DEEPTHY P. THOMAS II YEAR MSc NURSING GOVT.COLLEGE OF NURSING ALAPPUZHA BIRTH INJURIES AND ICTERUS NEONATARUM

Birth injuries and icterus neonatarum
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DEEPTHY P. THOMAS
II YEAR MSc NURSING
GOVT.COLLEGE OF NURSING
ALAPPUZHA
BIRTH INJURIES AND ICTERUS
NEONATARUM

DEFINITION-birth injuries
An impairment of the infant’s body function or structure due to adverse influences that occurred at birth.
National Vital Statistics Report
Birth injuries is defined as those sustained during labour and delivery. Birth injuries may be severe enough to cause neonatal deaths, still births or number of morbidities.
D C Dutta
RISK FACTORS
Primiparity
Small maternal stature
Maternal pelvic anomalies
Prolonged or unusually rapid labor
Oligohydraminos
Malpresentation of the fetus
Use of mid forceps or vacuum extraction
Versions and extraction
Very low birth weight or extreme
prematurity
Fetal macrosomia or large fetal head
Fetal anomalies
PREDISPOSING FACTORS
Prolonged or obstructed labor
Fetal macrosomia
Cephalopelvic disposition
Abnormal presentation (breech)
Instrumental delivery
Difficult labor
Shoulder dystocia
Precipitate labor

TYPES OF BIRTH INJURIES
Soft tissue: skin- laceration, abrasions,
aft necrosis.
Nerve: facial nerve, brachial plexus,
spinal cord, phrenic nerve, horner’s
syndrome
Eye: hemorrhages-subconjunctiva,
retina
Viscera: rupture of liver, adrenal gland,
spleen
Scalp: laceration, abscess,
haemorrhage.

Dislocation: hip, shoulder, cervical
vertebrae
Skull: cephal hematoma, subgleal
hematoma, fractures
Intracranial: haemorrhages-
intraventricular, subdural, subarachanoid
Bones: fractures-clavicle, humerus,
femur

HEAD AND NECK INJURIES
1.injuries associated with intrapartumfetal monitoring
2. Extracranial hemorrhage
b) cephalohematoma
b) cephalohematoma
c) subgleal hematoma
3. Intracranial haemorrhage
4. Skull fracture
5. Facial or mandibular fractures

6. Nasal injuries
7. ocular injuries
8. Ear injuries
9. Sternocleidomastoid injury
10. Pharyngeal injury
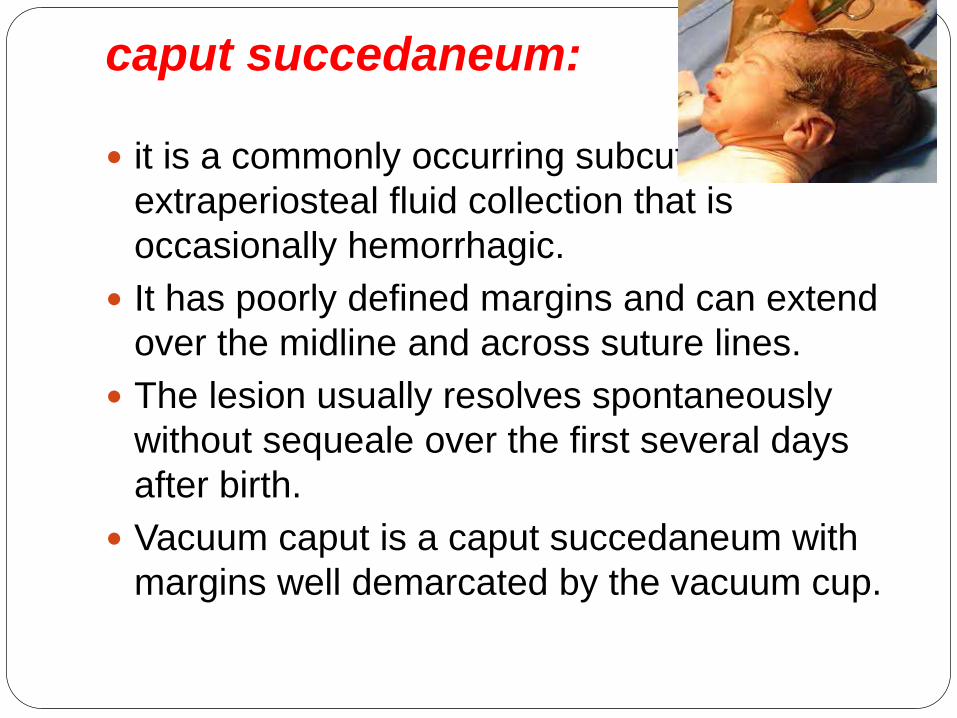
caput succedaneum:
it is a commonly occurring subcutaneous,
extraperiosteal fluid collection that is
occasionally hemorrhagic.
It has poorly defined margins and can extend
over the midline and across suture lines.
The lesion usually resolves spontaneously
without sequeale over the first several days
after birth.
Vacuum caput is a caput succedaneum with
margins well demarcated by the vacuum cup.

cephalohematoma
It is a collection of blood between the
pericranium and flat bone of the skull,
usually unilateral and over the parietal
bone.

Causes
rupture of small emissary vein from the
skull and may be associated with
fracture of the skull bone. It is never
present at birth but gradually develops
after 12-24 hours.
The condition may be confused with
caput succedaneum or meningocele.
Meningocele always lies over a suture
line or over a fontanelle and there is
impulse on crying. Prognosis is good.

subgleal hematoma
subgleal hematoma is hemorrhage
under the aponeurosis of the scalp. It is
more often seen after vaccum or forceps
assisted deliveries.
the hemorrhage can spread across the
entire calvarium.
Intracranial haemorrhageTraumatic:
Extradural haemorrhage:
Subdural:
Slight haemorrhage may occur following:
A] fracture of skullbone
B] rupture of the inferior sagital sinus
C] rupture of small veins leaving the cortex
massive haemorrhage:
a] tear of the tendorium cerebrii
b] injury of superior sagital sinus


mechanism of tentorial tear:
normally falx cerebri attached to the tentorium
cerebri and both anchoring the base of the skull
to the vault.
This results in the upward movement of the
vault from the base.
As a result, too much strain is put on the vertical
fibres of tentorium cerebella- called stress
fibres.
If the moulding is excessive or applied suddenly,
these fibres are torn.
as a result it allows excessive elongation of the
vault until the tear extends to involve the
straight sinus or vein of Galen or its tributaries.
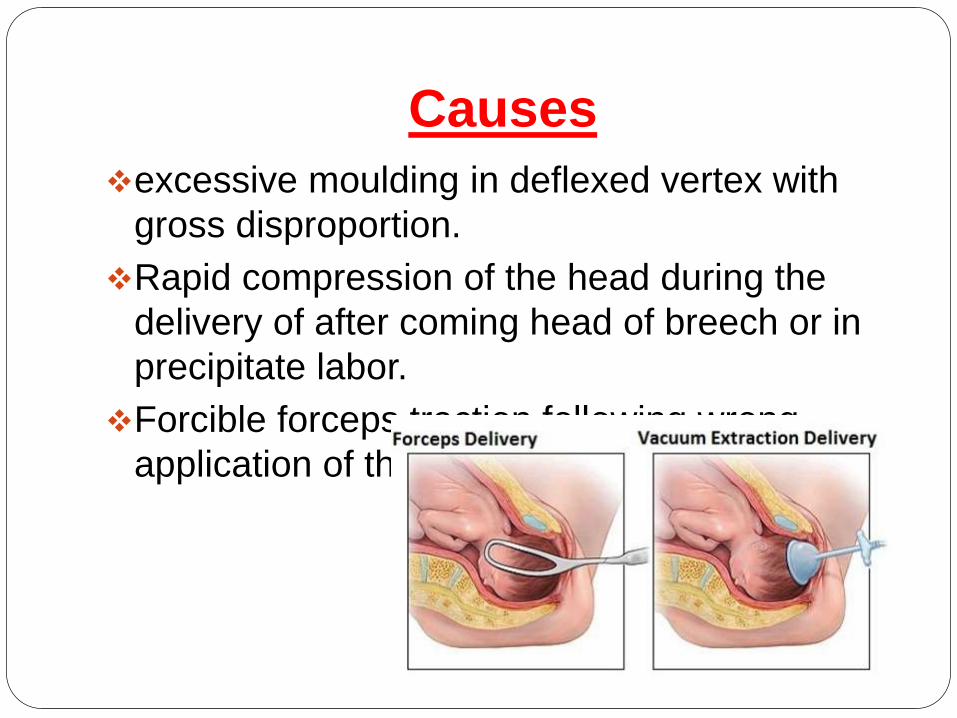
Causes
excessive moulding in deflexed vertex with
gross disproportion.
Rapid compression of the head during the
delivery of after coming head of breech or in
precipitate labor.
Forcible forceps traction following wrong
application of the blades.

Clinical features
The hemorrhage may be fatal
the baby is delivered stillborn or with severe
respiratory depression having an apgar score
0-3.
The features cerebral irritation include
frequent high pitch cry, neck retraction, in-
coordinate ocular movements, convulsions,
vomiting and bulging of anterior fontanelle.

Anoxic:
Intraventricular
Subarachanoid.
Intracerebral.

PREVENTION
To prevent or to detect earliest, intrauterine
fetal asphyxia
To avoid traumatic vaginal delivery.
To extend the use of caesarean section in
breech more liberally.
Administration of vitamin K 1 mg
intramuscularly soon after birth
INVESTIGATIONS:
Ultrasongraphy used to detect intraventricular
hemorrhage
Doppler ultrasonography to detect any change
in the cerebral circulation.
CT scan is useful to detect cortical neuronal
injury.
MRI used to identify hypoxic ischemic brain
injury.
CSF: hemorrahage

TREATMENT
The baby should be nursed in quite
surroundings.
Incubator nursery is preferable to supply
oxygen and to maintain the temperature and
humidity.
To maintain cleanliness of the air passages.
To maintain normal range of PaCO2 and to
avoid hypoxemia
To restrict handling the baby, as such bathing,
weighing and measuring should be withheld.
Feeding by nasogastric tube is advisable.
Fluid balance is to be maintained, if necessary
by parenteral route.
To administer vitamin K 1 mg intramuscularly
to prevent further bleeding due to
hypoprothrobinemia.
Prophylactic antibiotics is to be administered.
Anticonvulsants: phenobarbitone 5-10
mg/kg/day in divide doses at 6 hourly intervals
intramuscularly, phenytoin 10-15 mg/kg/day
with cardiac monitoring
Subdural tap for subdural hematoma

Skull fracture
Fracture of the vault of the skull may be
fissure or depressed type.
Fractures are due to
Effect of difficult forceps in disproportion or
due to wrong application of the fo4rceps.
Projected sacral promontory of the flat
pelvis may produce depressed fracture
even though the delivery is spontaneous.
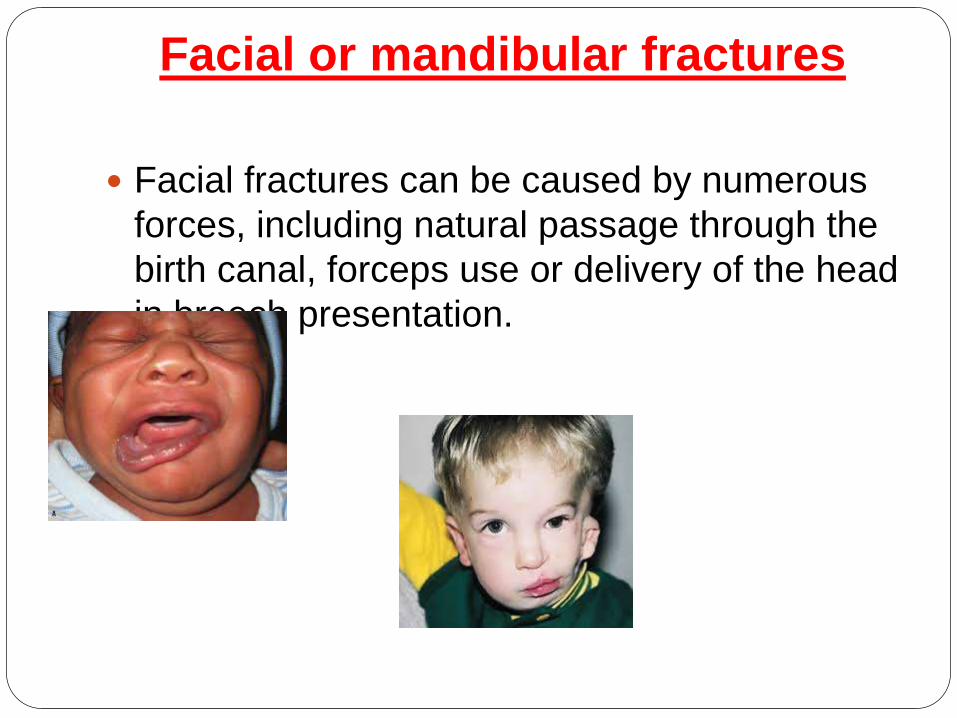
Facial or mandibular fractures
Facial fractures can be caused by numerous
forces, including natural passage through the
birth canal, forceps use or delivery of the head
in breech presentation.

Nasal injuries
Nasal fracture and dislocation may occur
during the birth process. The most frequent
nasal injury is dislocation of the nasal
cartilage, which may result from pressure
applied by the maternal symphysis pubis or
sacral promontory.

ocular injuries
They result from increased venous congestion
and pressure during delivery. Retinal
hemorrhages usually resolve within 1 to 5
days. Sub-conjunctival hemorrhages reabsorb
within 1 to 2 weeks.
Ear injuries
Ears are susceptible to injury particularly
with forceps application. More significant
injuries occurs with fetal malposition.

Sternocleidomastoid injury
referred to as congenital or muscular
torticollis. The etiology is uncertain. The most
likely cause is a muscular compartment
syndrome resulting from intrauterine
positioning.

Pharyngeal injury
Minor submucosal pharyngeal injuries
can occur with postpartum bulb
suctioning. More serious injury, such as
perforation into the mediastinal or
pleural cavity, may result from
nasogastric or endotracheal tube
placement.

CRANIAL NERVE, SPINAL CORD
AND PERIPHERAL NERVE INJURY
Cranial nerve injury
Facial nerve injury:
Recurrent laryngeal injury
spinal cord injuries
Vaginal delivery of an infant with a hyper
extended neck or head, breech delivery and
severe shoulder dystocia are risk factors for
spinal cord injury. Injuries include spinal
epidural hematomas, vertebral artery
injuries, traumatic cervical hematomyelia,
spinal artery occlusion and transaction of
the cord.

cervical nerve root injury
Phrenic nerve injury
Phrenic nerve damage leading to
paralysis of ipsilateral diaphragm may result
from a stretch injury due to lateral hyper
extension of the neck at birth. Risk factors
include breech and difficult forceps deliveries.

Brachial plexus injury
The cause is excessive traction on the head,
neck and arm during birth.the risk factors
include shoulder dystocia, macrosomia,
malpresentation and instrumented deliveries.

Duchenne- Erb palsy involves the upper
trunks (C5, C6 and occasionally C7) and is
the most common type of brachial plexus
injury. The arm is typically adducted and
internally rotated at the shoulder. There is
extension and pronation at the elbow and
flexion of the wrist and fingers in the
characteristics “waiter’s tip” posture, the
deltoid, infraspinatus and biceps, supination
and brachioradialis muscles and the
extensors of the wrist and the fingers may be
weak or paralysed. The moro, biceps, and the
radial reflexes are absent on the affected side.
Diaphragm paralysi occurs in 5% of cases.

Total brachial plexus injury accounts for
approximately10% of all cases. The entire
arm is flaccid. All reflexes including grasp and
sensation, are absent. If sympathetic fibres
are injured at T1, Horner syndrome may be
seen.

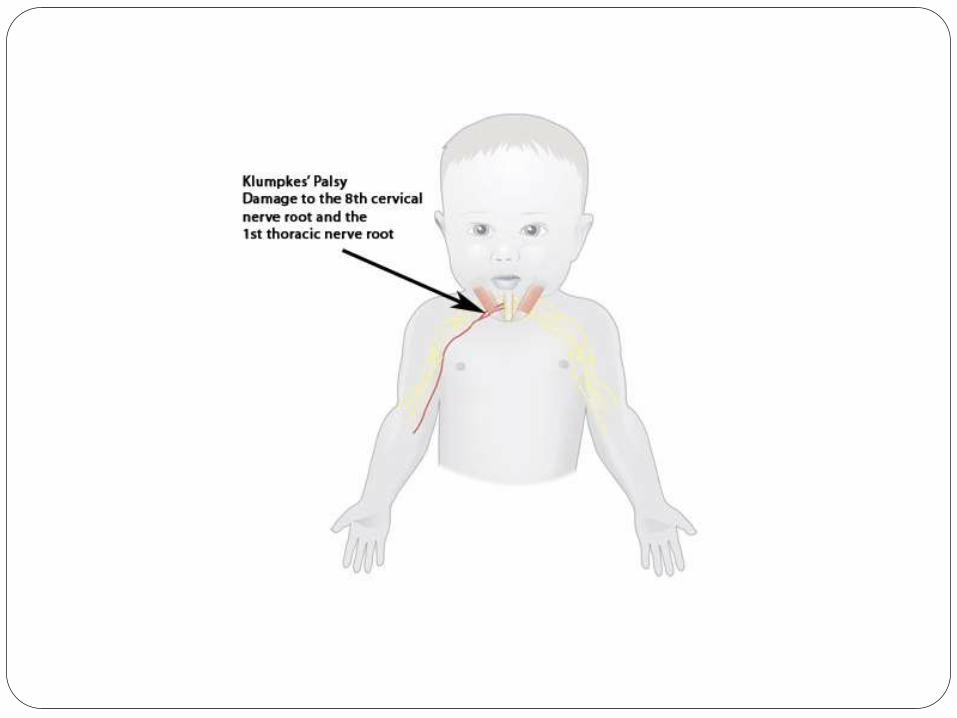
Klumpke palsy rarest of the palsies
accounting for <1% of brachial plexus
injuries. The lower arm paralysis affects
the intrinsic muscles of the hand and the
long flexors of the wrist and fingers. The
grasp reflex is absent. However, the
biceps and radial reflexes are present.
There is sensory impairment on the
ulnar side of the forearm and the hand.
Because the first thoracic root is actually
injured, its sympathetic fibres are
damaged, leading to an ipsilateral
Horner syndrome.

BONE INJURIES
clavicular fracture
These fractures are seen in vertex
presentations with shoulder dystocia
or in breech deliveries when the arms
are extended
long bone injuries
Humeral fractures typically occur during
adifficulty delivery of the arms in the breech
presentation and/ or of the shoulder in vertex.
Direct pressure on the humerus may also
result in fracture.
Femoral fractures usually follow a
breech delivery. Infants with congenital
hypotonia are at increased risk. Physical
examination usually reveals an obvious
deformity of the thigh

INTRA ABDOMINAL INJURIES
Hepatic injury
Splenic injury
Adrenal hemorrhage

SOFT TISSUE INJURIES
petechiae and ecchymosesThe birth history, location of lesions, they are
rarely appearance without new lesions, and the
absence of bleeding from other sites help to
differentiate petechiae and ecchymoses
secondary to birth trauma from those caused by a
vasculitis or coagulation disorder.

lacerations and abrasions
It may be secondary to scalp electrodes and
fetal scalp blood sampling or injury during birth.
Deep wound may require sutures. Infection is a
risk particularly with scalp lesions and an
underlying caput succedaneum or hematoma.
Treatment includes cleansing the wound and the
close observation.

Subcutaneous fat necrosis
It is not usually recognized at birth. It
usually presents during the first 2 weeks after
birth as sharply demarcated; irregularly
shaped; firm and non pitting subcutaneous
plaques or nodules on the extremities, face,
trunk or buttocks. The injury may be colorless
or have a deep red or purple discoloration.
Calcification may occur. No treatment is
necessary. Lesions typically resolve
completely over several weeks to months.
PREVENTION OF INJURIES IN
NEWBORN
ANTENATAL PERIOD
To screen out the at risk babies likely to
be traumatized during vaginal delivery and to
employ liberal use of elective CS. Contracted
pelvis and CPD or malpresentation like
breech or transverse lie are included in the list

INTRANATAL PERIOD
Normal delivery
continous fetal monitoring to prevent traumatic
cerebral anoxia
episotomy should be done carefully
the neck should not be unduly strechted while
delivering the shoulder to prevent injuries to the
brachial plexus or sternomastoid.
Special care to the preterm to prevent anoxia,
avoid strong sedatives, liberal episiotomy and to
administer Vit K 1mg IM to prevent haemorrhage
from the traumatized site.
Forceps delivery
Difficult forceps are to be avoided in preference to the safer CS.
Never apply traction unless the application is a correct one.
Ventouse delivery
It is relatively less traumatic. But it should be avoided in preterm.
Vaginal breech delivery
Proper selection of cases and utmost care and gentleness are to be executed while conducting breech delivery. Most crucial period of breech delivery is the delivery of the after coming head.
NURSING ASSESSMENT
Recognition of trauma and birth injuries is imperative so that early treatment can be initiative.
Review the labor and birth history for risk factors, such as a prolonged or abrupt labor, abnormal or difficult presentation, cephalopelvic disproportion or mechanical forces such as forceps or vaccum used during delivery.
Also review the history for multiple fetus deliveries, large for date infants, extreme prematurity, large fetal head or newborns with congenital anomalies.
Complete a careful physical and neurologic assessment of every newborn admitted to the nursery to establish whether injuries exist.

Inspect the head for lumps, bumps or bruises.
Note if swelling or bruising crosses the suture
line.
Assess the eyes and face for facial paralysis,
observing for asymmetry of the face with crying or
appearance of the mouth being drawn to the
unaffected side.
Ensure that the newborn spontaneously moves
all extremities.
Note any absence of or decrease in the deep
tendon reflexes or abnormal positioning of
extremities.
Assess and document symmetry of structure and
function. Be prepared to assist with scheduling
diagnostic studies to confirm trauma or injuries,
which will be important in determining treatment
NURSING MANAGEMENT
Nursing management is primarily supportive
and focuses on assessing for resolution of the
trauma or any associated complications along
with providing support and education to the
parents.
Provide the parents with explanations and
reassurance that these injuries resolve with
minimal or no treatment.
Parents are alarmed when their newborn is
unable to move an extremity or demonstrates
asymmetric facial movements.
Provide parents with a realistic picture of
situation to gain their understanding and trust.

Be readily available to answer questions and
teach them how to care for their newborn,
including any modifications that might be
necessary.
Allow parents adequate time to understand the
implications of the birth trauma or injury and what
treatment modalities are needed, if any.
Provide them with information of length of time
until the injury will resolve and when and if they
need to seek further medical attention for the
condition.
Spending time with parents and providing them
with support, information and teaching are
important to allow them to make decisions and
care for their newborn.
Anticipate the need for community referral for
ongoing follow up and care, if necessary.

ICTERUS
NEONATARUM
ENTERO HEPATIC CIRCULATION
AND NORMAL BILIRUBIN
METABOLISM IN A NEWBORN 1. Source of production: Bilirubin is derived
from the breakdown of hemeproteins which are
present in hemoglobin, myoglobin and certain
heme containing enzymes. Three fourths of the
bilirubin comes from hemoglobin catabolism.
One gram of hemoglobin results in the production
of 34 mg of bilirubin. A normal term newborn
produces about 6-10 mg/kg/ day of bilirubin.
2. Metabolism
i. Bilirubin is bound to albumin for transport in
the blood. This bound bilirubin does not enter
the central nervous system and is nontoxic.
ii. Upon reaching the liver, only bilirubin enters
the liver cell and gets bound to ligandin which
helps to transport it to the site of conjugation.
iii. Conjugation occurs with glucuronic acid to
produce mono- and diglucuronides which are
water soluble.

The conjugated bilirubin is transported with
the bile to the gut. In the sterile newborn gut,
there is an enzyme called beta- glucuronidase
which converts bilirubin glucuronide into
unconjugated bilirubin which is reabsorbed
into the circulation.


DEFINITION OF
HYPERBILIRUBINEMIA
The term Hyperbilirubinemia refers to an excessive level of accumulated bilirubin in the blood and is characterized by Jaundice or Icterus, a yellowish discolouration of the skin, sclera and nails.
Hyperbilirubinemia is caused by excessive concentrations of bilirubin in blood, which can result in Jaundice.
When the bilirubin [unconjugated] level rises more than the arbitrary cut-off point of 10 mg%, the condition is called hyperbilirubinemia of the newborn

CAUSES OF
HYPERBILIRUBINEMIA
Physiological
The jaundice appears on 2nd and 3rd day and
disappears by 7-10th day, a little later in
premature neonates. In term infant the level may
be 6-8 mg /dl on the 3rd day. arise of
unconjugated serum bilirubin to 12 mg/dl in the
first week may be without any abnormality.
Causes of excessive bilirubinproduction are:
Increased red cell volume and increased red cell destruction due to shorter life span in the neonate.
Transient decreased conjugation of bilirubin due to decreased UDPG-T activity
Increased enterohepatic circulation due to decreased gut mobility.
Decreased hepatic circulation due to decreased gut motility.
Decreased hepatic excretion of bilirubin
Decreased liver cell uptake of bilirubin due to decreased ligandin
Pathological:
Excessive red cell hemolysis
Hemolytic disease of the newborn
Neonatal septicemia: specially with e-coli.
Blood extravastion: sequestration of blood
within the cavities can cause increased
bilirubin.

Defective conjugation of bilirubin
Congenital deficiency of glucuronyl
transferase
Crigler najjar syndrome[ autosomal
recessive], gilbert syndrome [autosomal
dominant], preterm babies with impaired
liver function.
Breast milk jaundice:
The enzyme glucuronyl activity of the liver
is inhibited by a specific steroid 3α,20β-
pregnanediol and increased fatty acids of
breast milk. The bilirubin level rises from
the fourth day after birth to a maximum of

Metabolic disorders:
Galactosemia, hypothyroidism may be associated
with unconjugated hyperbilirubinemia
Increased enterohepatic circulation of
unconjugated bilirubin. It is seen with
duodenal atresia, pyloric stenosis.
Substances and disorders that affect binding
of bilirubin to albumin: aspirin, sulphonamides,
fatty acids and asphyxia, acidosis, sepsis or
hypothermia increases free unconjugated bilirubin
level.
Miscellaneous: congenital obstruction, viral
hepatitis, syphilis.

PATHOPHYSIOLOGY
Bilirubin production is increased due to
increased production of erythtocytes.
Heme
Heme oxygenase
biliverdin
Disslove in water
Unconjugated biirubin[insoluble]
Bound to albumin
Transported in plasma

Reaches the liver
Bilirubin transfered to liver cells
Binds with ligandin
Ligandin concentrations are low at birth
UGPT
Bound to glucuronic acid
Conjugated bilirubin
Water soluble molecule
Excreted into bile

Physiologic Jaundice
Increased bilirubin load on the
hepatic cell
Defective uptake from plasma into
liver cell
Defective conjugation
Decreased excretion
Increased entero-hepatic circulation

Characteristics of physiological jaundice.
First appears between 24-72 hours of
age
Maximum intensity seen on 4-5th day in
term and 7th day in preterm neonates
Bilirubin level does not exceed 15 mg/ dl
Clinically undetectable after 14 days.
No treatment is required but baby should
be observed closely for signs of
worsening jaundice.

Pathological jaundice
Clinical jaundice detected before 24
hours of age
Rise in serum bilirubin by more than 5
mg/ dl/ day
Serum bilirubin more than 15 mg/ dl
Clinical jaundice persisting beyond 14
days of life
Clay/white colored stool and/or dark
urine staining the clothes yellow
Direct bilirubin >2 mg/ dl at any time

TYPES OF HYPERBILIRUBINEMIA
Conjugated Hyperbilirubinemia
Unconjugated Hyperbilirubinemia

Conjugated hyperbilirubinemia(direct)
Diseases that reduce the rate of secretion of
conjugated bilirubin into the bile or the flow of bile
into the intestine produce a mixed or
predominantly conjugated hyperbilirubinemia due
to the reflux of conjugates back into the plasma

Causes of conjugated
Hyperbilirubinemia
Infective
Viral
CMV, Rubella, Reovirus III, Hepatitis B
Bacterial
E. Coli, Listeria,
Protozoal
Toxoplasma

Inherited Causes
Galactosemia
Alpa-1 antitrypsin deficiency
Biliary Hypoplasia (Syndromic)
Cholestasis with actin and microfilament
accumulation
Progressive intrahepatic cholestasis
Iron storage disorders
Chromosomal Anomalies:
Trisomy 13
Trisomy 18
Trisomy 21

Idiopathic Causes
Biliary atresia - Neonatal Hepatitis
Choledochal cyst
Circulatory Abnormalities
Hypoxia
Anemia

Miscellaneous Causes:
TPN
Hypothyroidism
Maternal alcohol ingestion
Erythromycin estolate
Frusemide
Hemolytic disease

UNCONJUGATED
HYPERBILIRUBINEMIA
(INDIRECT)
Types:
Physiologic jaundice: It is caused due to
immature hepatic function plus increased bilirubin
load from red blood cell (RBC) hemolysis. Its
onset is after 24 hours (Preterm infants,
prolonged). It becomes peak on 72-90 hours. It
declines on 5th to 7th day.

Treatment:
Increase frequency of feedings and avoid
supplements.
Evaluate stooling pattern.
Monitor Transcutaneous bilirubin (TcB) or Total
Serum Bilirubin level.
Perform risk assessment.
Use Phototherapy, if bilirubin levels increase
significantly or significant hemolysis is present
BREAST FEEDING ASSOCIATED JAUNDICE (EARLY ONSET):
It is due to decreased milk intake related to fewer calories consumed by infant before mother’s milk is well established
It’s onset is from second to fourth day. It’s peak is from 3rd to 5th day and duration is variable.
Treatment:
Breastfeed frequently ( 10- 12 times/ day)
Evaluate stooling pattern
Perform risk assessment.
Use phototherapy if Bilirubin levels increase significantly
Assist Mother with maintaining milk supply; feed expressed milk as appropriate.
After discharge , follow up according to hour of discharge.
BREAST MILK JAUNDICE( LATE ONSET):
It is because of the possible factors in breast milk that prevent bilirubin conjugation and less frequent stooling. It’s onset is fifth to seventh day and peak from tenth to fifteenth day. It’s duration is 3-12 weeks or more.
Treatment:
Increase frequency of breast feeding
Perform risk assessment.
Consider performing additional evaluations
May include home phototherapy with a temporary (10-12 hour)
Assist mother with maintenance of milk supply and therapy.
Use formula supplements only at Practitioner’s discretion.
HEMOLYTIC DISEASE:
It is due to Blood antigen incompatibility causing hemolysis of large number of RBC’S and liver is unable to conjugate andexcrete excess bilirubin from hemolysis. Its onset is during first 24 hours (levels increase greater than 5 mg/day)
Treatment:
Monitor TSB level.
Perform risk assessment.
Postnatal- Use Phototherapy; administer intravenous immunoglobulin per protocol, if severe, perform exchange transfusion.
Prenatal – Perform Fetal Transfusion.
Rh (D) Immunoglobulin.
breast feeding
Minimize maternal – infant separation

CLINICAL FEATURES
yellow color
Drowsiness
neurologic findings, such as changes in muscle
tone, seizures, or altered cry
Hepatosplenomegaly, petechiae, and
microcephaly may be associated with hemolytic
anemia, sepsis, and congenital infections
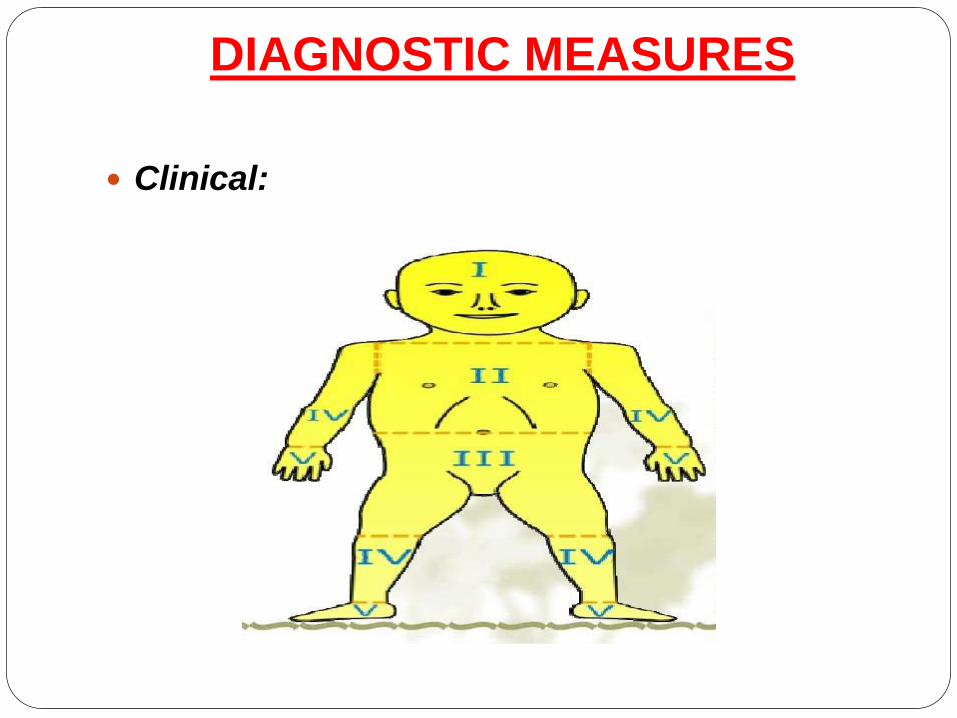
DIAGNOSTIC MEASURES
Clinical:

Laboratory studies:
Serum bilirubin level > 12 mg/dl,requires further investigations.
Total conjugated bilirubin and unconjugated bilirubin.
Complte hemogram including recticulocyte count
Hemolytic anemia: Hb decreases, recticulocyte count decreases, presence of nucleated red cells.
Polycytemia: hematocrit>65%
Sepsis: WBC count [ total or differential increases.
Hereditary spherocytosis: peripheral blood film
Blood group[ABO,Rh] status: mother and infant for ABO and Rh incompatibility.
Direct coomb’s test: for isoimmunization disorder.
Serum albumin to detect total bilirubin binding sites and to assess the need of albumin infusion.
Other laboratory investigations:
Urine for reducing substance, culture for infection
Hemoglobin electrophoresis
Osmotic fragility test
Thyroid and LFT.
Radiology and ultrasonography to detect intestinal obstruction
THERAPEUTIC MANAGEMENT:
Goals of Treatment:
To prevent Bilirubin encephalopathy and as in
any Blood group incompatibility
To reverse the hemolytic process.

PHOTO THERAPY
Phototherapy is the process of using special light toeliminate bilirubin in the blood.
Indications for Phototherapy
immaturity, acidosis, asphyxia, higher free bilirubin levels
Assessment should be Before Phototherapy:
GA Of the baby
Weight The baby
Postnatal Age
Types of Jaundice
the level of jaundice

American Academy of Pediatrics guidelines
For term healthy babies, can be followed.
2. Guidelines are provided for very low birth
weight babies. As a rough guide, Phototherapy is
indicated at a level equal to 1% of the body
weight (for e.g. 10 mg/dl in a 1000 gm baby or 15
mg/dl in a 1500 gm baby). Exchange blood
transfusion is warranted when the TSB level is 5
mg/dl higher than the phototherapy level.
However, the overall clinical situation needs to be
considered to arrive at a proper decision.

3.In case of hemolysis, start phototherapy at a
lower level.
4. Acidosis, asphyxia, hypoglycemia or sepsis
make the blood brain barrier more porous to
bilirubin. So, consider to start early phototherapy.
5. In case of prolonged jaundice (>3 wk), one
should always check fractional bilirubin
estimation. Phototherapy is contraindicated in the
presence of conjugated hyperbilirubinemia (
2mg/dl) because it may result in Bronze Baby
Syndrome.

Mechanisms in phototherapy
Phototherapy is effective because 3 reactions can
occur when bilirubin is exposed to light, as
follows:
photooxidation
Configurational isomerization
Structural isomerization
The photoisomers of bilirubin are excreted in bile
and, to some extent, in urine

Basic principles regarding
phototherapy:
Wavelength
a dose-response relationship
energy delivered to the infant's skin
the efficiency of phototherapy
the nature and character of the light source

Advantages:
Low risk of overheating the infant
No need for eye shields
Ability to deliver phototherapy with the infant in a
bassinet next to the mother's bed
Simple deployment for home phototherapy
The possibility of irradiating a large surface area
when combined with conventional overhead
phototherapy units (double/triple phototherapy)

Types of phototherapy:
Single surface phototherapy
Double surface photo therapy

Tips towards delivering safe and
effective phototherapy
1. Protect the eyes with eye patches
2. Keep the baby naked with a small nappy to
cover the genitalia
3. After switching on the unit check that all
tubes/bulbs are on
4. Place the baby as close to the lights

Encourage frequent breastfeeding. Unless there is
evidence of dehydration, supplementing
breastfeeding or providing IV fluids is unnecessary.
. Keep diaper area dry and clean
Phototherapy does not have to be continuous and
can be interrupted for feeding, clinical procedures,
and to allow maternal bonding.
Monitor temperature every 4 hours and weight every
24 hours.
Measure plasma/ serum bilirubin frequently ~ every
12 hours. Visual assessment of jaundice during
phototherapy is unreliable

EXCHANGE TRANSFUSION
The procedure involves slowly removing the
patient's blood and replacing it with fresh donor
blood or plasma.
The patient’s blood is slowly withdrawn (usually
about 5 to 20 mL at a time, depending on the
patient’s size and the severity of illness). An equal
amount of fresh, prewarmed blood or plasma
flows into the patient's body. This cycle is
repeated until the correct volume of blood has
been replaced.


Indications:
Neonatal polycythemia (dangerously high red
blood cell count in a newborn)
Rh-induced hemolytic disease of the newborn
Severe disturbances in body chemistry
Severe newborn jaundice that does not respond
to phototherapy with bili lights
Severe sickle cell crisis
Toxic effects of certain drugs.

Indications for exchange transfusion in Rh Isoimmunization.
An exchange transfusion soon after birth is indicated if:
Cord bilirubin is 5mg/dl
Cord Hb is £10 mg/dl, PCV <30
Previous sibling history and positive DCT.
Subsequent exchange transfusions are indicated if:
1. Bilirubin 10 mg/dl within 24 hours of age
2. Bilirubin15 mg/dl between 25-48 hours of age
3. Bilirubin 20 mg/dl after 48 hours of age.
4. Rate of rise of bilirubin is 0.5 mg/dl/hr.
Risks
Blood clots
Changes in blood chemistry (high or low
potassium, low calcium, low glucose, change in
acid-base balance in the blood)
Heart and lung problems
Infection (very low risk due to careful screening of
blood)
Shock if not enough blood is replaced

MAISEL'S CHART
It is used for taking decision regarding
treatment in cases of pathological jaundice. In
presence of any of the following, treat as in
next higher bilirubin category.
Perinatal asphyxia
Respiratory distress
Metabolic acidosis
Hypothermia
Low serum protein
Birth weight <1500 g
Signs of clinical or CNS deterioration


PHARMACOLOGIC
MANAGEMENT
Phenobarbital Therapy
Intravenous Immunoglobulins -0.5 to1 gm/kg
Pharmacologic Therapy:
Zinc/Metalloporphyrin
Ursodeoxycholic acid

COMPLICATIONSAcute bilirubin encephalopathy may include the
following neurologic symptoms:
Extra pyramidal movement disorders
Gaze abnormalities
Lethargy
Auditory disturbances (sensorineural hearing loss)
Hypo or hypertonia, truncal arching
Seizures
Coma
Death

Kernicterus (chronic bilirubin encephalopathy)
may include the following symptoms:
Severe cerebral palsy
Auditory dysfunction
Dental enamel dysplasia
Paralysis of upward gaze

PREVENTION
Pregnancy, labour and delivery
Test all pregnant women for ABO, Rh (D) blood types and red cell antibodies,1,2 during
pregnancy
If the mother has red blood cell antibodies noted antenatally then send cord blood
If the mother has not had antenatal blood tests send:
maternal blood for blood group (ABO/Rh) AND
baby’s cord blood for blood group ,Rh type and DAT
Umbilical cord blood total serum bilirubin, haemoglobin or haematocrit measurements do not aid in the prediction of severe hyperbilirubinaemia

Breastfeeding
Encourage all mothers to breastfeed their babies
8 - 12 times a day in the first 2 - 3 days of life.
Encourage the ingestion of colostrum to increase
stooling which prevents reabsorption of bilirubin.
Supplementation with water does not affect
bilirubin levels and is not recommended. If
supplementation is necessary due to inadequate
intake then give expressed breast milk and/or
formula
Educate parents regarding signs of adequate
hydration, feeding and signs of jaundice

NURSING MANAGEMENT
Assessment of jaundice
Colour
Hydration
Other illness
Feeding

NURSING DIAGNOSIS
Deficient Fluid Volume related to inadequate fluid
intake, photo-therapy, and diarrhea.
Hyperthermia related to the effects of
phototherapy
Impaired skin integrity related to
hyperbilirubinemia and diarrhea
Anxiety related to medical therapy given to the
baby.
Follow up
Babies discharged before 48 hours may need 2
follow up visits, the first visit between 24 - 72
hours and a second between 72 - 120 hours.
Follow up assessment must include:
• baby’s weight and percentage change from birth
weight
• adequacy of intake
• voiding and stooling pattern
• presence or absence of jaundice
• clinical judgement to determine the need for total
serum bilirubin level measurement

THANK YOU…
Related Documents