Pergamon J. AerosolSci. Vol.27. No. 5, pp. 785-801, 1996 Publishedby Elsevier Science Ltd. Printedin Great Britain 0021-8502/96 $15.00+ 0.00 S0021-8502 (96) 00029-8 IN VIVO MEASUREMENTS OF NASAL AIRWAY DIMENSIONS AND ULTRAFINE AEROSOL DEPOSITION IN THE HUMAN NASAL AND ORAL AIRWAYS Kuo-Hsi Cheng,* Yung-Sung Cheng,* Hsu-Chi Yeh, ** Raymond A. Guilmette,t Steven Q. Simpson, ~ Yi-Hsin Yang ~ and David L. Swift* * Department of Environmental Health Sciences, The Johns Hopkins School of Hygiene and Public Health, Baltimore, MD 21205, U.S.A. * Inhalation Toxicology Research Institute, P.O. Box 5890, Albuquerque, NM 87185, U.S.A. Department of Medicine, University of New Mexico, Albuquerque, NM 87131, U.S.A. I Department of Biostatistics, University of North Carolina, Chapel Hill, NC 27599, U.S.A. (First received 26 October 1995; and in final form 31 January 1996) Abstract--Understanding the filtration efficiency of the nasal and oral airways is essential for assessing doses of inhaled particles to the extrathoracic region as well as to the lung. This paper presents in vivo measurements of nasal airway dimensions and the extrathoracic deposition of ultrafine aerosols in 10 normal adult males. The nasal geometry of each subject was characterized using magnetic resonance imaging and acoustic rhinometry. The nasal and oral deposition efficien- cies were measured for particles ranging from 4 to 150 nm at constant flow rates of 167 and 333 cm 3 s- 1. Results indicated that both nasal dimensions and particle deposition varied signifi- cantly among individuals. Inter-individual variability in particle deposition was correlated with the wide inter-individual variation of nasal dimensions measured by the total surface area, minimum cross-sectional area, and complexity of the airway shape. We concluded that the significant biological variability in extrathoracic filtration of ultrafine aerosols must be considered in develop- ing population-wide dosimetry of inhaled particles. Published by Elsevier Science Ltd. INTRODUCTION Inhalation is the major route of entry into the body for airborne toxic particles in the atmosphere, workplace, and domestic dwellings. The biological response caused by these inhaled particles depends on their site of deposition in the respiratory tract and on the physiological or toxic effects within the target tissue. It is necessary to determine the regional distribution of particle deposition within the human respiratory tract for a proper evaluation of the health risks resulting from aerosol intake and for an adequate design of air samplers that can provide useful estimates of inhaled dose. The extrathoracic airways, including the nasal passage, oral passage (because humans breathe through their noses and/or their mouths), pharynx, and larynx, are the first targets for inhaled particles as well as an important defense for the lung by reducing the number of particles penetrating to the more distal airways. Understanding the filtration efficiency of the nasal and oral passages is therefore crucial for assessing doses of inhaled particles to the extrathoracic airways and the lung. To establish appropriate exposure-dose relationships, it is important to characterize factors that affect the deposition of inhaled particles. Aerosol deposition in human respira- tory airways is strongly influenced by three major factors: physical (particle diameter, shape, and density), physiological (respiratory ventilation and pattern), and morphological (airway size and shape). Early deposition experiments of micrometer-sized particles in the human nasal passage focused on the effects of particle size and flow rate (Hounam et al., 1971; Fry and Black, 1973; Heyder and Rudolf, 1977), but did not address the potential influ- ence of nasal geometry on particle deposition. Recent studies by Rasmussen et al. (1990) using 2.6 ~m particles in 10 human subjects recognized nasal geometry as an important Author to whom all correspondence should be addressed. 785

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pergamon J. Aerosol Sci. Vol. 27. No. 5, pp. 785-801, 1996 Published by Elsevier Science Ltd. Printed in Great Britain
0021-8502/96 $15.00 + 0.00 S0021-8502 (96) 00029-8
I N VIVO MEASUREMENTS OF NASAL AIRWAY DIMENSIONS AND ULTRAFINE AEROSOL DEPOSITION IN THE H U M A N
NASAL AND ORAL AIRWAYS
Kuo-Hsi Cheng,* Yung-Sung Cheng,* Hsu-Chi Yeh, ** Raymond A. Guilmette,t Steven Q. Simpson, ~ Yi-Hsin Yang ~ and David L. Swift*
* Department of Environmental Health Sciences, The Johns Hopkins School of Hygiene and Public Health, Baltimore, M D 21205, U.S.A.
* Inhalation Toxicology Research Institute, P.O. Box 5890, Albuquerque, NM 87185, U.S.A. Department of Medicine, University of New Mexico, Albuquerque, NM 87131, U.S.A.
I Department of Biostatistics, University of North Carolina, Chapel Hill, NC 27599, U.S.A.
(First received 26 October 1995; and in final form 31 January 1996)
Abstract--Understanding the filtration efficiency of the nasal and oral airways is essential for assessing doses of inhaled particles to the extrathoracic region as well as to the lung. This paper presents in vivo measurements of nasal airway dimensions and the extrathoracic deposition of ultrafine aerosols in 10 normal adult males. The nasal geometry of each subject was characterized using magnetic resonance imaging and acoustic rhinometry. The nasal and oral deposition efficien- cies were measured for particles ranging from 4 to 150 nm at constant flow rates of 167 and 333 cm 3 s - 1. Results indicated that both nasal dimensions and particle deposition varied signifi- cantly among individuals. Inter-individual variability in particle deposition was correlated with the wide inter-individual variation of nasal dimensions measured by the total surface area, minimum cross-sectional area, and complexity of the airway shape. We concluded that the significant biological variability in extrathoracic filtration of ultrafine aerosols must be considered in develop- ing population-wide dosimetry of inhaled particles. Published by Elsevier Science Ltd.
INTRODUCTION
Inhalation is the major route of entry into the body for airborne toxic particles in the atmosphere, workplace, and domestic dwellings. The biological response caused by these inhaled particles depends on their site of deposition in the respiratory tract and on the physiological or toxic effects within the target tissue. It is necessary to determine the regional distribution of particle deposition within the human respiratory tract for a proper evaluation of the health risks resulting from aerosol intake and for an adequate design of air samplers that can provide useful estimates of inhaled dose. The extrathoracic airways, including the nasal passage, oral passage (because humans breathe through their noses and/or their mouths), pharynx, and larynx, are the first targets for inhaled particles as well as an important defense for the lung by reducing the number of particles penetrating to the more distal airways. Understanding the filtration efficiency of the nasal and oral passages is therefore crucial for assessing doses of inhaled particles to the extrathoracic airways and the lung.
To establish appropriate exposure-dose relationships, it is important to characterize factors that affect the deposition of inhaled particles. Aerosol deposition in human respira- tory airways is strongly influenced by three major factors: physical (particle diameter, shape, and density), physiological (respiratory ventilation and pattern), and morphological (airway size and shape). Early deposition experiments of micrometer-sized particles in the human nasal passage focused on the effects of particle size and flow rate (Hounam et al., 1971; Fry and Black, 1973; Heyder and Rudolf, 1977), but did not address the potential influ- ence of nasal geometry on particle deposition. Recent studies by Rasmussen et al. (1990) using 2.6 ~m particles in 10 human subjects recognized nasal geometry as an important
Author to whom all correspondence should be addressed.
785
786 K.-H. Cheng et al.
parameter responsible for significant inter-subject variability observed in nasal deposition. Rasmussen et al. suggested that the geometric factors in terms of the actual shape of the airway passage should be determined to interpret biological variability.
Several aerosols found to produce adverse effects in the respiratory tract contain ultrafine particles ranging from 0.0005 to 0.2 pm in diameter. For example, a significant portion of radon progeny in mines and homes are within the ultrafine size range (George et al., 1975; Reineking and Porstend6rfer, 1990; Hopke et al., 1990), and an increased risk of lung cancer associated with exposure to radon progeny in underground miners has widely been reported by epidemiological studies (NRC, 1988). Environmental tobacco smoke, a major source of indoor pollution, contains a number of particulate compounds regarded as known human carcinogens (NRC, 1986). Several studies have reported that the aerosols generated from environmental tobacco smoke are in the size range of 0.01-1 #m (Tu and Knutson, 1988; Li et al., 1992; Morawska and Philips, 1992). Based on a series of chronic inhalation studies in rats with different sizes of TiO2 and A1203 particles, the adverse pulmonary effects have been found to be more severe if the inhaled particles are in the ultrafine size range ( ~ 20 nm) (Ferin et al., 1991). A recent study by Oberd6rster et al. (1994) suggested that inhalation exposure to ultrafine particles ( ~ 26 nm) of polytetrafluroethylene, a low toxicity material if it is in the particle form >0.5 ~m, causes acute pulmonary toxicity leading to acute mortality in rats.
Diffusion is the mechanism of deposition of ultrafine particles; their very small diameter precludes any significant contribution from particle inertia or gravity settling at flow rates typical of breathing, either at rest or during heavy exercise. The majority of air flowing through the nasal or oral airway is in turbulent flow (Swift and Proctor, 1977; Hahn et al., 1993), even though the calculated Reynolds number (based on pipe flow) is transitional (Cheng et al., 1988). The complicated shape of these airways promotes turbulent, convective diffusional transport of ultrafine aerosols, leading to much greater transport of particles through the thin concentration boundary layer (Schlichting, 1968). The dependence of deposition efficiency upon flow rate shown by Cheng et al. (1993) in nasal replicate deposition studies is consistent with this view.
Most data on the efficiency of the human nasal and oral airways in filtering ultrafine particles have been obtained from studies using physical replicate casts. Results indicated that a substantial fraction of ultrafine particles deposits in the nasal and oral passages (Yamada et al., 1988; Cheng et al., 1991, 1993), and that the oral passage collects particles less efficiently than the nasal passage (Swift et al., 1994). Although the replicate casts are regarded as accurate in rendering the physical shape and configuration of the airways, the rigid and dry nature of these plastic casts makes them difficult to simulate the flexible and wet surface of the human airways. I n v ivo evidence of aerosol deposition is fundamentally essential for examining whether there are artifacts in the findings from replicate airway casts.
Morphometry of human nasal airways (Guilmette et al., 1989) and aerosol deposition in the nose (Heyder and Rudolf, 1977) have been measured individually. However, no study has attempted to relate these two measurements systematically. The aims of the present study were to measure in v ivo the nasal airway dimensions and the deposition of ultrafine aerosols in the nasal and oral passages, and to determine the relationship between nasal airway dimensions and aerosol deposition. A statistical procedure incorporated with the diffusion theory was used to model dimensional features of the nasal airway responsible for the biological variability in particle deposition.
METHODS
Ten healthy, adult, male volunteers were recruited for the present study. Deposition was measured in all 10 subjects with aerosols of four different particle diameters (0.004, 0.008, 0.02, and 0.15/~m) at two constant flow rates (167 and 333 cm 3 s-1). The nasal geometry of each subject was characterized using magnetic resonance imaging (MRI) and acoustic rhinometry (AR) techniques. MRI measurements were taken to determine the coronal

In vivo nasal and oral deposition
Table 1. Background information of the 10 human male subjects
787
Smoking Height Weight Subject Age Ethnicity history (cm) (kg)
A 30 Caucas i an Nonsmoker 192 80 B 41 Caucas i an Nonsmoker 185 89 C 42 Caucas i an Nonsmoker 178 77 D 58 Caucas i an Nonsmoker 173 73 E 24 Hispanic Former smoker 170 68 F 45 Caucas i an Nonsmoker 183 93 G 47 Asian Nonsmoker 167 54 H 31 Caucas i an Nonsmoker 191 107 I 31 Hispanic Nonsmoker 165 74 J 37 Caucas i an Nonsmoker 185 95
airway images for the entire nasal passage at contiguous 3 mm intervals. AR was used to measure the nasal cross-sectional areas immediately prior to and following each aerosol deposition measurement.
Subjects
The human experimental procedures were approved by both the Institutional Review Board of The Lovelace Institutes (the review board for the Inhalation Toxicology Research Institute) and The Johns Hopkins University. Prior to experimental procedures, the subjects agreed to participate by signing a consent form which provided details of the experimental procedures. Each subject was given a physical examination by Dr Steven Simpson, a pulmonary physician licensed in the state of New Mexico, to determine fitness for participating in this study. Nine of the 10 subjects were never-smokers; Subject E was a former smoker and had been a nonsmoker for the past three years. The subjects had no preexisting lung disorders, nasal trauma, or upper airway diseases. Among the 10 subjects were seven Caucasians, two Hispanics, and one Asian, although no specific attempt was made to control for ethnicity. The subjects volunteered for the study and were included following the physical examination. Table 1 shows the subjects' characteristics with respect to age, ethnicity, smoking history, body height, and body weight.
Aerosol 9eneration system
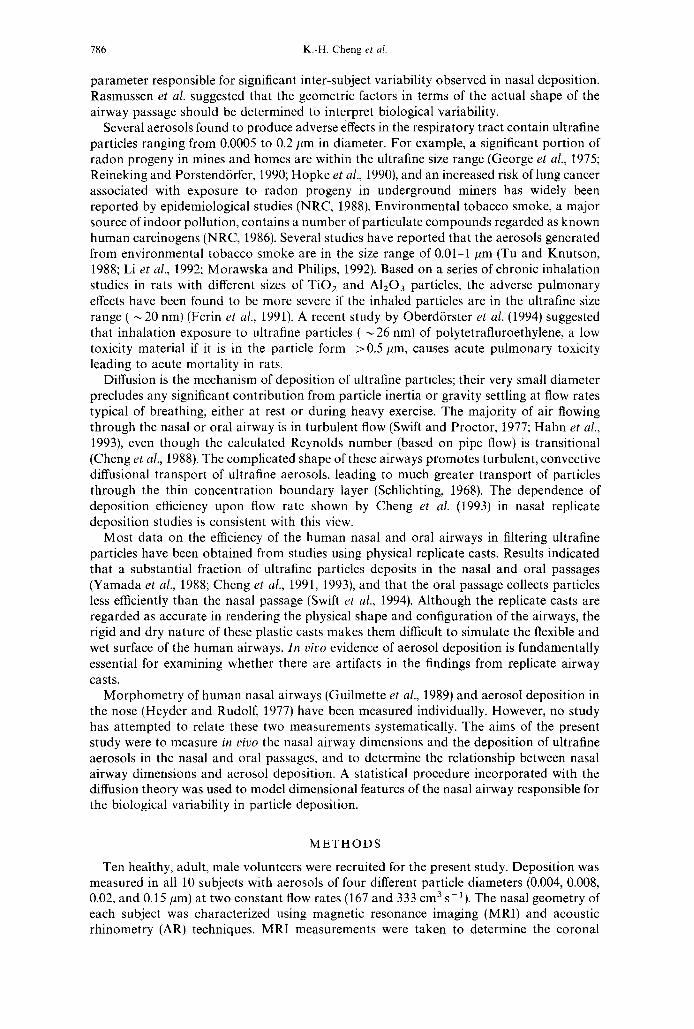
The aerosol exposure system consisted of an aerosol generation section, a particle size classifier, and a concentration measuring instrument (Fig. 1). Silver wool (99.9 + %, Aldrich Chemical Company Inc., Milwaukee, WI) was used to generate aerosol particles ~< 0.02 pm in diameter, and polystyrene latex particles in aqueous suspension (Duke Scientific Corp., Palo Alto, CA) were used for producing 0.15 pm particles. The silver particles, produced by an evaporation-condensation method, or the polystyrene latex particles, aerosolized by a Retec X-70 nebulizer, were passed through an electrostatic classifier (TSI Model 3071, St. Paul, MN) to obtain a monodisperse aerosol (geometric standard deviation < 1.2) of specified diameter. Aerosol particle diameter and geometric standard deviation were measured by a screen-type diffusion battery (TSI Model 3040, St. Paul, MN). This aerosol was then brought to Boltzmann charge equilibrium in a 8SKr discharger and diluted with filtered, humidified air to produce a specified flow rate. Concentrations of aerosols before entering and after exiting the subject's airways were measured by an ultrafine condensation particle counter (TSI Model 3025, St. Paul, MN). Typical entering aerosol concentrations were 200-600 particles cm-3. A model 386/33 personal computer, equipped with Labtech Notebook version 6.1.2. software (Laboratory Technologies Corp., San Francisco, CA) and the Strawberry Tree ACPC-12-16 data acquisition interface card (Strawberry Tree Inc., Sunnyvale, CA), was used to control the system operation and record the experimental data.
788 K.-H. Cheng et al.
I Furnace
H i . . . . I -vacuum
I
Retec Nebulizer V a c u u m ~
V Flow meter I - • i Electric Switch [ ~ ] Two-way Electric Valve [ ~ Three-way Electric Valve
= ~ = Filter UCPC: TS13025 Particle Counter E.C.: TS13071 Electrostatic Classifier S.C.: Sampling Chamber G.C.: Glass Chamber
Fig. I. Schematic diagram of the aerosol exposure system.
Aerosol exposure protocol
The human subject was connected to the aerosol exposure system (containing an aerosol with one of the four particle diameters described above) by a nasal mask (Respironics Inc., Murrysville, PA) and a mouthpiece (Warren E. Collins Inc., Braintree, MA). The aerosol exposure procedures consisted of the following four breathing patterns, each done during a period of breath holding: (1) the aerosol was drawn into the nose and out through the mouth (nose-in/mouth-out), (2) the aerosol was drawn into the mouth and out through the nose (mouth-in/nose-out), (3) nose-in/mouth-out (pattern 1) with an oral extension tube, and (4) mouth-in/nose-out (pattern 2) with an oral extension tube.
The oral extension tube was made from silicon rubber and designed to "bypass" the oral airway by providing a simple elliptical channel through which the aerosol passed rather than through the complex shape of the actual oral airway. The length of the extension tube inserted into the mouth of each subject depended primarily on the individual's distance between the lips and the uvula. The average tube length was 7 cm. The elliptical channel was approximately 0.75 cm wide and 2.0 cm long. Diffusional deposition in this tube was 3% for the smallest particle and lowest flow rate, and less than this for all other combinations of particle size and flow rate.
An external pump was used to draw the aerosols at a constant flow rate through the combined nose-mouth (or mouth-nose) airway path while the subject held his breath for 30M5 s. A complete deposition measurement consisted of a 30-s sampling from the pre- exposure port (upstream of the airway entrance) followed by a 30-s sampling from the post-exposure port (after the aerosol had passed through the subject's airways). The dead volume of the exposure system was small enough for steady state to be achieved in 5 s. For each breathing pattern, deposition was measured with aerosols of four particle sizes, each at two constant flow rates. This resulted in 32 total combinations of breathing patterns, particle sizes, and flow rates for each subject. Each aerosol deposition was measured in quadruplicate.
Because the aerosol was sampled upstream of the nasal mask for pre-exposure and downstream of the mouthpiece for post-exposure, correction was necessary to account for
In vivo nasal and oral deposition 789
particle losses in the artificial region other than the subject's airways. Using the same length of rubber tubing connected with a nasal mask containing an external nose model and a mouthpiece (with/without an oral extension tube), penetration fractions of the aerosol were determined for the same combinations of particle size, flow rate, and flow pattern as described above. These values were denoted as correction factors (Ci) to represent particle deposition in the transport lines, nasal mask, mouthpiece, and sampling ports. The C~'s were measured for each combination of particle size and flow rate and ranged from 6 to 30%. When the subjects were exposed to test aerosols, the measured particle penetration, P~, was the result of deposition in the airways and the aerosol transport system. Thus, the net deposition efficiency in the subject's airways was calculated as 1 - (PJC~), where i stands for each combination of experimental conditions.
Magnetic resonance imaging
Approximately one year prior to the aerosol exposure, MRI nasal images of each subject were taken at the New Mexico VA Medical Center (Albuquerque, NM) using a Siemens Magnatom 1.5 T proton imaging unit (Siemens Med. Systems, Islin, N J). A sagittal scan was performed to obtain reference positions of the nasal airway from the external nares to the nasopharynx. Coronal images were then obtained for the entire nasal passage at contiguous 3 mm intervals. Transparency films of these images were produced according to the imaging data collected on a VAX computer that was integral to the imager. Using transmitted light, images of the transparency films for each airway section were projected onto an acetate transparency sheet. The mucosa-airway interface was then traced by hand using a G R A F / P E N sonic digitizer (SAC, Southport, CT). The digitized data were collected and analyzed using SmartCAM DXF 2-D Data Translator and Advanced 3D-Machining softwares (Point Control Co., Eugene, OR) on a 486/66 personal computer. The cross- sectional areas and the perimeters were calculated based on the digitized data.
It was determined by physical examination and questionnaire that no nasal trauma or disease occurred between the time of the MRI measurement and the time of the deposition measurement. The subjects did not have seasonal allergies which might have altered the nasal geometry. However, as the MRI measurement was made at a specific time, small changes in nasal geometry related to the nasal cycle and diurnal variation in nasal passage perfusion could not be controlled. For this reason, acoustic rhinometry measurements were performed just prior to each deposition measurement in order to characterize the nasal state during measurement.
Acoustic rhinometry
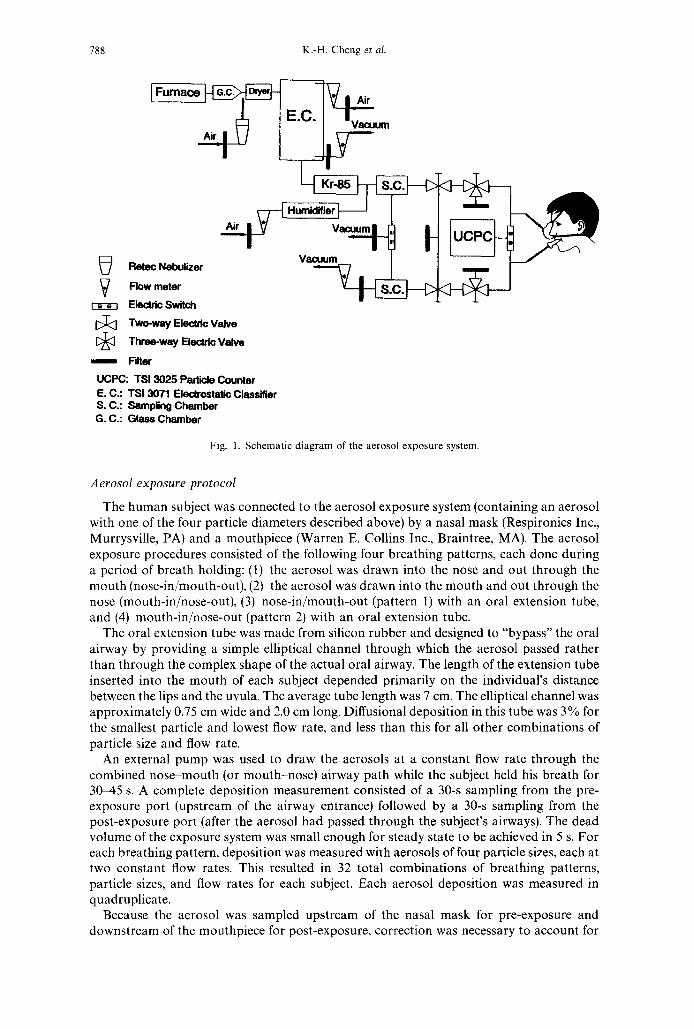
Acoustic rhinometry was used to measure in vivo the cross-sectional area of the nasal passage as a function of distance from the nostril based on changes in nasal impedance between incident and reflected acoustic signals (Hilberg et al., 1989). Figure 2 shows the experimental setup of the acoustic rhinometry system. The apparatus included a computer with an analog-to-digital expansion board (Model DAS-16, Keithley Instruments Inc., Taunton, MA) for data acquisition and processing; a spark generator for producing the sound pulse of short duration; an omnidirectional 64-dB microphone (Digi-Key Corp., Thief River Falls, MN) for detecting the sound pulse; a 20-dB amplifier; and a 10-kHz low-pass filter. A sound pulse, generated by the spark generator, traveled through a wave tube (1.5 cm ID, 60 cm long) and entered the human nose via a brass nosepiece (7.5 cm long). Different diameters of the nosepiece were used to fit various sizes of the nostril opening. By analyzing the time and amplitude of reflected sound, the cross-sectional area versus the distance from the nostril could be determined at a resolution of 0.35 cm.
Data analysis
As discussed above, studies of flow dynamics and aerosol deposition in human replicate nasal casts support the view that turbulent, convective diffusion is the dominant mechanism
790 K.-H. Cheng et al.
Nosepiece
l ~ =phL~:plifier ~--"~
\ Spark Generator
Low Pass Filter I
A/D Converter 0 0 0 ~
lllllllll ~ - - ~
Fig. 2. Schematic diagram of the acoustic rhinometry system.
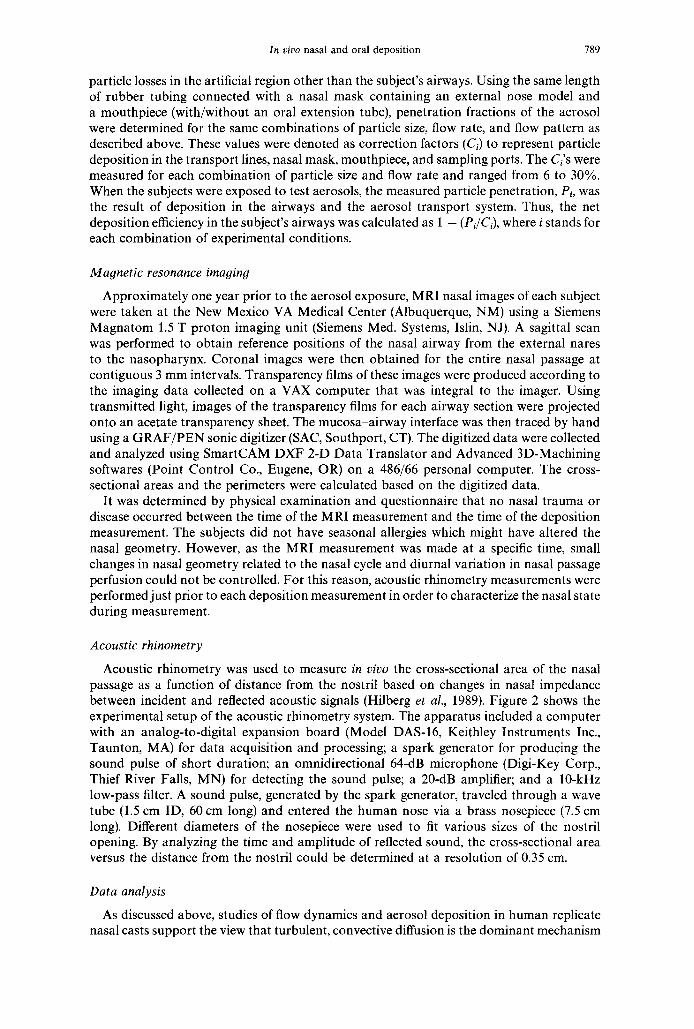
of ultrafine aerosol deposition. The turbulent diffusion theory in pipe flows (Schlichting, 1968) was extended to model the extrathoracic deposition of ultrafine aerosols as an exponential function of airway geometry, particle size, and flow rate:
P e n e = exp[-K(A~i~)"( 'f)b(D)C(Q)dl, (1)
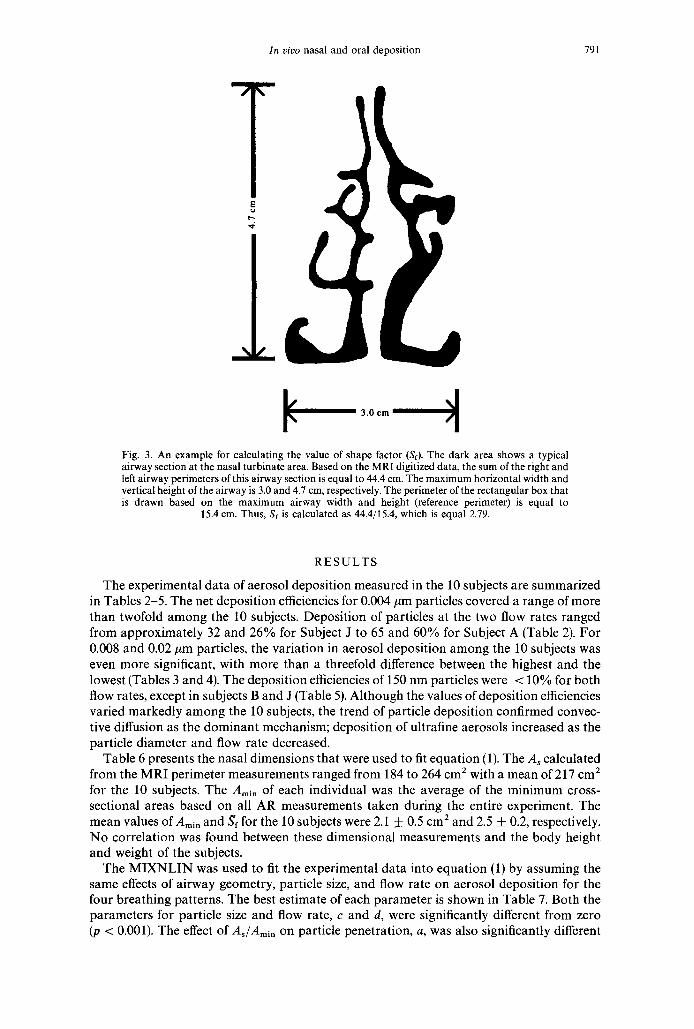
where Pene is the aerosol penetration fraction, K is a constant, A~ is the total surface area of the nasal passage from the anterior nostrils to the nasopharynx in cm 2, Ami, is the nasal minimum cross-sectional area in cm 2, D is the diffusion coefficient of the particles in cm 2 s- 1, Q is the volumetric flow rate in cm 3 s- 1, and Sf is the average airway shape factor of the nasal turbinate region, gf is defined as the ratio of the airway perimeter to a reference perimeter calculated from the periphery of the rectangle drawn on the maximum horizontal and vertical boundaries of each 3 mm bilateral airway section (see Fig. 3). A large airway perimeter could be attributed to a big airway size or to convoluted airway cross section. After the airway perimeter was divided by the reference perimeter (proportional to the airway size), the resulting Sf should represent the airway shape complexity. Calculation of Sf for a typical airway section is shown in Fig. 3.
The form of equation (1) is similar to that previously used (e.g. Swift et al., 1994) for studies in replicate airways except that it contains airway geometry parameters As, Amin,
and Sf. Without these parameters, the empirical equation was obtained by plotting depos- ition (1- penetration) versus a diffusion parameter, DXQ -r. When the airway geometry parameters are included, deposition is plotted versus the parameter shown in equation (1), and this parameter is noted as the geometry-related diffusion parameter, (AJAmin)a(sf)b(D)C(Q) a. Statistical analysis of the experimental data is used to obtain the numerical values of a, b, c, and d.
Because each subject was repeatedly measured for aerosol deposition during the 32 combinations of experimental conditions, the mixed-effects nonlinear regression procedure (MIXNLIN) (Vonesh, 1992) was used to account for the random effect of repeated measures on estimating the parameters a d in equation (1). The MIXNLIN computes estimated generalized least square, iteratively reweighed generalized least square, maximum likeli- hood, or restricted maximum likelihood estimates of the parameters of a generalized mixed-effects nonlinear regression model. A detailed description of applying the turbulent diffusion theory and the MIXNLIN for data analysis could be found in a companion article (Cheng et al., 1995b).
In vivo nasal and oral deposition 791
.-.3 ¢. ,
3.0 cm
Fig. 3. An example for calculating the value of shape factor (S0. The dark area shows a typical airway section at the nasal turbinate area. Based on the MRI digitized data, the sum of the right and left airway perimeters of this airway section is equal to 44.4 cm. The maximum horizontal width and vertical height of the airway is 3.0 and 4.7 cm, respectively. The perimeter of the rectangular box that is drawn based on the maximum airway width and height (reference perimeter) is equal to
15.4 cm. Thus, Sf is calculated as 44.4/15.4, which is equal 2.79.
RESULTS
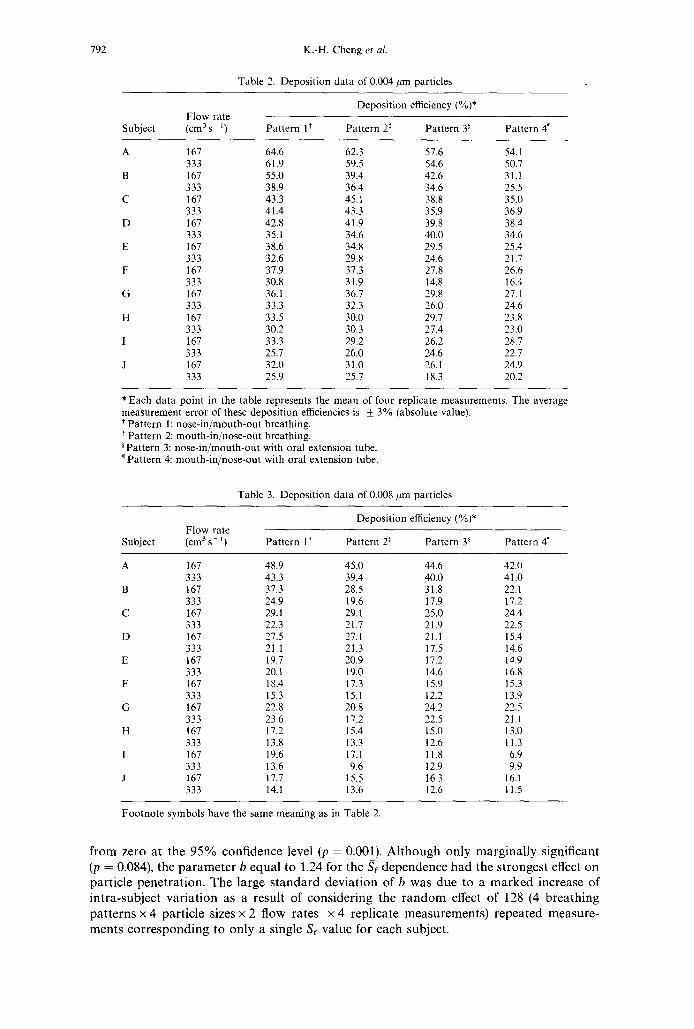
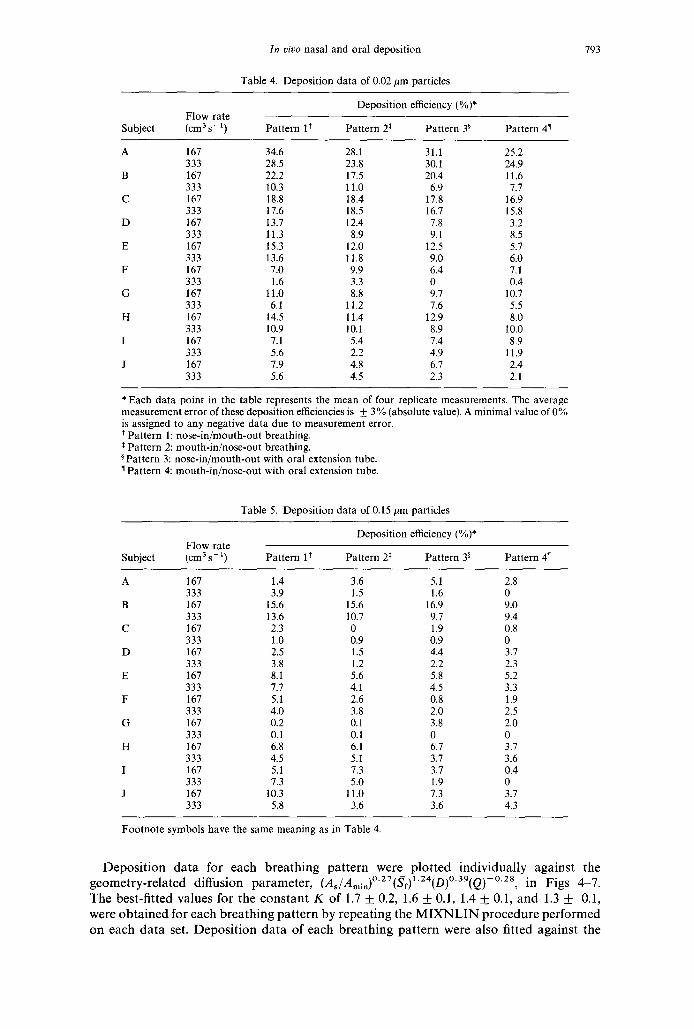
The experimental data of aerosol deposition measured in the 10 subjects are summarized in Tables 2-5. The net deposition efficiencies for 0.004 #m particles covered a range of more than twofold among the 10 subjects. Deposition of particles at the two flow rates ranged from approximately 32 and 26% for Subject J to 65 and 60% for Subject A (Table 2). For 0.008 and 0.02/~m particles, the variation in aerosol deposition among the 10 subjects was even more significant, with more than a threefold difference between the highest and the lowest (Tables 3 and 4). The deposition efficiencies of 150 nm particles were < 10% for both flow rates, except in subjects B and J (Table 5). Although the values of deposition efficiencies varied markedly among the 10 subjects, the trend of particle deposition confirmed convec- tive diffusion as the dominant mechanism; deposition of ultrafine aerosols increased as the particle diameter and flow rate decreased.
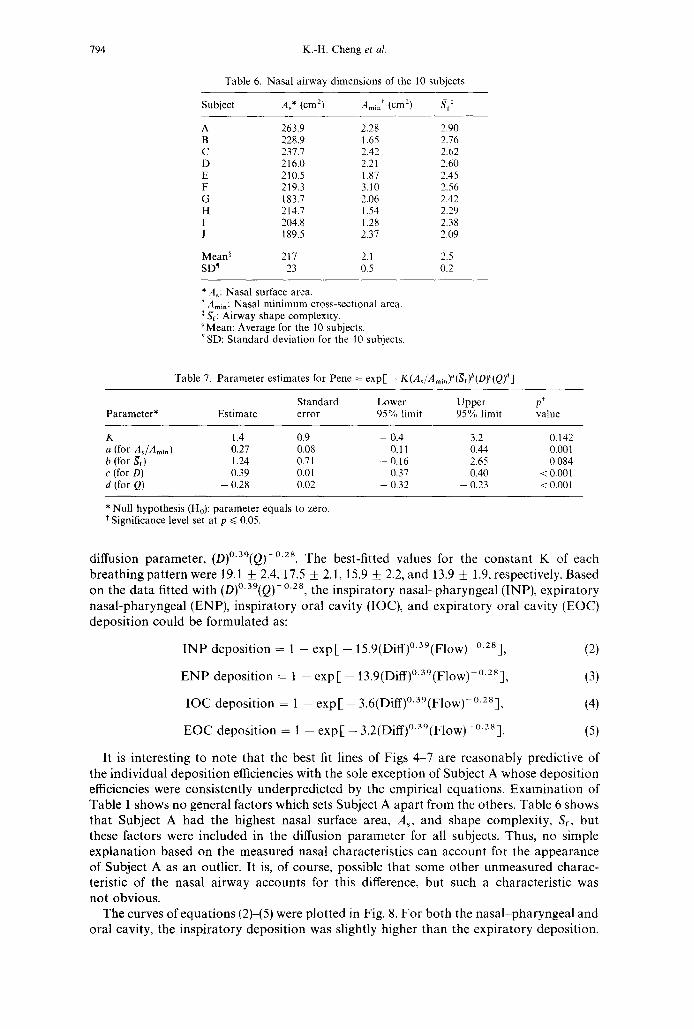
Table 6 presents the nasal dimensions that were used to fit equation (1). The As calculated from the MRI perimeter measurements ranged from 184 to 264 cm 2 with a mean of 217 cm 1 for the 10 subjects. The Amin of each individual was the average of the minimum cross- sectional areas based on all AR measurements taken during the entire experiment. The mean values of Amin and Sf for the 10 subjects were 2.1 _+ 0.5 cm 2 and 2.5 _+ 0.2, respectively. No correlation was found between these dimensional measurements and the body height and weight of the subjects.
The MIXNLIN was used to fit the experimental data into equation (1) by assuming the same effects of airway geometry, particle size, and flow rate on aerosol deposition for the four breathing patterns. The best estimate of each parameter is shown in Table 7. Both the parameters for particle size and flow rate, e and d, were significantly different from zero (p < 0.001). The effect of As/Amin on particle penetration, a, was also significantly different
792 K.-H. Cheng et al.
Table 2. Deposition data of 0.004/~m particles
Deposition efficiency (%)* Flow rate
Subject (cm3s ~) Pattern l* Pattern 2 ~ Pattern 3 ~ Pattern 4"
A 167 64.6 62.3 57.6 54.1 333 61.9 59.5 54.6 50.7
B 167 55.0 39.4 42.6 31 .! 333 38.9 36.4 34.6 25.5
C 167 43.3 45.1 38.8 35.0 333 41.4 43.3 35.9 36.9
D 167 42.8 41.9 39.8 38.4 333 35.1 34.6 40.0 34.6
E 167 38.6 34.8 29.5 25.4 333 32.6 29.8 24.6 21.7
F 167 37.9 37,3 27.8 26.6 333 30.8 31,9 14.8 16.4
G 167 36.1 36.7 29.8 27.1 333 33.3 32.3 26.0 24.6
H 167 33.5 30.0 29.7 23.8 333 30.2 30.3 27.4 23.0
I 167 33.3 29.2 26.2 28.7 333 25.7 26.0 24.6 22.7
J 167 32.0 31.0 26.1 24.9 333 25.9 25.7 18.3 20.2
* Each data point in the table represents the mean of four replicate measurements. The average measurement error of these deposition efficiencies is _+ 3% (absolute value). * Pattern 1: nose-in/mouth-out breathing.
Pattern 2: mouth-in/nose-out breathing. Pattern 3: nose-in/mouth-out with oral extension tube. Pattern 4: mouth-in/nose-out with oral extension tube.
Table 3. Deposition data of 0.008 ~tm particles
Deposition efficiency (%)* Flow rate
Subject (cm 3 s- 1) Pattern 1 * Pattern 2 * Pattern 3 ~ Pattern 4"
A 167 48.9 45.0 44.6 42.0 333 43.3 39.4 40.0 41.0
B 167 37.3 28.5 31.8 22.1 333 24.9 19.6 17.9 17.2
C 167 29.1 29.1 25.0 24.4 333 22.3 21.7 21.9 22.5
D 167 27.5 27.1 21.1 15.4 333 21.1 21.3 17.5 14.6
E 167 19.7 20.9 17.2 14.9 333 20.1 19.0 14.6 16.8
F 167 18.4 17.3 15.9 15.3 333 15.3 15.1 12.2 13.9
G 167 22.8 20.8 24.2 22.5 333 23.6 17.2 22.5 21.1
H 167 17.2 15.4 15.0 13.0 333 13.8 13.3 12.6 l 1.3
1 167 19.6 17.1 11.8 6.9 333 13.6 9.6 12.9 9.9
J 167 17.7 15.5 16.3 16.1 333 14.1 13.6 12.6 11.5
Footnote symbols have the same meaning as in Table 2.
f r o m ze ro a t t he 9 5 % c o n f i d e n c e level (p = 0.001). A l t h o u g h on ly m a r g i n a l l y s ign i f ican t
(p = 0.084), the p a r a m e t e r b e q u a l to 1.24 for the Sf d e p e n d e n c e h a d the s t r o n g e s t effect on
pa r t i c l e p e n e t r a t i o n . T h e l a rge s t a n d a r d d e v i a t i o n of b w a s d u e to a m a r k e d inc rease of
i n t r a - s u b j e c t v a r i a t i o n as a resu l t o f c o n s i d e r i n g the r a n d o m effect o f 128 (4 b r e a t h i n g
p a t t e r n s x 4 pa r t i c l e sizes x 2 f low ra tes x 4 r ep l i ca t e m e a s u r e m e n t s ) r e p e a t e d m e a s u r e -
m e n t s c o r r e s p o n d i n g to on ly a s ingle Sf va lue for e a c h subjec t .
In vivo nasal and oral deposition
Table 4. Deposition data of 0.02 pm particles
793
Deposition efficiency (%)* Flow rate
Subject (cm 3 s- 1) Pattern 1' Pattern 2 * Pattern 38 Pattern 47
A 167 34.6 28.1 31.1 25.2 333 28.5 23.8 30.1 24.9
B 167 22.2 17.5 20.4 11.6 333 10.3 11.0 6.9 7.7
C 167 18.8 18.4 17.8 16.9 333 17.6 18.5 16.7 15.8
D 167 13.7 12.4 7.8 3.2 333 11.3 8.9 9.1 8.5
E 167 15.3 12.0 12.5 5.7 333 13.6 11.8 9.0 6.0
F 167 7.0 9.9 6.4 7.1 333 1.6 3.3 0 0.4
G 167 1t.0 8.8 9.7 10.7 333 6.1 11.2 7.6 5.5
H 167 14.5 11.4 12.9 8.0 333 10.9 10.1 8.9 10.0
I 167 7.1 5.4 7.4 8.9 333 5.6 2.2 4.9 11.9
J 167 7.9 4.8 6.7 2.4 333 5.6 4.5 2.3 2.1
* Each data point in the table represents the mean of four replicate measurements. The average measurement error of these deposition efficiencies is + 3% (absolute value). A minimal value of 0% is assigned to any negative data due to measurement error. * Pattern 1: nose-in/mouth-out breathing.
Pattern 2: mouth-in/nose-out breathing. Pattern 3: nose-in/mouth-out with oral extension tube. Pattern 4: mouth-in/nose-out with oral extension tube.
Table 5. Deposition data of 0.15 #m particles
Deposition efficiency (%)* Flow rate
Subject (cm 3 s- 1) Pattern 1 * Pattern 2* Pattern 38 Pattern 4 ~
A 167 1.4 3.6 5.1 2.8 333 3.9 1.5 1.6 0
B 167 15.6 15.6 16.9 9.0 333 13.6 10.7 9.7 9.4
C 167 2.3 0 1.9 0.8 333 1.0 0.9 0.9 0
D 167 2.5 1.5 4.4 3.7 333 3.8 1.2 2.2 2.3
E 167 8.1 5.6 5.8 5.2 333 7.7 4.1 4.5 3.3
F 167 5.1 2.6 0.8 1.9 333 4.0 3.8 2.0 2.5
G 167 0.2 0.1 3.8 2.0 333 0.1 0.1 0 0
H 167 6.8 6.1 6.7 3.7 333 4.5 5.1 3.7 3.6
I 167 5.1 7.3 3.7 0.4 333 7.3 5.0 1.9 0
J 167 10.3 11.0 7.3 3.7 333 5.8 3.6 3.6 4.3
Footnote symbols have the same meaning as in Table 4.
D e p o s i t i o n d a t a for e a c h b r e a t h i n g p a t t e r n w e r e p l o t t e d i n d i v i d u a l l y a g a i n s t the 0 27 1 24 0 39 0 28
g e o m e t r y - r e l a t e d d i f fus ion p a r a m e t e r , (As/Amin)" (Sf)" (D)" ( Q ) - , in F igs 4 -7 .
T h e be s t - f i t t ed va lues fo r t he c o n s t a n t K o f 1.7 _+ 0.2, 1.6 _+ 0.1, 1.4 -4- 0.1, a n d 1.3 _+ 0.1,
w e r e o b t a i n e d for e a c h b r e a t h i n g p a t t e r n by r e p e a t i n g the M I X N L I N p r o c e d u r e p e r f o r m e d
o n e a c h d a t a set. D e p o s i t i o n d a t a o f e a c h b r e a t h i n g p a t t e r n w e r e a l so f i t ted a g a i n s t t he
794 K.-H. Cheng et al.
Table 6. Nasal airway dimensions of the 10 subjects
Subject As* (cm 2) Amin¢ (cm2) "~t*
A 263.9 2.28 2.90 B 228.9 1.65 2.76 C 237.7 2.42 2.62 D 216.0 2.21 2.60 E 210.5 1.87 2.45 F 219.3 3.10 2.56 G 183.7 2.06 2.42 H 214.7 1.54 2.29 1 204.8 1.28 2.38 J 189.5 2.37 2.09
Mean ~ 217 2.1 2.5 SD ~ 23 0.5 0.2
* A~: Nasal surface area. ¢Ami.: Nasal minimum cross-sectional area.
:gf: Airway shape complexity. Mean: Average for the 10 subjects.
• SD: Standard deviation for the 10 subjects.
Table 7. Parameter estimates for Pene = e x p [ - K(As/Ami,)"(Se)b(D)C(Q) a]
Standard Lower Upper p* Parameter* Estimate error 95% limit 95% limit value
K 1.4 0.9 - 0.4 3.2 0.142 a (for A~/A,,in) 0.27 0.08 0.11 0.44 0.001 b (for St) 1.24 0.71 - 0.16 2.65 0.084 c (for D) 0.39 0.01 0.37 0.40 < 0.001 d (for Q) - 0.28 0.02 - 0.32 - 0.23 < 0.001
* Null hypothesis (Ho): parameter equals to zero. t Significance level set at p ~< 0.05.
d i f fus ion pa rame te r , (D)°'39(Q) -°'28. The best- f i t ted va lues for the c o n s t a n t K of each b r e a t h i n g p a t t e r n were 19.1 + 2.4, 17.5 + 2.1, 15.9 + 2.2, a n d 13.9 + 1.9, respectively. Based o n the d a t a fit ted wi th (D) ° '39(Q)- 0.28, the i n s p i r a t o r y n a s a l - p h a r y n g e a l ( INP) , exp i r a to ry
n a s a l - p h a r y n g e a l (ENP) , i n s p i r a t o r y ora l cavi ty (IOC), a n d exp i r a to ry ora l cavi ty (EOC) d e p o s i t i o n cou l d be f o r m u l a t e d as:
I N P d e p o s i t i o n = 1 - exp [ - 15.9(Diff)° '39(Flow) o.28], (2)
E N P d e p o s i t i o n -- 1 - e x p [ - 1 3 . 9 ( D i f f ) ° 3 9 ( F l o w ) - ° ' 2 s ] , (3)
I O C d e p o s i t i o n = 1 - e x p [ - 3 . 6 ( D i f f ) ° ' a g ( F l o w ) - ° z s ] , (4)
E O C d e p o s i t i o n = 1 - e x p [ - 3 .2 (Di f f ) °39(F low) - 0.28]. (5)
I t is i n t e res t ing to n o t e tha t the best fit l ines of Figs 4 - 7 are r e a s o n a b l y predic t ive of the i n d i v i d u a l d e p o s i t i o n efficiencies wi th the sole excep t ion of Subjec t A whose depos i t i on efficiencies were cons i s t en t ly u n d e r p r e d i c t e d by the empi r i ca l equa t ions . E x a m i n a t i o n of T a b l e 1 shows n o genera l factors which sets Subjec t A a p a r t f rom the others. T a b l e 6 shows tha t Sub jec t A h ad the h ighes t nasa l surface area, As, a n d shape complexi ty , Sf, bu t these factors were i n c l u d e d in the di f fus ion p a r a m e t e r for all subjects. Thus , no s imple e x p l a n a t i o n based o n the m e a s u r e d nasa l charac ter i s t ics can a c c o u n t for the a p p e a r a n c e of Subjec t A as a n outl ier . It is, of course , poss ib le tha t some o the r u n m e a s u r e d charac - terist ic of the nasa l a i rway a c c o u n t s for this difference, bu t such a charac te r i s t ic was n o t obv ious .
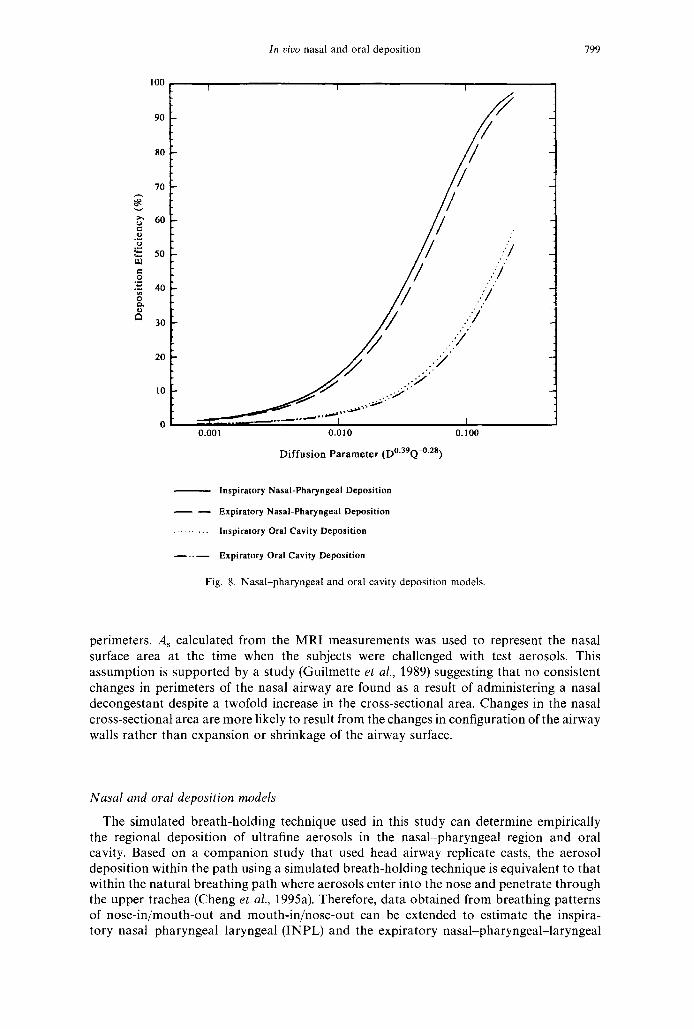
The curves of e q u a t i o n s (2)-(5) were p lo t t ed in Fig. 8. F o r b o t h the n a s a l - p h a r y n g e a l a n d ora l cavi ty, the i n s p i r a t o r y d e p o s i t i o n was sl ightly h igher t h a n the exp i r a to ry depos i t ion .
1 0 0
In vivo nasal and oral deposition
[
795
e~ o
o
o o
90
80
70
60
50
40
30
20
10
0
0.01
0 0
o°/ o j . o []
O A
v 0 V
i ° o . . . . o , , , , ,
0.10
(AJAmin)0-27Sf 1-24D°-39Q-°'28
O Subject A [] Subject C 0 Subject E ~7 Subject G /~ Subject I
~7 Subject B A Subject D O Subject F r:'l Subject H ~ Subject J
1 0 0 [1--exp(-l.73 (As/Amin)0"27(Sf)l'24(D)0"39(Q) -0"28]
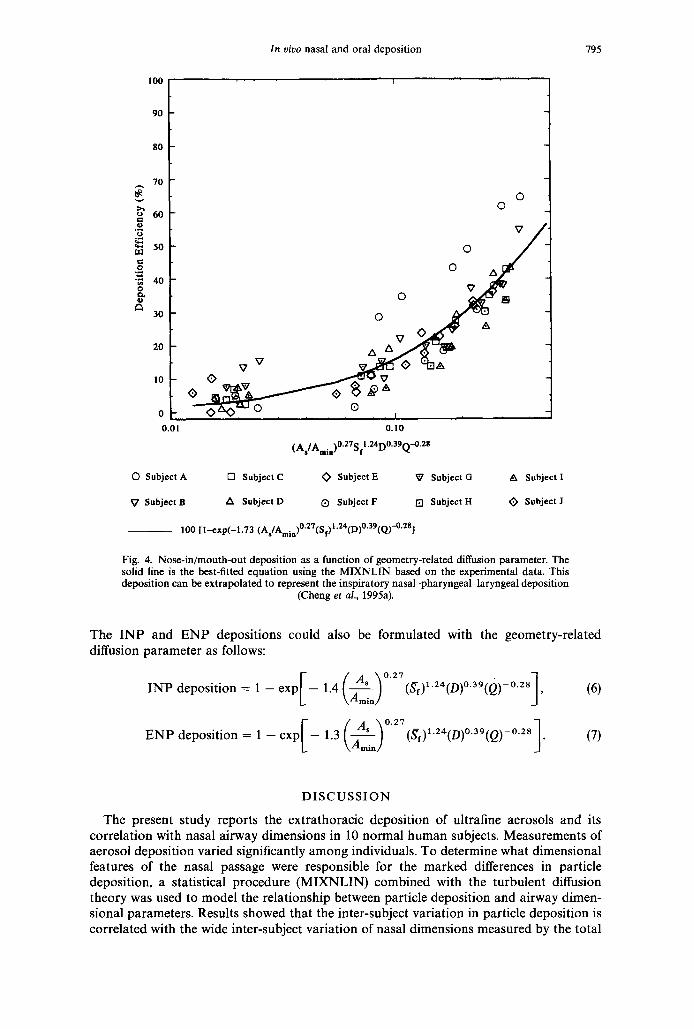
Fig. 4. Nose-in/mouth-out deposition as a function of geometry-related diffusion parameter. The solid line is the best-fitted equation using the MIXNL1N based on the experimental data. This deposition can be extrapolated to represent the inspiratory nasal-pharyngeal-laryngeal deposition
(Cheng et al., 1995a).
The INP and E N P depositions could also be formulated with the geometry-related diffusion parameter as follows:
deposition = 1 - e x p l - INP 1.4
ENP deposition = 1 - e x p [ - 1.3 k
(~f)l.24(D)O.39(~ (A~i~) °'27 i ) - ° '28] , (6)
D I S C U S S I O N
The present study reports the extrathoracic deposition of ultrafine aerosols and its correlation with nasal airway dimensions in 10 normal human subjects. Measurements of aerosol deposition varied significantly among individuals. To determine what dimensional features of the nasal passage were responsible for the marked differences in particle deposition, a statistical procedure (MIXNLIN) combined with the turbulent diffusion theory was used to model the relationship between particle deposition and airway dimen- sional parameters. Results showed that the inter-subject variation in particle deposition is correlated with the wide inter-subject variation of nasal dimensions measured by the total
796 K.-H. Cheng et al.
100 ' !
90
80
70
60 e ~
5o
0
"~n 40 0
c~ 30
20
10
0
0.01
O ©
°oj o o ° ° ~ A ~ v
v v ~ ~..~ ~ , ~ ~ ~ , ~ I ~ , 0.10
(As/Amin)°-27Sf 1.24D0.39Q-0-28
O Subject A Q Subject C O Subject E ~7 Subject G A Subject I
~7 Subject B A Subject D O Subject F [] Subject H ~ Subject J
100 l l-exp(-1.57 (As/Amin)0'27(Sf)I'24(D)0"39(Q)-0"281
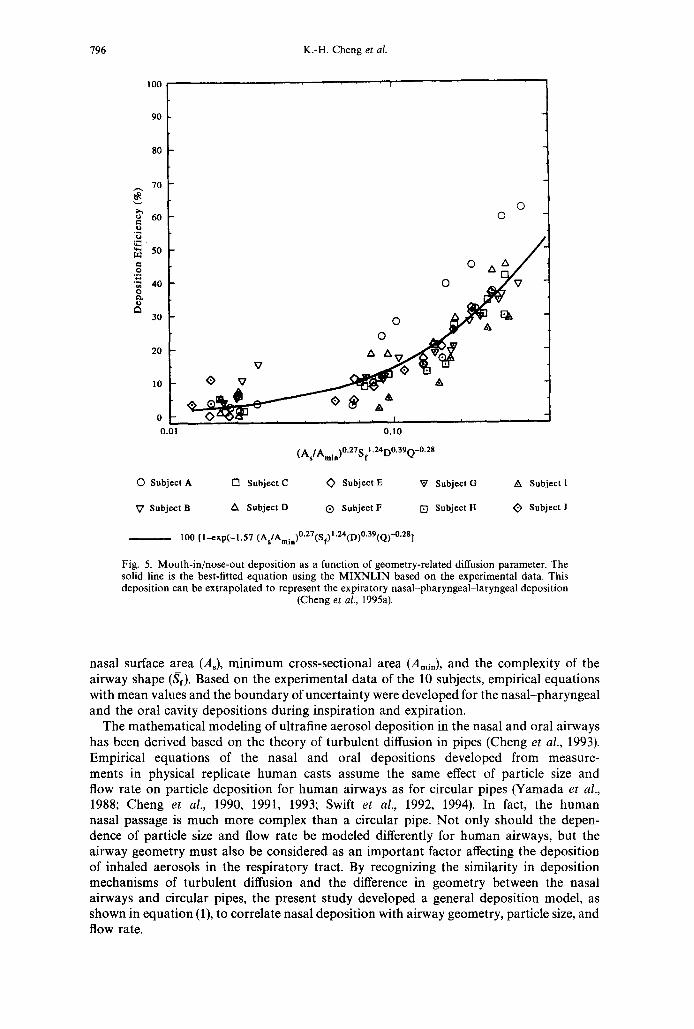
Fig. 5. Mouth- in /nose-ou t deposit ion as a function of geometry-related diffusion parameter. The solid line is the best-fitted equat ion using the M I X N L I N based on the experimental data. This deposit ion can be extrapolated to represent the expiratory nasa l -pharyngeal - la ryngeal deposit ion
(Cheng et al., 1995a).
nasal surface area (As), minimum cross-sectional a r e a (Amin) , and the complexity of the airway shape (Sf). Based on the experimental data of the 10 subjects, empirical equations with mean values and the boundary of uncertainty were developed for the nasal-pharyngeal and the oral cavity depositions during inspiration and expiration.
The mathematical modeling of ultrafine aerosol deposition in the nasal and oral airways has been derived based on the theory of turbulent diffusion in pipes (Cheng et al., 1993). Empirical equations of the nasal and oral depositions developed from measure- ments in physical replicate human casts assume the same effect of particle size and flow rate on particle deposition for human airways as for circular pipes (Yamada et al., 1988; Cheng et al., 1990, 1991, 1993; Swift et al., 1992, 1994). In fact, the human nasal passage is much more complex than a circular pipe. Not only should the depen- dence of particle size and flow rate be modeled differently for human airways, but the airway geometry must also be considered as an important factor affecting the deposition of inhaled aerosols in the respiratory tract. By recognizing the similarity in deposition mechanisms of turbulent diffusion and the difference in geometry between the nasal airways and circular pipes, the present study developed a general deposition model, as shown in equation (1), to correlate nasal deposition with airway geometry, particle size, and flow rate.
1 0 0
In vivo nasal and oral deposition
. . . . . i
797
o
o
~3
90
80
70
60
50
40
30
20
10
0 0.01
o o
oO [~ ~ ] /
o 0 v . ~ v . / 0 z x ~ e " -
L o - , 0.10
(AslAmia)°.27Sf 1-24D0-39Q-0'28
(3 Subject A I'3 Subject C O Subject E ~7 Subject G A Subject I
~7 Subject B A Subject D O Subject F [] Subject H ~ Subject J
1 0 0 [1-exp(-1.42 (As/Amin)0"27(sf)l'24(D)0"39(Q) -0"28]
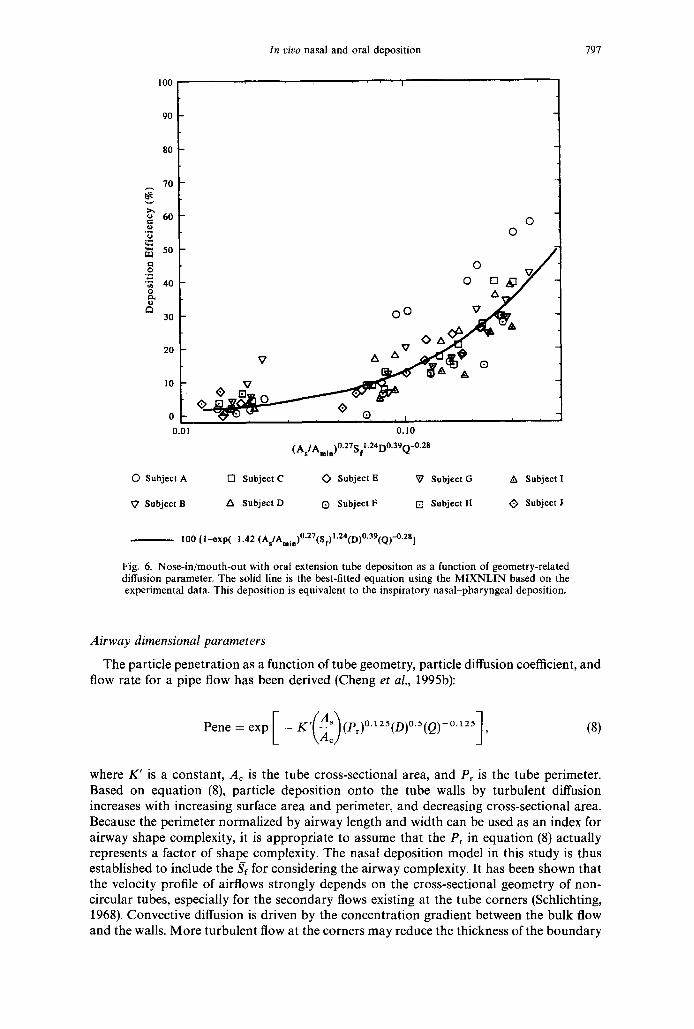
Fig. 6. Nose-in/mouth-out with oral extension tube deposition as a function of geometry-related diffusion parameter. The solid line is the best-fitted equation using the MIXNLIN based on the experimental data. This deposition is equivalent to the inspiratory nasal-pharyngeal deposition.
Airway dimensional parameters
The particle penetration as a function of tube geometry, particle diffusion coefficient, and flow rate for a pipe flow has been derived (Cheng et al., 1995b):
Pene = exp [ - K'(-~)(Pr)°'~25(D)°'S(Q)-°"25], (8)
where K' is a constant, Ac is the tube cross-sectional area, and Pr is the tube perimeter. Based on equation (8), particle deposition onto the tube walls by turbulent diffusion increases with increasing surface area and perimeter, and decreasing cross-sectional area. Because the perimeter normalized by airway length and width can be used as an index for airway shape complexity, it is appropriate to assume that the Pr in equation (8) actually represents a factor of shape complexity. The nasal deposition model in this study is thus established to include the Sf for considering the airway complexity. It has been shown that the velocity profile of airflows strongly depends on the cross-sectional geometry of non- circular tubes, especially for the secondary flows existing at the tube corners (Schlichting, 1968). Convective diffusion is driven by the concentration gradient between the bulk flow and the walls. More turbulent flow at the corners may reduce the thickness of the boundary
798 K.-H. Cheng et al.
1 0 0
.M o
e~ o
o
90
80
70
60
50
40
30
20
10
0
0.0!
© 0
Z~ []
o o o~ 0 A
zx ~ o
v v
0.10
( A / A )°27S I '24D°39Q-°'28 s rain f
O Subject A [] Subject C O Subject E ~7 Subject G
~7 Subject B A Subject D Q Subject F [] Subject H
100 [ I -exp(-1 .26 (As/Amin)O'27(sf)l'24(D)O'39(Q) -028]
A Subject I
<) Subject J
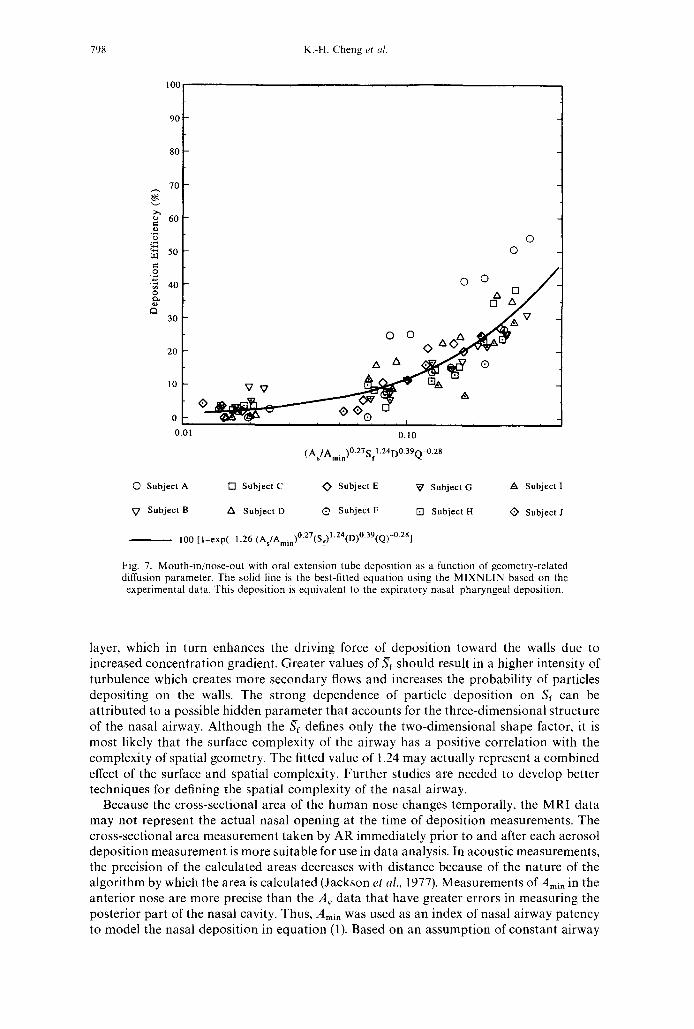
Fig. 7. Mouth-in/nose-out with oral extension tube deposition as a function of geometry-related diffusion parameter. The solid line is the best-fined equation using the MIXNLIN based on the experimental data. This deposition is equivalent to the expiratory nasal pharyngeal deposition.
layer, which in turn enhances the driving force of deposition toward the walls due to increased concentration gradient. Greater values of Sf should result in a higher intensity of turbulence which creates more secondary flows and increases the probability of particles depositing on the walls. The strong dependence of particle deposition on Sf can be attributed to a possible hidden parameter that accounts for the three-dimensional structure of the nasal airway. Although the St defines only the two-dimensional shape factor, it is most likely that the surface complexity of the airway has a positive correlation with the complexity of spatial geometry. The fitted value of 1.24 may actually represent a combined effect of the surface and spatial complexity. Further studies are needed to develop better techniques for defining the spatial complexity of the nasal airway.
Because the cross-sectional area of the human nose changes temporally, the MRI data may not represent the actual nasal opening at the time of deposition measurements. The cross-sectional area measurement taken by AR immediately prior to and after each aerosol deposition measurement is more suitable for use in data analysis. In acoustic measurements, the precision of the calculated areas decreases with distance because of the nature of the algorithm by which the area is calculated (Jackson et al., 1977). Measurements of Amin in the anterior nose are more precise than the A c data that have greater errors in measuring the posterior part of the nasal cavity. Thus, A m i n w a s used as an index of nasal airway patency to model the nasal deposition in equation (1). Based on an assumption of constant airway
In vivo nasal and oral deposition 799
100
90
80
7O
v
;~ 60
.2 50
m c - o
;~ 40
e ~
30
20
10
I I [
/ /
7 7
'1' 5 7 //
//' ..::/ /// ....../
/ / ..:J /71 . < : 7
. . '~"
0.001 0.010 O.10O
Dif fus ion Parameter (D°39Q m'28)
Inspiratory Nasal-Pharyngeal Deposition
- - Expiratory Nasal-Pharyngeal Deposition
. . . . . . . . . . Inspiratory Oral Cavity Deposition
Expiratory Oral Cavity Deposition
Fig. 8. Nasal-pharyngeal and oral cavity deposition models.
perimeters, As calculated from the MRI measurements was used to represent the nasal surface area at the time when the subjects were challenged with test aerosols. This assumption is supported by a study (Guilmette et al., 1989) suggesting that no consistent changes in perimeters of the nasal airway are found as a result of administering a nasal decongestant despite a twofold increase in the cross-sectional area. Changes in the nasal cross-sectional area are more likely to result from the changes in configuration of the airway walls rather than expansion or shrinkage of the airway surface.
Nasal and oral deposition models
The simulated breath-holding technique used in this study can determine empirically the regional deposition of ultrafine aerosols in the nasal-pharyngeal region and oral cavity. Based on a companion study that used head airway replicate casts, the aerosol deposition within the path using a simulated breath-holding technique is equivalent to that within the natural breathing path where aerosols enter into the nose and penetrate through the upper trachea (Cheng et al., 1995a). Therefore, data obtained from breathing patterns of nose-in/mouth-out and mouth-in/nose-out can be extended to estimate the inspira- tory nasal pharyngeal laryngeal (INPL) and the expiratory nasal-pharyngeal-laryngeal

800 K.-H. Cheng et al.
(ENPL) deposition:
I N P L deposition = 1 - e x p l - 1.7( A~ ~0.27 \ A mi n J (St) 124(D}°3° (Q) - ° 2 8 J (9)
= 1 - exp[ - 19.1(D)°30(Q) - °28 ]
[ / A \ ° 2 ~ ] E N P L deposition = 1 - exp 1.6 [ **s / (Sf)l.24.(D)O.39(Q) 0.28
\AminJ (10)
= 1 -- exp[ -- 17.5(D)°3O(Q) 0.28]
Based on the measurements of nasal dimensions in the 10 subjects, the reference values of As, Amin, and Jgr used in equations (9) and (10) are 217 cm 2, 2.1 cm 2, and 2.5 cm 2,
respectively.
C O N C L U S I O N S
This is the first study that correlates measurements of aerosol deposition with detailed and better definitions of nasal dimensions in a reasonable number of human subjects. Greater surface area, smaller cross-sectional area, and increasing complexity of airway shape are found to be associated with higher deposition of ultrafine aerosols in the extrathoracic airways. Because the nasal and oral airways are the first portal of entry for airborne particles, both extremely high and low efficiencies of the extrathoracic filtration have significant health implication for the lungs as well as the extrathoracic region. The signifi- cance of the present study is not only in the development of in vivo dosimetric models for the average population, but also in the recognition, based on the experimental data, that assessing the health effects on a population basis would not be complete without consider- ing the wide range of biological variability. It is necessary to include the information of biological variability in the extrathoracic filtration to define the population-wide lung dosimetry resulting from aerosol intakes.
Acknowledgements The authors thank Rick D. Brodbeck and Thomas D. Holmes for their technical assistance in establishing the aerosol exposure system, Christopher P. Vigil for assisting with the MRI measurements, Douglas J. Taylor and Keith E. Muller for providing the MIXNLIN software package, and Paula L. Bradley for editing the manuscript. This research was supported by the Office of Health and Environmental Research of the U.S. Department of Energy under Contract Numbers DE-FG02-88ER60655 at the Johns Hopkins University and DE-AC04-76EV01013 at the Inhalation Toxicology Research Institute.
R E F E R E N C E S
Cheng, K. H., Cheng, Y. S., Yeh, H. C. and Swift, D. L. (1995a) Deposition of ultrafine aerosols in the head airways during natural breathing and during simulated breath holding using replicate human upper airway casts. Aerosol Sci. Technol. 23, 465 474.
Cheng, K. H., Swift, D. L., Yang, Y. H., Cheng, Y. S. and Yeh, H. C. (1995b) Application of both a physical theory and statistical procedure in the analyses of an in vivo study of aerosol deposition. Proc. 1995 Int. Coi l on Aerosol Science and Technolo,qy, Taipei, Taiwan, pp. 231 236.
Cheng, Y. S., Su, Y. F., Yeh, H. C. and Swift, D. L. (1993) Deposition of thoron progeny in human head airways. Aerosol Sci. Technol. 18, 359 375.
Cheng, Y. S., Yamada, Y., Yeh, H.C. and Swift, D. L. ( t 988) Diffusional deposition of ultrafine aerosols in a human nasal cast. J. Aerosol Sci. 6, 741 751.
Cheng, Y. S., Yamada, Y., Yeh, H. C. and Swift, D. L. (1990) Deposition of ultrafine aerosols in a human oral cast. Aerosol Sci. Technol. 12, 1075 1081.
Cheng, Y. S., Yeh, H. C. and Swift, D. L. (1991) Aerosol deposition in human nasal airway for particles 1 nm to 20/~m: a model study. In Radiation Protection Dosimetry (Edited by Guilmette, R. A. and Boecker, B. B.). Nuclear Technology Publishing, England.
Ferin, J., Oberd6rster, G., Soderholm, S. C. and Gelein, R. {1991) Pulmonary tissue access of ultrafine particles. J. Aerosol Med. 4, 57 68.
Fry, F. A. and Black, A. (1973) Regional deposition and clearance of particles in the human nose. J. Aerosol Sci. 4, 113 124.
George, A. C., Hinchliffe, L. and Sladowski, R. (1975) Size distribution of radon daughter particles in uranium mine atmospheres. Am. Ind. Hy,q. Assoc. J. 36, 484 490.

In vivo nasal and oral deposition 801
Guilmette, R. A., Wicks, J. D. and Wolff, R. K. (1989) Morphometry of human nasal airways in vivo using magnetic resonance imaging. J. Aerosol Med. 2, 365-377.
Hahn, I., Scherer, P. W. and Mozell, M. M. (1993) Velocity profiles measured for airflow through a large-scale model of the human nasal cavity. J. Appl. Physiol. 75, 2273 2287.
Heyder, J. and Rudolf, G. (1977) Deposition of aerosol particles in the human nose. In Inhaled Particles I V (Edited by Walton, W. H.), pp.107 126. Pergamon Press, Oxford.
Hilberg, O., Jackson, A. C., Swift, D. L. and Pedersen, O. F. (1989) Acoustic rhinometry: evaluation of nasal cavity geometry by acoustic reflection. J. Appl. Physiol. 66, 295 303.
Hopke, P. K., Ramamurthi, M. and Li, C. S. (1990) Measurements of the size distributions of radon progeny in indoor air. Proc. 29th Hanford Symposium on Health and the Environment, Richland, WA, p. 113.
Hounam, R. F., Black, A. and Walsh, M. (1971) The deposition of aerosol particles in the nasopharyngeal region of the human respiratory tract. J. Aerosol Sci. 2, 24~61.
Jackson, A. C., Butler, J. P., Millet, E. J. and Hoppin Jr, F. G. (1977) Airway geometry by analysis of acoustic pulse response measurements. J. Appl. Physiol. 43, 523 536.
Li, C.-S., Jeng, F.-T. and Lin, W.-H. (1992) Field characterization of submicron aerosols from indoor combustion sources. J. Aerosol Sci. (Suppl. 1) 23, $547 $550.
Morawska, L. and Phillips, C. R. (1992) Attachment of radon progeny to cigarette smoke aerosol. Aerosol Sci. Technol. 17, 149 158.
National Research Council (NRC) (1986) Environmental tobacco smoke: measuring exposures and assessing health effects. National Academy Science, Washington, DC.
National Research Council (NRC) (1988) Health risks of radon and other internally deposited alpha-emitters- BEIR IV. Committee on the Biological Effects of Ionizing Radiations, National Academy Press, Washington, DC.
Oberd6rster, G., Gelein, R., Ferin, J. and Weiss, B. (1994) Association of particulate air pollution and acute mortality: involvement of ultrafine particles? Proceedings of the Colloquium on Particulate Air Pollution and Human Mortality and Morbidity, pp. 478-499. Irvine, CA.
Rasmussen, T. R., Swift, D. L., Hilberg, O. and Pedersen, O. F. (1990) Influence of nasal passage geometry on aerosol particle deposition in the nose. J. Aerosol Med. 3, 15-25.
Reineking, A. and Porstend6rfer, J. (1990) Unattached fractions of short lived Rn decay products in indoor and outdoor environment: an improved single screen method and results. Hlth. Phys. 58, 715-728.
Schlichting, H. (1968) Boundary-layer Theory (Translated by Kestin, J.). McGraw Hill, Stanford. Swift, D. L., Cheng, Y. S., Su, Y. F. and Yeh, H. C. (1994) Ultrafine aerosol deposition in the human nasal and oral
passages. In Inhaled Particles VII (Edited by Dodgson, J. and McCallum, R. I.), Ann. Occup. Hyg. 38, 77 81. Swift, D. L., Montassier, N., Hopke, P. K., Karpen-Hayes, K., Cheng, Y. S., Su, Y. F., Yeh, H. C. and Strong, J.
(1992) Inspiratory deposition of ultrafine particles in human nasal replicate cast. J. Aerosol Sci. 23, 65 72. Swift, D. L. and Proctor, D. F. (1977) Access of air to the respiratory tract. In Respiratory Defense Mechanisms
(Edited by Brain, J., Proctor, D. and Reid, L.), p. 63. Marcel Dekker, New York. Tu, K. W. and Knutson, E. O. (1988) Indoor outdoor aerosol measurements for two residential buildings in
New Jersey. Aerosol Sci. Technol. 9, 71-82. Vonesh, E. F. (1992) MIXNLIN: a SAS procedure for nonlinear mixed-effects models. Technical Report Number
TR92M-0300, Applied Statistics Center, Baxter Healthcare Corporation, Round Lake, IL. Yamada, Y., Cheng, Y. S., Yeh, H. C. and Swift, D. L. (1988) Inspiratory and expiratory deposition of ultrafine
particles in a human nasal cast. lnhal. Toxicol. 1, 1-11.
Related Documents











