VIKRAM MATHEWS, MD CMC, Vellore, India Professor & Chair, Department of Hematology, Christian Medical College, Vellore, India Dr. Matthews is leading hematologist in India. His interests include: Acute myeloid leukemia, Acute Promyelocytic leukemia, Evaluation of mechanisms of resistance to arsenic trioxide and impact of novel agents in the management of acute promyelocytic leukemia, Allogeneic stem cell transplant. Improving clinical outcomes by studying risk stratification, modifying conditioning regimens and graft manipulation. Study of inhibitors in hemophilia.

Ideal induction therapy for newly diagnosed AML. Do we have a consensus?
Aug 09, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
VIKRAM MATHEWS, MDCMC, Vellore, India
Professor & Chair, Department of Hematology, Christian Medical College, Vellore, India
Dr. Matthews is leading hematologist in India. His interests include: Acute myeloid leukemia, Acute Promyelocytic leukemia, Evaluation of mechanisms of resistance to arsenic trioxide and impact of novel agents in the management of acute promyelocytic leukemia, Allogeneic stem cell transplant. Improving clinical outcomes by studying risk stratification, modifying conditioning regimens and graft manipulation. Study of inhibitors in hemophilia.

Ideal induction therapy for newly diagnosed AML. Do we have a
consensus?BTG Beijing Jan 2015
Vikram MathewsDepartment of HaematologyChristian Medical CollegeVellore

Overview: Limit data and presentation to young adults Overview of risk stratification Bench mark clinical outcomes: which any
additional interventions should attempt to improve on.
Variations in induction: - Dose of anthracycline - Variations in anthracycline - Dose of Cytosine arabinoside - Addition of a third drug - Novel agents
Perspective from our data (developing country challenges)
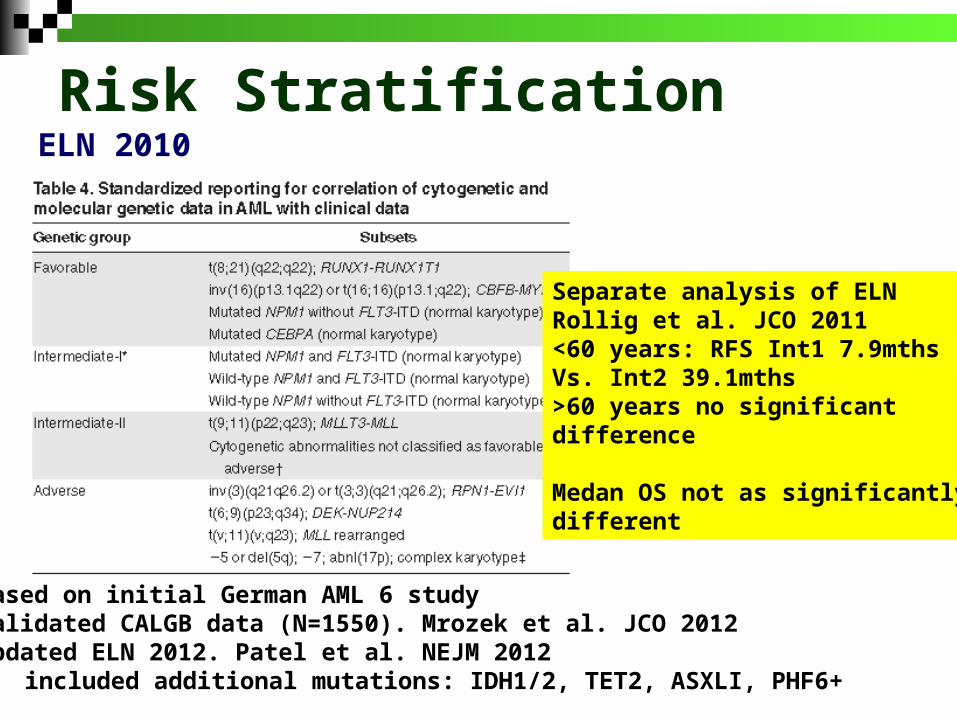
Risk StratificationELN 2010
Based on initial German AML 6 study Validated CALGB data (N=1550). Mrozek et al. JCO 2012Updated ELN 2012. Patel et al. NEJM 2012
included additional mutations: IDH1/2, TET2, ASXLI, PHF6+
Separate analysis of ELNRollig et al. JCO 2011<60 years: RFS Int1 7.9mthsVs. Int2 39.1mths>60 years no significant difference
Medan OS not as significantly different
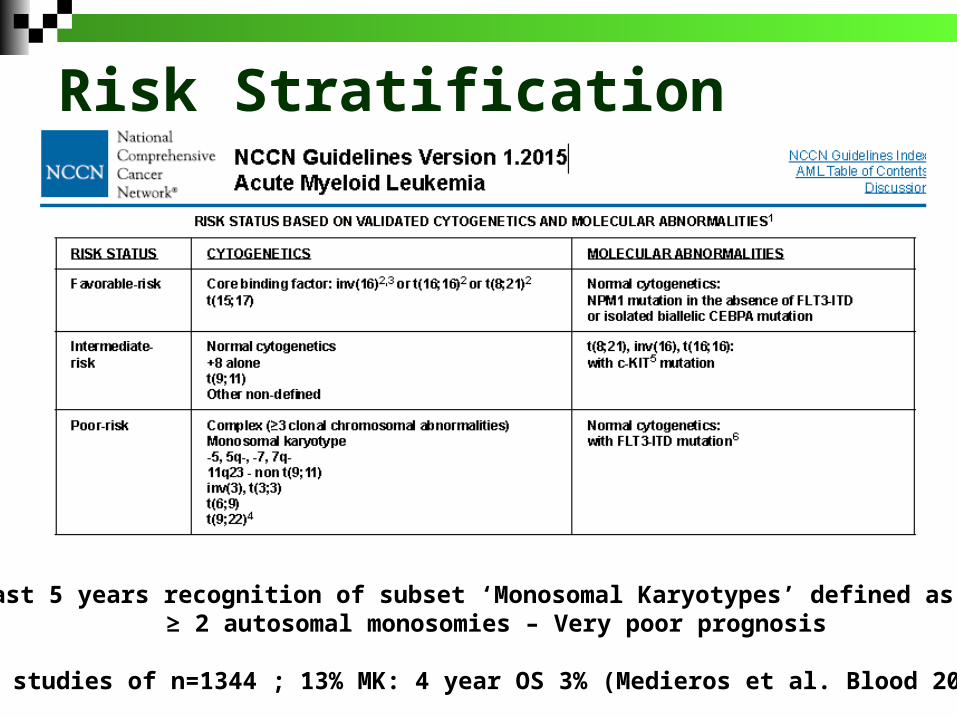
Risk Stratification
Last 5 years recognition of subset ‘Monosomal Karyotypes’ defined as ≥ 2 autosomal monosomies – Very poor prognosis
SWOG studies of n=1344 ; 13% MK: 4 year OS 3% (Medieros et al. Blood 2010)
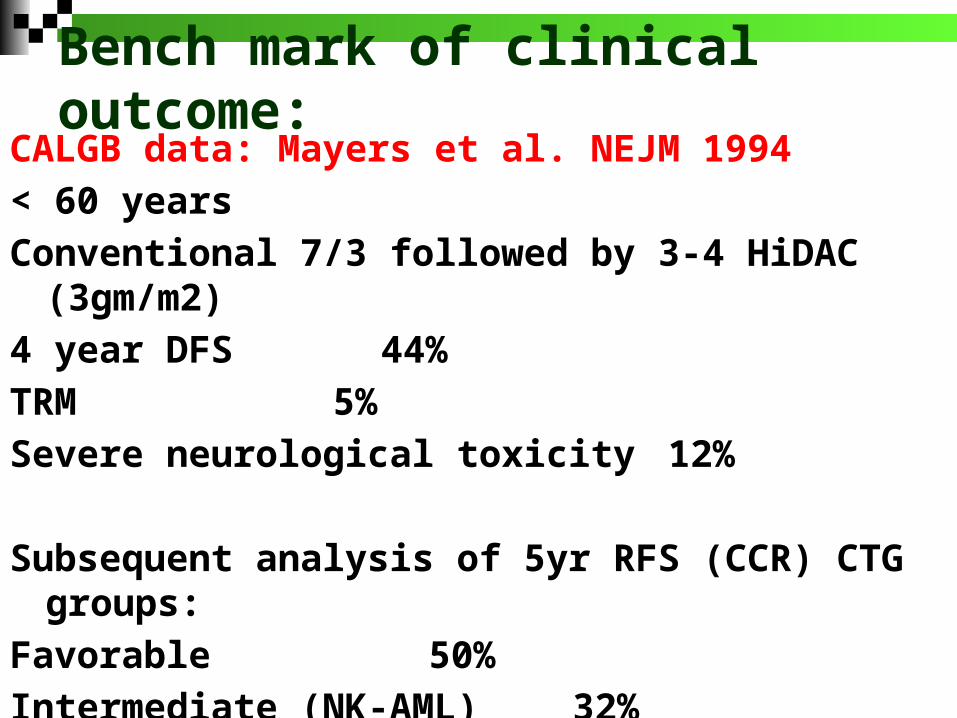
Bench mark of clinical outcome:CALGB data: Mayers et al. NEJM 1994
< 60 years
Conventional 7/3 followed by 3-4 HiDAC (3gm/m2)
4 year DFS 44%
TRM 5%
Severe neurological toxicity 12%
Subsequent analysis of 5yr RFS (CCR) CTG groups:
Favorable 50%
Intermediate (NK-AML) 32%
Others 15%
Dose of anthracycline:

Phase III study (ECOG):n = 657Age 17 – 60 yearsRandomized:
1. 45mg/m2 x 3 days2. 90mg/m2 x 3 days
Induction: Std dose 63.9% CR P<0.001High dose 70.6% CR
Toxicity profile comparableException of LV function (4 cases Vs. 0)
Prior SWOG study with 60mg/m2 better data?


ASH 2014A Randomised Comparison of Daunorubicin 90mg/m2 Vs 60mg/m2 in AML Induction: Results from the UK NCRI AML17 Trial in 1206 Patients. Burnett et al.
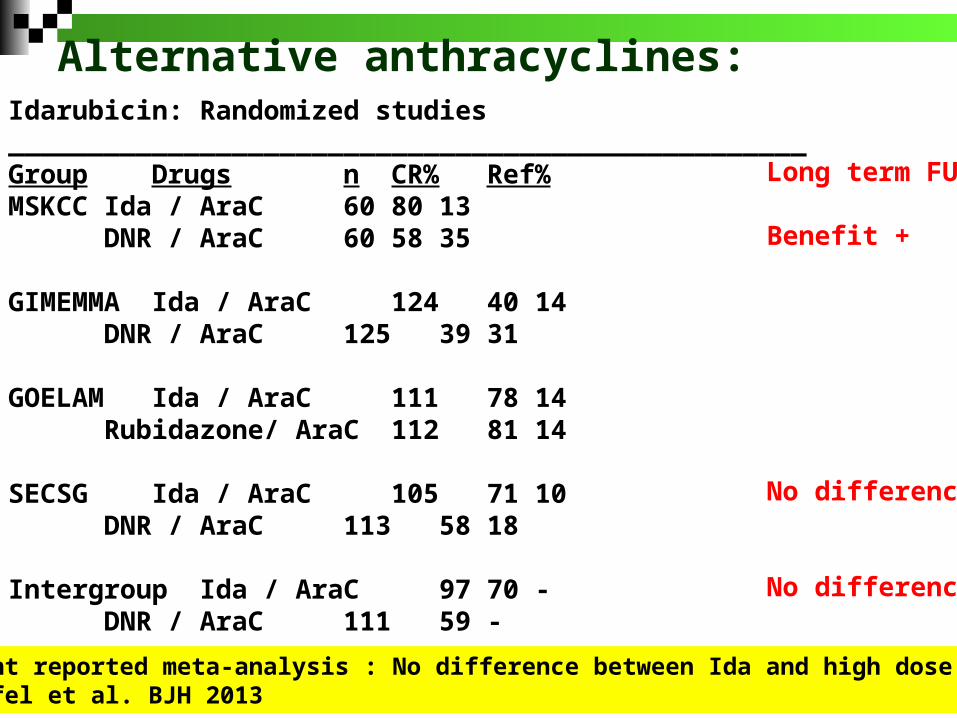
Idarubicin: Randomized studies__________________________________________________Group Drugs n CR% Ref%MSKCC Ida / AraC 60 80 13
DNR / AraC 60 58 35
GIMEMMA Ida / AraC 124 40 14DNR / AraC 125 39 31
GOELAM Ida / AraC 111 78 14Rubidazone/ AraC 112 81 14
SECSG Ida / AraC 105 71 10DNR / AraC 113 58 18
Intergroup Ida / AraC 97 70 -DNR / AraC 111 59 -
Long term FU
Benefit +
No difference
No difference
Alternative anthracyclines:
Recent reported meta-analysis : No difference between Ida and high dose DNRTeuffel et al. BJH 2013

JCO 2009
Dnr:Mito:Ida = 50:12:10 mg/m2

ALSG:Bishop et al. Blood 1996
SWOGAppelbaum et al.Blood 1996Note: OS not significantlydifferent from CALGB datawith standard approachBenefit<50 years
Similar experience in German AML Co-operative trial. No difference in CR, DFS or OS Subset with - poor risk karyotype ]
- > 50% blasts on BM on day 16 ] beneficial- high LDH ]
Buchner et al. Blood 1999
High dose cytosine in induction
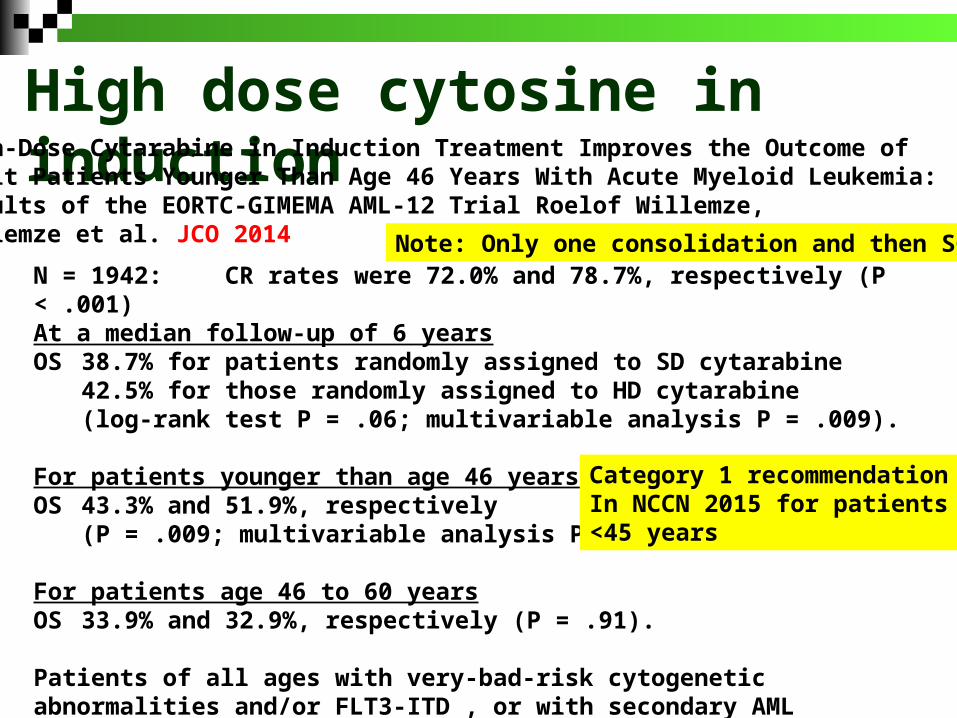
High dose cytosine in inductionHigh-Dose Cytarabine in Induction Treatment Improves the Outcome of Adult Patients Younger Than Age 46 Years With Acute Myeloid Leukemia: Results of the EORTC-GIMEMA AML-12 Trial Roelof Willemze, Willemze et al. JCO 2014
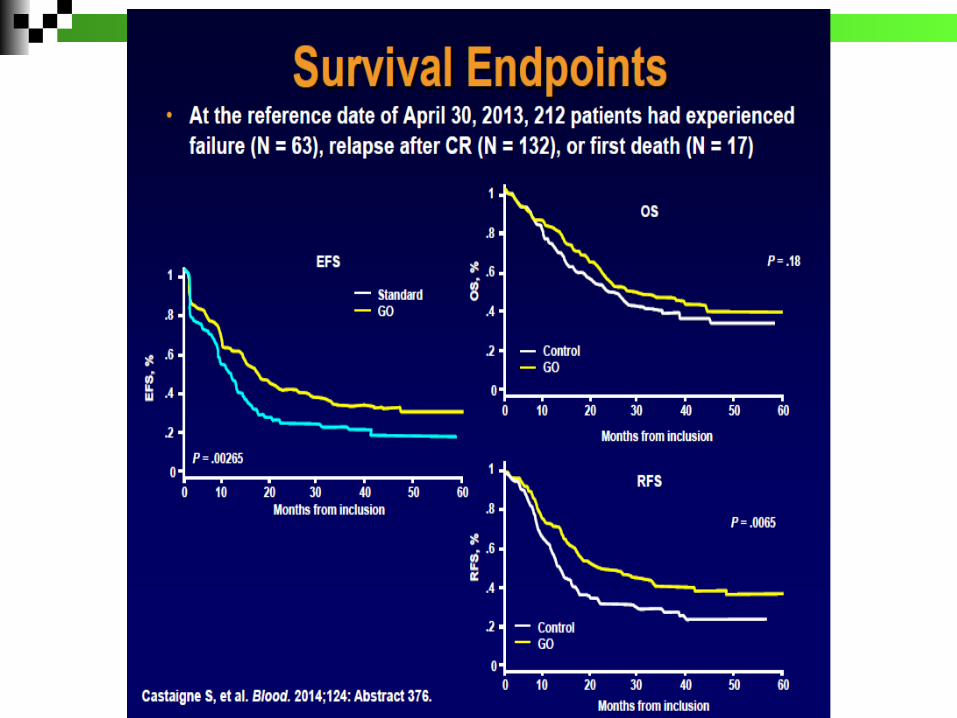
N = 1942: CR rates were 72.0% and 78.7%, respectively (P < .001)At a median follow-up of 6 yearsOS 38.7% for patients randomly assigned to SD cytarabine
42.5% for those randomly assigned to HD cytarabine (log-rank test P = .06; multivariable analysis P = .009).
For patients younger than age 46 years: OS 43.3% and 51.9%, respectively
(P = .009; multivariable analysis P = .003)
For patients age 46 to 60 yearsOS 33.9% and 32.9%, respectively (P = .91).
Patients of all ages with very-bad-risk cytogenetic abnormalities and/or FLT3-ITD , or with secondary AML benefitted from HD cytarabine.
Category 1 recommendationIn NCCN 2015 for patients<45 years
Note: Only one consolidation and then SCT

ALSG (Bishop et al. 1990) suggested that addition of etoposide beneficial to younger patients
There is little evidence to suggest that addition of third drugconfers any benefit (excluding high dose inductionprotocols)
UK MRC AML 10 trial no difference if third drug was thioguanineor etoposide
Similarly in more recent UK MRC AML 15 trial no benefit of additionof etoposide in induction (Burnett et al. JCO 2015)
Addition of third drug to induction regimen:

CR rate: no difference ~85%FLAG-Ida: reducing relapse (38% v 55%; P=.001)
relapse-free survival (45% v 34%; P=.01)
MACE/MidAc was superior for high-risk patients.
Cytarabine at 1.5 g/m2 is equivalent to a 3 g/m2 dose
A fifth course provided no benefit.
Patients receiving FLAG-Ida +Cytosine consolidation

N=632
DAC benefitted > 50 yearsHigh risk karyotypeWBC >50,000/mm3
Toxicity profile comparable

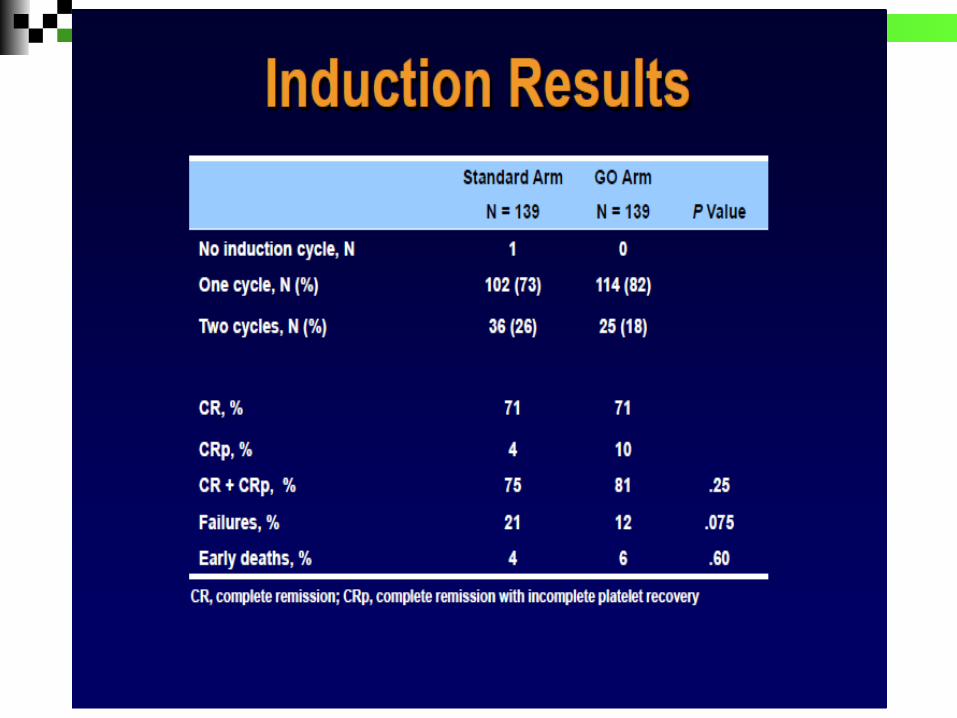
Novel agents Gemtuzumab Sorafenib Lestaurtinib (CEP701) – negative data at
ASH 2014 (UK; N=500 RCT) Dasatinib for Kit mutated CBF leukemia
(CALGB10801). Small numbers : n=59, 10 ckit mutated
Aurora kinase inhibitors – Phase I study Alisertib (n=14)

ASH2014


Sorafenib: Multi-kinase inhibitor Promise in FLT3 mutated AML Negative data in elderly RCT and
increased toxicity (Serve et al. JCO 2013)
ASH 2014: RCT in young adults (SAL-Soraml Trial, Germany) n = 276 Improvement in EFSNo significant benefit on OSSignificant increase risk of infection,
bleeding and hand foot syndrome
Presentation in India (?developing world) “DIFFERENT”
Younger age Delay in presentation / diagnosis More advanced disease and
co morbidities Partially treated Difficult to quantify adverse variables
Treatment expensive Predominantly self pay 39 million people / year go below the poverty
line due to medical related expenses

Results:Diagnosed AML: 427 Newly diagnosed 380≤ 15 years 47 (12.3%) >15 - <60 years 271 (71.3%)≥ 60 years 62 (16.3%)
Median age 40 (1 – 79)Males 244 (64.2%)
5
14.715.8
15
18.4
15.5
12.1
3.4
0
2
4
6
8
10
12
14
16
18
20
0--10 11--20 21--30 31--40 41--50 51--60 61--70 71--80
Perc
enta
ge
Age (years)
A
E
B C
D
BJH 2015 In Pres

Results: Median duration of symptoms 4 weeks (1 – 52)
Median distance from hospital 580 km (6 – 3200); 29 from another country
ECOG score ≥ 2 23%
6.5
16.8
6.5
26.1
9.67.9 6.8
9.2
6.1
2.6 1.8
0
10
20
30P
erc
en
tage
Duration of symptoms
BJH 2015 In Pres

Objective 2: Compare the frequency of these markers in our population with previously published data.
The trend suggests that for the majority of markers evaluated the incidence of of these mutations in our population is similar to that reported in the literature.
Gene N Mutation n(%) Reported (%)NPM1 337 96 (28.5) 35FLT3-ITD 336 64 (19) 20FLT3-TKD 335 13 (3.88) 5WT1 (exon7/9) 316 11 (3.5) 12JAK2 270 1 (0.3) NAc-KIT (exon 8/17) 272 6 (2.2) 7CEBPα - single 248 61 (21.5) 25CEBPα - double 284 10 (3.52) 5-7N-RAS 276 25 (9) 18AML1-ETO 337 30 (8.9) 5-10MYH-CBFβ 337 19 (5.6) 5-10MLL-PTD 297 8 (2.7) 5
Final report DBT COE June 2014
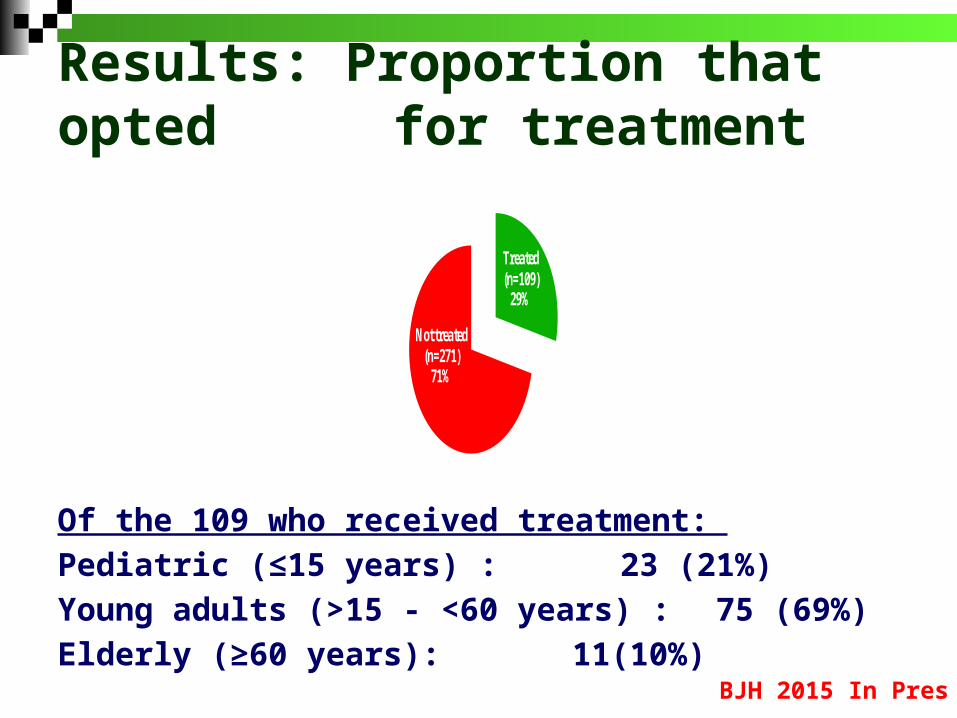
Results: Proportion that opted for treatment
Of the 109 who received treatment:
Pediatric (≤15 years) : 23 (21%)
Young adults (>15 - <60 years) : 75 (69%)
Elderly (≥60 years): 11(10%)
5
14.715.8
15
18.4
15.5
12.1
3.4
0
2
4
6
8
10
12
14
16
18
20
0--10 11--20 21--30 31--40 41--50 51--60 61--70 71--80
Perc
enta
ge
Age (years)
Treated (n=109)
29%
Not treated (n=271)
71%
A
E
B C
D
BJH 2015 In Pres
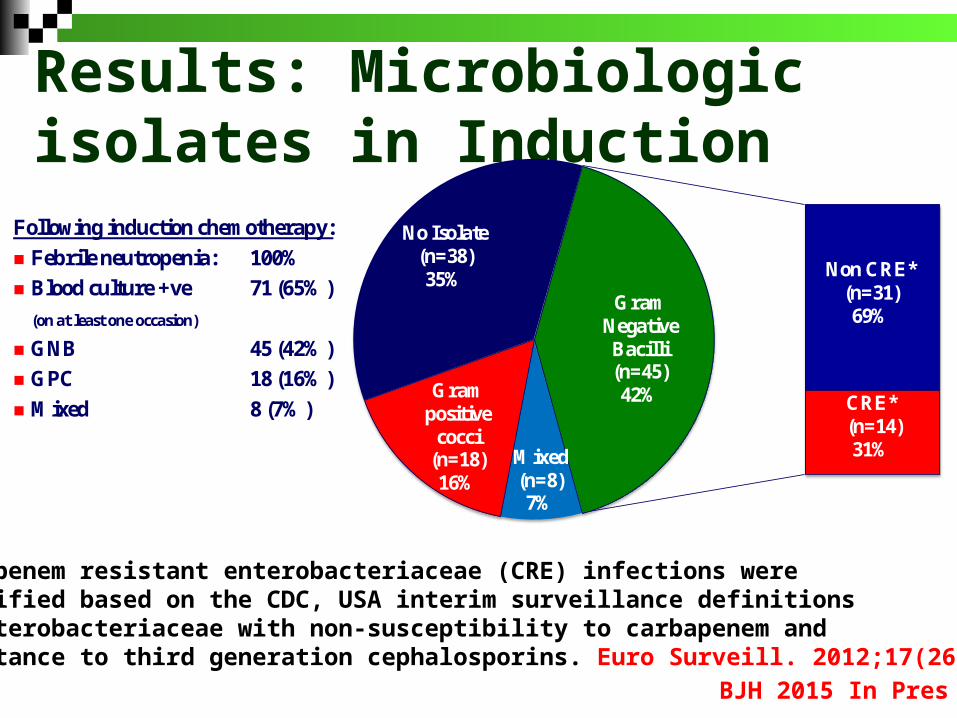
Results: Microbiologic isolates in Induction
Mixed (n=8)7%
Gram positive
cocci (n=18)16%
No Isolate (n=38)35% Non CRE*
(n=31)69%
CRE*(n=14)31%
Gram Negative Bacilli(n=45)42%
Carbapenem resistant enterobacteriaceae (CRE) infections were identified based on the CDC, USA interim surveillance definitions as enterobacteriaceae with non-susceptibility to carbapenem and resistance to third generation cephalosporins. Euro Surveill. 2012;17(26)
Following induction chemotherapy:
Febrile neutropenia: 100%
Blood culture +ve 71 (65%)
(on at least one occasion)
GNB 45 (42%)
GPC 18 (16%)
Mixed 8 (7%)
BJH 2015 In Pres

Results: Early deaths Following induction chemotherapy: Febrile neutropenia 100% Early post induction deaths 27 (24%) Majority related to sepsis and fungal
infection
An additional 17 died in period of study of which 9 due to disease recurrence
Mixed (n=3)11%
Gram positive cocci (n=2) 7%
No isolate(n=4)15%
CRE (n=7)39%
Non CRE (n=11)61%
Gram negative bacilli(n=18)67%
Of non-CRE Carbepenem Resistant Pseudomonas in 5
MDR organism 12 (45%)
Invasive fungal infection 12 (44%)
BJH 2015 In Pres

Results: Survival Numbers small
Follow up shortMedian FU 7 mths
22 alloSCT CR1 18 young adults 4 pediatric
One year KM values
BJH 2015 In Pres
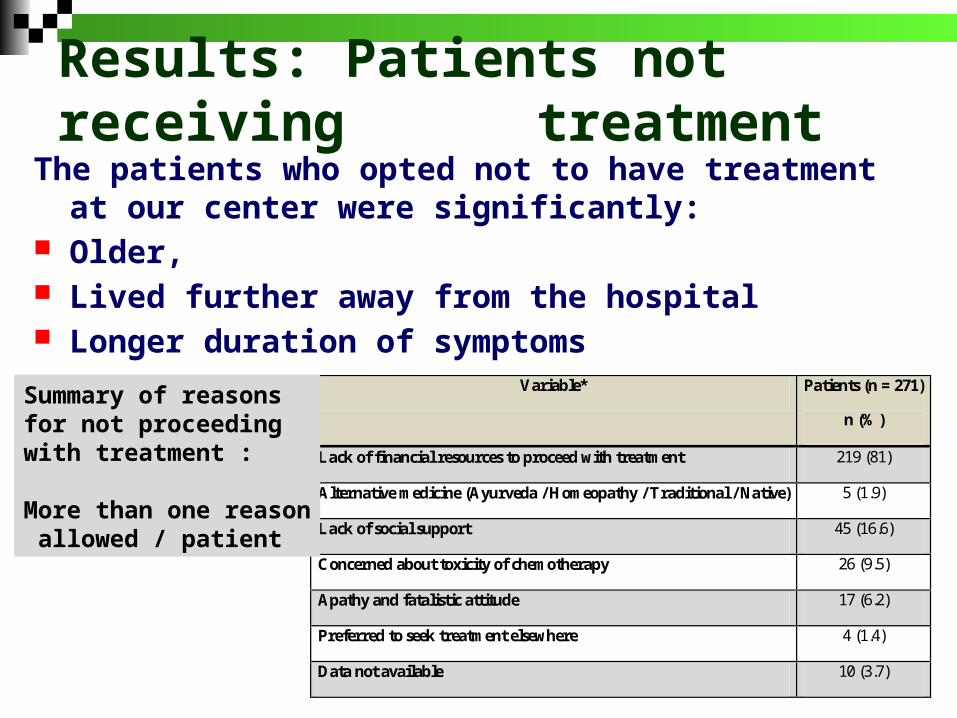
Results: Patients not receiving treatment
The patients who opted not to have treatment at our center were significantly:
Older, Lived further away from the hospital Longer duration of symptoms
Variable* Patients (n = 271)
n (%)
Lack of financial resources to proceed with treatment 219 (81)
Alternative medicine (Ayurveda / Homeopathy / Traditional / Native) 5 (1.9)
Lack of social support 45 (16.6)
Concerned about toxicity of chemotherapy 26 (9.5)
Apathy and fatalistic attitude 17 (6.2)
Preferred to seek treatment elsewhere 4 (1.4)
Data not available 10 (3.7)
Summary of reasons for not proceeding with treatment :
More than one reason allowed / patient

Conclusion : Major challenge is financial burden and absence of a
health security net to treat all newly diagnosed patients with AML
Fungal infections remain a problem MDR bacterial infections is major challenge. Likely
to increase world wide. Limits ability to intensify therapy to improve clinical outcomes
Cost of therapy directly related to recurrent cycles of cytopenia, duration of neutropenia and need for intensive support in ICU
Novel combinations and targeted therapy without recurrent cytopenia are needed

Thank you for your attention
Related Documents











