Guidance on programmatic management of latent TB infection: applicability for TB control in migrants Marieke J. van der Werf, Netta Beer, Sake J. de Vlas, Teymur Noori, Marije Vonk Noordegraaf-Schouten Liverpool, 27 October 2016

Guidance on programmatic management of latent TB infection: applicability for TB control in migrants
Jan 12, 2017
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Guidance on programmatic management of latent TB infection: applicability for TB control in migrants
Marieke J. van der Werf, Netta Beer, Sake J. de Vlas, Teymur Noori, Marije Vonk Noordegraaf-SchoutenLiverpool, 27 October 2016

BackgroundTB notifications by country, EU/EEA, 201458 008 TB cases in 29 EU/EEA countries12.8 per 100 000 population (range 2.5–79.7)
2
Not reporting
20 to 49 per 100 000
10 to 19 per 100 000
5 to 9 per 100 000< 5 per 100 000
≥ 50 per 100 000

BackgroundTowards TB elimination in EU/EEA With current mean annual change in the TB notification rate (-6%), the EU/EEA will achieve TB elimination by 2092.
To reach elimination by 2050, TB rates need to decline by 12% annually.
3
2010
2016
2022
2028
2034
2040
2046
2052
2058
2064
2070
2076
2082
2088
1
10
100
1000
Decline needed to reach TB elimination by 2050Current mean annual decline
TB n
otifi
catio
ns p
er 1
milli
on
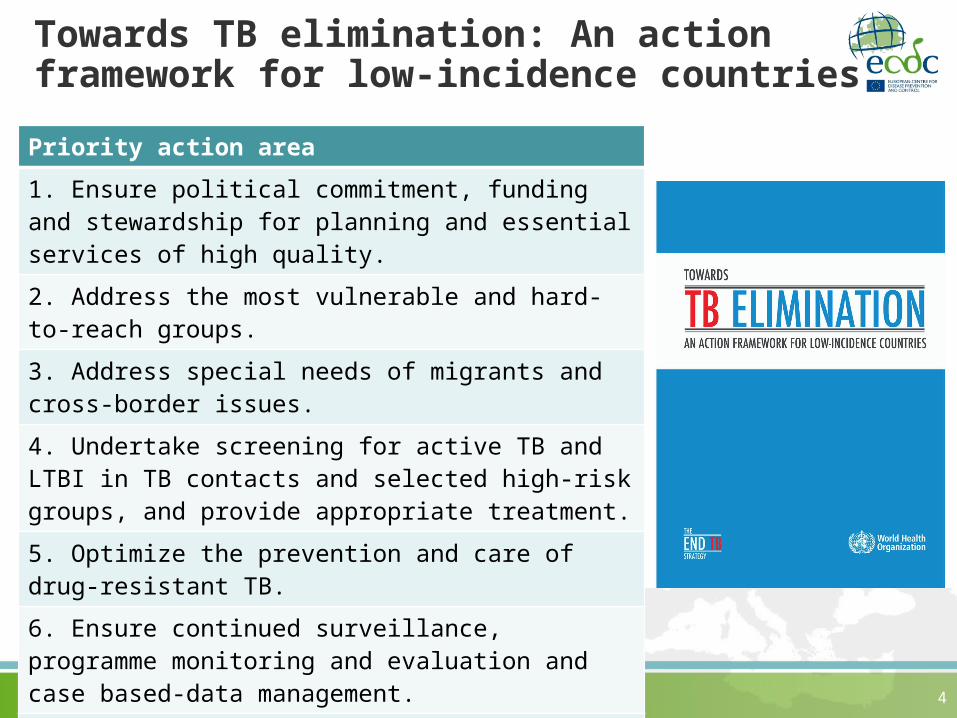
Towards TB elimination: An action framework for low-incidence countriesPriority action area1. Ensure political commitment, funding and stewardship for planning and essential services of high quality.2. Address the most vulnerable and hard-to-reach groups.3. Address special needs of migrants and cross-border issues.4. Undertake screening for active TB and LTBI in TB contacts and selected high-risk groups, and provide appropriate treatment.5. Optimize the prevention and care of drug-resistant TB.6. Ensure continued surveillance, programme monitoring and evaluation and case based-data management.7. Invest in research and new tools.8. Support global TB prevention, care and control. 4
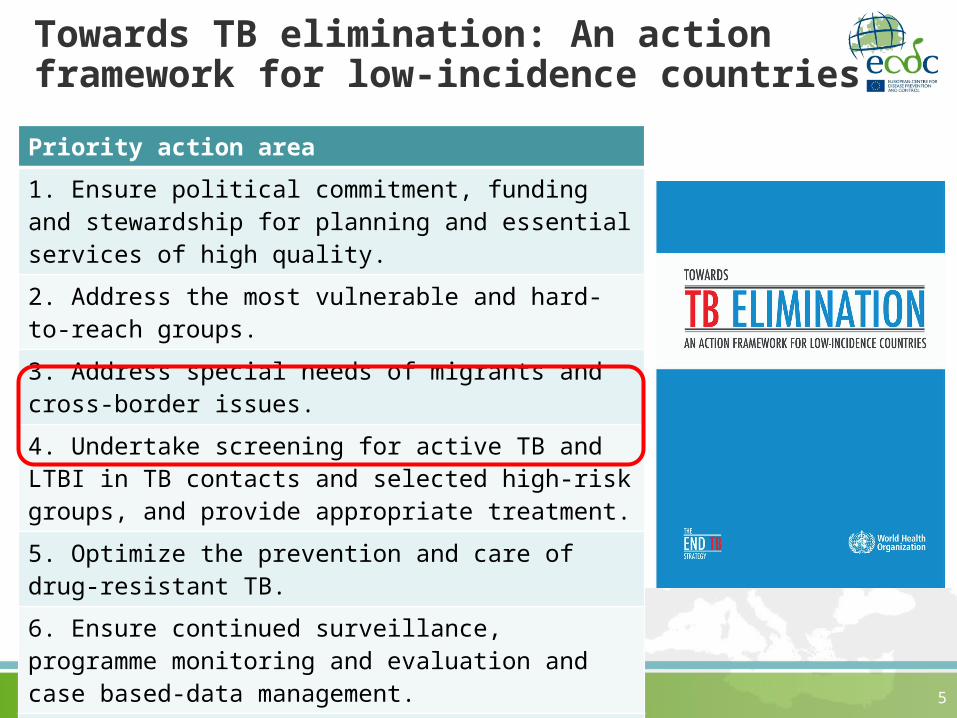
Towards TB elimination: An action framework for low-incidence countriesPriority action area1. Ensure political commitment, funding and stewardship for planning and essential services of high quality.2. Address the most vulnerable and hard-to-reach groups.3. Address special needs of migrants and cross-border issues.4. Undertake screening for active TB and LTBI in TB contacts and selected high-risk groups, and provide appropriate treatment.5. Optimize the prevention and care of drug-resistant TB.6. Ensure continued surveillance, programme monitoring and evaluation and case based-data management.7. Invest in research and new tools.8. Support global TB prevention, care and control. 5
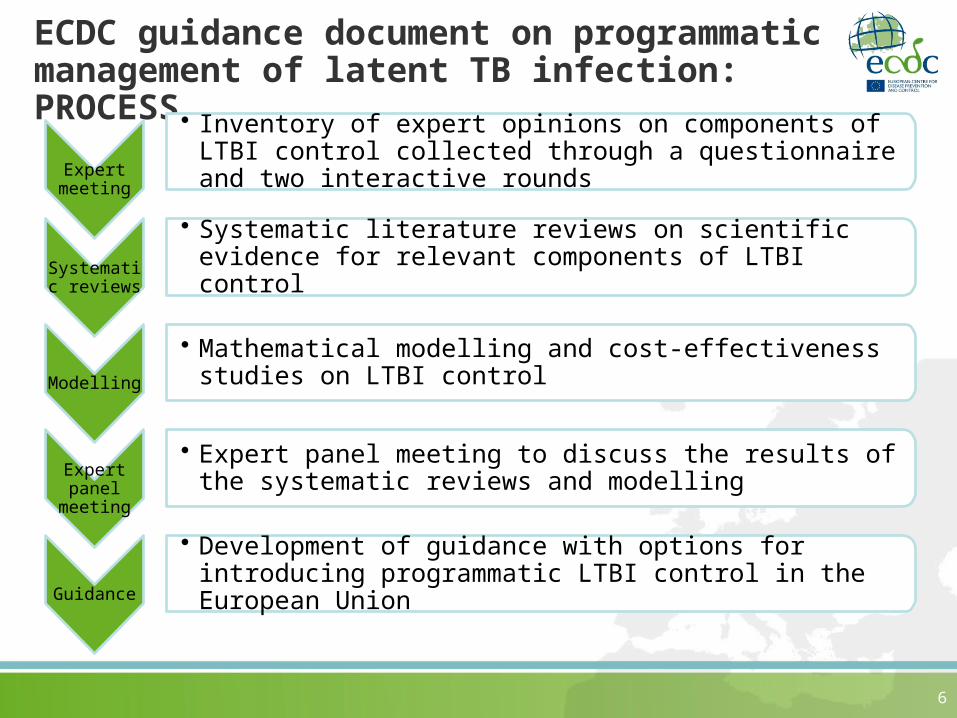
ECDC guidance document on programmatic management of latent TB infection: PROCESS
Expert meeting
• Inventory of expert opinions on components of LTBI control collected through a questionnaire and two interactive rounds
Systematic reviews
• Systematic literature reviews on scientific evidence for relevant components of LTBI control
Modelling• Mathematical modelling and cost-effectiveness studies
on LTBI control
Expert panel
meeting
• Expert panel meeting to discuss the results of the systematic reviews and modelling
Guidance• Development of guidance with options for introducing
programmatic LTBI control in the European Union
6

Step 1: Expert meeting
Components identified for guidance • diagnostic tests for LTBI• preventive treatment regimens• risk group specific interventions• combining LTBI control with other health
programmes
7Sandgren et al. Euro Surveill. 2016 Aug 25;21(34).

Step 2: Systematic literature reviews
8
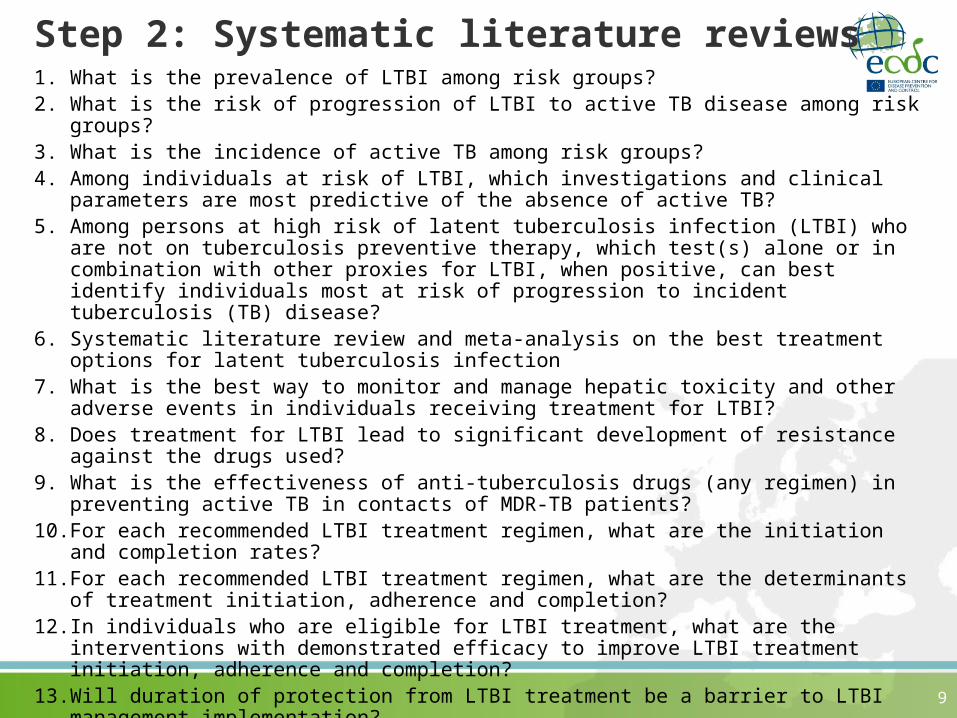
Step 2: Systematic literature reviews1. What is the prevalence of LTBI among risk groups?2. What is the risk of progression of LTBI to active TB disease among risk groups?3. What is the incidence of active TB among risk groups?4. Among individuals at risk of LTBI, which investigations and clinical parameters are
most predictive of the absence of active TB?5. Among persons at high risk of latent tuberculosis infection (LTBI) who are not on
tuberculosis preventive therapy, which test(s) alone or in combination with other proxies for LTBI, when positive, can best identify individuals most at risk of progression to incident tuberculosis (TB) disease?
6. Systematic literature review and meta-analysis on the best treatment options for latent tuberculosis infection
7. What is the best way to monitor and manage hepatic toxicity and other adverse events in individuals receiving treatment for LTBI?
8. Does treatment for LTBI lead to significant development of resistance against the drugs used?
9. What is the effectiveness of anti-tuberculosis drugs (any regimen) in preventing active TB in contacts of MDR-TB patients?
10. For each recommended LTBI treatment regimen, what are the initiation and completion rates?
11. For each recommended LTBI treatment regimen, what are the determinants of treatment initiation, adherence and completion?
12. In individuals who are eligible for LTBI treatment, what are the interventions with demonstrated efficacy to improve LTBI treatment initiation, adherence and completion?
13. Will duration of protection from LTBI treatment be a barrier to LTBI management implementation?
14. What is the cost-effectiveness of LTBI management interventions? 9
Step 2: Systematic literature reviews1. What is the prevalence of LTBI among risk groups?2. What is the risk of progression of LTBI to active TB disease among risk groups?3. What is the incidence of active TB among risk groups?4. Among individuals at risk of LTBI, which investigations and clinical parameters are
most predictive of the absence of active TB?5. Among persons at high risk of latent tuberculosis infection (LTBI) who are
not on tuberculosis preventive therapy, which test(s) alone or in combination with other proxies for LTBI, when positive, can best identify individuals most at risk of progression to incident tuberculosis (TB) disease?
6. Systematic literature review and meta-analysis on the best treatment options for latent tuberculosis infection
7. What is the best way to monitor and manage hepatic toxicity and other adverse events in individuals receiving treatment for LTBI?
8. Does treatment for LTBI lead to significant development of resistance against the drugs used?
9. What is the effectiveness of anti-tuberculosis drugs (any regimen) in preventing active TB in contacts of MDR-TB patients?
10. For each recommended LTBI treatment regimen, what are the initiation and completion rates?
11. For each recommended LTBI treatment regimen, what are the determinants of treatment initiation, adherence and completion?
12. In individuals who are eligible for LTBI treatment, what are the interventions with demonstrated efficacy to improve LTBI treatment initiation, adherence and completion?
13. Will duration of protection from LTBI treatment be a barrier to LTBI management implementation?
14. What is the cost-effectiveness of LTBI management interventions?10
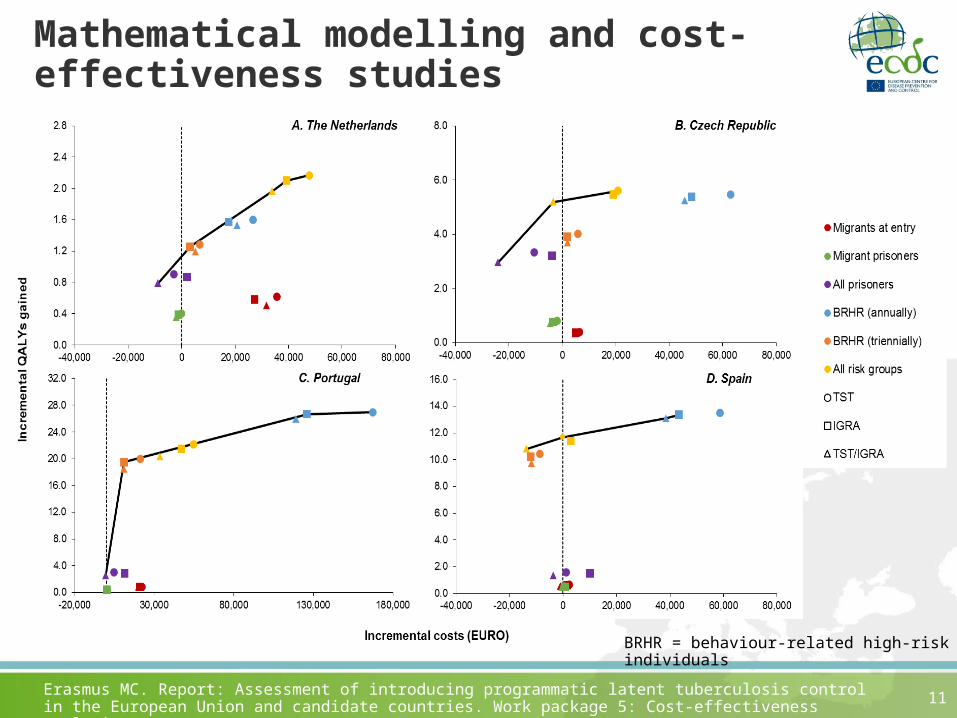
Mathematical modelling and cost-effectiveness studies
11Erasmus MC. Report: Assessment of introducing programmatic latent tuberculosis control in the European Union and candidate countries. Work package 5: Cost-effectiveness analysis
BRHR = behaviour-related high-risk individuals
ECDC guidance document on programmatic management of latent TB infection: PROCESS
Expert meeting
• Inventory of expert opinions on components of LTBI control collected through a questionnaire and two interactive rounds
Systematic reviews
• Systematic literature reviews on scientific evidence for relevant components of LTBI control
Modelling• Mathematical modelling and cost-effectiveness studies
on LTBI control
Expert panel
meeting
• Expert panel meeting to discuss the results of the systematic reviews and modelling
Guidance• Development of guidance with options for introducing
programmatic LTBI control in the European Union
12
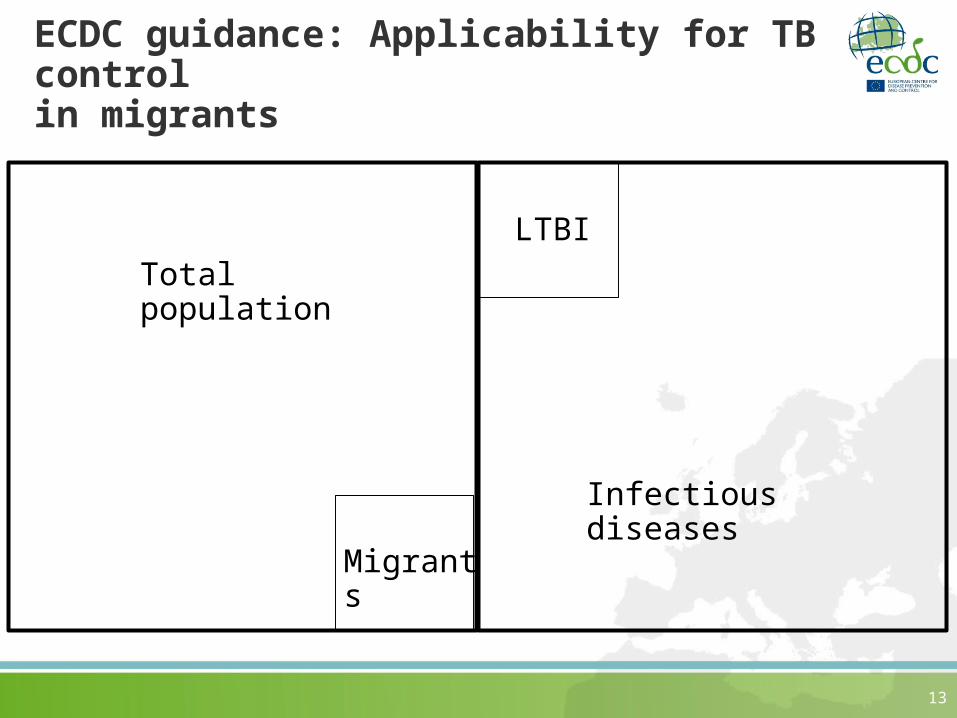
ECDC guidance: Applicability for TB control in migrants
13
Total population
Infectious diseases
LTBI
Migrants

ECDC guidance: Applicability for TB control in migrants
14
Total population
Infectious diseases
LTBI
Migrants
Guidance on
programmatic
management of LTBI
ECDC guidance: Applicability for TB control in migrants
15
Total population
Infectious diseases
LTBI
Migrants
Guidance on prevention
of infectio
us diseases
among newly arrived
migrants in the EU/EEA

Acknowledgements
Erasmus MCJan A.C. HontelezJoost VanhommerigSuzanne VerverRui Cai Rinke HoekstraJan Hendrik RichardusSake J. de Vlas
ECDCAndreas SandgrenNetta BeerTeymur Noori
16
Pallas, Health research and consultancy B.V.
Marije Vonk Noordegraaf-Schouten
Femke van KesselAnke StuurmanAnouk Oordt-Speets
Radbout UMCRob Baltussen
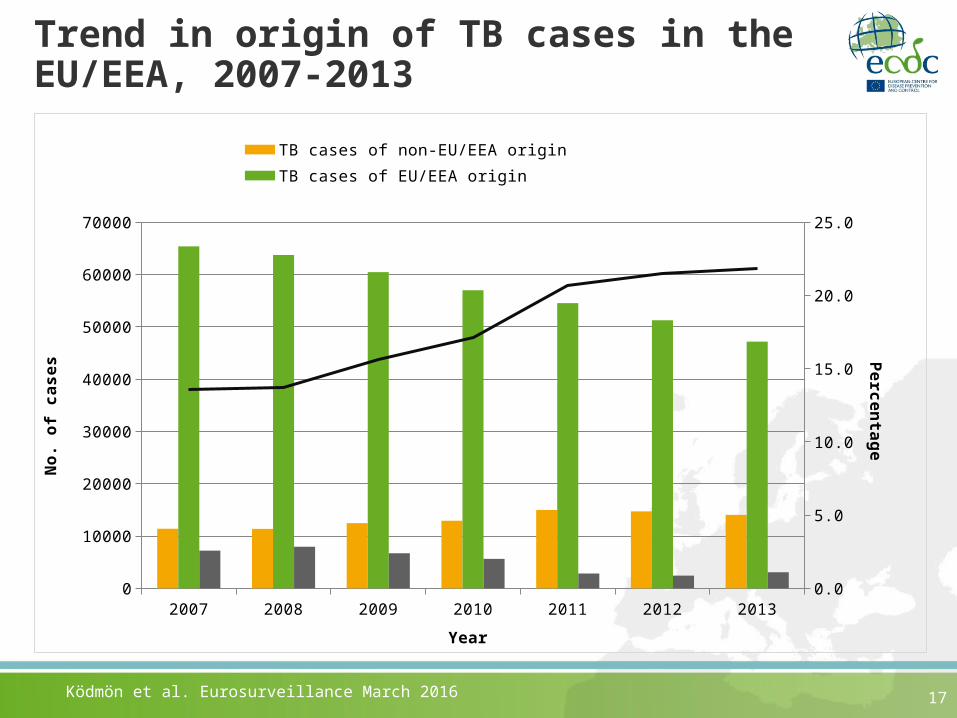
Trend in origin of TB cases in the EU/EEA, 2007-2013
17
2007 2008 2009 2010 2011 2012 20130
10000
20000
30000
40000
50000
60000
70000
0.0
5.0
10.0
15.0
20.0
25.0
TB cases of non-EU/EEA origin TB cases of EU/EEA originTB cases of unknown/not specified origin % of non-EU/EEA TB cases among all TB
Year
No.
of
case
s Percentage
Ködmön et al. Eurosurveillance March 2016
Conflict of interest disclosureX I have no, real or perceived, direct or indirect conflicts of interest that relate to this presentation. I have the following, real or perceived direct or indirect conflicts of interest that relate to
this presentation:
Affiliation / financial interest Nature of conflict / commercial company name
Tobacco-industry and tobacco corporate affiliate related conflict of interest
Grants/research support (to myself, my institution or department):
Honoraria or consultation fees:
Participation in a company sponsored bureau:
Stock shareholder:
Spouse/partner:
Other support or other potential conflict of interest:
This event is accredited for CME credits by EBAP and speakers are required to disclose their potential conflict of interest going back 3 years prior to this presentation. The intent of this disclosure is not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial products or services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgment. It remains for audience members to determine whether the speaker’s interests or relationships may influence the presentation. Drug or device advertisement is strictly forbidden.
Related Documents











