Dr Steve Taylor, MB ChB, PhD, FRCP Consultant Physician Sexual Health HIV Medicine Lead Consultant HIV Services Birmingham Heartlands Hospital Voluntary Work: Medical Director Saving Lives Charity twitter@HIVheartlands twitter @savinglivesuk HIV UPDATE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr Steve Taylor, MB ChB, PhD, FRCPConsultant Physician Sexual Health HIV Medicine
Lead Consultant HIV Services Birmingham Heartlands Hospital
Voluntary Work: Medical Director Saving Lives Charity
twitter@HIVheartlands twitter @savinglivesuk
HIV UPDATE
Learning Objectives:1. Where is our Service?
2. How common is HIV : Nationally and Locally?
3. What is the life expectancy of people living with HIV today?
4. What is HIV Viral Load test?
5. How do you interpret CD4 Counts?
6. ARV Drug interactions: what you need to know?
7. Can ARV Treatment Prevention transmission?
8. Does PREP Pre exposure prophylaxis work?
9. How to Test for HIV?
10. When to test HIV? Ten Top Tips
11. How to refer

Learning Outcomes 1. Our Service: Heartlands HIV Service: HIVBirmingham.nhs.uk
2. Nationally 100,000 and Locally 4000 1-3/1000, 1:5 Undiagnosed, Unaware and at risk serious Morbidity & Transmission
3. Life expectancy: Normal on effective ART and early diagnosis
4. Viral Load: Infectiousness and Effectiveness of ART: AIM <50
5. CD4 Counts: Health and Risk of Infections: AIM >350
6. ART Drug interactions: Will happen- HIVdrugInteractions.org or HIV Pharmacists
7. ARV Treatment Prevents Sexual Transmission, MTCT
8. PREP Pre-exposure prophylaxis works
9. Please normalise, recommend and Test for HIV
10. When to test : ”Flu without coold” GF-Rash, Weight loss & blood tests, Hep B & C, SOB Cough &▲RR, Oral thrush & Indicator Conditions , MSM, Africans, PWIDS, Return travellers and those with STIs
11. To refer? Please just call HIV CNS’s or HAs

www.HIVBirmingham.nhs.uk

• Based within the Directorate of Infection Heartlands Hospital
• We currently look after over >1200 HIV positive patients
• Inpatient and outpatient service , 24h on ID call
• Very strong multi-disciplinary ethos
• Regional Paediatric HIV Service
• The National Military HIV Service
• Regional Infectious Diseases Service
• Immunology and Allergy
• Regional TB service
• Viral Hepatitis Service
• Have an active research portfolio
• Have a co-located Umbrella sexual health satellite clinic at Hawthorn House

SAVINGLIVESUK.COM

Encourage Self Testing !
How common is HIV : Nationally and Locally?
By the end of 2012, an estimated 98,400 people were living with HIV in the UK
21,900 are estimated to be unaware of their infection –22% of the total
6,360 new diagnoses in UK in 2012, increase on 6,220 in 2011
DID YOU KNOW?
–25% of people living with HIV in the UK do not know they have it1
1. HIV in the United Kingdom: 2011 Report. http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1317131679504. Accessed July 2012.2. HV Testing Action Plan: Second edition 2012.http://www.nat.org.uk/media/Files/Policy/2012/May-2012-Testing-Action-Plan.pdf Accessed July 2012
–25% of those unaware of their diagnosis are
responsible for 50% of new transmissions2
Presenter
Presentation Notes
Key Facts; 25% are undiagnosed. 25% of the undiagnosed are responsible for 50% of onward transmission

What is Shopshire prevelence?Diag Prev/1000 15-60 2009
Undiagnosed Prev
Undiagnosed Prevalence of other conditions
Birmingham(HOBPCT)
3.3 1.1 1 in 900 SLE in black female 1 in 5000
Coventry 2.7 0.9 1 in 1100 Inflamatory bowel disease 1 in 800
Birmingham(South)
1.9 0.63 1 in 1600 Polymyositis 1 in 25000
Sandwell PCT 1.76 0.59 1 in 1700 Homozygous for alpha one antitrypsin def 1 in 1500
Shopshire County
0.53 0.18 1 in 5550
Lambeth 13.8 4.6 1 in 220 T1 DM 1/300

Ethnic group and Sexuality determines likelihood of a positive result
• White 1 in 1000
• Black Caribbean/BB 1 in 200
• Black African 1 in 25
• Gay Men 1-10/ 1-20
• HIV prevalence by ethnic group in UK 2007 age 15-59
Presenter
Presentation Notes
White wide range : re MSM vs heterosexual white women If arrived in UK last 15y risk depends on what part of africa


13
CD4 count – useful guide
CD4 Count cells/µl
Risk of (opportunistic) infection Risk of HIV associated tumours
>500 None/minimal V small
200-500 Little risk (except TB) Bacterial pneumoniaDermatological manifestationsHerpes (zoster/simplex)Oral thrush
Small:Kaposi’s SarcomaNon Hodgkins Lymph.
<200 PCPToxoplasmosisOesophageal candidiasis
Increasing risk of a number of tumours
<50-100 Atypical mycobacterium (MAI)CMV Cryptococcal meningitis
High risk/aggressive tumours
Presenter
Presentation Notes
This slide is animated to reveal a chunk at a time – see next slide for full table

Primary HIV Infection: Common Signs & Symptoms
44
52
55
57
59
74
86
0 10 20 30 40 50 60 70 80 90 100
adenopathy
pharyngitis
headache
rash
diarrhoea
lethargy
fever
N = 160 patients with PHI inGeneva, Seattle, and Sydney
Vanhems P et al. AIDS 2000; 14:0375-0381.
% of patients
Presenter
Presentation Notes
Arthralgia and myalgia 60`%

21
40
45
10
15
24
0 20 40 60 80 100
transaminitis
leukopenia
thrombocytopenia
genital ulcers
oral ulcers
aseptic meningitis
Primary HIV Infection: Other Signs & Symptoms
Kahn JO, Walker BD. N Engl J Med. 1998;339:33-39.
% of patients
Presenter
Presentation Notes
No cough and no rhinitis

THE WINDOW PERIOD
Infected but test reads Negative
Time of Infection
The earliest timea test could read
positive
The majority oftests will be
positive
All tests will be positive
D
Infected and the test reads POSITIVE
C B
Infected but the test reads NEGATIVE
A
Window Period
Incubation Time

Cost of late HIV diagnosis
• To the individual [lifetime treatment costs between £280K and £360K]
• increased morbidity: both short and longer term prognosis –increased risk of developing opportunistic infections
• 10x increased mortality for late diagnosed (90% of deaths 2000-09)
• To the wider community• increased community viral load / unchecked risk behaviours
• increased onward transmission (over 50% new infections from undiagnosed who are 3 times more likely to transmit the virus)
• To the NHS [50% of the annual £1.8bn spend on infectious diseases / £14K per patient]
• short term treatment costs .. 2x higher treatment costs in first year
• longer term treatment costs .. 50% higher treatment costs
17


Do people with undiagnosed HIV use primary care ?
A study of newly diagnosed HIV-positive Africans found:
Over 84% were registered with a GP:• 76% had seen their GP in the year prior to diagnosis• In 17% of those, the issue of HIV or HIV testing was raised
Burns et al (2008)
Presenter
Presentation Notes
Remind people of this slide already shown earlier in the session - many people diagnosed late have had prior contact with health care workers – including GPs – and opportunities for diagnosis have been missed

What symptoms and conditions are associated with HIV infection?
Recognising HIV indicator conditions
Presenter
Presentation Notes
ANIMATED – GREY BOX AND TEXT VISIBLE AT START BLUE STATEMENTS FLY IN ONE PER CLICK ‘HIV related immunosuppression can be difficult to diagnose. Patients can present in a multitude of different ways.’ Participants are given (amongst many other things) the UK 2008 testing guidelines to take at the end.

HIV indicator conditions
Conditions where HIV testing should be offered
Dermatology Severe or recalcitrant:Seborrhoeic dermatitisPsoriasisMultidermatomal or recurrent herpes zosterHerpes simplexKaposi’s sarcomaMolluscumFolliculitis

HIV indicator conditions
Conditions where HIV testing should be offered
Gastroenterology Oral candidiasisChronic diarrhoeaWeight loss of unknown causeRecurrent / persistent aphthous ulcersKaposis sarcomaOral hairy leukoplakiaGingivitisSalmonella, Shigella or Campylobacter[Hep B infection & Hep C infection because of shared transmission risks]
Presenter
Presentation Notes
Ask group to shout out what they have put under this heading. Indicate: OIs (eg candida) HIV-associated tumour, KS, (and is that just an OI anyway due to being caused by HHV8?) HIV direct effect (diarrhoea)

HIV indicator conditions
Conditions where HIV testing should be offered
Respiratory Bacterial pneumoniaAspergillosisTBPneumocystisKS can affect the lung
24
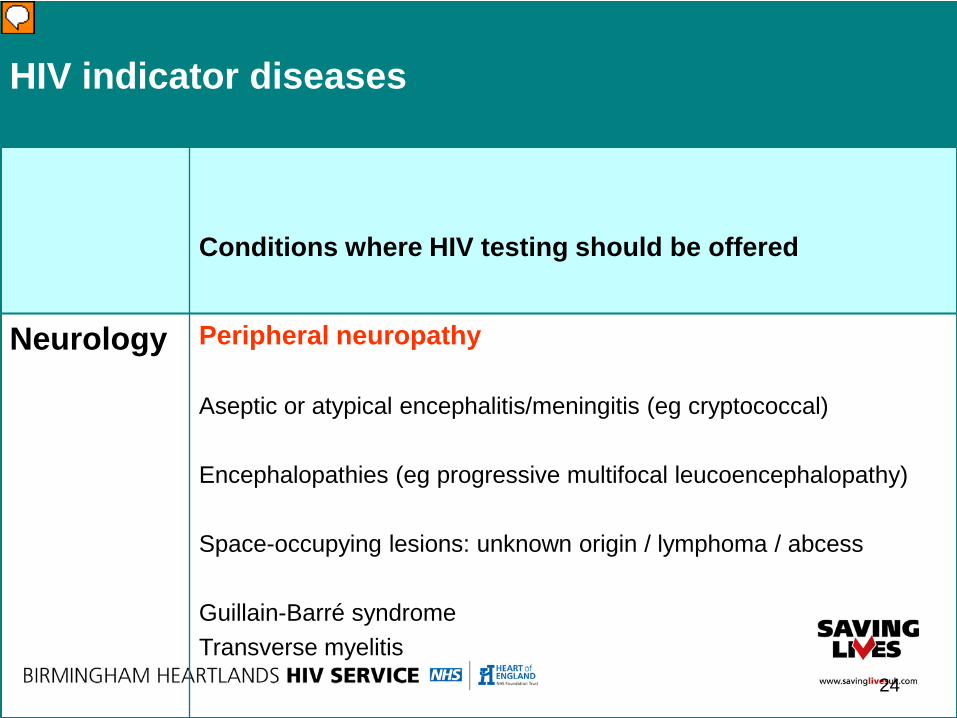
HIV indicator diseases
Conditions where HIV testing should be offered
Neurology Peripheral neuropathy
Aseptic or atypical encephalitis/meningitis (eg cryptococcal)
Encephalopathies (eg progressive multifocal leucoencephalopathy)
Space-occupying lesions: unknown origin / lymphoma / abcess
Guillain-Barré syndromeTransverse myelitis
Presenter
Presentation Notes
Just give them this one, not need to make them do it Basically – if worrying neuro picture: refer – but think HIV! ‘You might even help the hospital doctor if you think it is a possibility then mention that…’

25
HIV indicator diseases
Conditions where HIV testing should be offered
OphthalmologyInfective retinal diseases: including herpes viruses, CMV, Toxoplasma
Any unexplained retinopathy
Presenter
Presentation Notes
Just give them this too Basically – if worrying ophth picture: refer – but think HIV! ‘You might even help the hospital doctor if you think it is a possibility…’

HIV indicator diseases
Conditions where HIV testing should be offered
Gynaecology Cervical intraepithelial neoplasia grade 2 or above
Vaginal intraepithelial neoplasia
Hard to treat genital candidaHard to treat genital warts / also genital molluscum / Atypically severe herpes
ALL patients with an STI should be offered an HIV test!
Presenter
Presentation Notes
Cervical neoplasia is worth highlighting: remember practice nurses /GPs run the cervical screening programme… Ask: ‘who in your practice manages referral to colposcopy?’ Try to consider HIV when there is severe dyskariosis or worse…

27
HIV indicator diseases
Conditions where HIV testing should be offered
Haematology
Oncology
Any unexplained blood dyscrasia:Thrombocytopenia,Neutropenia,Lymphopenia, Anaemia
[And tumours below]
Anal cancer or anal intraepithelial dysplasiaLung cancerHead and neck cancerHodgkin’s lymphomaNon Hodgkins lymphomaCervical cancer – as before
Presenter
Presentation Notes
Unexplained abnormal blood count? Could it be HIV? This is important – the Tower Hamlets Nov 2012 letter found 5/25 of their avoidable late diagnosis pts had been found to have unexplained blood dyscrasis


Diagnostic catches for GPs
Many HIV-associated conditions… •are common•are considered benign•will respond, in the short term, to treatment
‘Watch and wait’ is NOTa good strategy for HIV!
Presenter
Presentation Notes
GP TEACH FROM NOW ANIMATED SLIDE – BLACK TEXT VISIBLE AT START BLUE BULLETS APPEAR ONE PER CLICK RED TEXT APPEARS ON FOURTH CLICK GP to teach from this slide for the following section HIV diagnosis is very difficult in GP context – but not impossible!

What conditions are urgent?
• PCP/ PJP (and perhaps other respiratory conditions)
• Neurological problems
• Some tumours
• CMV retinitis
Presenter
Presentation Notes
ANIMATED SLIDE – BLANK AT START BULLETS APPEAR ONE PER CLICK GP to deliver – there needs to be a clear recognition that diagnosing PCP (like PHI) is very difficult in general practice (PCP[PJP] is covered in the next slide) Strictly speaking PCP is now PJP - J for Jiroveci (Yeer-oh-vech-ee). But is still know as PCP Neurological problems and tumours are very likely to be referred, even if the GP has not diagnosed that the patient is immunosuppressed. CMV retinitis only occurs at very low CD4 counts, so the patient is highly likely to be already diagnosed (ALL visual symptoms in those known to be immunosuppressed should be taken very seriously and assessed urgently, including floaters). BUT PCP is important for general practice to be aware of as it tends to occur at higher CD4 counts . It may be the first HIV related problem for which the patient seeks help and they will go to their GP. Arguably PJP is the single most dangerous trap for the unwary GP.

Ask about weight loss; sweats; diarrhoea.
Examine mouth; skin; nodes.
Review notes for HIV related conditions in
the last 3 years. [General Practice is THE place where all these individual episodes can be put together]
Discuss with the patient ie introduce the
subject and do a risk assessment.HIV in Primary Care (Madge at al 2011)
Is my patient immunosuppressed ?
Presenter
Presentation Notes
ANIMATED SLIDE – BLANK AT START GREEN LINES APPEAR ONE PER CLICK This is one of the most important summaries in the whole session – encourage the group to memorise it for future use. Consider this for eg patients with severe dyskariosis on smear

2002 GP: Oral cold sores
2003 GP: Chest Infection “Smoker”GP: Shingles GP: Chest Infection Weight Loss ? Hospital Admission: Bacterial PneumoniaDentist: Sore Mouth Biopsy ? Thrush GP: Diarrhoea and weight Loss Referred Hospital: Ix for persistent diarrhoea, colonoscopy normal
2004 Re-referred Hospital: Anorexia, wt loss, indigestion, sore mouth Barium meal normal, coeliac ?
2005 GP: Chest infection, oral candida, molluscum face & arms, HSV, perianal warts
Margaret’s HistoryMissed Opportunities

2014 2015
Pict
ure
s sh
own w
ith p
atie
nts
per
mis
sion
to
Dr
S T
aylo
r
Pict
ure
s sh
own w
ith p
atie
nts
per
mis
sion
to
Dr
S T
aylo
r

If the clinical picture is worrying…
…you should still offer a test, even if the patient is at no apparent risk of having HIV:
‘From what you tell me you are at very low risk of having HIV.
Can I suggest that we do a test anyway - in order to rule it out?’
Presenter
Presentation Notes
ANIMATED SLIDE – BLACK TEXT VISIBLE AT START BLUE TEXT ALL APPEARS ON CLICK

Studied over 1700 couples: •One HIV pos one HIV neg (‘HIV disconcordant’)•HIV positive person also had CD4 count above threshold for treatment (above 350)
Randomised to: earlier-than-usual treatment, orno treatment
Presenter
Presentation Notes
Check animation – picture of paper appears first, text box later Paper to be discussed is one of a few landmark studies recently

39 HIV-1 transmissions occurred of which:•28 virologically linked with partner
Of the 28 linked transmissions•only 1 occurred in early treatment group
= 96% reduction!!
Those on early ART also fared better clinically:- fewer severe events, fewer deaths
Presenter
Presentation Notes
although it says a 96% reduction, the only transmission on the treatment arm was in a couple where the viral load had not yet become undetectable (at the very start of treatment) so there were actually no transmissions where the viral load was undetectable which is impressive.

PARTNER STUDY

PROUD STUDY

SAVING LIVES



THINK TALK TEST: What can you do?
–Don’t be afraid to discuss HIV with your patients
–Share your knowledge with those around you and help to dispell the myths surrounding HIV
–By helping to destigmatise the disease you can enhance the patient journey
–Speak with you local HIV specialist if you have any questions or concerns
Presenter
Presentation Notes
4 key points

North Africa and Middle EastSub-Saharan Africa
North AmericaSouth and Latin America
CaribbeanWestern and Central Europe
Eastern Europe and Central AsiaSouth and South East Asia
East Asia (eg China)Oceania
Which 3 world regions have thehighest adult prevalence of HIV?
Rank your choices in order of prevalence
Presenter
Presentation Notes
Participants have a sheet in their work book to help them mull this over: ask them to discuss in pairs. Give them just a minute to do this After discussion - invite participants to shout out their choices Feedback on following slide


7 New HIV diagnoses and number of persons accessing HIV care in the United Kingdom: 2012
Distribution of new HIV diagnoses by world region of birth: United Kingdom, 2003-2012
7,408 7,786 7,928 7,498 7,388 7,273 6,676 6,362 6,219 6,364
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Perc
enta
ge o
f HIV
dia
gnos
es
Year of first HIV diagnosis in the UK
UK Rest of Europe Africa Asia Australasia The Americas
*Excludes 13,899 cases diagnosed 2003-2012 where country of birth is not reported
Presenter
Presentation Notes
This mirrors prevalence in world regions. However where country of birth was available, over the past decade, the proportion of new HIV diagnoses among those born in the UK have increased from 27% (1,473/5,441) of all diagnoses in 2003 to 45% (2,217/4,928) in 2012. Conversely, the proportion of new diagnoses among those born in Africa declined – from 61% (3,321/5,441) of all diagnoses in 2003 to 29% (1,413/4,928) in 2012. Next few slides go no to consider patterns of HIV infection in the UK

Defined by who should have started treatment already.ie when CD4 count below 350 cells/mm3
In 2012, 47 % of new diagnoses in the UK were diagnosed late
They were ten times more likely to die within a year of diagnosis
Also •Higher risk of permanent disability•Acute serious illnesses•Slower response to treatment•Onward transmission of infection
Definition of late diagnosis
Presenter
Presentation Notes
ANIMATED SLIDE – NEW DEFINITION VISIBLE AT START (numbers below are the click number the item appears on) Don’t go too fast, let them absorb and keep up.
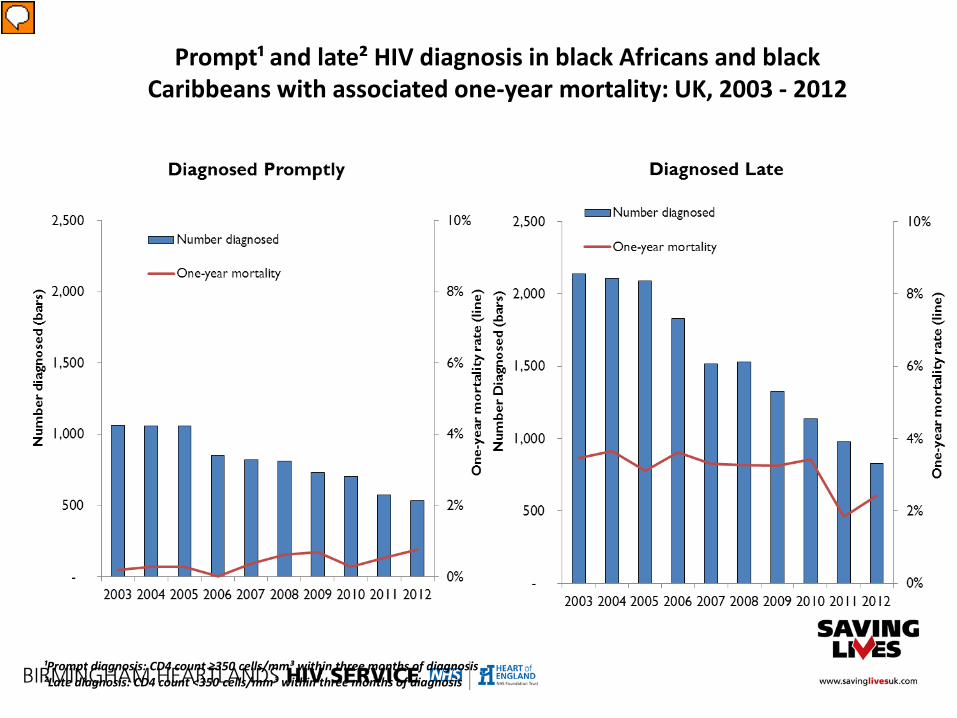
Prompt¹ and late² HIV diagnosis in black Africans and black Caribbeans with associated one-year mortality: UK, 2003 - 2012
¹Prompt diagnosis: CD4 count ≥350 cells/mm³ within three months of diagnosis²Late diagnosis: CD4 count <350 cells/mm³ within three months of diagnosis
Presenter
Presentation Notes
For Black African and Caribbean communities, HIV continues to cause serious illness and death due to late diagnosis. The proportion of Black African and Caribbean adults (aged 15 and over) diagnosed late has fallen slowly in the last 10 years from 67% in 2003 to 61% in 2012. Black African and Caribbean adults diagnosed late were three times more likely to die within a year of their HIV diagnosis than those with higher CD4 counts (2.42% compared to 0.75%).

Late diagnosis of HIV represents
a missed opportunity to protect
life and health…
..and to prevent transmission
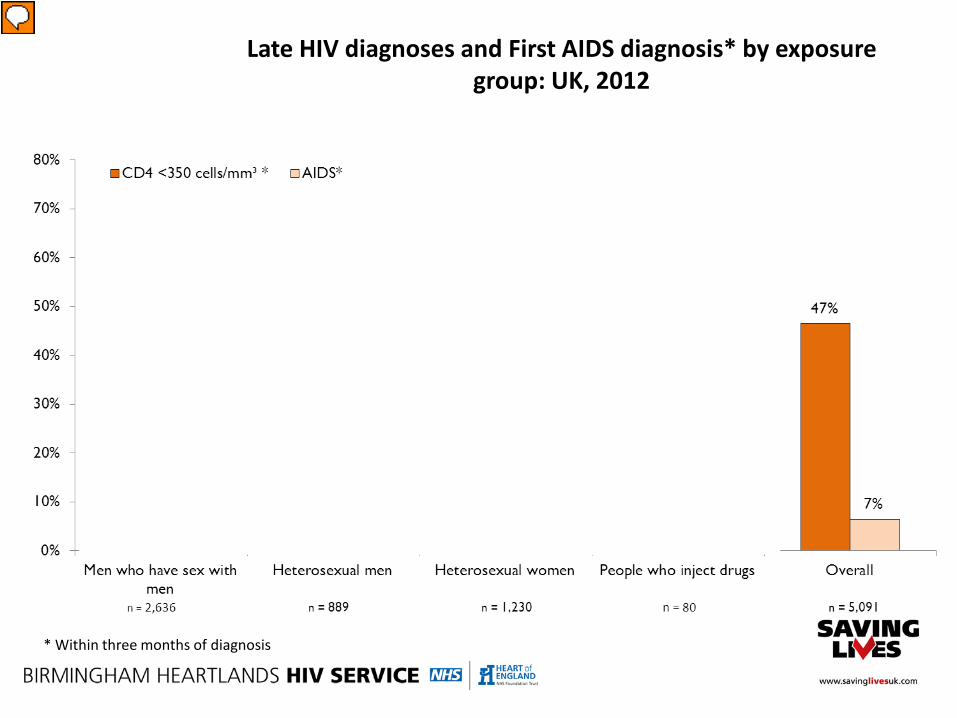
Late HIV diagnoses and First AIDS diagnosis* by exposure group: UK, 2012
* Within three months of diagnosis
Presenter
Presentation Notes
Indicate the overall figures for late diagnosis & ‘first AIDS diagnosis Ask the group to estimate which ‘exposure groups’ in the UK were MORE LIKELY to be diagnosed late, and which LESS LIKELY than the average ASK them to say why they have made their choices Next slide reveals In 2012, an estimated 47% of adults (aged 15 and over) were diagnosed late (CD4 count <350 cells within 3 months of diagnosis) and 7% had AIDS at the time of HIV diagnosis in the UK. The proportion of adults diagnosed late was lowest among MSM (34% with a low CD4 count and 4% with AIDS) and increased through heterosexual women (57% and 8%), injecting drug users (60% and 9%), and heterosexual men (65% and 11%).

Do people with undiagnosed HIV use primary care ?
A study of newly diagnosed HIV-positive Africans found:
• 50% presented with late stage disease
• 37% had a previous negative test
Over 84% were registered with a GP:• 76% had seen their GP in the year prior to diagnosis• In 17% of those, the issue of HIV or HIV testing was raised
Burns et al (2008)
Presenter
Presentation Notes
ANIMATED SLIDE – ‘A study of…’ VISIBLE AT START EACH BULLET APPEARS ON A CLICK Many people diagnosed late have had prior contact with health care workers – including GPs – and opportunities for diagnosis have been missed. Dorward 2012 letter reporting results in Tower Hamlets: NOW OMITTED BECAUSE SMALL STUDY AND PROBABLY ATYPICAL PRACTICES AND NO TIME

51
HIV is an entirely preventable andhighly treatable infection
…..but we are missing it
Presenter
Presentation Notes
AMINATED SLIDE – GREY BOX + TEXT VISIBLE AT START …but we are missing it FLIES IN FROM LEFT ON CLICK There are two strategies for ensuring the diagnosis of HIV is as early as possible: 1) Greatly increased HIV testing in asymptomatic people, especially amongst those assessed as being at highest risk. 2) Diagnosing Primary HIV Infection (PHI – HIV seroconversion illness) whenever possible . We will address testing for the asymptomatic first. Then we will consider PHI. Then we address symptomatic HIV in the more advanced stages of infection (i.e. late presentation).

SHIP’s four approachesto HIV testing
Patient requestOpportunistic testing
of those at risk
Diagnostic testing of those with symptoms
The UK national guidelines for testing advocate the offer and recommendation to accept an HIV test to all adults registering in general practice and general medical admissions patients in areas where diagnosed HIV prevalence is greater than 2 per 1,000 population.
Prevalence of diagnosed HIV infection, UK: 2009
HIV screening
Presenter
Presentation Notes
Ask participants Thinking about these different types of HIV testing identify barriers for clinicians Barriers (this list is too large for notes pages – there should be a separate crib sheet for facilitators) A lack of time – there are not many potentially life-saving interventions that a doctor omits due to lack of time. Sometimes, people blame lack of time when on reflection other issues are playing a part …… Lack of clinical knowledge – doctors who are unaware of the clinical manifestations of HIV infection – and doctors and nurses who are not aware of or do not respond to risk assessment- will not offer enough HIV tests Embarrassment – doctors and nurses who do not feel able to take sexual histories – or raise the subject of HIV – due to embarrassment will take fewer HIV tests. Fear of giving a positive result – if a result is positive the lab will call and you will have thinking time . First positive results will always be reported as provisional , as a confirmatory test will be needed. If you are not confident to discuss the test result with the patient you can arrange for confirmatory testing to be conducted at a sexual health clinic. But if your patient wanted you to do the test – does that mean they want you to give the result? Concern about lack of expertise or skills to take test- taking and discussing an HIV tests is simple and falls well within the existing skills of doctors and nurses. There is a prevailing view that old fashioned notions of complex counselling may still be acting as a barrier to testing . How to conduct a test will be discussed later … A sense that testing is not appropriate for the GP setting – general practice is in fact at the front line if we are to reduce the rates of undiagnosed HIV in the UK. Concerns about confidentiality – practices should already have procedures to protect confidentiality that are adequate for all patients including those with stigmatised problems. A sense that there is not much HIV around – HIV can be found throughout the UK.GPs can make wrong assumptions about how much HIV is in their area. Concern about insurance issues- insurance companies are now required not to ask about negative HIV tests. HIV, like any chronic illness, may affect insurance but mortgages etc can still be obtained. Not realising how much HIV there is Don’t know how to assess risk (not if SHIP trained!) ‘Patients don’t ask, I think they go elsewhere’ ….not appropriate to wait for ptnts to ask.. “I might know when to test – but I don’t think some of my colleagues do” Don’t know how to manage HIV Wouldn’t know what to tell the family members Patient already had a negative test Patient barriers: ?not confidential; ?insurance a worry; don’t want them to know I am gay; that receptionist is from my community; I am not at risk

• Patient Request • Clinic posters
• Opportunistic Screening• STIs /terminations/ contraception• Travel • Hepatitis B & C• PWIDS• MSM / African/ Caribean
• Diagnostic testing of those with indicator conditions• See Saving Lives Flyer
• Screening when prevalence > 2/1000• All new GP registrants • All AMU / A and E admissions having bloods

First line therapy 1996 First line therapy 2012
Ritonavir (PI) x 6d4T x 2, 3TC x 2 (NRTIs)
TWICE A DAY
Efavirenz (NNRTI) + Truvada(= FTC + Tenofivir, NRTIs)
ONCE A DAY
Evolution of HIV Therapy
Presenter
Presentation Notes
1996 – this is one typical combo – other PI combos had similar pill burdens 2012- first line

A fantastic resource……
Presenter
Presentation Notes
Tell them about this website – explain it is easy to use and suggest they play with it…

• Proton Pump Inhibitors• Fluticasone• Some anticonvulsants• Statins• Clarithromycin, erythromycin• Benzodiazepines
• Contraception: UK Medical Eligibility Criteria 2009, Drug Interactions with Hormonal Contraception FSRHC Jan 2011 http://www.ffprhc.org.uk/
Key prescribing issues
Presenter
Presentation Notes
WHIZZ through NOT comprehensive Fluticasone can lead to Cushings with atazanavir due to high blood levels- important because fluc is not ‘intuitively’ an interactor for GPs This is just a headsup – if they use the liverpool website and communicate with the HIV clinics (and vice versa!) then they will be fine.

Also
•Herbal remedies
•Recreational drugs
•More information available from:
www.hiv-druginteractions.org
Interactions

Related Documents











