maduromikosis

Infeksi jamur tulang
Jan 18, 2016
maduromikosis etiologi gambaran klinis
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

maduromikosis
Maduromycosis
• a destructive chronic disease usually restricted to the feet, marked by swelling and deformity resulting from the formation of granulomatous nodules drained by sinuses connecting with the exterior, and caused by various actinomycetes (as of the genus Nocardia) and fungi (as of the genus Madurella)—called also mycetoma

• Geographic distribution: Seen in tropical region e.g. Asia, Africa, central and south America.
Etiologi
• caused by various fungi – (e.g. madurella mycetomi) or – actinomycetes (e.g. nocardia brasiliensis)
which usually affects the feet.

• Mode of infection: – Organisms are normally present in
environment (soil & dust). – Infection occurs in bare-footed persons after
minor penetrating skin injury inoculating soil organisms, occurring preferentially in rural areas, usually among labourers who work barefoot.
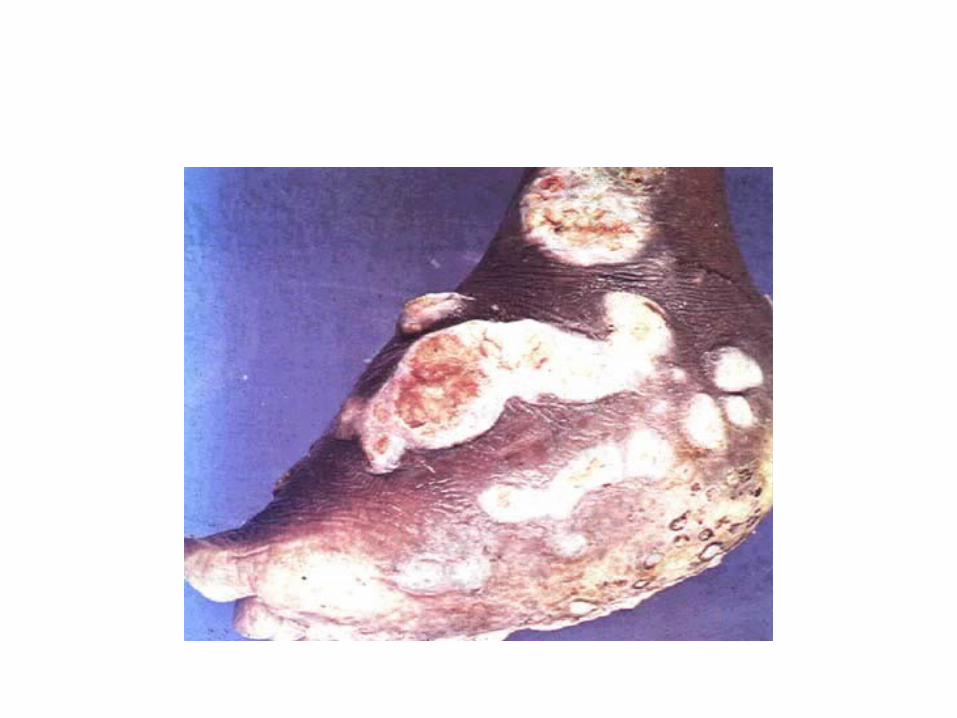
Gambaran Klinis• Initially a nodule, or abscess over months to years
progresses to a chronic infection • Lesions contain multiple sinus tracts that usually
discharge serosanguinous fluid and, at times, grossly visible granules of various colours, sized, and degrees of hardness depending on the agent involved. Superimposed bacterial infection may result in larger open ulcers.
• These changes eventually lead to deformity. • The changes on imaging are remarkable with the bones
being destroyed and remodeled.


Histopatologi
• Histologically, lapisan dermis dan subkutan mengandung abses yg terlokalisasi, terdapat satu atau lebih granule di bagian tengahnya.
• Eosinophilic, sel ‘Splendore-Hoeppli’ material sebagai batas granula nya.
• Between abscesses, there is extensive formation of granulation tissue, resulting in tumefaction and deformity that is often so severe as to be mistaken clinically for a neoplasm.
• Infection often involve contiguous bone, resulting in destructive osteomyelitis.
• Lymphatic or hematogenous dissemination from the primary subcutaneous lesion rarely occurs.


• Histologic section of mycetoma caused by Nocardiabrasiliensis demonstrating granulomatous inflammation and mixed cellular infiltrate.

• Histologic section of mycetoma caused by Nocardia brasiliensis, high magnification. Note the cellular infiltrate largely composed of lymphocytes and neutrophils, with scant eosinophils.
DD
• otentially similarly presenting conditions, including :– actinomycosis, – blastomycosis, – coccidioidomycosis, – leishmaniasis, – yaws, syphilis and – chronic osteomyelitis.
Treatment
• Eumycetomas should ideally be surgically removed prior to onset of bony involvement.
• Eumycetomas are frequently encapsulated, and care should be taken not to rupture the capsule, as this may lead to organism spread and mycetoma recurrence.
• Surgery may be curative, or may be followed by or performed in conjunction with systemic antifungal therapy.
• Antifungal options include itraconazole, posaconazole, fluconazole, ketoconazole and terbinafine, often given for a period of years.1,2,5
Related Documents











