Original article Identification of gene copy number variations in patients with mental retardation using array-CGH: Novel syndromes in a large French series Sylvie Jaillard a, b, * ,S everine Drunat c , Claude Bendavid b , Azzedine Aboura c , Amandine Etcheverry b , Hubert Journel d , Andr ee Delahaye e , Laurent Pasquier b, f , Dominique Bonneau g , Annick Toutain h , Lydie Burglen i , Agn es Guichet g , Eva Pipiras e , Brigitte Gilbert-Dussardier j , Brigitte Benzacken c, e , Dominique Martin-Coignard k , Catherine Henry a , Albert David l , Josette Lucas a , Jean Mosser b , V eronique David b, m , Sylvie Odent b, f , Alain Verloes c , Christ ele Dubourg b, m a Laboratoire de Cytog en etique et Biologie Cellulaire, CHU Pontchaillou, Rennes, France b CNRS UMR 6061, IFR 140 GFAS, Facult e de M edecine, Universit e de Rennes 1, France c D epartement de G en etique, INSERM U676, CHU Robert Debr e, APHP, Paris, France d Service de G en etique M edicale, CHBA, Vannes, France e Laboratoire de Cytog en etique, CHU Jean Verdier, SMBH, Paris XIII, U676 Gressens, Bondy, APHP, France f Service de G en etique M edicale, CHU Hôpital Sud, Rennes, France g Service de G en etique, CHU Angers, Angers, France h Service de G en etique, CHU Bretonneau, Tours, France i Service de G en etique et d'Embryologie M edicales, CHU Armand Trousseau, Paris, APHP, France j Service de G en etique M edicale, CHU Poitiers, Poitiers, France k Service de G en etique, CH Le Mans, Le Mans, France l Service de G en etique M edicale, Institut de Biologie, CHU Hôtel Dieu, Nantes, France m Laboratoire de G en etique Mol eculaire, CHU Pontchaillou, Rennes, France article info Article history: Received 14 April 2009 Accepted 17 October 2009 Available online 28 October 2009 Keywords: Array-CGH Novel syndromes Microdeletion Mental retardation abstract Array-CGH has revealed a large number of copy number variations (CNVs) in patients with multiple congenital anomalies and/or mental retardation (MCA/MR). According to criteria recently listed, pathogenicity was clearly suspected for some CNVs but benign CNVs, considered as polymorphisms, have complicated the interpretation of the results. In this study, genomic DNAs from 132 French patients with unexplained mental retardation were analysed by genome wide high-resolution Agilent Ò 44K oligonu- cleotide arrays. The results were in accordance with those observed in previous studies: the detection rate of pathogenic CNVs was 14.4%. A non-random involvement of several chromosomal regions was observed. Some of the microimbalances recurrently involved regions (1q21.1, 2q23.1, 2q32q33, 7p13, 17p13.3,17p11.2, 17q21.31) corresponding to known or novel syndromes. For all the pathogenic CNVs, further cases are needed to allow more accurate genotypeephenotype correlations underscoring the importance of databases to group patients with similar molecular data. Ó 2009 Elsevier Masson SAS. All rights reserved. 1. Introduction From the observation that subtelomeric anomalies can be found in about 5% of MCA/MR patients [22], it was suspected that small interstitial imbalances may also be an important cause of MCA/MR [46,65] that is underestimated by current cytogenetics methods (conventional and molecular cytogenetics). Whole-genome array- based technologies have became an essential tool for the detection of microimbalances and have identified such aberrations in 10e15% of MCA/MR patients with normal karyotype [17,20,21,23,24,29,40, 41,45,46,54,59,65,66]. The challenge now is to describe novel syndromes which can be achieved by comparing patients carrying the same subtle rearrangement. Array-CGH can give an accurate delineation of the imbalances which raises the possibility of making genotypeephenotype correlations, in order to identify minimal critical regions and candidate genes for a pattern of clinical features including learning disability. Fine mapping of genomic imbalances may indeed be useful to narrow down regions sus- pected to contain dosage sensitive genes critical for normal development [35]. * Corresponding author. Laboratoire de Cytog en etique et Biologie Cellulaire, CHU Pontchaillou, 2 rue Henri Le Guilloux, Rennes, France. Tel.: þ33 2 99 28 43 89. E-mail address: [email protected] (S. Jaillard). Contents lists available at ScienceDirect European Journal of Medical Genetics journal homepage: http://www.elsevier.com/locate/ejmg 1769-7212/$ e see front matter Ó 2009 Elsevier Masson SAS. All rights reserved. doi:10.1016/j.ejmg.2009.10.002 European Journal of Medical Genetics 53 (2010) 66e75

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
lable at ScienceDirect
European Journal of Medical Genetics 53 (2010) 66e75
Contents lists avai
European Journal of Medical Genetics
journal homepage: ht tp: / /www.elsevier .com/locate/e jmg
Original article
Identification of gene copy number variations in patients with mentalretardation using array-CGH: Novel syndromes in a large French series
Sylvie Jaillard a,b,*, S�everine Drunat c, Claude Bendavid b, Azzedine Aboura c, Amandine Etcheverry b,Hubert Journel d, Andr�ee Delahaye e, Laurent Pasquier b,f, Dominique Bonneau g, Annick Toutain h,Lydie Burglen i, Agn�es Guichet g, Eva Pipiras e, Brigitte Gilbert-Dussardier j, Brigitte Benzacken c,e,Dominique Martin-Coignard k, Catherine Henry a, Albert David l, Josette Lucas a, Jean Mosser b,V�eronique David b,m, Sylvie Odent b,f, Alain Verloes c, Christ�ele Dubourg b,m
a Laboratoire de Cytog�en�etique et Biologie Cellulaire, CHU Pontchaillou, Rennes, FrancebCNRS UMR 6061, IFR 140 GFAS, Facult�e de M�edecine, Universit�e de Rennes 1, FrancecD�epartement de G�en�etique, INSERM U676, CHU Robert Debr�e, APHP, Paris, Franced Service de G�en�etique M�edicale, CHBA, Vannes, Francee Laboratoire de Cytog�en�etique, CHU Jean Verdier, SMBH, Paris XIII, U676 Gressens, Bondy, APHP, Francef Service de G�en�etique M�edicale, CHU Hôpital Sud, Rennes, Franceg Service de G�en�etique, CHU Angers, Angers, Franceh Service de G�en�etique, CHU Bretonneau, Tours, Francei Service de G�en�etique et d'Embryologie M�edicales, CHU Armand Trousseau, Paris, APHP, Francej Service de G�en�etique M�edicale, CHU Poitiers, Poitiers, Francek Service de G�en�etique, CH Le Mans, Le Mans, Francel Service de G�en�etique M�edicale, Institut de Biologie, CHU Hôtel Dieu, Nantes, Francem Laboratoire de G�en�etique Mol�eculaire, CHU Pontchaillou, Rennes, France
a r t i c l e i n f o
Article history:Received 14 April 2009Accepted 17 October 2009Available online 28 October 2009
Keywords:Array-CGHNovel syndromesMicrodeletionMental retardation
* Corresponding author. Laboratoire de Cytog�en�etiqPontchaillou, 2 rue Henri Le Guilloux, Rennes, France
E-mail address: [email protected] (S. Ja
1769-7212/$ e see front matter � 2009 Elsevier Masdoi:10.1016/j.ejmg.2009.10.002
a b s t r a c t
Array-CGH has revealed a large number of copy number variations (CNVs) in patients with multiplecongenital anomalies and/or mental retardation (MCA/MR). According to criteria recently listed,pathogenicity was clearly suspected for some CNVs but benign CNVs, considered as polymorphisms, havecomplicated the interpretation of the results. In this study, genomic DNAs from 132 French patients withunexplained mental retardation were analysed by genome wide high-resolution Agilent� 44K oligonu-cleotide arrays. The results were in accordance with those observed in previous studies: the detectionrate of pathogenic CNVs was 14.4%. A non-random involvement of several chromosomal regions wasobserved. Some of the microimbalances recurrently involved regions (1q21.1, 2q23.1, 2q32q33, 7p13,17p13.3, 17p11.2, 17q21.31) corresponding to known or novel syndromes. For all the pathogenic CNVs,further cases are needed to allow more accurate genotypeephenotype correlations underscoring theimportance of databases to group patients with similar molecular data.
� 2009 Elsevier Masson SAS. All rights reserved.
1. Introduction
From the observation that subtelomeric anomalies can be foundin about 5% of MCA/MR patients [22], it was suspected that smallinterstitial imbalances may also be an important cause of MCA/MR[46,65] that is underestimated by current cytogenetics methods(conventional and molecular cytogenetics). Whole-genome array-based technologies have became an essential tool for the detection
ue et Biologie Cellulaire, CHU. Tel.: þ33 2 99 28 43 89.illard).
son SAS. All rights reserved.
of microimbalances and have identified such aberrations in 10e15%of MCA/MR patients with normal karyotype [17,20,21,23,24,29,40,41,45,46,54,59,65,66]. The challenge now is to describe novelsyndromes which can be achieved by comparing patients carryingthe same subtle rearrangement. Array-CGH can give an accuratedelineation of the imbalances which raises the possibility ofmaking genotypeephenotype correlations, in order to identifyminimal critical regions and candidate genes for a pattern of clinicalfeatures including learning disability. Fine mapping of genomicimbalances may indeed be useful to narrow down regions sus-pected to contain dosage sensitive genes critical for normaldevelopment [35].

S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e75 67
2. Materials and methods
2.1. Patients
Subjects with unexplained mental retardation were selected byclinical geneticists according to criteria derived from the checklist ofde Vries et al. [18], which is linked with a higher likelihood ofmanifesting submicroscopic copy number changes, particularly,subtelomeric imbalances. Criteria for the present study corres-ponded to mental retardation with at least one associated criterion(familial history of mental retardation, growth abnormalities, facialdysmorphic features, congenital malformations, seizures andbehavorial or sleeping disabilities). All patients hadnormal standardand/or high-resolution karyotyping and normal fragile X testing.Patientswere excluded from the study in case of identified aetiologyof mental retardation, abnormal karyotype and microdeletionsyndrome. Subtelomeric imbalanceswere excludedbysubtelomericFISH using the ToTel Vysion probes (Abbott Molecular Inc., DownersGrove, Illinois, USA) or by Multiplex Ligation-Dependant ProbeAmplification (MLPA) using the Salsa� MLPA� P036B and P070 kits(MRC-Holland b.v, Amsterdam, The Netherlands). Of the 132patients, 64were recruited at genetics clinical centers in theWest ofFrance (HUGO, Hôpitaux Universitaires du Grand Ouest) and 68were recruited at genetics clinical centers in Paris.
Informed consent for genetic investigations on mental retar-dation was obtained from participating families. Detailed clinicalhistory was obtained and physical examination was carried out forthe 132 patients.
2.2. Array-CGH
Oligonucleotide array-CGH was performed using the AgilentHuman Genome CGH microarray 44K (Agilent Technologies, SantaClara, CA, USA). These microarrays are constituted of more than44,000 60-mer oligonucleotide probes that span both coding andnon-coding regions, with emphasis on well-characterized genesrepresented by at least 1 probe and cancer-relevant genes by atleast 2 probes (more than 30,000 genes represented). Coverage ofthe human genome is made with an average spatial resolution of35 kb. The experiments were performed according to version 4.0(June 2006) of the protocol provided by Agilent (Agilent Oligo-nucleotide Array-Based CGH for Genomic DNA Analysis).Reference gDNA was from single male or female, in order tobetter characterize the copy number polymorphisms (CNPs).Microarrays were scanned using the Agilent scanner G2565BA.Images were analysed using Agilent Feature Extraction Softwareversion 9.1 (CGH-v4_91 protocol), permitting creation of QCreports for each patient where the value of the Derivative LogRatio Spread (DLRS), which is the spread of the derivative logratio values, was used as a quality criterion. A graphical overviewand analysis of the data were obtained by using the Agilent CGHanalytics software version 3.4.27 (statistical algorithm: z-score,sensitivity threshold: 2.5, moving average window: 5 points).Only imbalances involving three or more adjacent probes wereretained and further evaluated, based on previous assessmentsthat with this platform, the majority of the single and double-probe alterations observed are likely to be false-positive calls [21].Identification of probes with a significant gain or loss was basedon the log2 ratio plot deviation from 0 with cut-off values of0.5e1 and �0.5 to �1 respectively.
The validation method was chosen depending on the imba-lance type (deletion or duplication) and size, and on practicalreasons (type of sample available: DNA and/or metaphasespreads).
2.3. Multiplex PCR/liquid chromatography (MPLC)
Duplex PCR was designed, associating unlabeled primers for anendogenous control gene, HMBS, and for the region showingimbalance in the tested patient. This enables their simultaneousamplification under semi-quantitative conditions. Primers weredesigned using Primer Premier Software (Premier Biosoft Interna-tional, Palo Alto, CA, USA). Duplex PCR for normal control, eachpatient and parents gDNAs was performed as described elsewhere[5,19,26]. Data analysis was performed using the Navigator� Soft-ware (Transgenomic, Omaha, NE, USA), normalisationwas achievedwith HMBS peak and relative peak intensities for each amplicondirectly reflected genomic copy number.
2.4. Quantitative PCR
Real-time quantitative PCR (qPCR) was carried out on an ABIprism 7700 (Applied Biosystems, Foster City, CA, USA) with the useof fluorescent SYBR Green dye. Gene-specific primers for targetgenes and endogenous control genes (PLAGL1 and SDC4) weredesigned using Primer Express Software (Applied Biosystems,Foster City, CA, USA). Each sample was run in duplicate for thequantification of the target genes as compared to the endogenouscontrol genes. Data evaluation was carried out using the ABI PrismSequence Detection System (Applied Biosystems, Foster City, CA,USA) and Microsoft Excel, using the comparative DD thresholdcycle number (Ct) method.
2.5. Fluorescence in situ hybridization (FISH)
Clones mapping to the unbalanced regions were selected onpublic databases UCSC Genome Browser and Ensembl HumanGenome Browser. Clones were obtained for the RP11 library fromthe BACPAC Resource Center (Children's Hospital Oakland ResearchInstitute, Oakland, CA, USA), from Dr Mariano Rocchi (CytogeneticsDepartment, Institute of Genetics, Bari University, Italia), from DrJoris Andrieux (Genetics Department, Lille University Hospital,France), from the Wellcome Trust Sanger Institute and for the CTDlibrary from Invitrogen Corporation (Invitrogen�, Carlsbad, USA).The clones available for this study are listed in Table 1. DNAs werelabelled by random priming using the Bioprime� Array CGHGenomic Labeling System (Invitrogen�, Carlsbad, USA) or by nicktranslation using the Nick Translation Kit Vysis� (Abbott MolecularInc., Downers Grove, IL, USA). Probeswere hybridized tometaphaseslides obtained from phytohaemaglutinin-stimulated peripheralblood lymphocyte cultures for patients and parents. Slides wereanalysed with an epifluorescent microscope Olympus BX61 andimages were captured using Isis� software (MetaSystems, Altlus-sheim, Germany). FISH signals were examined both on metaphasechromosomes and interphase nuclei.
2.6. Multiplex ligation-dependant probe amplification (MLPA)
The Salsa�MLPA� kits P036B and P070 “human telomeres” fromMRC Holland were used concomitantly to detect deletions or gainsin subtelomeric regions and for the acrocentric chromosomes in thesubcentromeric region, according to the MLPA DNA detection andquantification protocol from MRC-Holland.
3. Results
Criteria of pathogenicity established by Lee et al. [31] wereused to determine clinical relevance of the CNVs observed.According to Lee et al. CNVs are more likely to be pathogenic ifcorrespond to one of the following criteria i.e. they are de novo,

Table 1Clinical and molecular features of patients with pathogenic CNVs.
Patient Chromosomalimbalance
Clinical features Imbalanceminimal size (bp)
Imbalancestart (bp)
Imbalanceend (bp)
Validation Method Origin Known syndrome orcandidate gene associated
P1 del(1)(q21.1q21.1)12 genes
Mental retardation, facial dysmorphism, post-natal growth retardation,extremity abnormalities, cerebellar vermis hypoplasia, atrial septaldefect, multi-cystic renal dysplasia
983,507 143,866,417 144,849,923 FISH (RP11-337C18,RP11e533N14,RP11-102F23)
maternal 1q21.1 microdeletion andmicroduplication [11,38]
P2 dup(2)(p16.1 p13.2)86 genes
Severe mental retardation, post-natal growth retardation,macrocephaly, epilepsy, aortic coarctation, facial dysmorphism, PierreRobin sequence
14,879,510 57,443,108 72,322,617 FISH (RP11-81L7,RP11-728F15,RP11-564H1)
de novo
P3 del(2)(q23.1q23.1)2 genes
Severe mental retardation, language impairment, inappropriatelaughter, post-natal growth retardation, microcephaly, epilepsy, largemouth, ataxia, valgus feet, micropenis
257,300 149,061,980 149,319,279 FISH (RP11-659J19) de novo 2q23.1 microdeletion [26]
P4 del(2)(q22.3q23.1)4 genes
Severe mental retardation, language impairment, inappropriatelaughter, autistic behaviour, aggressivity, sleeping difficulties,post-natal growth retardation, relative microcephaly, epilepsy, ataxia,feeding difficulties, facial dysmorphism, clinodactyly of the fifth finger,hypogenitalism
2,520,605 146,841,970 149,362,575 FISH (RP11-95O9,RP11-107E5,RP11-548K13,RP11-515K12,RP11-341F20,RP11-72H23)
de novo 2q23.1 microdeletion [26]
P5 del(2)(q31.2q33.1)128 genes
Severe mental retardation, post-natal growth retardation, ectodermaldysplasia (hair and teeth involvement)
26,090,717 176,637,788 202,728,505 FISH (RP11e91M5) de novo 2q33.1deletion syndrome[61]
P6 dup(3)(p14.3p14.3)10 genes
Mild to severe mental retardation, cerebellar vermis hypoplasia,anterior pachygyria, hypoplasia of the corpus callosum, facialdysmorphism, bilateral inguinal hernia, feet and legs distortion
1,056,177 56,305,073 57,361,250 qPCR de novo
P7 del(3)(q13.31q21.3)87 genes
Severe mental retardation, facial dysmorphism, hypotonia, agenesis ofthe corpus callosum, colic stenosis, genitalia abnormalities, jointstiffness
13,007,667 115,508,275 128,515,941 FISH (RP11-153K19,RP11-324H4,RP11-322C21,RP11-689D3)
NS
P8 del(3)(q26.33 q27.1)14 genes
Severe mental retardation, anophtalmia, agenesis of the corpuscallosum, post-natal growth retardation, microcephaly, coarse facies,epilepsy, hypotonia
3,788,389 180,966,165 184,754,554 FISH (RP11-43F17) de novo SOX2 deletion [36]
P9 del(5)(q14.3q14.3)1 gene
Severe mental retardation, hypotonia, epilepsy, craniofacial anomalies,stereotypic movements
216,432 88,051,970 88,268,402 MPLC and FISH (CTD-2328P23, RP11-1147F22, RP11-110I3)
de novo
P10 del(7)(p14.1 p13)50 genes
Severe mental retardation, hypotonia, bifid thumbs, feeding difficulties,renal abnormalities (bilateral renal hypoplasia, mega ureter,vesicoureteral reflux, renal insufficiency), cutis laxa, facialdysmorphism, cerebral atrophy
6,858,388 37,663,445 44,521,833 FISH (RP11e52M17) de novo Greig syndrome [7,47]
P11 del(10)(q24.32q24.32)10 genes
Severe mental retardation, autistic behaviour, hypotonia, macrocephaly,cerebellar vermis agenesis, partial sight
417,162 104,251,636 104,668,797 MPLC de novo
P12 dup(17)(p13.3p13.3)9 genes
Severe mental retardation, language impairment, epilepsy, facialdysmorphism, vaginal duplication
438,618 1,059,852 1498,470 FISH (RP11-818O24) NS Embedded in theMillereDieker syndromecritical region [13]
P13 del(17)(p11.2p11.2)18 genes
Moderate mental retardation, clinical features of Myhre syndrome 1,452,783 18,709,504 20,162,287 FISH (RP11-369K5) NS Embedded in the Smith-Magenis syndromecritical region
P14 del(17)(q21.31q21.31)6 genes
Moderate mental retardation, low birthweight, feeding problems,epilepsy, microcephaly, facial dysmorphism, atrial septal defect,ventricular septal defect, deafness, hypotonia, joint laxity, bilateralinguinal hernia
493,113 41,073,486 41,566,599 FISH (RP11-669E14) de novo 17q21.31 microdeletion[28,49,53]
P15 del(17)(q21.31q21.31)6 genes
Mental retardation, neonatal hypotonia, epilepsy, hypoplasia of thecorpus callosum, neuronal heterotopia, facial dysmorphism,cryptorchidism, hypermetropia
442,195 41,073,486 41,515,681 FISH (RP11-669E14) de novo 17q21.31 microdeletion[28,49,53]
P16 dup(18)(q21.2pter) anddel(18)(q21.2qter)
Mental retardation, hypoplasia of the corpus callosum, epilepsy, auralatresia, genitalia abnormalities, hypotonia, facial dysmorphism, ptosis,trigonocephaly
Borderlineprobe:51,501,43251,501,491
FISH (D18Z1) de novo
S.Jaillardet
al./European
Journalof
Medical
Genetics
53(2010)
66e75
68

P17
dup(22)(q11
.1q1
1.21
)5ge
nes
Seve
remen
talretardation,b
ehav
iouraldifficu
lties,post-natal
grow
thretardation,h
ypop
lasiaof
theco
rpuscallo
sum,e
pile
psy,h
ypoton
ia,
jointlaxity
267,45
016
,324
,514
16,591
,964
FISH
(RP1
1-15
0P15
)MLP
A(P03
6Bkit)
maternal
Embe
dded
intheCat
eye
syndromecritical
region
[37]
P18
dup(X
)(p22
.11p
22.11)
2ge
nes
Mod
erate-mild
men
talretardation,m
icrocephaly,
facial
dysmorphism,
cryp
torchidism,shortfinge
rswithsyndactylie
s,sh
ortan
dhollow
feet
468,00
921
,810
,551
22,278
,560
qPCR
maternal
P19
dup(X
)(p22
.11p
22.11)
2ge
nes
Mod
erate-mild
men
talretardation,m
icrocephaly,
facial
dysmorphism,
weigh
tþ2
SD,shortfinge
rsan
dfeet,clubfeet,leftfoot
syndactyly
II-III
468,00
921
,810
,551
22,278
,560
qPCR
maternal
Map
positionsreferto
theGen
omeAssem
blyMay
2004
hg1
7.Th
eva
lidationmethod
usedwas
either
multiplexPC
R/liquid
chromatog
raphy(M
PLC),fluorescence
insitu
hyb
ridization(FISH),multiplexlig
ation-dep
endan
tprobe
amplifi
cation
(MLP
A)or
quan
titative
PCR(qPC
R).Th
emethod
chosen
dep
endingon
theim
balance
typean
dsize
,andon
practical
reason
s.Th
enumbe
rof
genes
concern
edby
theCNVswas
evaluated
usingtheUCSC
datab
ase(U
CSC
Gen
omebrow
ser,hg1
7,RefSe
qge
nes).
NS:
not
studied.
S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e75 69
they are inherited from an affected parent or observed in anaffected relative, they do not overlap a polymorphism listed ina CNV database for healthy individuals but overlap a genomicimbalance in a CNV database for affected individuals, they containmorbid OMIM genes or are gene rich. Other characteristics includethe nature of the imbalance (deletion rather than duplication), thesize (>3 Mb) and the existence of regulatory elements. De novooccurrence or inheritance from a healthy parent is one of the mainpoints guiding toward pathogenic or benign characteristic ofa CNV respectively.
For the 132 patients studied, 193 CNVs were observed. Imba-lances corresponding to CNVs listed in the Database of GenomicVariants, either completely or partially overlapping, and imba-lances not listed in this database but showing redundancy in atleast two phenotypically different patients were considered ascopy number polymorphisms (CNPs). This corresponds to 166variations, with an average of 1.25 CNPs per patient, ranging fromw17-kb to w29-Mb in size for the deletions (average: 141,07-kbwithout the largest 29-Mb polymorphism in the chromosome 9pericentromeric regions [67]), and from w10,5-kb to w1,46-Mbfor the duplications (average: 168,91-kb). These data are inaccordance with the results reported using the same platform [21].These imbalances were not further studied by a validationmethod.
The 27 remaining CNVs were classified to prioritize those whichare most likely to be pathogenic for further study i.e. validation andparental studies. CNVs not listed in the database of genomicvariants and not yet described as pathogenic in a database foraffected individuals were supposed to be pathogenic. The nature,size, gene content of the CNVs were variable and priority wastherefore given to the CNVs with most of the criteria in favour ofpathogenicity. Validation and parental studies were first consid-ered for 25 patients. Parental studies were possible for 22 of these25 patients, showing de novo occurrence in 12 cases and familialsegregation in 10. In the 10 cases of inheritance from a phenotypi-cally normal parent (4 deletions fromw355 tow989-kb in size and6 duplications from w262 to w601-kb in size), absence of clinicalrelevance was assumed, except for inherited CNVs concerning Xchromosome (P18 and P19) and particular regions like the 22q11region (P17) and the 1q21.1 region (P1), where imbalances areassociated with familial segregation and variable clinical features[37,38]. When inheritance could not be established due to the lackof parental sample (P7, P12 and P13), pathogenicity could besupposed based on the gene content, the imbalance size and thegenomic region involved. Finally, 19 clinically relevant CNVs wereidentified in 19 patients (Fig.1): 12 deletions ranging fromw216-kbto w26-Mb in size (average: 4,71-Mb) and 6 duplications rangingfromw267-kb tow14,8-Mb in size (average: 2,93-Mb). In cases P2,P5 and P7, imbalanceswere larger than 10-Mb and should be visibleon conventional karyotype. The last case was patient P16 who wassuspected to have a mosaic chromosome 18 abnormality in about30e40% of the cells based on the level of the log2 ratio observed inarray-CGH. FISH using a chromosome 18 centromeric probeconfirmed the presence of an isodicentric chromosome 18 [idic(18)(q21.2)] but only in 5% of the cells. Table 1 summarizes molecularand clinical features of the patients carrying a pathogenicimbalance.
Finally, studies are still underway to determine the clinicalrelevance of 2 CNVs (2 imbalances in 2 patients, listed in Addi-tional file). These are not known as polymorphism but they aresuspected to be benign because of the small size, duplication typeand poor gene content and/or involvement of apparently non-morbid genes. These imbalances stress the difficulty to concludeabout the clinical relevance of some CNVs in the clinical settingand clinical diagnosis.

Fig. 1. Pathogenic genomic imbalances array-CGH profiles. Corresponding patients are indicated below each profile. The value of zero represents equal fluorescence intensity ratiobetween sample and reference gDNA. Copy number losses shift the ratio to the left and copy number gains to the right.
S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e7570

S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e75 71
4. Discussion
Our study further demonstrates the efficiency of whole-genomehigh-resolution array in the detection of chromosomal micro-imbalances. Out of the 132 patients with MCA/MR of unknownaetiology studied using genomewide array-CGH, 19 imbalancesinterpreted as pathogenic were identified (detection rate: 14.4%).Several studies have previously used array-CGH to make genome-wide screening of patients with MCA/MR and normal karyotype.This approach identified pathogenic imbalances in 10e15% of thepatients (Table 2). Nevertheless, comparison of the detection ratesof pathogenic imbalances is influenced by preselection criteria ofthe patients [62]. Indeed it has been shown that clinical preselec-tion of the patients increase the detection rate of chromosomalrearrangements [17]. As expected, chromosomal imbalances aremore frequently observed in patients with mild to severe mentalretardation. As a consequence, Engels et al. [20] have proposed thatthe severity of mental retardation should be used as a scoringcriterion for clinical preselection of the patients to be tested byarray-CGH. However, there is a significant proportion of patientswith moderate mental retardation with such imbalances. Wepropose to include for array-CGH studies patients irrespective ofthe level of mental retardation, so as to offer a genetic diagnosis toa maximum of patients presenting MCA/MR.
Whole-genome 1-Mb resolution for copy number screening firstappeared sufficient and reliable to detect the majority of submi-croscopic anomalies related to MR [21,40]. Array-CGH, using DNAfrom uncultured cells, has also shown its efficiency for the detec-tion of low-level mosaicism, which could be missed by conven-tional cytogenetic analysis [3,14]. Higher density arrays are nowavailable and the question is to determine the optimal resolution toadopt for routine diagnosis which is a resolution that offersa reasonable number of CNVs to check and a reliable diagnosis.Higher density arrays reveal a greater frequency of smaller CNVsand it may not be possible to confirm and to determine the clinicalrelevance of all the CNVs observed in a clinical setting [21]. Toovercome this problem, the use of an appropriate cut-off of a DNAsize, depending on the platform and indicating a positive result fora CNV has been suggested [21]. Nevertheless, Aradhya et al. [1]showed that high-density oligonucleotide arrays were able toidentify twice as many pathogenic rearrangements as did the low-density BAC arrays which highlights the strength of high-resolution
Table 2Chromosomal imbalance detection rate using whole-genome array technology(terminal and/or interstitial imbalances).
Studies Type of array Number ofpatients inthe study
Pathogenicimbalancesdetection rate
Vissers et al., 2003 [65] -BACs 3.5 K 20 15%Shaw-Smith et al., 2004 [54] -BACs 3.5 K 50 14%Schoumans et al., 2005 [46] -BACs 2.6 K 41 9.8%Tyson et al., 2005 [59] -BACs (1 Mb and
3 Mb resolution)22 9e13%
De Vries et al., 2005 [17] -BACs 32 K 100 10%Krepischi-Santos et al., 2006 [29] -BACs 3.5 K 95 15.8%Rosenberg et al., 2006 [45] -BACs 3.5 K 81 16%Menten et al., 2006 [40] -BACs 3.5 K 140 13.6%Miyake et al., 2006 [41] -BACs 2.173 K 30 17%Aradhya et al., 2007 [1] -BACs 2.6 K 20 30%
-Oligo 44K 50%Engels et al., 2007 [20] -BACs 6 et 8 K 60 10%Fan et al., 2007 [21] -Oligo 44 K 100 15%Friedman et al., 2006 [23] -SNP 100 K 100 11%Lybaek et al., 2008 [35] -BACs 3.5 K 20 20%Wagenstaller et al., 2007 [66] -SNP 100 K 67 16%Hoyer et al., 2007 [24] -SNP 100 K 105 9.1%
genomic arrays in detecting small pathogenic chromosomalimbalances. High-resolution array-CGH and SNP-array screens haveshown that 20% of all detected imbalances were smaller than 1-Mb,strengthening the idea that high-density genomewide arrays willimprove the diagnostic yield [62] and should be performed forpatients with MCA/MR in routine diagnosis. Studies [1,21] haveshown that the 44K oligonucleotide platform appears suitable forthis purpose. Moreover, arrays with an increasing density of probesor BACs offer a more precise delineation of the rearrangements,allowing detailed genotypeephenotype correlations [17] and, bydetecting small pathogenic CNVs, allow the definition of minimalcritical regions and the identification of candidate genes fordevelopmental anomalies.
The first early studies showed that most of the microdeletionsandmicroduplications were scattered throughout the genome [40],but subsequently a non-random involvement of several chromo-somal regions was observed [21] and some recurrent rearrange-ments have been recently described, concerning 1q21.1 [11,38],1q41q42 [48], 2p15p16.1 [42], 9q22.3 [43], 15q13.3 [50], 15q24 [51],16p13.1 [60], 16p11.2p12.2 [2] and 17q21.31 [28,49,53] regions(reviewed in [55]). For some of these regions, both deletions andduplications were found and their occurrence is probably caused bythe Non Allelic Homologous Recombination (NAHR) mechanismdue to flanking Low Copy Repeats (LCRs). This approach, consistingin a “genotype-first” approach and a secondary characterization ofthe associated phenotypes, can be called “reverse phenotypics”[55]. As novel syndromes can be described on the basis of clinicaldescription of patients with the same subtle rearrangement,pathogenic imbalances identified in this study were compared tothose observed in previous studies and/or described as pathogenicin databases collecting molecular cytogenetics and clinical data ofaffected individuals: DECIPHER, BACH and ECARUCA. Thiscomparative analysis is a way to facilitate interpretation of array-CGH results, increasing the probability for a CNV to be pathogenic ifit is observed in patients with common clinical features. Concur-rently, a comparative analysis with the data listed in a database forhealthy individuals like the Database of Genomic Variants was usedto disregard CNVs observed both in affected and in normal indi-viduals, although caution should be exercised for CNVs reportedonly in a single individual as they could represent rare variants orfalse positives [31]. Those comparisons are part of the character-istics defined by Lee et al. [31] and a guide toward pathogenic orbenign CNVs. In these criteria, CNVs inherited from a healthy parentare considered as CNPs although additional mechanisms can not beruled out at this stage such as the involvement of an imprintedregion, incomplete penetrance or variable expressivity, a recessivemutation on the non-deleted allele, the presence of genetic andenvironmental modifiers or different breakpoints at a higherresolution level [31,40,45,54,62]. It is to note, concerning thesecriteria, that novel microdeletion and microduplication syndromes(1q21.1, 15q13.3, 16p13.1) can be inherited from a healthy parent,this data complicates the usual reasoning that leads to considerinherited imbalances from a normal parent as benign.
Pathogenic imbalances identified in this study are listed inTable 1. Some of them have been described elsewhere (1q21.1[11,38], 2q23.1 [26], 3q26q27 [36], 7p13 [7,47], 17p13.3 [13]) andfocus was made on others (Fig. 2).
4.1. De novo imbalances
A de novo 2q31.2q33.1 deletion was observed in patient P5presenting severe growth retardation, severe developmental delayand partial ectodermal dysplasia (hair and teeth involvement). Thisdeletion encompasses the 2q microdeletion reported in 4 patientsby Van Bugghenhout et al. [61], who defined in 2005 the 2q32.2q33
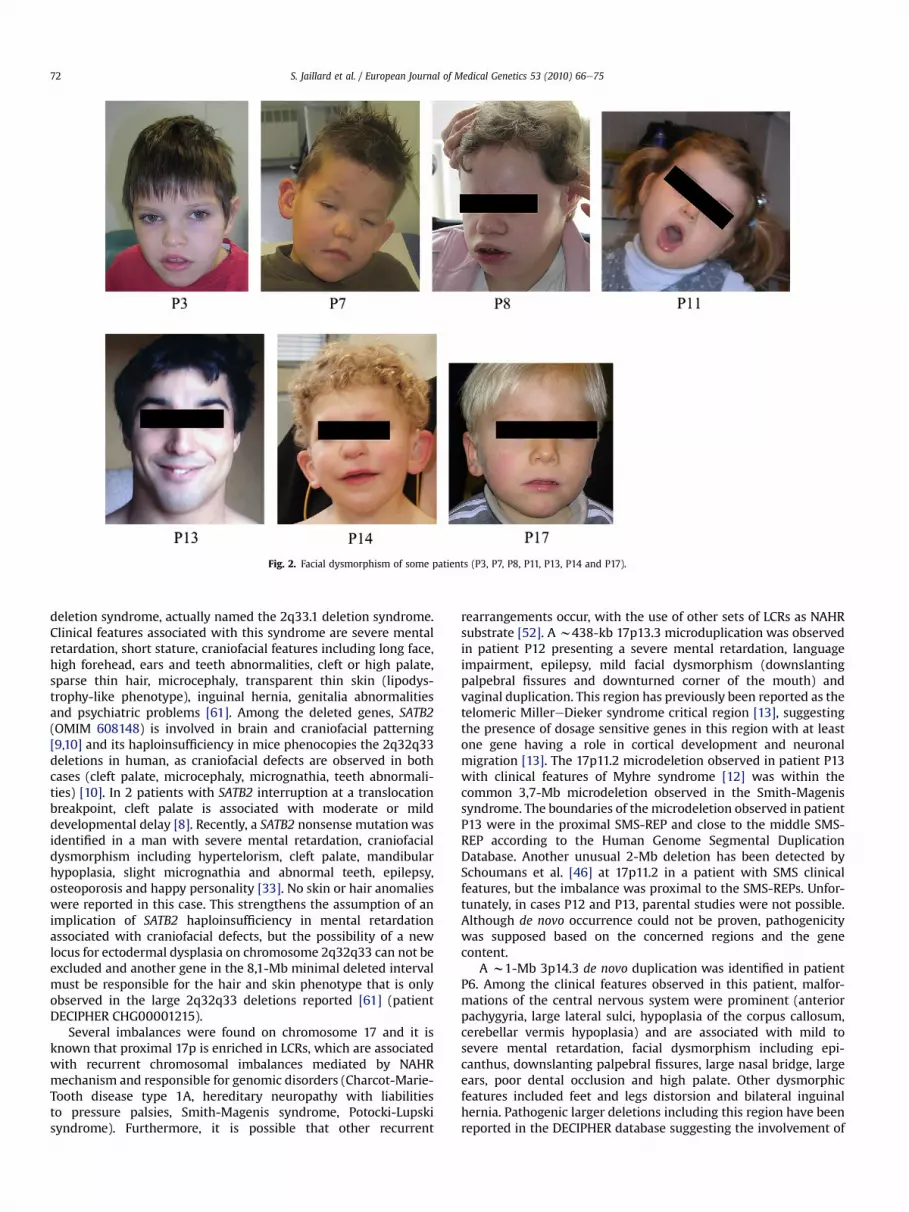
Fig. 2. Facial dysmorphism of some patients (P3, P7, P8, P11, P13, P14 and P17).
S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e7572
deletion syndrome, actually named the 2q33.1 deletion syndrome.Clinical features associated with this syndrome are severe mentalretardation, short stature, craniofacial features including long face,high forehead, ears and teeth abnormalities, cleft or high palate,sparse thin hair, microcephaly, transparent thin skin (lipodys-trophy-like phenotype), inguinal hernia, genitalia abnormalitiesand psychiatric problems [61]. Among the deleted genes, SATB2(OMIM 608148) is involved in brain and craniofacial patterning[9,10] and its haploinsufficiency in mice phenocopies the 2q32q33deletions in human, as craniofacial defects are observed in bothcases (cleft palate, microcephaly, micrognathia, teeth abnormali-ties) [10]. In 2 patients with SATB2 interruption at a translocationbreakpoint, cleft palate is associated with moderate or milddevelopmental delay [8]. Recently, a SATB2 nonsense mutation wasidentified in a man with severe mental retardation, craniofacialdysmorphism including hypertelorism, cleft palate, mandibularhypoplasia, slight micrognathia and abnormal teeth, epilepsy,osteoporosis and happy personality [33]. No skin or hair anomalieswere reported in this case. This strengthens the assumption of animplication of SATB2 haploinsufficiency in mental retardationassociated with craniofacial defects, but the possibility of a newlocus for ectodermal dysplasia on chromosome 2q32q33 can not beexcluded and another gene in the 8,1-Mb minimal deleted intervalmust be responsible for the hair and skin phenotype that is onlyobserved in the large 2q32q33 deletions reported [61] (patientDECIPHER CHG00001215).
Several imbalances were found on chromosome 17 and it isknown that proximal 17p is enriched in LCRs, which are associatedwith recurrent chromosomal imbalances mediated by NAHRmechanism and responsible for genomic disorders (Charcot-Marie-Tooth disease type 1A, hereditary neuropathy with liabilitiesto pressure palsies, Smith-Magenis syndrome, Potocki-Lupskisyndrome). Furthermore, it is possible that other recurrent
rearrangements occur, with the use of other sets of LCRs as NAHRsubstrate [52]. A w438-kb 17p13.3 microduplication was observedin patient P12 presenting a severe mental retardation, languageimpairment, epilepsy, mild facial dysmorphism (downslantingpalpebral fissures and downturned corner of the mouth) andvaginal duplication. This region has previously been reported as thetelomeric MillereDieker syndrome critical region [13], suggestingthe presence of dosage sensitive genes in this region with at leastone gene having a role in cortical development and neuronalmigration [13]. The 17p11.2 microdeletion observed in patient P13with clinical features of Myhre syndrome [12] was within thecommon 3,7-Mb microdeletion observed in the Smith-Magenissyndrome. The boundaries of the microdeletion observed in patientP13 were in the proximal SMS-REP and close to the middle SMS-REP according to the Human Genome Segmental DuplicationDatabase. Another unusual 2-Mb deletion has been detected bySchoumans et al. [46] at 17p11.2 in a patient with SMS clinicalfeatures, but the imbalance was proximal to the SMS-REPs. Unfor-tunately, in cases P12 and P13, parental studies were not possible.Although de novo occurrence could not be proven, pathogenicitywas supposed based on the concerned regions and the genecontent.
A w1-Mb 3p14.3 de novo duplication was identified in patientP6. Among the clinical features observed in this patient, malfor-mations of the central nervous system were prominent (anteriorpachygyria, large lateral sulci, hypoplasia of the corpus callosum,cerebellar vermis hypoplasia) and are associated with mild tosevere mental retardation, facial dysmorphism including epi-canthus, downslanting palpebral fissures, large nasal bridge, largeears, poor dental occlusion and high palate. Other dysmorphicfeatures included feet and legs distorsion and bilateral inguinalhernia. Pathogenic larger deletions including this region have beenreported in the DECIPHER database suggesting the involvement of

S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e75 73
dosage sensitive genes. Among the genes implicated in bothimbalances, HESX1 (OMIM 601802) is essential for forebrain andpituitary gland development and heterozygous mutations area cause of septo-optic dysplasia (SOD) [16] where agenesis orhypoplasia of midline brain structures is a common feature.
A small de novo 5q14.3 microdeletion (216,432-kb) includingonly one gene (MEF2C) was observed in patient P9 with severemental retardation, craniofacial anomalies and epilepsy. MEF2C(OMIM 600662) encodes an MEF2 family transcription factor,suspected to be an essential regulator of craniofacial development[63] and implicated in hippocampal dependent learning andmemory [4]. Larger deletions, including 5q14.3, have beenreported in patients with mental retardation and variable addi-tional features [24] (patients DECIPHER 00000135, DECIPHER00000596, ECARUCA 4521). Recently, Le Meur et al. published on6 patients with 5q14.3 imbalances (5 deletions and 1 duplication)and severe mental retardation with stereotypic movements,epilepsy and/or cerebral malformations (patient P9 is reported indetail in the study of Le Meur et al.). The role of MEF2C hap-loinsufficiency in a developmental phenotype have beenstrengthened by the identification of a de novo point mutation inthis gene resulting in a premature stop codon in a patient withsimilar clinical features [30].
A de novo 10q24.32 was identified in a 7 year old girl (P11) withsevere mental retardation, autistic behaviour, macrocephaly,hypotonia, cerebellar vermis agenesis and partial sight. This dele-tion includes the Suppressor of fused (SUFU) gene (OMIM 607035),encoding an intracellular negative regulator of the Sonic Hedgehog(SHH) pathway [57], and 9 other genes according to the UCSCdatabase. It is well known that dysregulation of the SHH pathwayleads to birth defects and cancers [64]. In mouse, homozygous lossof sufu is associated with embryonic lethality and developmentaldefects but SUFU haploinsufficiency do confer neither develop-mental phenotype nor tumor predisposition [15,32]. Taylor et al.[58] have shown that SUFU acts as a tumor-suppressor gene ina subset of desmoplastic medulloblastomas. Among the patientsshowing loss of heterozygosity for SUFU in the tumor, two patientshad a germline SUFU point mutation with no developmentalabnormalities while one patient (patient 1), with Nevoid Basal CellCarcinoma Syndrome-like phenotype associated with develop-mental delay, had a germline deletion of 28 contiguous genes,including SUFU. A 10q contiguous genes deletion including SUFU,rather than SUFU haploinsufficiency alone, could be responsible forthe developmental phenotype observed in Taylor et al.'s patient 1and in our study's patient P11, presenting with no tumoral history.
4.2. Inherited imbalances
Some imbalances although inherited from a phenotypicallynormal parent are nevertheless supposed to be pathogenic inchildren. Frequent situations are autosomal imbalances of animprinted region inherited from a normal parent and X-linkedimbalances inherited from a healthy mother with skewed X inac-tivation [62]. Nevertheless, X imbalances can be considered aspathogenic in male probands but for the female probands, imba-lances also observed in unaffected mothers are less convincing [1].Furthermore, it has been shown that a chromosomal anomaly mayhave a clinical significance even if it is inherited from a healthyparent [39]. For P18 and P19 patients (brothers), an Xp22.11duplication involving two genes (PHEX and ZNF645) was inheritedfrom a healthy mother. This duplication is possibly the cause of thesimilar phenotype in the brothers that includes mild mentalretardation, facial dysmorphism (short upslanting palpebralfissures, strabismus, epicanthus, low-set ears, nasal alae hypoplasia,smooth philtrum, thin upper lip) and extremity anomalies. PHEX
(OMIM 300550) mutations, leading to haploinsufficiency, areresponsible for X-linked dominant hypophosphatemic rickets [25].In the mouse model, the PHEX hyp-duk mutation is associated withdeafness, circling behaviour, and cranial dysmorphology [34]. It isnoteworthy that PHEX appears as a dosage sensitive genewhich canexert detrimental effects through absence/haploinsufficiency butalso through duplication/triplication.
Imbalances in particular chromosomal regions are also knownto be pathogenic, due to incomplete penetrance or variableexpressivity. The 22q11 genomic disorders are responsible for threemain syndromes with variable clinical features [37]. A 22q11duplication within the Cat Eye Syndrome (CES) critical region wasobserved in patient P17 and in his normal mother. Further familialstudies did not show this duplication in patient P17's half-brotherand half-sister. Pathogenicity of this imbalance remains unclearsince CES usually corresponds to a partial tetrasomy of the p-armand part of 22q11. Furthermore, patient P17 does not showcharacteristic clinical features usually reported in CES, includingiris coloboma, anal atresia and pre-auricular anomalies. Neverthe-less, interstitial 22q11 duplications have been described withclinical features of CES [27,44] and, due to the phenotypic vari-ability observed in this syndrome [6], we assume that the diagnosisof CES can not be ruled out for patient P17.
Several microrearrangements appear isolated and this empha-sizes the need to group cases for novel syndrome descriptions andgenotypeephenotype correlations. Best practice guidelines formolecular karyotyping are now available to help the implementa-tion of this technology in constitutional genetic diagnosis [62].Array CGH also represents a powerful tool in deciphering thegenomic basis of many novel microdeletion and microduplicationsyndromes. Conventional and molecular cytogenetics have showntheir complementarity and with the development of molecularkaryotyping, modern cytogenetics is decreasing the distinctionbetween cytological and molecular analysis [56]. Whole-genomehigher density arrays significantly increase the sensitivity of themethod but complicate the clinical interpretation of copy numbervariants of unclear significance.
Acknowledgements
This work was supported by grants from the CHU of Rennes(concours post-internat), PHRC inter-r�egional 2006 and DHOS(Direction de l'Hospitalisation et de l'Organisation des soins)“R�eseau de soutien pour le d�eveloppement dans les CHU deplateaux techniques mutualis�es de g�en�etique constitutionnellepour la d�etection de microremaniements chromosomiques”.
We are grateful to H. Beverley Osborne (UMR 6061, Rennes,France) for revising the English text.
Appendix. Supplementary material
Supplementary data associated with this article can be found inthe online version at doi:10.1016/j.ejmg.2009.10.002.
References
[1] S. Aradhya, M.A. Manning, A. Splendore, A.M. Cherry, Whole-genome array-CGH identifies novel contiguous gene deletions and duplications associatedwith developmental delay, mental retardation, and dysmorphic features. Am.J. Med. Genet. A 143A (2007) 1431e1441.
[2] B.C. Ballif, S.A. Hornor, E. Jenkins, S. Madan-Khetarpal, U. Surti, K.E. Jackson,A. Asamoah, P.L. Brock, G.C. Gowans, R.L. Conway, J.M. Graham Jr., L. Medne,E.H. Zackai, T.H. Shaikh, J. Geoghegan, R.R. Selzer, P.S. Eis, B.A. Bejjani, L.G. Shaffer,Discovery of a previously unrecognized microdeletion syndrome of16p11.2-p12.2. Nat. Genet. 39 (2007) 1071e1073.
[3] B.C. Ballif, E.A. Rorem, K. Sundin, M. Lincicum, S. Gaskin, J. Coppinger,C.D. Kashork, L.G. Shaffer, B.A. Bejjani, Detection of low-level mosaicism by

S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e7574
array CGH in routine diagnostic specimens. Am. J. Med. Genet. A 140 (2006)2757e2767.
[4] A.C. Barbosa, M.S. Kim, M. Ertunc, M. Adachi, E.D. Nelson, J. McAnally,J.A. Richardson, E.T. Kavalali, L.M. Monteggia, R. Bassel-Duby, E.N. Olson,MEF2C, a transcription factor that facilitates learning and memory by negativeregulation of synapse numbers and function. Proc. Natl. Acad. Sci. U S A 105(2008) 9391e9396.
[5] C. Bendavid, C. Dubourg, L. Pasquier, I. Gicquel, S. Le Gallou, S. Mottier,M.R. Durou, C. Henry, S. Odent, V. David, MLPA screening reveals novel sub-telomeric rearrangements in holoprosencephaly. Hum. Mutat. 28 (2007)1189e1197.
[6] M.J. Berends, G. Tan-Sindhunata, B. Leegte, A.J. van Essen, Phenotypic vari-ability of Cat-Eye syndrome. Genet. Couns. 12 (2001) 23e34.
[7] L.G. Biesecker, The Greig cephalopolysyndactyly syndrome. Orphanet J. RareDis. 3 (2008) 10.
[8] C.M. Brewer, J.P. Leek, A.J. Green, S. Holloway, D.T. Bonthron, A.F. Markham,D.R. FitzPatrick, A locus for isolated cleft palate, located on human chromo-some 2q32. Am. J. Hum. Genet. 65 (1999) 387e396.
[9] O. Britanova, S. Akopov, S. Lukyanov, P. Gruss, V. Tarabykin, Novel transcriptionfactor Satb2 interacts with matrix attachment region DNA elements ina tissue-specific manner and demonstrates cell-type-dependent expression inthe developing mouse CNS. Eur. J. Neurosci. 21 (2005) 658e668.
[10] O. Britanova, M.J. Depew, M. Schwark, B.L. Thomas, I. Miletich, P. Sharpe,V. Tarabykin, Satb2 haploinsufficiency phenocopies 2q32-q33 deletions,whereas loss suggests a fundamental role in the coordination of jaw devel-opment. Am. J. Hum. Genet. 79 (2006) 668e678.
[11] N. Brunetti-Pierri, J.S. Berg, F. Scaglia, J. Belmont, C.A. Bacino, T. Sahoo,S.R. Lalani, B. Graham, B. Lee, M. Shinawi, J. Shen, S.H. Kang, A. Pursley, T. Lotze,G. Kennedy, S. Lansky-Shafer, C. Weaver, E.R. Roeder, T.A. Grebe, G.L. Arnold,T. Hutchison, T. Reimschisel, S. Amato, M.T. Geragthy, J.W. Innis, E. Obersztyn,B. Nowakowska, S.S. Rosengren, P.I. Bader, D.K. Grange, S. Naqvi, A.D. Garnica,S.M. Bernes, C.T. Fong, A. Summers, W.D. Walters, J.R. Lupski, P. Stankiewicz,S.W. Cheung, A. Patel, Recurrent reciprocal 1q21.1 deletions and duplicationsassociated with microcephaly or macrocephaly and developmental andbehavioral abnormalities. Nat. Genet. 40 (2008) 1466e1471.
[12] L. Burglen, D. Heron, A. Moerman, A. Dieux-Coeslier, J.P. Bourguignon, A. Bachy,J.C. Carel, V. Cormier-Daire, S. Manouvrier, A. Verloes, Myhre syndrome: newreports, review, and differential diagnosis. J. Med. Genet. 40 (2003) 546e551.
[13] C. Cardoso, R.J. Leventer, H.L. Ward, K. Toyo-Oka, J. Chung, A. Gross, C.L. Martin,J. Allanson, D.T. Pilz, A.H. Olney, O.M. Mutchinick, S. Hirotsune, A. Wynshaw-Boris, W.B. Dobyns, D.H. Ledbetter, Refinement of a 400-kb critical regionallows genotypic differentiation between isolated lissencephaly, Miller-eDieker syndrome, and other phenotypes secondary to deletions of 17p13.3.Am. J. Hum. Genet. 72 (2003) 918e930.
[14] S.W. Cheung, C.A. Shaw, D.A. Scott, A. Patel, T. Sahoo, C.A. Bacino, A. Pursley,J. Li, R. Erickson, A.L. Gropman, D.T. Miller, M.R. Seashore, A.M. Summers,P. Stankiewicz, A.C. Chinault, J.R. Lupski, A.L. Beaudet, V.R. Sutton, Microarray-based CGH detects chromosomal mosaicism not revealed by conventionalcytogenetics. Am. J. Med. Genet. A 143 (2007) 1679e1686.
[15] A.F. Cooper, K.P. Yu, M. Brueckner, L.L. Brailey, L. Johnson, J.M. McGrath,A.E. Bale, Cardiac and CNS defects in a mouse with targeted disruption ofsuppressor of fused. Development 132 (2005) 4407e4417.
[16] M.T. Dattani, J.P. Martinez-Barbera, P.Q. Thomas, J.M. Brickman, R. Gupta,I.L. Martensson, H. Toresson, M. Fox, J.K. Wales, P.C. Hindmarsh, S. Krauss,R.S. Beddington, I.C. Robinson, Mutations in the homeobox gene HESX1/Hesx1associated with septo-optic dysplasia in human and mouse. Nat. Genet. 19(1998) 125e133.
[17] B.B. de Vries, R. Pfundt, M. Leisink, D.A. Koolen, L.E. Vissers, I.M. Janssen,S. Reijmersdal, W.M. Nillesen, E.H. Huys, N. Leeuw, D. Smeets, E.A. Sistermans,T. Feuth, C.M. van Ravenswaaij-Arts, A.G. van Kessel, E.F. Schoenmakers,H.G. Brunner, J.A. Veltman, Diagnostic genome profiling in mental retardation.Am. J. Hum. Genet. 77 (2005) 606e616.
[18] B.B. de Vries, S.M. White, S.J. Knight, R. Regan, T. Homfray, I.D. Young, M. Super,C. McKeown, M. Splitt, O.W. Quarrell, A.H. Trainer, M.F. Niermeijer, S. Malcolm,J. Flint, J.A. Hurst, R.M. Winter, Clinical studies on submicroscopic subtelomericrearrangements: a checklist. J. Med. Genet. 38 (2001) 145e150.
[19] C. Dehainault, A. Lauge, V. Caux-Moncoutier, S. Pages-Berhouet, F. Doz,L. Desjardins, J. Couturier, M. Gauthier-Villars, D. Stoppa-Lyonnet, C. Houdayer,Multiplex PCR/liquid chromatography assay for detection of gene rearrange-ments: application to RB1 gene. Nucleic Acids Res. 32 (2004) e139.
[20] H. Engels, A. Brockschmidt, A. Hoischen, C. Landwehr, K. Bosse, C. Walldorf,G. Toedt, B. Radlwimmer, P. Propping, P. Lichter, R.G. Weber, DNA microarrayanalysis identifies candidate regions and genes in unexplained mental retar-dation. Neurology 68 (2007) 743e750.
[21] Y.S. Fan, P. Jayakar, H. Zhu, D. Barbouth, S. Sacharow, A. Morales, V. Carver,P. Benke, P. Mundy, L.J. Elsas, Detection of pathogenic gene copy numbervariations in patients with mental retardation by genomewide oligonucleotidearray comparative genomic hybridization. Hum. Mutat. 28 (2007) 1124e1132.
[22] J. Flint, S. Knight, The use of telomere probes to investigate submicroscopicrearrangements associated with mental retardation. Curr. Opin. Genet. Dev. 13(2003) 310e316.
[23] J.M. Friedman, A. Baross, A.D. Delaney, A. Ally, L. Arbour, L. Armstrong, J. Asano,D.K. Bailey, S. Barber, P. Birch, M. Brown-John, M. Cao, S. Chan, D.L. Charest,N. Farnoud, N. Fernandes, S. Flibotte, A. Go, W.T. Gibson, R.A. Holt, S.J. Jones,G.C. Kennedy, M. Krzywinski, S. Langlois, H.I. Li, B.C. McGillivray, T. Nayar,
T.J. Pugh, E. Rajcan-Separovic, J.E. Schein, A. Schnerch, A. Siddiqui, M.I. VanAllen, G. Wilson, S.L. Yong, F. Zahir, P. Eydoux, M.A. Marra, Oligonucleotidemicroarray analysis of genomic imbalance in children with mental retarda-tion. Am. J. Hum. Genet. 79 (2006) 500e513.
[24] J. Hoyer, A. Dreweke, C. Becker, I. Gohring, C.T. Thiel, M.M. Peippo, R. Rauch,M. Hofbeck, U. Trautmann, C. Zweier, M. Zenker, U. Huffmeier, C. Kraus,A.B. Ekici, F. Ruschendorf, P. Nurnberg, A. Reis, A. Rauch, Molecular kar-yotyping in patients with mental retardation using 100K single-nucleotidepolymorphism arrays. J. Med. Genet. 44 (2007) 629e636.
[25] S. Ichikawa, E.A. Traxler, S.A. Estwick, L.R. Curry, M.L. Johnson, A.H. Sorenson,E.A. Imel, M.J. Econs, Mutational survey of the PHEX gene in patients withX-linked hypophosphatemic rickets. Bone 43 (2008) 663e666.
[26] S. Jaillard, C. Dubourg, M. Gerard-Blanluet, A. Delahaye, L. Pasquier, C. Dupont,C. Henry, A.C. Tabet, J. Lucas, A. Aboura, V. David, B. Benzacken, S. Odent,E. Pipiras, 2q23.1 microdeletion identified by array-CGH: an emergingphenotype with Angelman-like features? J. Med. Genet. (2008).
[27] J.H. Knoll, A. Asamoah, B.A. Pletcher, J. Wagstaff, Interstitial duplication ofproximal 22q: phenotypic overlap with cat eye syndrome. Am. J. Med. Genet.55 (1995) 221e224.
[28] D.A. Koolen, L.E. Vissers, R. Pfundt, N. de Leeuw, S.J. Knight, R. Regan, R.F. Kooy,E. Reyniers, C. Romano, M. Fichera, A. Schinzel, A. Baumer, B.M. Anderlid,J. Schoumans, N.V. Knoers, A.G. van Kessel, E.A. Sistermans, J.A. Veltman, H.G. Brunner, B.B. de Vries, A new chromosome 17q21.31 microdeletionsyndrome associated with a common inversion polymorphism. Nat. Genet. 38(2006) 999e1001.
[29] A.C. Krepischi-Santos, A.M. Vianna-Morgante, F.S. Jehee, M.R. Passos-Bueno,J. Knijnenburg, K. Szuhai, W. Sloos, J.F. Mazzeu, F. Kok, C. Cheroki, P.A. Otto,R.C. Mingroni-Netto, M. Varela, C. Koiffmann, C.A. Kim, D.R. Bertola,P.L. Pearson, C. Rosenberg, Whole-genome array-CGH screening in undiag-nosed syndromic patients: old syndromes revisited and new alterations.Cytogenet. Genome Res. 115 (2006) 254e261.
[30] N. Le Meur, M. Holder-Espinasse, S. Jaillard, A. Goldenberg, S. Joriot, P. Amati-Bonneau, A. Guichet, M. Barth, A. Charollais, H. Journel, S. Auvin, C. Boucher,J.-P. Kerckaert, V. David, S. Manouvrier-Hanu, P. Saugier-Veber, T. Fr�ebourg,C. Dubourg, J. Andrieux, D. Bonneau, MEF2C haploinsufficiency caused eitherby microdeletion of the 5q14.3 region or mutation is responsible for severemental retardation with stereotypic movements, epilepsy and/or cerebralmalformations, J. Med. Genet., in press.
[31] C. Lee, A.J. Iafrate, A.R. Brothman, Copy number variations and clinical cyto-genetic diagnosis of constitutional disorders. Nat. Genet. 39 (2007) S48eS54.
[32] Y. Lee, R. Kawagoe, K. Sasai, Y. Li, H.R. Russell, T. Curran, P.J. McKinnon, Loss ofsuppressor-of-fused function promotes tumorigenesis. Oncogene 26 (2007)6442e6447.
[33] P. Leoyklang, K. Suphapeetiporn, P. Siriwan, T. Desudchit, P. Chaowanapanja,W.A. Gahl, V. Shotelersuk, Heterozygous nonsense mutation SATB2 associatedwith cleft palate, osteoporosis, and cognitive defects. Hum. Mutat. 28 (2007)732e738.
[34] B. Lorenz-Depiereux, V.E. Guido, K.R. Johnson, Q.Y. Zheng, L.H. Gagnon,J.D. Bauschatz, M.T. Davisson, L.L. Washburn, L.R. Donahue, T.M. Strom,E.M. Eicher, New intragenic deletions in the Phex gene clarify X-linkedhypophosphatemia-related abnormalities in mice. Mamm. Genome 15 (2004)151e161.
[35] H. Lybaek, L.A. Meza-Zepeda, S.H. Kresse, T. Hoysaeter, V.M. Steen, G. Houge,Array-CGH fine mapping of minor and cryptic HR-CGH detected genomicimbalances in 80 out of 590 patients with abnormal development. Eur. J. Hum.Genet. 16 (2008) 1318e1328.
[36] A. Male, A. Davies, A. Bergbaum, J. Keeling, D. FitzPatrick, C. Mackie Ogilvie,J. Berg, Delineation of an estimated 6.7 MB candidate interval for an anoph-thalmia gene at 3q26.33-q28 and description of the syndrome associated withvisible chromosome deletions of this region. Eur. J. Hum. Genet. 10 (2002)807e812.
[37] H.E. McDermid, B.E. Morrow, Genomic disorders on 22q11. Am. J. Hum. Genet.70 (2002) 1077e1088.
[38] H.C. Mefford, A.J. Sharp, C. Baker, A. Itsara, Z. Jiang, K. Buysse, S. Huang,V.K. Maloney, J.A. Crolla, D. Baralle, A. Collins, C. Mercer, K. Norga, T. de Ravel,K. Devriendt, E.M. Bongers, N. de Leeuw, W. Reardon, S. Gimelli, F. Bena,R.C. Hennekam, A. Male, L. Gaunt, J. Clayton-Smith, I. Simonic, S.M. Park,S.G.Mehta, S. Nik-Zainal, C.G.Woods, H.V. Firth, G. Parkin,M. Fichera, S. Reitano,M. LoGiudice, K.E. Li, I. Casuga, A. Broomer, B. Conrad,M. Schwerzmann, L. Raber,S. Gallati, P. Striano, A. Coppola, J.L. Tolmie, E.S. Tobias, C. Lilley, L. Armengol,Y. Spysschaert, P. Verloo, A. De Coene, L. Goossens, G.Mortier, F. Speleman, E. vanBinsbergen, M.R. Nelen, R. Hochstenbach, M. Poot, L. Gallagher, M. Gill,J. McClellan, M.C. King, R. Regan, C. Skinner, R.E. Stevenson, S.E. Antonarakis,C. Chen, X. Estivill, B. Menten, G. Gimelli, S. Gribble, S. Schwartz, J.S. Sutcliffe,T.Walsh, S.J. Knight, J. Sebat, C. Romano, C.E. Schwartz, J.A. Veltman, B.B. deVries,J.R. Vermeesch, J.C. Barber, L. Willatt, M. Tassabehji, E.E. Eichler, Recurrentrearrangements of chromosome 1q21.1 and variable pediatric phenotypes.N. Engl. J. Med. 359 (2008) 1685e1699.
[39] M.A. Mencarelli, E. Katzaki, F.T. Papa, K. Sampieri, R. Caselli, V. Uliana,M. Pollazzon, R. Canitano, R. Mostardini, S. Grosso, I. Longo, F. Ariani, I. Meloni,J. Hayek, P. Balestri, F. Mari, A. Renieri, Private inherited microdeletion/microduplications: implications in clinical practice. Eur. J. Med. Genet. 51(2008) 409e416.
[40] B. Menten, N. Maas, B. Thienpont, K. Buysse, J. Vandesompele, C. Melotte, T. deRavel, S. Van Vooren, I. Balikova, L. Backx, S. Janssens, A. De Paepe, B. De Moor,

S. Jaillard et al. / European Journal of Medical Genetics 53 (2010) 66e75 75
Y. Moreau, P. Marynen, J.P. Fryns, G. Mortier, K. Devriendt, F. Speleman,J.R. Vermeesch, Emerging patterns of cryptic chromosomal imbalance inpatients with idiopathic mental retardation and multiple congenital anoma-lies: a new series of 140 patients and review of published reports. J. Med.Genet. 43 (2006) 625e633.
[41] N. Miyake, O. Shimokawa, N. Harada, N. Sosonkina, A. Okubo, H. Kawara,N. Okamoto, K. Kurosawa, H. Kawame, M. Iwakoshi, T. Kosho, Y. Fukushima,Y. Makita, Y. Yokoyama, T. Yamagata, M. Kato, Y. Hiraki, M. Nomura,K. Yoshiura, T. Kishino, T. Ohta, T. Mizuguchi, N. Niikawa, N. Matsumoto, BACarray CGH reveals genomic aberrations in idiopathic mental retardation. Am. J.Med. Genet. A 140 (2006) 205e211.
[42] E. Rajcan-Separovic, C. Harvard, X. Liu, B. McGillivray, J.G. Hall, Y. Qiao,J. Hurlburt, J. Hildebrand, E.C. Mickelson, J.J. Holden, M.E. Lewis, Clinical andmolecular cytogenetic characterisation of a newly recognised microdeletionsyndrome involving 2p15-16.1. J. Med. Genet. 44 (2007) 269e276.
[43] R. Redon, G. Baujat, D. Sanlaville, M. Le Merrer, M. Vekemans, A. Munnich,N.P. Carter, V. Cormier-Daire, L. Colleaux, Interstitial 9q22.3 microdeletion:clinical and molecular characterisation of a newly recognised overgrowthsyndrome. Eur. J. Hum. Genet. 14 (2006) 759e767.
[44] J.A. Reiss, R.G. Weleber, M.G. Brown, C.D. Bangs, E.W. Lovrien, R.E. Magenis,Tandem duplication of proximal 22q: a cause of cat-eye syndrome. Am. J. Med.Genet. 20 (1985) 165e171.
[45] C. Rosenberg, J. Knijnenburg, E. Bakker, A.M. Vianna-Morgante, W. Sloos,P.A. Otto, M. Kriek, K. Hansson, A.C. Krepischi-Santos, H. Fiegler, N.P. Carter,E.K. Bijlsma, A. van Haeringen, K. Szuhai, H.J. Tanke, Array-CGH detection ofmicro rearrangements in mentally retarded individuals: clinical significance ofimbalances present both in affected children and normal parents. J. Med.Genet. 43 (2006) 180e186.
[46] J. Schoumans, C. Ruivenkamp, E. Holmberg, M. Kyllerman, B.M. Anderlid,M. Nordenskjold, Detection of chromosomal imbalances in children withidiopathic mental retardation by array based comparative genomic hybrid-isation (array-CGH). J. Med. Genet. 42 (2005) 699e705.
[47] T. Schwarzbraun, C. Windpassinger, L. Ofner, J.B. Vincent, J. Cheung,S.W. Scherer, K. Wagner, P.M. Kroisel, E. Petek, Genomic analysis of fivechromosome 7p deletion patients with Greig cephalopolysyndactylysyndrome (GCPS). Eur. J. Med. Genet. 49 (2006) 338e345.
[48] L.G. Shaffer, A. Theisen, B.A. Bejjani, B.C. Ballif, A.S. Aylsworth, C. Lim,M. McDonald, J.W. Ellison, D. Kostiner, S. Saitta, T. Shaikh, The discovery ofmicrodeletion syndromes in the post-genomic era: review of the method-ology and characterization of a new 1q41q42 microdeletion syndrome. Genet.Med. 9 (2007) 607e616.
[49] A.J. Sharp, S. Hansen, R.R. Selzer, Z. Cheng, R. Regan, J.A. Hurst, H. Stewart,S.M. Price, E. Blair, R.C. Hennekam, C.A. Fitzpatrick, R. Segraves, T.A. Richmond,C. Guiver, D.G. Albertson, D. Pinkel, P.S. Eis, S. Schwartz, S.J. Knight, E.E. Eichler,Discovery of previously unidentified genomic disorders from the duplicationarchitecture of the human genome. Nat. Genet. 38 (2006) 1038e1042.
[50] A.J. Sharp, H.C. Mefford, K. Li, C. Baker, C. Skinner, R.E. Stevenson, R.J. Schroer,F. Novara, M. De Gregori, R. Ciccone, A. Broomer, I. Casuga, Y. Wang, C. Xiao,C. Barbacioru, G. Gimelli, B.D. Bernardina, C. Torniero, R. Giorda, R. Regan,V. Murday, S. Mansour, M. Fichera, L. Castiglia, P. Failla, M. Ventura, Z. Jiang,G.M. Cooper, S.J. Knight, C. Romano, O. Zuffardi, C. Chen, C.E. Schwartz,E.E. Eichler, A recurrent 15q13.3 microdeletion syndrome associated withmental retardation and seizures. Nat. Genet. 40 (2008) 322e328.
[51] A.J. Sharp, R.R. Selzer, J.A. Veltman, S. Gimelli, G. Gimelli, P. Striano,A. Coppola, R. Regan, S.M. Price, N.V. Knoers, P.S. Eis, H.G. Brunner, R.C. Hennekam, S.J. Knight, B.B. de Vries, O. Zuffardi, E.E. Eichler, Character-ization of a recurrent 15q24 microdeletion syndrome. Hum. Mol. Genet. 16(2007) 567e572.
[52] C.J. Shaw, M.A. Withers, J.R. Lupski, Uncommon deletions of theSmitheMagenis syndrome region can be recurrent when alternate low-copyrepeats act as homologous recombination substrates. Am. J. Hum. Genet. 75(2004) 75e81.
[53] C. Shaw-Smith, A.M. Pittman, L. Willatt, H. Martin, L. Rickman, S. Gribble,R. Curley, S. Cumming, C. Dunn, D. Kalaitzopoulos, K. Porter, E. Prigmore,A.C. Krepischi-Santos, M.C. Varela, C.P. Koiffmann, A.J. Lees, C. Rosenberg,H.V. Firth, R. de Silva, N.P. Carter, Microdeletion encompassing MAPT atchromosome 17q21.3 is associated with developmental delay and learningdisability. Nat. Genet. 38 (2006) 1032e1037.
[54] C. Shaw-Smith, R. Redon, L. Rickman, M. Rio, L. Willatt, H. Fiegler, H. Firth,D. Sanlaville, R. Winter, L. Colleaux, M. Bobrow, N.P. Carter, Microarraybased comparative genomic hybridisation (array-CGH) detects submicro-scopic chromosomal deletions and duplications in patients with learning
disability/mental retardation and dysmorphic features. J. Med. Genet. 41(2004) 241e248.
[55] A.M. Slavotinek, Novel microdeletion syndromes detected by chromosomemicroarrays. Hum. Genet. 124 (2008) 1e17.
[56] M.R. Speicher, N.P. Carter, The new cytogenetics: blurring the boundaries withmolecular biology. Nat. Rev. Genet. 6 (2005) 782e792.
[57] J. Svard, K. Heby-Henricson, M. Persson-Lek, B. Rozell, M. Lauth, A. Bergstrom,J. Ericson, R. Toftgard, S. Teglund, Genetic elimination of Suppressor of fusedreveals an essential repressor function in the mammalian Hedgehog signalingpathway. Dev. Cell. 10 (2006) 187e197.
[58] M.D. Taylor, L. Liu, C. Raffel, C.C. Hui, T.G. Mainprize, X. Zhang, R. Agatep,S. Chiappa, L. Gao, A. Lowrance, A. Hao, A.M. Goldstein, T. Stavrou, S.W. Scherer,W.T. Dura, B. Wainwright, J.A. Squire, J.T. Rutka, D. Hogg, Mutations in SUFUpredispose to medulloblastoma. Nat. Genet. 31 (2002) 306e310.
[59] C. Tyson, C. Harvard, R. Locker, J.M. Friedman, S. Langlois, M.E. Lewis, M. VanAllen, M. Somerville, L. Arbour, L. Clarke, B. McGilivray, S.L. Yong, J. Siegel-Bartel, E. Rajcan-Separovic, Submicroscopic deletions and duplications inindividuals with intellectual disability detected by array-CGH. Am. J. Med.Genet. A 139 (2005) 173e185.
[60] R. Ullmann, G. Turner, M. Kirchhoff, W. Chen, B. Tonge, C. Rosenberg, M. Field,A.M.Vianna-Morgante, L. Christie,A.C. Krepischi-Santos, L. Banna,A.V. Brereton,A. Hill, A.M. Bisgaard, I. Muller, C. Hultschig, F. Erdogan, G. Wieczorek,H.H. Ropers, Array CGH identifies reciprocal 16p13.1 duplications and deletionsthat predispose to autism and/or mental retardation. Hum. Mutat. 28 (2007)674e682.
[61] G. Van Buggenhout, C. Van Ravenswaaij-Arts, N. Mc Maas, R. Thoelen,A. Vogels, D. Smeets, I. Salden, G. Matthijs, J.P. Fryns, J.R. Vermeesch, The del(2)(q32.2q33) deletion syndrome defined by clinical and molecular character-ization of four patients. Eur. J. Med. Genet. 48 (2005) 276e289.
[62] J.R. Vermeesch, H. Fiegler, N. de Leeuw, K. Szuhai, J. Schoumans, R. Ciccone,F. Speleman, A. Rauch, J. Clayton-Smith, C. Van Ravenswaaij, D. Sanlaville,P.C. Patsalis, H. Firth, K. Devriendt, O. Zuffardi, Guidelines for molecular kar-yotyping in constitutional genetic diagnosis. Eur. J. Hum. Genet. 15 (2007)1105e1114.
[63] M.P. Verzi, P. Agarwal, C. Brown, D.J. McCulley, J.J. Schwarz, B.L. Black, Thetranscription factor MEF2C is required for craniofacial development. Dev. Cell.12 (2007) 645e652.
[64] E.H. Villavicencio, D.O. Walterhouse, P.M. Iannaccone, The sonic hedgehog-patched-gli pathway in human development and disease. Am. J. Hum. Genet.67 (2000) 1047e1054.
[65] L.E. Vissers, B.B. de Vries, K. Osoegawa, I.M. Janssen, T. Feuth, C.O. Choy,H. Straatman, W. van der Vliet, E.H. Huys, A. van Rijk, D. Smeets, C.M. vanRavenswaaij-Arts, N.V. Knoers, I. van der Burgt, P.J. de Jong, H.G. Brunner,A.G. van Kessel, E.F. Schoenmakers, J.A. Veltman, Array-based comparativegenomic hybridization for the genomewide detection of submicroscopicchromosomal abnormalities. Am. J. Hum. Genet. 73 (2003) 1261e1270.
[66] J. Wagenstaller, S. Spranger, B. Lorenz-Depiereux, B. Kazmierczak, M. Nathrath,D. Wahl, B. Heye, D. Glaser, V. Liebscher, T. Meitinger, T.M. Strom, Copy-number variations measured by single-nucleotide-polymorphism oligonu-cleotide arrays in patients with mental retardation. Am. J. Hum. Genet. 81(2007) 768e779.
[67] L.R. Willatt, J.C. Barber, A. Clarkson, I. Simonic, F.L. Raymond, Z. Docherty,C.M. Ogilvie, Novel deletion variants of 9q13-q21.12 and classical euchromaticvariants of 9q12/qh involve deletion, duplication and triplication of largetracts of segmentally duplicated pericentromeric euchromatin. Eur. J. Hum.Genet. 15 (2007) 45e52.
Internet resources
UCSC Genome Browser http://genome.ucsc.edu/.Ensembl Human Genome Browser http://ensembl.org.BACPAC Resource Center http://bacpac.chori.org.Resources for Molecular Cytogenetics http://www.biologia.uniba.it/rmc/.Wellcome Trust Sanger Institute http://www.sanger.ac.uk/.BACH https://www.genopole-lille.fr/bach/menu.php.DECIPHER https://decipher.sanger.ac.uk/.ECARUCA http://www.ecaruca.net/.TheCentre forAppliedGenomics,Database ofGenomicVariantshttp://www.tcag.ca/.Human Genome Segmental Duplication Database http://projects.tcag.ca/humandup/.OMIM http://www.ncbi.nlm.nih.gov/.MRC-Holland www.mrc-holland.com/.
Related Documents