EFSUMB – European Course Book Editor: Christoph F. Dietrich Ultrasound in tropical medicine. Human Immunodeficiency Virus (HIV) Infection Tom Heller 1 , Enrico Brunetti 2 , Maria Teresa Giordani 3 , Rosie Conlon 4 , Carlo Filice 2 , Sam Goblirsch 5 , Christoph F. Dietrich 6 1 Hlabisa Hospital, Kwazulu-Natal, South Africa 2 Department of Infectious Diseases, University of Pavia, San Matteo Hospital Foundation 3 Infectious and Tropical Diseases Unit, San Bortolo Hospital, Vicenza, Italy 4 National Rehabilitation Hospital, Dun Laoghaire, Co Dublin, Ireland 5 Department of Medicine and Pediatrics, University of Minnesota, Minneapolis, MN, USA 6 Caritas-Krankenhaus Bad Mergentheim, Germany

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EFSUMB – European Course Book
Editor: Christoph F. Dietrich
Ultrasound in tropical medicine. Human
Immunodeficiency Virus (HIV) Infection
Tom Heller1, Enrico Brunetti
2, Maria Teresa Giordani
3, Rosie Conlon
4, Carlo
Filice2, Sam Goblirsch
5, Christoph F. Dietrich
6
1Hlabisa Hospital, Kwazulu-Natal, South Africa 2Department of Infectious Diseases, University of Pavia, San Matteo Hospital Foundation 3Infectious and Tropical Diseases Unit, San Bortolo Hospital, Vicenza, Italy 4National Rehabilitation Hospital, Dun Laoghaire, Co Dublin, Ireland 5Department of Medicine and Pediatrics, University of Minnesota, Minneapolis, MN, USA 6Caritas-Krankenhaus Bad Mergentheim, Germany
Content
Content ....................................................................................................................................... 2
Introduction ................................................................................................................................ 2
Liver ........................................................................................................................................... 3
Diffuse pathologies ................................................................................................................ 3
Focal pathologies .................................................................................................................... 3
Gallbladder and bile ducts .......................................................................................................... 5
Spleen ......................................................................................................................................... 6
Pancreas ...................................................................................................................................... 8
Kidney ........................................................................................................................................ 9
Gastrointestinal tract ................................................................................................................ 11
Ascites ...................................................................................................................................... 11
Lymph nodes ............................................................................................................................ 12
Parotid ...................................................................................................................................... 13
Heart ......................................................................................................................................... 13
Tuberculosis ............................................................................................................................. 13
Pericarditis ............................................................................................................................ 14
Pleuritis ................................................................................................................................. 15
Peritonitis ............................................................................................................................. 16
Disseminated abdominal infection (lymph nodes and spleen) ............................................. 17
Liver ..................................................................................................................................... 18
Gastrointestinal tract ............................................................................................................ 18
Renal and urinary tract ......................................................................................................... 20
References ................................................................................................................................ 21
Introduction
Infection with human immunodeficiency virus (HIV) is a major cause of morbidity and
mortality in tropical countries, especially sub-Saharan Africa. In untreated infection,
destruction of CD4 T-helper lymphocytes leads to an increasing degree of immune
suppression, especially when the CD4 counts fall below 350 cells/mm3. When CD4 falls
below 200 cells/mm3, opportunistic infections and malignancies affect the patient who is then
defined as having acquired immunodeficiency syndrome (AIDS).
Ultrasound can be used to diagnose a wide array of diseases and infections in various organ
systems [(1, 2)]. It is also widely used to guide diagnostic needle biopsies for histological or
microbiological investigations.
This chapter is an overview of ultrasound findings that may be seen in the organs of patients
with HIV.

Liver
Diffuse pathologies
Hepatomegaly is one of the most frequent findings in patients who are HIV-positive, and was
found in up to 35% of patient screened in the Congo and Zambia [(3)]. Causes of
hepatomegaly in HIV-positive patients are numerous, but the most frequent are concomitant
hepatitis B and C virus infections, cytomegalovirus (CMV) infections, granulomatous
hepatitis e.g. due to Mycobacterium tuberculosis, atypical mycobacteria (mycobacterium
avium complex-MAC- M. kansasii) infections and diffuse lymphomatous infiltration. Often
no specific cause of hepatomegaly is found. Ultrasound-guided liver biopsy helps to narrow
the differential diagnosis. Lymph nodes are detectable within the hepatoduodenal ligament in
almost all patients with chronic HIV. Enlarged lymph nodes can be found in HIV-positive
patients with or without chronic virushepatitis C [(4)] and other inflammatory liver diseases
but also in lymphoma [Figure 1].
Figure 1 Enlarged perihepatic lymph nodes in the dorsal hepatoduodenal ligament (in between
markers) in a HIV-positive patient finally with the diagnosis of chronic virushepatitis C
and hepatic tuberculosis. For more details of perihepatic lymphadenopathy with and
without HIV, see chapter on the Liver.
Focal pathologies
Focal pathologies of the liver are common findings in patients with HIV. The echo-pattern of
the liver lesions may be described as hypoechoic, hyperechoic or of mixed echogenecity.

Diseases commonly presenting with hypoechoic liver lesions are lymphoma, M. tuberculosis
infection and abscesses.
AIDS-related lymphomatous lesions may vary in size from a few to several centimetres
[Figure 2], and in some instances they may appear echo-free and can be confused with cystic
lesions [Figure 3].
Figure 2 Complex lesion in the left lobe of the liver in a patient with HIV: lymphoma.
Figure 3 Round hypoechoic lesion in the liver of a patient with AIDS during fine-needle
biopsy: lymphoma.
Bacterial abscesses often show irregular borders and may contain small gas bubbles. Fungal
micro-abscesses can have a bull-eye appearance; in particular, this morphology has been
described in disseminated Candida albicans infections.

Disseminated Kaposi’s sarcoma (KS) presents with hyperechoic, disseminated lesions, 5–10
mm in size, which can be found even in the absence of cutaneous lesions. In larger KS
lesions, a complex echo-pattern with hyper- and hypoechoic areas is observed.
Small hyperechoic liver lesions are seen in disseminated MAC and Pneumocystis jirovecii
infections. Bacillary peliosis or bacillary angiomatosis is characterized by cystic, blood-filled
vasoproliferative lesions and spaces in the liver. This is linked to opportunistic infection with
Bartonella henselae and has a sonographic appearance of multiple hyperechogenic
hypervascular liver lesions [(5)]. Multiple, diffuse small echogenic lesions in the liver or
spleen are seen as a “snowstorm pattern”. Although this has been initially described with P.
jrovecii infections, other organisms such as Candida and Aspergillus can be a cause.
Histological features include foci of calcification, but their frequency is not sufficient to
explain the multiple echogenic foci. The interfaces caused by the fibrosis could be largely
responsible for the snowstorm appearance [(6)]. Fine-needle biopsy is used to determine the
diagnosis.
Gallbladder and bile ducts
Gallbladder wall thickening is a frequent finding in patients with HIV; however, in the
majority of patients this is an incidental finding. A thick-walled and distended gall bladder,
which shows the “sonographic Murphy’s sign” (tenderness on probe pressure in the
gallbladder area), may point to cholecystitis. In contrast to immune-competent individuals,
this may develop in the absence of gallstones (“acalculous cholecystitis”) [Figure 4].
Gallbladder thickening is a short-life sonographic phenomenon of early phase acute hepatitis
in approximately 50% of patients. This must not be confused with acute cholecystitis where
there is no circumscript pain under ultrasound visualized palpation [(7)].

Figure 4 Gallbladder thickening in emphysematous cholecystitis in a HIV-positive patient.
Air within the wall is indicated by the arrow.
Irregular or smooth dilatation of intrahepatic bile ducts and concentric thickening of the intra-
and extrahepatic biliary tree (sclerosing cholangitis) may be seen in patients with HIV.
Extrahepatic strictures, as well as papillary stenosis, have been described. Biliary-tract
infections can be caused by various organisms, but cryptosporidia and CMV are the most
frequently reported.
Spleen
Splenomegaly is found in about a third of patients with HIV in Africa [(3)]. This can be a
non-specific finding in general infection, but can also be accompanied by diffuse echogenic
infiltration e.g. lymphoma.
Focal lesions can be due to infections such as pyogenic abscesses (generally hypoechoic)
[Figure 5], mycobacterial micro-abscesses (hypoechoic) [Figure 6] or toxoplasmosis
(calcifications of a few millimetres in size with a posterior acoustic shadow).

Figure 5 Hypoechoic lesions in the spleen with a possible mycobacterial aetiology.
Figure 6 Tuberculosis of the spleen with small hypoechoic lesions in a HIV-positive patient.
Similar images can be seen in other infectious (fungal) disease, hemophagocytosis-
syndrome and lymphoma.
The snowstorm pattern has also been described (see liver section). The most frequent
neoplastic focal lesions of the spleen are lymphomas, commonly hypoechoic, ill-defined
lesions of varying size. Contrast enhanced ultrasound is helpful in delineating small
infiltrations including hemophagocytosis lesions [(8)] and extramedullary hematopoesis
[Figure 7].
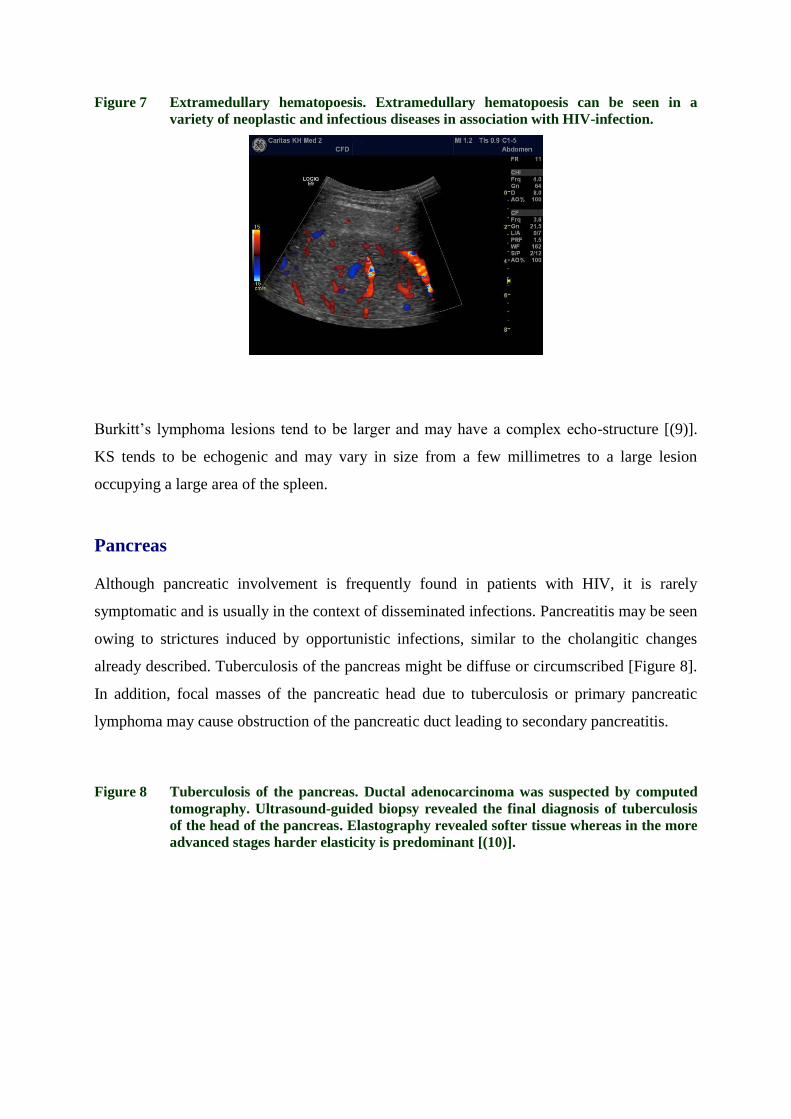
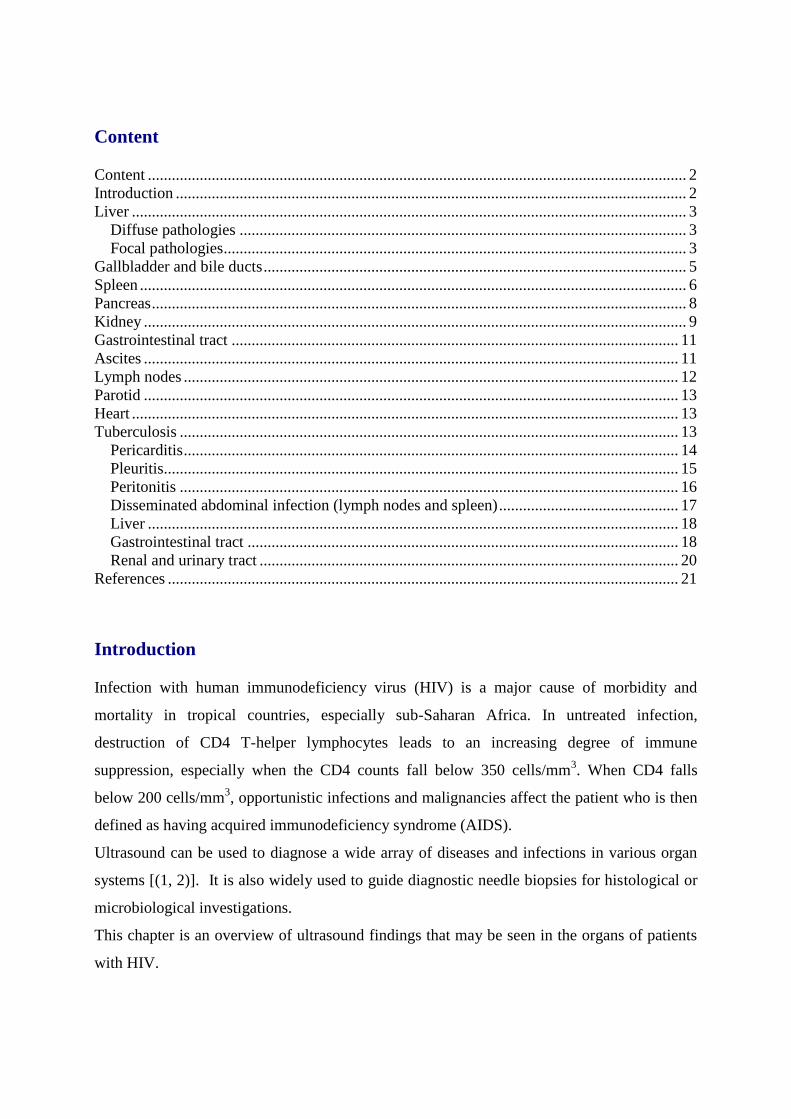
Figure 7 Extramedullary hematopoesis. Extramedullary hematopoesis can be seen in a
variety of neoplastic and infectious diseases in association with HIV-infection.
Burkitt’s lymphoma lesions tend to be larger and may have a complex echo-structure [(9)].
KS tends to be echogenic and may vary in size from a few millimetres to a large lesion
occupying a large area of the spleen.
Pancreas
Although pancreatic involvement is frequently found in patients with HIV, it is rarely
symptomatic and is usually in the context of disseminated infections. Pancreatitis may be seen
owing to strictures induced by opportunistic infections, similar to the cholangitic changes
already described. Tuberculosis of the pancreas might be diffuse or circumscribed [Figure 8].
In addition, focal masses of the pancreatic head due to tuberculosis or primary pancreatic
lymphoma may cause obstruction of the pancreatic duct leading to secondary pancreatitis.
Figure 8 Tuberculosis of the pancreas. Ductal adenocarcinoma was suspected by computed
tomography. Ultrasound-guided biopsy revealed the final diagnosis of tuberculosis
of the head of the pancreas. Elastography revealed softer tissue whereas in the more
advanced stages harder elasticity is predominant [(10)].

Kidney
Focal-segmental glomerulosclerosis is the most frequent renal pathology found on ultrasound.
The kidneys are typically normal or increased in size and the parenchyma is hyperechoic
[Figure 9]. This appearance is non-specific and can be seen in other renal diseases such as
diabetic glomerulosclerosis or other forms of chronic glomerulonephritis. The sonographic
finding should prompt an assessment of proteinuria. In some cases renal biopsy might be
indicated to determine the exact diagnosis.
Figure 9 Hyperechogenic kidney in a patient with AIDS.
Nephrocalcinosis with circumscribed renal calcifications might be seen in generalised MAC
and histoplasmosis infections, as well as patients taking medication such as sulfadiazine,
acyclovir and in particular indinavir, which can induce renal stone-like structures. Abscess
formation is typical in tuberculosis [Figure 10].
Retroperitoneal masses like lymphadenopathy can obstruct the ureters and result in
hydronephrosis.
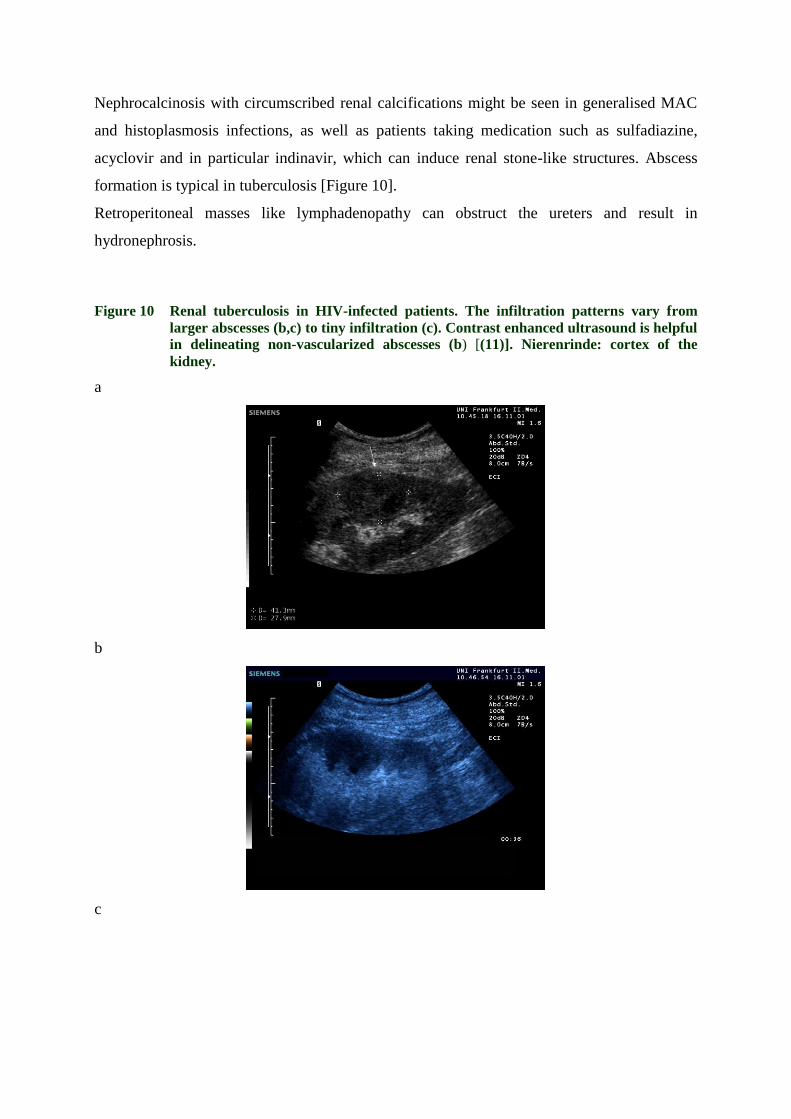
Figure 10 Renal tuberculosis in HIV-infected patients. The infiltration patterns vary from
larger abscesses (b,c) to tiny infiltration (c). Contrast enhanced ultrasound is helpful
in delineating non-vascularized abscesses (b) [(11)]. Nierenrinde: cortex of the
kidney.
a
b
c

Gastrointestinal tract
The intestinal tract is particularly prone to opportunistic infections owing to its large surface
area and the presence of lymphoid tissue in the bowel wall. Inhomogeneous masses may be
observed, but commonly the pathology presents as thickened (up to 2cm) hypoechoic bowel
wall that is similar to that seen in colitis. Often a central hyperechoic, gas-containing lumen is
visible (“target sign”). Rare intestinal diseases in HIV-positive patients have been described
[(12) (13)].
Again, there is a wide differential diagnosis, including opportunistic infections and
neoplasms. Endoscopy may be used to obtain diagnostic tissue samples, but because of the
submucosal location of the lesions this does not always allow diagnosis. Percutaneous
ultrasound-guided biopsy of the bowel wall was shown to be a safe way to obtain tissue
samples [(14)].
Ascites
Ascites is a relatively common finding that is encountered in up to 1 in 5 patients in some
African studies [(3)]. Ascites may be due to portal hypertension, especially in co-infected
patients (with hepatitis C or B virus) or those with alcoholic liver disease.
Exudates may be due to infections or tumours and numerous causes have been described.
Ultrasound helps to identify even small amounts of intraperitoneal fluid and can assist
paracentesis. Microbiological culture and PCR (polymerase chain reaction) may yield results

of M. tuberculosis, MAC and CMV, but in rare cases organisms such as C. albicans,
Cocciodiodes immitis, P jirovecii, T. gondii and Encephalitozoon cuniculi have been found.
Malignant ascites is seen less frequently and should be suspected in culture-negative
exudative peritoneal fluid. KS and lymphoma should be considered.
Primary effusion lymphoma associated with human herpes virus 8 (HHV-8) is a subgroup of
AIDS-related B-cell lymphoma affecting body cavities in patients with HIV.
Lymph nodes
Enlarged lymph nodes are frequently seen in patients with HIV and imply a wide differential
diagnosis. Intra-abdominal lymph nodes larger than 1.5 cm are commonly considered
pathological, and are often round and plump and can occasionally become very large [Figure
11].
Figure 11 Enlarged lymph nodes encasing the coeliac axis, common hepatic artery and splenic
artery (transverse section).
Often the nodes appear hypoechoic and have a disrupted architecture with absence of the
“hilum fat sign” and, sometimes, have liquid, necrotic areas. The differential diagnosis
includes tuberculosis, MAC, toxoplasmosis, CMV, as well as generalised KS and lymphoma.
Castleman’s disease is another lymphoprolipherative disease associated with HHV-8 in HIV
patients presenting with fever and lymphadenopathy. Ultrasound-guided fine-needle biopsy
can often help make a diagnosis.

Parotid
5–10% of patients with HIV-1 infection have parotid swellings, most commonly due to cystic
lymphoepithelial lesions of the salivary gland. Sonographic examination shows unilaterally or
bilaterally enlarged glands with cystic lesions. The size of the sonolucent areas may vary from
a few millimetres to a few centimetres, cyst number varies from a single cyst to numerous and
represent lymphoepithelial cysts, intraparotid lymphadenopathies and parenchymal
lymphoproliferation [(15)].
If necessary, the diagnosis can be confirmed through fine-needle aspiration, treatment
modalities include simple aspiration, surgical resection or radiotherapy; most cases that are
treated with antiretroviral therapy show regression.
Heart
HIV-associated cardiomyopathy is reported in 9–57% of patients who are HIV-positive in
Africa [(16)]. Variation in study design, population and a lack of a clear definition for
cardiomyopathy may account for this wide range.
If biopsies are obtained in these patients, myocarditis due to T. gondii, C. neoformans and M.
avium intracellulare have been shown; cardiotropic viruses are seen more frequently in
developed countries.
A direct HIV-associated cardiac inflammation is also common. A relationship between the
degree of immunosuppression and the likelihood of cardiomyopathy seems to exist;
antiretroviral therapy prevents immunosuppression, but it is unclear whether it reverses
cardiomyopathy.
Abdominal sonographic views may show the typically enlarged, dilated ventricle (diastolic
diameter more than 5.5 cm) with globally reduced contractility; this may prompt further
investigation by echocardiography.
Tuberculosis
Infections with M. tuberculosis commonly affect the lungs and are diagnosed by a chest
radiography as well as by sputum microscopy (acid-fast bacilli, AFB) and culture.
Nevertheless, because this is a systemic disease, extrapulmonary manifestations are seen
regularly and in cases of concomitant HIV infection these are even more frequent.

As material for microscopy and culture is not readily obtainable in extrapulmonary
tuberculosis (EPTB), diagnosis often depends on aspiration of suspicious fluids or on clinical
case definitions in high prevalence settings.
Ultrasound helps to provide significant information that leads to diagnosis and treatment
[(17)]. Standard treatment for all forms of EPTB is similar to pulmonary tuberculosis (TB);
usually 4 antibiotics (rifampicin, isoniazid, ethambutol and pyrazinamid) are given for 2
month followed by 4 month of rifampicin and isoniazid.
Pericarditis
TB pericarditis is one of the acutely life-threatening manifestations of EPTB owing to the
possibility of cardiac tamponade [(18)]. It is the most common cause of pericarditis in Africa,
in a South African series TB pericarditis accounted for up to 70% of cases referred for
diagnostic pericardiocentesis [(19)] [Figure 12].
Figure 12 Enlarged cardiac silhouette on a chest radiograph in tuberculosis pericarditis.
TB pericarditis usually develops by retrograde lymphatic spread of M. tuberculosis from
peribronchial or mediastinal lymph nodes; the immune response to viable acid-fast bacilli
penetrating the pericardium is responsible for morbidity.
Non-specific signs and symptoms such as fever, night sweats and weight loss are observed,
and chest pain, a cough and breathlessness are common.
In African patients, chronic cardiac compression mimicking congestive heart failure is
another common presentation.

Sonographically, two forms of disease can be differentiated: pericardial effusion and
constrictive pericarditis. Effusion is characterized by a large, anechoic-rim around the heart; it
should be assessed if the effusion impairs the normal filling of the right ventricle or atrium,
which would suggest cardiac tamponade [Figure 13].
Figure 13 Massive pericardial effusion seen on ultrasound (curvilinear probe).
Often a thickened pericardium with fibrinous strands and exudative coating material are
observed floating in the effusion. If aspirated, the effusion is typically exudative and may
yield positive results in mycobacterial culture or PCR. At the same time AFB should be
looked for in sputum. In cases of constrictive pericarditis a thick fibrinous exudate is seen in
the pericardial sac, which is associated with reduced movement of the surface of the heart.
The pericardial exudate condenses into a thick skin surrounding the heart, and this can usually
be distinguished from the myocardium [(20)].
Corticosteroids may be given in addition to antibiotic treatment, although their impact on
outcome is still controversial. In any case, a statistically non-significant, but potentially large
reduction in mortality was observed in one randomised trial [(21)] and patients experience a
more rapid clinical improvement, therefore we prescribe it for 6 weeks, especially in cases
with tamponade.
Pleuritis
The pleura may be affected by TB in different ways:
Effusion that develops usually a few months after primary infection (hypersensitivity
reaction).

Effusion developing as a result of lung disease in older adults, which might develop
into purulent effusion (empyema).
Rupture of a cavity and escape of bacteria and air into the pleural space, from which
empyema and pyopneumothorax may result.
Complicating miliary TB that involves polyserositis.
In all of the above, effusions can be observed sonographically, and fibrin strands may be seen
[(22)]. Ultrasound may guide aspiration, and if a total white blood cell count higher than 500
cells/mm3 and protein more than 2.5g/dl are found in the aspirate, empyema can be diagnosed.
This can be further differentiated clinically between “thin empyema” (possible to mobilize
through cannula) and “thick empyema” (which may need a transthoracal drain to be
mobilized). Antibiotic therapy is highly effective.
Peritonitis
TB peritonitis is probably caused by haematogenous spread and reactivation of long-latent
foci or mesenteric lymph nodes [(23)], but contiguous spread from bowel or fallopian tube is
also possible. Ultrasound findings are ascites (clear or complex), fixed membranes, septae,
strands, floating debris, omental thickening (“omental cake”), thickened mesentery and
abdominal lymphadenopathy [Figure 14].
Figure 14 Circumscribed peritoneal thickening in a HIV-positive patient with peritoneal
tuberculosis.

Ascites is usually straw-coloured, sometimes (10% of cases) blood stained, protein content is
usually more than 2.5 g/dl and leukocytes with lymphocytic predominance can be seen. Direct
microscopy is usually AFB negative, cultures are also only positive in approximately 20% of
cases. Laparoscopy-guided peritoneal biopsy has a higher diagnostic yield but is more
invasive. “Blind” peritoneal biopsy using a endoscopy biopsy forceps has been successfully
used as an alternative [(24)].
Disseminated abdominal infection (lymph nodes and spleen)
HIV positive patients may present with disseminated abdominal TB, affecting abdominal
lymph nodes and the spleen. Signs and symptoms are usually weight loss, abdominal pain and
diarrhoea. Abdominal lymph node enlargement and ascitis are the most common findings, and
hypoechoic lesions of the spleen are seen in about 50% of patients. [Figure 15]. These
represent “miliary” micro-abscesses, although patients frequently show no miliary pattern on
a chest radiograph [(25)].
These splenic hypoechogenic foci may suggest M. tuberculosis infection rather than non-
tuberculous mycobacteria, as they are rarely seen in the latter. A marked lymphadenopathy is
far more frequent in TB cases.
Figure 15 Hypoechogenic tuberculous nodules seen with a linear probe in the lower splenic
pole.

Liver
Involvement of the liver in TB is common (up to 80% in autopsies of PTB), while clinical
manifestations of this involvement are not.
Sonographically, two forms exist: an enlarged liver with a homogenous bright echo-pattern
points towards hepatic granulomatous disease (often wrongly described as granulomatous
hepatitis when the liver cells are unaffected). The diagnosis is reached by ultrasound-guided
liver biopsy.
Focal tuberculomas present as “abscess-like” masses, which are usually hypoechoic, may be
single or multiple and may vary in size from 0.5–12 cm. Tuberculosis infection may present
with an enormous heterogeneity [Figures 16]. It should be noted that these lesions (as all
tuberculous lesions) during successful treatment can initially increase in size as the improved
immunological response increases the inflammatory reaction. This does not point to treatment
failure and it should be observed.
Figure 16 Tuberculosis of the liver with granulomatous infiltration of the liver parenchyma
and bile ducts (in between markers).
Gastrointestinal tract
Although tuberculosis can involve any region of the gastrointestinal tract, in about 90% of
cases it affects the ileocoecal valve, and the adjacent ileum and colon [(17)]. Sonographic
appearance in most patients is a heterogenous and asymmetric bowel-wall thickening with
typical intramural necrosis [Figure 17], often with mesenteric enlargement of regional lymph
nodes and the so-called white bowel appearance [(26)] [Figure 18]. In some cases matted

masses are observed, which represent conglomerates of thickened bowel loops, thickened
mesentery, abscess formation [Figure 19], complex ascites and enlarged lymph nodes.
Figure 17 Gastrointestinal tuberculosis in a HIV-positive patient with intramural abscess
formation in between markers.
Figure 18 Gastrointestinal tuberculosis in a HIV-positive patient with complex inflammation
of the lymphatic vessels resulting in so-called white bowel. App: Appendix. Coe:
coecum.

Figure 19 Gastrointestinal tuberculosis in a HIV-positive patient with complex infiltration,
fistula (arrow) and abscess (abs) formation (panoramic imaging).
Renal and urinary tract
Genito-urinary TB is seen more commonly in Caucasians than in Africans patients. The
pathogenesis involves the haematogenous spread of M. tuberculosis followed by seeding in
the renal cortex in which a high oxygen tension exists. During reactivation, granuloma form
that spread into the medulla and can lead to necrosis of renal papillae, and renal obstruction
may occur. Bacilluria can lead to ureter and bladder involvement with fibrosis and reflux.
Sonography may show renal calcifications, papillary irregularities and intrarenal masses.
Hydronephrosis due to strictures, thickening and dilatation of the ureter and bladder
abnormalities (wall thickening and masses) may also be seen [(27)]. Diagnosis is usually
made with a urine culture.
Scrotal involvement in the form of a swelling due to “cold abscesses” in the epididymis and
testis are well described. Focal areas of decreased echogenicity can be demonstrated on
ultrasound. Differentiation from tumours may be difficult, so image-guided aspiration is often
needed.
Patients with TB involvement of the female genital tract often present with chronic pelvic
pain, infertility and vaginal bleeding. Most patients have abnormal hystrosalpingograms with
endometrial adhesions, fallopian tube constrictions and small calcifications in the adnexal
area. Ultrasound may show tubo-ovarian abscesses, extension of these collections to
extraperitoneal areas can suggest TB, so often the diagnosis is made by aspiration and
microbiological investigation of the material [(28)].

References
1. Brunetti E, Brigada R, Poletti F, Maiocchi L, Garlaschelli AL, Gulizia R, et al. The
current role of abdominal ultrasound in the clinical management of patients with AIDS.
Ultraschall Med2006 Feb;27(1):20-33.
2. Kawooya MG, Muyinda Z, Byanyima R, E KM. Abdominal Ultrasound Findings in
HIV Patients: a Pictorial Review. Ultrasound2008;16(2):62-72.
3. Tshibwabwa ET, Mwaba P, Bogle-Taylor J, Zumla A. Four-year study of abdominal
ultrasound in 900 Central African adults with AIDS referred for diagnostic imaging. Abdom
Imaging2000 2000 May-Jun;25(3):290-6.
4. Dietrich CF, Lee JH, Herrmann G, Teuber G, Roth WK, Caspary WF, et al.
Enlargement of perihepatic lymph nodes in relation to liver histology and viremia in patients
with chronic hepatitis C. Hepatology1997 Aug;26(2):467-72.
5. Braden B, Helm B, Fabian T, Dietrich CF. [Bacillary angiomatosis of the liver, a
suspected ultrasound diagnosis?]. Z Gastroenterol2000 Sep;38(9):785-9.
6. Keane MA, Finlayson C, Joseph AE. A histological basis for the 'sonographic
snowstorm' in opportunistic infection of the liver and spleen. Clin Radiol1995 Apr;50(4):220-
2.
7. Braden B, Faust D, Ignee A, Schreiber D, Hirche T, Dietrich CF. Clinical relevance of
perihepatic lymphadenopathy in acute and chronic liver disease. J Clin Gastroenterol2008
Sep;42(8):931-6.
8. von Herbay A, Barreiros AP, Ignee A, Westendorff J, Gregor M, Galle PR, et al.
Contrast-enhanced ultrasonography with SonoVue: differentiation between benign and
malignant lesions of the spleen. J Ultrasound Med2009 Apr;28(4):421-34.
9. Brunetti E, Brigada R, Poletti F, Maiocchi L, Garlaschelli AL, Gulizia R, et al. The
current role of abdominal ultrasound in the clinical management of patients with AIDS.
Ultraschall Med2006 Feb;27(1):20-33.
10. Hirche TO, Ignee A, Barreiros AP, Schreiber-Dietrich D, Jungblut S, Ott M, et al.
Indications and limitations of endoscopic ultrasound elastography for evaluation of focal
pancreatic lesions. Endoscopy2008 Nov;40(11):910-7.
11. Ignee A, Straub B, Schuessler G, Dietrich CF. Contrast enhanced ultrasound of renal
masses. World J Radiol2010 Jan;2(1):15-31.
12. Dietrich CF, Brunner V, Lembcke B. [Intestinal ultrasound in rare small and large
intestinal diseases]. Z Gastroenterol1998 Nov;36(11):955-70.
13. CF D. Ultrasonography of the large and small intestine. BD R, editor. Wellesley,MA:
UpToDate; 2012.
14. Bhaduri S, Wiselka MJ, Rogers PM. A review of ultrasound-guided percutaneous
biopsy of the gastrointestinal tract in HIV-infected patients. HIV Med1999 Oct;1(1):43-6.
15. Mandel L. Ultrasound findings in HIV-positive patients with parotid gland swellings. J
Oral Maxillofac Surg2001 Mar;59(3):283-6.
16. Ntsekhe M, Hakim J. Impact of human immunodeficiency virus infection on
cardiovascular disease in Africa. Circulation2005 Dec;112(23):3602-7.
17. Barreiros AP, Braden B, Schieferstein-Knauer C, Ignee A, Dietrich CF. Characteristics
of intestinal tuberculosis in ultrasonographic techniques. Scand J
Gastroenterol2008;43(10):1224-31.
18. Heller T, Lessells RJ, Wallrauch C, Brunetti E. Tuberculosis pericarditis with cardiac
tamponade: management in the resource-limited setting. Am J Trop Med Hyg2010
Dec;83(6):1311-4.
19. Reuter H, Burgess LJ, Doubell AF. Epidemiology of pericardial effusions at a large
academic hospital in South Africa. Epidemiol Infect2005 Jun;133(3):393-9.

20. Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation2005
Dec;112(23):3608-16.
21. Hakim JG, Ternouth I, Mushangi E, Siziya S, Robertson V, Malin A. Double blind
randomised placebo controlled trial of adjunctive prednisolone in the treatment of effusive
tuberculous pericarditis in HIV seropositive patients. Heart2000 Aug;84(2):183-8.
22. Chen HJ, Hsu WH, Tu CY, Yu YH, Chiu KL, Hang LW, et al. Sonographic septation in
lymphocyte-rich exudative pleural effusions: a useful diagnostic predictor for tuberculosis. J
Ultrasound Med2006 Jul;25(7):857-63.
23. Pereira JM, Madureira AJ, Vieira A, Ramos I. Abdominal tuberculosis: imaging
features. Eur J Radiol2005 Aug;55(2):173-80.
24. Qibi NM. New technique of blind peritoneal biopsy. Br Med J (Clin Res Ed)1987
Sep;295(6599):638.
25. Heller T, Goblirsch S, Wallrauch C, Lessells R, Brunetti E. Abdominal tuberculosis:
sonographic diagnosis and treatment response in HIV-positive adults in rural South Africa. Int
J Infect Dis2010 Sep;14 Suppl 3:e108-12.
26. Hollerweger A, Dietrich CF. ["White bowel". A sonographic sign of intestinal lymph
edema?]. Ultraschall Med2005 Apr;26(2):127-33.
27. Vijayaraghavan SB, Kandasamy SV, Arul M, Prabhakar M, Dhinakaran CL,
Palanisamy R. Spectrum of high-resolution sonographic features of urinary tuberculosis. J
Ultrasound Med2004 May;23(5):585-94.
28. Matos MJ, Bacelar MT, Pinto P, Ramos I. Genitourinary tuberculosis. Eur J Radiol2005
Aug;55(2):181-7.
Related Documents











