ICTERUS NEONATORUM Presented by: Ms. Sharon Vincent II yr MSc Nursing

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ICTERUS NEONATORU
M Presented by:
Ms. Sharon Vincent
II yr MSc Nursing
INTRODUCTION Jaundice is a yellow discoloration
of the skin, sclera and mucus menbrane caused by hyperbilirubinemia.
The newborn appear jaundice when level is >5mg/dl.
Jaundice usually becomes visible at
Sclera -2 to 3 mg/dL Face - 4 to 5 mg/dL Umbilicus -15 mg/dL Feet - 20 mg/dL.

INCIDENCE
25-60 % of full term newborns develop clinical jaundice
75-85% of preterm infants
3% of normal term infants show bilirubin levels > 15mg/dl

FETAL BILIRUBIN METABOLISM
Bilirubin can be be detected in normal amniotic fluid from 12 weeks of GA and disappears by 36 to 37 weeks .
Uridine diphosphoglucoronosyl transferace activity in 0.1 % fetal liver, reaches to 1% of adult value by term gestation.
The major route of fetal bilirubin excretion is across the placenta.

BILIRUBIN METABOLIS
M

TYPES Physiological jaundicePathological jaundice Breast feeding jaundice Breast milk jaundice
Physiological jaundiceIn term neonates: TSB reaches to 5-6 mg/dl by 48 to 120 hours of age.
10-14 mg/dl at 72-120 hours of age.
Rapid decline to approx 3mg/dl by fifth day of life.
This is designated as a phase I physiological jaundice.
From the 5-10 th day of life TSB concentration decline slowly reaching the normal adult value of less than 2mg/dl phase 2 physiological jaundice.
In preterm neonate: jaundice is more severe with mean peak TSB concentration reaching 10 to 12 mg/dl by the fifth day of life

Pathological jaundice
Clinical jaundice appearing in the first 24 hours. It increases in the level of TSB by more than 0.5 mg/dl /hr or 5mg/dl/24 hours
CAUSES Fetomaternal blood group incompatibility –
Rh, ABO Hereditary spherocytosis G6PD deficiency Vitamin induced hemolysis Sepsis Enterohepatic circulation Pyloric stenosis Large bowel obstruction Hypothyroidism
Breast feeding jaundice Occur in the I week of life in the
breast feed neonates. Maternal factors like lack of
proper technique, breast engorgement , cracked nipple .
Neonatal factors like ineffective and some congenital anomalies like cleft lip and palate.
All these leads to dehydration and delayed passage of meconium. Leads to increase in enterohepatic reuptake of bilirubin leading to unconjugated hyperbilirubinemia.

BREAST MILK JAUNDICEOccur during 2-3 weeks of life
beyond upto 3 months of age. Usually TSB reches a peak of 5 to
10 mg/dl at approximately 2 weeks of life or beyond upto 3 months of age.
Pregnadiol a progestrone metabolism found in the breast milk was thought to be the cause of the disorder.
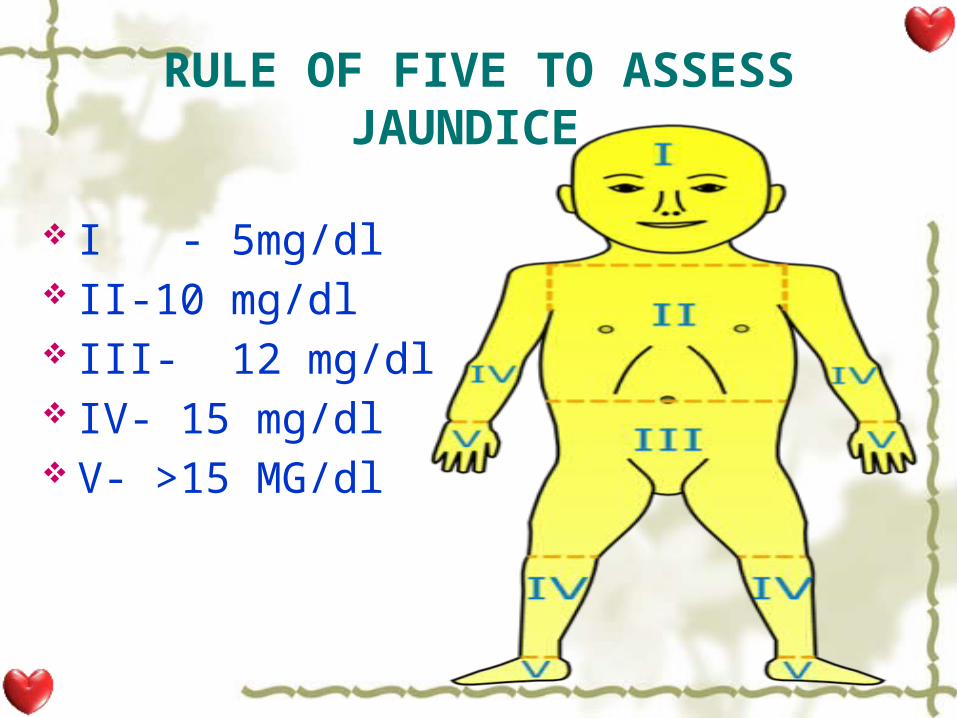
RULE OF FIVE TO ASSESS JAUNDICE
I - 5mg/dl II-10 mg/dl III- 12 mg/dl IV- 15 mg/dl V- >15 MG/dl
KERNICTERUS (CHRONIC BILIRUBIN ENCEPHALOPATHY
Kern: nuclear region of the brain and
Icterus – jaundice Kernicterus is brain damage
caused by unconjugated bilirubin deposition in basal ganglia and brain stem nuclei, caused by either acute or chronic hyperbilirubinemia.

Causes Bilirubin can cross the blood-brain barrier in
certain situations: When serum bilirubin concentration is
markedly elevated >20mg/dl When serum albumin concentration is
markedly low (eg, in preterm infants) When bilirubin is displaced from albumin
by competitive binders (eg, sulfisoxazole , ceftriaxone , aspirin and free fatty acids and hydrogen ions eg, in fasting, septic, or acidotic infants).
Clinical features
Extrapyramidal disturbances especially athetosis (slow, purposeless, and involuntary movements of the hands, feet, face, tongue, and neck as well as other muscle groups).
Auditory abnormalities especially sensori neural hearing loss
Gaze palsies especially upward gaze
Dental dysplasia

Clinical Features Of Bilirubin Encephalopathy
Initial phase
•slight stupor•(lethargy ,sleep)•Slight hypotonia •Poor sucking
Intermediate phase
•Moderate stupor •Tone variable , opisthotonus•Minimal feeding
Advanced phase
•Deep stupor to coma •Tone usually increased •No feeding shrill cry

INVESTIGATIONS HistoryTranscutaneous bilirubinometry Total serum bilirubin Blood type and Rh Direct antiglobulin test (DAT) in the infant (direct Coombs test)Hb, PCVSerum albumin levelsLiver function tests
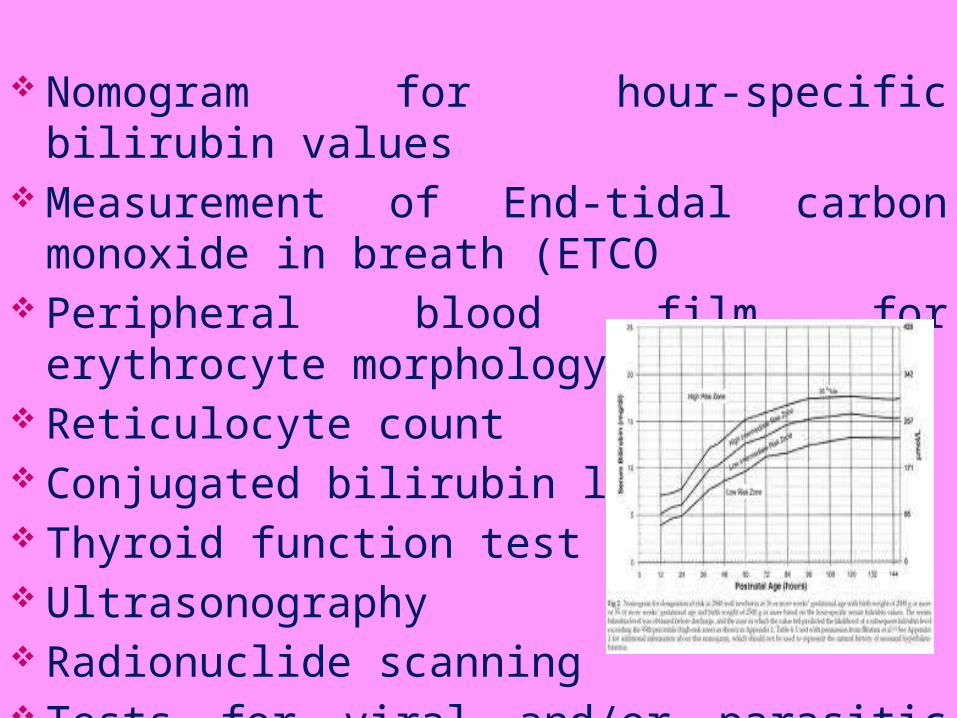
Nomogram for hour-specific bilirubin values
Measurement of End-tidal carbon monoxide in breath (ETCO
Peripheral blood film for erythrocyte morphology
Reticulocyte count Conjugated bilirubin levels: Thyroid function test Ultrasonography Radionuclide scanning Tests for viral and/or parasitic infection
MANAGEMENT
PHYSIOLOGIC JAUNDICEno specific treatment requiredcontinue breast feedingwatch for sudden rise in
bilirubin levelstreat any exaggerating factors.

PATHOLOGIC JAUNDICE Increase feeds in volume and calories. Early feeding lowers serum bilirubin level by stimulating the peristalsis. Stop drugs interfering with bilirubin metabolism. Correct hypoxia, infection, and acidosis. Phototherapy
Prophylactic: in LBW or bruised neonate. Therapeutic.
Exchange transfusion.PhenobarbitolAgar-AgarAlbumin infusionTin protoporphyrin
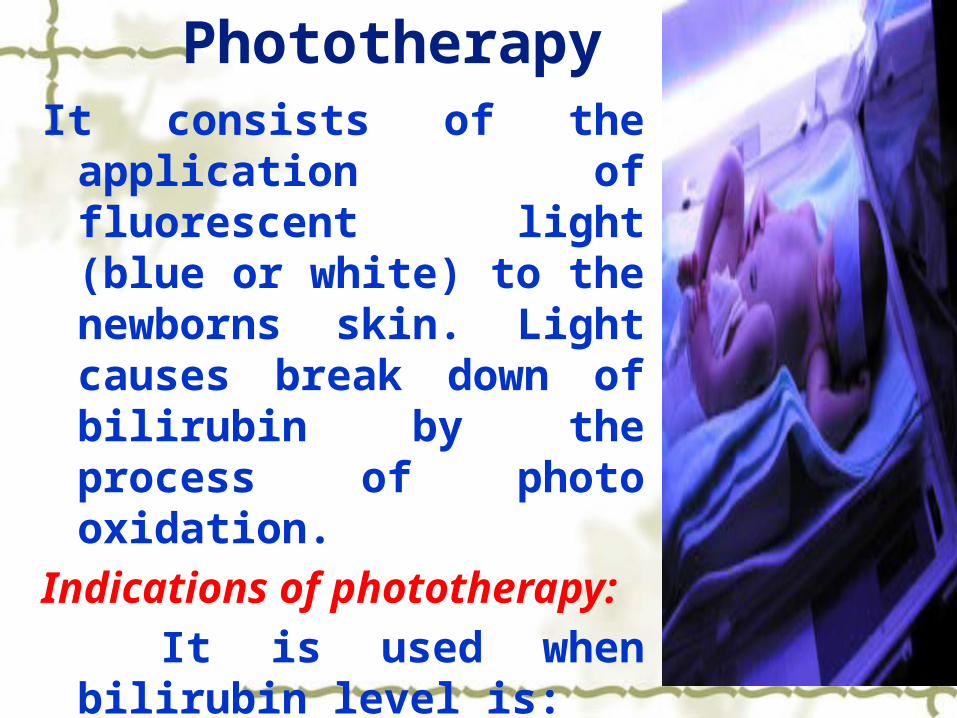
PhototherapyIt consists of the
application of fluorescent light (blue or white) to the newborns skin. Light causes break down of bilirubin by the process of photo oxidation.
Indications of phototherapy:
It is used when bilirubin level is:
5-9 mg/dl at the 1st day of life.
9-15 mg/dl at the 2nd day of life.
15-20 mg/dl at the 3rd day of life.
Side effects of phototherapy: Dehydration due to increased insensible water loss. Watery diarrhea. Hypocalcemia. Retinal damage. Erythema and skin rashs. Bronze baby syndrome. Maternal newborn interaction is affected. Dark yellow urine.

Nurse’s responsibility in phototherapy:
The lamp should be 5-8 cm over the incubator.
Continue the feeding. Shield the newborn’s eyes, genetalia change position frequently. Cleanse skin frequently to prevent irritation. prevent dehydration and calculate intake and
output.

Check newborn’s body temperature every four hours.
Weight newborn daily. Observe skin, mucous
membranes, and stool. Bilirubin levels should be
followed for at least 24 hours after discontinuing phototherapy.
EXCHANGE TRANSFUSION
It is an ideal dilution of S. Bilirubin and antibodies. A catheter is introduced into the umbilical vein after cutting the cord. Through a special valve, the umbilical catheter is connected with the donor blood. Exchange is carried out over 45-60 min period by alternating aspiration of 20 ml of newborn’s blood and infusions of 20 ml of the donor blood.

Exchange transfusion

Indication Despite phototherapy progressive rise of bilirubin>1mg/dl/hrTo improve anemia and CCF of neonateSerum bilirubin ≥ 20mg/dlCord blood HB < 12 mg/dl & bilirubin> 5mg/dl

Complications:Embolism, thrombosis,
infarction.Arrhythmias, heart failure,
arrest.Electrolyte disturbances.Thromobocytopenia. Infections Hypo and hyperthermia.

Nursing responsibilities: Keep the newborn NPO for 2-4
hours before exchange to prevent aspiration.
Check donor blood charts compatibility.
Keep resuscitation equipment at bedside: oxygen, ambu bag, endotracheal tubes, and laryngoscope.
Assist physician with exchange transfusion procedure.

Track amount of blood withdrawn and transfused to maintain balanced blood volume.
Maintain body temperature to avoid hypothermia and cold stress.
Monitor vital signs and observe for rash.
After transfusion, continue to monitor vital signs and check umbilical cord for bleeding or signs of infection.

PHENOBARBITAL Mechanism of Action: induces
activity of enzyme glucoronyl transferase and increases bilirubin conjugation and excretion.
Dosage: therapeutic- 5-8mg/kg/day to newborn indicated only in Crigler Najjar syndrome type II & other conjugated hyperbilirubinemia.
Side-Effects: drowsy child, slow feeding.
AGAR Mechanism of Action: binds bilirubin to gut and diminishes enterohepatic circulation. Dosage: 125mg/ 3 hrly in mild to moderate hyperbilirubinemia.TIN PROTOPORPHYRIN: hemeoxygenase enzyme inhibitor.
ALBUMIN INFUSION Mechanism of Action: raises bilirubin
binding capacity. Dosage: 1mg/kg of salt free albumin can
be used as an alternative for exchange transfusion.
BREAST MILK JAUNDICE
Interruption of breastfeeding for 24-48 hours and feeding with breast milk substitutes often helps to reduce the bilirubin level.
NURSING DIAGNOSIS Risk for injury from breakdown
products of red blood cells in greater numbers than normal and functional immaturity of liver
Altered family processes related to maturational crisis, birth of term infant, change in family unit
REFERENCE Singh M .Care of Newborn.6th edition. Published by Narinder K. Sagar: NewDelhi; 2004 Gupta Piyush . Essential paediatric Nursing . 1st edition .AP Jain & Co. NewDelhi; 2004 Gupta Suraj .Recent advancesin Paediatrics.1st edition. Jaypee publication : NewDelhi; 1991 Desai VJ, Avalokitha B. Achar’s text book of Pediatrics, 3rd edition, Madras, Orient Logmon Limited; 1991 Parthasarathy A, Menon PSN, Nair MKC. IAP text book of pediatrics. 2nd edition. New Delhi: Jaypee publishers;2000 http://www.ncbi.nlm.nih.gov/pubmed/19000294 http://emedicine.medscape.com/article/974786-overview

Related Documents











