Hypertension Heart Disease

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hypertension Heart Disease
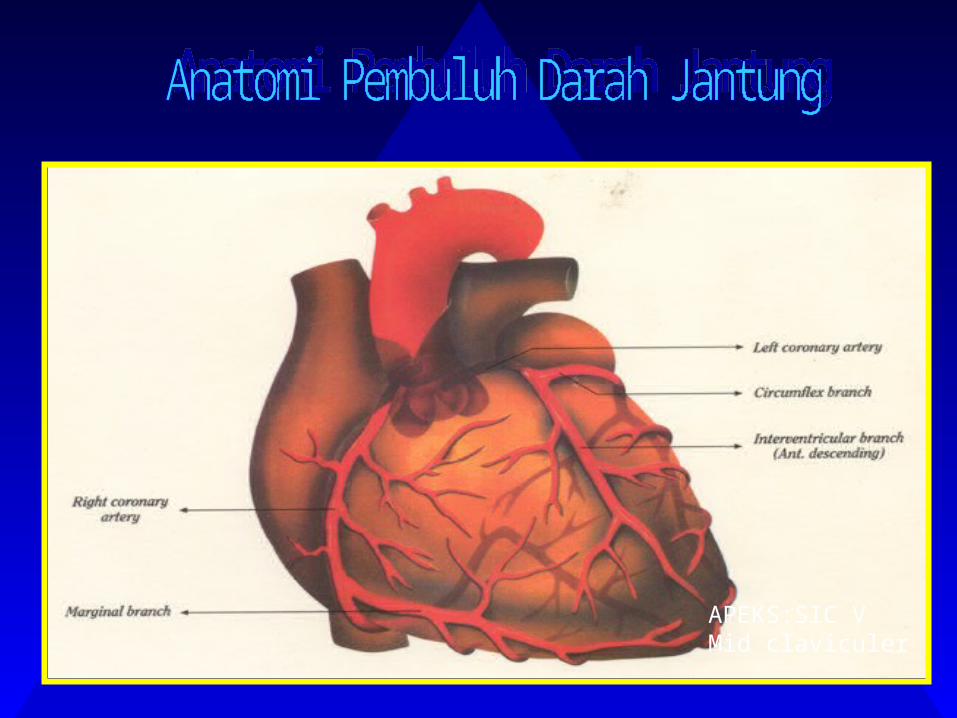
APEKS:SIC VMid claviculer
The World Health Organization (WHO)
estimates that 20% of the world’s
current adult population has
hypertension
Prevalence of hypertension

Awareness, Treatment and Control of High Blood Pressure in Canada
Patients unaware of their high blood pressurePatients unaware of their high blood pressure 43%43%Aware but not treated and not controlledAware but not treated and not controlled 22%22%Treated but not controlledTreated but not controlled 21%21%Treated and controlledTreated and controlled 13%13%
Joffres et al. Am J Hypertens 2001; 14(11):1099-1105Joffres et al. Am J Hypertens 2001; 14(11):1099-1105
4433%%
2222%%2211%%
1133%%
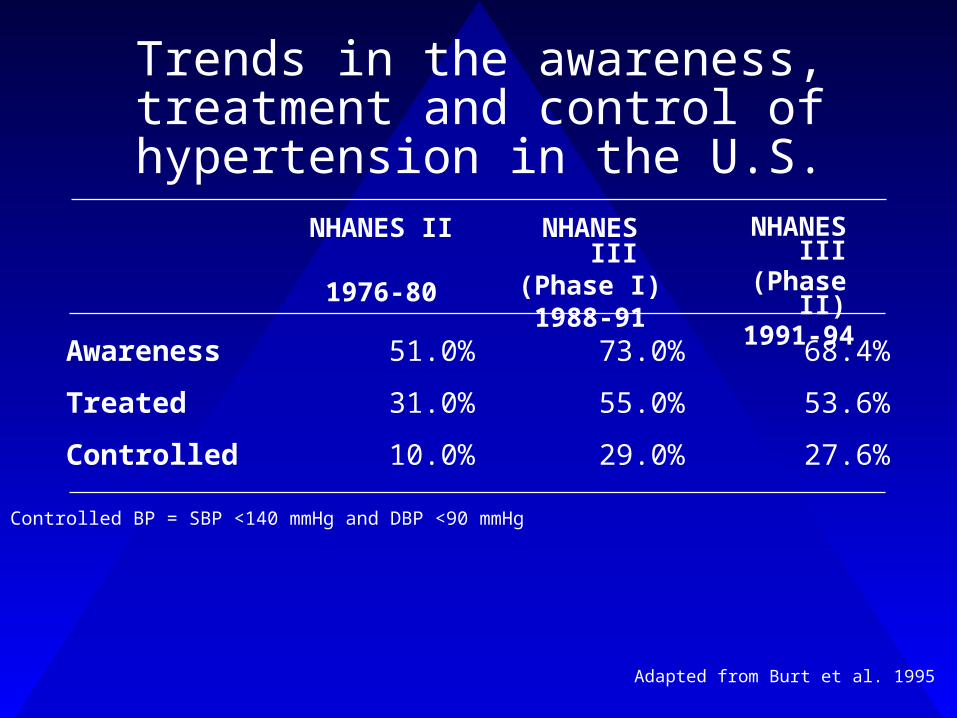
Trends in the awareness, treatment and control of hypertension in the
U.S.
Awareness 51.0% 73.0% 68.4%
Treated 31.0% 55.0% 53.6%
Controlled 10.0% 29.0% 27.6%
NHANES II
1976-80
NHANES III
(Phase I)1988-91
NHANES III
(Phase II)1991-94
Controlled BP = SBP <140 mmHg and DBP <90 mmHg
Adapted from Burt et al. 1995

Causes of Resistant Hypertension
Efficacy of medications
Patient compliance:– Side effects– Convenience– Lack of symptoms– Patient education– Cost
Failure to treat to target– MD Reluctance– Accurate blood pressure
measurements
Secondary Causes– Sleep apnea– Renal vascular HTN– Endocrine causes– Chronic renal failure– Rx Drugs (NSAIDS, steroids)– White-coat HTN– Pseudo-hypertension– Vasoactive substances
(non-Rx)
Relctnce: enggan Rstant : mlawan

Diseases Attributable to Hypertension
Hypertension
Heart failureHeart failureStrokeStroke
Coronary heart diseaseCoronary heart disease
Myocardial infarctionMyocardial infarction
Left ventricular Left ventricular hypertrophyhypertrophy
Aortic aneurysmAortic aneurysmRetinopathyRetinopathy
Peripheral vascular diseasePeripheral vascular disease
Hypertensive Hypertensive encephalopathyencephalopathy
Chronic kidney failureChronic kidney failure
Cerebral hemorrhageCerebral hemorrhage
AllVascular
Adapted from: Dustan et al. Arch Intern Med 1996; 156:1926-1935Adapted from: Dustan et al. Arch Intern Med 1996; 156:1926-1935
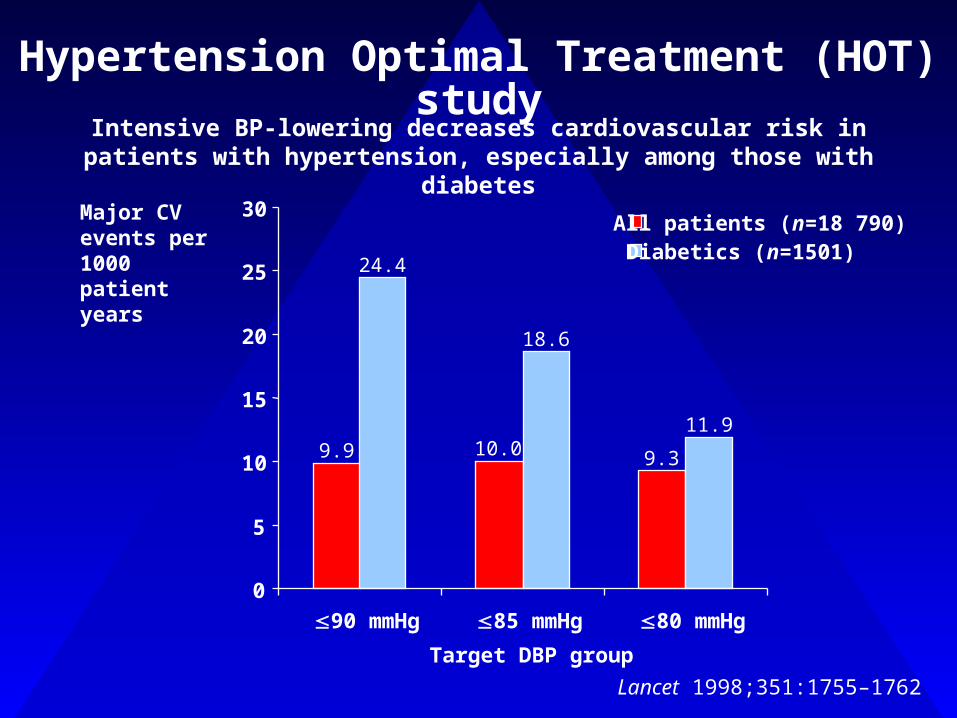
Hypertension Optimal Treatment (HOT) study
9.9 10.0 9.3
24.4
18.6
11.9
0
5
10
15
20
25
30
90 mmHg 85 mmHg 80 mmHgTarget DBP group
Major CV events per 1000 patient years
All patients (n=18 790)Diabetics (n=1501)
Lancet 1998;351:1755–1762
Intensive BP-lowering decreases cardiovascular risk in patients with hypertension, especially among those with diabetes

UKPDS: relative risk reduction with tight versus less tight blood pressure control
Any diabetes-related endpoint
Diabetes-related deaths
Stroke Microvascular disease
–24% P<0.005
–32% P<0.05
–44% P<0.05
–37% P<0.01
Tight control (n=758)Less tight control (n=390)
Deterioration in visual acuity
–47% P<0.005
BMJ 1998;317:703–713
Tight BP control decreases morbidity and mortality in patients with diabetes

BP targets
BP targets in guidelines are becoming more stringent
Coexistent cardiovascular risk factor profile is important
The relationship between BP and mortality is not dictated by a J-shaped curve
Strngt : ktat,kras
Initial Assessment
Target organ damage
Overall cardiovascular risk
Rule out secondary and often curable causes

Target end-organs should be assessed Target end-organs should be assessed by history and physical examinationby history and physical examination
Components of Risk StratificationTarget Organ Damage/Clinical Cardiovascular Disease
BrainBrain
HeartHeartKidneysKidneys
EyesEyes
ArteriesArteries
Adapted from: JNC VI. Arch Intern Med 1997;157: 2413-46Adapted from: JNC VI. Arch Intern Med 1997;157: 2413-46

Components of Risk StratificationMajor Cardiovascular Risk Factors
HypertensionAge
SmokingDyslipidemiaDiabetesFamily history
Obesity
> 45 years Male> 45 years Male> 55 years Female (Postmenopausal) > 55 years Female (Postmenopausal)
CAD <65 FemaleCAD <65 FemaleCAD <55 MaleCAD <55 Male
Adapted from: JNC VI. Arch Intern Med 1997;157: 2413-46Adapted from: JNC VI. Arch Intern Med 1997;157: 2413-46

1414
Stratification of risk to quantity Stratification of risk to quantity prognosisprognosis
Other risk factor and Other risk factor and disease historydisease history
Normal Normal SBP 120-SBP 120-129129DBP 80-84DBP 80-84
High High normalnormalSBP 130-SBP 130-139139DBP 85-89DBP 85-89
Grade 1Grade 1SBP140-SBP140-159159DBP 90-DBP 90-9999
Grade 2Grade 2SBP 160-SBP 160-179179DBP 100-DBP 100-109109
Grade 3Grade 3SBP SBP >> 180180DBP DBP > > 110110
No other risk factorsNo other risk factors Average Average riskrisk
Average Average riskrisk
Low Low added added risk risk
Moderate Moderate added riskadded risk
High High added added riskrisk
1 – 2 risk factors1 – 2 risk factors Low added Low added riskrisk
Low added Low added riskrisk
Moderate Moderate added added riskrisk
Moderate Moderate added riskadded risk
Very Very high high added added riskrisk
3 or more risk factors 3 or more risk factors or TOD or DMor TOD or DM
Moderate Moderate added riskadded risk
High High added riskadded risk
High High added added riskrisk
High High added riskadded risk
Very Very high high added added riskrisk
ACCACC High High added riskadded risk
Very high Very high added risk added risk
Very high Very high added added riskrisk
Very high Very high added rsikadded rsik
Very Very added added riskrisk
Blood pressure (mm Hg)
2003 ESH-ESC

Effectively reduces BP Maintains BP control over 24 h with
once-a-day dosing Effective in all hypertensive patients No adverse effects No negative metabolic side effects Affordable
The ideal antihypertensive agent

• Persistent use of monotherapy
• Obsession with “first line therapy”
• Poor recognition of the importance and efficacy of combination therapy
• Lack of advice on most appropriate drugs to use in combination
BP monotherapy: BP fall <10%Statin therapy: Cholesterol fall 30-40%
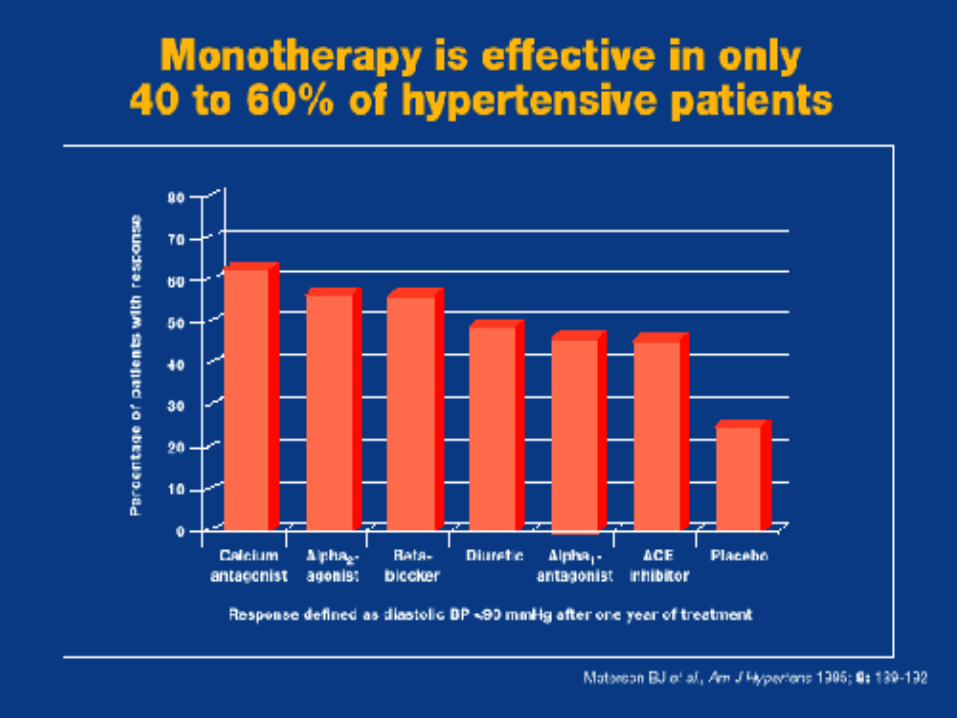

Clinical Practice:Most people with hypertension are treated with monotherapy
Clinical Evidence:Most people in clinical trials are treated with combination therapy
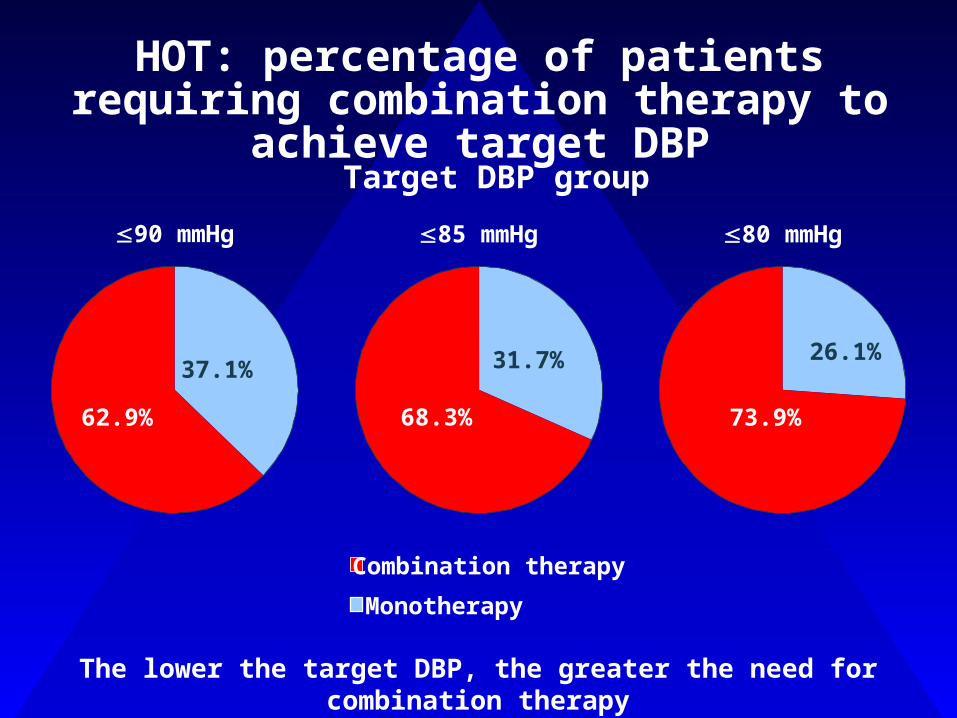
HOT: percentage of patients requiring combination therapy to achieve target DBP
90 mmHg
37.1%
62.9%
85 mmHg
31.7%
68.3%
80 mmHg
26.1%
73.9%
Combination therapyMonotherapy
Target DBP group
The lower the target DBP, the greater the need for combination therapyHOT:Hypertesion Optimal Treatment


Advantages of combination therapy
Additive antihypertensive efficacy (due to complementary mechanisms of action)
Higher patient response rates Simple titration and dosing schedules Maintained or improved tolerability Improved patient compliance Cost effective
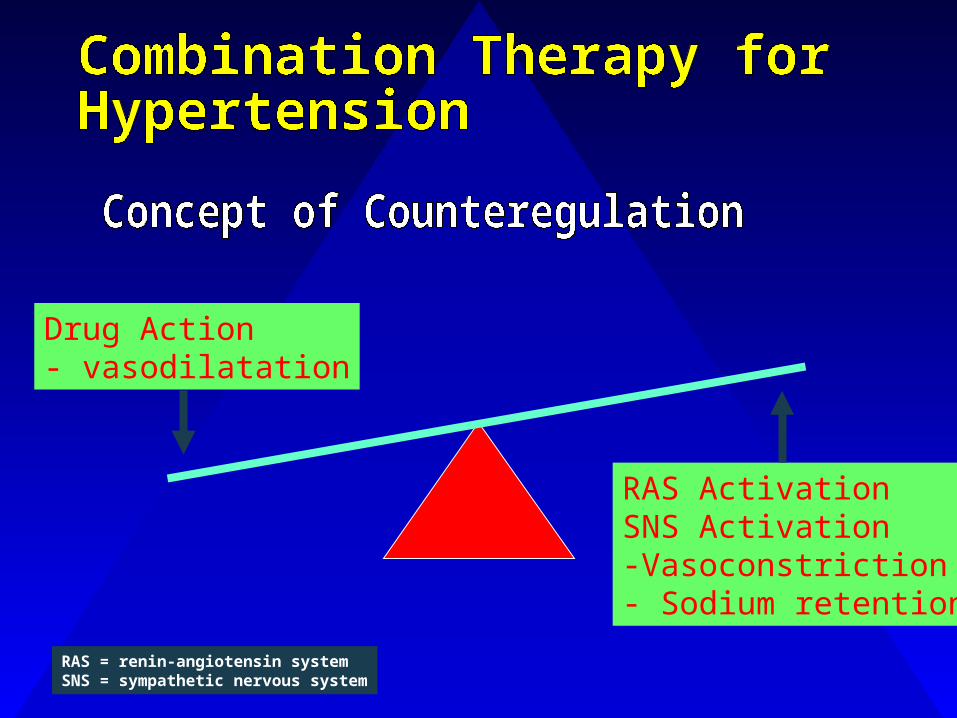
Drug Action- vasodilatation
RAS ActivationSNS Activation-Vasoconstriction- Sodium retention
RAS = renin-angiotensin systemSNS = sympathetic nervous system

24
Thiazide
Lowers BloodPressure
NatriureticActivates
Renin AngiotensinSystem
Reduces antihypertensive effect
25
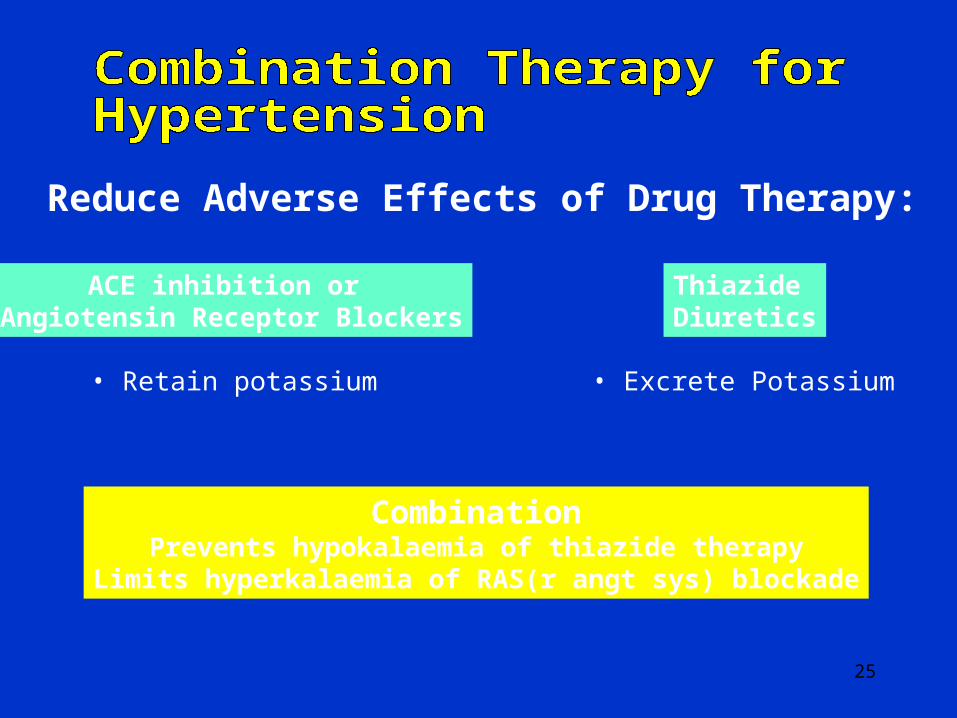
Reduce Adverse Effects of Drug Therapy:
ACE inhibition or Angiotensin Receptor Blockers
• Retain potassium
Thiazide Diuretics
• Excrete Potassium
CombinationPrevents hypokalaemia of thiazide therapy
Limits hyperkalaemia of RAS(r angt sys) blockade

26

27
28

29
WHAT IS THE IDEAL WAY OF CONTROLLING BP?
The new therapeutic window in hypertension
100
80
60
40
20
0
100
80
60
40
20
0
Efficacy (%)
Freedom from side effects (%)
Dose
Man In’t Veld AJ. J Hypert, 1997
IDEAL treatment
Traditional
30
31

32 ACE-I = angiotensin-converting enzyme inhibitor; ARB = angiotensin-receptor blocker; BB = beta blocker; CCB, = calcium channel blocker.Chobanian AV et al. Chobanian AV et al. JAMA. JAMA. 2003;289:2560-2572.2003;289:2560-2572.
Drug(s) for the compelling indications; other antihypertensive drugs (diuretics, ACE-I, ARB, BB, CCB) as needed
Drug(s) for the compelling indications; other antihypertensive drugs (diuretics, ACE-I, ARB, BB, CCB) as needed
BP ClassificationLifestyle Modification
Initial Drug TherapyWithout Compelling
IndicationWith Compelling
Indication
Normal<120/80 mm Hg
Prehypertension120-139/80-89 mm Hg
Stage 1 hypertension140-159/90-99 mm Hg
Stage 2 hypertension160/100 mm Hg
Encourage
Yes
Yes
Yes
No drug indicated Drug(s) for the compelling indications
Thiazide-type diuretics for most; may consider ACE-I, ARB, BB, CCB, or combination
2-drug combination for most (usually thiazide-type diuretic and ACE-I, ARB, BB, or CCB)

33
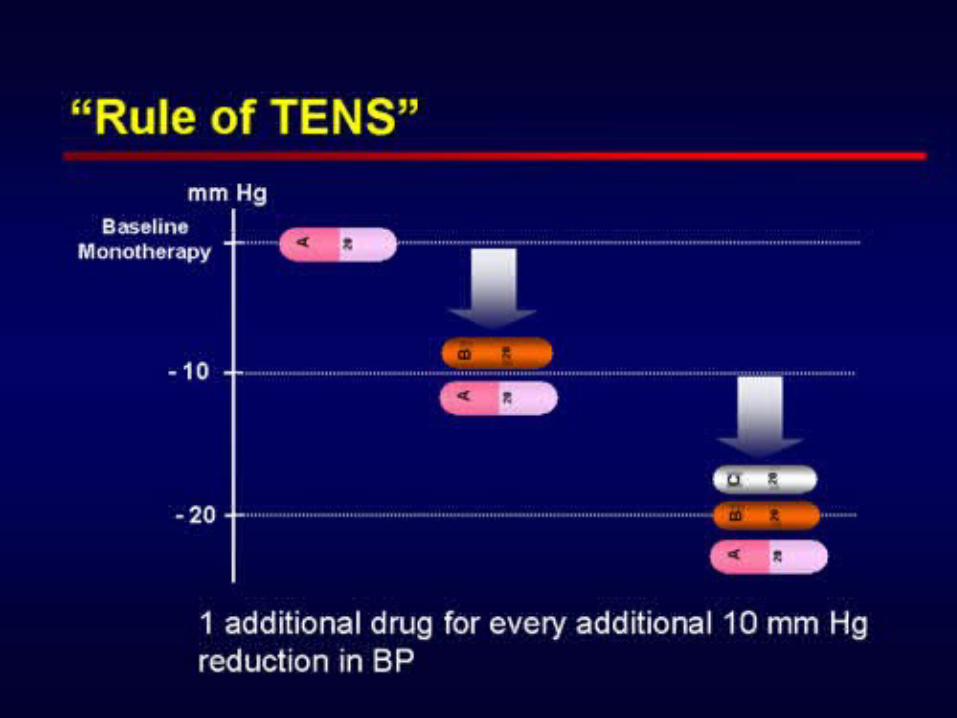
• BP target of <140/90 mm Hg for patients with uncomplicated hypertension without compelling indications
• BP target of <130/80 mm Hg for patients with diabetes
– Combinations of 2 or more drugs are usually needed to achieve target BP goal
• BP target of <130/80 mm Hg for patients with chronic renal disease*
– Combinations of 3 or more drugs are often needed to reach target BP goal
*Chronic kidney disease = GFR <60 mL/min per 1.73 m2 or presence of albuminuria (>300 mg/d or 200 mg/g creatinine).Chobanian AV et al. JAMA. 2003;289:2560-2572.American Diabetes Association. Diabetes Care. 2003;26(Suppl 1):S33-S50.Guidelines Committee. J Hypertens. 2003;21:1011-1053.
34
• Most patients with hypertension will require 2 or more antihypertensive drugs to achieve BP goals
• According to baseline BP and presence or absence of complications, therapy can be initiated either with a low dose of a single agent or with a low-dose combination of 2 agents
• When BP is >20/10 mm Hg above goal, consideration should be given to initiating 2 drugs, either as separate prescriptions or in fixed-dose combinations, one of which should be a thiazide-type diuretic
Chobanian AV et al. JAMA. 2003;289:2560-2572.Guidelines Committee. J Hypertens. 2003;21:1011-1053.

35
Easy as ABCDA = ACE-Inhibitor or Angiotensin Receptor Blocker
B = - Blocker
C = Calcium Channel Blocker
D = Diuretic (thiazide)
Adapted from : ‘Better blood pressure control: how to combine drugs’Journal of Human Hypertension (2003) 17, 81-86 www.bhsoc.org
36
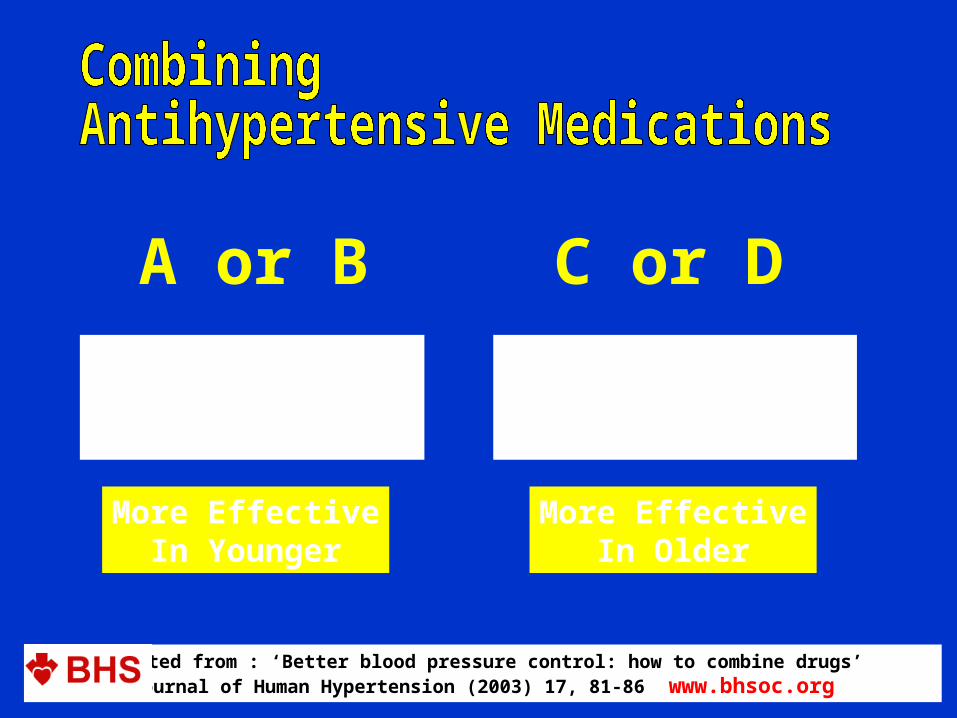
A or BInhibit the
Renin-AngiotensinSystem
C or DDo not inhibit the
Renin-AngiotensinSystem
More EffectiveIn Younger
More EffectiveIn Older
Adapted from : ‘Better blood pressure control: how to combine drugs’Journal of Human Hypertension (2003) 17, 81-86 www.bhsoc.org

YoungerOr Diabetes
( 55yrs)
Older (55yrs)or Black
A or B C or D1.
A or (B) + C or D2.
A or (B) + C + D3.
A or (B) + C + D + other4.Adapted from : ‘Better blood pressure control: how to combine drugs’
Journal of Human Hypertension (2003) 17, 81-86 www.bhsoc.org

38

39
Recommended Combinations
1. ACE inhibitors / AIIRA Diuretics2. ACE inhibitors / AIIRA Calcium antagonists3. ACE inhibitors / AIIRA Beta-blockers
(Special condition)4. Beta-Blockers Diuretics5. Beta-Blockers Calcium Antagonists

SUMMARY
COMBINATION THERAPY IN HTN MANAGEMENT IS LOGIC AND EVIDENCE BASED
MAXIMIZE EFFECT, MINIMIZE SIDE EFFECT
COMBINATION THERAPY IN HTN INCREASE COMPLIANCE
THE END

Related Documents











