Hirschsprung’s disease associated with Mowat-Wilson syndrome Ramnik V Patel, 1,2 Khalid Elmalik, 3 Nordine Bouhadiba, 3 Rang Shawis 3 1 Department of Paediatric Urology, University College London Hospitals NHS Foundation Trust, London, UK 2 Department of Paediatric Urology, Great Ormond Street Children Hospital NHS Trust, London, UK 3 Department of Paediatric Surgery, Sheffiled Children’s Hospital, Sheffiled, UK Correspondence to Ramnik V Patel, [email protected] Accepted 21 April 2014 To cite: Patel RV, Elmalik K, Bouhadiba N, et al. BMJ Case Rep Published online: [ please include Day Month Year] doi:10.1136/bcr-2013- 203262 DESCRIPTION A term male infant was born after an uneventful pregnancy and normal vaginal delivery with a birth weight of 3480 g. There was no consanguinity among parents. He required no resuscitation at birth. He had typical dysmorphic facial features such as square-shaped face, a prominent but narrow triangular chin, deep set but large eyes, hypertelor- ism, saddle nose, broad nasal bridge, open mouth, everted lower lip, posteriorly rotated ears and large uplifted ear lobes with a central depression. Recognition of the characteristic facies led to refer- ral for genetic counselling. He had delayed passage of meconium with abdominal distention and bilious vomiting on second day of life. He responded well to saline rectal washouts and rectal suction biopsy confirmed Hirschsprung’s disease ( figure 1). He was sent home with daily saline rectal washouts by parents until 3 months of age at which time he underwent primary Duhamel pull through oper- ation using small hockey stick smiling left lower abdominal incision. His postoperative period was uneventful. Genetic team on investigation found it to be sporadic resulting from de novo deletion of the ZFHX1B gene with cytogenetic deletion of 2q22-23. There was no indication of any deletion in the parental chromosomes on this identical location and therefore it was concluded that it was a de novo mutation rather than inherited pattern of the men- delian type. In addition he has glandular hypospa- dias, absent corpus callosum, abnormal EEG, moderate mental retardation and microcephaly. At 10-year follow-up he is progressing well, has normal bowel function and shows typical facial changes. Mowat-Wilson syndrome with Hirschsprung’s disease is a complex syndromic genetic disease with multiple congenital anomalies and typical dys- morphic features with mental retardation. 1 2 Generally, the outcome of syndromic Hirschsprung’s disease in such cases is very poor. 3 Our case is exceptional and a strong reminder of the fact that we should at least give definitive surgery a chance to see how they do, and meticulously per- formed surgery does help. Figure 1 (A–C) Histology: (A) normal control rectal biopsy showing several clusters of ganglion cells in the submucosa (arrows); (B) Patient’s rectal biopsy showing no ganglion cells in the submucosa; (C) several large nerve trunks seen in the submucosa (arrows). (D and E) Acetyl cholinesterase histochemistry: (D) normal control Ache stain. There is only a light brown blush in the muscularis mucosa. There are no large nerves (these would stain black); (E) Ache stain showing the large nerves in (C) (arrows). (F) Ache stain showing abnormal nerves in the muscularis mucosa and lamina propria (arrows). Patel RV, et al. BMJ Case Rep 2014. doi:10.1136/bcr-2013-203262 1 Images in … on 19 February 2020 by guest. Protected by copyright. http://casereports.bmj.com/ BMJ Case Reports: first published as 10.1136/bcr-2013-203262 on 14 May 2014. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hirschsprung’s disease associated withMowat-Wilson syndromeRamnik V Patel,1,2 Khalid Elmalik,3 Nordine Bouhadiba,3 Rang Shawis3
1Department of PaediatricUrology, University CollegeLondon Hospitals NHSFoundation Trust, London, UK2Department of PaediatricUrology, Great Ormond StreetChildren Hospital NHS Trust,London, UK3Department of PaediatricSurgery, Sheffiled Children’sHospital, Sheffiled, UK
Correspondence toRamnik V Patel,[email protected]
Accepted 21 April 2014
To cite: Patel RV, Elmalik K,Bouhadiba N, et al. BMJCase Rep Published online:[please include Day MonthYear] doi:10.1136/bcr-2013-203262
DESCRIPTIONA term male infant was born after an uneventfulpregnancy and normal vaginal delivery with a birthweight of 3480 g. There was no consanguinityamong parents. He required no resuscitation atbirth. He had typical dysmorphic facial featuressuch as square-shaped face, a prominent but narrowtriangular chin, deep set but large eyes, hypertelor-ism, saddle nose, broad nasal bridge, open mouth,everted lower lip, posteriorly rotated ears and largeuplifted ear lobes with a central depression.Recognition of the characteristic facies led to refer-ral for genetic counselling. He had delayed passageof meconium with abdominal distention and biliousvomiting on second day of life. He responded wellto saline rectal washouts and rectal suction biopsyconfirmed Hirschsprung’s disease (figure 1). He wassent home with daily saline rectal washouts byparents until 3 months of age at which time heunderwent primary Duhamel pull through oper-ation using small hockey stick smiling left lowerabdominal incision. His postoperative period was
uneventful. Genetic team on investigation found itto be sporadic resulting from de novo deletion ofthe ZFHX1B gene with cytogenetic deletion of2q22-23. There was no indication of any deletion inthe parental chromosomes on this identical locationand therefore it was concluded that it was a de novomutation rather than inherited pattern of the men-delian type. In addition he has glandular hypospa-dias, absent corpus callosum, abnormal EEG,moderate mental retardation and microcephaly. At10-year follow-up he is progressing well, has normalbowel function and shows typical facial changes.Mowat-Wilson syndrome with Hirschsprung’sdisease is a complex syndromic genetic disease withmultiple congenital anomalies and typical dys-morphic features with mental retardation.1 2
Generally, the outcome of syndromicHirschsprung’s disease in such cases is very poor.3
Our case is exceptional and a strong reminder of thefact that we should at least give definitive surgery achance to see how they do, and meticulously per-formed surgery does help.
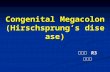
Figure 1 (A–C) Histology: (A) normal control rectal biopsy showing several clusters of ganglion cells in thesubmucosa (arrows); (B) Patient’s rectal biopsy showing no ganglion cells in the submucosa; (C) several large nervetrunks seen in the submucosa (arrows). (D and E) Acetyl cholinesterase histochemistry: (D) normal control Ache stain.There is only a light brown blush in the muscularis mucosa. There are no large nerves (these would stain black); (E)Ache stain showing the large nerves in (C) (arrows). (F) Ache stain showing abnormal nerves in the muscularis mucosaand lamina propria (arrows).
Patel RV, et al. BMJ Case Rep 2014. doi:10.1136/bcr-2013-203262 1
Images in…
on 19 February 2020 by guest. P
rotected by copyright.http://casereports.bm
j.com/
BM
J Case R
eports: first published as 10.1136/bcr-2013-203262 on 14 May 2014. D
ownloaded from

Learning points
▸ Characteristic dysmorphic features in association withHirschsprung’s disease and multiple congenital anomaliesand mental retardation should alert the possibility ofMowat-Wilson syndrome.
▸ Genetic counselling should be conducted and otherconditions should be excluded. Normal parental genes andchromosomes may suggest a de novo mutation in theoffspring.
▸ Generally speaking the outcome of pull-through operationfor Hirschsprung’s disease is very poor and our case is anexception to this rule perhaps due to de novo mutation andmeticulously performed single stage neonatal primarypull-through surgery.
Contributors All the authors have made substantial contributions to theconception and design of this paper, search of literature, the acquisition, analysisand interpretation of the data, to drafting the article or revising it critically forimportant intellectual content and to the final approval of the version to bepublished.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Leong M, Verey F, Newbury-Ecob R, et al. Supernumerary intestinal muscle coat in a
patient with Hirschsprung’s disease/Mowat-Wilson syndrome. Pediatr Dev Pathol2010;13:415–18.
2 Cuturilo G, Stefanović I, Jovanović I, et al. Mowat-Wilson syndrome—a case report.Srp Arh Celok Lek 2009;137:426–9.
3 Bonnard A, Zeidan S, Degas V, et al. Outcomes of Hirschsprung’s disease associatedwith Mowat-Wilson syndrome. J Pediatr Surg 2009;44:587–91.
Copyright 2014 BMJ Publishing Group. All rights reserved. For permission to reuse any of this content visithttp://group.bmj.com/group/rights-licensing/permissions.BMJ Case Report Fellows may re-use this article for personal use and teaching without any further permission.
Become a Fellow of BMJ Case Reports today and you can:▸ Submit as many cases as you like▸ Enjoy fast sympathetic peer review and rapid publication of accepted articles▸ Access all the published articles▸ Re-use any of the published material for personal use and teaching without further permission
For information on Institutional Fellowships contact [email protected]
Visit casereports.bmj.com for more articles like this and to become a Fellow
2 Patel RV, et al. BMJ Case Rep 2014. doi:10.1136/bcr-2013-203262
Images in…
on 19 February 2020 by guest. P
rotected by copyright.http://casereports.bm
j.com/
BM
J Case R
eports: first published as 10.1136/bcr-2013-203262 on 14 May 2014. D
ownloaded from
Related Documents