High Frequency Nasal Ventilation for 21 Days Maintains Gas Exchange with Lower Respiratory Pressures and Promotes Alveolarization in Preterm Lambs Donald M. Null 1 , Jeremy Alvord 1 , Wendy Leavitt 1 , Albert Wint 1 , Mar Janna Dahl 1 , Angela P. Presson 2 , Robert H. Lane 1 , Robert J. DiGeronimo 1 , Bradley A. Yoder 1 , and Kurt H. Albertine 1 1 Division of Neonatology, Department of Pediatrics, University of Utah, Salt Lake City, UT, USA 2 Division of Epidemiology, University of Utah, Salt Lake City, UT, USA Abstract Background—Short-term high-frequency nasal ventilation (HFNV) of preterm neonates provides acceptable gas exchange compared to endotracheal intubation and intermittent mandatory ventilation (IMV). Whether long-term HFNV will provide acceptable gas exchange is unknown. We hypothesized that HFNV for up to 21d would lead to acceptable gas exchange at lower inspired oxygen (O 2 ) levels and airway pressures compared to intubation and IMV. Methods—Preterm lambs were exposed to antenatal steroids, and treated with perinatal surfactant and postnatal caffeine. Lambs were intubated and resuscitated by IMV. At ~3h of age, half of the lambs were switched to non-invasive HFNV. Support was for 3d or 21d. By design, PaO 2 and PaCO 2 were not different between groups. Results—At 3d (n=5) and 21d (n=4) of HFNV, fractional inspired O 2 (F i O 2 ), peak inspiratory pressure, mean airway, intra-tracheal, and positive end-expiratory pressures, oxygenation index, and Alveolar-arterial gradient were significantly lower than matched periods of intubation and IMV. PaO 2 /F i O 2 ratio was significantly higher at 3d and 21d of HFNV compared to matched intubation and IMV. HFNV led to better alveolarization at 3d and 21d. Conclusion—Long-term HFNV provides acceptable gas exchange at lower inspired O 2 levels and respiratory pressures compared to intubation and IMV. Introduction Endotracheal intubation and intermittent mandatory ventilation (IMV) are important risk factors for neonatal chronic lung disease (CLD; bronchopulmonary dysplasia, BPD) (1–5). Experimental animal studies indicate that contributors to lung injury are volutrauma, atelectotrauma, and hyperoxia (6–9). Volutrauma results from cyclic over-distension of the inhomogeneously inflated parenchyma of the immature lung. Atelectotrauma occurs during reopening of collapsed lung parenchyma. Both volutrauma and atelectotrauma expose the parenchymal cells and extracellular matrix to distortion that lead to altered expression of genes involved with lung inflammation and development (10–13). Hyperoxia sets the stage Users may view, print, copy, download and text and data- mine the content in such documents, for the purposes of academic research, subject always to the full Conditions of use: http://www.nature.com/authors/editorial_policies/license.html#terms ADDRESS CORRESPONDENCE TO: Kurt H. Albertine, Ph.D., Division of Neonatology, Department of Pediatrics, University of Utah Health Sciences Center, Williams Building, PO Box 581289, Salt Lake City, Utah 84158, TEL: (801) 213-3494 FAX: (801) 585-7395, [email protected]. The authors have no financial ties to products used in this study. NIH Public Access Author Manuscript Pediatr Res. Author manuscript; available in PMC 2014 October 01. Published in final edited form as: Pediatr Res. 2014 April ; 75(4): 507–516. doi:10.1038/pr.2013.254. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
High Frequency Nasal Ventilation for 21 Days Maintains GasExchange with Lower Respiratory Pressures and PromotesAlveolarization in Preterm Lambs
Donald M. Null1, Jeremy Alvord1, Wendy Leavitt1, Albert Wint1, Mar Janna Dahl1, Angela P.Presson2, Robert H. Lane1, Robert J. DiGeronimo1, Bradley A. Yoder1, and Kurt H.Albertine1
1Division of Neonatology, Department of Pediatrics, University of Utah, Salt Lake City, UT, USA2Division of Epidemiology, University of Utah, Salt Lake City, UT, USA
AbstractBackground—Short-term high-frequency nasal ventilation (HFNV) of preterm neonatesprovides acceptable gas exchange compared to endotracheal intubation and intermittent mandatoryventilation (IMV). Whether long-term HFNV will provide acceptable gas exchange is unknown.We hypothesized that HFNV for up to 21d would lead to acceptable gas exchange at lowerinspired oxygen (O2) levels and airway pressures compared to intubation and IMV.
Methods—Preterm lambs were exposed to antenatal steroids, and treated with perinatalsurfactant and postnatal caffeine. Lambs were intubated and resuscitated by IMV. At ~3h of age,half of the lambs were switched to non-invasive HFNV. Support was for 3d or 21d. By design,PaO2 and PaCO2 were not different between groups.
Results—At 3d (n=5) and 21d (n=4) of HFNV, fractional inspired O2 (FiO2), peak inspiratorypressure, mean airway, intra-tracheal, and positive end-expiratory pressures, oxygenation index,and Alveolar-arterial gradient were significantly lower than matched periods of intubation andIMV. PaO2/FiO2 ratio was significantly higher at 3d and 21d of HFNV compared to matchedintubation and IMV. HFNV led to better alveolarization at 3d and 21d.
Conclusion—Long-term HFNV provides acceptable gas exchange at lower inspired O2 levelsand respiratory pressures compared to intubation and IMV.
IntroductionEndotracheal intubation and intermittent mandatory ventilation (IMV) are important riskfactors for neonatal chronic lung disease (CLD; bronchopulmonary dysplasia, BPD) (1–5).Experimental animal studies indicate that contributors to lung injury are volutrauma,atelectotrauma, and hyperoxia (6–9). Volutrauma results from cyclic over-distension of theinhomogeneously inflated parenchyma of the immature lung. Atelectotrauma occurs duringreopening of collapsed lung parenchyma. Both volutrauma and atelectotrauma expose theparenchymal cells and extracellular matrix to distortion that lead to altered expression ofgenes involved with lung inflammation and development (10–13). Hyperoxia sets the stage
Users may view, print, copy, download and text and data- mine the content in such documents, for the purposes of academic research,subject always to the full Conditions of use: http://www.nature.com/authors/editorial_policies/license.html#terms
ADDRESS CORRESPONDENCE TO: Kurt H. Albertine, Ph.D., Division of Neonatology, Department of Pediatrics, University ofUtah Health Sciences Center, Williams Building, PO Box 581289, Salt Lake City, Utah 84158, TEL: (801) 213-3494 FAX: (801)585-7395, [email protected].
The authors have no financial ties to products used in this study.
NIH Public AccessAuthor ManuscriptPediatr Res. Author manuscript; available in PMC 2014 October 01.
Published in final edited form as:Pediatr Res. 2014 April ; 75(4): 507–516. doi:10.1038/pr.2013.254.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
for cytotoxic reactive oxygen species that contribute to cellular injury and reprogramming ofdevelopmental processes (14). Disruptions of lung developmental processes are structurallymanifest as alveolar simplification.
Early use of non-invasive respiratory support, such as nasal continuous positive airwaypressure (CPAP), is associated with better outcomes. For example, nasal CPAP is associatedwith less use and fewer days of intubation and IMV, lower levels of inspired oxygen (O2)(15), and lower rates of BPD or BPD/death (1, 16, 17). Insights from studies using pretermexperimental animal models of evolving neonatal CLD reveal possible mechanisms forbetter outcomes of non-invasive respiratory support. Functional studies using preterm lambsreveal lower expression of genes involved in acute-phase responses and markers ofinflammation at 2h bubble nasal CPAP compared to intubation and IMV (18, 19). Structuralstudies using preterm baboons demonstrate that early use of non-invasive respiratory supportpromotes alveolarization compared to invasive respiratory support (9, 20, 21). Our previousstudy shows that an approach to non-invasive respiratory support for 3d leads toalveolarization compared to intubation and IMV of preterm.
Whether long-term non-invasive support will provide prolonged physiological gas exchangeacross the lung accompanied by alveolar formation is unknown. Therefore, we used ourpreterm lamb model of evolving neonatal CLD to prospectively determine the impact ofprolonged high-frequency nasal ventilation (HFNV) on physiological outcomes forrespiratory gas exchange and respiratory pressures, and morphological outcomes for alveolarformation. We hypothesized that HFNV for up to 21d would lead to acceptable respiratorygas exchange at lower inspired O2 levels and airway pressures, as well as alveolarformation, compared to intubation and IMV. The principal results of our study show thatHFNV out to 21d provides acceptable respiratory gas exchange that is accompanied byalveolar formation.
Materials and MethodsProtocols adhered to APS/NIH guidelines for humane use of animals for research, and wereprospectively approved by the IACUC at the University of Utah Health Sciences Center.
Surgical PreparationThe methods for chronically ventilating preterm lambs are reported (9, 22, 23). Briefly,time-pregnant ewes that carried one fetus or twin fetuses at 132±2d of gestation (term ~150dgestation) were used. The pregnant ewes were given an intramuscular injection ofdexamethasone phosphate (6 mg; Vedco, Inc., St. Joseph, MO), ~36h before operativedelivery. At delivery, we intubated all fetal lambs with a cuffed endotracheal tube (3.5 to 4.0French), through which 10 mL of lung liquid was aspirated and replaced with Survanta (2.5mL; NDC 0074-1040-08, Ross Products Division, Abbott Laboratories, Columbus, OH).
Additional Surgical Step for HFNVWe prospectively and randomly assigned a subset of all of the intubated preterm lambs to beweaned to high-frequency nasal ventilation (HFNV) within ~3h of life (see theRandomization subsection). This subset had an uncuffed oral/nasal true Murphy tube (3.0French; 13 cm length) inserted ~5 cm through a nostril. We used a Murphy tube becausepreliminary studies revealed that preterm lambs did not tolerate nasal prongs or a nasalmask.
Null et al. Page 2
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Initial Resuscitation of all Preterm LambsAll lambs were intubated and managed by IMV, with warmed and humidified O2 (Bird VIPventilator; model 15215, Palm Springs, CA). Initial settings were: respiratory rate 60breaths/min, inspiratory time 0.3 sec, positive end-expiratory pressure (PEEP) 7 cmH2O,flow 8 L/min of 50% O2, and expiratory tidal volume 5–7 mL/Kg. Within 30 min ofdelivery, the lambs were given an intravenous loading dose of caffeine citrate (15 mg/Kg,given over 2h, Mead Johnson & Company, Evansville, IN) to stimulate ventilatory drive.Caffeine citrate was given every 24h (5 mg/Kg). Arterial blood gases, pH, electrolytes, andglucose were measured hourly, as was O2 saturation by pulse oximetry. Vascular pressuresand heart rate were recorded continuously (model V6400, SurgVet, Inc.; Waukesha, WI).Dextrose was infused intravenously to maintain plasma glucose level between 60 and 90mg/dL. Plasma concentrations of total protein and hematocrit were measured at 6h intervals.
Arterial partial pressure of oxygen (PaO2) was targeted between 70 and 90 mmHg byadjusting fractional inspired O2 (FiO2). Arterial partial pressure of carbon dioxide (PaCO2)was targeted between 40 and 60 mmHg, and pH between 7.25–7.45, by adjusting peakinspiratory pressure (PIP). Mean pressure in the airway (Paw) also was measured. Wecalculated oxygenation index (OI) [(Paw × FiO2)/PaO2], Alveolar-arterial (A-a) gradient[((FiO2/100) × (640−47)) − (PaCO2/0.8) − PaO2], and PaO2/FiO2 (P/F) ratio.
RandomizationRandomization to invasive versus non-invasive of respiratory support for 3d or 21d wasdone using a block randomization approach. We studied two preterm lambs concurrently.
Two Modes of Respiratory SupportInvasive respiratory support was endotracheal intubation and IMV. Non-invasive respiratorysupport was a unique approach of nasal ventilation with a high-frequency componentcreated by a high-frequency, flow-interruption ventilator (model VDR4, Percussionaire Inc.,Sand Point, ID). We call this mode high-frequency nasal ventilation (HFNV). ThePercussionaire is a flow-regulated, time-cycled ventilator that provides controlled-pressuredelivery of low-frequency breathing cycles with a series of high-frequency, sub-physiologictidal volumes (24).
Weaning from IMV, begun at 2h of life, was successful when the lambs consistentlybreathed spontaneously while the ventilator circuit to the Bird VIP ventilator wasdisconnected from the endotracheal tube (9). At that time, the endotracheal tube waswithdrawn and the ventilator circuit from the Percussionaire ventilator was attached to thetube in the nose. Initial ventilator settings were background convective breaths at 5–10breaths per min PIP of 20–25 cmH2O, PEEP of 5–7 cmH2O, and high-frequency rate at 10Hz. The ventilator circuit included a gas humidifier. Adjustments were made to theventilator settings to reach the target ranges for PaO2 and PaCO2. Because a leak-free sealwas not possible during HFNV, lung volumes could not be directly measured.
Measurement of Airway Pressures in situPhasic and mean pressures from the ventilator to the trachea were measured in situ, using apressure-tipped wire (Samba Sensor model Preclin 420 LP, Samba Sensors SE, VästraFrölunda, Sweden). The wire was inserted through a rubber-covered side port of theconnector piece to the endotracheal tube or nasal tube.
Null et al. Page 3
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Management of Preterm LambsLambs were kept prone in a veterinary sling mounted on a radiantly heated bed. Antibioticswere given daily (potassium penicillin, 100,000 U/Kg, Pfizer; and gentamicin, 2.5 mg/Kg/d,Hospira, Inc.). Gentamicin was discontinued at 10d. Sedation was provided, usingpentobarbital sodium and buprenorphine hydrochloride. Lambs that were randomized tointubation and IMV received 3–5 mg/Kg of pentobarbital sodium (Abbott Laboratories,North Chicago, IL) as needed to minimize discomfort and agitation associated withendotracheal intubation. Lambs that were randomized to HFNV received only 1–2 mg/Kg ofpentobarbital as needed to permit spontaneous breathing. All lambs were initially givenbuprenorphine hydrochloride (5 mcg/Kg every 3h, Reckitt & Colman Pharmaceuticals,Richmond, VA) for the 3d study. For the 21d study, buprenorphine dosage was reduced at 1wk of life and thereafter for the HFNV group to minimize respiratory depression.
An orogastric feeding tube was used for enteral feedings, using ewe’s colostrum, beginningat 4h of life (3 mL/Kg every 2h) and continued for 3d. The volume was increased graduallyby 3–5 mL increments, as tolerated, to attain a goal of 60–80 Kcal/Kg/d of total energysubstrate, based on daily weight. After 3d, ewe’s milk was given. Volume was increased astolerated. We monitored total fluid intake (saline, dextrose, and milk) and output (withdrawnblood, urine, and stool), and made adjustments to maintain fluid homeostasis, as indicatedby urine output (>1–2 mL/Kg/h) and mean arterial blood pressure (>45 mmHg). None of thelambs required pressors. Chest radiographs were taken on days of life 1, 2, and 3 of all of the3d (n=5/group) and 21d lambs (n=4/group), and weekly thereafter for the 21d lambs, toassess lung inflation volume and to identify atelectasis. Indices of infection were monitoredby daily leukocyte total and differential cell counts, and rectal temperature.
Terminal Collection of TissueBlood samples were collected before the lambs were given heparin (1000 U, intravenously)followed by 5 mg/Kg of pentobarbital (9, 23). Both HFNV groups were intubated andreconnected to the Percussionaire ventilator to maintain lung inflation when the chest wasopened to remove the lungs. All lambs were given 60 mg/Kg pentobarbital sodium solutionintravenously (Beuthanasia solution, Ovation Pharmaceuticals, Inc., Deerfield, IL). Thechest was opened, the trachea was ligated at end-inspiration (to minimize atelectasis), andthe lungs and heart were removed. The whole left lung was insufflated with 10% bufferedneutral formalin (static pressure of 25 cmH2O). Fixed-lung displacement volume wasmeasured by suspension in formalin before the lung was stored in fixative (4°C, 24h).Paraffin-embedded tissue blocks were prepared for histology.
Quantification of Alveolar Secondary Septation and Distal Airspace Wall ThicknessWe used quantitative histology (morphometry and stereology) to statistically comparealveolar secondary septation (radial alveolar count and secondary septal volume density) anddistal airspace wall thickness, using methods previously reported by our group (9).
Data AnalysisContinuous variables that were approximately normally distributed are summarized by mean± standard deviation (SD). These results were compared by unpaired t-test. Continuousvariables that were not approximately normally distributed are summarized by the medianand interquartile range (IQR). These results were analyzed by Mann-Whitney U-test. Linearmixed effects models were used to test whether FiO2, PIP, and Paw changed differently overtime (time effects) during intubation and IMV versus HFNV, and whether the tworespiratory support groups changed differently over time (group-time interaction). We useda simple random intercept model, with a variance-covariance structure that assumed
Null et al. Page 4
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

compound symmetry across time points. Statistical analyses were done using StatView5(SAS Institute, Inc., Cary, NC) or R v2.15.0. Statistical significance was assessed at p<0.05.
ResultsWe defined successful experiments as reaching the prospective 3d or 21d of respiratorysupport. By this definition, overall success was ~75%. For the 3d studies, the sample size isfive. Seven preterm lambs were necessary because two male lambs developed respiratorydistress secondary to uncontrolled air leaks that occurred within the first 12h of life. Bothlambs died shortly thereafter and thus were excluded. All five preterm lambs that wereweaned to HFNV survived. For the 21d studies, the sample size is four. Seven pretermlambs were necessary because three lambs (2 male; 1 female) developed respiratory distresssecondary to uncontrolled air leaks or renal failure within week of life 3, before 21d, andtherefore were excluded. The male lamb required re-intubation and IMV during week of life3 (day 15) and could not be weaned back to HFNV.
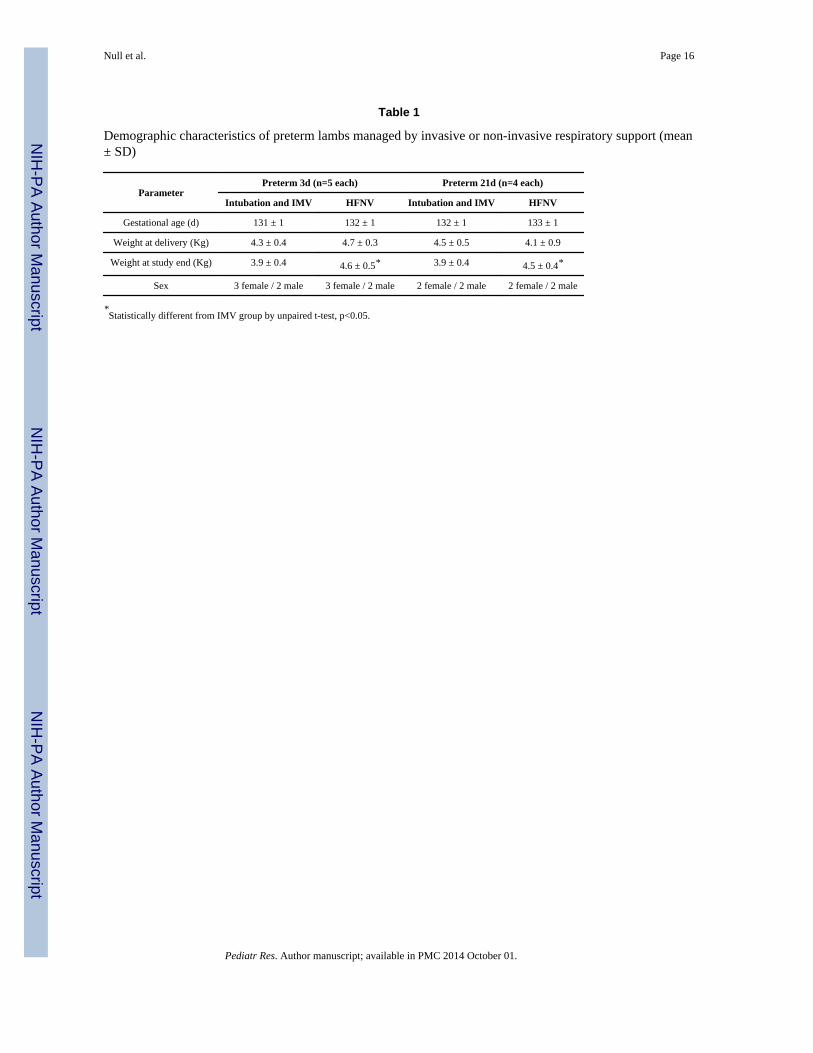
Demographic characteristics are summarized in Table 1. Gestational age, birth weight, andsex were the same within and between the 3d and 21d groups. However, body weight at 3dor 21d was significantly greater in HFNV group compared to the corresponding intubationand IMV group (p<0.05).
The radiographic shadow of the uncuffed true Murphy tube is visible in the midline of thehead (Figure 1a). Postmortem, the nasal cavity was opened for all five 3d HFNV lambs tomeasure the location of the tip from the nostril. The tip was ~5 cm into the nasal cavity (~10cm long; data not shown).
A segment of an intra-tracheal pressure trace in a lamb supported by HFNV is shown inFigure 1b. The Percussionaire ventilator was configured to provide high-frequency, lowamplitude pressure fluctuations during both inspiration and expiration (Figure 1b). Alsoevident are two background low-frequency breaths (pressure-limited at 17 cmH2O).
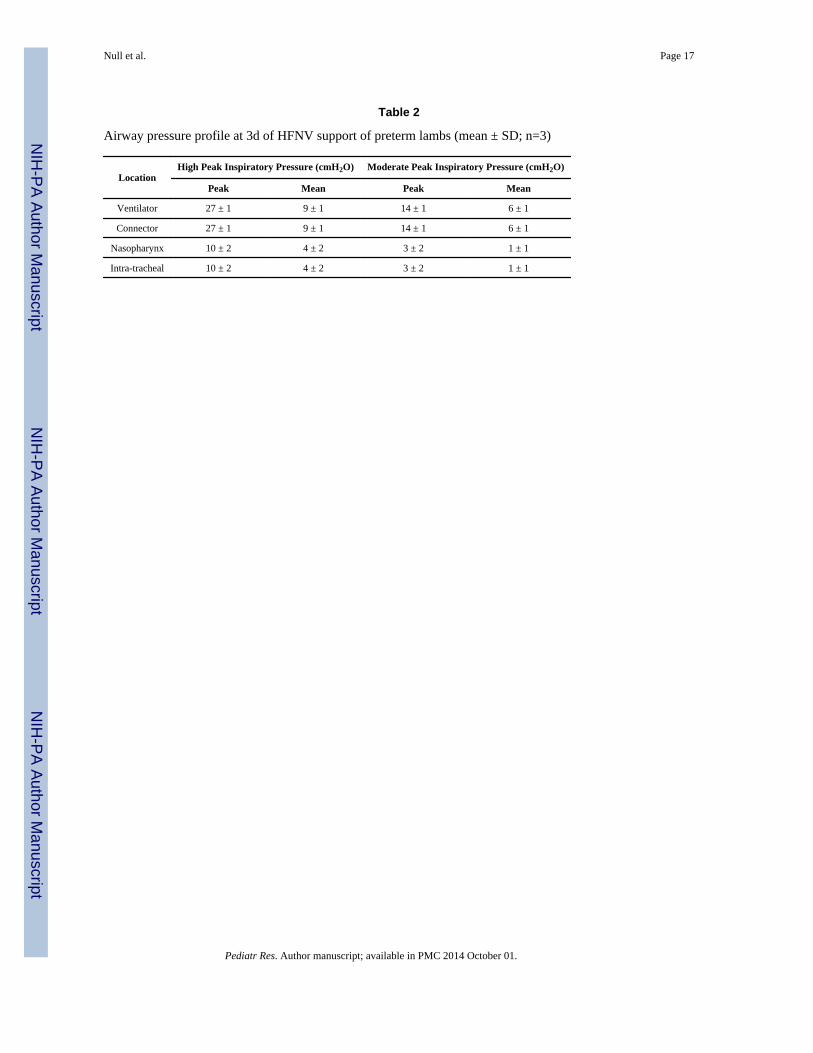
Pressure measurements at the ventilator, connector piece from the ventilator circuit to thenasal tube, in the nasopharynx, and intra-tracheally are summarized in Table 2. We testedtwo peak pressure settings: high PIP (~27 cmH2O) or moderate PIP (~14 cmH2O).Regardless of PIP setting, the corresponding peak and mean pressures persisted at thejunction of the connector to the nasal tube. However, peak and mean pressures were ~60%less at the nasopharynx (1–2 cm cranial to the vocal cords), as well as in the trachea (~10 cmcaudal to the vocal cords).
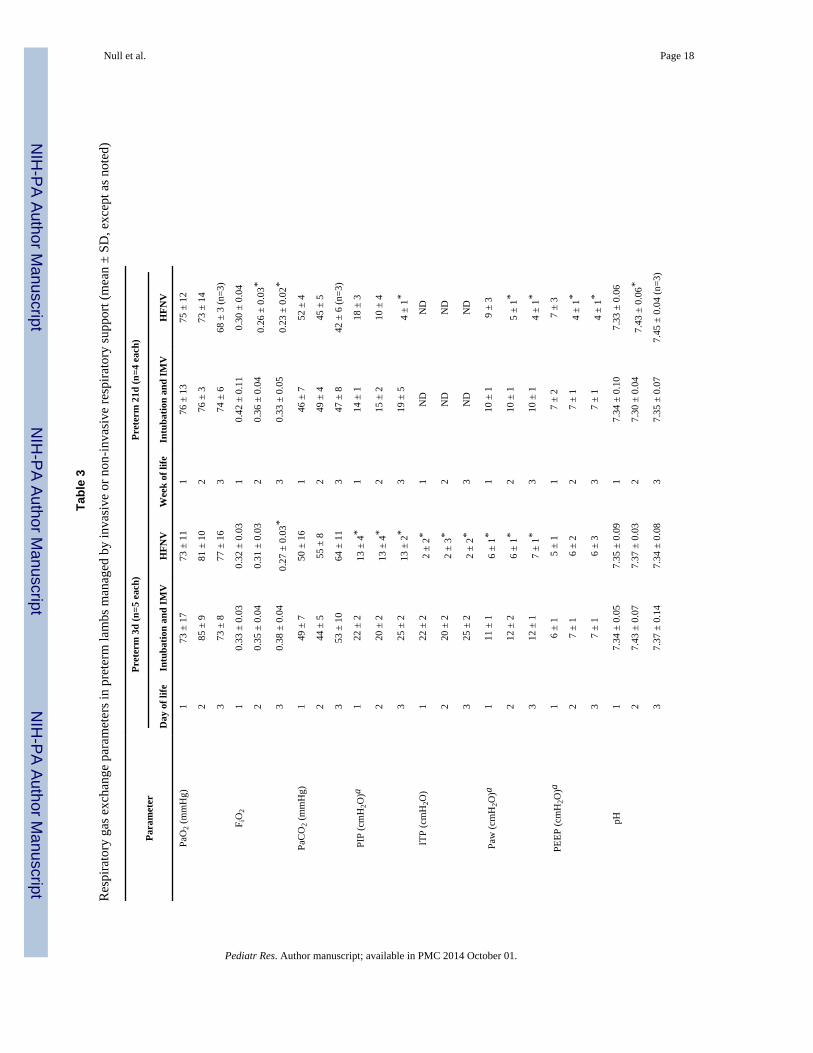
Daily gas exchange and respiratory support results for the 3d groups of ventilated pretermlambs are summarized in Table 3 (middle columns). By design, the two groups (n=5 each)had the same targeted range for PaO2 (73–85 mmHg) and targeted range for PaCO2 (44–64mmHg) at days of life 1, 2, and 3. The physiologically targeted PaO2 range was attainedusing ~30% lower FiO2 on day of life 3 (p<0.05) for the HFNV group compared to theintubation and IMV group. Likewise, the physiologically targeted PaCO2 range was attainedusing ~40% lower PIP (p<0.05) at each day-of-life for the HFNV group. Paw was ~50%lower (p<0.05). PEEP at the ventilator was the same between the two groups at each day oflife. Intra-tracheal pressure (ITP) measured in situ was ~90% lower (p<0.05) at each day oflife for the HFNV group compared to the intubation and IMV group.
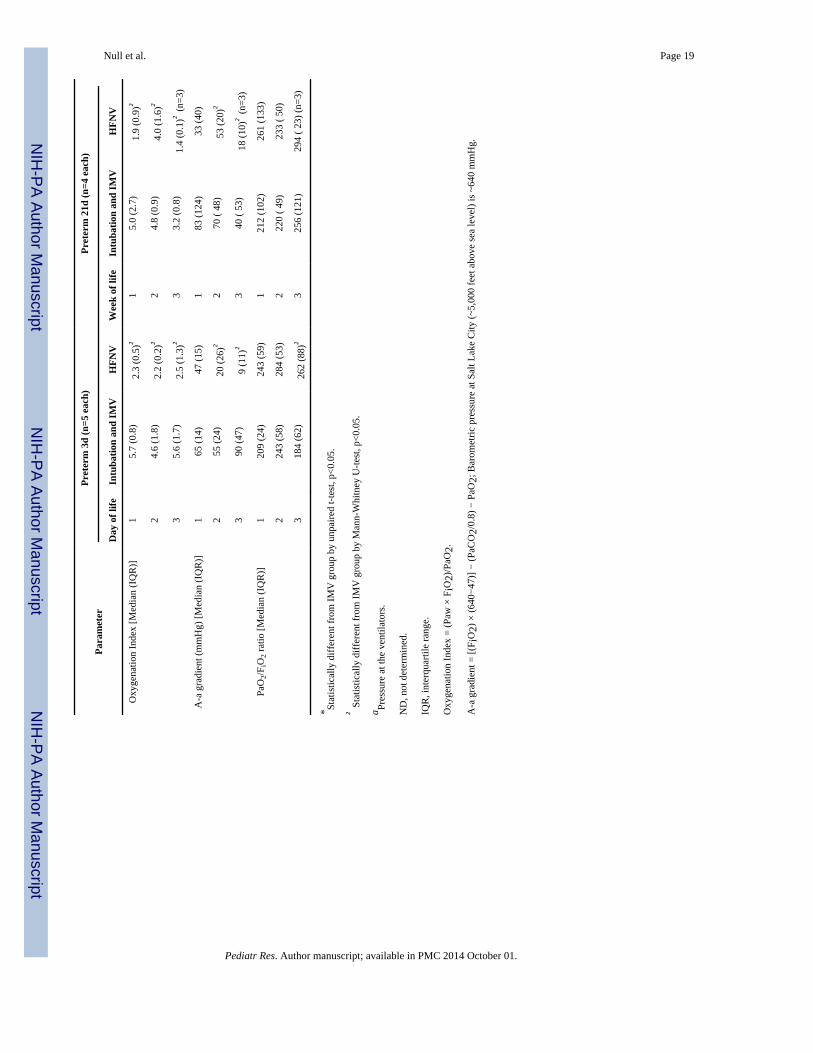
We calculated oxygenation index (OI), Alveolar-arterial gradient of O2 (A-a gradient), andPaO2/FiO2 (P/F) ratio (Table 3). Median OI was ~60% lower at each day of life (p<0.05) forthe HFNV group compared to the intubation and IMV group. The difference was even largerwhen we substituted mean ITP measured in situ for Paw in the formula for OI. Using ITP in
Null et al. Page 5
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
the formula, median OI was ~80% lower at each day of life (p<0.05) for the HFNV groupcompared to the intubation and IMV group. Median A-a gradient was ~60 to 90% lower atdays of life 2 and 3 for the HFNV group. The calculation of A-a gradient took into accountthe lower barometric pressure at Salt Lake City (~5,000 feet above sea level). Conversely,median P/F ratio was ~50% higher at day-of-life 3 for the HFNV group of lambs supportedfor 3d.
Prolonged HFNV for 21d also provided acceptable gas exchange and respiratory systempressures (Table 3; right-most columns). A caveat is one lamb in the HFNV groupdeveloped a blood clot in its arterial catheter. Therefore, arterial blood could not be sampledduring its final week of life. Thus, sample size became 3 for just arterial blood gas values atweek of life 3 for the HFNV group. We continued to measure O2 saturation, which remainedbetween 88% and 94%, and therefore was within the same range as all of the other lambs inthe 21d groups (data not shown).
For the 21d groups, targeted arterial PaO2 range was attained using ~30% lower FiO2 atweeks of life 2 and 3 (p<0.05) for the HFNV group compared to the same weeks for thematched intubation and IMV group. The targeted PaCO2 range was attained using ~75%lower respiratory system pressures for the HFNV group (p<0.05). Both Paw and PEEP were~50% lower at weeks of life 2 and 3 (p<0.05) compared to the matched weeks of life for theintubation and IMV group. At weeks of life 2 and 3, pH was significantly higher (p<0.05)for the HFNV group. We did not measure ITP in situ in the 21d HFNV group because thatwould have required sedating and intubating the lambs, which could have affected thephysiological results. For this reason, OI was calculated using Paw for the 21d groups.Median OI was ~20 to 60% lower at each week of life (p<0.05) for the HFNV groupcompared to the intubation and IMV group. Median A-a gradient was ~25 to 50% lower atweeks of life 2 and 3 (p<0.05) for the HFNV group. Median P/F ratio, while larger for theHFNV group at each week of life, was not different between the two 21d groups. Thesephysiological improvements for the HFNV group were not influenced by initial differencesin ventilator settings during the first 3h of IMV, before weaning to HFNV (see the table inonline supplemental material).
We found time effects and group-time interactions between the HFNV group and theintubation and IMV group for the 21d study, using linear mixed effects models. Time effectswere detected overall for both PIP (β = −5.6, t(16) = −6.0, p<0.05) and Paw (β = −2.4, t(16)= −5.3, p<0.05). PIP and Paw decreased from week-of-life 1 to 3 for the HFNV group,whereas PIP increased slightly and Paw remained constant during the same time period forthe intubation and IMV group. These group differences were corroborated by group-timeinteractions (PIP: β = 7.5, t(16) = 6.0, p<0.05; Paw: (β= 2.4, t(16) = 4.0, p<0.05). Themodels also showed that FiO2 tended to decrease from week-of-life 1 to 3; however, thetrend was not statistically significant (β = −0.04, t(16) = 1.8, p=0.09).
The physiologically better outcomes for the HFNV groups at 3d and 21d were associatedwith better radiographic and histologic appearances of the lungs (Figure 2).Radiographically, the lung fields were more translucent and lung volumes appeared largerfor all five preterm lambs at 3d of HFNV and all four preterm lambs at 21d of HFNVcompared to the matched number of preterm lambs per period of intubation and IMV. Also,air bronchograms were less obvious radiographically for all of the preterm lambs in the twoHFNV groups. Histologically, terminal respiratory units appeared more developed in theHFNV group than the matched intubation and IMV groups. That is, the lung’s parenchymalappearance in the HFNV groups included distal airspaces that had more uniform andhomogeneous size and shape. These observations were borne out by quantitative histology(Figure 3). Morphometry and stereology showed that at 21d of ventilation support, the
Null et al. Page 6
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

HFNV group had greater radial alveolar count (p<0.05) and volume density for alveolarsecondary septa (p<0.05), and narrower distal airspace walls (p<0.05), compared to the IMVgroup.
We compared the feeding volume between HFNV and IMV groups because of the potentialfor differences in nutrition to influence lung development. For the 3d study, the dailyvolume of colostrum was the same between the HFNV group and the intubation and IMVgroup (Table 4). For the 21d study, by comparison, the weekly volume of colostrum/milkincreased for the HFNV group, whereas the weekly volume decreased for the intubation andIMV group (Table 4). At week of life 3, the volume of milk delivered was 3.5-fold larger forthe HFNV group. Nonetheless, plasma glucose remained physiological in between HFNVand IMV groups (Table 4).
We also compared the dosages of pentobarbital and buprenorphine that were given to theHFNV and IMV groups (Table 4). For the 3d study, the daily dosages of pentobarbital andbuprenorphine were comparable between the HFNV group and the intubation and IMVgroup. However, for the 21d study, weekly dosages of pentobarbital and buprenorphine weresignificantly lower for the HFNV group (p<0.05).
DiscussionOur study has two principal results for chronically ventilated preterm lambs. The firstprincipal result is physiological arterial blood gas values are maintained for 21d of HFNV,with significantly lower applied O2 and respiratory system pressures, compared to intubationand IMV. Secondly, alveolar formation progressed during 21d of HFNV, whereas alveolarsimplification occurred during 21d of intubation and IMV. Together, these principal resultsshow that non-invasive HFNV leads to prolonged improvement in functional and structuraldevelopment of the lung of preterm lambs. Conversely, prolonged invasive ventilationevolves into neonatal CLD through persistent disruption of both functional and structuraldevelopment of the parenchyma of the immature lung.
The driver for non-invasive respiratory support was a Percussionaire ventilator (Sand Point,ID). This ventilator allows for a combined low-frequency conventional/high-frequencypercussive approach, whereby a conventional pressure-limited, time-cycled breath providedat low background frequency is coupled with an underlying high-frequency pattern of small,percussive pressures that deliver sub-physiological tidal volumes (24). Thus, bothconventional and high-frequency gas exchange principles were configured. Thiscombination of principles is similar to combining conventional pressure-limited breaths withhigh-amplitude bubble nasal CPAP, which augments volume delivery and reduces work ofbreathing (25). Coupling creates “biologic noise” (also called stochastic resonance) in thetotal waveform that is postulated to contribute to recruitment of lung volume (26–28). ThePercussionaire ventilator, when configured to provide low-frequency conventional breaths,is unique in its ability to continuously provide sub-physiologic tidal volume, high-frequencybreaths throughout both inspiratory and expiratory phases of respiration.
We used low-frequency conventional and high-frequency percussive configuration becausepreterm lambs that were supported by bubble nasal CPAP for more than 3–4h hadprogressive deterioration of respiratory gas exchange (9). We initially tried bubble nasalCPAP because it is associated with less abundance of pro-inflammatory mediators (18) andmore production of surfactant in the lung (29). However, we found that during prolongedbubble nasal CPAP, PaCO2 and pH became unphysiological even though the lambs weretreated with antenatal corticosteroids to promote lung development, exogenous surfactant toenhance lung compliance, and caffeine citrate to stimulate respiratory drive. While the cause
Null et al. Page 7
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
of progressive deterioration of respiratory gas exchange remains unknown, we suspect thatthe long nose and neck of lambs, which increase anatomic dead space, may be contributory.Our results suggest that long-term use of HFNV as applied in this study may be a moreeffective approach to non-invasive respiratory support than either nasal CPAP or nasal IMV(30–33).
Use of short-term non-invasive ventilation support, with supra-physiological respiratoryfrequency through a nasopharyngeal tube, is reported for preterm infants. Two studies usedan Infant Star HFV ventilator in its HFV mode. Van der Hoeven and colleagues (34) usednasal HFV in 21 premature infants within the first 20 d of life; 72% of infants were startedon nasal HFV within 36 hours of age. Nearly 80% of infants showed improved ventilationand oxygenation, with a median of 36 hours support via nasal HFV. Colaizy and coworkers(35) used the same type of ventilator to support 14 stable preterm infants for 2h. Theirresults showed that nasal HFV significantly reduced PaCO2 and raised pH. However, theInfant Star ventilator is no longer made. Furthermore, the Infant Star ventilator was limitedby maximum amplitude that it could generate, which limited the tidal volume that wasdelivered. A third study used a Draeger Babylog 8000 ventilator for 24h after extubation ofa 760 gm preterm infant. Hoehn and Krause (36) showed that the infant’s PaCO2 remainedin physiological range, thereby avoiding reintubation. A fourth study used the VDR3Percussionaire, which is what we used. Dumas De La Roque (37) used HFNV in aprospective, unmasked, randomized, controlled clinical trial for 46 eligible newborn infantswho were hospitalized for transient tachypnea of the newborn. HFNV reduced the period oftransient tachypnea by 50%. However, those studies did not test long-term efficacy. Ourexperimental animal model’s results show that 21d of HFNV, as we used it, facilitatesphysiological arterial blood gas values at lower FiO2 and respiratory pressures. Whether ourresults in preterm lambs are translatable will require testing HFNV in high-risk preterminfants. This test will be important because of anatomic differences of the nose and neckbetween lambs and infants.
Only one of the lambs failed to reach 21d of HFNV. Failure was related to progressiverespiratory failure. Another observation of our study is that air accumulated in the stomachof some of the lambs that were supported by HFNV. This observation, also common amongpreterm infants on nasal ventilation, was easily managed by vented orogastric tube and didnot impair feeding tolerance.
An important physiological point made by our study is that intra-tracheal pressure is verylow during HFNV. The in situ measurements show that intra-tracheal pressure during HFNVof spontaneously breathing preterm lambs is about 1/10th that during intubation and IMV(Table 3). The location where pressure is attenuated is after the connector piece, in thenasopharynx. Attenuation is ~60% of the pressure setting at the ventilator (Table 2). Peakand mean airway pressures were respectively constant within the nasopharynx and trachea.The in situ measurements also reveal that HFNV maintains positive mean intra-trachealpressure of 1–2 cmH2O, therefore low PEEP. In our model, substantial opportunity existsfor leak from the nasal-oropharyngeal cavity. In the presence of substantial leak, others alsodemonstrated, through direct or indirect measurements, more significant reduction in distalairway pressure than expected based on the measured or set pressure at the device interface(38, 39). During intubation and IMV support, by comparison, airway pressures reflected thepressure settings at the ventilator (Table 3). The latter finding is consistent with the resultsof a study showing that intratracheal pressure during invasive mechanical ventilation iscomparable to ventilator pressure (40).
Low peak and mean intra-tracheal pressures during HFNV, combined with more uniforminflation seen radiographically, may contribute to the better structural development of the
Null et al. Page 8
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

lung’s parenchyma. Indeed, studies using chronically ventilated preterm baboonsdemonstrate that early nasal CPAP promotes alveolar formation compared to intubation andIMV (20, 21). We recently reported that progression of alveolar formation at the end of 3dof HFNV is associated with more apoptosis, and less proliferation, among mesenchymalcells in the walls of the distal airspaces compared to intubation and IMV (9). This level ofbalance between apoptosis and proliferation of mesenchymal cells is related to thinning ofthe distal airspace walls, which is necessary for efficient respiratory gas exchange. We are inthe process of quantifying apoptosis and proliferation of mesenchymal cells in pretermlambs that were supported by HFNV versus IMV for 21d, and will report the resultsseparately.
A potential confounding element of our study design is that all of the preterm lambs wereendotracheally intubated and supported by IMV during the ~3h transition period leading toHFNV support. However, no differences in the initial ventilator settings or respiratoryphysiological results occurred (refer to supplemental online data), suggesting that the 3htransition period of IMV did not confound the outcomes for the HFNV groups.
Better pulmonary outcomes at 21d of HFNV may be related to better enteral feeding andweight gain (Table 4) (41, 42). Better enteral feeding and weight gain, in turn, may beimpacted by less sedation (Table 4) because sedation decreases gastrointestinal motility andabsorption, as well as growth and development of the lung (43). In new studies, we aredetermining the separate effects of enteral feeding versus sedation on lung structural andfunctional outcomes. We are assessing the impact of matched-feeding (mL (calories)/Kg/d)versus matched-sedation (mg/Kg/d) in separate groups of preterm lambs on HFNV.Matching is done at the daily level for intubated preterm lambs on IMV. Initial resultssuggest that only matched enteral feeding shifts lung outcomes toward the poorer outcomesthat occur in intubated lambs on IMV.
We conclude that early non-invasive respiratory support via HFNV as we applied using ahigh-frequency flow interrupter ventilator, coupled with maternal antenatal steroids,prophylactic surfactant replacement, and postnatal caffeine therapy, effectively maintainsgas exchange at lower O2 levels and respiratory pressures out to 21d. In addition, thequantitative histological results indicate that HFNV out to 21d improves alveolarization. Ourstudy’s results raise the possibility that long-term HFNV may be an alternative approach toacceptable respiratory support for preterm infants. Our observation that lung development isoccurring raises the possibility that HFNV may reduce neonatal CLD (17). Translating ourresults from preterm lambs to preterm infants will require clinical studies.
AcknowledgmentsSupported by National Institutes of Health (NIH) grants HL110002, HL062875, HL007744, the Division ofNeonatology, and the Children’s Health Research Center in the Department of Pediatrics, and the University ofUtah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resourcesand the National Center for Advancing Translational Sciences, NIH grant 8UL1 TR000105 (formerly UL1RR025764).
We thank the large number of undergraduate students and medical students who tended the chronically ventilatedpreterm lambs. We also thank Ronald S. Bloom, MD for suggestions.
References1. Van Marter LJ, Allred EN, Pagano M, et al. Do clinical markers of barotrauma and oxygen toxicity
explain interhospital variation in rates of chronic lung disease? The Neonatology Committee for theDevelopmental Network. Pediatrics. 2000; 105:1194–1201. [PubMed: 10835057]
Null et al. Page 9
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
2. Henderson-Smart DJ, Cools F, Bhuta T, Offringa M. Elective high frequency oscillatory ventilationversus conventional ventilation for acute pulmonary dysfunction in preterm infants. CochraneDatabase Syst Rev. 2007:CD000104. [PubMed: 17636590]
3. Yoder BA, Harrison M, Clark RH. Time-related changes in steroid use and bronchopulmonarydysplasia in preterm infants. Pediatrics. 2009; 124:673–679. [PubMed: 19620192]
4. Gortner L, Misselwitz B, Milligan D, et al. Rates of bronchopulmonary dysplasia in very pretermneonates in Europe: results from the MOSAIC cohort. Neonatology. 2011; 99:112–117. [PubMed:20733331]
5. Laughon MM, Langer JC, Bose CL, et al. Prediction of bronchopulmonary dysplasia by postnatalage in extremely premature infants. Am J Respir Crit Care Med. 2011; 183:1715–1722. [PubMed:21471086]
6. Delemos RA, Coalson JJ, Gerstmann DR, et al. Ventilatory management of infant baboons withhyaline membrane disease: the use of high frequency ventilation. Pediatr Res. 1987; 21:594–602.[PubMed: 3299231]
7. Carlton DP, Cummings JJ, Scheerer RG, Poulain FR, Bland RD. Lung overexpansion increasespulmonary microvascular protein permeability in young lambs. J Appl Physiol. 1990; 69:577–583.[PubMed: 2228868]
8. Davis JM, Dickerson B, Metlay L, Penney DP. Differential effects of oxygen and barotrauma onlung injury in the neonatal piglet. Pediatr Pulmonol. 1991; 10:157–163. [PubMed: 1852512]
9. Reyburn B, Li M, Metcalfe DB, et al. Nasal ventilation alters mesenchymal cell turnover andimproves alveolarization in preterm lambs. Am J Respir Crit Care Med. 2008; 178:407–418.[PubMed: 18556628]
10. Han B, Lodyga M, Liu M. Ventilator-induced lung injury: role of protein-protein interaction inmechanosensation. Proc Am Thorac Soc. 2005; 2:181–187. [PubMed: 16222035]
11. Harding R, Hooper SB. Regulation of lung expansion and lung growth before birth. J ApplPhysiol. 1996; 81:209–224. [PubMed: 8828667]
12. Kitterman JA. The effects of mechanical forces on fetal lung growth. Clin Perinatol. 1996; 23:727–740. [PubMed: 8982567]
13. Albertine KH. Progress in understanding the pathogenesis of BPD using the baboon and sheepmodels. Seminars in perinatology. 2013; 37:60–68. [PubMed: 23582959]
14. Buczynski BW, Maduekwe ET, O’Reilly MA. The role of hyperoxia in the pathogenesis ofexperimental BPD. Seminars in perinatology. 2013; 37:69–78. [PubMed: 23582960]
15. Finer NN, Carlo WA, Walsh MC, et al. Early CPAP versus surfactant in extremely preterm infants.NEJM. 2010; 362:1970–1979. [PubMed: 20472939]
16. Levesque BM, Kalish LA, LaPierre J, Welch M, Porter V. Impact of implementing 5 potentiallybetter respiratory practices on neonatal outcomes and costs. Pediatrics. 2011; 128:e218–226.[PubMed: 21669893]
17. Carlo WA. Gentle ventilation: the new evidence from the SUPPORT, COIN, VON, CURPAP,Colombian Network, and Neocosur Network trials. Early Hum Dev. 2012; 88 (Suppl 2):S81–83.[PubMed: 22633522]
18. Jobe AH, Kramer BW, Moss TJ, Newnham JP, Ikegami M. Decreased indicators of lung injurywith continuous positive expiratory pressure in preterm lambs. Pediatr Res. 2002; 52:387–392.[PubMed: 12193673]
19. Hillman NH, Moss TJ, Nitsos I, Jobe AH. Moderate tidal volumes and oxygen exposure duringinitiation of ventilation in preterm fetal sheep. Pediatr Res. 2012; 72:593–599. [PubMed:23037872]
20. Thomson MA, Yoder BA, Winter VT, et al. Treatment of immature baboons for 28 days with earlynasal continuous positive airway pressure. Am J Respir Crit Care Med. 2004; 169:1054–1062.[PubMed: 14962819]
21. Thomson MA, Yoder BA, Winter VT, Giavedoni L, Chang LY, Coalson JJ. Delayed extubation tonasal continuous positive airway pressure in the immature baboon model of bronchopulmonarydysplasia: lung clinical and pathological findings. Pediatrics. 2006; 118:2038–2050. [PubMed:17079577]
Null et al. Page 10
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
22. Albertine KH, Jones GP, Starcher BC, et al. Chronic lung injury in preterm lambs. Disorderedrespiratory tract development. Am J Respir Crit Care Med. 1999; 159:945–958. [PubMed:10051278]
23. Albertine KH, Dahl MJ, Gonzales LW, et al. Chronic lung disease in preterm lambs: effect of dailyvitamin A treatment on alveolarization. Am J Physiol Lung Cell Mol Physiol. 2010; 299:L59–L72.[PubMed: 20382748]
24. Lucangelo U, Fontanesi L, Antonaglia V, et al. High frequency percussive ventilation (HFPV).Principles and technique Minerva Anestesiol. 2003; 69:841–848.
25. Diblasi RM, Zignego JC, Tang DM, et al. Noninvasive respiratory support of juvenile rabbits byhigh-amplitude bubble continuous positive airway pressure. Pediatr Res. 2010; 67:624–629.[PubMed: 20308940]
26. Suki B, Alencar AM, Sujeer MK, et al. Life-support system benefits from noise. Nature. 1998;393:127–128. [PubMed: 9603516]
27. Pillow JJ, Travadi JN. Bubble CPAP: is the noise important? An in vitro study Pediatr Res. 2005;57:826–830.
28. Pillow JJ, Hillman N, Moss TJ, et al. Bubble continuous positive airway pressure enhances lungvolume and gas exchange in preterm lambs. Am J Respir Crit Care Med. 2007; 176:63–69.[PubMed: 17431223]
29. Mulrooney N, Champion Z, Moss TJ, Nitsos I, Ikegami M, Jobe AH. Surfactant and physiologicresponses of preterm lambs to continuous positive airway pressure. Am J Respir Crit Care Med.2005; 171:488–493. [PubMed: 15502113]
30. Friedlich P, Lecart C, Posen R, Ramicone E, Chan L, Ramanathan R. A randomized trial ofnasopharyngeal-synchronized intermittent mandatory ventilation versus nasopharyngealcontinuous positive airway pressure in very low birth weight infants after extubation. J Perinatol.1999; 19:413–418. [PubMed: 10685270]
31. Khalaf MN, Brodsky N, Hurley J, Bhandari V. A prospective randomized, controlled trialcomparing synchronized nasal intermittent positive pressure ventilation versus nasal continuouspositive airway pressure as modes of extubation. Pediatrics. 2001; 108:13–17. [PubMed:11433048]
32. Barrington KJ, Bull D, Finer NN. Randomized trial of nasal synchronized intermittent mandatoryventilation compared with continuous positive airway pressure after extubation of very low birthweight infants. Pediatrics. 2001; 107:638–641. [PubMed: 11335736]
33. De Paoli AG, Davis PG, Lemyre B. Nasal continuous positive airway pressure versus nasalintermittent positive pressure ventilation for preterm neonates: a systematic review and meta-analysis. Acta Paediatr. 2003; 92:70–75. [PubMed: 12650303]
34. van der Hoeven M, Brouwer E, Blanco CE. Nasal high frequency ventilation in neonates withmoderate respiratory insufficiency. Arch Dis Child Fetal Neonatal Ed. 1998; 79:F61–63.[PubMed: 9797628]
35. Colaizy TT, Younis UM, Bell EF, Klein JM. Nasal high-frequency ventilation for prematureinfants. Acta Paediatr. 2008; 97:1518–1522. [PubMed: 18549418]
36. Hoehn T, Krause MF. Effective elimination of carbon dioxide by nasopharyngeal high-frequencyventilation. Respir Med. 2000; 94:1132–1134. [PubMed: 11127504]
37. Dumas De La Roque E, Bertrand C, Tandonnet O, et al. Nasal high frequency percussiveventilation versus nasal continuous positive airway pressure in transient tachypnea of the newborn:A pilot randomized controlled trial (NCT00556738). Pediatr Pulmonol. 2010
38. Saslow JG, Aghai ZH, Nakhla TA, et al. Work of breathing using high-flow nasal cannula inpreterm infants. J Perinatol. 2006; 26:476–480. [PubMed: 16688202]
39. Kahn DJ, Courtney SE, Steele AM, Habib RH. Unpredictability of delivered bubble nasalcontinuous positive airway pressure: role of bias flow magnitude and nares-prong air leaks. PediatrRes. 2007; 62:343–347. [PubMed: 17622958]
40. Sondergaard S, Karason S, Hanson A, et al. Direct measurement of intratracheal pressure inpediatric respiratory monitoring. Pediatr Res. 2002; 51:339–345. [PubMed: 11861940]
Null et al. Page 11
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
41. Massaro D, Massaro GD, Baras A, Hoffman EP, Clerch LB. Calorie-related rapid onset of alveolarloss, regeneration, and changes in mouse lung gene expression. Am J Physiol Lung Cell MolPhysiol. 2004; 286:L896–L906. [PubMed: 14594731]
42. Dias CM, Passaro CP, Cagido VR, et al. Effects of undernutrition on respiratory mechanics andlung parenchyma remodeling. J Appl Physiol. 2004; 97:1888–1896. [PubMed: 15194671]
43. Paugam-Burtz C, Molliex S, Lardeux B, et al. Differential effects of halothane and thiopental onsurfactant protein C messenger RNA in vivo and in vitro in rats. Anesthesiology. 2000; 93:805–810. [PubMed: 10969314]
Null et al. Page 12
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.HFNV support preparation and airway pressure tracings. Panel a: Head radiograph of apreterm lamb supported by HFNV for 3d (posterior-anterior view; L, left). Black arrowshighlight the uncuffed tube in the nasal cavity. The vertical black arrow identifies the tube’stip, which is ~5 cm along the length of the nose (~10 cm). Panel b: View of the displaypanel of the Percussionaire VDR4 ventilator, showing phasic trace of intra-tracheal pressureand numeric data for respiratory values. The intra-tracheal pressure trace has continuoushigh-frequency percussions (jagged contours), including through ‘conventional inspiration’.The convective rate is 26, PIP is 17 cmH2O, and PEEP is 8 cmH2O. High-frequency rate is~7 Hz (445 cycles/min) and mean pressure is 7 cmH2O.
Null et al. Page 13
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
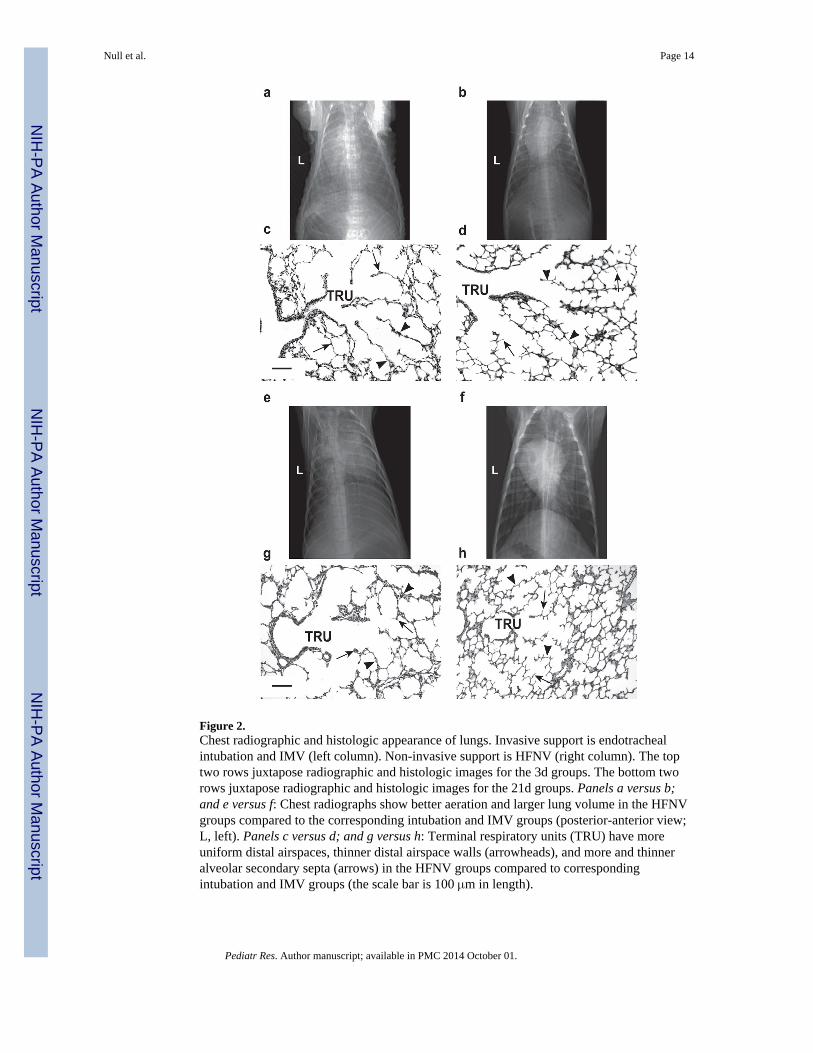
Figure 2.Chest radiographic and histologic appearance of lungs. Invasive support is endotrachealintubation and IMV (left column). Non-invasive support is HFNV (right column). The toptwo rows juxtapose radiographic and histologic images for the 3d groups. The bottom tworows juxtapose radiographic and histologic images for the 21d groups. Panels a versus b;and e versus f: Chest radiographs show better aeration and larger lung volume in the HFNVgroups compared to the corresponding intubation and IMV groups (posterior-anterior view;L, left). Panels c versus d; and g versus h: Terminal respiratory units (TRU) have moreuniform distal airspaces, thinner distal airspace walls (arrowheads), and more and thinneralveolar secondary septa (arrows) in the HFNV groups compared to correspondingintubation and IMV groups (the scale bar is 100 μm in length).
Null et al. Page 14
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
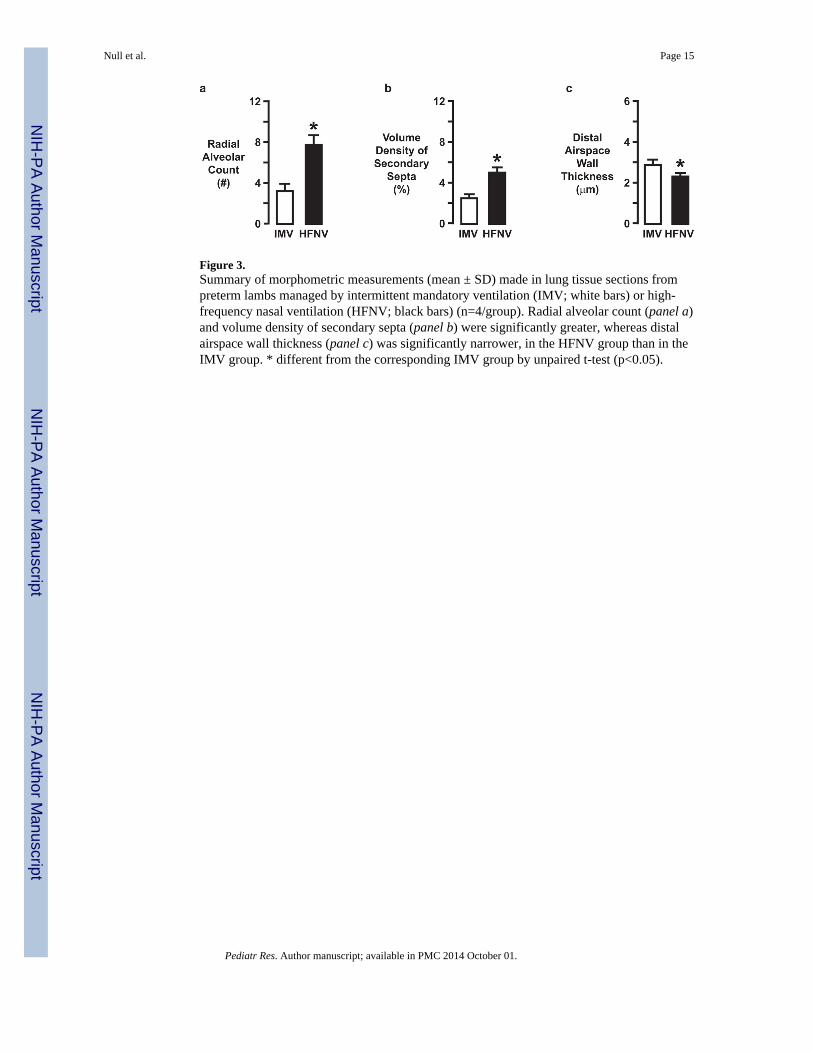
Figure 3.Summary of morphometric measurements (mean ± SD) made in lung tissue sections frompreterm lambs managed by intermittent mandatory ventilation (IMV; white bars) or high-frequency nasal ventilation (HFNV; black bars) (n=4/group). Radial alveolar count (panel a)and volume density of secondary septa (panel b) were significantly greater, whereas distalairspace wall thickness (panel c) was significantly narrower, in the HFNV group than in theIMV group. * different from the corresponding IMV group by unpaired t-test (p<0.05).
Null et al. Page 15
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Null et al. Page 16
Table 1
Demographic characteristics of preterm lambs managed by invasive or non-invasive respiratory support (mean± SD)
ParameterPreterm 3d (n=5 each) Preterm 21d (n=4 each)
Intubation and IMV HFNV Intubation and IMV HFNV
Gestational age (d) 131 ± 1 132 ± 1 132 ± 1 133 ± 1
Weight at delivery (Kg) 4.3 ± 0.4 4.7 ± 0.3 4.5 ± 0.5 4.1 ± 0.9
Weight at study end (Kg) 3.9 ± 0.4 4.6 ± 0.5* 3.9 ± 0.4 4.5 ± 0.4*
Sex 3 female / 2 male 3 female / 2 male 2 female / 2 male 2 female / 2 male
*Statistically different from IMV group by unpaired t-test, p<0.05.
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Null et al. Page 17
Table 2
Airway pressure profile at 3d of HFNV support of preterm lambs (mean ± SD; n=3)
LocationHigh Peak Inspiratory Pressure (cmH2O) Moderate Peak Inspiratory Pressure (cmH2O)
Peak Mean Peak Mean
Ventilator 27 ± 1 9 ± 1 14 ± 1 6 ± 1
Connector 27 ± 1 9 ± 1 14 ± 1 6 ± 1
Nasopharynx 10 ± 2 4 ± 2 3 ± 2 1 ± 1
Intra-tracheal 10 ± 2 4 ± 2 3 ± 2 1 ± 1
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Null et al. Page 18
Tabl
e 3
Res
pira
tory
gas
exc
hang
e pa
ram
eter
s in
pre
term
lam
bs m
anag
ed b
y in
vasi
ve o
r no
n-in
vasi
ve r
espi
rato
ry s
uppo
rt (
mea
n ±
SD
, exc
ept a
s no
ted)
Par
amet
erP
rete
rm 3
d (n
=5 e
ach)
Pre
term
21d
(n=
4 ea
ch)
Day
of
life
Intu
bati
on a
nd I
MV
HF
NV
Wee
k of
life
Intu
bati
on a
nd I
MV
HF
NV
PaO
2 (m
mH
g)1
73 ±
17
73 ±
11
176
± 1
375
± 1
2
285
± 9
81 ±
10
276
± 3
73 ±
14
373
± 8
77 ±
16
374
± 6
68 ±
3 (
n=3)
F iO
21
0.33
± 0
.03
0.32
± 0
.03
10.
42 ±
0.1
10.
30 ±
0.0
4
20.
35 ±
0.0
40.
31 ±
0.0
32
0.36
± 0
.04
0.26
± 0
.03*
30.
38 ±
0.0
40.
27 ±
0.0
3*3
0.33
± 0
.05
0.23
± 0
.02*
PaC
O2
(mm
Hg)
149
± 7
50 ±
16
146
± 7
52 ±
4
244
± 5
55 ±
82
49 ±
445
± 5
353
± 1
064
± 1
13
47 ±
842
± 6
(n=
3)
PIP
(cm
H2O
)a1
22 ±
213
± 4
*1
14 ±
118
± 3
220
± 2
13 ±
4*
215
± 2
10 ±
4
325
± 2
13 ±
2*
319
± 5
4 ±
1*
ITP
(cm
H2O
)1
22 ±
22
± 2
*1
ND
ND
220
± 2
2 ±
3*
2N
DN
D
325
± 2
2 ±
2*
3N
DN
D
Paw
(cm
H2O
)a1
11 ±
16
± 1
*1
10 ±
19
± 3
212
± 2
6 ±
1*
210
± 1
5 ±
1*
312
± 1
7 ±
1*
310
± 1
4 ±
1*
PEE
P (c
mH
2O)a
16
± 1
5 ±
11
7 ±
27
± 3
27
± 1
6 ±
22
7 ±
14
± 1
*
37
± 1
6 ±
33
7 ±
14
± 1
*
pH1
7.34
± 0
.05
7.35
± 0
.09
17.
34 ±
0.1
07.
33 ±
0.0
6
27.
43 ±
0.0
77.
37 ±
0.0
32
7.30
± 0
.04
7.43
± 0
.06*
37.
37 ±
0.1
47.
34 ±
0.0
83
7.35
± 0
.07
7.45
± 0
.04
(n=
3)
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Null et al. Page 19
Par
amet
erP
rete
rm 3
d (n
=5 e
ach)
Pre
term
21d
(n=
4 ea
ch)
Day
of
life
Intu
bati
on a
nd I
MV
HF
NV
Wee
k of
life
Intu
bati
on a
nd I
MV
HF
NV
Oxy
gena
tion
Inde
x [M
edia
n (I
QR
)]1
5.7
(0.8
)2.
3 (0
.5)†
15.
0 (2
.7)
1.9
(0.9
)†
24.
6 (1
.8)
2.2
(0.2
)†2
4.8
(0.9
)4.
0 (1
.6)†
35.
6 (1
.7)
2.5
(1.3
)†3
3.2
(0.8
)1.
4 (0
.1)†
(n=
3)
A-a
gra
dien
t (m
mH
g) [
Med
ian
(IQ
R)]
165
(14
)47
(15
)1
83 (
124)
33 (
40)
255
(24
)20
(26
)†2
70 (
48)
53 (
20)†
390
(47
)9
(11)
†3
40 (
53)
18 (
10)†
(n=
3)
PaO
2/F i
O2
ratio
[M
edia
n (I
QR
)]1
209
(24)
243
(59)
121
2 (1
02)
261
(133
)
224
3 (5
8)28
4 (5
3)2
220
( 49
)23
3 (
50)
318
4 (6
2)26
2 (8
8)†
325
6 (1
21)
294
( 23
) (n
=3)
* Stat
istic
ally
dif
fere
nt f
rom
IM
V g
roup
by
unpa
ired
t-te
st, p
<0.
05.
† Sta
tistic
ally
dif
fere
nt f
rom
IM
V g
roup
by
Man
n-W
hitn
ey U
-tes
t, p<
0.05
.
a Pres
sure
at t
he v
entil
ator
s.
ND
, not
det
erm
ined
.
IQR
, int
erqu
artil
e ra
nge.
Oxy
gena
tion
Inde
x =
(Pa
w ×
FiO
2)/P
aO2.
A-a
gra
dien
t = [
(FiO
2) ×
(64
0−47
)] −
(Pa
CO
2/0.
8) −
PaO
2; B
arom
etri
c pr
essu
re a
t Sal
t Lak
e C
ity (
~5,0
00 f
eet a
bove
sea
leve
l) is
~64
0 m
mH
g.
Pediatr Res. Author manuscript; available in PMC 2014 October 01.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Null et al. Page 20
Tabl
e 4
Feed
ing
and
seda
tion
para
met
ers
in p
rete
rm la
mbs
man
aged
by
inva
sive
or
non-
inva
sive
res
pira
tory
sup
port
(m
ean
± S
D)
Par
amet
erP
rete
rm 3
d (n
=5 e
ach)
Pre
term
21d
(n=
4 ea
ch)
Day
of
life
Intu
bati
on a
nd I
MV
HF
NV
Wee
k of
life
Intu
bati
on a
nd I
MV
HF
NV
Plas
ma
gluc
ose
(gm
/dL
)1
101
± 7
511
8 ±
46
184
± 2
095
± 1
0
296
± 3
210
9 ±
30
281
± 2
010
5 ±
7
383
± 2
593
± 1
33
84 ±
799
± 6
Ent
eral
fee
ding
(m
L/K
g/d)
a1
13 ±
99
± 7
110
6 ±
10
107
± 1
0
235
± 2
224
± 1
52
81 ±
55
149
± 5
9
351
± 3
552
± 3
13
53 ±
23
188
± 7
0*
Pent
obar
bita
l (m
g/K
g/d)
17
± 4
4 ±
41
24 ±
20
1 ±
1*
22
± 2
1 ±
12
29 ±
31
1 ±
1
34
± 2
2 ±
13
73 ±
64
1 ±
1*
Bup
reno
rphi
ne (
mcg
/Kg/
d)1
0.04
± 0
.01
0.04
± 0
.01
10.
06 ±
0.0
20.
03 ±
0.0
3*
20.
04 ±
0.0
30.
05 ±
0.0
12
0.06
± 0
.01
0.03
± 0
.03*
30.
05 ±
0.0
10.
05 ±
0.0
13
0.05
± 0
.01
0.01
± 0
.01*
a Ew
e’s
colo
stru
m (
days
of
life
1–3)
fol
low
ed b
y ew
e’s
mat
urin
g m
ilk (
day
of li
fe 4
and
ther
eaft
er).
* Stat
istic
ally
dif
fere
nt f
rom
IM
V g
roup
by
unpa
ired
t-te
st, p
<0.
05.
Pediatr Res. Author manuscript; available in PMC 2014 October 01.
Related Documents







![€¦ · Web view[Title] Successful Maintenance of Key Physiological Parameters in Preterm Lambs Treated with Ex Vivo Uterine Environment (EVE) Therapy for a Period of One Week](https://static.cupdf.com/doc/110x72/60c3f9ea7651a131d91826ef/web-view-title-successful-maintenance-of-key-physiological-parameters-in-preterm.jpg)



