A. M.; WONG, L. R. A transição da estrutura etária da
população brasileira na primeira metade do séculoXXI. Cad. Saúde Pública,
Rio de Janeiro, n. 24, v. 3, p. 597-605, mar. 2008.
CHENG, M. H.; WANG, S. J.; YANG, F. Y.; WANG, P. H.; FUH, J. L.
Menopause and physical performance: a community-based cross-sectional
study. Menopause. v. 16, n. 5, p. 892–896, 2009.
CHO, G.J.; SHIN, J.H.; YI, K.W.; PARK, H.T.; KIM, T.; HUR, J.Y.; KIM, S.H.
Adolescent pregnancy is associated with osteoporosis in postmenopausal
women. Menopause. v.19, n.4, p.456–460, 2012.
COOPER, R.; MISHRA, G.; CLENNELL, S.; GURALNIK, J.; KUH, D.
Menopausal status and physical performance in midlife: findings from a British
birth cohort study. Menopause. v.15, p.1079–1085, 2008.
CRAIG, C. L.; MARSHALL, A.L.; SJÖSTRÖM, M.; BAUMAN, A. E.; BOOTH, M.
L.; AINSWORTH, B. E.; PRATT, M.; EKELUND, U; YNGVE, A.; SALLIS, J. F.;
OJA, P. International physical activity questionnaire: 12-country reliability and
validity. Medicine & Science in Sports & Exercise. v. 35, n. 8, p. 1381-1395,
2003.
CRESSWELL, A.G.; GRUNDSTRÖM, H.; THORSTENSSON, A. Observations
on intraabdominal pressure and patterns of abdominal intra-muscular activity in
man. Acta Physiol Scand. v.144, p.409-418, 1992.
DA CÂMARA, S.M.; ZUNZUNEGUI, M.V.; PIRKLE, C.; MOREIRA, M.A.;
MACIEL, A.C. Menopausal status and physical performance in middle aged
111
women: a cross-sectional community-based study in Northeast Brazil. PLoS
One. v.10, n.3, e0119480, 2015.
DA CÂMARA, S.M.; PIRKLE, C.; MOREIRA., M.A.; VIEIRA, M.C.A.; VAFAEI,
A.; MACIEL, A.C. Early maternal age and multiparity are associated to poor
physical performance in middle-aged women from Northeast Brazil: a cross-
sectional community based study. BMC Womens Health. v. 15, p.56, 2015.
DE YEBENES, M. J., OTERO, A., ZUNZUNEGUI, M. V., RODRIGUEZ-LASO,
A., SANCHEZ- SANCHEZ, F., & DEL SER, T. Validation of a short cognitive
tool for the screening of dementia in elderly people with low educational level.
International Journal of Geriatric Psychiatry. v.18, n.10, p.925-936, 2003.
DEL NERO, U. Alterações Orgânicas no Climatério e Menopausa que
Repercutem sobre a Sexualidade Feminina. Femina. v.34, n.11, p.749-752,
nov. 2006.
DEMURA, S; SATO, S; KITABAYASHI, T. Percentage of total body fat as
estimated by three automatic bioelectrical impedance analyzers. Journal of
Physiological Anthropology and Applied Human Science. v. 23, p. 93–99, 2004.
DIAS, C.M.; PÁSSARO, C.P.; CAGIDO, V.R., EINICKER-LAMAS, M.; LOWE,
J.; NEGRI, E.M.; et al. Effects of undernutrition on respiratory mechanics and
lung parenchyma remodeling. J Appl Physiol. v.97, n.5, p.1888-96, 2004.
DIETZ, H.P. Prolapse worsens with age, doesn't it? Aust N Z J Obstet
Gynaecol. v. 48, n.6, p. 587-591, 2008.
DOHERTY, T. J. Physiology of ageing invited review: ageing and sarcopenia.
Journal of Applied Physiology, v. 95, n. 4, p. 1717-1727, 2003.
DORLAND, M.; VAN KOOIJ, R.J.; TE VELDE, E.R. General ageing and ovarian
ageing. Maturitas. v.30, p.113–118,1998.
112
ELBISS, H.M.; OSMAN, N.; HAMMAD, F.T. Prevalence, risk factors and
severity of symptoms of pelvic organ prolapse among Emirati women. BMC
Urology. v.15, p.66-71, 2015. doi:10.1186/s12894-015-0062-1.
ENRIGHT, P.L.; KRONMAL, R.A.; MANOLIO, T.A.; SCHENKER, M.B.; HYATT,
R.E. Respiratory muscle strength in the elderly. Correlates and reference
values. Cardiovascular Health Study Research Group. Am J Respir Crit Care
Med. v.149, p.430-8,1994.
FESS, E. Grip strength. In: Casanova JS, editor. Clinical assessment
recommendations. 2 ed. Chicago: American Society of Hand Therapists; 1992.
FRAGOSO, C.A.V.; GILL, T.M. Respiratory Impairment and the Aging Lung: A
Novel Paradigm for Assessing Pulmonary Function. J Gerontol A Biol Sci Med
Sci. v.67A, n.3, p.264-25, 2012.doi: 10.1093/gerona/glr198
FREITAS, S.F.; IBIAPINA, C.C.; ALVIM, C.G.; BRITTO, R.R.; PARREIRA, V.R.
Relação entre força de tosse e nível funcional em um grupo de idosos. Rev
Bras Fisioter, São Carlos. v.14, n.6, p.470-476, 2010.
GALVÃO, Lílian Lira Lisboa Fagundes. Tradução, adaptação e validação da
versão brasileira do questionário utian quality of life (uqol) para avaliação da
qualidade de vida no climatério. 2007. 78 f. Dissertação (Mestrado em Ciências
da Saúde) - Universidade Federal do Rio Grande do Norte, Natal, 2007.
GIRI, A., HARTMANN, K.E., HELLWEGE, J.N et al. Obesity and pelvic organ
prolapse: a systematic review and meta-analysis of observational studies. Am J
Obstet Gynecol. v.217, n.1, p.11-26, 2017.
GLASIER, A., GÜLMEZOGLU, A.M.; SCHMID, G.P.; MORENO, C.G.; VAN
LOOK, P.F.A. Sexual and reproductive health: a matter of life and death.
Lancet. v.368, p.1595-607, 2006.

113
GÓMEZ-CABELLO, A.; VICENTE-RODRÍGUEZ, G.; PINDADO, M.; VILA, S.;
CASAJÚS, J.A.; DE LA FUENTE, P.F.; et al. Increased risk of obesity and
central obesity in sedentary postmenopausal women. Nutr Hosp. v.27, p.865-
70, 2012.
GREENE, J. G. Construcción de una escala climatérica estándar. Rev
Climaterio, v. 1, p. 292-301, 1998.
GREGORY, P.C.; SZANTON, S.L.; XUE, Q.L.; TIAN, J.; THORPE, R.J.; FRIED,
L.P. Education predicts incidence of preclinical mobility disability in initially
highfunctioning older women. The Women’s health and aging study II. J
Gerontol A Biol Sci Med Sci, v.66, n.5, p.577–581, 2011.
GURALNIK, J.M.; SIMONSICK, E.M.; FERRUCCI, L.; GLYNN, R.J.;
BERKMAN, L.F.; et al. A Short Physical Performance Battery assessing lower
extremity function: Association with self-reported disability and prediction of
mortality and nursing home admission. J. Gerontol. v.49, n.2, M85–M94,1994.
HALE, G.E.; BURGER, H.G. Hormonal changes and biomarkers in late
reproductive age, menopausal transition and menopause. Best Pract Res Clin
Obstet Gynaecol., v. 23, n. 1, p. 7-23, 2009.
HANSEN, Å.M.; ANDERSEN, L.L.; SKOTTE, J.; CHRISTENSEN,
U.; MORTENSEN, O.S.; MOLBO, D.; et al. Social class differences in physical
functions in middle-aged men and women. J. Aging Health. v.26, n.1, p.88–105,
2014.
HARDY, R.; KUH, D. Social and environmental conditions across the life course
and age at menopause in a British birth cohort study. BJOG. v.112, n.3, p.346–
354, 2005.
114
HARLOW, S.D.; GASS, M.; HALL, J.E.; LOBO, R.; MAKI. P.; REBAR, R.W.; et
al. Executive summary of the Stages of Reproductive Aging Workshop + 10:
addressing the unfinished agenda of staging reproductive aging. J. Clin.
Endocrinol. Metab. v.97, n.4, p.1159–68, 2012.
HENDRIX, S.L.; CLARK, A.; NYGAARD, I.; ARAGAKI, A.; BARNABEI,
V.; MCTIERNAN, A. Pelvic organ prolapse in the Women's Health Initiative:
gravity and gravidity. Am J Obstet Gynecol. v.186, n.6, p.1160-6, 2002.
HENRETTA, J.C. Early childbearing, marital status, and women’s health and
mortality after age 50. J Health Soc Behav. v.48, n.3, p.254-266, 2007.
HODGES, P.W.; SAPSFORD, R.; PENGEL, L.H.M. Postural and Respiratory
Functions of the Pelvic Floor Muscles. Neurourology and Urodynamics. v.26,
p.362-371, 2007.
HUGHES, M.A.; MYERS, B.S.; SCHENKMAN, M.L. The role of strength in
rising from a chair in the functionally impaired elderly. J Biomech. v.29, n.12,
p.1509-13, 1996.
IBGE - Instituto Brasileiro de Geografia e estatística. Diretoria de Pesquisas,
Coordenação de População e Indicadores Sociais, Estimativas da população
residente com data de referência 1º de julho de 2017. [online] Disponível na
internet via www URL:
https://cidades.ibge.gov.br/xtras/perfil.php?codmun=241120. Arquivo
consultado em 23 de outubro de 2017.
IGLESIA, C.B.; SMITHLING, K.R. Pelvic Organ Prolapse. Am Fam Physician. v.
96, n. 3, p.179-185, 2017.
IGLESIA, C.B.; SMITHLING, K.R. Pelvic Organ Prolapse. Am Fam Physician.
v.96, n.3, p.79-185, 2017.

115
INOUYE, S.K.; STUDENSKI, S.; TINETTI, M.E.; KUCHEL, G.A. Geriatric
syndromes: clinical, research and policy implications of a core geriatric concept.
Journal of the American Geriatrics Society, v.55, n.5, p.780–791, Mai, 2007.
INSTITUTO BRASILEIRO DE GEOGRAFIA E ESTATÍSTICA. Projeção da
população do Brasil por sexo e idade para o período 2000-2060; PROJEÇÃO
da população das Unidades da Federação por sexo e idade 2000-2030. Rio d e
Janeiro: IBGE, 2013. 21.
Disponívelem:<http://www.ibge.gov.br/home/estatistica/populacao/projecao_da
_populacao/2013/default.shtm>. Acesso em: maio. 2015.
JANSSEN, I; ROSS, R. Linking age - related changes in skeletal muscle mass
and composition with metabolism and disease. Journal of Nutrition, Health and
Ageing, v.9, n.6, p.408 - 419, nov/dez. 2005.
JANSSENS, J.P.; PACHE, J.C.; NOCOD, L.P. Physiological changes in
respiratory function associated with ageing. Eur Respir J. v.13, n.1, p.197-205,
1999.
JENSEN, D.; OFIR, D.; O'DONNELL, D.E. Effects of pregnancy, obesity and
aging on the intensity of perceived breathlessness during exercise in healthy
humans. Respir Physiol Neurobiol. v.167, n.1, p.87-100, 2009.
KAAJA RJ, GREER IA: Manifestations of chronic disease during pregnancy.
JAMA. v. 294, n.21, p.2751–2757, 2005.
KING, J. C. Physiology of pregnancy and nutrient metabolism. Amerincan
Journal of Clinical Nutrition. v. 71, n. 5, p. 1218S–1225S, 2000
KUH, D.; BASSEY, E.J.; BUTTERWORTH, S.; HARDY, R.; WADSWORTH,
M.E.; TEAM, M.S. Grip strength, postural control, and functional leg power in a
representative cohort of British men and women: associations with physical

116
activity, health status, and socioeconomic conditions. J Gerontol A Biol Sci Med
Sci. v.60, p.224–231, 2005.
LIEBERMAN D, KOPERNIK G, PORATH A, LAZER S, HEIMER D. Sub-clinical
worsening of bronchial asthma during estrogen replacement therapy in
asthmatic postmenopausal women. Maturitas. v.21, p.153-157, 1995.
LIMA, L.C.V.; BUENO, C.M.L.B. Envelhecimento E Gênero: A Vulnerabilidade
De Idosas No Brasil. Revista Saúde e Pesquisa. v. 2, n. 2, p. 273-280, 2009.
LORENZI, D. R. S.; BARACAT, E. C.; SACILOTO, B.; PADILHA, Jr I. Fatores
associados à qualidade de vida após a menopausa. Revista da Associação
Médica Brasileira. v. 52, n. 5, p. 312-317, 2006.
LORENZI, D. R.; CATAN, L. B.; MOREIRA, K.; ÁRTICO, G. R. Assistência à
mulher climatérica: novos paradigmas. Revista Brasileira de Enfermagem. v.
62, n. 2, p. 287-293, 2009.
LOWDER, J.L.; GHETTI, C.; NIKOLAJSKI, C.; OLIPHANT, S.; ZYCZYNSKI, H.
Body image perceptions in women with pelvic organ prolapse: a qualitative
study. Am J Obstet Gynecol. v.204, n.5, p.441, 2011. doi:
10.1016/j.ajog.2010.12.024.
MALAVOLTI, M.; MUSSI, C.; POLI, M.; FANTUZZI, A. L.; SALVIOLI, G.;
BATTISTINI, N., et al. Cross-calibration of eight-polar bioelectrical impedance
analysis versus dual-energy X-ray absorptiometry for the assessment of total
and appendicular body composition in healthy subjects aged 21-82 years. Annal
of Human Biology. v. 30, n. 4, p. 380-391, 2003.
MALTAIS, M.L.; DESROCHES, J.; DIONNE, I.J. Changes in muscle mass and
strength after menopause. J Musculoskelet Neuronal Interact. v.9, n4, p.186–
197, 2009.

117
MATSUDO, S.; ARAÚJO, T.; MATSUDO, V.; ANDRADE, D.; ANDRADE, E.;
OLIVEIRA, L. C.; BRAGGION, G. Questionário Internacional de Atividade
Física (IPAQ): Estudo de Validade e Reprodutibilidade no Brasil. Atividade
Física & Saúde. v. 6, n. 2, p. 5-18, 2001.
MATSUDO, S.; MATSUDO, V. Prescrição e benefícios da atividade física na
terceira idade. Revista Brasileira de Ciência e Movimento. v.6, n.4, p.19-30,
1992.
MCCLEAN, K.M.; KEE, F.; YOUNG, I.S.; ELBORN, J.S. Obesity and the lung:
1. Epidemiology. Thorax. v.63, n.7, p.649-54, 2008.
MCKINLAY, S.M.; BRAMBILLA, D.J.; POSNER, J.G. The normal menopause
transition. Maturitas. v.14, n.2, p.103–15, 1992
MOREIRA, E.C.H.; BRUNETTO, A.F.; CASTANHO, M.M.J.; NAKAGAWA, T.H.;
YAMAGUTI, W.P.S. Estudo da ação sinérgica dos músculos respiratórios e do
assoalho pélvico. Rev Bras Fisioter.v.6, n.2, p.71-76, 2002.
MURRAY, E.T.; HARDY, R.; STRAND, B.H.; COOPER, R.; GURALNIK,
J.M.; KUH, D. Gender and life course occupational social class differences in
trajectories of functional limitations in midlife: findings from the 1946 British birth
cohort. J. Gerontol. A. Biol. Sci. Med. Sci. v.66, n.12, p.1350–1359, 2011.
NAGIB, A.B.L.; GUIRRO, E.C.O.; PALAURO, V.A; GUIRRO, R.R.J. Avaliação
da sinergia da musculatura abdomino-pélvica em nulíparas com eletromiografia
e biofeedback perineal. Rev. Bras. Ginecol. Obstet. v.27, n.4, p.210-15, 2005.
NAIR, K.S. Aging muscle. The American Jounal of Clinical Nutrition. v.81,
n.5,p. 953-963, 2005.
NAKANO, M.M. Versão brasileira da Short Physical Performance Battery –
SPPB: adaptação cultural e estudo da confiabilidade. São Paulo, 2007.

118
Dissertação (Mestrado) - Faculdade de Educação, Universidade Estadual de
Campinas.
NARICI, M.V.; MAFFULLI, N. Sarcopenia: characteristics, mechanisms and
functional significance. British Medical Bulletin. v. 95, p. 139–159, 2010.
NEDER, J.A.; ANDREONI, S.; LERARIO, M.C.; NERY, L.E. References values
for lung fucntion tests. Maximal respiratory pressures and voluntary ventilation.
Braz J Med Biol Res. v.32, n.6, p. 719-727, 1999.
NEUMANN, P,; GILL, V. Pelvic floor and abdominal muscle interaction: EMG
activity and intra-abdominal pressure. Int Urogynecol J Pelvic Floor Dysfunct.
v.13, p.125-132, 2002.
NYGAARD, I.E.; SHAW, J.M.; BARDSLEY, T.; EGGER, M.J. Lifetime physical
activity and pelvic organ prolapse in middle-aged women. Am J Obstet Gynecol.
v.210, p.477, 2014.
OFIR, D.; LAVENEZIANA, P.; WEBB, K.A.; LAM, Y.M.; O’DONNELL, D.E. Sex
differences in the perceived intensity of breathlessness during exercise with
advancing age. J. Appl. Physiol. v.104, n.6, p.1583–1593, 2008.
OMS. Global database on Body Mass Index. Disponível em:
http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Acesso em: 10 de
Janeiro de 2017.
OMS. Waist circumference and waist–hip ratio: report of a WHO expert
consultation, Genébra, 8–11 de Dezembro, 2008.
ONADJA, Y.; ATCHESSI, N.; SOURA, B.A.; ROSSIER, C.; ZUNZUNEGUI,
M.V. Gender differences in cognitive impairment and mobility disability in old
age: a cross-sectional study in Ouagadougou, Burkina Faso. Arch Gerontol
Geriatr v.57, n.3, p.311–8, 2013.
119
OSKVIG RM. Special problems in the elderly. Chest. v.115(Suppl 5), p.158S-
64, 1999;
OUCHI, M.; KATO, K.; GOTOH, M.; SUZUKI, S. Physical activity and pelvic
floor muscle training in patients with pelvic organ prolapse: a pilot study. Int
Urogynecol J. 2017 Jun 17. doi: 10.1007/s00192-017-3356-x.
PARIKH, N.I.; Cnattingius, S.; Dickman, P.W.; Mittleman, M.A.; Ludvigsson,
J.F.; Ingelsson, E. Parity and risk of later-life maternal cardiovascular disease.
Am Heart J. v.159, p.215-21, 2010.
PARK, H.; HAN, D. The effect of the correlation between the contraction of the
pelvic floor muscles and diaphragmatic motion during breathing. J. Phys. Ther.
Sci. v. 27,p. 2113–2115, 2015.
PARK, H.; HWANG, B.; KIM, Y. The impact of the pelvic floor muscles on
dynamic ventilation maneuvers. J. Phys. Ther. Sci. v.27, p. 3155-3157, 2015.
PEGORARI, M.S.; RUAS, G.; PATRIZZI, L.J. Relationship between frailty and
respiratory function in the community-dwelling elderly. Braz J Phys Ther. v.17,
n.1, p.9-16, 2013.
PEREIRA, L.S., NARCISO, F.M.; OLIVEIRA, D.M.; COELHO, F.M.; SOUZA,
DDA G; DIAS, R,C. Correlation between manual muscle strength and
interleukin-6 (IL-6) plasma levels in elderly community-dwelling women.
Archives of Gerontology and Geriatrics. v. 48, p. 313–316, 2009.
PIRKLE, C.; SOUSA, A.C.P.A.; ALVARADO, B.; ZUNZUNEGUI, M.V. Early
maternal age at first birth is associated with chronic diseases and poor physical
performance in older age: cross-sectional analysis from the International
Mobility. BMC public Health. v.14, n.1, 293, 2014.
http://www.ncbi.nlm.nih.gov/pubmed/?term=Pegorari%20MS%5BAuthor%5D&cauthor=true&cauthor_uid=23538454
http://www.ncbi.nlm.nih.gov/pubmed/?term=Patrizzi%20LJ%5BAuthor%5D&cauthor=true&cauthor_uid=23538454
https://www.ncbi.nlm.nih.gov/pubmed/?term=Pereira%20LS%5BAuthor%5D&cauthor=true&cauthor_uid=18462819

120
RAYAMAJHI R, THAPA M, PANDE S. The challenge of grandmultiparity in
obstetric practice. Kathmandu University Medical Journal, v.4, n.1, p. 70-74,
2006.
RESENDE, A.P.; STÜPP, L.; BERNARDES, B.T.; OLIVEIRA, E.; CASTRO,
R.A.; GIRÃO, M.J.; SARTORI, M.G. Can hypopressive exercises provide
additional benefits to pelvic floor muscle training in women with pelvic organ
prolapse? Neurourol Urodyn. v.31, n. 1, p.121-125, 2012. doi:
10.1002/nau.21149. Epub 2011 Oct 28.
RESENDE, A.P.M.; STUPP, L.; BERNARDES, B.T.; FRANCO, G.R.;
OLIVEIRA, E.; GIRÃO, M.J.B.C.; SARTORI, M.G.F. Prolapso genital e
reabilitação do assoalho pélvico. Femina. v.38, n.2, , p.101-104, 2010.
RODOSKY, M.W., ANDRIACCHI, T.P.; ANDERSSON, G.B. The influence of
chair height on lower limb mechanics during rising. J Orthop Res. v.7, n.2,
p.266-71, 1989.
RODRIGUES, A.M.; OLIVEIRA, L.M.; MARTINS, K.F.; ROY, C.A.; SARTORI,
M.G.F.; GIRÃO, M.J.B.C.; CASTRO, R.A. Fatores de risco para o prolapso
genital em uma população brasileira. Rev Bras Ginecol Obstet. v.31, n.1, p.17-
21, 2009.
ROGERS, R.G.; ROCKWOOD, T.H.; CONSTANTINE, M.; et al. A new measure
of sexual function in women with pelvic floor disorders (PFD); Pelvic Organ
Prolapse/Incontinence Sexual Questionnaire, IUGA-Revised (PISQ-IR). Int
Urogynecol J. v.24, n.7, p.1091-103, 2013. doi:10.1007/s00192- 012-2020-8.
RUPPEL, G. Lung volume tests. In: Ruppel G (Editor), Manual of Pulmonary
Function Testing. 6th edn. Mosby, St. Louis, p. 1-25, 1994.
121
SAMSON, M.M.; MEEUWSEN, I.B.; CROWE, A.; DESSENS, J.A.; DUURSMA,
S.A.; VERHAAR, H.J. Relationships between physical performance measures,
age, height and body weight in healthy adults. Age Ageing. v.29, n.3, p.235–42,
2000.
SANSES, T.V.D.; SCHILTZ, N.K.; COURI, B.M.; et al. Functional Status in
Older Women Diagnosed with Pelvic Organ Prolapse. American journal of
obstetrics and gynecology. v.214, n.5, p.613, 2016.
doi:10.1016/j.ajog.2015.11.038.
SANTIAGO-RECUERDA, A.; GÓMEZ-TERREROS, F.J.; CABALLERO, P.;
MARTIN-DUCE, A.; SOLETO, M.J.; VESPERINAS, G.; et al. Relationship
between the upper airway and obstructive sleep apneahypopnea syndrome in
morbidly obese women. Obes Surg. v.17, n.5, p.689-97, 2007.
SANTOS, C.A.S.; DANTAS, E.E.M.; MOREIRA, M.H.R. Correlations of physical
aptitude: functional capacity, corporal balance and quality of life (QoL) among
eldery women submitted to a post-menopausal physical activities program.
Archives of Gerontology and Geriatrics, v. 55, p. 344-349, 2011.
SANTOS, TM; TRAVENSOLO, C. F. Comparação da força muscular
respiratória entre idosos sedentários e ativos: estudo transversal. Revista
Kairós Gerontologia, v.14, n.6, p.107-121, 2011.
TANTISUWAT, A.; THAVEERATITHAM, P. Effects of smoking on chest
expansion, lung function, and respiratory muscle strength of youths. J Phys
Ther Sci. v.26, n.2, p.167-70, 2014. doi: 10.1589/jpts.26.167.
SANTOS, TM; TRAVENSOLO, C. F. Comparação da força muscular
respiratória entre idosos sedentários e ativos: estudo transversal. Revista
Kairós Gerontologia, v.14, n.6. p.107-121, 2011.

122
SAPSFORD, R.R.; HODGES, P.W. Contraction of the pelvic floor muscles
during abdominal maneuvers. Arch Phys Med Rehabil. v.82, n.8, p.1081-8,
2001.
SHARMA G, GOODWIN J. Effect of aging on respiratory system physiology and
immunology. Clin Interv Aging. v.1, p. 253-260, 2006.
SILVA, T.A.A.; FRISOLI JUNIOR, A.; PINHEIRO, M.M.; SZEJNFELD, V.L.
Sarcopenia Associada ao Envelhecimento: Aspectos Etiológicos e Opções
Terapêuticas. Revista Brasileira de Reumatologia. v. 46, n.6, p. 391- 397,
nov/dez 2006.
SIMÕES, R.P.; CASTELLO, V.; AUAD, M.A.; DIONÍSIO, J.; MAZZONETTO, M.
Força muscular respiratória e sua relação com a idade em idosos de sessenta
a noventa anos. RBCEH. v.7, n.1, p.52-61, 2010.
SOULES, M.R.; SHERMAN, PARROTT, REBAR, R.; SANTORO, N.; UTIAN,
W.; WOODS, N. Executive summary: Stages of Reproductive Aging Workshop
(STRAW). Fertility and sterility. v. 76, n. 5, p. 874-878, 2001.
SOUSA, A.C.P. DE A.; GUERRA, R.O.; THANH, T.U.M.; PHILLIPS, S.P.;
GURALNIK, J.M.; ZUNZUNEGUI, M.V. Lifecourse Adversity and Physical
Performance across Countries among Men and Women Aged 65-74. PLoS
ONE. v.9, n.8, e102299, 2014. doi:10.1371/journal.pone.0102299.
SOUZA, R.B. Pressões respiratórias estáticas máximas. J Pneumol. v.28,
Suppl 3, p.S155-65, 2002.
SOWERS, M.; ZHENG, H.; TOMEY, K.; KARVONEN-GUTIERREZ,
C..; JANNAUSCH, M.; LI, X. Changes in Body Composition in Women over Six
Years at Midlife: Ovarian and Chronological Aging. J Clin Endocrinol Metab., v.
13, p. 895-901, 2007.

123
SOWERS, M.F.; POPE, S.; WELCH, G.; STERNFELD, B.; ALBRECHT, G. The
association of menopause and physical functioning in women at midlife. J Am
Geriatr Soc. v.49, n.11, p.1485–1492, 2001.
SPOSITO, G.; DIOGO, M.J.; CINTRA, F.A.; NERI, A.L.; GUARIENTO, M.E.; DE
SOUSA, M.L. Relationship between subjective well-being and the functionality
of elderly outpatients. Rev Bras Fisioter. v. 14, n. 1, p. 81-9, 2010.
STRINIC, T.; ETEROVIC, D.; DUJIC, Z.; MARKOVLC, V.; TOCILJ, J.
Spirometric disorders in women with genital descensus. Acta Obster Gynecol
Scand. v. 16, p.879-883, 1997.
TALASZ, H.; KREMSER, C.; KOFLER, M.; KALCHSCHMID, E.;
LECHLEITNER, M.; RUDISCH, A. Proof of concept: differential effects of
Valsalva and straining maneuvers on the pelvic floor. Eur J Obstet Gynecol
Reprod Biol. v.164, n.2, p.227-233, 2012. doi: 10.1016/j.ejogrb.2012.06.019.
TAN, J.S.; LUKACZ, E.S.; MENEFEE, S.A.; POWELL, C.R.; NAGER, C.W.
Predictive value of prolapse symptoms: a large database study. Int Urogynecol
J. v. 16, p.203-209, 2005.
THUBERT, T.; BAKKER, E.; FRITEL, X. Pelvic floor muscle training and pelvic
floor disorders in women. Gynecol Obstet Fertil. v.43, n.5, p.389-94, 2015. doi:
10.1016/j.gyobfe.2015.03.026. Epub 2015 Apr 25.
TOLEP, K.; HIGGINS, N.; MUZA, S.; CRINER, G.; KELSEN, S.G. Comparison
of diaphragm strength between healthy adult elderly and young men. Am J
Respir Crit Care Med. v.152, n.2, p.677-82, 1995.
TOM, S.E.; COOPER, R.; PATEL, K.V.; GURALNIK, J.M. Menopausal
Characteristics and Physical Functioning in Older Adulthood in the NHANES III.
Menopause. v.19, n.3, p.283–289, 2012.
124
TOOHEY, JS; KEEGAN, K.A. JR.; MORGAN, M.A.; FRANCIS, J.; TASK, S.;
DE VECIANA, M. The “dangerous multipara”: fact or fiction? Am J Obstet
Gynecol. v.172, p.683-6,1995.
TSENG, L.A.; EL KHOUDARY, S.R.; YOUNG, E.A.; FARHAT, G.N.; SOWERS,
M.; SUTTON-TYRRELL, K.; NEWMAN, A.B. The Association of Menopausal
Status with Physical Function:The Study of Women’s Health Across the Nation
(SWAN): Menopausal Status and Physical Function. Menopause. v.19, n.11,
p.1186-92, 2012.
VAN GEEL, T.A.; GEUSENS, P.P.; WINKENS, B.; SELS, J.P.; DINANT, G.J.
Measures of bioavailable serum testosterone and estradiol and their
relationships with muscle mass, muscle strength and bone mineral density in
postmenopausal women: a cross-sectional study. Eur. J. Endocrinol. v.160, n.4,
p.681–687, 2009.
VÉLEZ, M. P.; ALVARADO, B. E.; LORD, C.; ZUNZUNEGUI, M. V. Life course
socioeconomic adversity and age at natural menopause in women from Latin
America and the Caribbean. Menopause. v. 17, n. 3, p. 552-559, 2010.
ventilation maneuvers. J. Phys. Ther. Sci. v.27, p. 3155-3157, 2015.
VILAÇA, K.H.C.; CARNEIRO, J.A.O.; PESSANHA, F.P.A.S.; LIMA, N.K.C.;
FERRIOLLI, E.; MORIGUTI, J.C. Estudo comparativo da composição corporal
de idosas fisicamente ativas pelos métodos DXA e antropométrico. Rev. bras.
Ci. e Mov, v. 20, n. 3, p. 5-13, 2012.
WALL LL: Birth trauma and the pelvic floor: lessons from the developing
world. J women’s Health / Soc Adv Women’s Health Res. v.8, n.2, p.149-155,
1999.
125
WATSFORD, M.L.; MURPHY, A.J.; PINE, M.J.; COUTTS, A.J. The effect of
habitual exercise on respiratorymuscle function in older adults. J Aging Phys
Act. v.13, n.1, p.34-44. 2005.
WEST, J.B. Fisiologia Respiratória - Princípios Básicos - 9ª Ediçao, São Paulo,
2013.
WHITWORTH, J.A. World Health Organization (WHO)/International Society of
Hypertension (ISH) statement on management of hypertension. J. Hypertens.
v.21, n.11, p.1983–1992, 2003.
WORLD HEALTH ORGANIZATION (WHO). Facts about ageing 2015.
Disponível em: http://www.who.int/features/factfiles/ageing/ageing_facts/en/
Acesso em: 05 de janeiro de 2017.
WU, J.M.; HUNDLEY, A.F.; FULTON, R.G.; MYERS, E.R. Forecasting the
prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstet
Gynecol. v.114, n.6, p. 1278, 2009.
WU, J.M.; VAUGHAN, C.P.; GOODE, P.S.; REDDEN, D.T.; BURGIO, K.L.;
RICHTER, H.E.; et al. Prevalence and trends of symptomatic pelvic floor
disorders in U.S. women. Obstet Gynecol. v.123, n.1, p.141-8, 2014. doi:
10.1097/AOG.0000000000000057.
YOKOBA, M.; ABE, T.; KATAGIRI, M.; TOMITA, T.; EASTON, P.A. Respiratory
muscle electromyogram and mouth pressure during isometric contraction.
Respir Physiol Neurobiol. v.137, p.51-60, 2003.

126
8. APÊNDICES
127
APÊNDICE A – Termo de Consentimento Livre e Esclarecido
TERMO DE CONSENTIMENTO
UNIVERSIDADE FEDERAL DO RIO GRANDE DO NORTE
CENTRO DE CIÊNCIAS DA SAÚDE
CURSO DE FISIOTERAPIA
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
Prezada participante,
A senhora está sendo convidada a participar de uma pesquisa intitulada
“INFLUÊNCIA DO STATUS MENOPAUSAL E NÍVEIS HORMONAIS NA
FUNCIONALIDADE, FORÇA MUSCULAR E COMPOSIÇÃO CORPÓREA:
UM ESTUDO LONGITUDINAL”. O objetivo desta pesquisa é investigar as
alterações na funcionalidade, na força muscular e na composição corporal em
mulheres na perimenopausa e após a menopausa, bem como a influência dos
hormônios sexuais nessas possíveis alterações. A pesquisa será realizada
durante o período de 2 anos, com a realização de avaliações uma vez por ano.
Em cada avaliação, a senhora irá responder um Protocolo de Avaliação com
perguntas sobre os seus dados pessoais, dados sobre seu histórico
ginecológico e menstrual, também serão feitos exames de sangue para
avaliação de parâmetros bioquímicos e dosagem dos hormônios sexuais, além
de uma avaliação física sobre sua função, força muscular e composição
corporal. Não haverá qualquer procedimento que determine risco à sua vida ou
saúde durante a participação nessa pesquisa, porém você poderá sentir algum
desconforto durante a coleta de sangue devido à picada da agulha. Ainda
assim, na ocorrência de qualquer prejuízo comprovadamente decorrente desta
128
pesquisa, a senhora será indenizada pelos pesquisadores responsáveis. Os
resultados da pesquisa serão divulgados sem a identificação das voluntárias e
serão cumpridas as exigências da Resolução nº 196/96 do Conselho Nacional
de Saúde que trata sobre a bioética, sendo assegurada a sua privacidade
quanto aos dados confidenciais envolvidos na pesquisa. Para participar desta
pesquisa é necessário que a senhora autorize assinando este termo de
consentimento. Não haverá compensação financeira para a sua participação,
ela é voluntária. A senhora tem a liberdade de recusar-se a participar ou retirar
seu consentimento em qualquer fase da pesquisa, sem qualquer penalidade ou
prejuízo à sua saúde. E todos os gastos pertinentes ao desenvolvimento deste
estudo serão de responsabilidade dos pesquisadores. Em caso de dúvidas
sobre a pesquisa ou para qualquer pergunta sobre os seus direitos como
participante deste estudo, entrar em contato com Dr. Álvaro Campos Cavalcanti
Maciel na Universidade Federal do Rio Grande do Norte no endereço: Campus
Universitário, CP 1666 – Natal / RN, CEP: 59078 – 970 ou pelos telefones (84)
3342-2001; (84) 9129-6796, em qualquer momento da pesquisa ou até mesmo
após o término da mesma. Dúvidas a respeito da ética dessa pesquisa poderão
ser questionadas ao Comitê de Ética em Pesquisa da UFRN no endereço
Praça do Campus, Campus Universitário, CP 1666 – Natal / RN, CEP: 59078 –
970.
CONSENTIMENTO INFORMADO:
Li e entendi as informações acima. Conheço os objetivos e procedimentos, que
foram explicados pela pesquisadora e lidos posteriormente por mim. Concordo
em participar deste estudo baseado nas informações fornecidas. Sei que
receberei uma cópia assinada e datada deste termo de consentimento.

129
PARTICIPANTE DA PESQUISA:
Nome: ______________________________________________
Local: _______________________ Data: _______/_______/_______
_____________________________________________ Assinatura da participante
130
APÊNDICE B – Ficha de Avaliação
CENTRO DE CIÊNCIAS DA SAÚDE
DEPARTAMENTO DE FISIOTERAPIA
QUESTIONÁRIO DE AVALIAÇÃO
Identificação do entrevistador: ___________ Data: ____/____/_____
1-IDENTIFICAÇÃO DA PARTICIPANTE (No): _____________
Nº Cartão SUS:
Participou da pesquisa anterior? ( ) Sim ( ) Não _____________
Nome:_________________________________________________________________________________________
___________
Data de Nasc.: ___/___/____ Idade:_________ Telefone:_______________________________________
Endereço (ponto de
referência):________________________________________________________________________________
______________________________________________________________________________________________
__
Renda Individual mensal:___________________ Renda familiar
mensal:____________________________
LEGANES
As questões a seguir devem ser respondidas por você sem a ajuda de nenhuma outra
pessoa.”
Qual a data de hoje? Certo 1 Errado 0
Que horas são? Certo 1 Errado 0
Que dia da semana é hoje? Certo 1 Errado 0
Qual seu endereço completo? Certo 1 Errado 0
Em que cidade estamos? Certo 1 Errado 0
Qual a sua idade? Certo 1 Errado 0
Qual sua data de nascimento? Certo 1 Errado 0
Qual era o nome de solteira da sua mãe? Certo 1 Errado 0
4 Erros ou mais significa entrevista excluída.
Quantas pessoas dependem parcial ou totalmente da sua renda individual? (Fora você)___________
Até que ponto sua renda lhe permite atender às suas necessidades?
( 1 )Muito bem ( 2 )Suficiente ( 3 ) Não muito bem ( 4 ) Nem um pouco
Quantos anos de estudo têm o seu pai? ______________________ E a sua mãe? _____________________________
Qual a profissão do seu pai na maior parte da sua infância (primeiros 15 anos)?________________( ) Não sabe ( )
Não trabalhava
E da sua mãe? ______________________ ( ) Não sabe ( ) Não trabalhava
131
Anos de estudo:_____________________ Cor/Etnia (informado pela própria):
_________________
União Estável: ( ) Sim ( ) Não Tempo vida conjugal: ____________ Número de residentes:_______________
Religião:________________________-
DADOS DA BIOIMPEDÂNCIA: Avaliador ___________________ No de
registro:__________________
2- HISTÓRICO GINECOLÓGICO/OBSTÉTRICO
Idade da menarca: ___ anos Gestações:____ Partos:____ Normais: ___ Cesáreas: ____ Abortos:__________
Idade da primeira gestação:__________ Idade da última gestação:__________
Quanto tempo faz da última menstruação:__________________________
Já fez TH? (0) Nunca; (1) Estou usando atualmente; (2) Já usei. Qual a medicação?_______________________
Idade de ocorrência e sintomas climatéricos/menopausa:_________________
Já fez alguma cirurgia? ( ) Não
( ) HISTERECTOMIA (retirada do útero) há________(tempo) ( ) OOFORECTOMIA PARCIAL (1 ovário) há
________(tempo)
( ) OOFORECTOMIA TOTAL (retirada dos dois ovários) há _________(tempo) **EXCLUSÃO
( ) OUTRAS CIRURGIAS – Quais foram e há quanto
tempo?________________________________________________________
______________________________________________________________________________________________
_____________
3- DOENÇAS ASSOCIADAS
Algum médico ou enfermeiro já lhe disse que você possui:
Hipertensão arterial: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual?
_________________________________
Doenças cardíacas (coronária, angina, insuficiência cardíaca): (0) Não; (1) Sim; (2) Não sei – Usa medicamento?
Qual? _________________________________
Diabetes tipo 2: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual?
____________________________________
Câncer: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual? _________________________________
Doença respiratória crônica (bronquite, enfisema, asma, DPOC): (0) Não; (1) Sim; (2) Não sei – Usa medicamento?
Qual? _________________________________
Artrite/Artrose: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual? _________________________________
Depressão: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual? _________________________________
Dislipidemia: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual?
______________________________________
Osteoporose: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual?
______________________________________
Doenças na tireoide: (0) Não; (1) Sim; (2) Não sei – Usa medicamento? Qual?
_________________________________
Labirintite (0) Não; (1) Sim; (2) Não sei – Usa medicamento?
Qual?_________________________________________
Outras:________________________________________________________________________________________
__
132
Você diria que sua saúde é: ( ) excelente ( ) muito boa ( )boa ( )mais ou menos ( )ruim ( )não sei
4–HÁBITOS DE VIDA
Tabagismo: (0) Nunca fumou (1) Fumante atual – Quantos cig./dia?_______ (2) Ex-fumante
OBS: Fumantes são pessoas que fizeram uso de mais de três cigarros por dia por mais de seis meses até
o momento da pesquisa, e ex-fumantes são aqueles que não fumam mais, porém já fumaram em algum
momento da vida por um período > seis meses
Você ingere bebida alcoólica? (0) Não (1) Sim Frequência por mês:_______vezes
Você pratica exercícios físicos regularmente? (0) Não (1) Sim Qual? __________________ Frequência
por semana: ______ vezes duração em minutos da atividade
_______________________________
5- AVALIAÇÃO DO NÍVEL DE ATIVIDADE FÍSICA
NÍVEL DE ATIVIDADE FÍSICA (IPAQ):
1. a. Em quantos dias da última semana você caminhou por pelo menos 10 minutos contínuos, em casa ou
no trabalho, como meio de transporte para ir de um lugar para outro, por lazer, por prazer ou como forma de
exercício? ____dias/semana ( ) nenhum
1. b. Nos dias em que você caminhou pelo menos 10 minutos contínuos, quanto tempo no total você gastou
caminhando por dia? ____ horas ____minutos
2. a. Em quantos dias na semana você realizou atividades moderadas por pelo menos 10 minutos contínuos,
como por exemplo, pedalar leve na bicicleta, nadar, dançar, fazer ginástica aeróbica leve, jogar vôlei recreativo,
carregar pesos leves, fazer serviços domésticos na casa, no quintal ou no jardim, como varrer, aspirar, cuidar do
jardim, ou qualquer atividade que fez aumentar moderadamente sua respiração ou batimentos do coração (por favor,
não inclua a caminhada)? ____dias/semana ( ) nenhum
2. b. Nos dias em que você fez essas atividades moderadas por pelo menos 10 minutos contínuos, quanto
tempo no total você gastou fazendo essas atividades por dia? _____horas ____minutos
3. a. Em quantos dias da última semana você realizou atividades vigorosas por pelo menos 10 minutos
contínuos, como por exemplo correr, fazer ginástica aeróbica, jogar futebol, pedalar rápido na bicicleta, jogar
basquete, fazer serviços domésticos pesados em casa, no quintal, ou cavoucar no jardim, carregar pesos elevados ou
qualquer exercícios que fez aumentar muito sua respiração ou os batimentos do coração. _____dias/semana (
) nenhum
3. b. Nos dias em que você fez essas atividades vigorosas por pelo menos 10 minutos contínuos, quanto
tempo no total você gastou fazendo essas atividades por dia? _____horas _____minutos
As duas últimas questões são sobre o tempo em que você permanece sentado todo dia, no trabalho,
estudando, assistindo aula, em casa e durante o seu tempo livre. Isso inclui o tempo sentado estudando, descansando,
visitando um amigo, lendo, sentado ou deitado assistindo TV. Não inclua o tempo gasto sentado durante o transporte
em ônibus, trem ou carro.
4. a. Quanto tempo no total você gasta sentado durante um dia de semana? ____horas ____minutos
5. b. Quanto tempo no total você gasta sentado durante um dia de final de semana? ____horas _____minutos
6. MANOVACUOMETRIA – Avaliador_______________ Turno______________
PImáx
PEmáx

133
Related Documents











