AIDS HAART and Sexual Behaviour: A Comparison of HAART-Initiated and HAART-Naïve Clients in The AIDS Support Organisation, Uganda --Manuscript Draft-- Manuscript Number: Full Title: HAART and Sexual Behaviour: A Comparison of HAART-Initiated and HAART-Naïve Clients in The AIDS Support Organisation, Uganda Article Type: Original paper (Epidemiology / Social) Keywords: HIV; AIDS; Sexual Behaviour; ART; HAART; Prevention Corresponding Author: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK) The AIDS Support Organisation (TASO) Uganda Limited Kampala, UGANDA Corresponding Author Secondary Information: Corresponding Author's Institution: The AIDS Support Organisation (TASO) Uganda Limited Corresponding Author's Secondary Institution: First Author: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK) First Author Secondary Information: Order of Authors: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK) Andy Beke, MBChB (Ghana), MMed (CommHealth) (Medunsa), FCPHM Order of Authors Secondary Information: Abstract: Objectives: This study sought to establish whether there is a relationship between HAART initiation and change in risky sexual behaviour using HAART-naïve clients as a control group. Design: A cohort study was retrospectively carried out. This design was appropriate both ethically and to improve the validity of the findings through use of the appropriate counter-factual. Methods: Stratified sampling with simple random sampling within strata was used to select the sample of size 340 (170 on HAART and 170 HAART-naïve; 68 males and 272 females) with HAART status as the stratifying variable. Only clients aged 15 through 40 at the start of the study were included studied. Data analysis was performed using binary logistic regression. Results: HAART was not a significant predictor of change in risky sexual behaviour (OR: 0.976; 95% CI: 0.63 to 1.511; p=0.912). Significant co-factors were: baseline risk level (adjusted OR for a 0.0001 change in baseline risk: 1.603; 95% CI: 1.181 to 2.175; p=0.003); age (adjusted OR: 1.11; 95% CI: 1.048 to 1.176; p<0.0001); being in a monogamous marriage (adjusted OR: 0.487; 95% CI: 0.263 to 0.9; p=0.022); being in a polygamous marriage (adjusted OR: 0.325; 95% CI: 0.13 to 0.811; p=0.016); and having never been in marriage (adjusted OR: 0.159; 95% CI: 0.031 to 0.833; p=0.03). Conclusion: There was no statistically significant evidence for HAART as a predictor for change in sexual behaviour among TASO clients. Prevention efforts should be concerned with aspects like age, marital status and current sexual risk levels of clients. Suggested Reviewers: Opposed Reviewers: Powered by Editorial Manager® and Preprint Manager® from Aries Systems Corporation

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

AIDS
HAART and Sexual Behaviour: A Comparison of HAART-Initiated and HAART-NaïveClients in The AIDS Support Organisation, Uganda
--Manuscript Draft--
Manuscript Number:
Full Title: HAART and Sexual Behaviour: A Comparison of HAART-Initiated and HAART-NaïveClients in The AIDS Support Organisation, Uganda
Article Type: Original paper (Epidemiology / Social)
Keywords: HIV; AIDS; Sexual Behaviour; ART; HAART; Prevention
Corresponding Author: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK)The AIDS Support Organisation (TASO) Uganda LimitedKampala, UGANDA
Corresponding Author SecondaryInformation:
Corresponding Author's Institution: The AIDS Support Organisation (TASO) Uganda Limited
Corresponding Author's SecondaryInstitution:
First Author: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK)
First Author Secondary Information:
Order of Authors: Francis Wasagami, MPH (cand.), M.Sc (MUK), B.Stat (MUK)
Andy Beke, MBChB (Ghana), MMed (CommHealth) (Medunsa), FCPHM
Order of Authors Secondary Information:
Abstract: Objectives: This study sought to establish whether there is a relationship betweenHAART initiation and change in risky sexual behaviour using HAART-naïve clients as acontrol group.Design: A cohort study was retrospectively carried out. This design was appropriateboth ethically and to improve the validity of the findings through use of the appropriatecounter-factual.Methods: Stratified sampling with simple random sampling within strata was used toselect the sample of size 340 (170 on HAART and 170 HAART-naïve; 68 males and272 females) with HAART status as the stratifying variable. Only clients aged 15through 40 at the start of the study were included studied. Data analysis wasperformed using binary logistic regression.Results: HAART was not a significant predictor of change in risky sexual behaviour(OR: 0.976; 95% CI: 0.63 to 1.511; p=0.912). Significant co-factors were: baseline risklevel (adjusted OR for a 0.0001 change in baseline risk: 1.603; 95% CI: 1.181 to 2.175;p=0.003); age (adjusted OR: 1.11; 95% CI: 1.048 to 1.176; p<0.0001); being in amonogamous marriage (adjusted OR: 0.487; 95% CI: 0.263 to 0.9; p=0.022); being ina polygamous marriage (adjusted OR: 0.325; 95% CI: 0.13 to 0.811; p=0.016); andhaving never been in marriage (adjusted OR: 0.159; 95% CI: 0.031 to 0.833; p=0.03).Conclusion: There was no statistically significant evidence for HAART as a predictor forchange in sexual behaviour among TASO clients. Prevention efforts should beconcerned with aspects like age, marital status and current sexual risk levels of clients.
Suggested Reviewers:
Opposed Reviewers:
Powered by Editorial Manager® and Preprint Manager® from Aries Systems Corporation

Abstract
Objectives: This study sought to establish whether there is a relationship
between HAART initiation and change in risky sexual behaviour using HAART-naïve
clients as a control group.
Design: A cohort study was retrospectively carried out. This design was
appropriate both ethically and to improve the validity of the findings through use of
the appropriate counterfactual.
Methods: Stratified sampling with simple random sampling within strata was
used to select the sample of size 340 (170 on HAART and 170 HAART-naïve; 68
males and 272 females) with HAART status as the stratifying variable. Only clients
aged 15 through 40 at the start of the study were included studied. Data analysis
was performed using binary logistic regression.
Results: HAART was not a significant predictor of change in risky sexual
behaviour (OR: 0.976; 95% CI: 0.63 to 1.511; p=0.912). Significant co-factors were:
baseline risk level (adjusted OR for a 0.0001 change in baseline risk: 1.603; 95% CI:
1.181 to 2.175; p=0.003); age (adjusted OR: 1.11; 95% CI: 1.048 to 1.176;
p<0.0001); being in a monogamous marriage (adjusted OR: 0.487; 95% CI: 0.263 to
0.9; p=0.022); being in a polygamous marriage (adjusted OR: 0.325; 95% CI: 0.13 to
0.811; p=0.016); and having never been in marriage (adjusted OR: 0.159; 95% CI:
0.031 to 0.833; p=0.03).
Conclusion: There was no statistically significant evidence for HAART as a
predictor for change in sexual behaviour among TASO clients. Prevention efforts
Abstract

should be concerned with aspects like age, marital status and current sexual risk
levels of clients.

1
HAART and Sexual Behaviour: A Comparison of HAART-Initiated
and HAART-Naïve Clients in The AIDS Support Organisation,
Uganda
Authors: Francis WASAGAMI 1,2
, Andy BEKE 2
Affiliation: 1. The AIDS Support Organisation (TASO) Uganda
2. School of Health Systems and Public Health, University of
Pretoria; Email: [email protected]
Correspondence to: Francis Wasagami
Email: [email protected]
This study was funded under a Master of Public Health Fellowship offered to Francis Wasagami
by the USAID through MEASURE Evaluation Project
Total number of words: Abstract: 249; Text: 3,481
Article

2
Introduction
Background
Highly Active Antiretroviral Therapy (HAART) is known to delay progression
to full-blown AIDS disease and prolong the lives of persons with HIV. This may
revive a desire for sexual relationships. This revived sexual desire in the case of
persons living with HIV (PLWH) may result in increased spread of the virus.
A number of studies with varying results have been carried out to
scientifically assess changes in sexual behaviour after commencement of HAART
[1-4]. In a prospective cohort study to assess change in sexual risky behavior
among largely heterosexual HIV-positive persons on ART for 12 months in
Mombasa, Kenya, Sarna et al. [3] found no statistically significant difference in
self-reported sexual activity at baseline (48%) and at 12 months (58%) (p=0.07).
Similarly there was no significant change in the number of sexual partners at
baseline (90% had one partner) and at 12 months (94% with one partner). The
study design did not, however, allow comparison with HIV-positive people not on
HAART to enable conclusions on whether the risk of transmission was higher or
lower for non-HAART clients. For this reason, it could not be deduced whether
HAART clients had a different level of sexual urge or engage in a higher number of
encounters than their counterparts who were not HAART.
In a study carried out in rural Uganda [2], a cohort of 926 PLWH were
started on HAART and prospectively followed for six months to assess changes in

3
their sexual behaviour. In this study, Bunnell et al. [2] found that risky sexual
behavior dropped by up to 70% (adjusted risk ratio, 0.3; 95% confidence interval
(CI), 0.2-0.7; P = 0.0017) in six months. A possible limitation of this study was that
the follow-up period of only six months was too short for clients to exhibit
objectively observable changes. Besides, no comparison group was used for
comparison of the observed change in risky sexual behaviour so as to draw more
valid conclusions. Similar to Sarna et al.’s [3] study, Bunnell et al. [2] did not
compare the study participants with other PLWH receiving all other services
except HAART, which meant that these researchers could not conclusively deduce
that the 70% reduction in sexual risky behavior was significantly due to HAART.
In a study [5] done in UThukela health district in KwaZulu-Natal, South
Africa, Peltzer et al [5] found a significant reduction in risky sexual behavior after
initiation of HAART of and following up 735 PLWH at 6 and 12 months. This result
supports that of Bunnell et al [2]. Similarly, the design of the Peltzer et al [5] study
did not allow for comparison with PLWH who were not on HAART during the study
period.
The above studies show that the effect of HAART on sexual risk behavior is
varied. While some studies have found no significant change in sexual risky
behavior after HAART initiation, others have either reported an increase or a
reduction in the risky behavior. Also notable is the fact that all these studies did not
have control groups to enable more valid conclusions on the effect of HAART on
sexual behaviour.

4
The objectives of the current study were to determine and compare levels
of risky sexual behaviour of clients on HAART with those for clients not on HAART
during the baseline period (2005 – 2007); and to determine and compare changes
in the level of risky sexual behaviour for HAART and HAART-naïve clients after 24
months of care in TASO clinics (2007 to 2009). The study hypothesized that there
is no difference between clients on HAART and those not on HAART in terms of
change in risky sexual behaviour for clients receiving HIV/AIDS services in a
health service delivery setting of TASO.
Sexual Risk Index
This study used a technique suggested by Bell and Trevino [6] to quantify
clients’ two-year sexual risk indices during and after the base period. The Bell and
Trevino [6] sexual risk index (SRI) is given by:
……………..…… (1)
where;
is the probability (risk) of person i being infected through sexual
contact with partner k,
is the HIV prevalence within the sub-population from which sexual partner k
is selected,
is the known (published) probability (risk) of HIV transmission through
sexual behaviour of type j and
is the number of sexual contacts/events with partner k and practicing
sexual behaviour of type j.

5
If client i has sexual events with n partners in a given period of time, the overall
sexual risk of is given as,
………………………. (2)
Because TASO is a routine service delivery setting whereby data are not
gathered on all variables of interest, the following assumptions were made in order
to compute the sexual risk index:
1. The number of sexual events in each recall period (three months) for
every self-reported sexual partner is 1;
2. The number of sexual partners, n, in any period of consideration is equal to
the cumulative number of sexual partners reported for that entire period
irrespective of whether the reported partner in any one 3-month period was
reported in an another 3-month period;
3. The sub-population prevalence is equal to the national prevalence and
4. We made the assumption that all reported sexual events were heterosexual
and vaginal [7] i.e. , the probability of HIV transmission through
vaginal sex, which depends on whether sex was insertive or receptive, and
whether a condom was used.
With the above-mentioned assumptions, equation (1) becomes,
………………………….. (3)

6
Because we utilised routine service data, the number of quarterly records
on sexual activity per client per year were less than the expected four for some
clients since clients are under no obligation to make contact with clinic staff at
least once every quarter. Clients with missing data for certain quarters may have
lower risk indices, which may makes them appear to be at lower risk than those
with more records. The missing data would render comparison of the clients
invalid.
There was therefore a need to prepare the study data in such a way as to
ensure validity of comparisons made. To achieve this, a mean quarterly sexual risk
index (SRI) was computed for each client for each year using the available
quarterly SRIs. The resulting mean quarterly SRI was used as the SRI for the
quarters where data were missing for the particular year. In the cases where there
was completely no data on sexual risk in a given year, the quarterly risk indices for
that year were estimated using the quarterly average of the nearest year to the left
of the affected year where quarterly risk data were available.
Since sexual activity in TASO is reported using 3-monthly recall method,
only one record per quarter of a given year was considered in the analysis in case
the client had more than one record for a given quarter. In this case the record
with the smallest response code to the question "Have you had sex in the last

7
three months? 1.Yes 2. No 3. Not applicable" was considered in the estimation of
that quarter's sexual risk index.
To adjust for variation of risk according to type of sexual partner, the
weights were attached to types of sexual partners. A weight of 1 was used for
casual partners, 0.5 for steadies, 0.1 for spouses, and 0 if the client did not have
sex with anyone; in this case n is taken as equal to 1 for computation purposes.
The estimated prevalence for the sub-population from which partner k is selected
is therefore given by . Applying this prevalence in equation (3) gives a finer
estimate for the risk posed by partner k, as shown in equation (4).
……………………………………………. (4)
Equation (4) provides an estimate of the sexual risk of infection/re-infection
by partner k in a routine health care environment and was used with equation (2)
to compute the estimated sexual risk index for each participant in the study. That
is,

8
Methods
Study Design
A cohort study was retrospectively carried out. The change in risky sexual
behaviour for clients on HAART was compared with the change in risky sexual
behaviour among clients not initiated on HAART during the study period.
Change in risky sexual behaviour was determined by comparing the sexual
risk index two years before HAART initiation and two years after HAART initiation
for clients on HAART; and two years before the reference quarter and two years
after the reference quarter for HAART-naïve clients. The reference quarter was the
quarter of HAART initiation 2007 for clients on HAART while for all HAART naïve
clients, it was taken to be 15th June 2007 since this is mid-way between January
2005 and December 2009.
Clients in both groups were those who had been registered for care at
TASO in or before 2005 and had been retained in care up to the end of 2009.
Retention in care for the purpose of this study meant receiving at least one
counselling consultation per year from 2005 to 2009 and not being reported dead.
The treatment group was the cohort of clients initiated on HAART in 2007. The
control/comparison group comprised of clients who did not start HAART until after
2009.

9
Study Population
Clients started on HAART between January and December 2007 who meet
the inclusion criteria formed the sub-population for the treatment group. For the
control group, HAART-naïve clients who meet the inclusion criteria were eligible
for the study.
Inclusion and exclusion criteria
Records for clients started on HAART between January and December
2007, who had been receiving services in TASO for at least two years at the time
of HAART initiation; and remained on HAART up to 2009, were included in the
study as the treatment group. Clients for the control group were those who had
been in care by 2005, were retained in care in TASO till 2009 and did not initiate
HAART until after 2009.
Both categories included only clients aged between 15 through 40 by
January 2005 who received at least one counselling consultation per each of the
study years (2005 to 2009) and were not reported dead during the study period.
This was to ensure that valid comparisons and conclusions are made.
Clients who did not remain alive until the end of 2009 were excluded from
the study. Also excluded were clients stopped from taking HAART, lost to follow-
up or were not retained in care during the study period.

10
Sample Size and Sample Selection
Stratified sampling methodology using HAART status as the stratifying
variable was used. For each stratum an equal number of records was selected
using simple random sampling technique.
A precision of 10% was targeted in all parameter estimations at a 95%
confidence level with a significance level of 0.05. Assuming a design effect due to
stratification of 2; 80% file recovery rate (analogous to response rate) in case of
need for data verification, and the proportion of clients at risk of sexual risky
behaviour i.e. p, of 50%, the sample size per stratum was determined to be 170.
That is, 170 records for clients on HAART and 170 records for HAART-naïve
clients were randomly selected resulting in a total of 340 clients.
Data Management and Analysis
Data analysis was done using Stata 11 [8] statistical software after random
sampling using Microsoft Excel [9]. For each client, his or her sexual risk index
was computed for the period before the cut-off quarter (base quarter) in the case
of the treatment group; and before 15th June 2007 for the control group. The
sexual risk index was also computed for the period after the base date/quarter. For
a given client the difference between the two sexual risk indexes was computed.
That is, the sexual risk index after the base date/quarter minus the sexual risk
index before the base date/quarter.

11
For each participant, a decreased or constant risk at zero level (the desired
outcome) was assigned a value of 1 while an increased or constant non-zero risk
was assigned a value of 0 (the undesired outcome). Binary logistic regression was
used to adjust for the effect of covariates such as sex, age-group and number of
counselling sessions on the relationship between HAART status and change in
sexual risk. Complex sample analysis using weights was performed with a weight
of 20 for non-HAART clients and a weight of 5 for clients on HAART.
Ethical Considerations
This study was reviewed and evaluated by the relevant bodies for ethical
and scientific merit. Approvals were obtained from the Faculty of Health Sciences
Research and Ethics Committee; TASO Institutional Review Committee; and from
the Uganda National Council for Science and Technology (UNCST).
Permission was granted by TASO to access and use their routine
healthcare data. To ensure confidentiality, no personal identifiers such as names
and registration numbers of clients were included in the report. Only the
researchers directly involved in this study had access to the data and only for the
purpose of this study.
Funding of this study was part of the Fellowship offered to Francis
Wasagami by MEASURE Evaluation. Francis has worked with TASO Uganda
since 2002. Prof Andy Beke was Francis’ supervisor and is lecturer in the School
of Health Systems and Public Health at the University of Pretoria.

12
Results
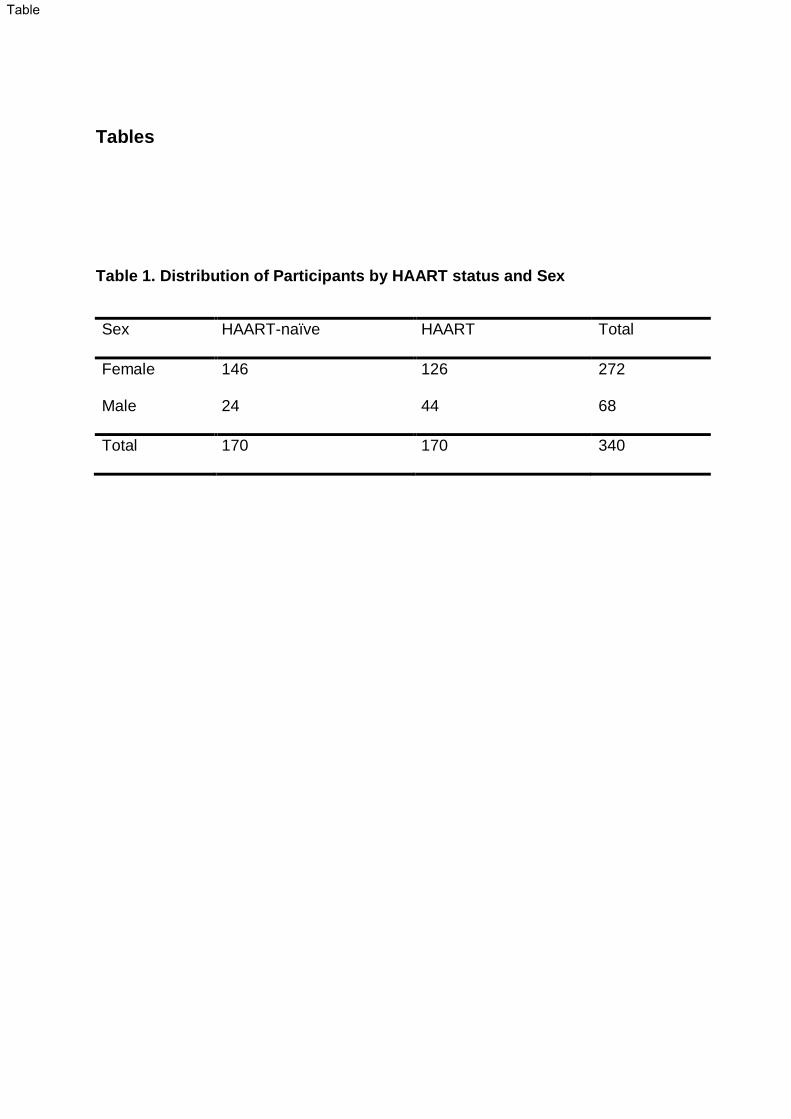
Table 1 shows the distribution of the sample by sex and HAART status. The
mean age at the beginning of study period for clients on HAART was 33.1 years
(95% CI: 32.3 to 33.8) while that of the HAART-naïve was 32.1 years (95% CI:
31.3 to 32.8). The rank-sum test showed that clients in both groups were similar in
terms of the baseline sexual risk index (p= 0.1605).
After adjusting for sex, education level, religion, TASO branch, alcohol use,
number of children alive, baseline sexual risk index, age, number of counselling
session in the study period, duration in care, occupation and residence, HAART
was not a significant predictor of change in risky sexual behaviour (OR: 0.976;
95% CI: 0.63 to 1.511; p=0.912). Instead, significant co-factors were: baseline risk
(adjusted OR for a 0.0001 change in baseline risk: 1.603; 95% CI: 1.181 to 2.175;
p=0.003); age of the client (adjusted OR: 1.11; 95% CI: 1.048 to 1.176; p<0.0001);
being in a monogamous marriage (adjusted OR: 0.487; 95% CI: 0.263 to 0.9;
p=0.022); being in a polygamous marriage (adjusted OR: 0.325; 95% CI: 0.13 to
0.811; p=0.016); and having never been in marriage (adjusted OR: 0.159; 95% CI:
0.031 to 0.833; p=0.03).
A rank-sum test did not reveal a significant difference in two-year risk at
baseline for the two study groups (p= 0.295). A similar test did not show a
significant difference between the two groups in terms of the two-year sexual risk
index at the end of the study period (p= 0.88)

13
The estimated percentage of HAART initiated clients that experienced a
reduced risk or constant zero-risk sexual behaviour was 60% (95% CI: 52.59% to
67.41%) while that for HAART-naïve clients was 61% (95% CI: 53.19% to
67.98%).
The test for equality of proportions of clients that experienced a reduced
risky sexual behaviour among the treatment and comparison groups showed that
the two proportions were not statistically different at 5% level of significance (p=
0.9117).

14
Discussion
The findings of this study are consistent with those of Sarna et al. [3] who
found no statistically significant difference in self-reported sexual activity at
baseline (48%) and at 12 months (58%) (p=0.07) in their Mombasa, Kenya study
despite the design of Sarna et al ’s [3] study (prospective cohort with no control
group) being different from the current study’s design (retrospective cohort with a
control group). Similarity of Sarna et al’s [3] findings may therefore be purely
coincidental.
The findings of the current study however contrast with those of Bunnell et
al. [2] who attributed to HAART initiation a 70% (adjusted risk ratio, 0.3; 95%
confidence interval (CI), 0.2-0.7; p= 0.0017) drop in risky sexual behaviour after
six months of the initiation in their rural Uganda study. The lack of a HAART naïve
control group in the Bunnell et al. [2] study might have led to their contrasting
conclusion.
Findings from the current study also contrast with those established by a
study involving men who have sex with men conducted in Amsterdam [4] where
HAART initiation was associated with increased risky sexual behavior among the
participants. The lack of a HAART naïve control group in this Amsterdam study [4],
like in the Bunnell et al. [2] study, might also have led to this finding that is different
from that established by our study.

15
Another study with findings that contrasted with the results of this study was
that carried out by Peltzer et al. [5] in Uthukela health district in KwaZulu-Natal,
South Africa, which showed a significant reduction in risky sexual behavior after
starting HAART. In this study, Peltzer et al. [5] followed up 735 PLWH at 6 and 12
months after initiation on HAART but they did not do the same for HAART naïve
PLWH. This might have rendered their attribution of the reduction in risky sexual
behavior to HAART less reliable.
In a meta-analysis of 12 controlled trials in the USA, Crepaz et al.[10] found
a significant effect of behavioral interventions on change in sexual behaviour of
PLWH. For those studies that established a change in risky sexual behavior
[2,4,5], the observed change may therefore be attributed to the
behavioural/psychosocial sub-components and other aspects of the respective
HIV/AIDS programmes; as well as to personal and environmental attributes of the
PLWH rather than to HAART initiation.
Emerging Predictors of Change in Risky Sexual Behaviour in TASO
The factors that emerged as statistically significant for change in risky
sexual behaviour were: baseline risk (adjusted OR for a 0.0001 change in baseline
risk: 1.603; 95% CI: 1.181 to 2.175; p=0.003); age of the client (adjusted OR: 1.11;
95% CI: 1.048 to 1.176; p<0.0001); being in a monogamous marriage (adjusted
OR: 0.487; 95% CI: 0.263 to 0.9; p=0.022); being in a polygamous marriage
(adjusted OR: 0.325; 95% CI: 0.13 to 0.811; p=0.016); and having never been in
marriage (adjusted OR: 0.159; 95% CI: 0.031 to 0.833; p=0.03).

16
This study established that baseline sexual risk index (SRI) was positively
associated with reduced risky sexual behaviour. In other words, clients with higher
levels of risky sexual behaviour at baseline were more likely to experience a
reduction in risky sexual behaviour than those with lower baseline sexual risk. It
appears that the psychosocial (counselling) component of TASO HIV/AIDS
programme had a profound effect of causing a reduction in risky sexual behaviour
among the more-at-sexual-risk than among the less-at-sexual-risk clients. This
may have resulted from preventive counselling efforts being directed more towards
clients thought to be more-at-risk of risky sexual behaviour, leaving those
perceived to be less-at-risk to deteriorate in terms of risky sexual behaviour since
counselling has been shown to have an effect on sexual behaviour of HIV positive
persons [11].
Another factor that emerged as significant for reduced risky sexual
behaviour was the age of the client. Age was positively related to reduced risky
sexual behaviour, that is, the older the clients the more likely they were to
experience reduced risky sexual behaviour behaviour. This may be attributed to
reduction in sexual desire with age [12] which may as such put older clients at a
lesser risky sexual behaviour than young clients.
The study also found a statistically significant relationship between being
married and change in sexual risky behaviour. Both the clients in monogamous
and polygamous marriages were less likely to reduce their sexual risky levels
(respective adjusted OR of 0.487 and 0.325). This can be attributed to married

17
people’s high likelihood to engage in sex acts quite often in any given quarter; and
also to a possibility that the married were engaging in risky extra-marital affairs.
This result is consistent with the reports which showed increased risk of HIV in
marriages in Uganda [13].
Finally, the study found that clients who reported that they had never been
married at the time of registration into care in TASO were less likely to reduce their
risky sexual behaviour (adjusted OR: 0.159). This may be attributed to the
possibility of engaging in risky sexual acts during their search for possible
marriage partners and also involvement in sexual activities for pleasure.
In conclusion, this study established that there is no statistically significant
evidence for HAART as being associated with change in sexual behaviour. The
results from the study showed that changes in sexual behaviour after HAART
initiation observed in other studies may have been caused by different
programmatic and environmental factors rather than being on HAART.

18
Acknowledgements
Thanks TASO Management for allowing this study to be conducted in the
organisation. Also acknowledged is the support from TASO staffs who enabled
access to the data and the clients’ files. To Prof Girdler-Brown and Dr. Stephanie
Mullen, thanks for all your technical and statistical guidance.
The study was funded under a Fellowship from the USAID-funded
MEASURE Evaluation Project

19
References
1. Seeley J, Russell S, Khana K, Ezati E, King R, Bunnell R. Sex after ART:
sexual partnerships established by HIV-infected persons taking anti-
retroviral therapy in Eastern Uganda. Cult Health Sex. Oct 2009; 11(7):703-
16. Accessed on 7th March 2011 at
http://www.ncbi.nlm.nih.gov/pubmed/19544115.
2. Bunnell R, Ekwaru JP, Solberg P, Wamai N, Bikaako-Kajura W, Were W.
Changes in sexual behavior and risk of HIV transmission after antiretroviral
therapy and prevention interventions in rural Uganda. AIDS. 2nd January
2006; 20(1):85-92. Accessed on 7th March 2011 at
http://journals.lww.com/aidsonline/Fulltext/2006/01020/Changes_in_sexual_
behavior_and_risk_of_HIV.12.aspx
3. Sarna A, Chersich M, Okal J, Luchters SM, Mandaliya KN, Rutenberg N,
Temmerman M. Changes in sexual risk taking with antiretroviral treatment:
influence of context and gender norms in Mombasa, Kenya. Cult Health
Sex. 2009 Nov; 11(8):783-97.
4. Dukers NHTM, Goudsmit J, de Wit JBF, Prins M, WeverlingGJ, Coutinho
RA. Sexual risk behaviour relates to the virological and immunological
improvements during highly active antiretroviral therapy in HIV-1 infection.
AIDS. 16 February 2001; 15 (3):369-378.

20
5. Peltzer K, Ramlagan S. Safer sexual behaviours after 1 year of
antiretroviral treatment in KwaZulu-Natal, South Africa: a prospective cohort
study. Sex Health. 2010 June; 7(2):135-41.
6. Bell DC, Trevino RA. Modeling HIV Risk. JAIDS. 1 November 1999; 22
(3):280. Accessed on 22 May 2011 at
http://journals.lww.com/jaids/Fulltext/1999/11010/Modeling_HIV_Risk.10.as
px.
7. Uganda Ministry of Health. Uganda HIV Prevention Response and Modes
of Transmission Analysis, March 2009.
8. StataCorp. Stata Statistical Software: Release 11. 2009. College Station,
TX: StataCorp LP.
9. Microsoft Corporation Inc. USA. Microsoft Excel 2007.
10. Crepaz N, Lyles CM, Wolitski RJ, PassinWF, Rama SM, HerbstJH, et al.
Do Prevention Interventions Reduce HIV Risk Behaviors Among People
Living With HIV? A Meta-Analytic Review of Controlled Trials. AIDS. 2006;
20(2):143-157. Accessed on 8th March 2011 at
http://www.medscape.com/viewarticle/521053.
11. Richardson JL, Milam J, McCutchan A, Stoyanoff S, Bolan R, Weiss J,
Kemper C et al. Effect of brief safer-sex counseling by medical providers to
HIV-1 seropositive patients: a multi-clinic assessment. AIDS. 21 May 2004;
18 (8):1179-1186.
12. Delamater JD, Sill M. Sexual desire in later life. Journal of Sex Research.
2005; 42 (2) : 138 – 149.

21
13. Namutebi J. New Vision Newspaper, Uganda. June 13, 2007. Newspaper
article accessed on 18th June 2012 at
http://aidscarewatch.blogspot.com/2007/06/uganda-married-women-at-
higher-risk-of.html.
Tables
Table 1. Distribution of Participants by HAART status and Sex
Sex HAART-naïve HAART Total
Female 146 126 272
Male 24 44 68
Total 170 170 340
Table

Francis WasagamiClick here to download LWW Copyright Transfer and Disclosure Form: copyrightTransferWASAGAMI.pdf

Andy BekeClick here to download LWW Copyright Transfer and Disclosure Form: copyrightTransfer_Andy Beke.pdf

AIDS: Author’s paper submission checklist
Title of paper: ► HAART and Sexual Behaviour: A Comparison of HAART-Initiated
and HAART-Naïve Clients in The AIDS Support Organisation, Uganda
Names of
authors:
► Francis Wasagami; Andy Beke
AUTHORS SHOULD PLEASE ENSURE THAT ALL APPROPRIATE
INFORMATION (EG. CONFLICT OF INTEREST STATEMENTS) ARE
ALSO INCLUDED IN THE TEXT OF THE ARTICLE.
1. DUPLICATE PUBLICATION is not acceptable and includes papers, or letters to
the Editor reporting the same data previously published in any journal. Abstracts of
papers presented at meetings and published in the proceedings of such meetings do
not constitute duplicate publication, but should be disclosed by including a note at the
beginning of the paper, i.e.. "Data presented previously at (state meeting) and
published as abstract in (give reference)". Have you published these data previously?
► No
2. CONFLICT OF INTEREST include financial support from the biomedical
industry or other commercial sources in the form of research grants, bench fees,
consultancy or lecture fees, travelling expenses, payment of registration fees,
consultancy appointments, posts held in the biomedical industry or equipment
manufacturers, stock holdings in the company, free supply of drugs and the like.
These should be stated in relation to each author. Has any of the authors any conflict
of interest? Please state details.
► This study was funded through a Fellowship offered to Francis Wasagami by the USAID
through MEASURE Evaluation Project. Francis Wasagami has worked with The AIDS
Support Organisation (TASO). Prof. Andy Beke was an academic supervisor to Francis
3. CONSENT Please note that patient's, or normal control’s, written consent is
needed not only for full papers, but also for case reports. The written consent needs to
include not only agreement to undergo treatment, or participate in an experiment or an
randomised control trial, but also agreement for anonymised data to be published in a
scientific journal. Was patient’s consent obtained and in what form?
► Because this study used secondary data, no consent was obtained from patients. However all necessary ethical approvals were obtained and the principles strictly adhered to in the
handling and use of these data.
4. ETHICS All studies need to be approved by the local Ethical Committees. Was
your study? Please provide the approval from your local Ethical Committees for any
animal experimentation or human subject studies.
► This study was approved by: University of Pretoria's Faculty of Health Sciences Research and Ethics Committee, The AIDS Support Organisation's Institutional Review Committee and
Uganda National Council for Science and Technology
Author's Checklist

5. AUTHOR’S CONTRIBUTIONS AND APPROVAL OF TEXT Please state
briefly how each of the authors contributed to the study, to data analysis and to the
writing of your paper. Subject to your agreement, we will print this information, if the
paper is accepted for publication. In addition, please confirm that all the authors have
read and approved the text as submitted to AIDS. Justify individual’s contributions
when the author list exceeds 10.
► Francis developed the research protocol, prepared and analysed the data; and wrote the report. Prof Andy Beke conceptualised and finalised the protocol, revised statistical methods,
and revised all stages of drafting of the manuscript
6. STATISTICAL ANALYSIS Kindly please let me know who performed the
statistical analysis of you data.
► The data analysis was done by Francis Wasagami with some guidance from Prof Brendan
Girdler-Brown from School of Health Systems and Public Health, University of Pretoria
7. ARTICLE LENGTH Please acknowledge that you have kept within the word and insert
limits for your submission by ticking the relevant boxes below, and that you have indicated
the word count on the title page of your article
Article length
√ Original papers, 3500 words of text excluding references with no more than five inserts
(figures/tables)
Concise communications, 1800 words of text excluding references with maximum of two
inserts (figures/tables)
Research Letters, 1000 words excluding summary with no more than one insert (figure/table)
Correspondence, 750 words excluding references with no more than one insert (figure/table)
Title page
√ Title no more than 120 characters
Running head, no more than 40 characters
Justification of the number of contributors greater than 10 included in this document
Abstract page
√ Abstract no more than 250 words
√ 5–7 keywords listed
Word count
√ Word count of text (excluding references) included on title page

8. CLINICAL TRIALS AND BEHAVIOURAL EVALUATIONS: Authors reporting
results of randomized controlled trials should include with their submission a complete
checklist from the CONSORT statement, see JAMA 1996; 227:637-639 or
http://www.consort-statement.org. For behavioural and public health evaluations involving
non-randomized designs, authors should include with their submission a complete checklist
from the TREND statement, see Am J Public Health 2004; 94:361-366 or www.trend-
statement.org .
REGISTRATION OF CLINICAL TRIALS: As a condition for publication of a clinical
trial in AIDS, registration of the trial in a public registry is required. Registration of a trial must be at or before the enrollment of participants. The editors of AIDS also do not advocate
one particular registry but require that the registry utilized meet the criteria set out in the
statement of policy of the ICMJE (www.ijcme.org).
Please state that your article includes a clinical trial and that the conditions of submission
above have been met.
► Not Applicable
Other information for the Editor:
►
Name of person completing this form:
► Francis Wasagami
Date: ►26/06/2012
Related Documents











