
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


CARDIOVASCULAR DISORDERS
LECTURER: ABDIAZIZ SH: FARAH

HYPERLIPIDEMIA❶ The risk of atherosclerosis is directly related to increasing levels of serum cholesterol.
Hypercholesterolemia (elevation in serum cholesterol) and other abnormalities in serum lipids play a major role in plaque formation leading to coronary heart disease (CHD) as well as other forms of atherosclerosis, such as carotid and peripheral artery disease (atherosclerosis of the peripheral arteries). This predictive relationship has been demonstrated from large epidemiologic,1 animal, and genetic studies. Coronary heart disease is the leading cause of death in both men and women in the United States and most industrialized nations.
It is also the chief cause of premature, permanent disability in the United States work force.
Annually, approximately 700,000 Americans will suffer a new heart attack and 500,000 will have a recurrent event.
The average age of a first heart attack is 66 years for American men and 70 years for women. The direct and indirect cost of CHD to the United States economy is almost $140 billion.

PATHOPHYSIOLOGYLipid and Lipoprotein Metabolism
Cholesterol is an essential substance manufactured by most cells in the body. Cholesterol is used to maintain cell wall integrity and for the biosynthesis of bile acids and steroid hormones. Other major lipids in our body are triglycerides and phospholipids. Since cholesterol is a relatively water-insoluble molecule, it is unable to circulate through the blood alone.
Cholesterol along with triglycerides and phospholipids are packaged in a large carrier-protein called a lipoprotein (Fig. 9–1). Lipoproteins are water soluble, which allows transportation of the major lipids in the blood. These lipoproteins are spherical and vary in size (~1,000 to 6 nm) and density (less than 0.94 to 1.21 g/mL)4 (Table 9–1).
PATHOPHYSIOLOGYThe amount of cholesterol and triglycerides vary by lipoprotein size. The major lipoproteins in descending size and ascending density are chylomicrons, very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), and high-density lipoprotein (HDL).
When clinical laboratories measure and report serum total cholesterol, what they are measuring and reporting are total cholesterol molecules in all the major lipoproteins. The estimated value of LDL cholesterol is found using the following equation:

Conditions Associated with Angina

PATHOPHYSIOLOGYThe determinants of oxygen supply and demand are shown in Fig. 4–1. Increases in heart rate, left ventricular wall tension, and cardiac contractility increase the rate of myocardial oxygen consumption (MVO2). Left ventricular wall tension is a function of blood pressure, left ventricular end-diastolic volume, and ventricular wall thickness.
Physical exertion increases heart rate, blood pressure, and cardiac contractility, and commonly precipitates ischemia and symptoms of angina in patients with significant coronary atherosclerosis.
Medications that reduce heart rate, cardiac contractility, and/or ventricularwall tension are commonly prescribed to prevent ischemicsymptoms in patients with chronic stable angina.


Coronary AtherosclerosisThe normal arterial wall consists of the intima, media, and adventitia, as illustrated in Fig. 4–3A. The endothelium is located in the intima and consists of a layer of endothelial cells that line the lumen of the artery and form a selective barrier between the vessel wall and blood contents. The internal elastic lamina separates the intima and media, where vascular smooth muscle cells are found. The vascular adventitia comprises the artery’s outer layer. Atherosclerotic lesions form in the sub endothelial space between the endothelial cells and internal elastic lamina.
Dysfunction of the endothelium allows lipoproteins, predominantly low-density lipoprotein (LDL) cholesterol, and inflammatory cells, namely monocytes and T lymphocytes, to migrate from the plasma to the sub-endothelial space.Monocyte-derived macrophages ingest lipoproteins to form foam cells. Macrophages also secrete growth factors that promote smooth muscle cell migration from the media to the intima.




A fatty streak consists of lipid-laden macrophages and smooth muscle cells and is the earliest type of atherosclerotic lesion.Lipid-laden macrophages, smooth muscle cells, and necrotic debris from the death of foam cells accumulate in the sub endothelial space, leading to enlargement of the fatty streak. A collagen matrix forms a fibrous cap that covers the lipid core of the lesion to establish a fibrous plaque called an atherosclerotic plaque. Initially, the diameter of the coronary artery lumen is maintained as the plaque grows outward (external to the lumen) in a process referred to as arterial remodeling.9 However, with significant plaque progression, the atherosclerotic plaque begins to protrude into the artery lumen and impede blood flow.
When the plaque occludes 70% or more of the artery, the patient may begin to experience angina during activities that increase myocardial oxygen demand (i.e., chronic stable angina).

Other causes of pathophysiology
Stable versus Unstable Atherosclerotic Plaques
Atherosclerotic Plaque Rupture
Coronary Artery Vasospasm




Distinguishing Characteristics of Chronic StableAngina and Unstable AnginaChronic stable angina should be distinguished from unstable angina since the latter is associated with a greater risk for MI and death and requires more aggressive treatment. Because the pathophysiology of chronic stable angina is due primarily to increases in oxygen demand, not acute changes in oxygen supply, symptoms are typically reproducible and reversible.Specifically, a patient will generally experience a similar pattern ofdiscomfort (i.e., same quality, location, and accompanying symptoms) with a similar level of exertion with each angina attack.Chronic stable angina is usually relieved within minutes by restor sublingual nitroglycerin.

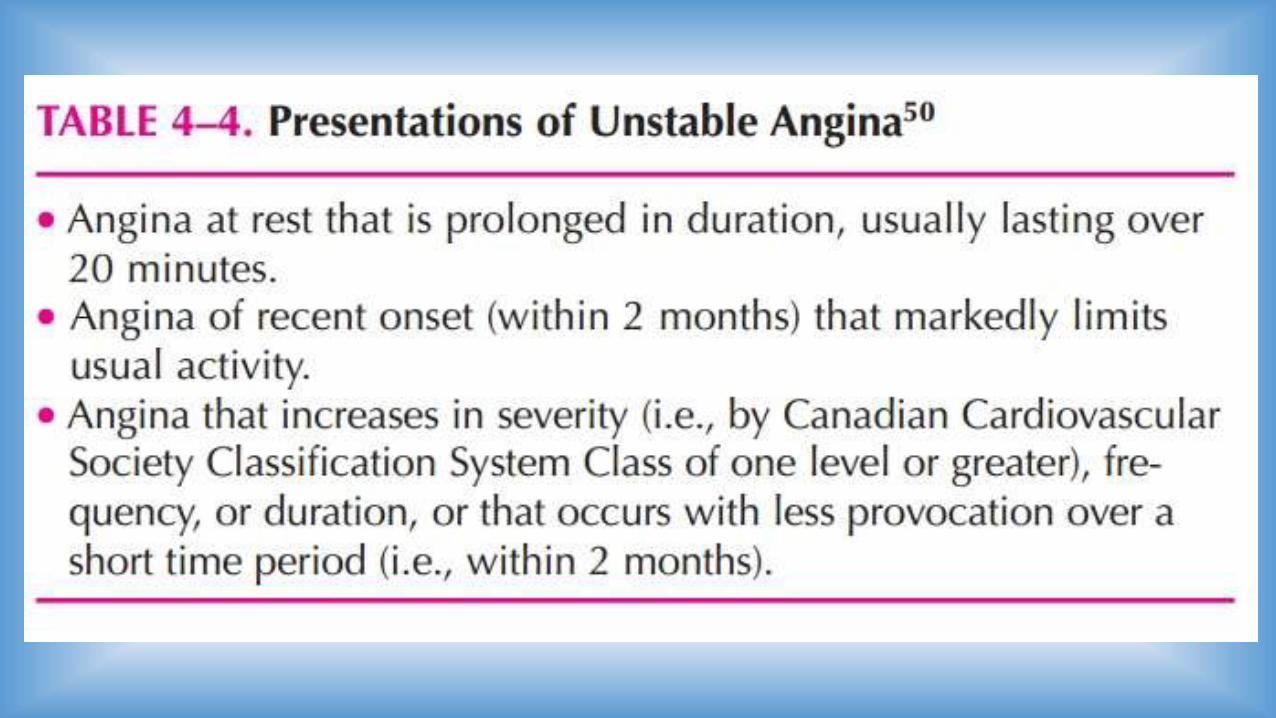
In contrast, unstable angina is due to an acute decrease in coronary blood flow leading to insufficient oxygen supply. Consequently, unstable angina is marked by prolonged symptoms (greater than or equal to 20 minutes) or an escalation in the frequency or severity of angina over a short period of time. Unstable angina frequently occurs at rest withoutany precipitating factors, whereas chronic stable angina usually occurs with exertion. Unstable angina may be less responsive torest or medication.
The presentation of unstable angina is described in greater detail in Table 4–4.

TREATMENT
Desired Outcomes
Once the diagnosis of IHD is established in a patient, the clinician should provide counseling on lifestyle modifications,institute appropriate pharmacologic therapy, and evaluate the
need for surgical revascularization. ❹ The major goals for thetreatment of IHD are to:
• Prevent acute coronary syndromes and death;• Alleviate acute symptoms of myocardial ischemia;
• Prevent recurrent symptoms of myocardial ischemia; and• Avoid or minimize adverse treatment effects.



Percutaneous Coronary Intervention
Coronary Artery Bypass Graft Surgery

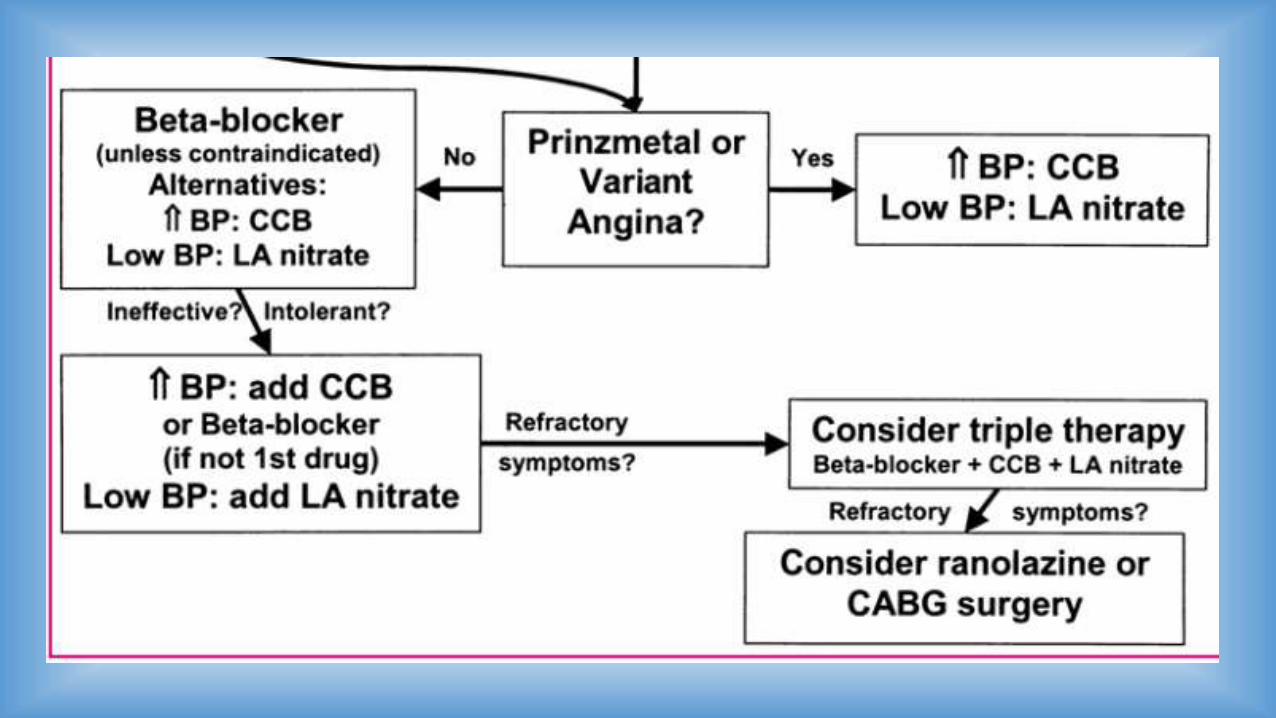
Pharmacologic Therapy





REFERNCE
pharmacotherapy_principles 2007-mcgraw-hill

DHAMAAD
Related Documents











