HRET HIIN GET UP Virtual Event 1 November 16, 2017 Early Mobility Matters: In & Out of the ICU

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

HRET HIIN GET UP Virtual Event
1
November 16, 2017
Early Mobility Matters: In & Out of the ICU

WELCOME AND INTRODUCTIONS
2
Nerissa Legge, Program Manager| HRET
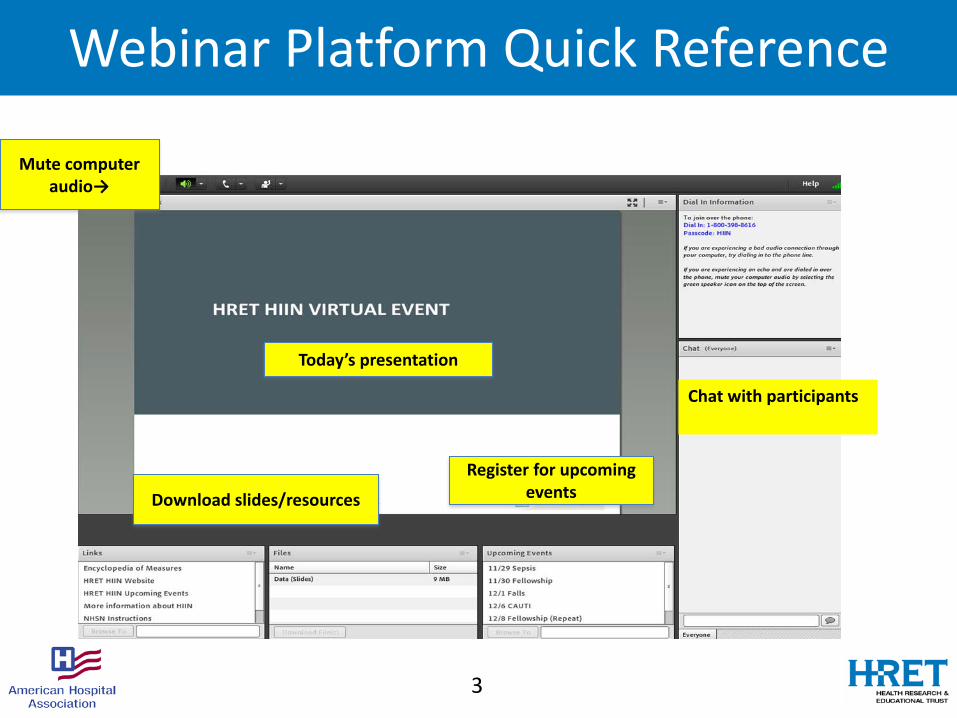
Webinar Platform Quick Reference
3
Mute computer audio→
Today’s presentation
Download slides/resources
Register for upcoming events
Chat with participants

Agenda for Today
4
5
Poll: How did you hear about this event?
How did you hear about today’s virtual event?a. HRET HIIN flyerb. HRET HIIN websitec. HRET LISTSERV d. State hospital associatione. QIN-QIO f. Your organization/colleagueg. Other, please specify

GET UP! A CROSS CUTTING APPROACH TO ACCELERATE HARM REDUCTION
Jackie Conrad, RN, MBA, RCCImprovement Advisor, Cynosure Health
6
Maryanne Whitney, RN, CNS, MSN Improvement Advisor, Cynosure Health
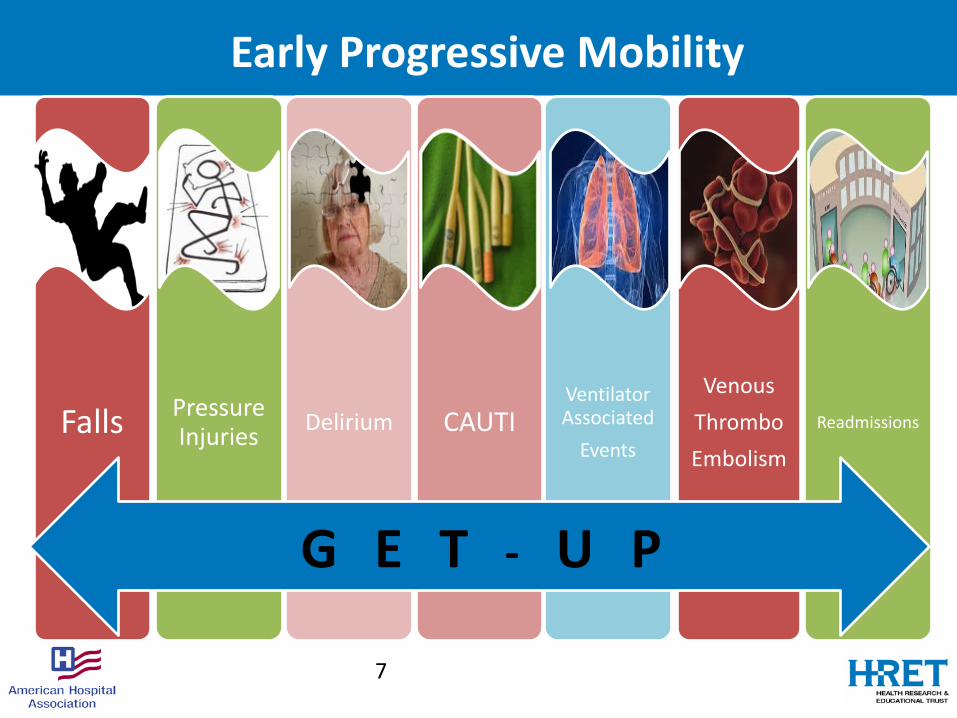
Early Progressive Mobility
Falls Pressure Injuries Delirium CAUTI
Ventilator Associated
Events
VenousThromboEmbolism
Readmissions
7
G E T - U P
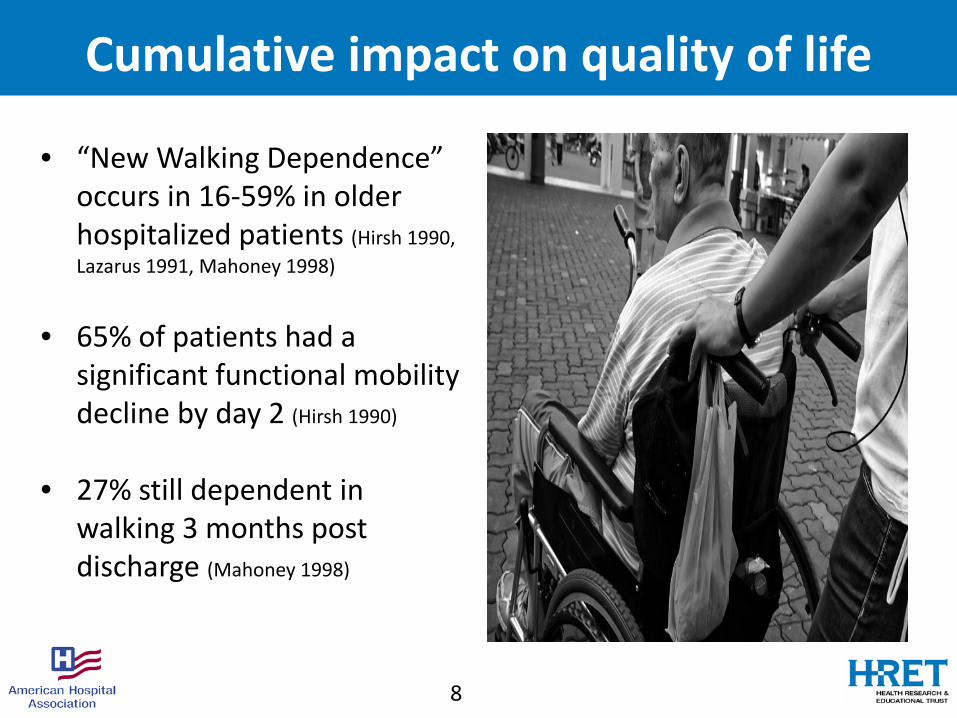
Cumulative impact on quality of life
• “New Walking Dependence” occurs in 16-59% in older hospitalized patients (Hirsh 1990, Lazarus 1991, Mahoney 1998)
• 65% of patients had a significant functional mobility decline by day 2 (Hirsh 1990)
• 27% still dependent in walking 3 months post discharge (Mahoney 1998)
8

• Progressive mobility is defined as a series of planned movements in a sequential matter beginning at a patient's current mobility status with goal of returning to his/her baseline
(Vollman 2010)
9
What is progressive mobility?
Elevate HOB
Manual turning
PROM AROM
CLRT and Prone positioning
Upright / leg down position
Chair position
Dangling
Ambulation
MUST DO #1Walk In, Walk During, Walk Out!
10
• Determine pre admission ambulation status• Don’t assume a frail appearance means weakness• Use Get Up and Go or Timed Get Up and Go test to
assess ambulation skills

MUST DO #2Grab and Go Mobility Devices!
• Gait Belts in every room• Patients and staff have access to mobility devices• Safe mobilization and patient handling training for staff
11Gait belts are used to help control the patient’s center of balance.
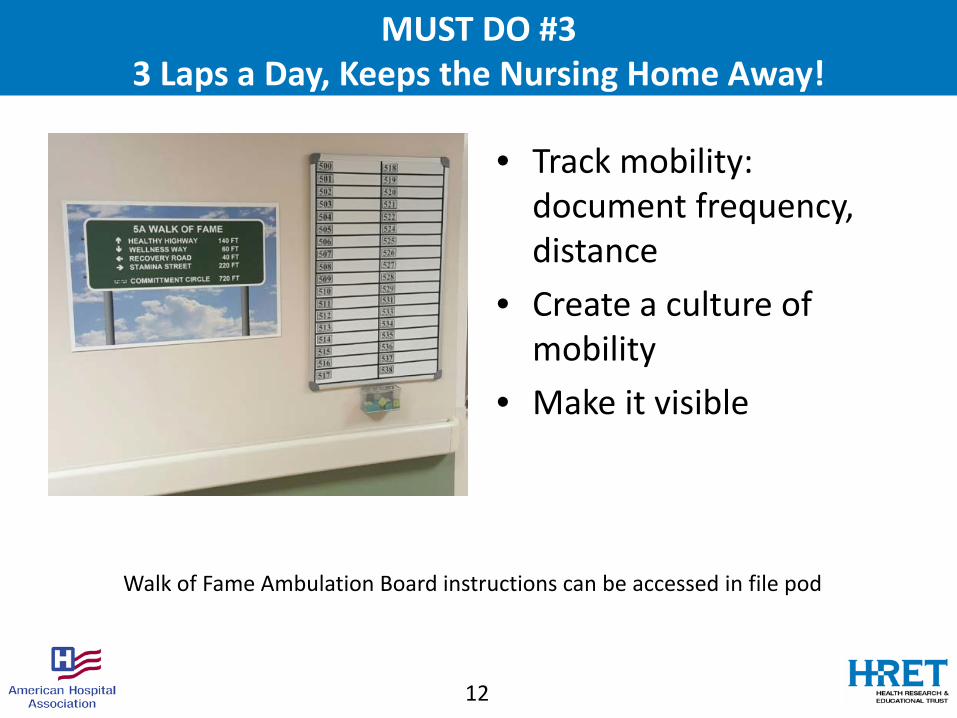
MUST DO #33 Laps a Day, Keeps the Nursing Home Away!
• Track mobility: document frequency, distance
• Create a culture of mobility
• Make it visible
12
Walk of Fame Ambulation Board instructions can be accessed in file pod

Evidence to support mobility
in ICU patients?
Dale M Needham FCPA. MD, PhDProfessor, Medical Director, Critical Care Physical Medicine &Rehabilitation ProgramJohn Hopkins University
Is EARLY activity in the ICU
SAFE?

• Adult studies of ICU mobility with safety data
• Exclusion: in-bed intervention (cycle, NMES); no report of # of sessions
• 48 publications (n=7,546 pts; 22,351 sessions) – 6 RCT, 2 non-rdm trial, 5 before-after, 22 prosp. cohort, 11 retro cohort, 2 pt prev
• 583 (2.6%) potential safety events – Most common: De-sat, hemodynamic changes, catheter removal
• Only 2 ETT removals (1 without replacement; 1 with in-bed mobility)
– Events w/ consequence, incl. stop rehab (subset of studies): 78 (0.6%) • 1 fall, 11 tube removal, 34 hemodynamic change, 18 desaturation, 14 other
Safety of Patient Mobilization and Rehabilitation in the ICU:Systematic Review with Meta-Analysis
Nydahl, P.; Sricharoenchai, T.; Chandra, S; Kundt, F.; Huang, M.; Fischill, M.; Needham, DM.Annals of the American Thoracic Society; 2017
Is early activity in the ICUBENEFICIAL?
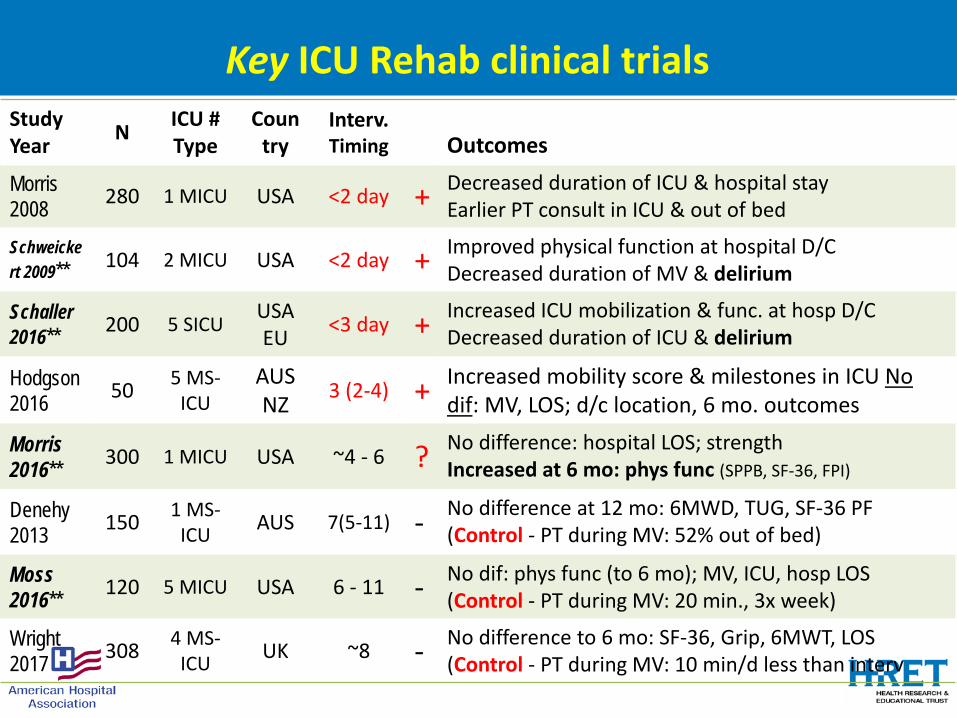
Key ICU Rehab clinical trialsStudyYear N ICU #
TypeCoun
tryInterv. Timing Outcomes
Morris2008 280 1 MICU USA <2 day + Decreased duration of ICU & hospital stay
Earlier PT consult in ICU & out of bed
Schweickert 2009** 104 2 MICU USA <2 day + Improved physical function at hospital D/C
Decreased duration of MV & delirium
Schaller 2016** 200 5 SICU USA
EU <3 day + Increased ICU mobilization & func. at hosp D/CDecreased duration of ICU & delirium
Hodgson2016 50 5 MS-
ICUAUS NZ 3 (2-4) + Increased mobility score & milestones in ICU No
dif: MV, LOS; d/c location, 6 mo. outcomes
Morris 2016** 300 1 MICU USA ~4 - 6 ? No difference: hospital LOS; strength
Increased at 6 mo: phys func (SPPB, SF-36, FPI)
Denehy2013 150 1 MS-
ICU AUS 7(5-11) - No difference at 12 mo: 6MWD, TUG, SF-36 PF (Control - PT during MV: 52% out of bed)
Moss 2016** 120 5 MICU USA 6 - 11 - No dif: phys func (to 6 mo); MV, ICU, hosp LOS
(Control - PT during MV: 20 min., 3x week)
Wright2017 308 4 MS-
ICU UK ~8 - No difference to 6 mo: SF-36, Grip, 6MWT, LOS (Control - PT during MV: 10 min/d less than interv
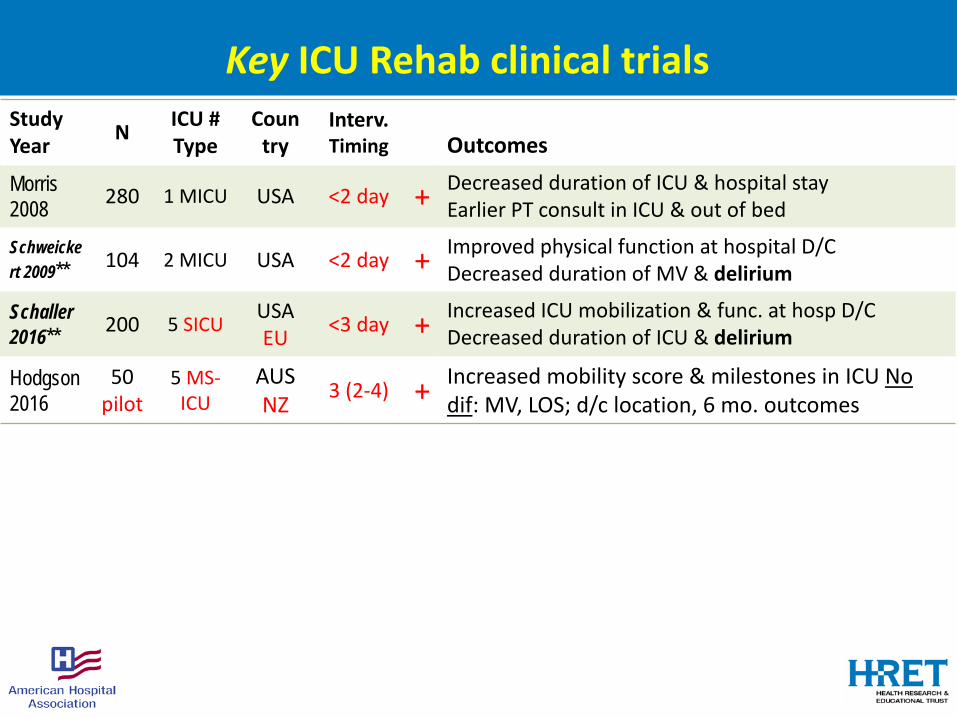
Key ICU Rehab clinical trialsStudyYear N ICU #
TypeCoun
tryInterv. Timing Outcomes
Morris2008 280 1 MICU USA <2 day + Decreased duration of ICU & hospital stay
Earlier PT consult in ICU & out of bed
Schweickert 2009** 104 2 MICU USA <2 day + Improved physical function at hospital D/C
Decreased duration of MV & delirium
Schaller 2016** 200 5 SICU USA
EU <3 day + Increased ICU mobilization & func. at hosp D/CDecreased duration of ICU & delirium
Hodgson2016
50pilot
5 MS-ICU
AUS NZ 3 (2-4) + Increased mobility score & milestones in ICU No
dif: MV, LOS; d/c location, 6 mo. outcomes
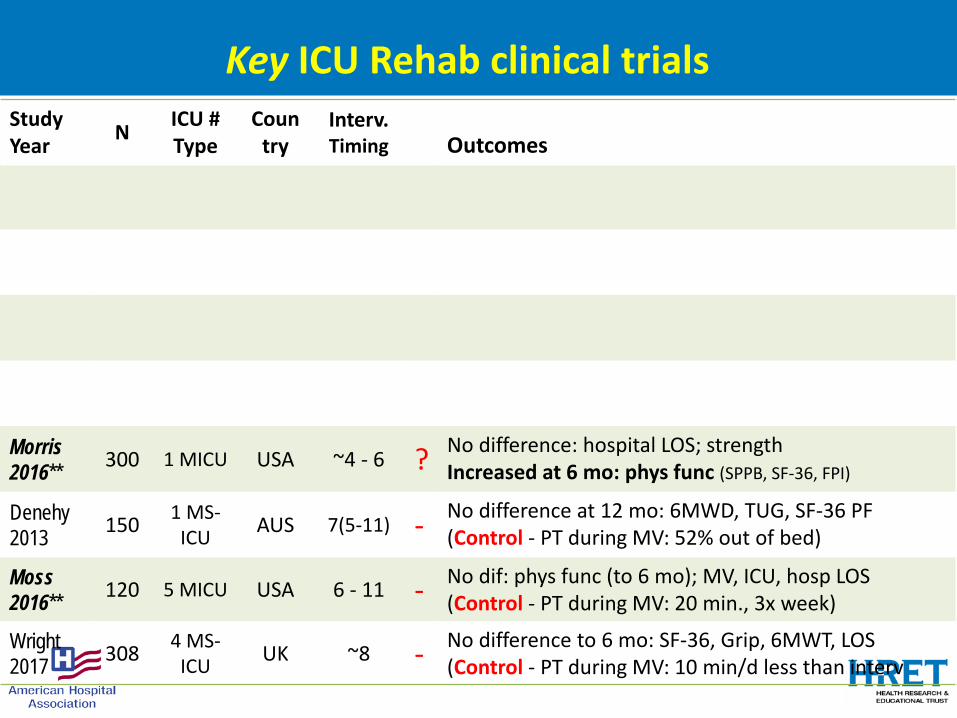
Key ICU Rehab clinical trialsStudyYear N ICU #
TypeCoun
tryInterv. Timing Outcomes
Morris 2016** 300 1 MICU USA ~4 - 6 ? No difference: hospital LOS; strength
Increased at 6 mo: phys func (SPPB, SF-36, FPI)
Denehy2013 150 1 MS-
ICU AUS 7(5-11) - No difference at 12 mo: 6MWD, TUG, SF-36 PF (Control - PT during MV: 52% out of bed)
Moss 2016** 120 5 MICU USA 6 - 11 - No dif: phys func (to 6 mo); MV, ICU, hosp LOS
(Control - PT during MV: 20 min., 3x week)
Wright2017 308 4 MS-
ICU UK ~8 - No difference to 6 mo: SF-36, Grip, 6MWT, LOS (Control - PT during MV: 10 min/d less than interv

Key ICU Rehab clinical trialsStudyYear N ICU #
TypeCoun
tryInterv. Timing Outcomes
Morris2008 280 1 MICU USA <2 day + Decreased duration of ICU & hospital stay
Earlier PT consult in ICU & out of bed
Schweickert 2009** 104 2 MICU USA <2 day + Improved physical function at hospital D/C
Decreased duration of MV & delirium
Schaller 2016** 200 5 SICU USA
EU <3 day + Increased ICU mobilization & func. at hosp D/CDecreased duration of ICU & delirium
Hodgson2016 50 5 MS-
ICUAUS NZ 3 (2-4) + Increased mobility score & milestones in ICU No
dif: MV, LOS; d/c location, 6 mo. outcomes
Morris 2016** 300 1 MICU USA ~4 - 6 ? No difference: hospital LOS; strength
Increased at 6 mo: phys func (SPPB, SF-36, FPI)
Denehy2013 150 1 MS-
ICU AUS 7(5-11) - No difference at 12 mo: 6MWD, TUG, SF-36 PF (Control - PT during MV: 52% out of bed)
Moss 2016** 120 5 MICU USA 6 - 11 - No dif: phys func (to 6 mo); MV, ICU, hosp LOS
(Control - PT during MV: 20 min., 3x week)
Wright2017 308 4 MS-
ICU UK ~8 - No difference to 6 mo: SF-36, Grip, 6MWT, LOS (Control - PT during MV: 10 min/d less than interv
Full text: https://iii.hm/ddw

Design: RCT at U of Chicago & U of Iowa
Subjects: 104 MICU patients require MV
Intervention vs. Control: daily sedation interruption, plus:
• PT & OT (7d/wk –ICU & ward) starting at Day 1-2 vs.
• “Usual care” PT & OT starting at Day 6 -10
Lancet May 2009

Benefit is from receiving PT/OTEARLY while on mech. ventilation
Intervention• PROM• AAROM• AROM• Bed
Mobility• Transfers
(sitting)• Sitting
balance• ADLs• Transfers
(standing)• Ambulation
InterventionN=49
ControlN=55
Median duration of therapy:
After MV (minutes/day) 13 [5 to 20] 11 [0 to 23]
During MV (minutes/day)* 19 [10 to 29] 0 [0 to 0]
* p<0.0001
How was PT/OT provided to get benefits?
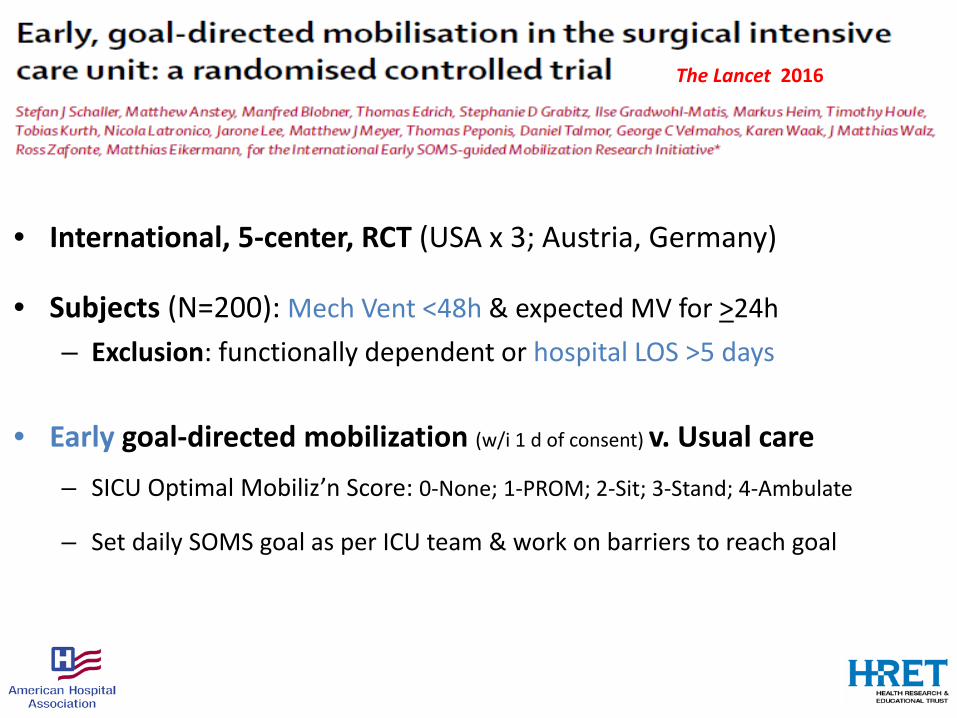
• International, 5-center, RCT (USA x 3; Austria, Germany)
• Subjects (N=200): Mech Vent <48h & expected MV for >24h – Exclusion: functionally dependent or hospital LOS >5 days
• Early goal-directed mobilization (w/i 1 d of consent) v. Usual care– SICU Optimal Mobiliz’n Score: 0-None; 1-PROM; 2-Sit; 3-Stand; 4-Ambulate
– Set daily SOMS goal as per ICU team & work on barriers to reach goal
The Lancet 2016
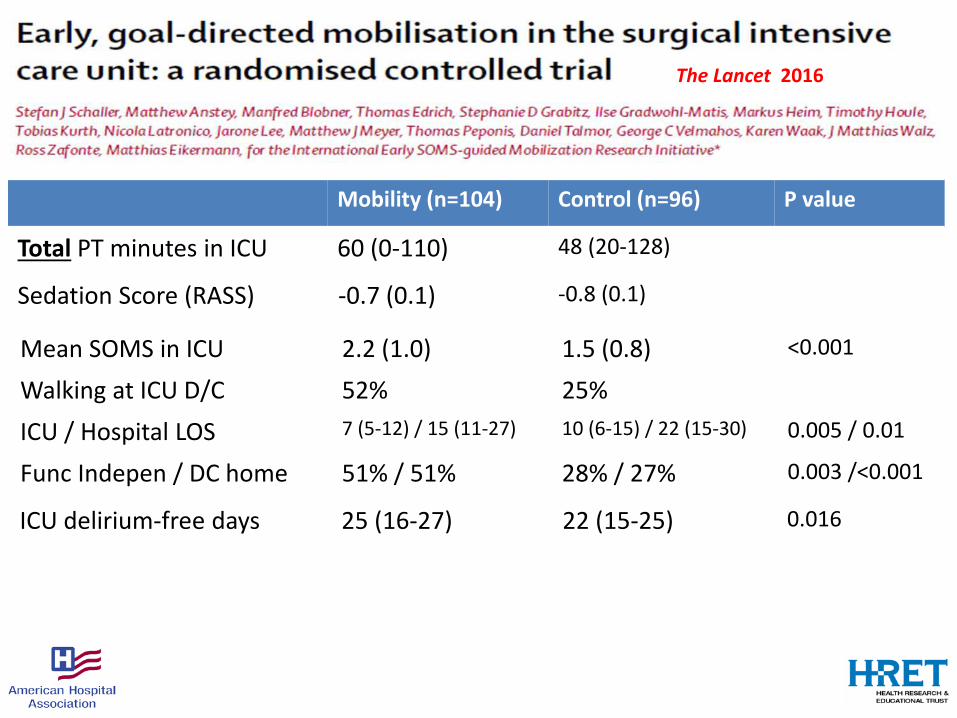
ICU delirium-free days 25 (16-27) 22 (15-25) 0.016
The Lancet 2016
Mobility (n=104) Control (n=96) P value
Total PT minutes in ICU 60 (0-110) 48 (20-128)
Sedation Score (RASS) -0.7 (0.1) -0.8 (0.1)
Mean SOMS in ICU 2.2 (1.0) 1.5 (0.8) <0.001
Walking at ICU D/C 52% 25%ICU / Hospital LOS 7 (5-12) / 15 (11-27) 10 (6-15) / 22 (15-30) 0.005 / 0.01
Func Indepen / DC home 51% / 51% 28% / 27% 0.003 /<0.001
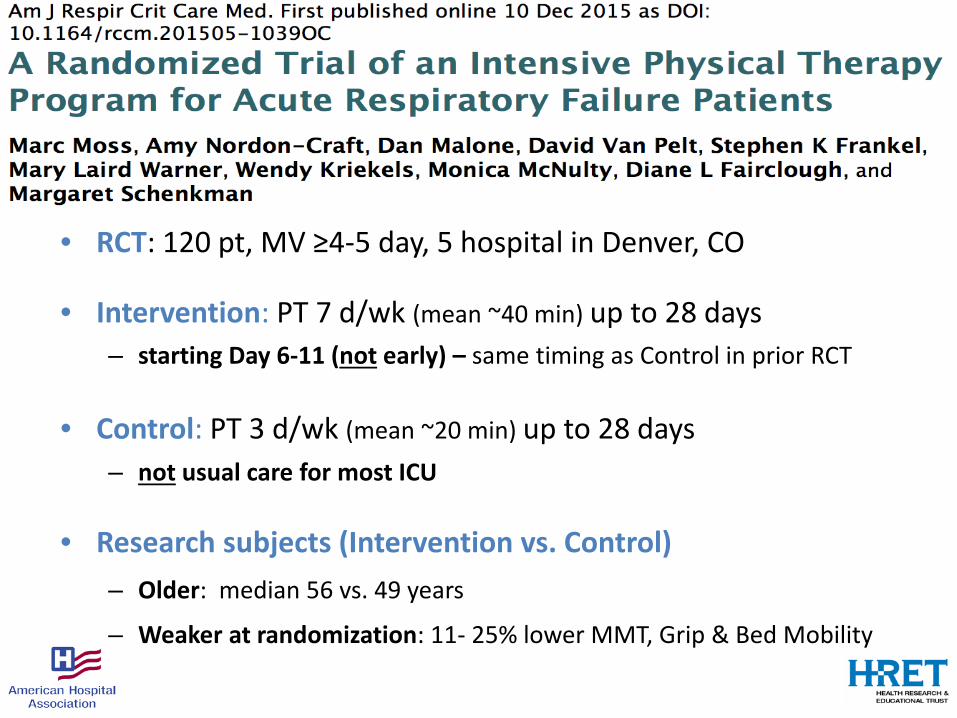
• RCT: 120 pt, MV ≥4-5 day, 5 hospital in Denver, CO
• Intervention: PT 7 d/wk (mean ~40 min) up to 28 days – starting Day 6-11 (not early) – same timing as Control in prior RCT
• Control: PT 3 d/wk (mean ~20 min) up to 28 days – not usual care for most ICU
• Research subjects (Intervention vs. Control) – Older: median 56 vs. 49 years
– Weaker at randomization: 11- 25% lower MMT, Grip & Bed Mobility

• Result: no effect on PFP-10 phys func scale at 1 month– Only 33% with assessment (N = 20 & 19 in each group)
• 45% LTACH/facility (25% at 3 mo.)
• Concl: ?Higher intensity, late-onset PT may not have benefit– Older/weaker patients in intervention group – Control more rehab than most centers – decreasing treatment effect– Did not measure outcomes in 50% of patients d/c to facility
– Focus on early start to PT (i.e., replicate Schweickert Lancet RCT)
– Focus on getting ICU patients to PT at least 3x/week

• Single-center, assessor-blinded RCT• 300 MICU MV patients• Standardized Rehab Therapy (SRT) vs Usual Care
• Outcomes: ICU & hospital d/c + 2, 4 & 6 month
• SRT: 3 session/day, 7 d/week, during entire hospital stay:• Passive range of motion• PT: bed mobility, transfer and balance training• Progressive resistance exercises
• Usual Care: PT on week days, if ordered

Days to first therapy, median (IQR)
SRTPROM PT Strength
1 (0-2) 3 (1-6) 4 (2-7)
Usual Care 7 (4-10)

Days to first therapy, median (IQR)
Days of therapy per patient,median (IQR)
SRTPROM PT Strength PROM PT Strength
1 (0-2) 3 (1-6) 4 (2-7) 8 (5-14) 5 (3-8) 3 (1-5)
Usual Care 7 (4-10) 1 (0-8)
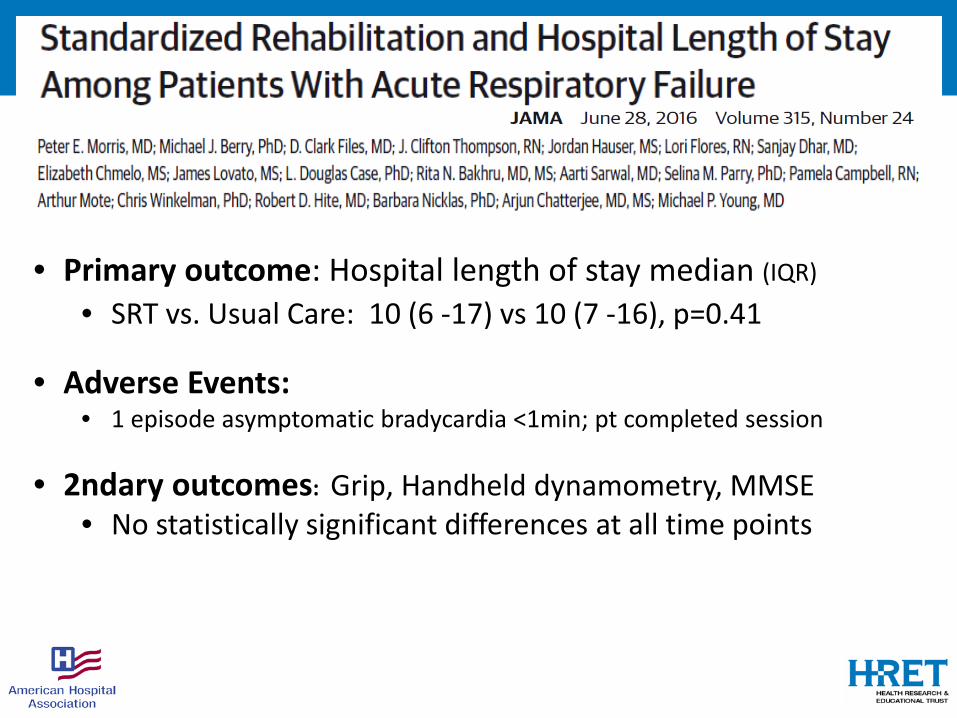
• Primary outcome: Hospital length of stay median (IQR)
• SRT vs. Usual Care: 10 (6 -17) vs 10 (7 -16), p=0.41
• Adverse Events:• 1 episode asymptomatic bradycardia <1min; pt completed session
• 2ndary outcomes: Grip, Handheld dynamometry, MMSE• No statistically significant differences at all time points
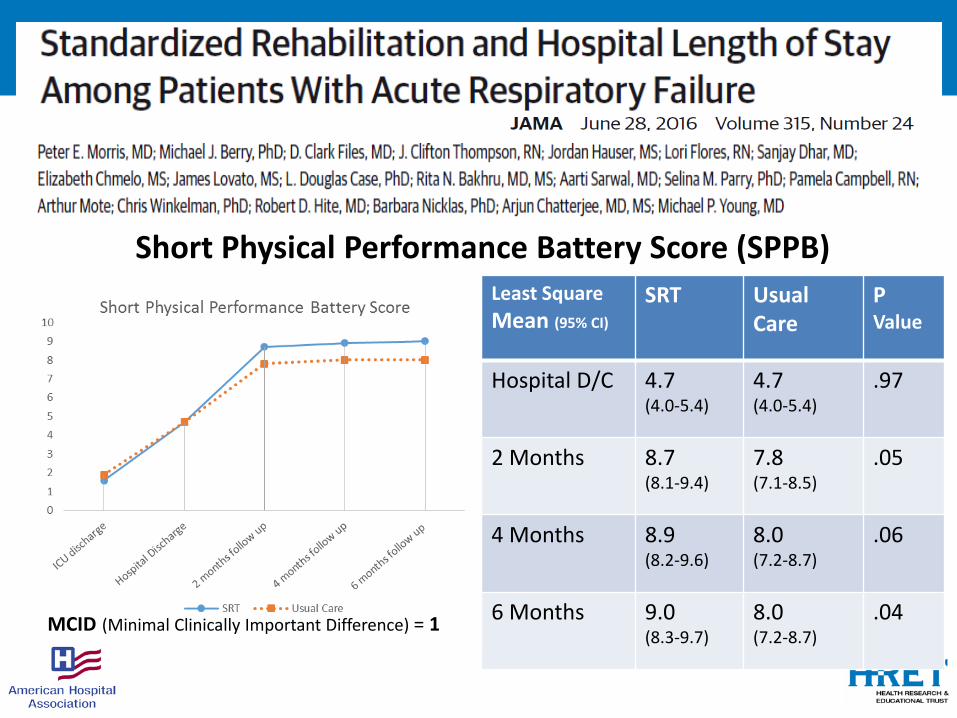
Short Physical Performance Battery Score (SPPB)Least Square Mean (95% CI)
SRT Usual Care
PValue
Hospital D/C 4.7(4.0-5.4)
4.7 (4.0-5.4)
.97
2 Months 8.7 (8.1-9.4)
7.8 (7.1-8.5)
.05
4 Months 8.9 (8.2-9.6)
8.0 (7.2-8.7)
.06
6 Months 9.0 (8.3-9.7)
8.0 (7.2-8.7)
.04MCID (Minimal Clinically Important Difference) = 1
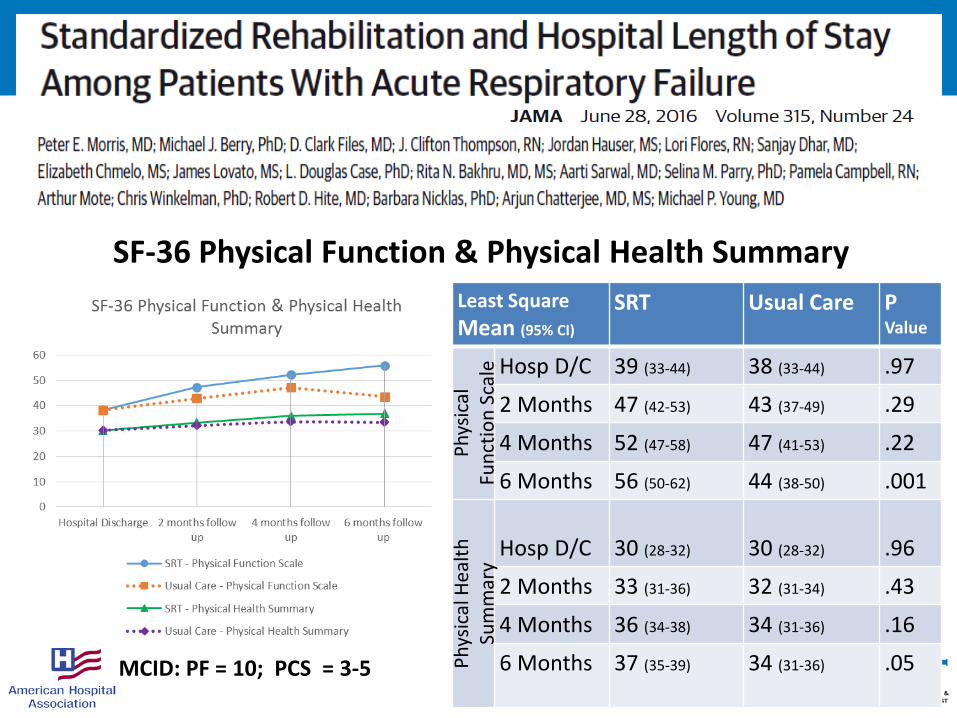
SF-36 Physical Function & Physical Health SummaryLeast Square Mean (95% CI)
SRT Usual Care PValue
Phys
ical
Fu
nctio
nSc
ale Hosp D/C 39 (33-44) 38 (33-44) .97
2 Months 47 (42-53) 43 (37-49) .29
4 Months 52 (47-58) 47 (41-53) .22
6 Months 56 (50-62) 44 (38-50) .001Ph
ysic
al H
ealth
Su
mm
ary
Hosp D/C 30 (28-32) 30 (28-32) .96
2 Months 33 (31-36) 32 (31-34) .43
4 Months 36 (34-38) 34 (31-36) .16
6 Months 37 (35-39) 34 (31-36) .05MCID: PF = 10; PCS = 3-5
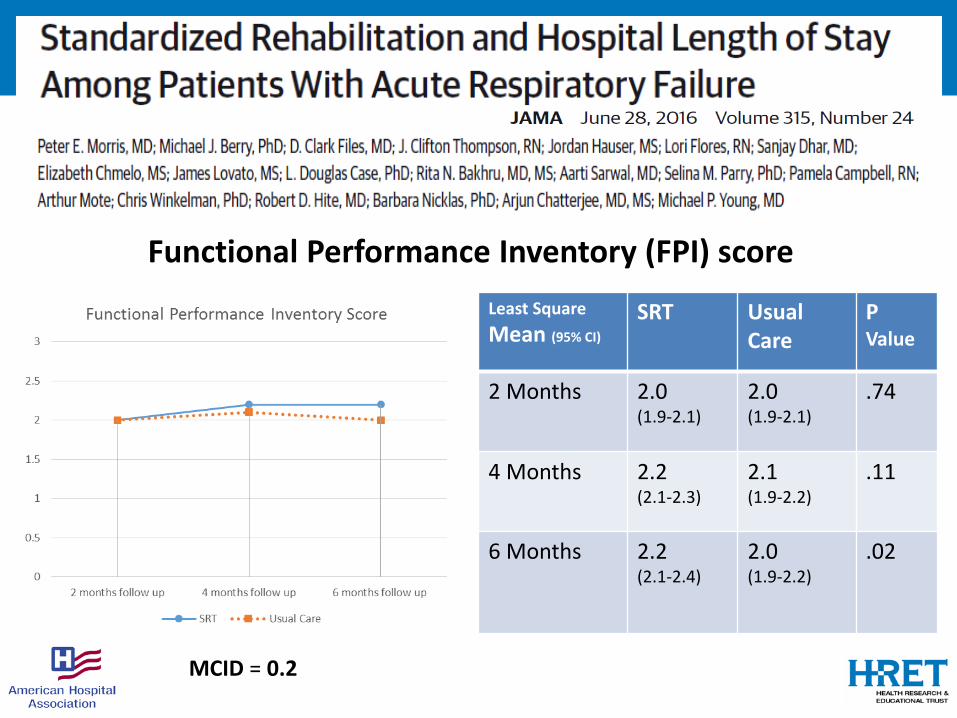
Functional Performance Inventory (FPI) scoreLeast Square Mean (95% CI)
SRT Usual Care
PValue
2 Months 2.0 (1.9-2.1)
2.0 (1.9-2.1)
.74
4 Months 2.2 (2.1-2.3)
2.1 (1.9-2.2)
.11
6 Months 2.2 (2.1-2.4)
2.0 (1.9-2.2)
.02
MCID = 0.2
• Study Limitations:• No sedation protocol: delayed start & # of session (esp strengthening)
• Up to 3.3 d for consent + 3 d for PT to start (?early enough)
• Loss to f/u ~30% of survivor: under-powered for post-d/c outcomes
• Conclusions:• SRT vs. usual care did not decrease hospital LOS• All physical function measures higher, increasing over 2- 6 mo.
• Future: • Pair rehab + sedation (?use cycling or NMES for early ICU)

• Over-sedation compromises the ability to participate in rehabilitation• Review of sedation practice is key to improving mobility• Target RASS -1 to +1 rather than Daily Interruption of sedation infusion
- Green J Multi-D Healthcare 2016
• Mobility, sedation, delirium, and sleep are inseparably linked• To successfully mobilize patients, sedation, sleep & delirium monitoring
must be routine and vigorously addressed- Clemmer CCM 2014
• ICUs that implemented exercise with both sedation interruption &delirium screening were 3.5 (CI 1.4-8.6) times more likely to achievehigher exercise levels in ventilated patients
- Miller Annals ATS 2015
The Importance of Sedation to Early Mobility
How to Start Early PM&R?The JHH MICU Experience
Exposure to rehab in JHH MICU is low:
- PT & OT in only 17% & 20% of ARDS pts
opportunity for Quality Improvement
Barriers to Activity in ICU• Time requirements and adequate staffing• Need for staff training• Need for team work and coordination• Over-sedation of ICU patients• Dislodgement of devices (CVC, ETT, feeding tubes)
• Worsening gas exchange• Unstable hemodynamics• Inadequate patient comfort, pain control
40
Review of 40 studies • 28 unique barriers
– Severity of illness, pain, mental status, devices/equipment– Staffing, lack of guidelines and equipment– Culture, lack of knowledge
• 70 strategies– Inter-professional team/champions with training & rounding– Safety guidelines and screening– Mobility protocols & daily goals sheets– Creating business case, dedicated staffing

QI Project DescriptionMulti-faceted QI focused on ventilated pts in MICU:
- dedicated OT & PT in MICU (pilot test)
- OT, PT, RN & MD training & education
- guidelines for consultation of OT and PT in ICU
- decrease over-sedation via prn vs. infusions
Topics in Stroke Rehab 2010;17:271-281
JHH Experience: FeasibilityDuring 4 month period (May – Aug 2007)
• 2 - 4x incr in PT & OT consult & Tx (vs prior yr)
• Of all PT and OT treatments– 68% while ventilated– 24% with ETT – 13% with femoral line
• New PM&R consults on weak patients
Archives of Physical Med & Rehab, 2010
MICU QI project D15
Walked 4 times:• Max dur’n 10 min• Max dist. 240 feet
(vs. 3 feet on QI day 1)
Our Experience with Feasibility
Removed for privacy purposes
Patient interviews & Video of ambulation process at:
www.hopkinsmedicine.org/OACIS
(OACIS = Outcomes After Critical Illness & Surgery)

JHH Experience: Safety
• 4 events (~1% of treatments)– feeding/rectal tubes dislodged
• also occurred with routine RN care
• Update from after the QI project….

46
• JHH MICU over 2.5 years (June 2009 – Dec 2011)
• 1,110 admissions with >= 1 PT session
• 5,267 total PT tx (not individual activities)
– 66% of PT days: sitting at edge of bed or higher

47
• JHH MICU over 2.5 years (June 2009 – Dec 2011)
• 34 potential safety events in 25 admissions
– 0.6% of PT sessions (i.e., 6 per 1,000 PT tx)• 80% of events = transient physiological (HR, BP, Sp02)
– 4 events required any Tx (8 per 10,000 PT tx)• 2 NG tube, 1 A-line, 1 fall with laceration & suture
Annals of ATS (2016)
Physical Therapy J (2013)
Cardiopulm PT (2015)
Journal of Critical Care (2013)
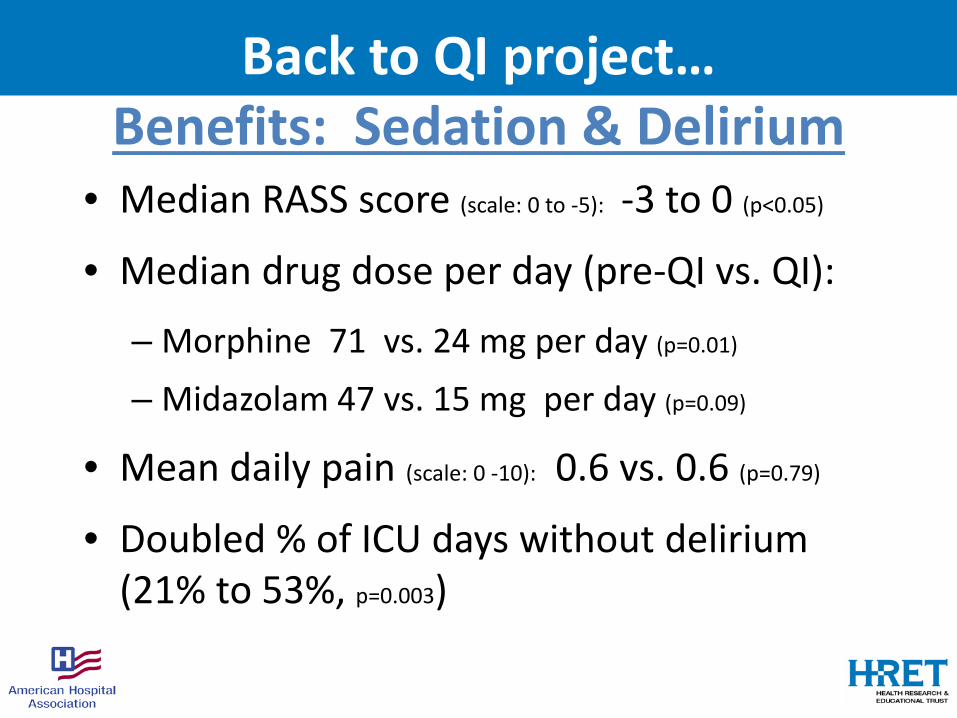
Back to QI project…Benefits: Sedation & Delirium
• Median RASS score (scale: 0 to -5): -3 to 0 (p<0.05)
• Median drug dose per day (pre-QI vs. QI):
– Morphine 71 vs. 24 mg per day (p=0.01)
– Midazolam 47 vs. 15 mg per day (p=0.09)
• Mean daily pain (scale: 0 -10): 0.6 vs. 0.6 (p=0.79)
• Doubled % of ICU days without delirium (21% to 53%, p=0.003)

Potential Benefits to HospitalWhy so many empty MICU beds?
Versus same 4-month period in 2006:
• 20% increase in MICU admissions• 10% reduction in hospital mortality• 30% (2.1 day) reduction in MICU LOS• 18% (3.1 day) reduction in hosp LOS

Acknowledgements• Dr. Landon King, Director PCCM for financial support• Dr. Jeff Palmer, Director PM&R for PT & OT support• Dr. Eddy Fan, MICU physician • Dr. Roy Brower, MICU Director • Drs. Radha Korupolu & Pranoti Pradhan, project coordinators
• Dr. Kashif Janjua & Mr. Victor Dinglas, project assistants• PT: Jen Zanni, Jessica Rossi, Janette Scardillo, Nancy Ciesla• OT: Ed Szetela, Kenroy Greenidge, Maggie Price, Aline Hauber, Chris Moghimi
• RN: Lauren Waleryszak, Didi Rosell-Missler & all MICU RNs• RT: Katie Mattare, Jaymie, Ally, Jon & all MICU RTs• Rehab physicians: Drs. David Pitts & Mohammad Yavari-Rad• Neurology physicians: Drs. Argye Hillis, David Cornblath
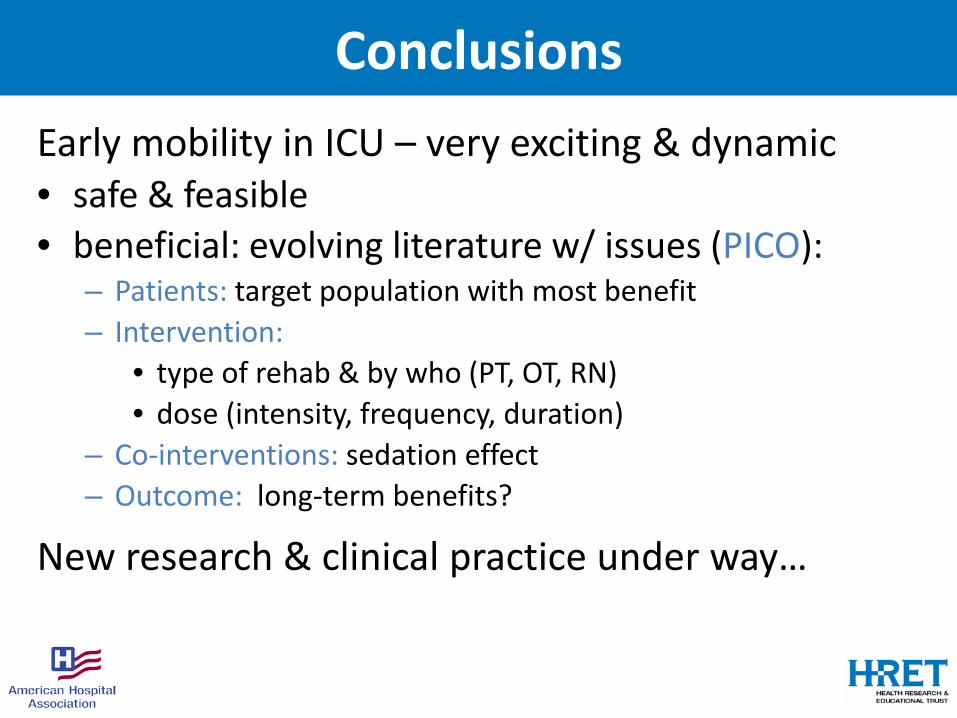
ConclusionsEarly mobility in ICU – very exciting & dynamic• safe & feasible• beneficial: evolving literature w/ issues (PICO):
– Patients: target population with most benefit– Intervention:
• type of rehab & by who (PT, OT, RN) • dose (intensity, frequency, duration)
– Co-interventions: sedation effect – Outcome: long-term benefits?
New research & clinical practice under way…

For more info…
www.hopkinsmedicine.org/OACIS
Removed for privacy purposes

Monthly ICU Rehab Email
• Update on latest research, videos, conferences & announcements
• Join via email request to:[email protected]
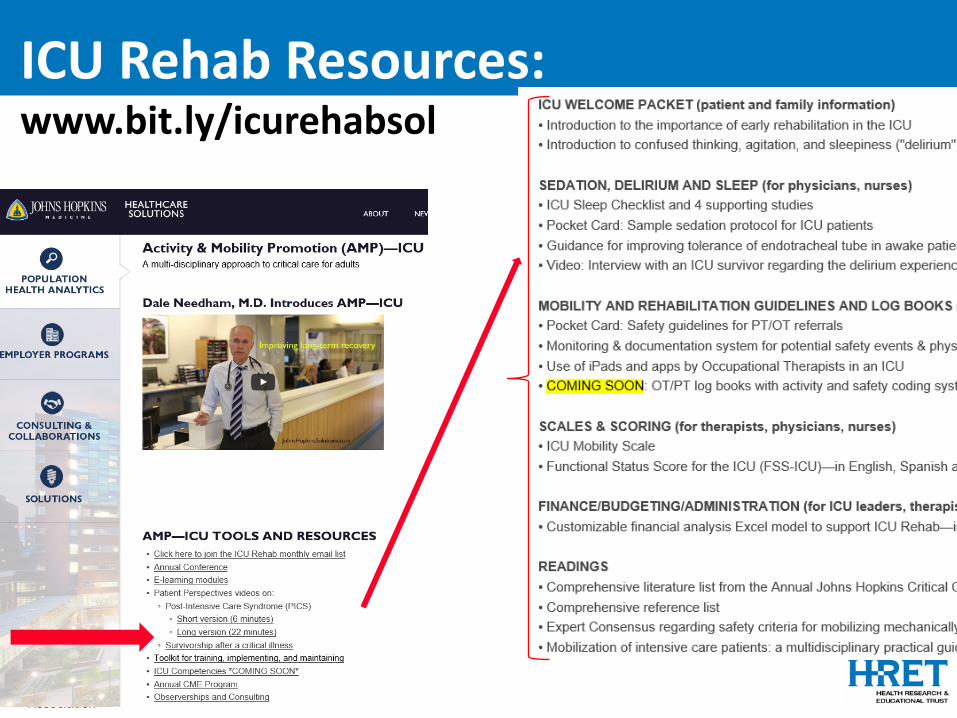
ICU Rehab Resources: www.bit.ly/icurehabsol
•
The Future is Large-Scale Learning Networks & Collaborations
www.mobilization-network.org
Follow on Twitter: @icurehab
@DrDaleNeedham
Contribute to Twitter at: #icurehab

The ICU Recovery Network (IRN) (like a simple version of Facebook)
• To access & contribute to ICU Rehab content: – videos, documents, website links, and event information
• To interact w/ other ICU Rehab clinicians from world• Joining is simple (< 5 min.)
You receive invitation email with link to set up account
The web-based platform is provided, free-of-charge, by MedConcert.
Enter basic info into web form
To Join (only clinicians/researchers):

11th Int’l Mtg of PM&R in ICUTime: Sat. May 19, 2018 (~1.30 - 6.30pm)
Location: Univ California San Diego
Cost: Free
By Invitation Only [email protected]
Follow on Twitter: @icurehab @DrDaleNeedhamContribute to Twitter at: #icurehab
Pre-ATS Meeting
7th Annual Johns Hopkins Critical Care Rehabilitation Conference
Including a NEW one-day pre-conference:International ICU Diary Conference
November 1 - 3, 2018Johns Hopkins Hospital, Baltimore, MD
For more Conference info: [email protected] and bit.ly/icurehab
For ICU Rehab Solutions/Resources: bit.ly/icurehabsol
Follow Us on Twitter: @icurehab @DrDaleNeedham
Questions?
Developing our Culture of Mobility
A Journey by Franciscan Health Michigan City, Indiana
Presented by Brooke Nack, PTInpatient Therapy ManagerMobility Program Manager

Polling QuestionIn your hospital setting, who
“owns” mobility?For example: When your patient needs to do his or her
highest level of activity, Who do you call?
1. Nurses2. Nurses aides3. Therapists, physical or occupational4. Mobility Team/Lift Team5. Physicians6. Ghost Busters!
62
Our Mobility Committee: “We Have an idea…”
Property of Brooke Nack, Inpatient Therapy Manager Franciscan Health Michigan City Not to be copied or reproduced without permission

Motivation to Move…Our Lit Review
“A study of 45 elderly patients on a general medical unit , who had neither delirium or dementia and were able to walk prior to
admission, found that they spent 20 out of every 24 hours in bed over the mean 5.1 days
they were in the hospital.”
Wood et al. A mobility program for an inpatient acute care medical unit. AJN. 2014; 114(10)34-40.
Property of Brooke Nack, Inpatient Therapy /Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
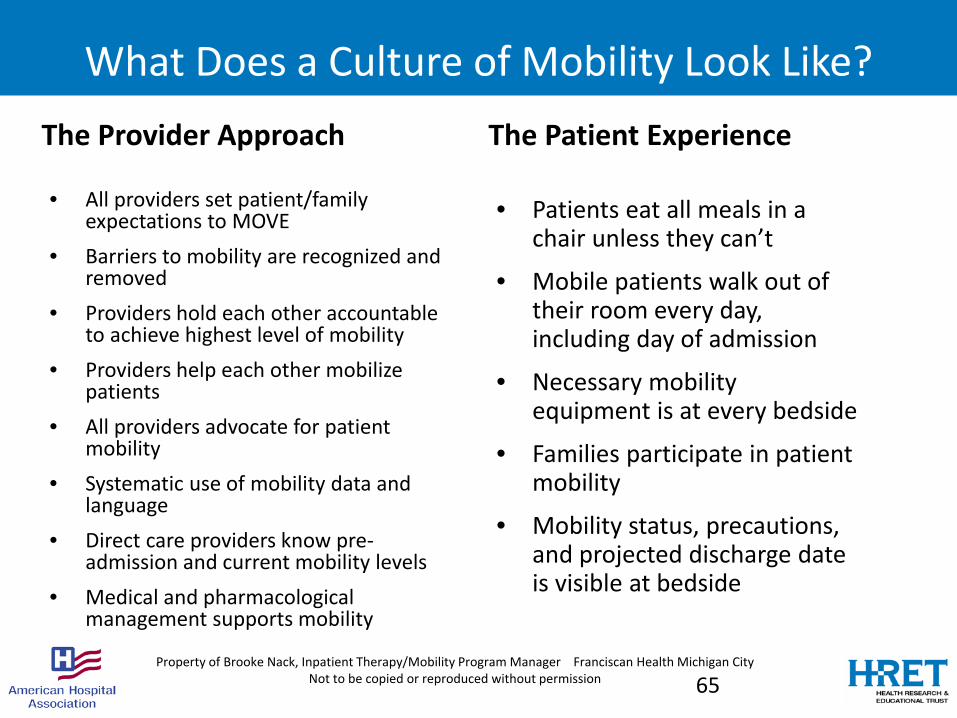
What Does a Culture of Mobility Look Like?The Provider Approach
• All providers set patient/family expectations to MOVE
• Barriers to mobility are recognized and removed
• Providers hold each other accountable to achieve highest level of mobility
• Providers help each other mobilize patients
• All providers advocate for patient mobility
• Systematic use of mobility data and language
• Direct care providers know pre-admission and current mobility levels
• Medical and pharmacological management supports mobility
The Patient Experience
• Patients eat all meals in a chair unless they can’t
• Mobile patients walk out of their room every day, including day of admission
• Necessary mobility equipment is at every bedside
• Families participate in patient mobility
• Mobility status, precautions, and projected discharge date is visible at bedside
65Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission

Who Owns Mobility?
Physicians?
Patients?
Families?
Administration?
Therapists?
Nurses?
66Property of Brooke Nack, Inpatient Therapy /Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
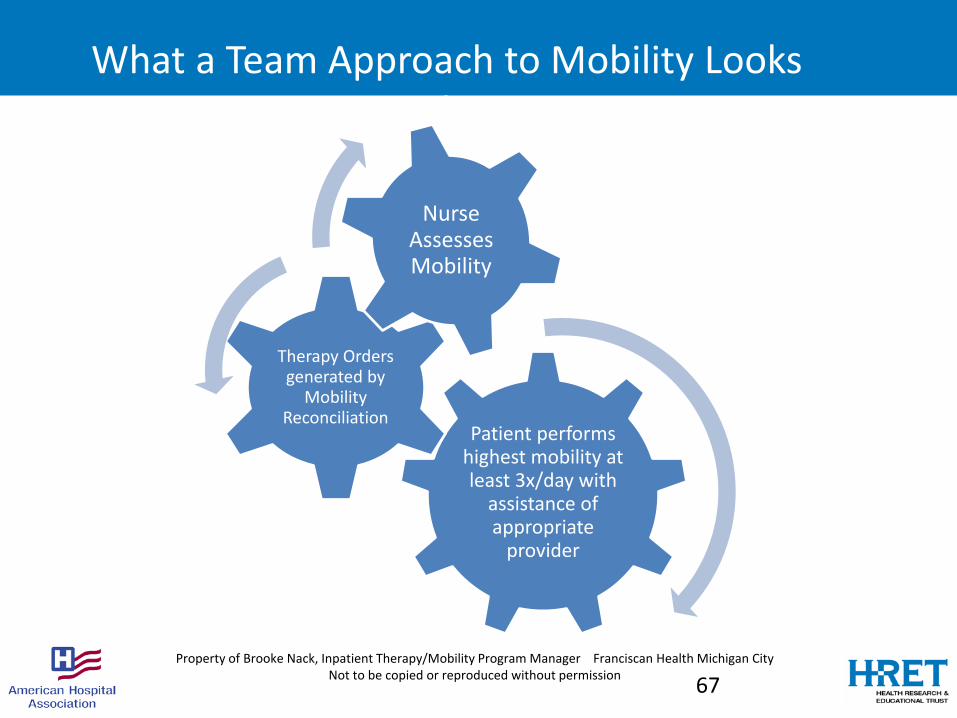
What a Team Approach to Mobility Looks Like
Patient performs highest mobility at least 3x/day with
assistance of appropriate
provider
Therapy Orders generated by
Mobility Reconciliation
Nurse Assesses Mobility
67Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
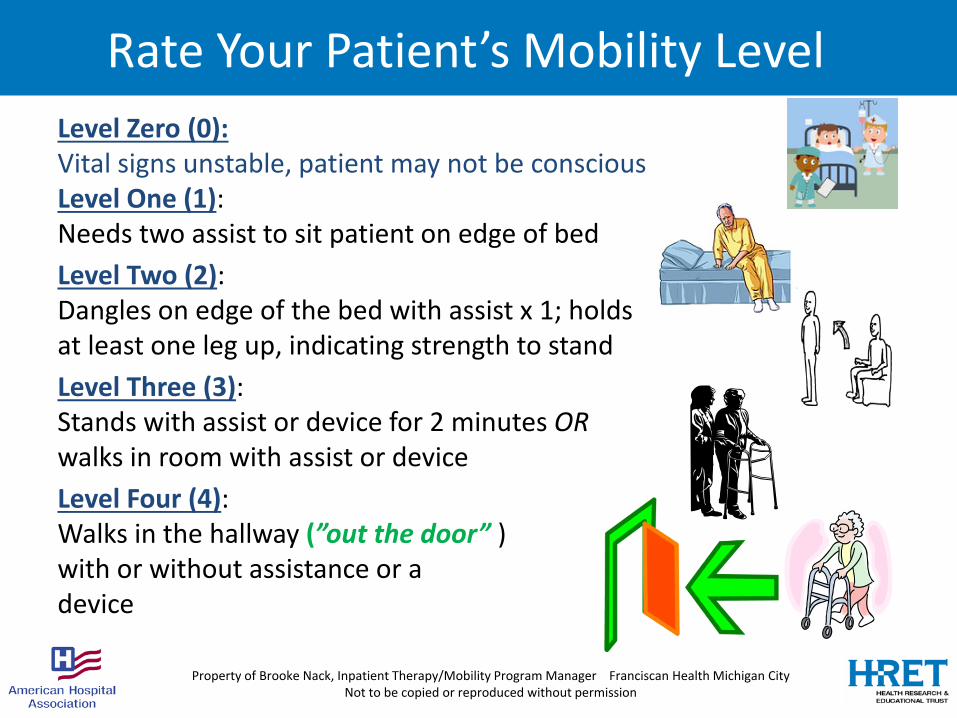
Rate Your Patient’s Mobility LevelLevel Zero (0):Vital signs unstable, patient may not be consciousLevel One (1): Needs two assist to sit patient on edge of bedLevel Two (2): Dangles on edge of the bed with assist x 1; holds at least one leg up, indicating strength to standLevel Three (3): Stands with assist or device for 2 minutes ORwalks in room with assist or deviceLevel Four (4): Walks in the hallway (”out the door” )with or without assistance or a device
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
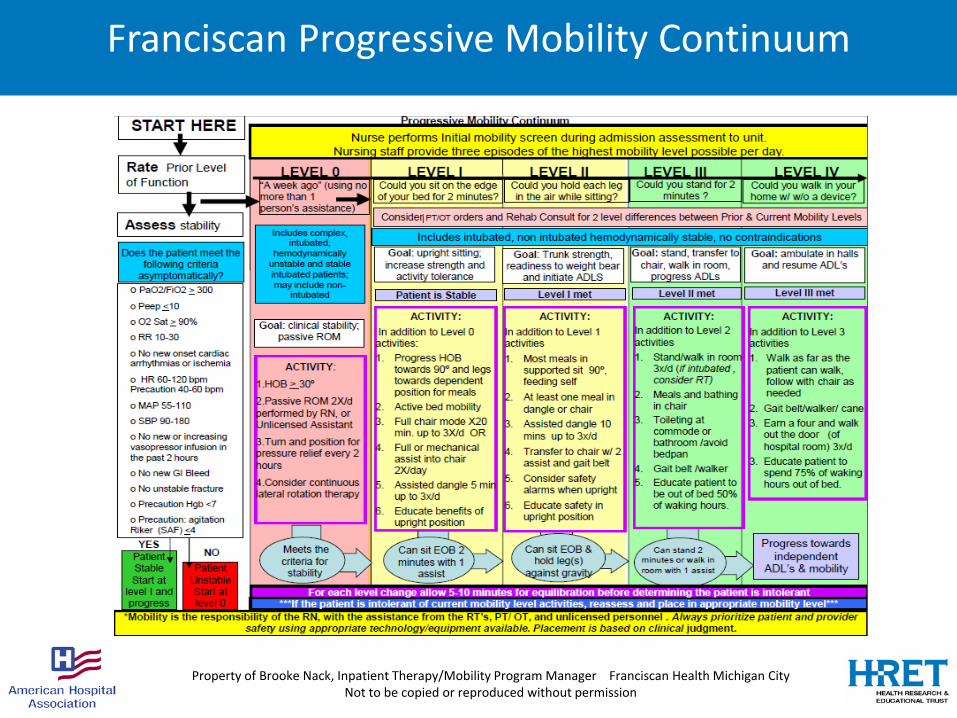
Franciscan Progressive Mobility Continuum
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
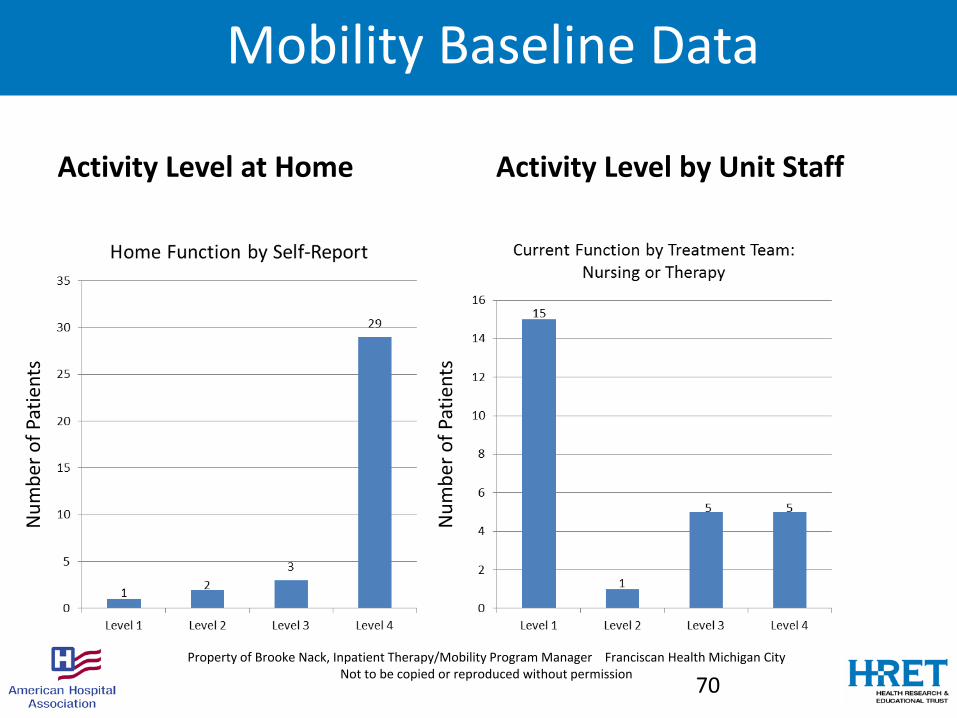
Mobility Baseline Data
Activity Level at Home Activity Level by Unit Staff
70Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
Num
ber o
f Pat
ient
s
Num
ber o
f Pat
ient
s
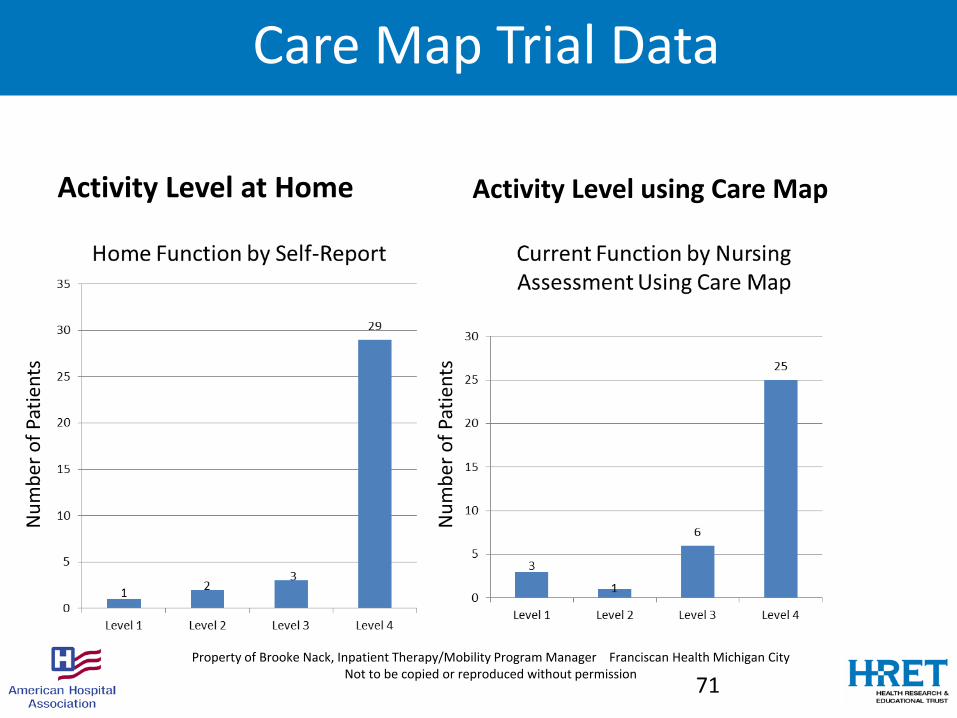
Care Map Trial Data
Activity Level at Home Activity Level using Care Map
71Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
Num
ber o
f Pat
ient
s
Num
ber o
f Pat
ient
s

Implementation Timeline
June July August September October November December FIRST QTR ‘16
10-1-15
MOBILITY TEAM GO-LIVE
Whole House Mobility Training and Stake-Holder Buy-In
Administrative Approval and Position Requests
Staff Surveys:
Mobility Needs and perceptions.
Analyze 4th Quarter 2015 Results
9-1-15
MOBILITY CARE MAP GO-LIVE
Culture of Mobility Mobility Team 1. Policies
2. Job Descriptions
3. Create Staff and patient Education Materials
Med Exec approval then
Announce and Interview for Positions
7-6-15
Patient Engage-ment Video Shoot
4-1-16
Assess performance
72Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
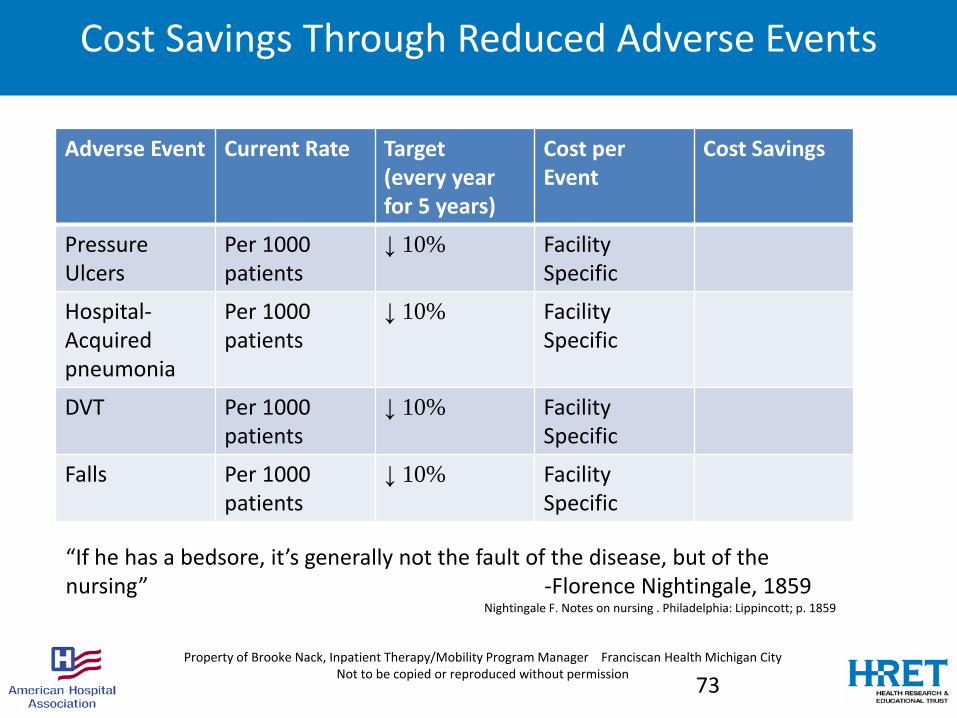
Cost Savings Through Reduced Adverse Events
Adverse Event Current Rate Target(every year for 5 years)
Cost per Event
Cost Savings
Pressure Ulcers
Per 1000 patients
↓ 10% Facility Specific
Hospital-Acquired pneumonia
Per 1000 patients
↓ 10% Facility Specific
DVT Per 1000 patients
↓ 10% Facility Specific
Falls Per 1000 patients
↓ 10% Facility Specific
“If he has a bedsore, it’s generally not the fault of the disease, but of the nursing” -Florence Nightingale, 1859
Nightingale F. Notes on nursing . Philadelphia: Lippincott; p. 1859
73Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission

Evidence-Based Goals for Mobility Program ROI
74
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission

Nursing Survey Results
Question 1 2 Neg Response 4 5 Pos. ResponseI always get enough information 3 11 14 20 4 24 Inadeq I have had enough training 0 10 10 18 10 28 Mobil I have enough equipment 2 15 17 16 6 22 Gait b I believe patients are more likely to fall 17 15 32 4 1 5I believe patients are resistant, so low satisfaction 17 16 33 5 1 6Mobility Masters = higher job satisfaction 0 3 3 15 17 32
Schedule 8-4:30 11-7:30 10-6:30 write in 9-5:30 later s 8 20 12 1 covers
Best result of Mobility Team: Job satisfaction Teamwork Pt satisfactionHealthcare OrgHope All of the above2 10 8 2 10 8
75Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission

“Move Me”: Engaging our Peers and our Patients…https://www.youtube.com/embed/e6BOqd0JPwc?rel=0
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission

Skills-Development for Progressive Mobility…Have a Little Fun
77Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
Idea to reality… Introducing our Mobility Team
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
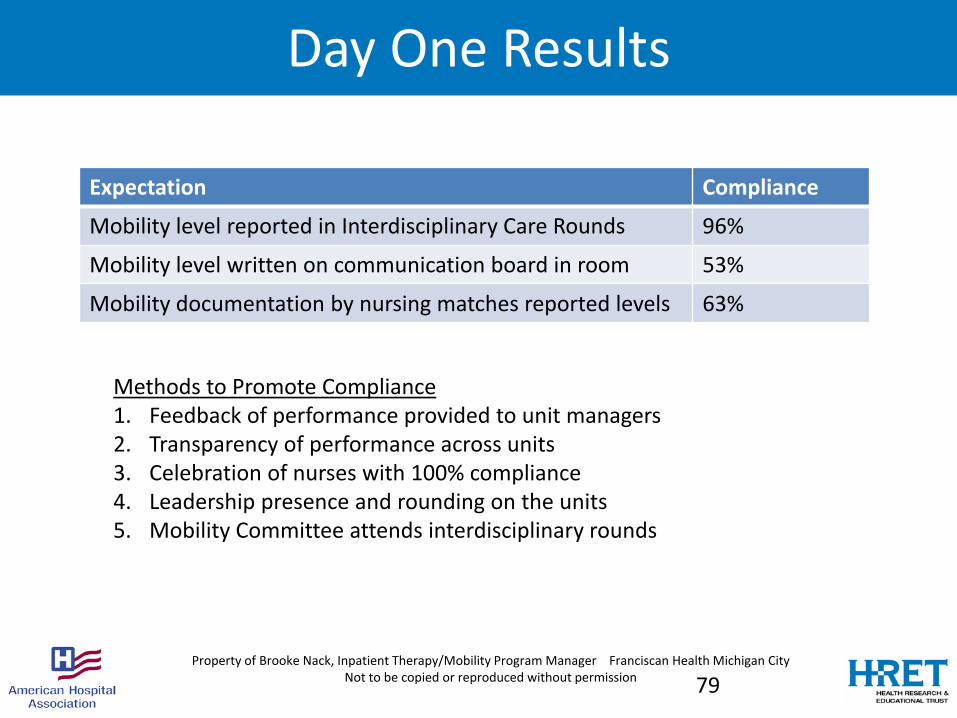
Day One Results
Expectation Compliance
Mobility level reported in Interdisciplinary Care Rounds 96%
Mobility level written on communication board in room 53%
Mobility documentation by nursing matches reported levels 63%
Methods to Promote Compliance1. Feedback of performance provided to unit managers2. Transparency of performance across units3. Celebration of nurses with 100% compliance4. Leadership presence and rounding on the units5. Mobility Committee attends interdisciplinary rounds
79Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City
Not to be copied or reproduced without permission
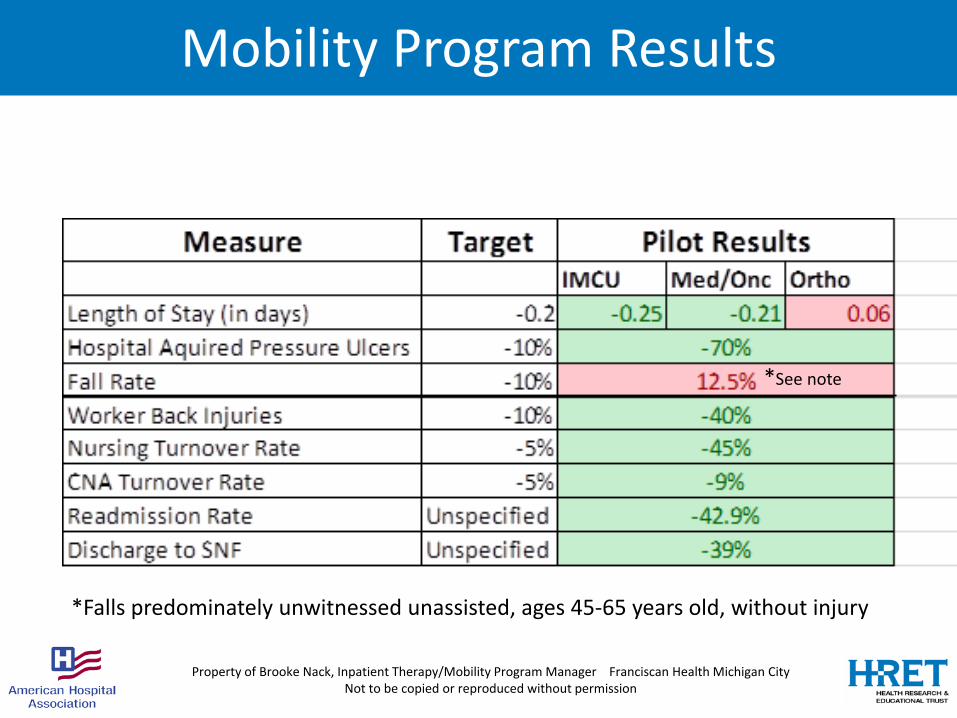
Mobility Program Results
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
*Falls predominately unwitnessed unassisted, ages 45-65 years old, without injury
*See note

Mobility Program Survey ResultsQuestion NURSING STAFF NON-NURSING PROFESSIONALS
Agree/Strongly Agree(n = 38-41)
Disagree/ Strongly Disagree(n = 1-3)
Agree/Strongly Agree(n = 14-19)
Disagree/Strongly Disagree
Patients receive more opportunities to move since Mobility Team
100% 0% 100% 0%
My patients are satisfied with the Mobility Team
100% 0% 100% 0%
The Mobility Team safely mobilizes patients
97% 3% 100% 0%
Parts of my job are easier because we have a Mobility Team
95% 5% 100% 0%
The Mobility Team has contributed to my job satisfaction
92% 8% 100% 0%
The Mobility Team contributes positively to DC planning
93% 7% 100% 0%
Property of Brooke Nack, Inpatient Therapy/Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
Mobility Program Survey Results April 2016
I see so many more patients now up in chairs and walking the halls. Great job! I think as the Mobility Team continues to work with our patients the need will increase even more. It will become the norm which is wonderful. Great program! (CNA)
Early Mobilization and discharge… Patients do get better with early ambulation. (RN)
Best results are decreased decubiti, decreased aspiration and overall reduced LOS. Excellent idea. Well managed and standardized. Easy to follow process. One of my favorite projects that has helped my patients tremendously. (Hospitalist)
Property of Brooke Nack, Inpatient Therapy /Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
Conclusion
It is feasible and effective for both community and university based healthcare organizations to make great strides in developing a Culture of Mobility.
A systematic team approach to mobility is key to a sustainable value and values based approach to preventing hospital acquired conditions.
Franciscan Health Michigan City’s Mobility Program is recognized as the Innovation Award winner by the Indiana Hospital Association at the Safety Summit on June 6, 2017.
For further information on Franciscan’s Mobility Program, contactBrooke Nack, Inpatient Therapy Manager
Brooke will be presenting a more detailed description of the Franciscan Mobility Program, including program development, return on investment, and corporate-wide dissemination in the Indiana Hospital Association Webinar titled: “GET UP: Improving Mobility in Indiana 4 of 4” on Tuesday December 12th at 2:00 pm CST.
Property of Brooke Nack, Inpatient Therapy /Mobility Program Manager Franciscan Health Michigan City Not to be copied or reproduced without permission
You have questions? We have answers
84
BRING IT HOME
85
Nerissa Legge, Program Manager| HRET

GET UP Resources• Mobility Assessments
– Get up and Go Test– Timed get up and go– BMAT: Banner Mobility Assessment Tool for Nurses
• Mobility Training Resources– "CAPTURE Falls" Mobility Training Videos
• Mobility Protocols– ICU Progressive Mobility Continuum– Med Surg Mobility Protocol
• Implementation Guide- ICU Liberation
• Early Mobility Resources- Early Mobility.com
86

GET UP Resources
• UP Resource Page on HRET HIIN Website
87
LISTSERV
• Join the LISTSERV® – Ask questions– Share best practices, tools and resources– Learn from subject matter experts– Receive follow up from this event and notice of
future events
Sign up at http://www.hret-hiin.org/engage/listserv.shtml
88

Upcoming Events
89
HRET HIIN Rural CAH Affinity Group Virtual EventTopic: Rural and Critical Access Hospitals (CAH) Webinar: November 27, 2017 1:00pm -2:00pm (CT)Register
Disparity exists in access to palliative services especially in the rural and frontier regions of our country. Register for the HRET HIIN Rural CAH Affinity Group Event on Monday, November 27th at 1pm CT to learn why this disparity exists and what rural communities are doing to address it. The event will feature Dr. Phil Lawson, an emergency room physician and palliative care director from Littleton Regional Hospital, a critical access hospital in New Hampshire. Dr. Lawson will dive into the patient, community and provider level drivers of disparity and offer strategies for organizations ready to fill the gap. We will then explore systems that support end of life conversations and advanced care planning for some practical next steps in addressing this important issue.

Thank You!
Find more information on our website: www.hret-hiin.org
Questions or Comments: [email protected]
90
Related Documents