in the clinic in the clinic Hypothyroidism Screening page ITC6-2 Diagnosis page ITC6-4 Treatment page ITC6-6 Practice Improvement page ITC6-13 CME Questions page ITC6-16 Section Editor Christine Laine, MD, MPH Sankey Williams, MD Barbara Turner, MD Physician Writer Michael T. McDermott MD The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), including PIER (Physicians’ Information and Education Resource) and MKSAP (Medical Knowledge and Self-Assessment Program). Annals of Internal Medicine editors develop In the Clinic from these primary sources in collaboration with the ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIER and MKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org and other resources referenced in each issue of In the Clinic. CME Objective: To provide information on the screening, diagnosis, and treatment of hypothyroidism. The information contained herein should never be used as a substitute for clinical judgment. © 2009 American College of Physicians

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
inthe
clinicin the clinic
HypothyroidismScreening page ITC6-2
Diagnosis page ITC6-4
Treatment page ITC6-6
Practice Improvement page ITC6-13
CME Questions page ITC6-16
Section EditorChristine Laine, MD, MPHSankey Williams, MDBarbara Turner, MD
Physician WriterMichael T. McDermott MD
The content of In the Clinic is drawn from the clinical information and education resources of the American College of Physicians (ACP), includingPIER (Physicians’ Information and Education Resource) and MKSAP (MedicalKnowledge and Self-Assessment Program). Annals of Internal Medicineeditors develop In the Clinic from these primary sources in collaboration withthe ACP’s Medical Education and Publishing Division and with the assistance of science writers and physician writers. Editorial consultants from PIER andMKSAP provide expert review of the content. Readers who are interested in these primary resources for more detail can consult http://pier.acponline.org and otherresources referenced in each issue of In the Clinic.
CME Objective: To provide information on the screening, diagnosis, and treatmentof hypothyroidism.
The information contained herein should never be used as a substitute for clinicaljudgment.
© 2009 American College of Physicians

Which patients are at elevatedrisk for hypothyroidism?Patients at increased risk for hypo-thyroidism are those who have 1 ormore symptoms of thyroid hormonedeficiency; a goiter; history of thyroiddisease or treatment for a thyroidcondition; personal history of otherautoimmune diseases, particularlytype 1 diabetes mellitus, adrenal in-sufficiency, or vitiligo; family historyof thyroid disease; high-dose headand neck radiation therapy; use ofmedications, such as lithium, α-interferon, and amiodarone; pituitarysurgery; pituitary radiation therapy;or advanced age.
Should clinicians screen nonpreg-nant patients for hypothyroidism?Aggressive case finding is recom-mended for all patients who are atincreased risk for hypothyroidism.Screening the rest of the populationis controversial, with different or-ganizations making different rec-ommendations (4–9). The U.S.Preventive Services Task Force
(6, 7) and a separate multidiscipli-nary expert panel (8) concludedthat evidence is insufficient to rec-ommend for or against populationscreening. Screening for hypothy-roidism has been more strongly ad-vocated by other groups (9).
A computer model–based cost–utilityanalysis estimated that screening for hy-pothyroidism is as cost-effective as mam-mography and other generally recom-mended screening procedures (4).
Should clinicians screen pregnantwomen for hypothyroidism?Screening as part of a prepregnancyor early pregnancy evaluation re-mains controversial. An expertpanel concluded that evidence isinsufficient to recommend for oragainst routine TSH testing butdid recommend TSH testing inwomen with symptoms of thyroiddysfunction, personal or familyhistory of thyroid disease, an ab-normal thyroid gland on palpation,or type 1 diabetes mellitus or other
© 2009 American College of Physicians ITC6-2 In the Clinic Annals of Internal Medicine 1 December 2009
1. Tunbridge WM,Evered DC, Hall R, etal. The spectrum ofthyroid disease in acommunity: theWhickham survey.Clin Endocrinol (Oxf ).1977;7:481-93.[PMID: 598014]
2. Canaris GJ, ManowitzNR, Mayor G, et al.The Colorado thyroiddisease prevalencestudy. Arch InternMed. 2000;160:526-34. [PMID: 10695693]
3. Hollowell JG,Staehling NW, Flan-ders WD, et al. SerumTSH, T4, and thyroidantibodies in theUnited States popula-tion (1988 to 1994):National Health andNutrition Examina-tion Survey (NHANESIII). J Clin EndocrinolMetab. 2002;87:489-99. [PMID: 11836274]
4. Danese MD, Powe NR,Sawin CT, et al.Screening for mildthyroid failure at theperiodic health ex-amination: a decisionand cost-effective-ness analysis. JAMA.1996;276:285-92.[PMID: 8656540]
5. Singer PA, Cooper DS,Levy EG, et al. Treat-ment guidelines forpatients with hyper-thyroidism and hy-pothyroidism. Stan-dards of CareCommittee, Ameri-can Thyroid Associa-tion. JAMA.1995;273:808-12.[PMID: 7532241]
6. Screening for thyroiddisease: recommen-dation statement.Ann Intern Med.2004;140:125-7.[PMID: 14734336]
7. Helfand M. Screeningfor subclinical thyroiddysfunction in non-pregnant adults: asummary of the evi-dence for the U.S.Preventive ServicesTask Force. Ann In-tern Med.2004;140:128-41.[PMID: 14734337][Full Text]
8. Surks MI, Ortiz E,Daniels GH, et al.Subclinical thyroiddisease: scientific re-view and guidelinesfor diagnosis andmanagement. JAMA.2004;291:228-38.[PMID: 14722150]
Hypothyroidism is a condition in which the thyroid gland cannot makeenough thyroid hormone to meet the requirements of peripheral tis-sues. It is the most common functional disorder of the thyroid gland.
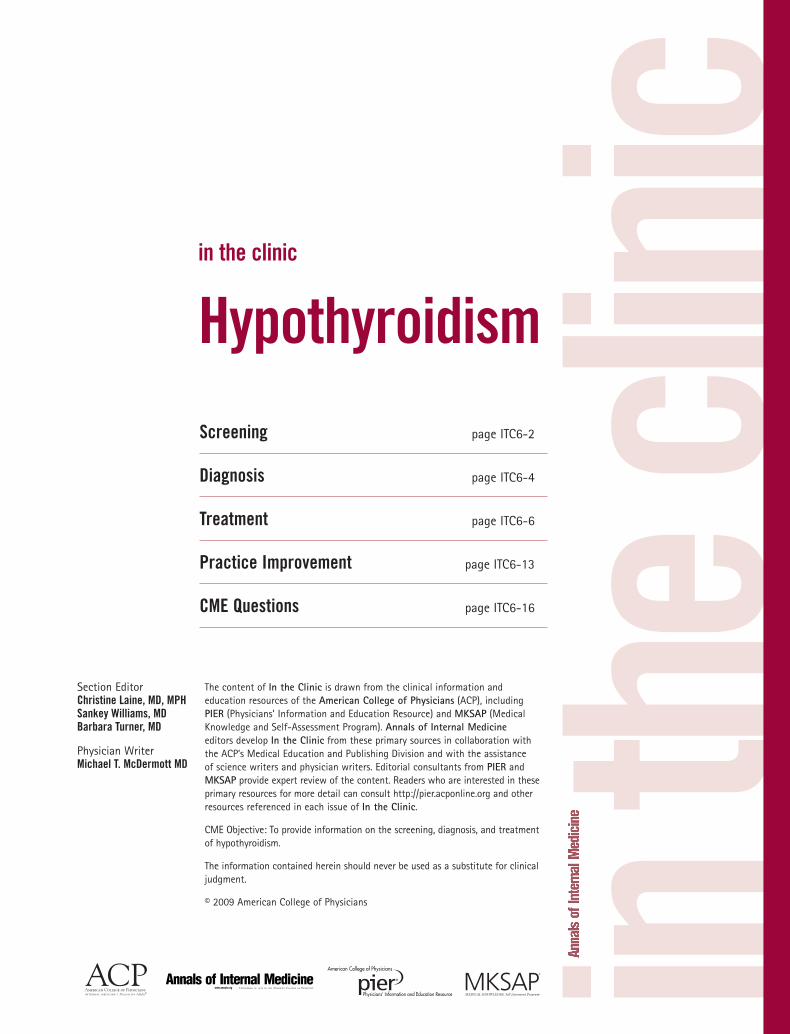
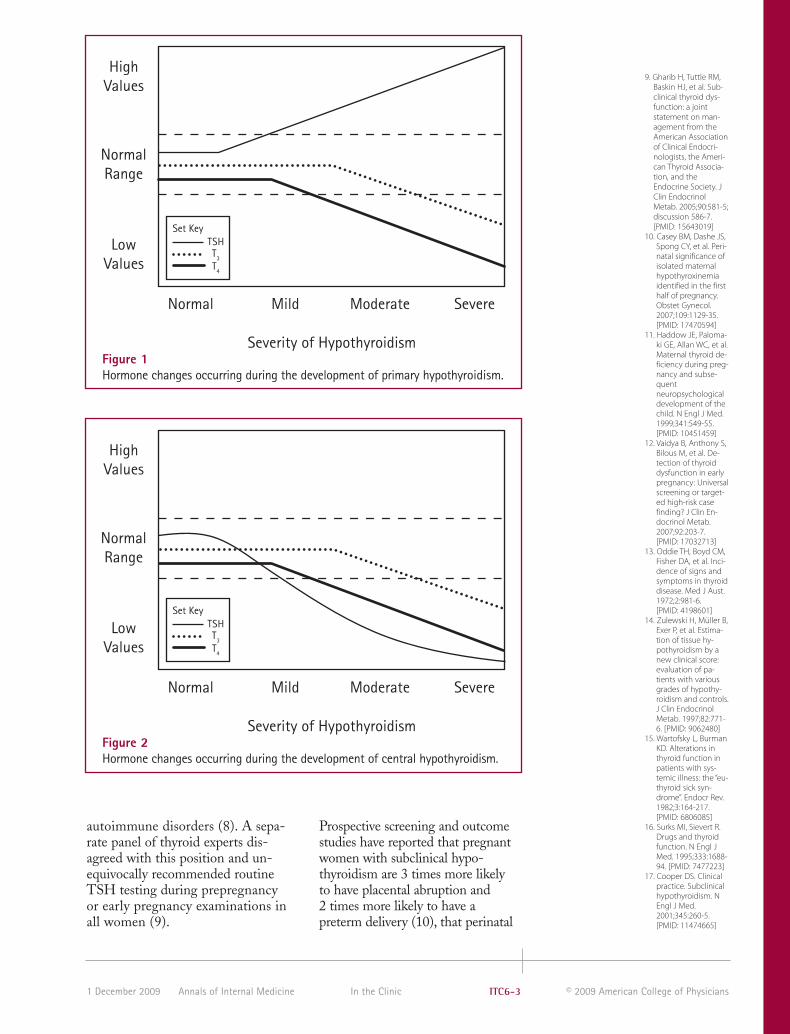
Primary hypothyroidism occurs when thyroid failure results from disease of thethyroid gland itself and it accounts for more than 99% of all cases of hypothy-roidism (Figure 1). The most common causes of primary hypothyroidism inadults are chronic lymphocytic thyroiditis (Hashimoto disease); radioiodine thy-roid ablation; thyroidectomy; high-dose head and neck radiation therapy; andmedications, such as lithium, α-interferon, and amiodarone. Central hypothy-roidism occurs when thyroid failure results from pituitary or hypothalamic dis-orders that cause insufficient production of thyroid-stimulating hormone (TSH)by the pituitary gland (Figure 2). The most common causes of central hypothy-roidism in adults are tumors, inflammatory conditions, infiltrative diseases, in-fections, pituitary surgery, pituitary radiation therapy, and head trauma.
Primary hypothyroidism is overt when the serum TSH level is high and theserum total thyroxine (T4) or free T
4level is less than the population refer-
ence range. Subclinical hypothyroidism is a milder degree of thyroid failurecharacterized by mildly to moderately increased levels of serum TSH butwith total T
4and free T
4values still within the population range. The preva-
lence of overt hypothyroidism is approximately 1% to 2% in women and0.1% in men (1, 2), whereas subclinical hypothyroidism has been identifiedin 4% to 10% of different population groups (1, 2) and in up to 18% of elder-ly persons (1–3). Progression from subclinical to overt hypothyroidism occursin 5% to 18% of persons with subclinical hypothyroidism per year.
Screening
© 2009 American College of PhysiciansITC6-3In the ClinicAnnals of Internal Medicine1 December 2009
autoimmune disorders (8). A sepa-rate panel of thyroid experts dis-agreed with this position and un-equivocally recommended routineTSH testing during prepregnancyor early pregnancy examinations inall women (9).
Prospective screening and outcomestudies have reported that pregnantwomen with subclinical hypo -thyroidism are 3 times more likely to have placental abruption and 2 times more likely to have apreterm delivery (10), that perinatal
9. Gharib H, Tuttle RM,Baskin HJ, et al. Sub-clinical thyroid dys-function: a jointstatement on man-agement from theAmerican Associationof Clinical Endocri-nologists, the Ameri-can Thyroid Associa-tion, and theEndocrine Society. JClin EndocrinolMetab. 2005;90:581-5;discussion 586-7.[PMID: 15643019]
10. Casey BM, Dashe JS,Spong CY, et al. Peri-natal significance ofisolated maternalhypothyroxinemiaidentified in the firsthalf of pregnancy.Obstet Gynecol.2007;109:1129-35.[PMID: 17470594]
11. Haddow JE, Paloma-ki GE, Allan WC, et al.Maternal thyroid de-ficiency during preg-nancy and subse-quentneuropsychologicaldevelopment of thechild. N Engl J Med.1999;341:549-55.[PMID: 10451459]
12. Vaidya B, Anthony S,Bilous M, et al. De-tection of thyroiddysfunction in earlypregnancy: Universalscreening or target-ed high-risk casefinding? J Clin En-docrinol Metab.2007;92:203-7.[PMID: 17032713]
13. Oddie TH, Boyd CM,Fisher DA, et al. Inci-dence of signs andsymptoms in thyroiddisease. Med J Aust.1972;2:981-6.[PMID: 4198601]
14. Zulewski H, Müller B,Exer P, et al. Estima-tion of tissue hy-pothyroidism by anew clinical score:evaluation of pa-tients with variousgrades of hypothy-roidism and controls.J Clin EndocrinolMetab. 1997;82:771-6. [PMID: 9062480]
15. Wartofsky L, BurmanKD. Alterations inthyroid function inpatients with sys-temic illness: the “eu-thyroid sick syn-drome”. Endocr Rev.1982;3:164-217.[PMID: 6806085]
16. Surks MI, Sievert R.Drugs and thyroidfunction. N Engl JMed. 1995;333:1688-94. [PMID: 7477223]
17. Cooper DS. Clinicalpractice. Subclinicalhypothyroidism. NEngl J Med.2001;345:260-5.[PMID: 11474665]
HighValues
NormalRange
LowValues
Normal Mild Moderate Severe
Severity of Hypothyroidism
TSHT3
T4
Set Key
Figure 1Hormone changes occurring during the development of primary hypothyroidism.
HighValues
NormalRange
LowValues
Normal Mild Moderate Severe
Severity of Hypothyroidism
TSHT3
T4
Set Key
Figure 2Hormone changes occurring during the development of central hypothyroidism.

18. McDermott MT,Ridgway EC. Subclin-ical hypothyroidismis mild thyroid failureand should be treat-ed. J Clin EndocrinolMetab.2001;86:4585-90.[PMID: 11600507]
19. Meier C, Staub JJ,Roth CB, et al. TSH-controlled L-thyrox-ine therapy reducescholesterol levelsand clinical symp-toms in subclinicalhypothyroidism: adouble blind, place-bo-controlled trial(Basel ThyroidStudy). J Clin En-docrinol Metab.2001;86:4860-6.[PMID: 11600554]
20. Cooper DS, HalpernR, Wood LC, et al. L-Thyroxine therapy insubclinical hypothy-roidism. A double-blind, placebo-con-trolled trial. AnnIntern Med.1984;101:18-24.[PMID: 6428290]
21. Nyström E, CaidahlK, Fager G, et al. Adouble-blind cross-over 12-monthstudy of L-thyroxinetreatment of womenwith ‘subclinical’ hy-pothyroidism. ClinEndocrinol (Oxf ).1988;29:63-75.[PMID: 3073880]
22. Staub JJ, Althaus BU,Engler H, et al. Spec-trum of subclinicaland overt hypothy-roidism: effect onthyrotropin, pro-lactin, and thyroidreserve, and meta-bolic impact on pe-ripheral target tis-sues. Am J Med.1992;92:631-42.[PMID: 1605145]
23. Monzani F, Del Guer-ra P, Caraccio N, et al.Subclinical hypothy-roidism: neurobe-havioral features andbeneficial effect of L-thyroxine treatment.Clin Investig.1993;71:367-71.[PMID: 8508006]
24. Carani C, Isidori AM,Granata A, et al. Mul-ticenter study on theprevalence of sexualsymptoms in malehypo- and hyperthy-roid patients. J ClinEndocrinol Metab.2005;90:6472-9.[PMID: 16204360]
25. Samuels MH, SchuffKG, Carlson NE, et al.Health status, mood,and cognition in ex-perimentally in-duced subclinicalhypothyroidism. JClin EndocrinolMetab.2007;92:2545-51.[PMID: 17473069]
© 2009 American College of Physicians ITC6-4 In the Clinic Annals of Internal Medicine 1 December 2009
intraventricular hemorrhage and res-piratory distress syndrome occurmore often in infants of women withsubclinical hypothyroidism (10), andthat children born to mothers whohad untreated or inadequately treat-ed hypothyroidism during pregnancyhave lower IQ scores than do chil-dren whose mothers were euthyroidduring pregnancy (11). A prospectivecohort study determined that screen-ing only high-risk patients would
miss 30% of pregnant women withhypothyroidism (12).
If clinicians screen forhypothyroidism, which test should they use?The serum TSH level is the screen-ing test of choice for hypothyroidismbecause more than 99% of hypothy-roidism cases are primary hypothy-roidism and an elevated serum TSHlevel is the first laboratory abnormal-ity to occur in this condition (5, 6).
Screening... Population screening for thyroid dysfunction is controversial, but aggressive case-finding is appropriate in patients at increased risk for hypo-thyroidism, such as those who have symptoms of thyroid hormone deficiency; a goiter;history of previous thyroid disease or treatment for a thyroid condition; personal history of other autoimmune diseases, particularly type 1 diabetes mellitus, adrenalinsufficiency, or vitiligo; or family history of thyroid disease. Screening should also beconsidered for all women who are planning a pregnancy or who are pregnant. SerumTSH level is the best screening test for primary hypothyroidism.
CLINICAL BOTTOM LINE
DiagnosisWhat laboratory tests shouldclinicians use to diagnosehypothyroidism?Measurement of the serum TSH lev-el is the best test to diagnose primaryhypothyroidism (Table 1) (5). If theTSH level is high, further measure-ment of the serum free T4 should bedone. A low serum free T
4in con-
junction with an elevated serumTSH level establishes a diagnosis ofovert hypothyroidism. If a patient issuspected of having central hypothy-roidism, measurement of free T
4is
the test of choice, because TSH levelcannot be accurately interpreted inthis situation. When central hy-pothyroidism is identified, magneticresonance imaging or computed to-mography of the pituitary gland andhypothalamus should be ordered.
What other conditions shouldclinicians consider in patients whopresent with possiblehypothyroidism?In addition to the causes of hypothy-roidism (Table 2), the serum TSHlevel may be mildly elevated during
What symptoms should promptclinicians to consider hypothyroid-ism as a possible diagnosis?The most common symptoms ofhypothyroidism are fatigue, weak-ness, lethargy, weight gain, im-paired memory, impaired learning,cold intolerance, dry skin, constipa-tion, paresthesias, hoarseness,sleepiness, hair loss, sexual dysfunc-tion, menstrual irregularity, and depression (13, 14).
What physical examination andlaboratory findings indicatepossible hypothyroidism?Physical findings most commonlyseen in hypothyroidism include hypertension, bradycardia, goiter,periorbital puffiness, dry skin,coarse skin, cold skin, thinning ofthe lateral eyebrows, and delayedrelaxation phase of the deep tendonreflexes (13, 14). Routine laborato-ry abnormalities that may suggesthypothyroidism include macrocyticanemia, hyponatremia, hypercho-lesterolemia, and elevated level ofserum creatine kinase.

26. Biondi B, Cooper DS.The clinical signifi-cance of subclinicalthyroid dysfunction.Endocr Rev 2008;29:76-131.
27. Danese MD, Laden-son PW, Meinert CL,et al. Clinical review115: effect of thyrox-ine therapy onserum lipoproteinsin patients with mildthyroid failure: aquantitative reviewof the literature. JClin EndocrinolMetab.2000;85:2993-3001.[PMID: 10999775]
28. Caraccio N, Ferranni-ni E, Monzani F.Lipoprotein profilein subclinical hy-pothyroidism: re-sponse to levothy-roxine replacement,a randomized place-bo-controlled study.J Clin endocrinolMetab.2002;87:1533-8.[PMID: 11932277]
29. Ito M, Takamatsu J,Sasaki I, et al. Dis-turbed metabolismof remnant lipopro-teins in patients withsubclinical hypothy-roidism. Am J Med.2004;117:696-9.[PMID: 15501208]
30. Roos A, Bakker SJ,Links TP, et al. Thy-roid function is asso-ciated with compo-nents of themetabolic syndromein euthyroid sub-jects. J Clin En-docrinol Metab.2007;92:491-6.[PMID: 17090642]
31. Kahaly GJ. Cardio-vascular and athero-genic aspects ofsubclinical hypothy-roidism. Thyroid.2000;10:665-79.[PMID: 11014311]
32. Monzani F, Di BelloV, Caraccio N, et al.Effect of levothyrox-ine on cardiac func-tion and structure insubclinical hypothy-roidism: a doubleblind, placebo-con-trolled study. J ClinEndocrinol Metab.2001;86:1110-5.[PMID: 11238494]
33. Vitale G, Galderisi M,Pupoli GA, et al. Leftventricular myocar-dial impairment insubclinical hypothy-roidism assessed bya new ultrasoundtool: pulsed tissueDoppler. J Clin En-docrinol Metab.2002;87:4350-5.[PMID: 12213897]
© 2009 American College of PhysiciansITC6-5In the ClinicAnnals of Internal Medicine1 December 2009
the recovery phase of a variety ofnonthyroidal illnesses (15). If a patient with a mildly elevated serumTSH level has recently had such anillness, the TSH level should berechecked in 6 to 8 weeks. Also,TSH levels may be elevated in therecovery phase of DeQuervain orsilent thyroiditis. TSH levels are oth-erwise elevated only in very rare con-ditions, such as TSH-secreting pitu-itary tumors and the syndrome ofGeneralized Resistance to ThyroidHormone. Medications, such as glu-cocorticoids, dopamine, and oc-treotide, may be associated withtransient decreases in TSH level (16).
What is subclinicalhypothyroidism, and is itassociated with adverse health outcomes?Subclinical hypothyroidism, ormild thyroid failure, is an elevatedserum TSH level with serum freeT4 or total T
4levels still within the
population reference range (17, 18).High TSH level indicates a serumT
4value that is within the reference
range but is lower than normal forthat person. The increase in serumTSH stimulates the thyroid glandto compensate, at least temporarily,and produce nearly adequateamounts of thyroid hormone.
Table 2. Differential Diagnosis of HypothyroidismDisease Characteristics Notes
Hashimoto disease TSH high; TPO antibodies Slowly progressiveThyroidectomy TSH high; history of surgery Surgical scarRadioiodine therapy TSH high; history of 131-I treatment History of thyrotoxicosisExternal radiation therapy TSH high; history of radiation therapy History of cancerIodine deficiency TSH high; urine iodine low Iodine deficient areaPostpartum thyroiditis TSH high; TPO antibodies Recent pregnancySilent thyroiditis TSH high; TPO antibodies Recent thyrotoxicosisSubacute thyroiditis TSH high; painful; ESR elevated Recent thyrotoxicosisDrug induced TSH high; use of amiodarone, lithium, Medication history
interferon, iodine, or thionamidesPituitary/hypothalamic mass TSH low or normal; FT
4low; Headaches, visual field cuts,
abnormal MRI/CT scan ophthalmoplegiaPituitary/hypothalamic surgery TSH low or normal; FT
4low History of surgery
Pituitary/hypothalamic TSH low or normal; FT4
low History of radiation therapyradiation therapyPituitary/hypothalamic TSH low or normal; FT
4low; Headaches, visual field cuts,
infiltration/infection abnormal MRI/CT scan ophthalmoplegia
CT = computed tomography; ESR = erythrocyte sedimentation rate; FT4
= free thyroxine; MRI = magnetic resonanceimaging; TPO = thyroid peroxidase.
Table 1. Laboratory and Other Studies for Hypothyroidism*Likelihood Likelihood
Test Sensitivity, % Specificity, % Positive Negative Notes
TSH >99 >99 >99 <0.01FT
490 90 9 0.11
Total T4
90 80 4.5 0.12Anti-TPO antibodies Found in >90% of patients
with Hashimoto diseaseESR Elevated in >90% of
patients with subacutethyroiditis
ESR = erythrocyte sedimentation rate; FT4
= free T4; T
4= thyroxine; TPO = thyroid peroxidase;
TSH = thyroid-stimulating hormone.
* Adapted from Dolan JG, Wittlin SD. Hyperthyroidism and hypothyroidism. In: Black ER, Bordley DR, Tape TG, PanzerRJ, eds. Diagnostic Strategies for Common Medical Problems. 2nd ed. Philadelphia: American Coll of Physicians;1999:473-83.

34. Brenta G, Mutti LA,Schnitman M, et al.Assessment of leftventricular diastolicfunction by radionu-clide ventriculogra-phy at rest and exer-cise in subclinicalhypothyroidism, andits response to L-thy-roxine therapy. Am JCardiol.2003;91:1327-30.[PMID: 12767425]
35. Yazici M, Gorgulu S,Sertbas Y, et al. Ef-fects of thyroxintherapy on cardiacfunction in patientswith subclinical hy-pothyroidism: indexof myocardial per-formance in theevaluation of leftventricular function.Int J Cardiol.2004;95:135-43.[PMID: 15193811]
36. Nagasaki T, Inaba M,Kumeda Y, et al. In-creased pulse wavevelocity in subclini-cal hypothyroidism.J Clin EndocrinolMetab. 2006;91:154-8. [PMID: 16234303]
37. Taddei S, Caraccio N,Virdis A, et al. Im-paired endothelium-dependent vasodi-latation insubclinical hypothy-roidism: beneficialeffect of levothyrox-ine therapy. J ClinEndocrinol Metab.2003;88:3731-7.[PMID: 12915662]
38. Cikim AS, Oflaz H,Ozbey N, et al. Evalu-ation of endothelialfunction in subclini-cal hypothyroidismand subclinical hy-perthyroidism. Thy-roid. 2004;14:605-9.[PMID: 15320973]
39. Kvetny J, HeldgaardPE, Bladbjerg EM, etal. Subclinical hy-pothyroidism is as-sociated with a low-grade inflammation,increased triglyc-eride levels and pre-dicts cardiovasculardisease in males be-low 50 years. ClinEndocrinol (Oxf ).2004;61:232-8.[PMID: 15272919]
40. Monzani F, CaraccioN, Kozakowa M, et al.Effect of levothyrox-ine replacement onlipid profile and inti-ma-media thicknessin subclinical hy-pothyroidism: a dou-ble-blind, placebo-controlled study. JClin EndocrinolMetab.2004;89:2099-106.[PMID: 15126526]
© 2009 American College of Physicians ITC6-6 In the Clinic Annals of Internal Medicine 1 December 2009
Subclinical hypothyroidism may beassociated with various nonspecificsymptoms and signs that are similarto but generally milder than those ofovert hypothyroidism (2, 17–26).Similarly, subclinical hypothyroidismcan result in elevated serum totalcholesterol and low-density lipopro-tein cholesterol levels (2, 26–28) andabnormal lipoprotein remnant me-tabolism (29). Mildly impaired thy-roid function is also associated withfeatures of the metabolic syndrome,including hypertension, increasedwaist circumference, elevated serumtriglyceride level, low serum high-density lipoprotein cholesterol level,and insulin resistance (30). Subclini-cal hypothyroidism has been associ-ated with subtle abnormalities ofcardiac function (31–35), impairedblood pressure regulation (36), im-paired endothelial function (37, 38),increased levels of C-reactive protein(39), increased carotid artery intima-media thickness (40), increased arte-rial stiffness (41), and increased arterial pulse wave velocity (36). Inaddition, subclinical hypothyroidismhas been associated with abnormalcerebral nerve conduction latency(42) and alterations of cerebral bloodflow (43). Although gross neuropsy-chological function does not seem tobe affected (44), working memoryhas been shown to be impaired (25).
Subclinical hypothyroidism pro-gresses to overt hypothyroidism at arate of 5% to 18% per year (45). Pro-gression is more likely in patientswho have circulating antithyroid an-tibodies but is most reliably predict-ed by the magnitude of the TSH elevation (46, 47).
Large cross-sectional and longitu-dinal observation studies have re-ported that mild thyroid failure is asignificant risk factor for the devel-opment of atherosclerosis (31,48–52) and congestive heart failure(53), although 1 study did not findan increased risk for cardiovasculardisorders or mortality (54).
When should clinicians consultwith an endocrinologist forpatients with possiblehypothyroidism?Consultation with an endocrinologistis recommended when a patient withhypothyroidism has DeQuervain orsilent thyroiditis or known or proba-ble coronary artery disease, has car-diac rhythm disturbances, has centralhypothyroidism, or is suspected ofhaving myxedema coma. Consulta-tion may also be helpful if the clini-cian is uncertain about whether anabnormal thyroid hormone profile isthe result of hypothyroidism or of anonthyroidal illness (the euthyroidsick syndrome).
Diagnosis... Patients with hypothyroidism often have a spectrum of clinical featuresthat can be identified by a complete history and physical examination and routinelaboratory testing. An elevated serum TSH level is the most reliable laboratory testfor the diagnosis of primary hypothyroidism. Measurement of the serum free T4 levelshould be done in all patients who have elevated serum TSH levels to determine theseverity of the hypothyroidism. When central hypothyroidism is suspected, radi-ographic imaging of the pituitary and hypothalamus is indicated.
CLINICAL BOTTOM LINE
Treatmenteffectively, and reliably relievessymptoms and normalizes labora-tory test results in most patientswith hypothyroidism (5, 55, 56).LT
4is converted to liothyronine
How should clinicians choose drug therapy and dose forhypothyroidism?Levothyroxine (LT4) is the treat-ment of choice because it safely,

© 2009 American College of PhysiciansITC6-7In the ClinicAnnals of Internal Medicine1 December 2009
41. Owen PJ, Rajiv C,Vinereanu D, et al.Subclinical hypothy-roidism, arterial stiff-ness, and myocardialreserve. J Clin En-docrinol Metab.2006;91:2126-32.[PMID: 16537677]
42. Tütüncü NB, Kara-ta≈ü M, Sözay S. Pro-longed P300 latencyin thyroid failure: aparadox. P300 laten-cy recovers later inmild hypothyroidismthan in severe hy-pothyroidism. Thy-roid. 2004;14:622-7.[PMID: 15320976]
43. Krausz Y, FreedmanN, Lester H, et al. Re-gional cerebralblood flow in pa-tients with mild hy-pothyroidism. J NuclMed. 2004;45:1712-5. [PMID: 15471838]
44. Jorde R, Waterloo K,Storhaug H, et al.Neuropsychologicalfunction and symp-toms in subjectswith subclinical hy-pothyroidism andthe effect of thyrox-ine treatment. J ClinEndocrinol Metab.2006;91:145-53.[PMID: 16263815]
45. Kabadi UM. ‘Subclini-cal hypothyroidism.’Natural course ofthe syndrome dur-ing a prolonged fol-low-up study. ArchIntern Med.1993;153:957-61.[PMID: 8481068]
46. Huber G, Staub JJ,Meier C, et al.Prospective study ofthe spontaneouscourse of subclinicalhypothyroidism:prognostic value ofthyrotropin, thyroidreserve, and thyroidantibodies. J Clin En-docrinol Metab.2002;87:3221-6.[PMID: 12107228]
47. Díez JJ, Iglesias P.Spontaneous sub-clinical hypothy-roidism in patientsolder than 55 years:an analysis of naturalcourse and risk fac-tors for the develop-ment of overt thy-roid failure. J ClinEndocrinol Metab.2004;89:4890-7.[PMID: 15472181]
48. Hak AE, Pols HA,Visser TJ, et al. Sub-clinical hypothy-roidism is an inde-pendent risk factorfor atherosclerosisand myocardial in-farction in elderlywomen: the Rotter-dam Study. Ann In-tern Med.2000;132:270-8.[PMID: 10681281]
(LT3) by peripheral tissues at a
rate that is appropriate for overallmetabolic needs (57). BedtimeLT
4dosing may normalize serum
TSH levels more effectively thanmorning dosing (58). Residualsymptoms may persist in somepatients with treated hypothy-roidism (59, 60), suggesting thatundertreatment may be relativelycommon. LT
4is available in sev-
eral doses, allowing precise titra-tion until the TSH level is withinthe optimal range. The relativelyslow intestinal absorption andlong serum half-life of LT
4pro-
duce stable serum TSH, T4, and
T3
levels with minimal diurnalvariation (55, 56).
Prospective intervention studieshave determined that the averageLT
4replacement dose in adults
with overt hypothyroidism is 1.6 µg/kg per day (61, 62) andthat lean body mass is a betterpredictor of thyroid hormone requirements than total bodyweight (63).
Young, otherwise healthy patientstolerate initial full doses well andusually obtain rapid relief ofsymptoms that are due to thyroidhormone deficiency. In obese pa-tients, the initial dose should becalculated by using ideal bodyweight with subsequent titrationof the LT4 dose every 6 to 8weeks until the serum TSH levelis in the optimal range. Patientswith known heart disease andelderly patients, who sometimeshave undiagnosed heart disease,may develop dysrhythmias, angi-na pectoris, or myocardial infarctions when started on full replacement doses or when theirdose is increased too rapidly (64).Overt hypothyroidism in a pa-tient older than 60 years shouldbe treated with an initial LT
4
dose of 25 to 50 µg/d and doseincreases in 12.5- to 25-µg incre-ments every 6 to 8 weeks untilthe desired dose is reached.
Does evidence show differences ineffectiveness and safety of variousthyroid hormone preparations?No high-quality randomized,controlled trials compare thesafety and efficacy of name-brandLT4 with generic LT
4products
(Table 3). The U.S. Food andDrug Administration (FDA) cur-rently requires all LT
4prepara-
tions to contain between 95% and105% of the stated amount ofLT
4. Some generic LT
4manufac-
turers also have shown that, byFDA standards, their productsprovide blood levels equivalent tothe name-brand products, whichmeans that pharmacists cansometimes switch from 1 genericformulation to another withoutnotifying the prescriber. Becauseof the narrow therapeutic indexof LT
4, even small differences in
bioavailability between formula-tions may cause clinical hypo- orhyperthyroidism. Therefore,many experts recommend usingLT
4from a single manufacturer,
which is easier to do with name-brand than generic products, es-pecially because the differences incost are small.
One RCT reported that co-admin-istration of LT
4and LT
3(Cytomel)
preparations improved some symp-toms more than LT
4alone (65);
however, multiple subsequentRCTs using LT
4and LT
3in various
ratios have not confirmed a benefi-cial effect of combined LT
4–LT
3
therapy (66, 67).
Combined LT4–LT3
products,such as Liotrix and desiccatedthyroid, contain a higher fixed ra-tio of T
4to T
3than that of normal
thyroid secretions (68, 69). T3
inthese preparations is rapidly ab-sorbed into the circulation andmay result in supraphysiologicserum T
3levels for several hours
after administration. This may beparticularly hazardous to patientswith underlying coronary arterydisease or dysrhythmias.
49. Mya MM, AronowWS. Subclinical hy-pothyroidism is as-sociated with coro-nary artery diseasein older persons. JGerontol A Biol SciMed Sci.2002;57:M658-9.[PMID: 12242320]
50. Imaizumi M, Aka-hoshi M, Ichimaru S,et al. Risk for is-chemic heart dis-ease and all-causemortality in subclini-cal hypothyroidism.J Clin EndocrinolMetab.2004;89:3365-70.[PMID: 15240616]
51. Walsh JP, BremnerAP, Bulsara MK, et al.Subclinical thyroiddysfunction as a riskfactor for cardiovas-cular disease. ArchIntern Med.2005;165:2467-72.[PMID: 16314542]
© 2009 American College of Physicians ITC6-8 In the Clinic Annals of Internal Medicine 1 December 2009
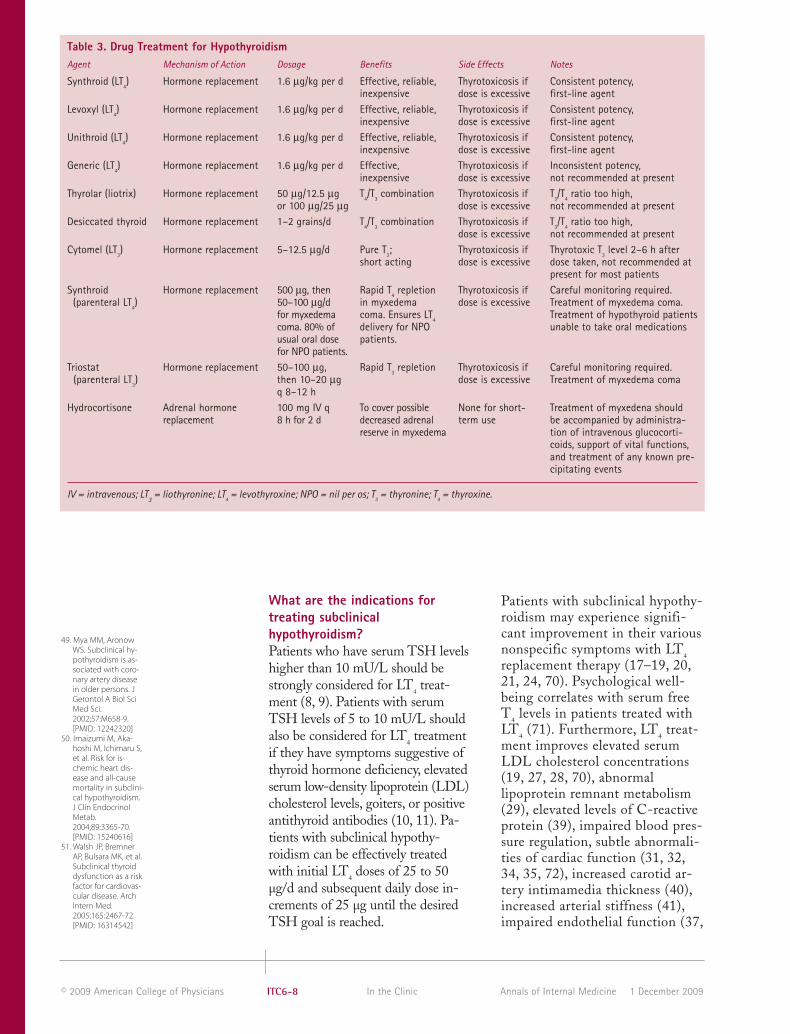
What are the indications fortreating subclinicalhypothyroidism?Patients who have serum TSH levelshigher than 10 mU/L should bestrongly considered for LT4 treat-ment (8, 9). Patients with serumTSH levels of 5 to 10 mU/L shouldalso be considered for LT
4treatment
if they have symptoms suggestive ofthyroid hormone deficiency, elevatedserum low-density lipoprotein (LDL)cholesterol levels, goiters, or positiveantithyroid antibodies (10, 11). Pa-tients with subclinical hypothy-roidism can be effectively treatedwith initial LT
4doses of 25 to 50
µg/d and subsequent daily dose in-crements of 25 µg until the desiredTSH goal is reached.
Patients with subclinical hypothy-roidism may experience signifi-cant improvement in their variousnonspecific symptoms with LT4replacement therapy (17–19, 20,21, 24, 70). Psychological well-being correlates with serum freeT
4levels in patients treated with
LT4
(71). Furthermore, LT4
treat-ment improves elevated serumLDL cholesterol concentrations(19, 27, 28, 70), abnormallipoprotein remnant metabolism(29), elevated levels of C-reactiveprotein (39), impaired blood pres-sure regulation, subtle abnormali-ties of cardiac function (31, 32,34, 35, 72), increased carotid ar-tery intimamedia thickness (40),increased arterial stiffness (41),impaired endothelial function (37,
Table 3. Drug Treatment for HypothyroidismAgent Mechanism of Action Dosage Benefits Side Effects Notes
Synthroid (LT4) Hormone replacement 1.6 μg/kg per d Effective, reliable, Thyrotoxicosis if Consistent potency,
inexpensive dose is excessive first-line agentLevoxyl (LT
4) Hormone replacement 1.6 μg/kg per d Effective, reliable, Thyrotoxicosis if Consistent potency,
inexpensive dose is excessive first-line agentUnithroid (LT
4) Hormone replacement 1.6 μg/kg per d Effective, reliable, Thyrotoxicosis if Consistent potency,
inexpensive dose is excessive first-line agentGeneric (LT
4) Hormone replacement 1.6 μg/kg per d Effective, Thyrotoxicosis if Inconsistent potency,
inexpensive dose is excessive not recommended at presentThyrolar (liotrix) Hormone replacement 50 μg/12.5 μg T
4/T
3combination Thyrotoxicosis if T
3/T
4ratio too high,
or 100 μg/25 μg dose is excessive not recommended at presentDesiccated thyroid Hormone replacement 1–2 grains/d T
4/T
3combination Thyrotoxicosis if T
3/T
4ratio too high,
dose is excessive not recommended at presentCytomel (LT
3) Hormone replacement 5–12.5 μg/d Pure T
3; Thyrotoxicosis if Thyrotoxic T
3level 2–6 h after
short acting dose is excessive dose taken, not recommended atpresent for most patients
Synthroid Hormone replacement 500 μg, then Rapid T4
repletion Thyrotoxicosis if Careful monitoring required. (parenteral LT
4) 50–100 μg/d in myxedema dose is excessive Treatment of myxedema coma.
for myxedema coma. Ensures LT4
Treatment of hypothyroid patients coma. 80% of delivery for NPO unable to take oral medicationsusual oral dose patients.for NPO patients.
Triostat Hormone replacement 50–100 μg, Rapid T3
repletion Thyrotoxicosis if Careful monitoring required. (parenteral LT
3) then 10–20 μg dose is excessive Treatment of myxedema coma
q 8–12 hHydrocortisone Adrenal hormone 100 mg IV q To cover possible None for short- Treatment of myxedena should
replacement 8 h for 2 d decreased adrenal term use be accompanied by administra-reserve in myxedema tion of intravenous glucocorti-
coids, support of vital functions,and treatment of any known pre-cipitating events
IV = intravenous; LT3
= liothyronine; LT4
= levothyroxine; NPO = nil per os; T3
= thyronine; T4
= thyroxine.

52. Rodondi N, AujeskyD, Vittinghoff E, et al.Subclinical hypothy-roidism and the riskof coronary heartdisease: a meta-analysis. Am J Med.2006;119:541-51.[PMID: 16828622]
53. Rodondi N, New-man AB, VittinghoffE, et al. Subclinicalhypothyroidism andthe risk of heart fail-ure, other cardiovas-cular events, anddeath. Arch InternMed. 2005;165:2460-6. [PMID: 16314541]
54. Cappola AR, Fried LP,Arnold AM, et al.Thyroid status, car-diovascular risk, andmortality in olderadults. JAMA.2006;295:1033-41.[PMID: 16507804]
55. Toft AD. Thyroxinetherapy. N Engl JMed. 1994;331:174-80. [PMID: 8008032]
56. Oppenheimer JH,Braverman LE, Toft A,et al. A therapeuticcontroversy. Thyroidhormone treatment:when and what? JClin EndocrinolMetab.1995;80:2873-83.[PMID: 7559868]
57. Lum SM, Nicoloff JT,Spencer CA, et al.Peripheral tissuemechanism formaintenance ofserum triiodothyro-nine values in a thy-roxine-deficientstate in man. J ClinInvest. 1984;73:570-5. [PMID: 6699177]
58. Bolk N, Visser TJ,Kalsbeek A, et al. Ef-fects of evening vsmorning thyroxineingestion on serumthyroid hormoneprofiles in hypothy-roid patients. ClinEndocrinol (Oxf ).2007;66:43-8. ([pmid]17201800[/pmid])
59. Samuels MH, SchuffKG, Carlson NE, et al.Health status, psy-chological symp-toms, mood, andcognition in L-thy-roxine-treated hy-pothyroid subjects.Thyroid.2007;17:249-58.[PMID: 17381359]
60. Saravanan P, ChauWF, Roberts N, et al.Psychological well-being in patients on‘adequate’ doses of l-thyroxine: results ofa large, controlledcommunity-basedquestionnaire study.Clin Endocrinol(Oxf ). 2002;57:577-85. [PMID: 12390330]
© 2009 American College of PhysiciansITC6-9In the ClinicAnnals of Internal Medicine1 December 2009
38, 70), and abnormal cerebralnerve conduction latency (42).RCTs to determine whethertreatment of subclinical hypothy-roidism reduces the rate of ad-verse cardiovascular events ormortality are needed (8, 26).
Most of the evidence showing bene-ficial effects of LT
4treatment on
symptoms, lipid and lipoprotein profiles and tests of vascular andneurological function in subclinicalhypothyroidism comes from RCTsinvolving patients with TSH levelsof 10 mU/L or greater (8, 26).RCT evidence that patients withserum TSH levels of 5 to 10 mU/Lshow similar improvement insymptoms and lipid profiles withLT
4treatment is inconclusive (8,
26) but suggestive (70). One obser-vational study reported an unex-pected increase in cardiovascularmorbidity in patients treated forhypothyroidism (73); however, theauthors conceded that this wasprobably related to atherosclerosisfrom the preexisting hypothy-roidism, inappropriate thyroid hor-mone dosing, or both (73).
What are the adverse effects ofthyroid replacement therapy?Side effects of proper thyroid hormone replacement, except in
rare patients, occur only when themedication is given in excessivedoses. Excessive LT4 doses mayresult in symptoms of thyrotoxico-sis. In elderly patients, LT
4excess
may also cause bone loss and atrialfibrillation.
How should clinicians monitorpatients with hypothyroidism?Clinicians should assess symptomsand signs of hypothyroidism ateach follow-up visit for patients onthyroid hormone therapy (Table 4).LT4 effectively relieves the manifes-tations of thyroid hormone defi-ciency in most patients with overt(55, 56) and subclinical (18–21)hypothyroidism. Serum LDL andnon–high-density lipoprotein cho-lesterol levels also decrease withtreatment (19, 27, 28, 70, 74). Also,clinicians should evaluate compli-ance with LT
4dosing instructions
and the use of other medications ateach follow-up visit.
Requirements for thyroid hormonereplacement may change over timein response to changes in healthstatus and the use of certain med-ications. Situations in which LT4dose requirements increase includepregnancy (75–77); the use of es-trogens (78); noncompliance (79);weight gain; malabsorption;
Table 4. Elements of Follow-up for HypothyroidismCategory Issue How? How often? Note
History Weakness Question Every visit Improvement expected History Lethargy Question Every visit Improvement expectedHistory Fatigue Question Every visit Improvement expectedHistory Cold intolerance Question Every visit Improvement expectedHistory Impaired memory Question Every visit Improvement expectedHistory Adherence Question Every visit Adherence essentialHistory Other drugs Question Every visit May interfere with LT
4
Physical examination Dry skin Palpation Every visit Improvement expectedPhysical examination Coarse skin Palpation Every visit Improvement expectedPhysical examination Periorbital puffiness Inspection Every visit Improvement expectedLaboratory TSH Measure by q6–8 wk until Normal: 0.5–5.0 mU/L;
second- normal, 3–6 mo Optimal: 0.5–2.0 mU/Lgeneration later, then TSH assay annually
LT4
= levothyroxine; TSH = thyroid-stimulating hormone.
61. Fish LH, SchwartzHL, Cavanaugh J, etal. Replacementdose, metabolism,and bioavailability oflevothyroxine in thetreatment of hy-pothyroidism. Roleof triiodothyroninein pituitary feedbackin humans. N Engl JMed. 1987;316:764-70. [PMID: 3821822]
62. Roos A, Linn-RaskerSP, van Domburg RT,et al. The startingdose of levothyrox-ine in primary hy-pothyroidism treat-ment: a prospective,randomized, double-blind trial. Arch In-tern Med.2005;165:1714-20.[PMID: 16087818]
63. Santini F, Pinchera A,Marsili A, et al. Leanbody mass is a ma-jor determinant oflevothyroxinedosage in the treat-ment of thyroid dis-eases. J Clin En-docrinol Metab.2005;90:124-7.[PMID: 15483074]
64. Becker C. Hypothy-roidism and athero-sclerotic heart dis-ease: pathogenesis,medical manage-ment, and the roleof coronary arterybypass surgery. En-docr Rev.1985;6:432-40.[PMID: 3896769]
65. Bunevicius R,Kazanavicius G, Za-linkevicius R, et al. Ef-fects of thyroxine ascompared with thy-roxine plus tri-iodothyronine in pa-tients withhypothyroidism. NEngl J Med.1999;340:424-9.[PMID: 9971866]
66. Escobar-MorrealeHF, Botella-CarreteroJI, Escobar del Rey F,et al. REVIEW: Treat-ment of hypothy-roidism with combi-nations oflevothyroxine plusliothyronine. J ClinEndocrinol Metab.2005;90:4946-54.[PMID: 15928247]
67. Grozinsky-GlasbergS, Fraser A, NahshoniE, et al. Thyroxine-tri-iodothyronine com-bination therapyversus thyroxinemonotherapy forclinical hypothy-roidism: meta-analy-sis of randomizedcontrolled trials. JClin EndocrinolMetab.2006;91:2592-9.[PMID: 16670166]
© 2009 American College of Physicians ITC6-10 In the Clinic Annals of Internal Medicine 1 December 2009
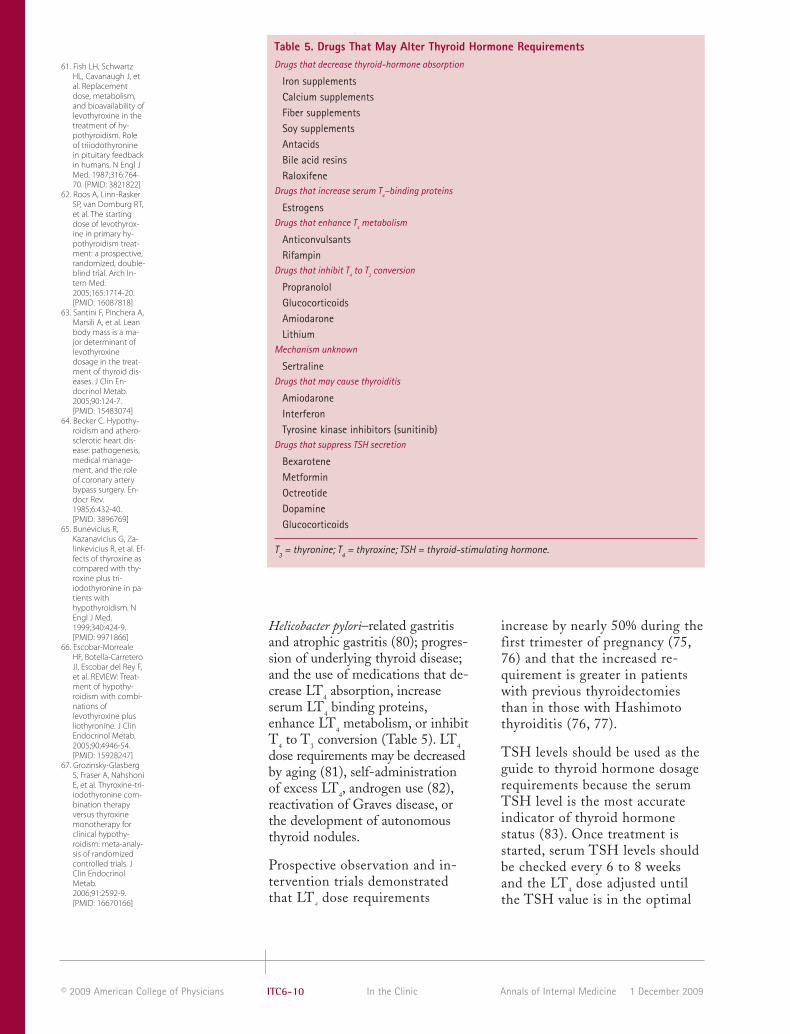
Helicobacter pylori–related gastritisand atrophic gastritis (80); progres-sion of underlying thyroid disease;and the use of medications that de-crease LT
4absorption, increase
serum LT4
binding proteins, enhance LT
4metabolism, or inhibit
T4
to T3
conversion (Table 5). LT4
dose requirements may be decreasedby aging (81), self-administrationof excess LT
4, androgen use (82),
reactivation of Graves disease, orthe development of autonomousthyroid nodules.
Prospective observation and in-tervention trials demonstratedthat LT
4dose requirements
increase by nearly 50% during thefirst trimester of pregnancy (75,76) and that the increased re-quirement is greater in patientswith previous thyroidectomiesthan in those with Hashimotothyroiditis (76, 77).
TSH levels should be used as theguide to thyroid hormone dosagerequirements because the serumTSH level is the most accurateindicator of thyroid hormone status (83). Once treatment isstarted, serum TSH levels shouldbe checked every 6 to 8 weeksand the LT4 dose adjusted untilthe TSH value is in the optimal
Table 5. Drugs That May Alter Thyroid Hormone RequirementsDrugs that decrease thyroid-hormone absorption
Iron supplementsCalcium supplementsFiber supplementsSoy supplementsAntacidsBile acid resinsRaloxifene
Drugs that increase serum T4–binding proteins
EstrogensDrugs that enhance T
4metabolism
AnticonvulsantsRifampin
Drugs that inhibit T4
to T3
conversion
PropranololGlucocorticoidsAmiodaroneLithium
Mechanism unknown
SertralineDrugs that may cause thyroiditis
AmiodaroneInterferonTyrosine kinase inhibitors (sunitinib)
Drugs that suppress TSH secretion
BexaroteneMetforminOctreotideDopamineGlucocorticoids
T3
= thyronine; T4
= thyroxine; TSH = thyroid-stimulating hormone.

68. Rees-Jones RW, RollaAR, Larsen PR. Hor-monal content ofthyroid replacementpreparations. JAMA.1980;243:549-50.[PMID: 7351788]
69. Pilo A, Iervasi G,Vitek F, et al. Thy-roidal and peripheralproduction of 3,5.3’-triiodothyronine inhumans by multi-compartmentalanalysis. Am J Physi-ol. 1990;258:E715-26.[PMID: 2333963]
70. Razvi S, Ingoe L,Keeka G, et al. Thebeneficial effect of L-thyroxine on cardio-vascular risk factors,endothelial function,and quality of life insubclinical hypothy-roidism: randomized,crossover trial. J ClinEndocrinol Metab.2007;92:1715-23.[PMID: 17299073]
71. Saravanan P, VisserTJ, Dayan CM. Psy-chological well-be-ing correlates withfree thyroxine butnot free 3,5,3’-tri-iodothyronine levelsin patients on thy-roid hormone re-placement. J Clin En-docrinol Metab.2006;91:3389-93.[PMID: 16804044]
72. Turhan S, Tulunay C,Ozduman Cin M, etal. Effects of thyrox-ine therapy on rightventricular systolicand diastolic func-tion in patients withsubclinical hypothy-roidism: a study bypulsed wave tissueDoppler imaging. JClin EndocrinolMetab.2006;91:3490-3.[PMID: 16822817]
73. Flynn RW, Macdon-ald TM, Jung RT, etal. Mortality and vas-cular outcomes inpatients treated forthyroid dysfunction.J Clin EndocrinolMetab.2006;91:2159-64.[PMID: 16537678]
74. Ito M, Arishima T,Kudo T, et al. Effectof levo-thyroxine re-placement on non-high-densitylipoprotein choles-terol in hypothyroidpatients. J Clin En-docrinol Metab.2007;92:608-11.[PMID: 17148561]
© 2009 American College of PhysiciansITC6-11In the ClinicAnnals of Internal Medicine1 December 2009
roidism (Table 6) (85, 86). Itmost often occurs in elderly patients who have untreated orinadequately treated hypothy-roidism and who then develop aprecipitating event, such as use ofa drug that suppresses the centralnervous system, myocardial in-farction, stroke, pulmonary embolus, sepsis, or prolonged exposure to cold temperatures.Without appropriate treatment,the mortality rate of this condi-tion approaches 100%. Patientsshould be hospitalized in an in-tensive care unit for intensivemonitoring and treatment whenthey are suspected of havingmyxedema coma because prompt
Free
T4,
pmol
/L
10
20
30
-25 +25 +50 +75Optimum
Dosage LT4, µgFigure 3The effect on free T4 of fine adjustment of LT
4doses in patients with primary
hypothyroidism. Reprinted with permission from Carr D, McLeod DT, Parry G,Thornes HM. Fine adjustment of thyroxine replacement dosage: comparisonof the thyrotrophin releasing hormone test using a sensitive thyrotrophinassay with measurement of free thyroid hormones and clinical assessment.Clin Endocrinol (Oxf). 1988;28:325-33.
range; the TSH level should thenbe rechecked 3 to 6 months later,and annually thereafter. Whenfollow-up serum TSH levels driftoutside the normal range, adjust-ing the daily LT
4dose by 12.5- to
25-µg will usually return theserum TSH level to normal (84)(Figure 3). The optimal TSH lev-el is 0.5 to 2.0 mU/L, becausemost persons have TSH levels inthis lower end of the populationnormal range (3).
When should patients withhypothyroidism be hospitalized?Myxedema coma is a life-threat-ening condition that is the mostsevere expression of hypothy-

75. Mandel SJ, LarsenPR, Seely EW, et al.Increased need forthyroxine duringpregnancy inwomen with pri-mary hypothy-roidism. N Engl JMed. 1990;323:91-6.[PMID: 2359428]
76. Alexander EK, Mar-qusee E, Lawrence J,et al. Timing andmagnitude of in-creases in levothy-roxine requirementsduring pregnancy inwomen with hy-pothyroidism. N EnglJ Med. 2004;351:241-9. [PMID: 15254282]
77. Rotondi M, MazziottiG, Sorvillo F, et al. Ef-fects of increasedthyroxine dosagepre-conception onthyroid function dur-ing early pregnancy.Eur J Endocrinol.2004;151:695-700.[PMID: 15588235]
78. Arafah BM. In-creased need forthyroxine in womenwith hypothyroidismduring estrogentherapy. N Engl JMed. 2001;344:1743-9. [PMID: 11396440]
79. Ain KB, Refetoff S,Fein HG, et al.Pseudomalabsorp-tion of levothyrox-ine. JAMA.1991;266:2118-20.[PMID: 1920700]
80. Centanni M,Gargano L, Canet-tieri G, et al. Thyrox-ine in goiter, Heli-cobacter pyloriinfection, and chron-ic gastritis. N Engl JMed. 2006;354:1787-95. [PMID: 16641395]
81. Rosenbaum RL,Barzel US. Levothy-roxine replacementdose for primary hy-pothyroidism de-creases with age.Ann Intern Med.1982;96:53-5.[PMID: 7053703]
82. Arafah BM. De-creased levothyrox-ine requirement inwomen with hy-pothyroidism duringandrogen therapyfor breast cancer.Ann Intern Med.1994;121:247-51.[PMID: 7518657]
83. Mandel SJ, Brent GA,Larsen PR. Levothy-roxine therapy in pa-tients with thyroiddisease. Ann InternMed. 1993;119:492-502. [PMID: 8357116]
© 2009 American College of Physicians ITC6-12 In the Clinic Annals of Internal Medicine 1 December 2009
recognition and proper manage-ment significantly improve theprognosis. Nonetheless, the mor-tality rate of myxedema coma remains nearly 50% because of co-morbid precipitating conditions.
The cornerstone of treatment ofmyxedema coma is rapid replacement
of the thyroid hormone deficit withintravenous LT4, LT
3, or a combina-
tion of the 2 (85). Aggressive thyroidhormone replacement should be ac-companied by administration ofstress doses of intravenous glucocor-ticoids, support of vital functions, andtreatment of any known precipitatingevents (85).
Table 6. Key Clinical Features of Myxedema ComaElement, by Category Notes
History
Hypothyroidism; undiagnosed, untreated The underlying hypothyroidism does not have to or inadequately treated be severe
Precipitating factor
Prolonged cold exposure Particularly in elderly personsSedative use Particularly in elderly personsInfection Particularly in elderly personsPulmonary embolus Particularly in elderly personsRespiratory failure Particularly in elderly personsMyocardial infarction Particularly in elderly personsCongestive heart failure Particularly in elderly personsStroke Particularly in elderly personsGastrointestinal bleeding Particularly in elderly personsTrauma Particularly in elderly personsSurgery Particularly in elderly persons
Physical
HypothermiaBradycardiaHypotensionHypoventilationSeizuresStuporComaMyxedematous skin changesPeriorbital edemaDelayed relaxation of reflexes Distended abdomen IleusDistended bladder Urinary retention
Radiology
Pleural effusionsPericardial effusions
Electrocardiogram
Low voltage, bradycardiaLaboratory
Macrocytic anemiaHyponatremiaElevated creatine kinase Hypercarbia (CO
2retention)
Elevated serum thyroid-stimulating Need not be significantly elevatedhormone
Low serum free thyroxine Need not be significantly depressed

84. Carr D, McLeod DT,Parry G, et al. Fineadjustment of thy-roxine replacementdosage: comparisonof the thyrotrophinreleasing hormonetest using a sensitivethyrotrophin assaywith measurementof free thyroid hor-mones and clinicalassessment. Clin En-docrinol (Oxf ).1988;28:325-33.[PMID: 3139338]
85. Nicoloff JT, LoPrestiJS. Myxedema coma.A form of decom-pensated hypothy-roidism. EndocrinolMetab Clin NorthAm. 1993;22:279-90.[PMID: 8325287]
86. Yamamoto T,Fukuyama J, Fu-jiyoshi A. Factors as-sociated with mor-tality of myxedemacoma: report ofeight cases and liter-ature survey. Thy-roid. 1999;9:1167-74.[PMID: 10646654]
87. Ladenson PW,Singer PA, Ain KB, etal. American ThyroidAssociation guide-lines for detection ofthyroid dysfunction.Arch Intern Med.2000;160:1573-5.[PMID: 10847249]
© 2009 American College of PhysiciansITC6-13In the ClinicAnnals of Internal Medicine1 December 2009
What measures do stakeholdersuse to evaluate the quality of care for patients withhypothyroidism?Federal legislation passed in 2006required the Centers forMedicare & Medicaid Services(CMS) to create a physicianquality reporting system that in-cluded an incentive payment foreligible professionals who satis-factorily report data on qualitymeasures for covered services fur-nished to Medicare beneficiaries.CMS named this program thePhysician Quality Reporting Ini-tiative (PQRI). Eligible profes-sionals who meet the criteria forsatisfactory submission of datafor services provided from 1 Jan-uary, 2009 to 31 December, 2009will earn an incentive payment of2.0% of their total allowedcharges. The 2009 PQRI consistsof 153 quality measures and 7measures groups. None of thesemeasures applies specifically topersons with hypothyroidism.
What do professionalorganizations recommendregarding the care of patientswith hypothyroidism?The American Thyroid Associationpublished its most recent treatmentguidelines for patients with hy-pothyroidism in 1995 (5) andguidelines for the detection of thy-roid dysfunction in 2000 (87).
The American Association of Clin-ical Endocrinologists publishedclinical practice guidelines for man-aging people with hypothyroidismand suspected hypothyroidism in2002 that were amended in 2006(www.aace.com/pub/pdf/guide-lines/hypo_hyper.pdf ). Theseguidelines emphasize the use of asensitive TSH or thyrotropin assayas the best screening test for hy-pothyroidism, and in most outpa-tient clinical situations, the use ofserum TSH level as the most sensi-tive test for detecting mild thyroidhormone excess or deficiency. Inclinical hypothyroidism, the guide-lines recommend LT4 as standardtreatment, which must be tailoredto the individual patient. Theseguidelines emphasize awareness ofsubclinical thyroid disease, whichoften remains undiagnosed, and asystem of care that incorporatesregular follow-up surveillance by 1physician as well as education andinvolvement of the patient.
In 2007, the Endocrine Societypublished guidelines for the man-agement of thyroid dysfunctionduring pregnancy (88). Theseguidelines emphasize that manage-ment of thyroid diseases duringpregnancy requires special consid-erations because pregnancy inducesmajor changes in thyroid function,and maternal thyroid disease canhave adverse effects on the
Practice Improvement
Treatment... Levothyroxine replacement is the cornerstone of therapy for hy-pothyroidism. Young and otherwise healthy patients can be started on a full re-placement dose of 1.6 µg/kg per day based on ideal body weight. Elderly patientsand those with known or suspected cardiac disease should be started on lowerdoses, such as 25 to 50 µg/d with gradual titration upward. Serum TSH levelsshould be checked at 6- to 12-week intervals to guide dosage titrations until theserum TSH level is within the population reference range or, optimally, within 0.5to 2.0 mU/L. The clinical manifestations of hypothyroidism resolve in the majorityof patients treated with adequate LT4 doses. Myxedema coma, the most severeform of hypothyroidism, is a life-threatening emergency that should be treated inan intensive care unit with rapid intravenous repletion of the large thyroid hor-mone deficit, in conjunction with stress glucocorticoid therapy, maintenance ofvital functions and treatment of any identified precipitating causes.
CLINICAL BOTTOM LINE

88. Abalovich M, AminoN, Barbour LA, et al.Management of thy-roid dysfunctionduring pregnancyand postpartum: anEndocrine SocietyClinical PracticeGuideline. J Clin En-docrinol Metab.2007;92:S1-47.[PMID: 17948378]
inthe
c linicTool Kit
in the clinic
Hypothyroidism
PIER Modulespier.acponline.orgAccess the PIER module on hypothyroidism. PIER modules provide evidence-based, updated information on current diagnosis and treatment in an electronicformat designed for rapid access at the point of care.
Patient Education Resourceswww.annals.org/intheclinic/toolkit-thyroid.htmlAccess the patient information located on the following page to download anddistribute to your patients.
www.acponline.org/patients_families/diseases_conditions/hypothyroidism/Access information for patients with hypothyroidism prepared by the AmericanCollege of Physicians.
www.nlm.nih.gov/medlineplus/ency/article/000353.htmAccess information for patients with hypothyroidism prepared by the NationalLibrary of Medicine of the National Institutes of Health.
www.thyroid.org/patients/patient_brochures/hypothyroidism.htmlAccess information for patients with hypothyroidism prepared by the AmericanThyroid Association.
1 December 2009Annals of Internal MedicineIn the ClinicITC6-14© 2009 American College of Physicians
pregnancy and the fetus. Care re-quires coordination among severalhealth care professionals. Avoidingmaternal (and fetal) hypothyroidismis of major importance because ofpotential damage to fetal neural de-velopment, an increased incidenceof miscarriage, and preterm delivery.Autoimmune thyroid disease is as-sociated with both increased rates ofmiscarriage, for which the appropri-ate medical response is uncertain,and postpartum thyroiditis. Ra-dioactive isotopes must be avoidedduring pregnancy and lactation.Universal screening of pregnantwomen for thyroid disease is notsupported by adequate studies, butcase finding targeted to specificgroups of patients who are at in-creased risk is strongly supported.
In 2005, the American Associationof Clinical Endocrinologists, theAmerican Thyroid Association, andthe Endocrine Society published aconsensus statement about themanagement of subclinical thyroiddysfunction (11). Although thestatement found that the correctapproach to subclinical thyroid dys-function remained unsettled, it rec-ommended routine screening forthyroid disease in the general pop-ulation, especially in pregnant
women. It also recommended thatmost patients with subclinical hy-pothyroidism should be treated andcautioned that best clinical practiceshould combine clinical judgmentand patients’ preferences.
In 2008, several British organiza-tions, including the Royal Collegeof Physicians, the Society for En-docrinology, and the British Thy-roid Association, published a state-ment about the diagnosis andmanagement of primary hypothy-roidism that expressed concernabout the possibility that somepeople were being diagnosed andmanaged inappropriately (www.rcplondon.ac.uk/specialties/Endocrinology-Diabetes/Documents/Hypothyroidism.pdf ).The statement concluded that pa-tients with suspected primary hy-pothyroidism should be diagnosedonly with blood tests, not tests ofother bodily fluids, such as urine;that patients with primary hypothy-roidism should be treated only withLT4 tablets, not thyroid extracts orcombinations of LT
4with LT
3; and
that patients with all thyroid bloodtests in the reference ranges shouldnot be treated for hypothyroidism,even if they have some symptomscompatible with hypothyroidism.
In the ClinicAnnals of Internal Medicine
Pati
ent
Info
rmat
ion
THINGS YOU SHOULDKNOW ABOUT HYPOTHYROIDISM
What is the thyroid gland?The thyroid gland is a hormone-secreting gland locatedin the neck, just below the Adam’s apple.
What do thyroid hormones do?Thyroid hormones regulate the body’s use of energy.
What is hypothyroidism?Hypothyroidism is a condition in which the thyroidgland secretes too little thyroid hormone into thecirculation.
What are the symptoms of hypothyroidism?Symptoms include fatigue, depression, increased needfor sleep, dry skin, cold intolerance, hoarseness, weightgain, menstrual irregularity, and constipation.
How is the diagnosis of hypothyroidism made?Blood tests can detect low levels of thyroid hormones.
How is hypothyroidism treated?Hypothyroidism is treated with oral thyroid hormonereplacement.
How long do I have to take thyroidhormone replacement?Once a person has developed hypothyroidism, the con-dition is usually permanent. Thyroid hormone replace-ment is a lifelong requirement.
For More Information
Web Sites With Good Information About Hypothyroidismwww.acponline.org/patients_families/diseases_conditions/hypothyroidism/Access information for patients with hypothyroidism prepared bythe American College of Physicians.
www.nlm.nih.gov/medlineplus/ency/article/000353.htmAccess information for patients with hypothyroidism prepared bythe National Library of Medicine of the National Institutes ofHealth.
www.thyroid.org/patients/patient_brochures/hypothyroidism.htmlAccess information for patients with hypothyroidism prepared bythe American Thyroid Association.

4.
3.
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP). Go to www.annals.org/intheclinic/ to obtain up to 1.5 CME credits, to view explanations for correct answers, or to purchase the complete MKSAP program.
CME Questions
1 December 2009Annals of Internal MedicineIn the ClinicITC6-16© 2009 American College of Physicians
A 28-year-old woman is evaluated forfatigue, weight gain, and occasionalconstipation. The patient has history ofcraniopharyngioma, which was resect-ed; she was subsequently given radia-tion therapy. She has hypopituitarismand diabetes insipidus after tumor re-section and radiation. Her medicationsinclude hydrocortisone, levothyroxine,oral contraceptives, and desmopressin.She does not have dizziness, nausea,vomiting, polyuria, or polydipsia. Shehas regular menstrual cycles. The physi-cal examination is unremarkable. Hercomplete blood count and electrolytepanel are normal. Her TSH level is 0.1mU/mL and her free T
4level is 6.4
pmol/L (0.5 ng/dL).
Which of the following changes shouldbe made to the patient’s therapy?
A. Hydrocortisone dose should belowered
B. Oral contraceptives should bediscontinued
C. Desmopressin should bediscontinued
D. Thyroid hormone dose should beincreased
A 45-year-old obese woman undergoesevaluation after learning her nonfastingserum total cholesterol level, which wasmeasured at a health screening fair 1month ago, was 6.72 mmol/L (260 mg/dL).The review of systems indicates increas-ingly heavy menstruation and constipa-tion. Her family history is negative forcoronary artery disease. The patient is oth-erwise healthy and does not smoke.
On physical examination, blood pressureis 120/80 mm Hg. The remainder of theexamination is normal. Her serum totalcholesterol level is 6.62 mmol/L (256mg/dL). Her serum triglyceride level is2.31 mmol/L (205 mg/dL). Her serumhigh-density lipoprotein cholesterol levelis 1.03 mmol/L (40 mg/dL). And herserum low-density lipoprotein choles-terol level is 4.53 mmol/L (175 mg/dL).
Which of the following is the most ap-propriate next step in the managementof this patient?
A. Fibric acid derivativeB. StatinC. Fish oil supplementD. Serum thyroid-stimulating
hormone measurement
A 45-year-old man presents with fatigue,constipation, and a 2-kg (5-lb) weight gain.The patient has Hashimoto thyroiditis andis adherent with his levothyroxine regimen,0.25 mg/d. Six months ago, the serum thy-roid-stimulating hormone (TSH) level was1.9 mU/mL and the serum free T
4level was
16.5 pmol/L (1.3 ng/dL). The serum TSH isnow 12.0 mU/mL, and the serum free T
4
level is 10.2 pmol/L (0.8 ng/dL).
What is the most likely explanation forthe change in thyroid hormone levels?
A. He has been taking sertraline fordepression starting 3 months ago.
B. He has begun taking an over-the-counter vitamin B complexsupplement and high-dose vitaminC tablets.
C. The pharmacy inadvertentlydispensed 0.025-mg tablets to him3 months earlier.
D. His weight gain has led to adecreased volume of distribution.
E. He has developed adrenalinsufficiency.
A 23-year-old woman is evaluated in theemergency department for nausea,anorexia, dizziness, and diffuse moderateabdominal discomfort. Three weeks ago,she had been evaluated for fatigue andcold intolerance and was noted to have afirm goiter, with the thyroid estimated tobe twice the size expected in a womanof her build. Thyroid peroxidase antibod-ies were positive, and her serum thyroid-stimulating hormone (TSH) level was 20mU/mL. Hashimoto thyroiditis was diag-nosed, and therapy with levothyroxine,100 µg/d, is begun. In addition to her
symptoms, she has had a 2-kg (4.5-lb)weight loss. In the emergency depart-ment, the blood pressure is 90/60 mmHg; the pulse rate is 100/min, and sheseems darkly pigmented. Laboratory re-sults include serum sodium, 132 mmol/L,potassium, 5.0 mmol/L, TSH level, 6.0mU/mL, and normal thyroxine (T4).
Which of the following would be themost appropriate next test in the evalua-tion of this patient?
A. Triiodothyronine (T3)B. Adrenocorticotropic hormone,
cortisol followed by cosyntropinstimulation
C. Thyroid-stimulatingimmunoglobulins
D. 24-hour urine collection for freecortisol
1.
2.
Related Documents











