Surgery: Open Access Case Report Open Access Hepatic Abscess Secondary to Sigmoid Colon Foreign Body David Aughton 1 , Sepehr Karimi 1 , Robert Leventhal 2 , Thomas Rockoff 2 , Marco Verga 3 , Eric Hyson 3 and Zhongqiu John Zhang 1 * 1 Department of Surgery, Waterbury Hospital, Waterbury, Connecticut, USA 2 Naugatuck Valley Gastroenterology Consultants LLC, USA 3 Department of Radiology, Waterbury Hospital, Waterbury, Connecticut, USA *Corresponding author: Zhongqiu John Zhang, Email: [email protected] Received: 12 June 2019; Accepted: 26 July 2019; Published: 29 July 2019 Abstract Hepatic abscesses can occur via direct or indirect spread. Direct spread occurs in the setting of biliary infection and indirect spread occurs through leakage of intraabdominal bowel contents and uptake by the portal circulation. Hematogenous spread in the setting of systemic infection is also an etiology of hepatic abscess. We present a 64 year old female who was suffering from a large abscess of the right hepatic lobe. On the initial CT scan of the abdomen and pelvis we identified a 7 x 6 x 5 cm abscess of the right hepatic lobe and a linear echogenic focus within the sigmoid colon consistent with a foreign body. After drainage of the abscess by interventional radiology, colonoscopy was performed which did not identify a foreign body in the sigmoid colon. Subsequently, CT guided localization with Indian ink marking was performed and patient was taken to the OR for robotic assisted sigmoid resection with colorectal anastomosis. The pathology report was consistent with a foreign body, and more specifically a piece of bone. In cases of hepatic abscess unidentified foreign bodies are typically under-recognized and as a result the curative treatment is delayed. The precise etiology of hepatic abscess can be elusive. Although a less likely cause, gastrointestinal foreign body should be suspected as a causative agent. Introduction Gastrointestinal foreign bodies are seen not uncommonly. These often cause no permanent damage and are simply managed with observation. It is however possible for a foreign body to cause bleeding or perforation of the gastrointestinal tract. A pyogenic hepatic abscess is a phenomenon that is commonly seen following peritonitis secondary to leakage of intraluminal bowel contents with subsequent uptake and spread to the liver via the portal circulation. It can also occur via direct spread from a biliary infection. In the setting of systemic infection there could also be potential hematogenous seeding of the liver leading to the formation of pyogenic hepatic abscesses [1,2]. Although rare, a pyogenic liver abscess to be secondary to a perforation from an ingested foreign body [3]. Case Report A 64 year old Caucasian female presented to the emergency department with a 5 day history of high grade intermittent fevers, nausea, vomiting, and right upper quadrant abdominal pain and discomfort. She described the pain as constant and aching with no alleviating or exacerbating factors. She had also experienced anorexia for four days prior to presentation. She had no significant past medical or surgical history. A screening colonoscopy within the past year was normal. On physical examination she was noted to be alert and in no acute distress. She was afebrile with a temperature of 37.2 C. Her blood Copyright © 2019 The Authors. Published by Scientific Open Access Journals LLC. pressure was 128/69 mmHg, and a pulse of 84 BPM and regular was recorded. On abdominal exam she was soft to palpation, but with mild diffuse tenderness that was maximal in the right upper and lower quadrants. Bowel sounds were normal, and there was no palpable organomegaly. She displayed no guarding or rebound tenderness. The results of her laboratory tests were as follows: white blood cell count 24.4 thousand/mm 3 , neutrophils% of 95.4%, and creatinine of 1.87 mg/dL. Liver function tests revealed: ALT of 523 IntUnit/L, AST 418 IntUnit/L, and Alkaline Phosphatase of 279 IntUnit/L. A right upper quadrant abdominal ultrasound was obtained which demonstrated a 5.4 cm heterogeneous mass in the anterior segment of the liver which contained a possible fluid level. This was thought to represent a hematoma or abscess (Figure 1). An abdominal CT with intravenous contrast was obtained without IV contrast secondary to the patient’s acute kidney injury. The Abdominal CT confirmed a large right lobe liver mass and a linear echogenic focus within the sigmoid colon thought to possibly represent a foreign body, with some mild thickening of this portion of the colon noted. The patient was empirically started on broad spectrum antibiotics (Piperacillin-Tazobactam) and the gastroenterology service was consulted. They believed the liver lesion to be an abscess and recommended drainage. The interventional radiology department was consulted and took the patient for ultrasound guided percutaneous drainage and drain placement of the pyogenic hepatic abscess, where 45 cc’s of purulent fluid was obtained and a drain left in place. Our patient was found to be bacteremia secondary to Streptococcus intermedius. Four days after initial presentation the patient’s AKI had resolved and she was sent for an interval CT scan of the abdomen and pelvis with IV contrast. This demonstrated marked interval decrease in size of a collection within the right hepatic lobe following placement of a percutaneous drainage catheter with no new collection. Seven days after initial presentation the patient was improving so it was deemed appropriate by the gastroenterology service to conduct colonoscopy to attempt to locate the suspected foreign body. The colonoscopy demonstrated evidence of diverticulosis and internal hemorrhoids but no intraluminal foreign body was found. A PICC line was placed and the patient completed a 14 day course of antibiotics secondary to her bacteremia. She ultimately improved and was discharged on hospital day 10 (Figure 2). Twelve days after discharge our patient was seen by the IR department for a catheter check. At that time the cavity was deemed small enough for the drainage catheter to be removed. She was then Figure 1: Right upper quadrant ultrasound demonstrating mass in the anterior segment of the liver with a fluid level.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Surgery: Open AccessCase Report Open Access
Hepatic Abscess Secondary to Sigmoid Colon Foreign Body
David Aughton1, Sepehr Karimi1, Robert Leventhal2, Thomas Rockoff2, Marco Verga3, Eric Hyson3 and Zhongqiu John Zhang1*1Department of Surgery, Waterbury Hospital, Waterbury, Connecticut, USA2Naugatuck Valley Gastroenterology Consultants LLC, USA3Department of Radiology, Waterbury Hospital, Waterbury, Connecticut, USA
*Corresponding author: Zhongqiu John Zhang, Email: [email protected]
Received: 12 June 2019; Accepted: 26 July 2019; Published: 29 July 2019
AbstractHepatic abscesses can occur via direct or indirect spread. Direct
spread occurs in the setting of biliary infection and indirect spread occurs through leakage of intraabdominal bowel contents and uptake by the portal circulation. Hematogenous spread in the setting of systemic infection is also an etiology of hepatic abscess.
We present a 64 year old female who was suffering from a large abscess of the right hepatic lobe. On the initial CT scan of the abdomen and pelvis we identified a 7 x 6 x 5 cm abscess of the right hepatic lobe and a linear echogenic focus within the sigmoid colon consistent with a foreign body. After drainage of the abscess by interventional radiology, colonoscopy was performed which did not identify a foreign body in the sigmoid colon. Subsequently, CT guided localization with Indian ink marking was performed and patient was taken to the OR for robotic assisted sigmoid resection with colorectal anastomosis. The pathology report was consistent with a foreign body, and more specifically a piece of bone.
In cases of hepatic abscess unidentified foreign bodies are typically under-recognized and as a result the curative treatment is delayed. The precise etiology of hepatic abscess can be elusive. Although a less likely cause, gastrointestinal foreign body should be suspected as a causative agent.
IntroductionGastrointestinal foreign bodies are seen not uncommonly. These
often cause no permanent damage and are simply managed with observation. It is however possible for a foreign body to cause bleeding or perforation of the gastrointestinal tract. A pyogenic hepatic abscess is a phenomenon that is commonly seen following peritonitis secondary to leakage of intraluminal bowel contents with subsequent uptake and spread to the liver via the portal circulation. It can also occur via direct spread from a biliary infection. In the setting of systemic infection there could also be potential hematogenous seeding of the liver leading to the formation of pyogenic hepatic abscesses [1,2]. Although rare, a pyogenic liver abscess to be secondary to a perforation from an ingested foreign body [3].
Case ReportA 64 year old Caucasian female presented to the emergency
department with a 5 day history of high grade intermittent fevers, nausea, vomiting, and right upper quadrant abdominal pain and discomfort. She described the pain as constant and aching with no alleviating or exacerbating factors. She had also experienced anorexia for four days prior to presentation. She had no significant past medical or surgical history. A screening colonoscopy within the past year was normal.
On physical examination she was noted to be alert and in no acute distress. She was afebrile with a temperature of 37.2 C. Her blood
Copyright © 2019 The Authors. Published by Scientific Open Access Journals LLC.
pressure was 128/69 mmHg, and a pulse of 84 BPM and regular was recorded. On abdominal exam she was soft to palpation, but with mild diffuse tenderness that was maximal in the right upper and lower quadrants. Bowel sounds were normal, and there was no palpable organomegaly. She displayed no guarding or rebound tenderness.
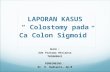
The results of her laboratory tests were as follows: white blood cell count 24.4 thousand/mm3, neutrophils% of 95.4%, and creatinine of 1.87 mg/dL. Liver function tests revealed: ALT of 523 IntUnit/L, AST 418 IntUnit/L, and Alkaline Phosphatase of 279 IntUnit/L. A right upper quadrant abdominal ultrasound was obtained which demonstrated a 5.4 cm heterogeneous mass in the anterior segment of the liver which contained a possible fluid level. This was thought to represent a hematoma or abscess (Figure 1). An abdominal CT with intravenous contrast was obtained without IV contrast secondary to the patient’s acute kidney injury. The Abdominal CT confirmed a large right lobe liver mass and a linear echogenic focus within the sigmoid colon thought to possibly represent a foreign body, with some mild thickening of this portion of the colon noted. The patient was empirically started on broad spectrum antibiotics (Piperacillin-Tazobactam) and the gastroenterology service was consulted. They believed the liver lesion to be an abscess and recommended drainage. The interventional radiology department was consulted and took the patient for ultrasound guided percutaneous drainage and drain placement of the pyogenic hepatic abscess, where 45 cc’s of purulent fluid was obtained and a drain left in place.
Our patient was found to be bacteremia secondary to Streptococcus intermedius. Four days after initial presentation the patient’s AKI had resolved and she was sent for an interval CT scan of the abdomen and pelvis with IV contrast. This demonstrated marked interval decrease in size of a collection within the right hepatic lobe following placement of a percutaneous drainage catheter with no new collection. Seven days after initial presentation the patient was improving so it was deemed appropriate by the gastroenterology service to conduct colonoscopy to attempt to locate the suspected foreign body. The colonoscopy demonstrated evidence of diverticulosis and internal hemorrhoids but no intraluminal foreign body was found. A PICC line was placed and the patient completed a 14 day course of antibiotics secondary to her bacteremia. She ultimately improved and was discharged on hospital day 10 (Figure 2).
Twelve days after discharge our patient was seen by the IR department for a catheter check. At that time the cavity was deemed small enough for the drainage catheter to be removed. She was then
Figure 1: Right upper quadrant ultrasound demonstrating mass in the anterior segment of the liver with a fluid level.

Volume 1, Issue 1Zhang et al. Surg Open Acc 2019; 1:002
Citation: Aughton D, Karimi S, Leventhal R, et al. Hepatic Abscess Secondary to Sigmoid Colon Foreign Body. Surg Open Acc 2019; 1:002.
DiscussionWhile ingested foreign bodies do occur, they normally do not
cause perforation. These occur in less than 1% of patients overall. The most common site of perforation is in the stomach and duodenum; a sigmoid perforation is quite uncommon [4]. Pyogenic liver abscesses can usually be adequately managed with antibiotics, percutaneous drainage, surgery, or a combination of these three [1].
Many times the only initial presenting symptoms of a GI perforation from a foreign body are fever, anorexia, and abdominal pain [1]. The patient is usually unaware that they could have ingested a foreign body [4]. The symptoms are often secondary to a systemic inflammatory response. It is also possible for symptoms to be delayed from the initial time of unrecognized ingestion for weeks to months.
Routine laboratory testing is non-specific but may reveal leukocytosis and mildly abnormal liver function tests. Typically diagnostic imaging workup will start with an abdominal ultrasound, but the abdominal CT appears to be the preferred diagnostic imaging study as it provides both clear pictures of the anatomy as well as high resolution, and can direct therapeutic plans. Quick diagnosis and treatment are key to a reduction in morbidity and mortality [2].
ConclusionsIn patients with pyogenic hepatic abscesses it is imperative to
perform a complete history and physical and a thorough diagnostic workup. Presenting symptoms can be vague. While they are often times secondary to peritonitis from an intraabdominal perforation, or a biliary source, a rare but still significant cause could be a foreign body leading to gastrointestinal perforation. And while it is uncommon, it should remain on the differential diagnosis especially in the setting of diagnostic testing that supports it. Although antibiotic treatment will often improve symptoms the patient will likely not completely improve until the underlying cause has been fully addressed.
References1. Huang CJ, Pitt HA, Lipsett PA, Osterman FA, Lillemoe KD, Cameron JL, et
al. Pyogenic Hepatic Abscess. Changing Trends Over 42 Years. Ann Surg. 1996; 223:600-609.
2. Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin Infect Dis. 2004; 39:1654-1659.
3. Lam YH, Wong SK, Lee DW, Lau JY, Chan AC, Yiu RY, et al. ERCP and pyogenic liver abscess. Gastrointest Endosc. 1999; 50:340.
4. Leggieri N, Marques-Vidal P, Cerwenka H, Denys A, Dorta G, Moutardier V, et al. Migrated foreign body liver abscess: illustrative case report, systematic review, and proposed diagnostic algorithm. Medicine (Baltimore). 2010; 89:85-95.
seen by the surgical team as an outpatient to discuss segmental colonic resection where the suspected foreign body was seen on initial CT. The patient agreed to undergo CT guided localization of the colonic segment containing the foreign body (Figure 3), followed by robotic assisted sigmoid colectomy with colorectal anastomosis.(Figures 4 and 5) Post-operatively the patient had a routine recovery and was discharged on post-operative day 1. Pathology revealed that the foreign body was a 3.5 cm long piece of bone within the wall of the sigmoid colon. Throughout this entire episode the patient denied any knowledge of ingesting a foreign body.
Figure 2: CT Abdomen and Pelvis without IV contrast which demonstrated a large right lobe liver mass and a linear echogenic focus within the sigmoid colon, thought to possibly represent a foreign body, with some mild thickening of this portion of the colon noted as well.
Figure 3: Image guided localization of a foreign body in the sigmoid colon prior to surgical resection.
Figure 4: Resected sigmoid colon with dye from CT guidance and foreign body between mucosal folds.
Figure 5: Foreign body (bone) next to resected sigmoid colon.
Related Documents



![Case Report Conservative Management of Large Rectosigmoid … · 2019. 7. 31. · sigmoid colon, rectosigmoid junction, and hepatic exure [ ]. In perforations that developed in distal](https://static.cupdf.com/doc/110x72/613152021ecc51586944a961/case-report-conservative-management-of-large-rectosigmoid-2019-7-31-sigmoid.jpg)



![Successful treatment of a hepatic abscess formed secondary ......the abdominal or thoracic wall, migration from the gastro-intestinal tract, or through blood.[11] Majority of hepatic](https://static.cupdf.com/doc/110x72/60a4790550fdea2994056671/successful-treatment-of-a-hepatic-abscess-formed-secondary-the-abdominal.jpg)