Holistic Approach for Acute coronary syndrome กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกก กก. กกกกกกกก กกกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกกกกกก Acute coronary syndrome ( ACS ) กกก กกกกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก ( coronary arteries ) กกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกก กกก กกกกกกกกก atherosclerotic plaque กกกกกกกกกกกกกกกกก 1-2 กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกก กกกกกก กกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก ACS กกกกกกกก กกกกกกกกกกกก 1. Acute ST-segment elevated myocardial infarction ( STEMI) 2. Acute Non-ST- segment elevated myocardial infarction ( NSTEMI) กกก Unstable angina กกกกกกกกกกกกกกก ACS กกกกกกกกกกกก กกกกกกกกก กกกกกกกกกกกกกก กกกกกกกกกก กกกกกกก กกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกกกกกก sudden cardiac arrest กกกกกกกกกกกก กกกกกกกกกก ACS กกกก most common cause กกก sudden cardiac death 3-5 Holistic Approach ผผผผผผผ ACS ผผผผผผผผผผผผผ 3 ผผผผผผผ ผผผผผผผผผผผ 1. กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก 2. กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกก ACS กกกกกกกกก กกกกก กกกกกกกกก กกกกกกกกกกก ก ( Interventions) 3. กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกก กกกกกกก กกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกก กกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกก ACS กกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกกกก กกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก กกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกกก

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Holistic Approach for Acute coronary syndrome
การดู�แลผู้�ป่�วยโรคหลอดูเล�อดูห�วใจตี�บเฉี�ยบพล�น โดูย พญ. ธั�ญร�ตีน� อร ามเสร�วงศ์� สถาบ�นห�วใจเพอร�เฟคฮาร�ท โรงพยาบาล
ป่)ยะเวท
Acute coronary syndrome ( ACS ) ค�อ ภาวะท�,เก-ดูจาก การอ.ดูตี�นหร�อตี�บแคบของหลอดูเล�อดูห�วใจ ( coronary arteries ) อย างฉี�บพล�น ซึ่1,งสาเหตี.ส วนใหญ เก-ดูจาก
การแตีกตี�วของ atherosclerotic plaque เขาไป่ในหลอดูเล�อดู 1-2 และก อใหเก-ดูการจ�บตี�วก�นของเกร3ดูเล�อดู และล-,มเล�อดูภายในหลอดูเล�อดูท�,ไป่เล�4ยงห�วใจ ผู้ลส.ดูทาย ท5าให เก-ดูการขาดูเล�อดูไป่เล�4ยงห�วใจอย างฉี�บพล�น ACS โดูยรวมจะป่ระกอบไป่ดูวย1. Acute ST-segment elevated myocardial infarction ( STEMI)2. Acute Non-ST- segment elevated myocardial infarction ( NSTEMI) และ
Unstable angina อาการของผู้�ป่�วย ACS ท�,พบไดูบ อย ท�,ส.ดูค�อ เจ3บแน นหนาอก รองลงมาค�อ เหน�,อย หายใจอ�ดูอ�ดู ผู้�ป่�วยบางรายอาจมาโรงพยาบาลดูวยเร�,อง sudden cardiac arrest จากรายงานการศ์1กษาพบว า ACS เป่7น most common cause ของ sudden cardiac death3-5
Holistic Approach ผู้��ป่�วย ACS ขอแบ่�งออกเป่�น 3 ข��นตอน ดั�งต�อไป่น��1. การว-น-จฉี�ยแยกโรคและการดู�แลเบ�4องตีนท�,หองฉี.กเฉี-น
2. การร�กษาจ5าเพาะเจาะจงในแตี ละภาวะ ของ ACS รวมถ1งการใช้ยา และการท5า
ห�ตีถการตี าง ๆ ( Interventions)
3. การดู�แลผู้�ป่�วยหล�งจากผู้ านพนช้ วงว-กฤตีแลว เพ�,อใหผู้�ป่�วย กล�บบานไป่อย างป่ลอดูภ�ย และไม กล�บมาเป่7นซึ่54าอ�ก
การว-น-จฉี�ยแยกโรคและการดู�แลเบ�4องตีนท�,หองฉี.กเฉี-น ข�4นตีอนแรกน�4น าจะเป่7นข�4นตีอนท�,ส5าค�ญท�,ส.ดูเน�,องจาก ภาวะ ACS เป่7นภาวะท�,ฉี.กเฉี-นและเร งดู วน ถาใหการร�กษาไม ท�นการณ์� อาจช้ วยช้�ว-ตีไม ท�นและกลามเน�4อห�วใจท�,ขาดูเล�อดูแลวไม สามารถก�ใหค�นกล�บมาไดู ข��นที่�� 1 แยกผู้�ป่�วยท�,มาท�,หองฉี.กเฉี-นดูวยอาการดู�งตี อไป่น�4ค�อ เจ3บหนาอก แน นหนาอก
อ1ดูอ�ดูในอก หายใจไม สะดูวก หนาม�ดูเป่7นลม จ.กแน นล-4นป่=, อาการเหม�อนอาหารไม ย อย ใหส งส�ยว าเป่7น ACS และเขาส� Chest pain assessment pathway
ข�4นท�, 2. ใหการร�กษาเบ�4องตีนอย างท�นท�ท�นใดูดู�งตี อไป่น�4 ( ภายในเวลา 10 นาท� ) 1. Monitor EKG เตีร�ยมช้.ดู CPR พรอมท�4ง defribrillator ใหพรอม2. vital sign และ O2 satuation ให Oxygen 4 ล-ตีรตี อนาท� เพ�,อใหระดู�บ O2 sat > 90%
3. ให Aspirin Gr. V เค�4ยวท�นท� ถาผู้�ป่�วยไม ม�ป่ระว�ตี-แพยา Aspirin หร�อไม ม�ป่ระว�ตี- Active GI bleeding
4. ท5า EKG 12 lead ท�นท�

5. เป่)ดูเสนเล�อดู และเจาะเล�อดูเก3บไว เป่)ดูเสนเล�อดูใหน54าเกล�อเพ�,อเตีร�ยมไวในกรณ์�ฉี.กเฉี-น
6. เตีร�ยมให Nitroglycerin spray หร�อยา อมใตีล-4น ถาความดู�นโลห-ตี ดู� ( BP > 100
mmHg, HR อย� ระหว าง 50 ถ1ง 100 คร�4งตี อนาท�
7. เตีร�ยม ให Morphine 2-5 mg IV ถาให Nitroglycerin แลวไม หายเจ3บหนาอก
เพ�,อใหเก-ดูความรวดูเร3วและท�นเวลาขอ 1 ถ1ง 6 สามารถท5าไดูเลย ไม ตีองรอค5าส�,งแพทย� เพราะเป่>าหมายในข�4นท�, 1 น�4ตีองท5าไดูภายใน 10 นาท� แพทย�จะตีองมาซึ่�กป่ระว�ตี- ตีรวจร างกายอย างคร าว ๆ ส�,งตีรวจเล�อดู ส วนใหญ จะส ง
CBC, kidney function, Coagulogram, CKMB และ Troponin T หร�อ I
ยาท�,จ5าเป่7นตีองใช้ท�,หองฉี.กเฉี-น1. Aspirin ( acetylsalicylic acid , ASA) การให aspirin อย างรวดูเร3ว รวมท�4งการให
นอกโรงพยาบาล 6 สามารถอ�ตีราการเส�ยช้�ว-ตีไดูอย างช้�ดูเจน 7-9 ในผู้�ป่�วย ACS ท�4งสามกล. มเน�,องจาก Aspirin ออกฤทธั-?ตีาน การสราง Thromboxane A2 ในการเกาะตี�วก�นของเกร3ดูเล�อดู ( Platelet aggregation) การให aspirin ควรให เค�4ยวเพ�,อใหออกฤทธั-?ท�นท� ในขนาดู 160 ถ1ง 325 ม-ลล-กร�ม ถาผู้�ป่�วยก-นไม ไดูม�คล�,นไสอาเจ�ยนมาก อาจพ-จารณ์าใหในร�ป่แบบอ�,น เช้ น ใหทางน54าเกล�อ ( soluble, IV) หร�อ Aspirin
suppositories ( 300 mg) สอดูเขาทางทวารหน�กไดู2. Nitroglycerin ( NTG) NTG เป่7นอย าง anti-ischemic pain อย างดู� ออกฤทธั-?ขยายหลอดูเล�อดูโคโรนาร�โดูยตีรง นอกจากน�4นแลวย�งม�ผู้ลทาง hemodynamic ค�อลดูความดู�นและลดู
pulmonary wedge pressure ดูวย ถ1งแมยาไนเตีรทจะเป่7นยาท�,ใช้ลดูอาการไดูดู� แตี จากการศ์1กษา randomized control trial ไม พบป่ระโยช้น�ในแง การลดูอ�ตีราการเส�ยช้�ว-ตีใน
STEMI เพราะฉีะน�4นจ1งไม ม�การใช้ยาในเตีรทโดูยไม ม�ขอบ งช้�4 ดู�งตี อไป่น�4 เจ็�บ่แน�นหน�าอก (Ongoing Ischemic chest discomfort)
ความดั�นโลห"ตสู�ง pulmonary congestion จาก ACC/AHA guideline11-13 ท�4งใน STEMI และ NSTEMI ไดูแนะน5าแพทย�ใหอน.ญาตี-ใหผู้�ป่�วยอมยาใตีล-4นไดูเพ�ยง 1 เม3ดู ถาอาการไม ดู�ข14นหร�ออาการท.เลา แตี ย�งม�อาการอย� ใหร �บเร�ยกรถพยาบาลมาร�บ หามข�บรถมาโรงพยาบาลเอง เพราะอาจเก-ดูอ�นตีรายระหว างทางไดู แตี ถาผู้�ป่�วยมาท�,หองฉี.กเฉี-น หร�ออย� ในการดู�แลของบ.คคลากรทางการแพทย�อน.ญาตี-ให ไดูถ1ง 3 เม3ดูห างก�นท.ก 10 ถ1ง 15 นาท� ถาไม ม�ป่@ญหาเร�,องความดู�นตี5,า
ห�วใจเตีนเร3ว หร�อช้าเก-นไป่ หร�อในผู้�ป่�วยท�,ไดูร �บยา antiphosphodiesterease inhibitors
ท�,ใช้ในการร�กษาโรค electile dysfunction มาภายใน 24 ช้�,วโมง เพราะอาจท5าใหความดู�นตี5,ามากจนถ1งอ�นตีรายถ1งช้�ว-ตีไดู ( profound hypotension)
3. Morphine sulphate เป่7นยาแกป่วดูท�,เหมาะสมท�,จะใช้เพ�,อลดูอาการเจ3บหนาอกในภาวะ ACS ถาใช้ NTG แลวย�งไม ไดู ผู้ล นอกจากน�4นแลวจะช้ วยลดู pulmonary
congestion ดูวย

morphine ออกฤทธั-? เป่7น venodilator ลดู ventricular preload และความตีองการใช้ ออกซึ่-เจนของ กลามเน�4อห�วใจ ขนาดูท�,ใหม�กให 2- 4 ม-ลล-กร�มทางน54าเกล�อฉี�ดูเขาช้า ๆ
ผู้ลขางเค�ยงท�,พบบ อยม�กจะเป่7นอาการ คล�,นไสอาเจ�ยน ม�การศ์1กษาแบบ observation
study เม�,อไม นานมาน�4ไดูรายงานว า morphine sulphate อาจจะท5าใหผู้�ป่�วยเส�ยช้�ว-ตีมากข14น 13 Guideline ของ ACC/AHA UA/NSTEMI 2007 จ1งไดูลดูอ�นดู�บ การให morphine sulphate จาก class I เป่7น class IIa
Pitfall 1. แพทย� อาจพ-จารณ์าท5า portable CXR ไดู ถาคล�,นห�วใจป่รกตี- ( แตี หามส งผู้�ป่�วย
ไป่ท5า CXR ท�,หอง X-ray ถาย�งไม สามารถแยก ภาวะ ACS ออกไป่ไดู เพราะผู้�ป่�วยอาจเก-ดู cardiac arrest เม�,อใดูก3ไดู 2. การท5า CXR ควรท5าไดูภายในเวลา 30 นาท� ไม ควรเส�ยเวลารอท5า CXR เพราะจะท5าให
เส�ยโอกาสท�,จะเป่)ดูหลอดูเล�อดูห�วใจไป่ การท5า CXR ก3เพ�,อจะ rule out ภาวะอ�,น ท�,อาจม�อ�นตีรายถ1งช้�ว-ตี เช้ น Aortic dissection , acute pulmonary embolism หร�อ ภาวะ Pneumothorax โดูยเฉีพาะในกล. มผู้�ป่�วยท�,ม�คล�,นห�วใจป่รกตี- แตี ม�อาการมาก เช้ น ผู้�ป่�วยเจ3บหนาอกมาก ร วมก�บ ป่ระว�ตี- ความดู�นตี5,า และ shock หร�อ cardiac arrest มาก อน ควรดู� CXR เพ�,อมองหา widening of mediastinum ในภาวะ aortic dissection
3. ส วนผู้�ป่�วยท�,อาการเหน�,อยมาก แตี ฟ@งเส�ยงป่อดูป่รกตี- , O2 satuation ตี5,า ๆ คล�,น
ห�วใจไม พบความผู้�ป่รกตี- หร�อพบเพ�ยง sinus tachycardia หร�อพบภาวะ acute right
ventricular stain เช้ น S1Q3T3 pattern ( ร�ป่ 1) ซึ่1,งเป่7น pathonomonic sign ของ
acute pulmonary embolism ร วมก�บ X-ray ป่อดูป่รกตี- ควรร�บส งผู้�ป่�วยไป่ท5า CT-
pulmonary artery เพ�,อ rule out acute pulmonary embolism
4. โดูยสร.ป่ค�อถาผู้�ป่�วยมาดูวยอาการเจ3บแน นหนาอกคร�4งแรก ในภาวะฉี.กเฉี-น ควรว-น-จฉี�ยแยกโรค 3 สามโรคท�,เป่7นอ�นตีรายถ1งช้�ว-ตี ( Triple rule out = ACS,
Pulmonary embolism และ Aortic dissection ) ท�,เหล�อสามารถรอ และป่ร1กษาผู้�เช้�,ยวช้าญภายหล�งไดู
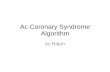
ข��นที่�� 2 แบ่�งผู้��ป่�วยออกเป่�นกล%�มโดัยใช้� EKG เป่�นต�วแยก ( Algorithm ท�, 1 )
กล%�มที่�� 1 ไดั�แก� ST elevation หรื)อ New Left Bundle Branch Block โดัยม�ค*าจ็*าก�ดัความดั�งต�อไป่น��- EKG ม� ST- segment elevation มากกว�า หรื)อเที่�าก�บ่ 1 mm ( 0.1 mV) โดัยม�ต"ดัก�นมากกว�า 2 leads
- ม� New Left Bundle Branch Block เก"ดัข+�น ( โดัยม�คล)�นห�วใจ็เก�าเป่รื�ยบ่เที่�ยบ่)
กล%�มที่�� 2 ม� Ischemic ST- Segment depression มากกว�าหรื)อเที่�าก�บ่ 0.5 mm ( 0.05
mV) หรื)อม� dynamic T-wave inversion ในขณะที่��ม�เจ็�บ่หน�าอก เรืาจ็ะเรื�ยกผู้��ป่�วยกล%�มน��ว�าเป่�น High risk unstable angina หรื)อ Non-STEMI ( ถ้�าม� CKMB ข��น)

ผู้��ป่�วยที่��ม� Non-persistent หรื)อ transient ST-segment elevation มากกว�าหรื)อเที่�าก�บ่ 5
mm แต�น�อยกว�า 20 นาที่�ก�จ็�ดัเข�าอย��ในกล%�มน��ดั�วยกล%�มที่�� 3 ค)อ กล%�มที่��ม�คล)�นห�วใจ็ป่รืกต" หรื)อ ม�คล)�นห�วใจ็ที่��ไม�สูามารืถ้ว"น"จ็ฉั�ยจ็�ดัเข�าในกล%�มแรืกหรื)อกล%�มที่��สูองไดั� ( Non- diagnostic EKG)
Cardiac biomarker Cardiac myomarker ใหม ๆ เช้ น Troponin T และ Troponin I จะม�ความไว และ
ความจ5าเพาะส�งกว า Myocardia muscle creatinine Kinase Isoemzym ( CK-MB) ท�4งในแง การว-น-จฉี�ยและการบอกพยากรณ์�โรค ในผู้�ป่�วย Unstable angina/ NSTEMI การเพ-,มข14นของระดู�บ Cardiac Troponin จะส�มพ�นธั�ก�บอ�ตีราการเส�ยช้�ว-ตีและการเพ-,มข14นของ cardiac
event อย างม�น�ยส5าค�ญ 6 Cardiac Biomarker ควรจะไดูร�บการเจาะตีรวจตี�4งแตี ท�,หองฉี.กเฉี-น แตี การตี�ดูส-นใจการร�กษาโดูยเฉีพาะในกล. ม STEMI ไม ตีองรอผู้ลเล�อดูกล�บมาเน�,องจากจะท5าใหเก-ดูความล าช้าและเส�ยหายมากข14น เพราะ Cardiac Biomarker ท�,เราม�ใช้ในป่@จจ.บ�น ม�ความไวไม มากพอใน 4-6 ช้�,วโมงแรก ยกเวนในผู้�ป่�วยบางรายเท าน�4นท�,มาพบแพทย�ช้ากว า 4-
6 ช้�,วโมงหล�งจากเร-,มม�อาการเจ3บแน นหนาอก ดู�งแสดูงในร�ป่ท�, 27 ส วนการใช้ Myoglobin ถ1งแมจะใช้ไดูดู�ในช้ วง early detection ค�อระดู�บในเล�อดูจะข14นหล�งจากม� myocardial injury
ป่ระมาณ์ 2 ช้�,วโมง แตี ความจ5าเพาะก3ย�งค อนขางตี5,าอย� จ1งไม ไดูน5ามาใช้ช้ในทางคล�น-คมากน�ก ในอนาคตีอาจจะม�การใช้ biomarker อ�,น ๆ ร วมดูวยในการป่ระเม-นผู้�ป่�วย ACS อย างเช้ น CRP และ BNP พบว าการใช้ multimarker approach อาจไดูผู้ลดู�กว าการใช้ marker
เพ�ยงหน1,งหร�อสองตี�วอย างท�,ใช้ในป่@จจ.บ�น 8-9
ในตีารางท�, 1 จะสร.ป่ขอดู�และขอเส�ยของ Cardiac Marker แตี ละช้น-ดู Cardiac Troponin 1. Powerful tool for risk stratification
2. Greater sensitivity and specificitythan CK-MB3. Detection of recent MI up to
1. Low sensitivity in veryearly phase of MI(less than 6 h aftersymptom onset) and

2 weeks after onset4. Useful for selection of therapy5. Detection of reperfusion
requires repeatmeasurement at 8 to12 h, if negative2. Limited ability todetect late minorreinfarction
CK-MB 1. Rapid, cost-efficient, accurateassays2. Ability to detect early reinfarction
1. Loss of specificityin setting of skeletalmuscle disease orinjury, includingsurgery2. Low sensitivity duringvery early MI (less than6 h after symptomonset) or later aftersymptom onset (morethan 36 h) and forminor myocardialdamage (detectablewith troponins)
Myoglobin 1. High sensitivity2. Useful in early detection of MI3. Detection of reperfusion4. Most useful in ruling out MI
1. Very low specificity insetting of skeletalmuscle injury ordisease2. Rapid return to normalrange limits sensitivityfor later presentations
การดู�แลร�กษาในผู้�ป่�วยในกล. มท�, 1 ( STEMI ) ท�,ส5าค�ญท�,ส.ดูค�อการืเป่0ดัหลอดัเล)อดั( Reperfusion ) ใหท�นเวลา ไม ว าจะเป่7นการเป่)ดูหลอดูเล�อดูโดูยการใช้บ�ลล�น ท�,เร�ยกว า Primary percutaneous balloon angioplasty หร�อ Primary Percutaneous Coronary
Intervention ( Primary PCI ) หร�อการใช้ยาสลายล-,มเล�อดู ( Fibrinolytic drug) ไม ว าจะเป่)ดูหลอดูเล�อดูดูวยว-ธั�ใดู ตีองเป่)ดูใหท�นเวลา โดูยก5าหนดู ให Door to balloon time นอยกว า หร�อเท าก�บ 90 นาท� ค�อตี�4งแตี เวลาท�,ผู้�ป่�วยเขามาถ1งโรงพยาบาลจนถ1งเวลาท�,ผู้�ป่�วยไดูร�บการขยายหลอดูเล�อดูดูวย บ�ลล�น ตีองนอยกว า 90 นาท�Door to needle time นอยกว า หร�อเท าก�บ 30 นาท� ค�อ ตี�4งแตี เวลาท�,ผู้�ป่�วยมาถ1งโรงพยาบาลจนกระท�,งไดูยาตีองนอยกว า 30 นาท� ตีารางท�, 2 แสดูง ข�4นตีอนตี าง ๆ ในการ ป่ระเม-นทางเล�อกของการเป่)ดูหลอดูเล�อดู
( reperfusion options ในผู้�ป่�วย STEMI
ข�4นท�, 1 ป่ระเม-นเวลาและความเส�,ยง
เวลาตี�4งแตี เร-,มม�อาการ
ความเส�,ยงของ STEMI ( killip classification)
ความเส�,ยงของ ยา Fibrinolytic
เวลาท�,ใช้ในการยายผู้�ป่�วยไป่ท5า PCI
ข�4นท�, 2 เล�อกว าจะให เป่)ดูหลอดูเล�อดูโดูยว-ธั�ใดู ถาผู้�ป่�วยมาถ1งโรงพยาบาลนอยกว า 3 ช้�,วโมงหล�งเจ3บหนาอกและระยะเวลาในการยาย ผู้�ป่�วยไม นาน เล�อกไดูท�4ง 2 ว-ธั�ควรืเล)อก Fribinolytic drug เม)�อ
1. Early presentation ( นอยกว า 3 ช้�,วโมง)

2. ไม ม� Catheterization laboratory ท�,ม�ความช้5านาญอย� ใกล 3. Door to balloon – Door to needle time มากกว า 1 ช้�,วโมง
ควรืเล)อก Primary PCI เม)�อ
1. Late presentation ( มากกว า 3 ช้�,วโมง)
2. ไม แน ใจในการว-น-จฉี�ย ไม แน ใจว าเป่7น STEMI หร�อไม ( การท5า PCI จะป่ลอดูภ�ย
กว าการใหยาละลายล-,มเล�อดู )
3. ม�ขอหามในการใหยาละลายล-,มเล�อดู และในผู้�ป่�วยท�,ม�ความเส�,ยงตี อการเก-ดู เล�อดูออกในสมองส�ง
4. High risk for STEMI เช้ น Cardiogenic shock , Killip class มากกว าเท าก�บ 3
ยาละลายล-,มเล�อดู ( Fibrinolytics) เม�,อพ-จารณ์าใหยา fibrinolytics ตีองป่ระกอบไป่ดูวย
1. ม� ST-segment elevate มากกว า 1 mm ตี-ดูก�น 2 lead หร�อม� new LBBB ( class I) หร�อคล�,นห�วใจเขาไดูก�บ posterior wall infarction ( Class IIa)
2. ไม ม�ขอหาม ( contraindication ) 3. อาการเป่7น นอยกว า 12 ช้� ,วโมง
Fibrinolytic Therapy: Contraindications and Cautions for Fibrinolytic Use in STEMI From ACC/AHA 2004 Guideline
Update* Absolute Contraindications • Any prior intracranial hemorrhage • Known structural cerebral vascular lesion (eg, AVM) • Known malignant intracranial neoplasm (primary or metastatic) • Ischemic stroke within 3 months EXCEPT acute ischemic stroke within 3 hours • Suspected aortic dissection • Active bleeding or bleeding diathesis (excluding menses) • Significant closed head trauma or facial trauma within 3 monthsRelative Contraindications • History of chronic, severe, poorly controlled hypertension • Severe uncontrolled hypertension on presentation (SBP >180 mm Hg or DBP >110 mm Hg) • History of prior ischemic stroke >3 months, dementia, or known intracranial pathology not covered in contraindications • Traumatic or prolonged (>10 minutes) CPR or major surgery (<3 weeks) • Recent (within 2 to 4 weeks) internal bleeding • Noncompressible vascular punctures • For streptokinase/anistreplase: prior exposure (>5 days ago) or prior allergic reaction to these agents • Pregnancy • Active peptic ulcer • Current use of anticoagulants: the higher the INR, the higher the risk of bleeding
การใหยา Fibinolytic drug ควรใหเร3วท�,ส.ดูเท าท�,จะท5าไดู ถาสามารถให fibrinolytic drug
ไดูภายในเวลา 70 นาท�หล�งจากม�อาการจะลดูอ�ตีราการเส�ยช้�ว-ตีถ1ง 75% จากขอม�ล 22
randomized controlled trial พบว า การให fibrinolytic drugs จะร�กษาช้�ว-ตีผู้�ป่�วยไวไดู 131 คนจากการร�กษา 1,000 ถาสามารถใหไดูใน 3 ช้�,วโมงแรก หล�งจากน�4นจะม�ป่ระโยช้น�เล3กนอย แตี ถาเก-น 12 ช้�,วโมงจะไม ไดูป่ระโยช้น� โดูยป่รกตี- ถาผู้�ป่�วยม�อาการมากกว า 12
ช้�,วโมงจะไม ใหยา fibrinolytic เลย ยกเวนแตี ใน ผู้�ป่�วยท�,ย�งม� ย�งม� ST-segment elevate
มากกว า 1 mm และร วมก�บอาการเจ3บแน นหนาอกมาก และถาเลย 24 ช้�,วโมงแลว ยา

Fibrinolytic drugs ไม ควรใหเป่7นอย างย-,ง ส วนผู้�ป่�วยท�,เป่7น cardiogenic shock ก3ไม ควรให fibrinolytic drug ควรจะเล�อกท5า Primary PCI มากกว าช้น-ดูของ fibrinolytic drug โดูยท�,วไป่ Fibrinolytic drug จะม�หลายร. น แตี ท�,เป่7นท�,น-ยมท�,ส.ดูในป่ระเทศ์ไทย ค�อ
streptokinease ซึ่1,งเป่7น Nonselective fibrinolytic agent
streptokinease ม� 90% patency rate เพ�ยง 50% และ ม� TIMI 3 flow เพ�ยง 32 %
เท าน�4น หมายถ1งท�, 90 นาท�ในผู้�ป่�วยท�,ไดู SK ถาไป่ฉี�ดูส�ดู�จะม�เพ�ยง คร1,งเดู�ยวเท าน�4น ท�, หลอดูเล�อดูเป่)ดูดู� ส วน ยาอ�,น ๆ เช้ น Alteplase , Reteplase และ TNK-t-PA ซึ่1,งเป่7น
fibrin-specific fibrinolytic drug ถ1งแมจะม� ป่ระส-ทธั-?ภาพดู�กว า ม� patency rate ท�,ส�งกว า แตี ม� โอกาสเก-ดู Hemorrhagic stroke ไดูส�งกว าเช้ นเดู�ยวก�น นอกจากน�4นแลวราคาย�งส�งกว ามาก
Streptokinease จ1งย�งเป่7นยาท�,ไดูร �บความน-ยมอย� ในโรงพยาบาลตี าง ๆ เราจ1งจ5าเป่7นตีองร� จ�กว-ธั�การให streptokinease เป่7นอย างดู� ส วน ยา TNK-t- PA เป่7น fibrinolytic
drug ท�,ใช้ง ายเพราะใหเป่7น bolus dose ตีามน54าหน�กตี�วไดู ไม จ5าเป่7นตีองใช้ส�ตีรการใหท�,สล�บซึ่�บซึ่อน แบบ t-PA อ�,น ๆและ side effect ค อนขางนอยจ1งเป่7นยาท�,อาจจะม�โอกาสไดูใช้ในอนาคตีค อนขางมากถาราคาไม ส�งจนเก-นไป่
Tip and trick ในการให SK
ใหช้า ๆ ทางน54าเกล�อ อาจให hydrocortisone 100 mg ก อน ให SK เพ�,อลดู reaction แมไม ม� evidence
base ร�บรองเร�,องน�4แตี จากป่ระสบการณ์�พบว าไดูผู้ลค อนขางดู� เตีร�ยม ยาแกคล�,นไสอาเจ�ยนไว เพราะผู้�ป่�วยอาจม�อาการคล�,นไสหล�งให ผู้สมใน NSS หร�อ 5% D/W 100 cc drip in 1 hr
ระหว างให ตีอง monitor EKG และ BP ตีลอดู เพราะ อาจเก-ดู arrhythmia ระหว าง
drip ไดูตีลอดูเวลา โดูยเฉีพาะ Ventricular tachycardia และ ventricular fibrillation
ม�กจะเก-ดูตีอน หลอดูเล�อดูเป่)ดู หร�อบางคร�4งอาจเก-ดู bradycardia หล�งเป่)ดูไดู ก อนใหหร�อหล�งใหไม ควร ท5าห�ตีถการตี าง ๆ เช้ น cut down หร�อ แทง central line
ใส foley catheter ตีองระว�งมาก ๆ ถาตีองการท5า ห�ตีถการจร-ง ๆ ควรรอหล�งจากใหยาไป่แลวนานกว า 24 ช้�,วโมง
ค.ณ์ล�กษณ์ะของ fibrinolytic drugs ท�,จะไดูม�โอกาสไดูใช้ในป่ระเทศ์ไทย
Streptokinease TNK-t-PA
Dose 1.5 MU in 30-60 min 30-50 mg Push
Antigenic Yes No

Allergic reaction ( Hypotension)
Yes No
90 นาท� patency rate 50% 75%
TIMI 3 32% 63%
ควรเส�,ยงของการใหยา fibrinolytic drugs ท�,ส5าค�ญท�,ส.ดูค�อ intracranial hemorrhage ซึ่1,งจะมากหร�อนอยข14นอย� ก�บ ป่@จจ�ยดู�งตี อ
ไป่น�4อ�นไดูแก 1. อาย. ( > 65 ป่=) 2. น54าหน�กตี�วนอย ( < 70 ก-โลกร�ม)
3. ความดู�นโลห-ตีส�ง ( > 180/110)
4. การใช้ tPA ( ซึ่1,งตีองใหร วมก�บ heparin หร�อ LMWH) จะม�ความเส�,ยงส�งกว าการให SK
ความเส�,ยงของการเก-ดู Hemorrhagic stroke จะอย� ท�, 0.25 ถ1ง 2.5% ถาม�ความเส�,ยงมากกว า 3 ขอ
ป่ระโยช้น�ท�,ไดูจากการให fibrinolytic และภาวะแทรกซึ่อนท�,อาจจะเก-ดูข14นไดูเป่7นส-,งท�,แพทย�ตีองอธั-บายใหผู้�ป่�วยและญาตี-ทราบอย างละเอ�ยดู ก อนท�,จะเร-,มใหยา
จ็*าเป่�นต�องให� Heparin หรื)อ LMWH ต�อหล�งจ็ากให� fibrinolytic drug
หรื)อไม� ? ถ้�าเป่�น Fibrin specific fibrinolytic จ็*าเป่�นต�องให� Heparin drip หรื)อ
LMWH ต�อ แต�ถ้�าเป่�น SK ไม�จ็*าเป่�นต�องให� Anticoagulant ( Heparin
หรื)อ LMWH ) ต�อ อ�ก ยกเว�นในกรืณ�ที่��ผู้��ป่�วยจ็ะม�โอกาสูจ็ะเก"ดั systemic
embolism สู�งเช้�น1. Extensive anterior wall myocardial infarction2. Atrial fribrillation 3. เก"ดั TIA หรื)อ Ischemic stroke
4. ม� Left ventricular thrombus
5. ผู้��ป่�วย ambulate ไม�ไดั� ต�องการืให�เพื่)�อป่2องก�น deep vein thrombosis
ยาอ)�น ๆ ที่��อาจ็จ็ะ ให�รื�วมดั�วยป่รืะกอบ่ไป่ดั�วย 1. Beta Blocker ควรใหในท.กรายท�,ไม ม�ขอหาม เพราะยา Beta-Blocker ลดู
ท�4ง mortality rate, infarct size ลดู Reinfarction และการเส�ยช้�ว-ตีอย างฉี�บพล�น ดู�งน�4นถาไม ม�ขอหามท�,ส5าค�ญ เช้ น ไม ม� Heart block, ไม ม� Heart

Failure ไม ม� Severe Bronchospasm ผู้�ป่�วยควรไดูร�บ Beta-blocker
การใหยา Beta-blocker ควรเร-,มใหท�ละนอยและค อย ๆ เพ-,มขนาดู ถาม�ยา IV สามารถใหแบบ IV form ไดูแตี ในป่ระเทศ์ไทยขณ์ะน�4ไม ม�ยา Beta-
Blocker แบบ IV form เลย จ1งตีองใหแบบร�บป่ระทานเท าน�4น2. Inhibitor of Renin – Angiotensin- Aldosterone System ( RAS)
a. ACE Inhibitor ยากล. มน�4จะลดู Ventricular remodeling และป่ร�บเป่ล�,ยน Hemodynamic ของ heart failure ใหดู�ข14น การใหยาในกล. มน�4สามารถลดูอ�ตีราการเส�ยช้�ว-ตีไดูอย างม�น�ยส5าค�ญโดูยเฉีพาะการใหในว�นแรกของการเก-ดู AMI แตี ป่@ญหาท�,ส5าค�ญและตีองระว�งค�อเร�,องของความดู�น ถาความดู�นไม ตี5,ากว า 100 mmHg ควรใหท.กราย ยาท�,ไดูร �บการพ-ส�จน�ว าม�ป่ระโยช้น�ค�อ Ramipril, Trendolapril, และ Captopril การใหควรใหโดูยการร�บป่ระทาน และเร-,มใหตี�4งแตี 24 ช้�,วโมงแรกหล�งเก-ดู STEMI
Dosage of ACEI from studies after MI - LV dysfunction with or without HF
SAVE, 1992 Captopril 50 mg t.i.d.AIRE, 1993 Ramipril 5 mg b.i.d.TRACE, 1995 Trandolapril 4 mg daily
b. Angiotensin receptor blockage ใหผู้ลดู�แบบเดู�ยวก�บ ACEI แตี ราคาแพงกว ามาก เพราะฉีะน�4นจ1งอาจเล�อกยากล. มน�4ใหเฉีพาะในผู้�ป่�วยท�,ม�ขอหามตี อการให ACEI เช้ น ในผู้�ป่�วยท�,ม�ไอมาก และ ม� angioedema
c. Aldosterone blockage เป่7นข�4นตีอนส.ดูทายท1,จะย�บย�4งระบบ RAS
จากการศ์1กษา EPHESUS โดูยให ยา epherenone เท�ยบก�บการร�กษาอ�,น ๆ
ท�,วไป่ในผู้�ป่�วย Acute MI ท�,ม� left ventricular dysfunction พบว า ลดูอ�ตีราการเส�ยช้�ว-ตี แตี เก-ดู hyperkalemia เพ-,มข14น เพราะฉีะน�4นผู้�ป่�วย acute MI ท�,ม� LV dysfunction ควรไดูร�บยากล. มน�4โดูยระม�ดูระว�งเร�,อง hyperkalemia
3. Clopidogrel เป่7นยาตีานเกร3ดูเล�อดูท�,ออกฤทธั-?ย�งย�4ง ADP ซึ่1,งเป่7นขบวนการ Platelet Ativation สามารถใหแทน Aspirin ไดูในผู้�ป่�วยท�,ม�ขอหามของการให aspirin หร�อใหร วมก�บ aspirin ไดูในผู้�ป่�วย STEMI จากการศ์1กษา Randomized controlled trial , CLARITY- TIMI- 26 และ COMMIT trials พบว าการให Clopidogrel ร วมก�บ aspirin ลดูอ�ตีราการเก-ดู recurrent infarction เม�,อเท�ยบก�บการให aspirin อย างเดู�ยว
4. HMG Coenzyme A reductase Inhibitors ( statins)การใหยา Statin ใน ACS เพ�,อลดู inflammation และ complications
ตี าง ๆ เช้ น Reinfartion, Recurrent angina และ arrhythmia โดูยเฉีพาะเม�,อใหภายในว�นแรกๆ ของโรค ถ1งแมว าขอม�ลสน�บสน.นจะย�งไม มากพอ
แตี การให statin สามารถใหไดูอย างป่ลอดูภ�ยถ1งแมว าจะไม ม�ระดู�บไขม�นในเล�อดูส�งก3ตีาม

5. GPIIb/IIIa antagonist เป่7นยาตีานเกร3ดูเล�อดูท�,ข� 4นตีอนส.ดูทายของ
platelet aggregation หล�กฐานการใช้ยากล. มน�4ย�งไม ม�มากในผู้�ป่�วย
STEMI จะใหยากล. มน�4เฉีพาะในผู้�ป่�วยท�,ไดูร �บการท5า PCI เท าน�4น6. Calcium Channel blocker
ยากล. มน�4อาจจะพ-จารณ์าใหในผู้�ป่�วย acute MI เฉีพาะในผู้�ป่�วยท�,ม� contraindication ตี อยาตีานเบตีาเท าน�4น เพราะยากล. มน�4ไม ม�หล�กฐานพ-ส�จน�ว าลดูอ�ตีราการเส�ยช้�ว-ตีในผู้�ป่�วย Acute MI
การร�กษาอ�,น ๆ ท�,อาจจะจ5าเป่7นตีองใช้ในผู้�ป่�วย Acute MI1. Intra- aortic balloon pump ( IABP) เป่7น บ�ลล�น ขนาดูใหญ ท�,ใส เขาไป่ใน aorta เพ�,อป่@4 มเพ-,มเล�อดูไป่เล�4ยงห�วใจขณ์ะท�,ห�วใจคลายตี�ว ( diastole) และ บ�ลล�นหดูตี�วท�นท�ในช้ วงท�,ห�วใจบ�บเล�อดูไป่เล�4ยงร างกาย ( Systole) แรงจากการหดูตี�วท�นท�จะช้ วยลดู after load ท5าใหผู้ อนการท5างานของห�วใจลง ขอบ งช้�4ในการใช้ IABP ค�อ Cardiogenic shock การใช้ IABP จะช้ วยป่ระค�บป่ระคองผู้�ป่�วยท�,เป่7น
cardiogenic shock ผู้ านพนช้ วงเวลาท�,ว-กฤตีไป่ไดู2. Primary VF พบบ อยมากในผู้�ป่�วย Acute STEMI โดูยเฉีพาะเม�,อ 4 ช้�,วโมงแรก แตี ม�ผู้ลตี ออ�ตีราการเส�ยช้�ว-ตีในช้ วง 24 ช้�,วโมงแรก ส วน Secondary VF จะเก-ดูข14นตีามมาเน�,องจากม� Cardiogenic shock หร�อ congestive heart failure การใหการร�กษาดูวยยาตีานเบตีาจะลดูอ.บ�ตี-การณ์�ของการเก-ดู primary VF
การใหยา Lidocaine IV drip หล�งการเก-ดู VF ไม ม�หล�กฐานว าลดูการเก-ดู VF ซึ่54า แตี การใหยาตีานเบตีาในกล. มท�,ไม ม� contraindication จะม�ป่ระโยช้น�มาก ถาผู้�ป่�วยไดูร�บ Lidocaine อย� ไดู อน.ญาตี-ให drip ตี อไดู แตี ไม ควรเก-น 24 ช้�,วโมง
3. เพ�,อป่>องก�นการเก-ดู arrhythmia ผู้�ป่�วย Acute STEMI ควรม�ระดู�บ K > 4 mEq/L และระดู�บ Megnesium > 2 mEq/L แตี การให rountine magnesium ไม ม�ป่ระโยช้น�
การดู�แลผู้�ป่�วยในกล. มท�, 2 Non-STEMI หร�อ high risk unstable angina
ว�ตีถ.ป่ระสงค� เพ�,อป่>องก�น ไม หลอดูเล�อดูท�,ตี�บเก�อบจะตี�น กลายเป่7นหลอดูเล�อดูท�,ตี�น 100%
เพราะฉีะน�4น การร�กษาท�,ส5าค�ญค�อ ใหยาตีานการเกาะก�นของล-,มเล�อดูและเกร3ดูเล�อดู
( anticoagulant และ anti-platelet) และลดูการท5างานของห�วใจใหนอยท�,ส.ดู ป่ระค�บป่ระคองไม ใหเก-ดูภาวะแทรกซึ่อน และ เก-ดูการขาดูเล�อดูมากข14น การร�กษาในผู้�ป่�วยกล. มน�4ย�งพอม�เวลาใหรอ อาจพ-จารณ์าฉี�ดูส�สวนห�วใจและท5า PCI ในกล. มท�,ม�ล�กษณ์ะเส�,ยงส�ง โดูยดู�ตีาม
Brundwald Risk Strafication ( ตีารางท�, 3 ม� TIMI risk score ส�ง เร�ยกว-ธั�น�4ว า early
invasive หร�อ อาจจะพ-จารณ์าใหยาก อน แลวดู�ว า ผู้�ป่�วย อาการดู�ข14น แลวค อยไป่ฉี�ดูส�สวนห�วใจก3ไดูเช้ นก�น ( early conservative)
ผู้�ป่�วย high risk ดู�งตี อไป่น�4ควรไดูร�บการร�กษาแบบ early invasivePatient CharacteristicRecurrent angina or ischemia at rest or with low-levelactivities despite intensive medical therapyElevated cardiac biomarkers (TnT or TnI)New or presumably new ST-segment depressionSigns or symptoms of HF or new or worsening mitralregurgitation

High-risk findings from noninvasive testingHemodynamic instabilitySustained ventricular tachycardiaPCI within 6 monthsPrior CABGHigh risk score (e.g., TIMI, GRACE)Reduced left ventricular function (LVEF less than 40%)
ยาท�,ใช้ร �กษาผู้�ป่�วยกล. มน�4ท�,ส5าค�ญค�อAntiplatelete และ Anticoagulant เพ�,อป่>องก�นไม ใหหลอดูเล�อดูตี�บมากข14น ส วนท�,เหล�อก3เช้ นเดู�ยวก�บกล. มของ STEMI ค�อ Beta blocker , ACEI, ARB, Statin เพ�,อลดู cardiac
event ท�,จะเก-ดูข14นช้ วงส�ป่ดูาห�แรกRecommendation Class I ส5าหร�บ antiplatelet ในผู้�ป่�วย UA/NSTEMI
1. Aspirin ตีองใหท.กรายในขนาดูเร-,มตีนท�, 160- 325 mg ตี อว�น2. ถาแพ Aspirin หร�อ ม� Severe active GI bleeding ให Clopidogrel ( loading 300
mg ตีามดูวย 75 mg ตี อว�น) แทน3. ถาผู้�ป่�วยม�ป่ระว�ตี- GI bleeding ควรใหยา Proton pump inhibitor ร วมดูวยในผู้�ป่�วย
ท�,ไดูร �บ aspirin หร�อ ไดูร�บ aspirin ร วมก�บ clopidogrel
4. Clopidogrel ควรจะใหร วมก�บ aspirin ในผู้�ป่�วยท�,เล�อกจะใช้ early conservative
strategy โดูยใหอย างนอยนาน 1 เดู�อนและถาใหดู�ท�,ส.ดูควรใหนาน หน1,งป่=5. ยา GPIIb/IIIa antagonist ควรใหในผู้�ป่�วยท�,เป่7น กล. ม high risk ( TIMI risk score
ส�ง ) และในกล. มท�,วางแผู้นว าจะท5า PCI โดูยยาท�,ม�หล�กฐานว าใช้ไดูป่ระโยช้น�ในผู้�ป่�วย UA/NSTEMI ท�,ไม ไดูท5า PCI ค�อ Tirofiban และ Epifibatide ส วน ยา Abciximab
ใหสงวนไวใช้เฉีพาะผู้�ป่�วยท�,ม�การวางแผู้นว าจะท5า PCI เท าน�4น
Recommendation ส5าหร�บการใช้ anticoagulant ใน UA/NSTEMI
ผู้�ป่�วยท.กรายท�,ไดูร �บการว-น-จฉี�ยเป่7น UA/NSTEMI ควรไดูร�บการร�กษาดูวยยา
anticoagulant ตี�วใดูตี�วหน1,งดู�งตี อไป่น�4 ขนาดูของยาตีามตีารางท�, 61. Unfrationated heparin ( UHF) ออกฤทธั-?ตีาน factor IIa ให IV drip นาน 24- 48
ช้�,วโมง ป่ร�บ PTT ท�,ระดู�บ 2 เท า ( ดู� normogram ในการป่ร�บ ) เหมาะส5าหร�บผู้�ป่�วยท�,ไตีไม ดู� หร�อผู้�ป่�วยท�,ม�ความจ5าเป่7นอาจตีองผู้ าตี�ดูดู วน เพราะ half life ส�4นสามารถหย.ดูยาไดูภายใน 2-3 ช้�,วโมงระดู�บ PTT ก3จะกล�บมาป่รกตี-ไดู
2. Low molecular weight heparin ใช้สะดูวกกว า heparin ใหขนาดูเพ�ยงว�นละ 2 คร�4ง
ขนาดู 0.1 mg/kg เท าน�4น ไม ม� antidote ถาม�ป่@ญหาเร�,องไตีควรลดูขนาดูลงเหล�อว�นละคร�4ง หล�กเล�,ยงในกรณ์�ท�,ม�ไตีวายอย างร.นแรง ยกเวนแตี กรณ์�ท�,ม�การเจาะระดู�บ
antiXa ไดู 3. Fondaparinux เป่7นยาตีาน Factor Xa เหม�อน LMWH แตี ออกฤทธั-?ย�บย�4ง
Pentasaccharide sequence ใช้ง ายใหว�นละคร�4งเดู�ยว ขนาดู 2.5 mg SC ใหนาน 6 ว�น ควรหล�กเล�,ยง ถาผู้�ป่�วยม�ป่@ญหาเร�,องการท5างานของไตีบกพร อง ถจ5าเป่7นตีองท5า
PCI ควรให UFH ร วมดูวย เพราะม-เช้ นน�4นจะเก-ดู intracatheter thrombus ข14น

4. Direct thrombus inhibitors เช้ น Hirudin หร�อ Bivalirudin ย�งไม ม�ท�,ใช้ในผู้�ป่�วยท�,วไป่ท�,ไม ไดูท5า PCI ย�งคงสงวนไวใช้เฉีพาะในผู้�ป่�วยท�, เป่7น Heparin induced
thrombocytopenia ( HIT ) เท าน�4น
Standardized Normogram for Titation of HeparinInitial dose 60U/kg ตีามดูวย 12 U/kg , Check aPTT ท�, 6, 12, 24 ช้�,วโมงหล�งใหและ ท�, 4-
6 ช้�,วโมงหล�งป่ร�บยา
aPTT (sec Change Intravenous infusionU/kg/hr
< 35 60U/kg bolus +335-49 30U/kg bolus +250-70 0 071-90 0 -2>100 Hold for 30 min -3
การืดั�แลรื�กษาผู้��ป่�วยในกล%�มที่�� 3 Non-diagnostic change in ST-
segment หรื)อ T wave change ว�ตีถ.ป่ระสงค�ในการร�กษาผู้�ป่�วยกล. มน�4ค�อเฝ้>าระว�งและค�ดูกรองผู้�ป่�วยท�,จะม�โอกาสเป่ล�,ยนเส�,ยงท�,จะเป่ล�,ยนเป่7นกล. ม 1 และกล. ม 2 และแยกผู้�ป่�วยท�,ม�ความเส�,ยงตี5,าออกไป่ เพ�,อใหกล�บบานไป่ไดูอย างงป่ลอดูภ�ย ผู้�ป่�วยกล. มน�4ควรไดูร�บการตี-ดูตีามอาการ ท5าคล�,นห�วใจซึ่54า และ ตีรวจเล�อดูซึ่54า ภายใน 6 ถ1ง 12 ช้�,วโมง ถาไม ม�เจ3บแน นหนาอกอ�ก ก3อาจพ-จารณ์าท5า การตีรวจเพ-,มเตี-,ม เช้ น Exercise stress test หร�อ Non- invasive stress test อ�,น ๆ เช้ น CT coronary angiography ข��นที่�� 3 การืดั�แลผู้��ป่�วย เพื่)�อให�ผู้��ป่�วยกล�บ่ไป่บ่�านอย�างป่ลอดัภั�ย และไม�กล�บ่มา เป่�น ACS
ซ้ำ*�าอ�กหล�งจากผู้�ป่�วยไดูร�บการร�กษาภาวะ ACS แลว ไม ว าจะดูวยการใช้ยา หร�อการท5า PCI ก3ตีาม
แตี น�,นเป่7นการร�กษาเฉีพาะจ.ดูท�,ตี�บตี�นเท าน�4น ย�งม�หลอดูเล�อดูบร-เวณ์อ�,น ๆใน ห�วใจ หร�อแมกระท�,งหลอดูเล�อดูท�,อ�,นท�, พรอมจะแตีกป่ระท.ออกมาและท5าใหเก-ดู ACS ไดู อ�กเสมอ เพราะฉีะน�4น การป่>องก�นจ1งส5าค�ญมาก ก อนผู้�ป่�วยกล�บบาน ยาล�มยาท�,ส5าค�ญและม�ป่ระโยช้น� ในระยะยาว อ�นไดูแก
1. ยาตีานเกร3ดูเล�อดู ไดูแก Aspirin and Clopidogrel ควรใหท.กรายโดูย aspirin ใหไป่ตีลอดูช้�ว-ตี ส วน clopidogrel ใหอย างนอยหน1,งเดู�อน หร�อ อย างนอย หน1,งป่= ถาไดูร�บการใส ขดูลวดูเคล�อบยา
2. ยาตีานเบตีา ( Beta-blocker ) จ5าเป่7นตีองใหในท.กรายท�,ไม ม�ขอหาม3. Angiotensin coverter emzym inhibitor หร�อ ยา Angiotensin receptor blockage
ควรใหในรายท�, ม�โรค เบาหวาน ความดู�นโลห-ตีส�ง และ การท5างานของห�วใจบกพร อง ( LV dysfunction)
4. Statin ควรให และป่ร�บขนาดูยาเป่7นระยะจน ไดูระดู�บ LDL นอยกว า 100 mg/dl
การป่>องการไม ใหกล�บมาเป่7น ACS ซึ่54า ( Secondary prevention ) ส-,งเหล าน�4ค�อส-,งท�,ตีองแนะน5าผู้�ป่�วยก อนกล�บบานท.กราย

1. การงดูบ.หร�, ควรจะม� โป่รแกรมส5าหร�บงดูบ.หร�,ใหผู้�ป่�วยโดูยเฉีพาะ 2. ควรค.มความดู�นใหอย� ท�,ระดู�บตี5,ากว า 140/80 หร�อ 130/80 ในผู้�ป่�วยเบาหวานท.กราย3. ในผู้�ป่�วยเบาหวานตีองควบค.มระดู�บน54าตีาล HbA1C ใหตี5,ากว า 7 %
4. ควบค.มน54าหน�ก ให Body Mass Index ( BMI ) = 18.5 – 24.9
5. ออกก5าล�งกาย แบบ แอโรบ-ค 30- 50 นาท� อย างนอย 5 คร�4งตี อส�ป่ดูาห�
Acute coronary syndrome Algorithym

Table 3. Short-Term Risk of Death or Nonfatal MI in Patients With UA/NSTEMI*
High Risk Intermediate Risk Low Risk
At least 1 of the following features must
No high-risk feature, but must have 1 of the
No high-or intermediate-risk feature but
Feature be present: following: may have any of the following features:
History Accelerating tempo of ischemic symptoms
Prior MI, peripheral or cerebrovascular disease,
in preceding 48 h or CABG; prior aspirin use
Character of pain
Prolonged ongoing (greater than 20 min)
Prolonged (greater than 20 min) rest angina,
Increased angina frequency, severity, or
rest pain now resolved, with moderate or high duration likelihood of CAD Angina provoked at a lower
threshold Rest angina (greater than 20 min) or relieved
New onset angina with onset 2 weeks to
with rest or sublingual NTG 2 months prior to presentation
Nocturnal angina
New-onset or progressive CCS class III or IV angina in the past 2 weeks without
prolonged (greater than 20 min) rest pain but with intermediate or high likelihood of CAD (see Table 6)
Clinical findings
Pulmonary edema, most likely due to Age greater than 70 years
ischemia
New or worsening MR murmur
S3 or new/worsening rales
Hypotension, bradycardia, tachycardia
Age greater than 75 years
ECG Angina at rest with transient ST-segment
T-wave changes Normal or unchanged ECG
changes greater than 0.5 mm Pathological Q waves or resting ST-depression
Bundle-branch block, new or presumed
less than 1 mm in multiple lead groups
new (anterior, inferior, lateral)
Sustained ventricular tachycardia
Cardiac markers
Elevated cardiac TnT, TnI, or CK-MB (e.g.,
Slightly elevated cardiac TnT, TnI, or CK-MB
Normal
TnT or TnI greater than 0.1 ng per ml) (e.g., TnT greater than 0.01 but less than
0.1 ng per ml)

TABLE 4. TIMI Risk Score for Patients With Unstable Angina and Non–ST-Segment Elevation MI: Predictor Variables
Predictor Variable Point Value of Variable Definition
Age 65 years 13 risk factors for CAD 1 Risk factors
• Family history of CAD• Hypertension• Hypercholesterolemia• Diabetes• Current smoker
Aspirin use in last 7 days 1Recent, severe symptoms of angina 1 2 anginal events in last 24 hoursElevated cardiac markers 1 CK-MB or cardiac-specific troponin levelST deviation 0.5 mm 1 ST depression 0.5 mm is significant; transient ST elevation >0.5
mm for <20 minutes is treated as ST-segment depression and is high risk; ST elevation 1 mm for more than 20 minutes places these patients in the STEMI treatment category
Prior coronary artery stenosis 50% 1 Risk predictor remains valid even if this information is unknown
Calculated TIMI Risk Score Risk of 1 Primary End
Point* in 14 Days Risk Status
0 or 1 5% Low2 8%3 13% Intermediate4 20%5 26% High6 or 7 41%
*Primary end points: death, new or recurrent MI, or need for urgent revascularization.
Table 5 . Properties of Beta Blockers in Clinical Use
Drugs Selectivity Partial Agonist Activity Usual Dose for Angina
Propranolol None No 20 to 80 mg twice daily
Metoprolol Beta1 No 50 to 200 mg twice daily Atenolol Beta1 No 50 to 200 mg per d Nadolol None No 40 to 80 mg per d
Timolol None No 10 mg twice daily
Acebutolol Beta1 Yes 200 to 600 mg twice daily
Betaxolol Beta1 No 10 to 20 mg per d
Bisoprolol Beta1 No 10 mg per d Esmolol (intravenous)
Beta1 No 50 to 300 mcg per kg per min
Labetalol None Yes 200 to 600 mg twice daily
Pindolol None Yes 2.5 to 7.5 mg 3 times daily
Carvedilol None Yes 6.25 mg twice daily, uptitrated to a maximum of 25 mg twice daily

ตีารางท�, 6. Dosage Table for Antiplatelet and anticoagulant in patient with UA/ NSTEMI
Drug* Initial Medical Treatment
During PCI
After PCI At Hospital Discharge
Patient Received Initial Medical Treatment
Patient Did Not Receive Initial Medical Treatment
Oral Antiplatelet Therapy
Aspirin 162 to 325 mg nonenteric formulation, orally or chewed
No additional treatment
162 to 325 mg nonenteric formulation orally or chewed
162 to 325 mg daily should be given† for at least 1 month after BMS implantation, 3 months after SES implantation, and 6 months after PES implantation, after which daily chronic aspirin should be continued indefinitely at a dose of 75 to 162 mg
162 to 325 mg daily should be given† for at least 1 month after BMS implantation, 3 months after SES implantation, and 6 months after PES implantation, after which daily chronic aspirin should be continued indefinitely at a dose of 75 to 162 mg
Clopidogrel LD of 300 to 600 mg orally MD of 75 mg
orally per day
A second LD of 300 mg orally may be given to supplement a prior LD of 300 mg
LD of 300 to 600 mg orally
For BMS: 75 mg daily for at least 1 month and ideally up to 1 year. For DES, 75 mg daily for at least 1 year (in patients who are not at high risk of bleeding) (See Fig. 11)
For BMS: 75 mg daily for at least 1 month and ideally up to 1 year. For DES, 75 mg daily for at least 1 year (in patients who are not at high risk of bleeding) (See Fig. 11)
Ticlopidine LD of 500 mg orally MD of 250 mg orally twice daily
No additional treatment
LD of 500 mg orally
MD of 250 mg orally twice daily (duration same as clopidogrel)
MD of 250 mg orally twice daily (duration same as clopidogrel)
Anticoagulants
Enoxaparin LD of 30 mg IV bolus may be given� MD � 1 mg per kg SC every 12 h_; extend dosing interval to 1 mg per kg every 24 h if estimated creatinine clearance less than 30 mL per min�
Last SC dose less than 8 h: no additional therapy Last SC dose greater than 8 h: 0.3 mg per kg IV bolus
0.5 to 0.75 mg per kg IV bolus
No additional treatment
Fondaparinux 2.5 mg SC once daily.
Avoid for creatinine 50 to 60 U per kg IV bolus of UFH is
50 to 60 U per kg IV bolus of UFH is
No additional treatment
clearance less than 30 mL per min�
recommended by the OASIS 5 Investigators¶
recommended by the OASIS 5 Investigators¶
Unfractionated heparin
LD of 60 U per kg (max 4,000 U) as IV bolus� MD of IV infusion of 12 U per kg per h (max 1,000 U per h) to maintain aPTT at 1.5 to 2.0 times control (approximately 50 to 70 s)�
IV GP IIb/IIIa planned: target ACT 200 s No IV GP IIb/IIIa planned: target ACT 250 to 300 s for HemoTec; 300 to 350 s for Hemochron
IV GP IIb/IIIa planned: 60 to 70 U per kg§ No IV GP IIb/IIIa planned: 100 to 140 U per kg
No additional treatment

Reference
1. Fuster V, Fallon JT, Badimon JJ, Nemerson Y. The unstable atheroscleroticplaque: clinical significance and therapeutic intervention. Thromb Haemost. 1997;78:247–255.2. Fuster V. Elucidation of the role of plaque instability and rupture in acute coronary events. Am J Cardiol. 1995; 76: 24C–33C3. Davies MJ. Anatomic features in victims of sudden coronary death:coronary artery pathology. Circulation. 1992;85(suppl I):I-19 –I-24.4. Burke AP, Farb A, Malcom GT, Liang Y, Smialek JE, Virmani R. Plaque rupture and sudden death related to exertion in men with coronary artery disease. JAMA. 1999;281:921–926.5. Farb A, Tang AL, Burke AP, Sessums L, Liang Y, Virmani R. Sudden coronary death: frequency of active coronary lesions, inactive coronary lesions, and myocardial infarction. Circulation. 1995;92:1701–1709.6.Freimark D, Matetzky S, Leor J, Boyko V, Barbash IM, Behar S, Hod H. Timing of aspirin administration as a determinant of survival of patients with acute myocardial infarction treated with thrombolysis. Am J Cardiol. 2002; 89: 381–3857.Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet. 1988; 2: 349–360.8.Gurfinkel EP, Manos EJ, Mejail RI, Cerda MA, Duronto EA, Garcia CN, Daroca AM, Mautner B. Low molecular weight heparin versus regular heparin or aspirin in the treatment of unstable angina and silent ischemia. J Am Coll Cardiol. 1995; 26: 313–318.[Abstract]9.Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002; 324: 71–8610. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. Lancet. 1995; 345: 669–685.11. American Heart Association . Guidelines 2005 for cardiopulmonary recuscitation ( CPR). Part 8 : Stabilzation of the patient with acute coronary syndrome. Circulation 2005;89-110.12. Antman EM, Anbe DT, Armstrong PW et at. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction— executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revisethe 1999 Guidelines for the Management of Patients With Acute MyocardialInfarction). Circulation. 2004;110:588–63613. Anderson JL, Adam CD, Antman EM et al. ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction.Circulation, Aug 2007; 116: e148 - e304.14. Meine TJ, Roe MT, Chen AY, et al. Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J2005;149:1043–9.15. Antman EM, Tanasijevic MJ, Thompson B, Schactman M, McCabe CH, Cannon CP, Fischer GA, Fung AY, Thompson C, Wybenga D, Braunwald E. Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med. 1996; 335: 1342–1349.16. Shapiro BP, Jaffe AS. Cardiac biomarkers. In: Murphy JG, Lloyd MA, editors. Mayo Clinic Cardiology: ConciseTextbook. 3rd ed. Rochester, MN: Mayo Clinic Scientific Press and New York: Informa Healthcare USA, 2007:773–8017 Sabatine MS, Morrow DA, de Lemos JA, et al. Multimarker approach to risk stratification in non-ST elevation acute coronarysyndromes: simultaneous assessment of troponin I, C-reactive protein, and B-type natriuretic peptide. Circulation 2002;105:1760 –3.18.. Morrow DA, de Lemos JA, Sabatine MS, et al. Evaluation of B-type natriuretic peptide for risk assessment in unstable angina/non-STelevation myocardial infarction: B-type natriuretic peptide and prognosis in TACTICS-TIMI 18. J Am Coll Cardiol 2003;41:1264 –72.
ม�ป่7ญหาป่รื+กษา โที่รื 02-6256500 ต�อ CCU หรื)อ fax ป่รื+กษา EKG ที่�� 02-6256686 ตลอดั 24
ช้��วโมง
Related Documents