Journal of Back and Musculoskeletal Rehabilitation 25 (2012) 245–252 245 DOI 10.3233/BMR-2012-0331 IOS Press Influence of cortisol and DHEA-S on pain and other symptoms in post menopausal women with fibromyalgia Rodrigo Pegado de Abreu Freitas a,∗ , Telma Maria Ara´ ujo Moura Lemos b , Maria Helena Constantino Spyrides c and Maria Bernardete Cordeiro de Sousa a a Department of Physiology – Graduate Program in Psychobiology, Federal University of Rio Grande do Norte, Natal, Brazil b Department of Clinical Analysis and Toxicology, Center for Health Sciences, Federal University of Rio Grande do Norte, Natal, Brazil c Department of Statistics, Federal University of Rio Grande do Norte, Natal, Brazil Abstract. Objective: This study aims to assess cortisol and dehydroepiandrosterone sulfate (DHEA-S) levels in post-menopausal women with FMS and correlate it with pain threshold and tolerance, depression and quality of life. Methods: We conducted a cross sectional observational study of 17 women with FMS (FMS group), and 19 healthy volunteers (CT group). Algometry, the Beck Depression Index (BDI) and Fibromyalgia Impact Questionnaire (FIQ) were used. Blood samples were collected in the morning (8:00–9:30 am) to determine cortisol and DHEA-S plasmatic levels by chemiluminescence. Results: Significant differences between groups were recorded for pain threshold and tolerance (p< 0.0001), BDI (p< 0.0001) and all FIQ parameters (p< 0.0001). No significant differences in cortisol levels were found between the two groups (p = 0.325). In the FMS group, a tangential effect was observed for DHEA-S (p = 0.094) and positive correlations were found between DHEA-S, pain threshold (p = 0.017) and pain tolerance (p = 0.044). No correlation was observed between cortisol and DHEA-S levels and the variables of depression and quality of life for either group. Conclusions: There seems to be an influence of the decreased levels of DHEA-S and increased pain sensitivity in post-menopausal women with FMS. Keywords: Fibromyalgia, cortisol, DHEA-S, pain, depression 1. Introduction Clinical experience in physical rehabilitation ser- vices, associated with findings in the literature, show a history of patients with physical and psychological symptoms related to functional limitation and loss of quality of life. Complementary evaluations show no ∗ Address for correspondence: Rodrigo P.A. Freitas, Department of Physiology, Postgraduate Program in Psychobiology, Federal Uni- versity of Rio Grande do Norte. Av. Sen. Salgado Filho, 3000 – Lagoa Nova, Natal–RN, 59075-000, Brazil. Tel.: +55 84 32153409; E-mail: [email protected]. alteration in muscles, tendons or bone structure and laboratory tests indicate no substantial abnormalities. It is significant that the clinical condition of patients worsens and treatment progress decreases when they report physical or emotional stress. This clinical pro- file is typical of fibromyalgia syndrome (FMS), a non- inflammatory rheumatic disease of unknown etiology. Symptoms include diffuse and chronic pain and the presence of tender points, mostly in the axial skele- ton [1,2]. Among the frequently associated symptoms are fa- tigue, sleep disturbances, morning stiffness, changes in pain perception, anxiety and depression [2]. When symptoms are present, FMS patients experience diffi- ISSN 1053-8127/12/$27.50 2012 – IOS Press and the authors. All rights reserved AUTHOR COPY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Journal of Back and Musculoskeletal Rehabilitation 25 (2012) 245–252 245DOI 10.3233/BMR-2012-0331IOS Press
Influence of cortisol and DHEA-S on painand other symptoms in post menopausalwomen with fibromyalgia
Rodrigo Pegado de Abreu Freitasa,∗, Telma Maria Araujo Moura Lemosb,Maria Helena Constantino Spyridesc and Maria Bernardete Cordeiro de Sousaa
aDepartment of Physiology – Graduate Program in Psychobiology, Federal University of Rio Grande do Norte,Natal, BrazilbDepartment of Clinical Analysis and Toxicology, Center for Health Sciences, Federal University of Rio Grande doNorte, Natal, BrazilcDepartment of Statistics, Federal University of Rio Grande do Norte, Natal, Brazil
Abstract. Objective: This study aims to assess cortisol and dehydroepiandrosterone sulfate (DHEA-S) levels in post-menopausalwomen with FMS and correlate it with pain threshold and tolerance, depression and quality of life.Methods: We conducted a cross sectional observational study of 17 women with FMS (FMS group), and 19 healthy volunteers(CT group). Algometry, the Beck Depression Index (BDI) and Fibromyalgia Impact Questionnaire (FIQ) were used. Bloodsamples were collected in the morning (8:00–9:30 am) to determine cortisol and DHEA-S plasmatic levels by chemiluminescence.Results: Significant differences between groups were recorded for pain threshold and tolerance (p < 0.0001), BDI (p < 0.0001)and all FIQ parameters (p < 0.0001). No significant differences in cortisol levels were found between the two groups (p =0.325). In the FMS group, a tangential effect was observed for DHEA-S (p = 0.094) and positive correlations were foundbetween DHEA-S, pain threshold (p = 0.017) and pain tolerance (p = 0.044). No correlation was observed between cortisol andDHEA-S levels and the variables of depression and quality of life for either group.Conclusions: There seems to be an influence of the decreased levels of DHEA-S and increased pain sensitivity in post-menopausalwomen with FMS.
Keywords: Fibromyalgia, cortisol, DHEA-S, pain, depression
1. Introduction
Clinical experience in physical rehabilitation ser-vices, associated with findings in the literature, showa history of patients with physical and psychologicalsymptoms related to functional limitation and loss ofquality of life. Complementary evaluations show no
∗Address for correspondence: Rodrigo P.A. Freitas, Departmentof Physiology, Postgraduate Program in Psychobiology, Federal Uni-versity of Rio Grande do Norte. Av. Sen. Salgado Filho, 3000 –Lagoa Nova, Natal–RN, 59075-000, Brazil. Tel.: +55 84 32153409;E-mail: [email protected].
alteration in muscles, tendons or bone structure andlaboratory tests indicate no substantial abnormalities.It is significant that the clinical condition of patientsworsens and treatment progress decreases when theyreport physical or emotional stress. This clinical pro-file is typical of fibromyalgia syndrome (FMS), a non-inflammatory rheumatic disease of unknown etiology.Symptoms include diffuse and chronic pain and thepresence of tender points, mostly in the axial skele-ton [1,2].
Among the frequently associated symptoms are fa-tigue, sleep disturbances, morning stiffness, changesin pain perception, anxiety and depression [2]. Whensymptoms are present, FMS patients experience diffi-
ISSN 1053-8127/12/$27.50 2012 – IOS Press and the authors. All rights reserved
AUTH
OR
COPY

246 R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia
culty performing physical activities, which negativelyaffects their quality of life [3–5]. FMSprevalence variesbetween 0.66% and 4.4% in the general population andis more common among women than men, particularlyin the 35- to 60- year age group [6].
Due to the lack of complementary exams describingcharacteristic alterations, FMS diagnosis is based onclinical criteria. The American College of Rheumatol-ogy [1] (ACR) established diagnostic criteria for thissyndrome in 1990. These include signs of intense mus-cle pain in different areas of the body (extensive pain)for at least three months, associated with increased sen-sitivity to pain in at least 11 of the 18 tender points.Other symptoms such as fatigue, depression, stress andsleep disturbances are also significant, but not essentialfor diagnosis [1,7].
Staud and Spaeth [8] described an abnormality inthe central pain processing system, including temporalsummation, as a possible cause for FMS. The persis-tence of nociceptive receptors in peripheral tissue mayprovoke plastic alterations in the central nervous system(CNS), causing central sensitization and greater painsensitivity. Walker and Littlejohn [9] suggest that men-tal health problems, especially depression, may occurwith musculoskeletal disturbances. Reciprocal rela-tionships exist between depression, sleep disturbances,pain and physical incapacity, leading to a vicious cycleof poor mental and physical health.
In addition to pain, fatigue and depression, we foundevidence of hormonal changes occurring with alter-ations in cortisol and adrenal steroid levels, such as de-hydroepiandrosterone (DHEA) and dehydroepiandros-terone sulfate (DHEA-S). Since this syndrome is high-ly common in perimenopausal and post-menopausalwomen, it is important to note the hormonal changes inthis reproductive period, with low testosterone, proges-terone, DHEA and DHEA-S [10,11]. Hormonal alter-ations occurring in the fertile,pre- and post-menopausalperiods appear to influence FMS symptoms. This sug-gests that sexual hormones may play an important rolein the pathogenesis and deterioration of FMS symp-toms [10,12,13].
Pamuk et al. [12] report an increase and worseningof generalized pain, fatigue and other FMS symptomsin post-menopausal women. In the same study, the au-thors observed that the incidence of early menopauseis significantly higher in FMS patients when comparedwith rheumatoid arthritis patients and healthy controls.The authors proposemenopause as one of the contribut-ing factors to FMS deterioration.
Some studies of women suffering from FMS showa correlation between low cortisol levels, pain and de-
pression. This finding points to a relationship betweendaily variations in the release of cortisol and pain in-tensity. Women with FMS have low levels of adrenalandrogens, changes in pain perception and increasinglevels of muscular fatigue [14,15].
There are no previous studies evaluating levels ofcortisol and DHEA-S in post-menopausal women withFMS who do not use hormone replacement and engagein physical therapies. Alterations in the production ofsex hormones during this reproductive period shouldbe considered. We aim to analyze possible changes inadrenocortical, cortisol and DHEA-S hormones usingchemiluminescence, as well as their possible correla-tion with pain, depression and quality of life in post-menopausal women with FMS.
2. Methods
This is a cross-sectional, observational study. Partic-ipantswere female volunteers clinically diagnosedwithFMS living in the city ofNatal,Brazil. All subjects con-sulted at the Medical Clinic of the Onofre Lopes Uni-versity Hospital (Federal University of Rio Grande doNorte) and attended the Physiotherapy Teaching Clinicat the Potiguar University. The study was approved bythe Research Ethics Committee of the Federal Univer-sity of Rio Grande do Norte.
2.1. Experimental groups
A total of 17 patients were examined, aged 42–68 years, who met the 1990 ACR [1] criteria for theclassification of FMS. The control group (CT) con-sisted of 19 healthy volunteers chosen randomly fromhospital personnel and those accompanying patients.
The reduced number of FMS group subjects is dueto the inclusion criteria adopted, namely: (a) med-ical diagnosis of FMS, (b) ability to understand thestudy objective and answer the questions, (c) beingpost-menopausal, (d) not using hormone replacementor other medications that affect the metabolism of sexhormones and cortisol, (e) not participating in physi-cal therapy or rehabilitation programs in the previousmonth. The CT group met all the inclusion criteriaexcept diagnosis of FMS and absence of both rheumat-ic and endocrinal disease. Exclusion criteria for bothgroups were: (a) proven cognitive deficit, such as de-mentia, (b) physical and/or organic difficulties, whenthese compromised questionnaire application and anal-gesic tests; (c) endocrine, rheumatic and/or autoim-
AUTH
OR
COPY

R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia 247
mune diseases including chronic fatigue syndrome,chronic pelvic pain, atypical depression, irritable bow-el syndrome, rheumatoid arthritis, gout and lupus; (d)use of corticosteroids, analgesics, anti-inflammatories,psychoactives and antidepressants; (e) history of seri-ous psychiatric disorders, alcohol or stimulant depen-dence, schizophrenia and personality disorders.
All participants were free of infection, inflammationor allergies for at least two weeks before blood collec-tion. Subjects were also asked if they had suffered anystressful experiences over that period, such as quarrelsor receiving bad news, or if they had engaged in intensephysical activity.
2.2. Hormonal measurements
Blood samples were collected in the early morn-ing (08:00–09:30 am) after an all night fast (at least8 hours). Three 15ml blood samples were taken atone-day intervals. Samples were centrifuged to obtainplasma and stored in a freezer at−20◦C for subsequentanalysis of cortisol and DHEA-S concentrations. Hor-mone levels were determined in duplicate by chemi-luminescence, using an Immulite 1000 ImmunoassaySystem and commercially available kits (Diagnos-tic Products Corporation – Immunolite Kits – 2000,USA). Subjects also underwent hematology, lipid, hep-atic and renal profiling. Variation coefficients were2.20% for cortisol and 1.32% for DHEA-S. Evalua-tions of pain sensitivity, mood and quality of life wereconducted on the first day of blood collection.
2.3. Evaluation of pain sensitivity and symptoms ofFMS
Algometry was carried out immediately after bloodcollection to record pain threshold and pain toleranceto pressure. Eighteen tender points were marked witha demographic pencil and assessed while patients werein an orthostatic position, with their feet slightly sep-arated. Pain sensitivity tests were performed on the18 points identified by ACR in accordance with Okifujiet al. [16]. This was done perpendicular to the skin at5- to 10- second intervals by the same qualified exam-iner. A pressure algometer was used (Pain Diagnosticsand Thermography , Great Neck, NY, USA), with arubber point 1cm in diameter. Pain threshold and tol-erance to pressure were quantified in kg/cm2. The ex-aminer positioned the rubber point above the area tobe examined and gradually increased the pressure by1 kg/cm2 per second. The pain thresholdwas measured
when the patient said “I’m starting to feel pain”. Tomeasure tolerance to pain, the patient was asked to bearthe maximum amount of pressure from the algometerand use the phrase “Stop, I cannot take anymore” whenthey were no longer able to do so. Patients were askedto use these exact phrases for total standardization ofthe test.
The purpose of the exam and instructions for re-sponding were first explained to the patients. Moodevaluationwas carried out individuallywith no interfer-ence from the examiner; however doubts were clarifiedwhen necessary.
Participant depression levels were assessed using theBeck Depression Inventory (BDI) [17], a self-reportingtool composed of 21 questions related to cognitivesymptoms and attitudes. For each question, patientsmust choose one or more phrases that best describe howthey felt in the previous week. The maximum score is63 points and high scores indicate severe depression.Beck et al. [18] suggest the following quantificationscores for depression: a score of less than 10 indicatesminimal or no depression; 10 to 18 signifies mild tomoderate depression, 19–29moderate to severe depres-sion and from 30 to 63 severe depression.
Quality of life was evaluated using the Brazilianversion of the Fibromyalgia Impact Questionnaire(FIQ) [3]. The FIQ is a brief 10-item, self-administeredinstrument that measures physical function, work sta-tus, depression, anxiety, sleep, pain, stiffness, fatigue,and well being. All the scales vary from 1 to 10, withhigh scores indicating negative impact and greater im-pairment. The total FIQ score is graded from 1 to100 points. Higher scores are related to greater im-pact of the disease on the patients’ functionality and acorresponding reduction in their quality of life [3,19].
2.4. Statistical analysis
Statistical analyses were developed using 6 soft-ware, with public access at http://www.r-project.org/,as well as GraphPad Prism 5 (GraphPad Software Inc.2009). Quantitative parameters were statistically de-scribed by mean (Mn) and standard deviation (SD).
The first step of statistical analysis was to test the nor-mal patterns of all parameters using the Shapiro-Wilktest. One-wayAnalysis ofVariance (ANOVA)was usedfor intragroup analyses to determine hormonal varia-tions between the three blood samples, in addition tothe unpaired Student’s t-test for intergroup paramet-ric analysis. The Mann-Whitney U-test was applied tocompare intergroup nonparametric means. A general-
AUTH
OR
COPY
248 R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia
Table 1Mean values (± SD) for measured variables in the fibromyalgia and control groupsand P-values for the comparison between both groups
GroupsVariables Fibromyalgia (N = 17) Control (N = 19) P-value
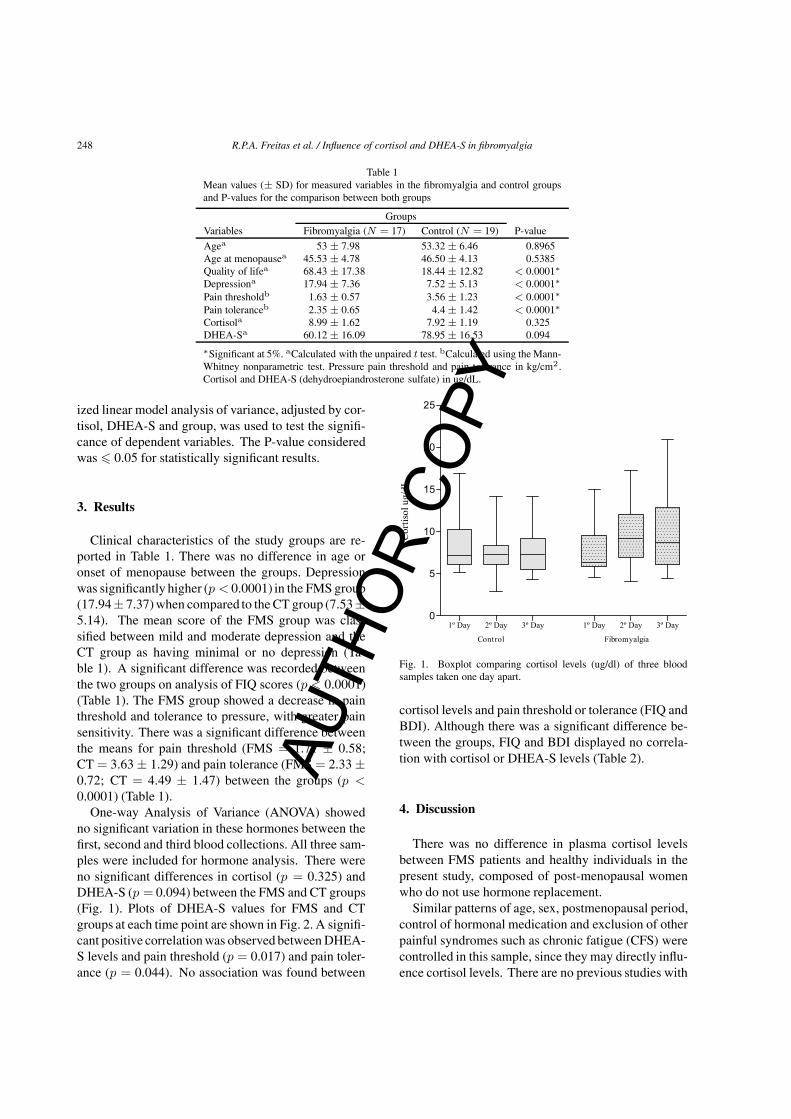
Agea 53 ± 7.98 53.32 ± 6.46 0.8965Age at menopausea 45.53 ± 4.78 46.50 ± 4.13 0.5385Quality of lifea 68.43 ± 17.38 18.44 ± 12.82 < 0.0001∗Depressiona 17.94 ± 7.36 7.52 ± 5.13 < 0.0001∗Pain thresholdb 1.63 ± 0.57 3.56 ± 1.23 < 0.0001∗Pain toleranceb 2.35 ± 0.65 4.4 ± 1.42 < 0.0001∗Cortisola 8.99 ± 1.62 7.92 ± 1.19 0.325DHEA-Sa 60.12 ± 16.09 78.95 ± 16.53 0.094
∗Significant at 5%. aCalculated with the unpaired t test. bCalculated using the Mann-Whitney nonparametric test. Pressure pain threshold and pain tolerance in kg/cm2 .Cortisol and DHEA-S (dehydroepiandrosterone sulfate) in ug/dL.
ized linear model analysis of variance, adjusted by cor-tisol, DHEA-S and group, was used to test the signifi-cance of dependent variables. The P-value consideredwas � 0.05 for statistically significant results.
3. Results
Clinical characteristics of the study groups are re-ported in Table 1. There was no difference in age oronset of menopause between the groups. Depressionwas significantly higher (p < 0.0001) in the FMS group(17.94± 7.37)when compared to the CT group (7.53±5.14). The mean score of the FMS group was clas-sified between mild and moderate depression and theCT group as having minimal or no depression (Ta-ble 1). A significant difference was recorded betweenthe two groups on analysis of FIQ scores (p < 0.0001)(Table 1). The FMS group showed a decrease in painthreshold and tolerance to pressure, with greater painsensitivity. There was a significant difference betweenthe means for pain threshold (FMS = 1.71 ± 0.58;CT = 3.63 ± 1.29) and pain tolerance (FMS = 2.33 ±0.72; CT = 4.49 ± 1.47) between the groups (p <0.0001) (Table 1).
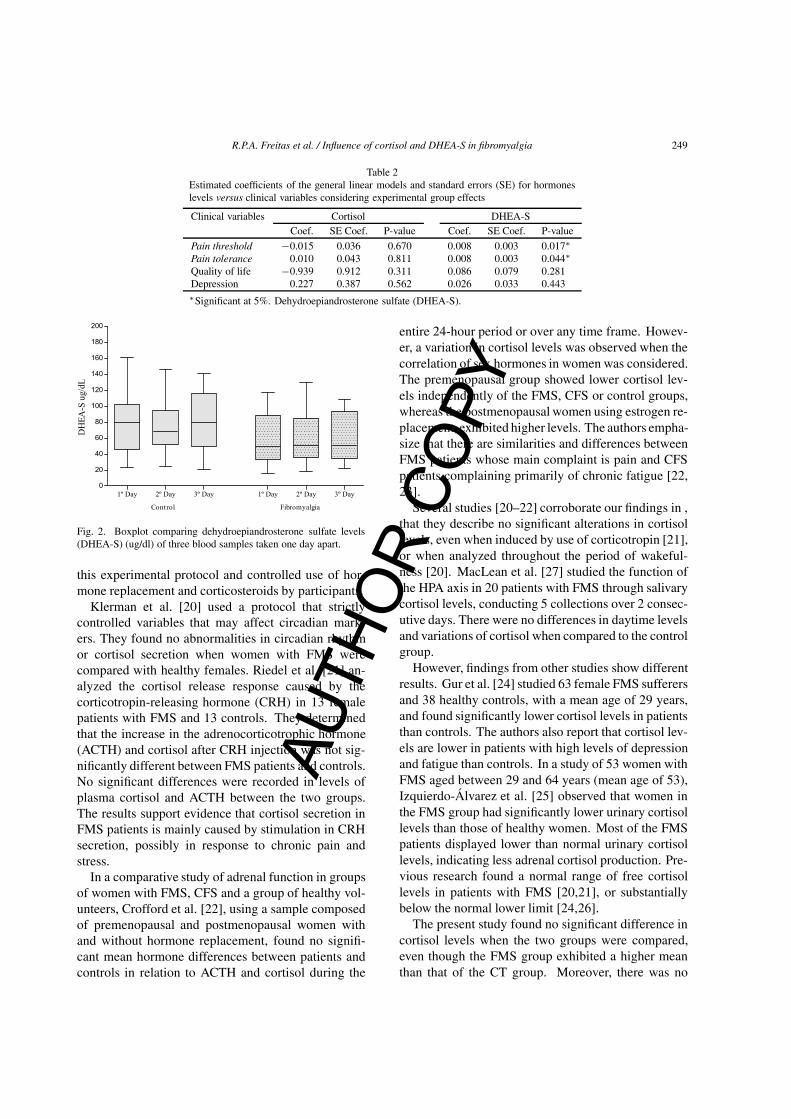
One-way Analysis of Variance (ANOVA) showedno significant variation in these hormones between thefirst, second and third blood collections. All three sam-ples were included for hormone analysis. There wereno significant differences in cortisol (p = 0.325) andDHEA-S (p = 0.094) between the FMS and CT groups(Fig. 1). Plots of DHEA-S values for FMS and CTgroups at each time point are shown in Fig. 2. A signifi-cant positive correlationwas observed between DHEA-S levels and pain threshold (p = 0.017) and pain toler-ance (p = 0.044). No association was found between
Fig. 1. Boxplot comparing cortisol levels (ug/dl) of three bloodsamples taken one day apart.
cortisol levels and pain threshold or tolerance (FIQ andBDI). Although there was a significant difference be-tween the groups, FIQ and BDI displayed no correla-tion with cortisol or DHEA-S levels (Table 2).
4. Discussion
There was no difference in plasma cortisol levelsbetween FMS patients and healthy individuals in thepresent study, composed of post-menopausal womenwho do not use hormone replacement.
Similar patterns of age, sex, postmenopausal period,control of hormonal medication and exclusion of otherpainful syndromes such as chronic fatigue (CFS) werecontrolled in this sample, since they may directly influ-ence cortisol levels. There are no previous studies with
AUTH
OR
COPY
R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia 249
Table 2Estimated coefficients of the general linear models and standard errors (SE) for hormoneslevels versus clinical variables considering experimental group effects
Clinical variables Cortisol DHEA-SCoef. SE Coef. P-value Coef. SE Coef. P-value
Pain threshold −0.015 0.036 0.670 0.008 0.003 0.017∗Pain tolerance 0.010 0.043 0.811 0.008 0.003 0.044∗Quality of life −0.939 0.912 0.311 0.086 0.079 0.281Depression 0.227 0.387 0.562 0.026 0.033 0.443∗Significant at 5%. Dehydroepiandrosterone sulfate (DHEA-S).
Fig. 2. Boxplot comparing dehydroepiandrosterone sulfate levels(DHEA-S) (ug/dl) of three blood samples taken one day apart.
this experimental protocol and controlled use of hor-mone replacement and corticosteroids by participants.
Klerman et al. [20] used a protocol that strictlycontrolled variables that may affect circadian mark-ers. They found no abnormalities in circadian rhythmor cortisol secretion when women with FMS werecompared with healthy females. Riedel et al. [21] an-alyzed the cortisol release response caused by thecorticotropin-releasing hormone (CRH) in 13 femalepatients with FMS and 13 controls. They determinedthat the increase in the adrenocorticotrophic hormone(ACTH) and cortisol after CRH injection was not sig-nificantly different between FMS patients and controls.No significant differences were recorded in levels ofplasma cortisol and ACTH between the two groups.The results support evidence that cortisol secretion inFMS patients is mainly caused by stimulation in CRHsecretion, possibly in response to chronic pain andstress.
In a comparative study of adrenal function in groupsof women with FMS, CFS and a group of healthy vol-unteers, Crofford et al. [22], using a sample composedof premenopausal and postmenopausal women withand without hormone replacement, found no signifi-cant mean hormone differences between patients andcontrols in relation to ACTH and cortisol during the
entire 24-hour period or over any time frame. Howev-er, a variation in cortisol levels was observed when thecorrelation of sex hormones in women was considered.The premenopausal group showed lower cortisol lev-els independently of the FMS, CFS or control groups,whereas the postmenopausal women using estrogen re-placement, exhibited higher levels. The authors empha-size that there are similarities and differences betweenFMS patients whose main complaint is pain and CFSpatients complaining primarily of chronic fatigue [22,23].
Several studies [20–22] corroborate our findings in ,that they describe no significant alterations in cortisollevels, even when induced by use of corticotropin [21],or when analyzed throughout the period of wakeful-ness [20]. MacLean et al. [27] studied the function ofthe HPA axis in 20 patients with FMS through salivarycortisol levels, conducting 5 collections over 2 consec-utive days. There were no differences in daytime levelsand variations of cortisol when compared to the controlgroup.
However, findings from other studies show differentresults. Gur et al. [24] studied 63 female FMS sufferersand 38 healthy controls, with a mean age of 29 years,and found significantly lower cortisol levels in patientsthan controls. The authors also report that cortisol lev-els are lower in patients with high levels of depressionand fatigue than controls. In a study of 53 women withFMS aged between 29 and 64 years (mean age of 53),Izquierdo-Alvarez et al. [25] observed that women inthe FMS group had significantly lower urinary cortisollevels than those of healthy women. Most of the FMSpatients displayed lower than normal urinary cortisollevels, indicating less adrenal cortisol production. Pre-vious research found a normal range of free cortisollevels in patients with FMS [20,21], or substantiallybelow the normal lower limit [24,26].
The present study found no significant difference incortisol levels when the two groups were compared,even though the FMS group exhibited a higher meanthan that of the CT group. Moreover, there was no
AUTH
OR
COPY

250 R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia
important correlation between cortisol and the symp-toms of pain, depression and quality of life in the FMSgroup.
FMS is predominant among women and its preva-lence increases with age. This suggests the role of sexsteroids in its etiopathology, indicating a relationshipbetween other neuroendocrine changes and symptomsof the syndrome. The adrenal gland is the main sourceof testosterone in women and is directly responsiblefor its production through DHEA and DHEA-S. Levelsof these androgens decrease in pre and postmenopauseand are inversely related to perceptions of stress andcortisol levels. This causes antagonistic physiologicaleffects with regard to corticosteroids [28–32].
Dessein et al. [32] studied 56 women with FMSin preand postmenopause and a group of healthy vol-unteers. They found a correlation between decreasedDHEA and pain perception. Several variables may af-fect this relationship, including age, menopausal state,body mass, use of oral contraceptives and recent use ofglucocorticoids. Our investigation observed a tendencytowards reduction in DHEA-S levels (p = 0.094) in theFMS group, suggesting a positive correlation betweenthis hormone and the pressure pain threshold (p =0.017) and tolerance (p = 0.044). There is indirectevidence that FMS may be a consequence of a declinein androgens since many of its antianabolic symptoms,such as muscular pain and fatigue, are typically asso-ciated with androgen deficiencies. Our data corrobo-rate the theory that androgens are associated with FMSsymptoms and are significant to pain perception [26,32].
In addition to relationship with reduced DHEA-S,the present study found that FMS significantly affectsquality of life, indicated by high FIQ scores. Manystudies show a decline in functional capacity in FMSpatients, especially among women, with pain and fa-tigue as the main causes [3,5,7]. Mood disturbancesand chronic depression are also related to functionalloss. Depression may worsen with physical or mentalstress as described in previous research [31,33,34].
All patients in the FMS group suffered from lightto moderate or moderate to serious depression. Thereis an obvious connection between FMS and depres-sion; however, its trigger mechanism is still uncertain.Depression in FMS is independent of the character-istics and severity of pain, but contributes to a deck-ine in quality of life and performance of daily activi-ties [34]. Berber et al. [35] studied the prevalence ofdepression and its relationship with quality of life in70 FMS patients. They observed a prevalence of 32.9%
for mild depression, 21.4% for moderate depressionand 12.9% for severe depression. The authors foundthat depression was responsible for a statistically sig-nificant decrease in quality of life scores, physical con-dition, physical functionality, pain perception, social,mental and emotional health and general health percep-tion [35,36]. Pae et al. [37] observed significant simi-larities between clinical signs of FMS, such as seriousdepression, neuroendocrinal abnormalities, psycholog-ical characteristics, and physical symptoms. However,current findings do not support the theory that seriousdepression and FMS have the same etiology; in otherwords, that one pathology supports the other.
In most FMS patients generalized pain is precededby chronic pain at the site of the initial painful stimu-lus. This nociceptive change is likely caused by alter-ations in neural plasticity due to constant neural stim-ulus by pain impulses in the spine, transmitted by A-Delta and C fibers. Tonic activity in C and A-Deltafibers can maintain central sensitivity [38–40]. Staudand Spaeth [8] refer to hyperexcitability in the spinaldorsal horn neurons as underlying the central sensitiv-ity occurring in FMS patients. This causes nociceptivestimulus in the brain. As a result, small stimulationsof the skin or muscle tissue highly stimulate the brain,intensifying pain sensitivity. A significant portion ofthe substantial pain variance in FMS patients can beexplained by psychological factors and disturbances inthe autonomic nervous system and HPA axis, owing totheir high degree of correlation [39].
In conclusion, this study shows that postmenopausalwomen with FMS that do not use hormone replace-ment exhibit higher pain sensitivity, depression andlower quality of life than healthy women. There was nosignificant difference in cortisol levels between FMSand CT groups, but positive correlations were foundbetween DHEA-S, pain threshold and pain tolerance.We suggest that reduced DHEA-S seems to influencethe symptoms of increased sensitivity to pain at thispost-reproductive phase.
Although the present study had some limitations,such as the small sample size and only three cortisolsamples per subject, our findings provide new informa-tion for clinical management in decreasing FMS symp-toms and improving the physical and psychologicalwell- being of patients. However, prospective longitu-dinal studies are needed to determine whether adreno-cortical parameters are a cause and/or consequence ofincreased sensitivity to pain in women with FMS.
AUTH
OR
COPY
R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia 251
Conflict of interest
The authors declare there is no conflict of interest.
References
[1] Wolfe F, Smythe HA, Yunus MB, et al. The American Col-lege of Rheumatology 1990 criteria for the classification offibromyalgia. Report of the multicenter criteria committee.Arthritis Rheum. 1990; 33: 160-172.
[2] Clauw DJ. Fibromyalgia: an overview. Am J Med. 2009;122(12 Suppl): S3-S13.
[3] MarquesAP, SantosAMB,AssumpcaoA,MatsutaniLA, LageLV, Pereira CAB. Validation of the brazilian version of the Fi-bromyalgia Impact Questionnaire (FIQ). Rev Bras Reumatol.2006; 46: 24-31.
[4] Robert M Bennett. Clinical Manifestations and Diagnosisof Fibromyalgia. Rheum Dis Clin N Am doi:10.1016/j.rdc.2009.05.009.
[5] Martinez JE, FerrazMB, SatoEI,AtraE. Sequential evaluationof the impact of fibromyalgia and rheumatoid arthritis in thequality of life. Rev Bras Reumatol. 1994; 34: 309-16.
[6] Cavalcante AB, Sauer JF, Chalot SD, et al. The Prevalence ofFibromyalgia: a Literature Review. Rev Bras Reumatol. 2006;46: 40-48.
[7] HaunMVA, FerrazMB, PollakDF. Validation of theAmericanCollege of Rheumatology 1990 criteria for the classificationof fibromyalgia in a Brazilian population. Rev Bras Reumatol.1990; 39: 221-30.
[8] Staud R, Spaeth M. Psychophysical and Neurochemical Ab-normalities of Pain Processing in Fibromyalgia. CNS Spectr.2008; 13: 12-17.
[9] Walker GJ, Littlejohn GO. Measuring quality of life inrheumatic conditions. Clin Rheumatol. 2007; 26: 671-3.
[10] Gupta A, Silman AJ. Psychological stress and fibromyalgia:a review of the evidence suggesting a neuroendocrine link.Arthritis Res Ther. 2004; 6: 98-106.
[11] Shuer ML. Fibromyalgia. Symptom constellation and poten-tial therapeutic options. Endocrine, 2003; 22: 67-75.
[12] Pamuk ON, Donmez S, Cakir N. Increased frequencies ofhysterectomy and early menopause in fibromyalgia patients:a comparative study. Clin Rheumatol. 2009; 28: 561-4.
[13] AbelesAM, PillingerMH, SolitarBM,AbelesM.Narrative re-view: the pathophysiology of Fibromyalgia. Ann Intern Med.2007; 15: 726-34.
[14] Bradley LA, McKendree-Smith NL, Alberts KR, Alarcon GS,Mountz JM, Deutsch G. Use of neuroimaging to understandabnormal pain sensitivity in fibromyalgia. Curr RheumatolRep. 2000; 2: 131-40.
[15] Finckh A, Berner IC, Aubry-Rozier B, So AK. A randomizedcontrolled trial of dehydroepiandrosterone in postmenopausalwomen with fibromyalgia. J Rheumatol. 2005; 32: 1336-40.
[16] Okifuji A, Turk JD, Sinclair D, Starz TW, Marcus DA. Astandardized manual tender point survey. Development anddetermination of a threshold point for identification of positivetender points in Fibromyalgia Syndrome. J Rheumatol. 1997;24: 377-383.
[17] Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An in-ventory for measuring depression. Arch Gen Psychiatry. 1961;4: 561-571.
[18] Beck AT, Steer RA, Garbin MG. Psychometric Properties ofthe Beck Depression Inventory: Twenty-Five Years of Evalu-ation. Clinical Psychology Review. 1988; 8: 77-100.
[19] Burckhardt CS, Clark SR, Bennett RM. The Fibromyalgia Im-pact Questionnaire: development and validation. J Rheumatol.1991; 18: 728-733.
[20] Klerman EB, Goldenberg DL, Brown EN, Maliszewski AM,Adler GK. Circadian Rhythms of Women with Fibromyalgia.J Clin Endocrinol Metab. 2007; 86: 1034-9.
[21] Riedel W, Schlapp U, Leck S, Netter P, Neeck G. Blunt-ed ACTH and Cortisol Responses to Systemic Injection ofCorticotropin-Releasing Hormone (CRH) in Fibromyalgia.Ann N Y Acad Sci. 2002; 966: 483-490.
[22] Crofford LJ, Young EA, Engleberg NC, et al. Basal circadianand pulsatile ACTH and cortisol secretion in patients withfibromyalgia and/or chronic fatigue syndrome. Brain BehavImmun. 2004; 18: 314-325.
[23] Crofford LJ, Neeck G. Neuroendocrine perturbations in fi-bromyalgia and chronic fatigue syndrome. Rheum Dis ClinNorth Am. 2000; 26: 989-1002.
[24] Gur A, Cevik R, Sarac AJ, Colpan L, Em S. Hypothalamic-pituitary-gonadal axis and cortisol in young women with pri-mary fibromyalgia: the potential roles of depression, fatigue,and sleep disturbance in the occurrence of hypocortisolism.Ann Rheum Dis. 2004; 63: 1504-1506.
[25] Izquierdo-Alvarez S, Bocos-Terraz JP, Bancalero-Flores JL,Pavon-Romero L, Serrano-Ostariz E, de Miquel CA. Is therean association between fibromyalgia and below-normal levelsof urinary cortisol? BMC Res Notes. 2008; 22; 1: 134.
[26] Geenen R, Jacobs J, Bijlsma J. Evaluation and managementof endocrine dysfunction in Fibromyalgia Rheumatic Disease.Rheum Dis Clin North Am. 2002; 28: 389-404.
[27] McLean SA, Williams DA, Harris RE, et al. Momentary rela-tionship between cortisol secretion and symptoms in patientswithfibromyalgia. Arthritis Rheum. 2005; 52: 3660-9.
[28] Tanriverdi F, Karaca Z, Unluhizarci K, Kelestimur F. Thehypothalamo-pituitary-adrenal axis in chronic fatigue syn-drome and fibromyalgia syndrome. Stress. 2007; 10: 13-25.
[29] Adler GK, Manfredsdottir VF, Creskoff KW. NeuroendocrineAbnormalities in Fibromyalgia. Curr Pain Headache Rep.2002; 6: 289-298.
[30] Cleare AJ, Miell J, Heap E, et al. Hypothalamic-pituitary-adrenal axis disfunction in chronic fatigue syndrome, and theeffects of low-close hydrocortisone therapy. J Clin EndocrinolMetab. 2001; 86: 3545-3554.
[31] Van Houdenhove B, Luyten P. Stress, depression and fi-bromyalgia. Acta Neurol Belg. 2006; 106: 149-56.
[32] Dessein PH, Shipton EA, Joffe BI, Hadebe DP, Stanwix AE,Van der Merwe BA. Hyposecretion of adrenal androgens andthe relation of serum adrenal steroids, serotonin and insulin-like growth factor-1 to clinical features in women with fi-bromyalgia. Pain. 1999; 83: 313-319.
[33] Vishne T, Fostick L, Silberman A, et al. Fibromyalgiaamong major depression disorder females compared to males.Rheumatol Int. 2008; 28: 831-836.
[34] Okifuji A, TurkDC, Sherman JJ. Evaluation of the relationshipbetween depression and fibromyalgia syndrome: why aren’tall patients depressed? J Rheumatol. 2002; 27: 212-9.
[35] Berber JSS, KupekE, Berber SC. Prevalence of depression andits relationshipwith quality of life in patientswithfibromyalgiasyndrome. Rev Bras Reumatol. 2005; 45: 47-54.
[36] Ravindran AV, Matheson K, Griffiths J, Merali Z, AnismanH. Stress, coping, uplifts and quality of life in subtypes of
AUTH
OR
COPY
252 R.P.A. Freitas et al. / Influence of cortisol and DHEA-S in fibromyalgia
depression: a conceptual frame and emerging data. J AffectDisord. 2002; 71: 121-30.
[37] Pae CU, Luyten P, Marks DM, et al. The relationship betweenfibromyalgia and major depressive disorder: a comprehensivereview. Curr Med Res Opin. 2008; 24: 2359-71.
[38] Staud R, Vierck CJ, Robinson ME, Price DD. Overall fi-bromyalgia pain is predicted by ratings of local pain and painrelated negative affect: possible role of peripheral tissues.
Rheumatology (Oxford). 2006; 45: 1409-1415.[39] Nielsen AL. Pathophysiological mechanisms in chronic mus-
culoskeletal pain (fibromyalgia): the role of central and pe-ripheral sensitization and pain disinhibition. Best Pract ResClin Rheumatol. 2007; 21: 465-480.
[40] Malt EA, Olafsson S, Lund A, Ursin H. Factors explainingvariance in perceived pain in women with Fibromyalgia. BMCMusculoskelet Disord. 2002; 25: 3-12.
AUTH
OR
COPY
Related Documents











