Major Articles Grading system for retinal hemorrhages in abusive head trauma: Clinical description and reliability study Gaurav Bhardwaj, BMed, PhD, a Mark B. Jacobs, MD, FRANZCO, a,b Frank J. Martin, FRANZCO, FRACS, b,c,d Craig Donaldson, FRANZCO, FRACS, b,c Kieran T. Moran, MBBCh, FRACP, a,e Ute Vollmer-Conna, BSc (Psych), PhD, f Paul Mitchell, MD, PhD, g and Minas T. Coroneo, MD, FRACS a,b PURPOSE There is currently no universally accepted grading system for describing retinal hemor- rhages (RH) in abusive head trauma (AHT). The purpose of this study was to devise and evaluate a novel grading system and descriptive nomenclature for RH in AHT for clinical and research purposes. METHODS A traumatic hemorrhagic retinopathy (THR) grading system was developed for assessing and quantitatively analyzing retinal findings in abusive head trauma. The criteria for the THR grade included the extent, spread, and morphology of RH. Extent was classified as region 1 (posterior pole) or region 2 (peripheral). Spread, based on number of retinal hem- orrhages, was classified as mild (10 or fewer RH), moderate (more than 10 RH) and severe (more than half of involved regions covered by RH). Morphology was classified by its intra- retinal or extraretinal involvement. Two independent graders calculated the THR grade from RetCam images of 38 eyes of 19 patients \ 3 years of age with retinal hemorrhages associated with head injury. Grading was performed on two separate occasions. Intra- and interobserver reliability was assessed with Spearman correlation coefficient (r) and intraclass correlation coefficient (ICC). RESULTS There was a high level of intraobserver agreement across both assessments (97% agreement [Spearman r 5 0.997; P \ 0.0001] and 100% agreement [Spearman r 5 1.0; P \ 0.0000]). Intraclass correlation (ICC, 0.995; 95% CI, 0.991-0.997; P \ 0.0001) confirmed a very high level of agreement overall. CONCLUSIONS The traumatic hemorrhagic retinopathy grading system demonstrated excellent intraob- server and interobserver reliability. The nomenclature is easily understood and may be use- ful in medical records and medicolegal reports. ( J AAPOS 2014;18:523-528) R etinal hemorrhages in infants and young children with abusive head trauma (AHT) are frequently too numerous to count, may involve a large pro- portion of the retina, and are sometimes seen in association with other clinical features, such as retinoschisis and retinal folds. This variety of findings can be difficult to document comprehensively and accurately. Prior to the RetCam (Massie Research Laboratories, Pleasanton, CA), it was challenging to obtain widefield images of the infant fundus. This made it difficult to objectively compare findings be- tween patients and even in each eye of the same patient. The use of photographic documentation has made it easier for judges, juries, and legal professionals to comprehend retinal hemorrhages (RH). Nevertheless, the need still ex- ists for a classification system and nomenclature for medi- colegal purposes and clinical studies. Although a classification system has been developed for the grading of retinopathy of prematurity (ROP) 1-3 and retinoblastoma, 4 no such system exists for the grading of hemorrhagic retinopathy from AHT. This is surprising given the importance of accurate assessment and documentation in See accompanying editorial on page 521. Author affiliations: a Faculty of Medicine, University of New South Wales (UNSW), Sydney NSW, Australia; b Department of Ophthalmology, Prince of Wales and Sydney Children’s Hospital, Randwick, NSW; c Department of Ophthalmology, The Children’s Hospital at Westmead, Westmead, NSW; d Faculty of Medicine, University of Sydney, NSW; e Child Protection Unit, Sydney Children’s Hospital, Randwick, NSW; f School of Psychiatry, Faculty of Medicine, University of New South Wales (UNSW), Randwick, NSW; g Centre for Vision Research, Westmead Millennium Institute, University of Sydney, NSW Study supported by funding from the Sydney Children’s Hospital Foundation, Randwick, NSW (MTC, GB, MBJ). The funding organization had no role in the design or conduct of this research. Financial disclosures: Frank Martin receives reimbursement of expenses to attend American Academy of Ophthalmology board meetings. Paul Mitchell is a consultant to Bayer, Novartis and Allergan, and receives payment for lectures, and reimbursement of travel expenses from these companies. Institution where study conducted: Sydney Children’s Hospital, Randwick, NSW, 2031 and the Children’s Hospital at Westmead, NSW, 2145, Australia. Presented in part at the Annual Congress of the Royal Australian and New Zealand College of Ophthalmologists (RANZCO), Adelaide, NSW, Australia, November 22, 2010. Submitted June 1, 2014. Revision accepted September 2, 2014. Correspondence: Dr Gaurav Bhardwaj, BMed, PhD, Department of Ophthalmology, 2nd floor, South Wing, Edmund Blacket Building, Prince of Wales Hospital, Randwick, NSW, 2031 (email: [email protected]). Crown Copyright Ó 2014 Published by American Association for Pediatric Ophthalmology and Strabismus. All rights reserved. 1091-8531/$36.00 http://dx.doi.org/10.1016/j.jaapos.2014.09.006 Journal of AAPOS 523

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Major Articles
Grading system for retinal hemorrhages in abusivehead trauma: Clinical description and reliability studyGaurav Bhardwaj, BMed, PhD,a Mark B. Jacobs, MD, FRANZCO,a,b
Frank J. Martin, FRANZCO, FRACS,b,c,d Craig Donaldson, FRANZCO, FRACS,b,c
Kieran T. Moran, MBBCh, FRACP,a,e Ute Vollmer-Conna, BSc (Psych), PhD,f
Paul Mitchell, MD, PhD,g and Minas T. Coroneo, MD, FRACSa,b
PURPOSE There is currently no universally accepted grading system for describing retinal hemor-
See accompanying editorial on p
Author affiliations: aFaculty of MNSW, Australia; bDepartment oHospital, Randwick, NSW; cDepWestmead, Westmead, NSW; dFProtection Unit, Sydney ChildreFaculty of Medicine, Universityfor Vision Research, Westmead MStudy supported by funding fro
NSW (MTC, GB,MBJ). The futhis research.Financial disclosures: Frank M
American Academy of OphthalmBayer, Novartis and Allergan, atravel expenses from these compaInstitution where study conduc
and the Children’s Hospital at WPresented in part at theAnnual
of Ophthalmologists (RANZCO),Submitted June 1, 2014.Revision accepted September 2Correspondence: Dr Gaurav B
floor, South Wing, Edmund BlaNSW, 2031 (email: gauravb23Crown Copyright � 2014 Pu
Ophthalmology and Strabismus.1091-8531/$36.00http://dx.doi.org/10.1016/j.ja
Journal of AAPOS
rhages (RH) in abusive head trauma (AHT). The purpose of this study was to devise andevaluate a novel grading system and descriptive nomenclature for RH in AHT for clinicaland research purposes.
METHODS A traumatic hemorrhagic retinopathy (THR) grading system was developed for assessing
and quantitatively analyzing retinal findings in abusive head trauma. The criteria for theTHR grade included the extent, spread, and morphology of RH. Extent was classified asregion 1 (posterior pole) or region 2 (peripheral). Spread, based on number of retinal hem-orrhages, was classified as mild (10 or fewer RH), moderate (more than 10 RH) and severe(more than half of involved regions covered by RH).Morphology was classified by its intra-retinal or extraretinal involvement. Two independent graders calculated the THR gradefrom RetCam images of 38 eyes of 19 patients\3 years of age with retinal hemorrhagesassociated with head injury. Grading was performed on two separate occasions. Intra-and interobserver reliability was assessed with Spearman correlation coefficient (r) andintraclass correlation coefficient (ICC).RESULTS There was a high level of intraobserver agreement across both assessments (97%
agreement [Spearman r 5 0.997; P\ 0.0001] and 100% agreement [Spearman r 5 1.0;P \ 0.0000]). Intraclass correlation (ICC, 0.995; 95% CI, 0.991-0.997; P \ 0.0001)confirmed a very high level of agreement overall.CONCLUSIONS The traumatic hemorrhagic retinopathy grading system demonstrated excellent intraob-
server and interobserver reliability. The nomenclature is easily understood andmay be use-ful in medical records and medicolegal reports. ( J AAPOS 2014;18:523-528)age 521.
edicine, University of New SouthWales (UNSW), Sydneyf Ophthalmology, Prince of Wales and Sydney Children’sartment of Ophthalmology, The Children’s Hospital ataculty of Medicine, University of Sydney, NSW; eChildn’s Hospital, Randwick, NSW; fSchool of Psychiatry,of New South Wales (UNSW), Randwick, NSW; gCentreillennium Institute, University of Sydney, NSW
m the Sydney Children’s Hospital Foundation, Randwick,nding organization had no role in the design or conduct of
artin receives reimbursement of expenses to attendology board meetings. Paul Mitchell is a consultant tond receives payment for lectures, and reimbursement ofnies.ted: Sydney Children’s Hospital, Randwick, NSW, 2031estmead, NSW, 2145, Australia.Congress of theRoyalAustralian andNewZealandCollegeAdelaide, NSW, Australia, November 22, 2010.
, 2014.hardwaj, BMed, PhD, Department of Ophthalmology, 2ndcket Building, Prince of Wales Hospital, Randwick,@gmail.com).blished by American Association for PediatricAll rights reserved.
apos.2014.09.006
Retinal hemorrhages in infants and young childrenwith abusive head trauma (AHT) are frequentlytoo numerous to count, may involve a large pro-
portion of the retina, and are sometimes seen in associationwith other clinical features, such as retinoschisis and retinalfolds. This variety of findings can be difficult to documentcomprehensively and accurately. Prior to the RetCam(Massie Research Laboratories, Pleasanton, CA), it waschallenging to obtain widefield images of the infant fundus.This made it difficult to objectively compare findings be-tween patients and even in each eye of the same patient.The use of photographic documentation has made it easierfor judges, juries, and legal professionals to comprehendretinal hemorrhages (RH). Nevertheless, the need still ex-ists for a classification system and nomenclature for medi-colegal purposes and clinical studies.
Although a classification systemhas been developed for thegrading of retinopathy of prematurity (ROP)1-3 andretinoblastoma,4 no such system exists for the grading ofhemorrhagic retinopathy fromAHT.This is surprising giventhe importance of accurate assessment and documentation in
523

FIG 1. Hemorrhagic retinopathy grading regions. Region 1 comprisesa circle centered at the fovea with a radius of twice the disk to foveadistance (r). Region 2 is the remaining retina outside region 1. Hem-orrhages at the border are considered within region 1.
524 Bhardwaj et al Volume 18 Number 6 / December 2014
these cases from a medicolegal perspective. The descriptionof a retinopathy as “severe” or “extensive” is not sufficientlydetailed and can encompass a wide range of findings.
In contrast to the grading systems for ROP or retino-blastoma, in which management decisions are based onthe grade, the main purpose of the grading system forRH in AHT is to describe the severity and distribution ofRH. Once a system is established and utilized in clinicalstudies, the grade may be able to predict the likelihood ofAHT or even neurological outcome.
The purpose of this study was to devise and clinicallyevaluate a grading system and descriptive nomenclaturefor RH in AHT. The current grading system was devel-oped alongside a clinical study examining the extent ofretinal findings in infants with conditions previously re-ported to cause retinal hemorrhages. The grading systemwas intended to be useful in both clinical and medicolegalsettings as a tool for accurately documenting the extent ofhemorrhagic retinopathy in infants with head injury.
Methods and Material
Description of Traumatic Hemorrhagic RetinopathyGrading System
Each eye is evaluated separately according to the followingcategories:
(E) Extent
Extent is described according to two retinal regions, asdesignated in Figure 1: region 1, the posterior pole; and re-gion 2, the periphery.
1. Region 1 is defined by a circle centered at the fovea witha radius5 2� disk to fovea distance (fovea to the centerof the disk), that is, ROP zone I but centered at the fovearather than the disk. If any part of a retinal hemorrhage(RH) lies at the junction of region 1 and 2, it is countedas being in region 1.
2. Region 2 comprises the retinal area outside region 1.
(S) Spread
Spread is described according to the following strict termi-nology:
A. Mild—10 or fewer RH present.B. Moderate—more than 10 RH present but\50% of the
retina (or region 1 if no region 2 involvement) involved.C. Severe—involvement of .50% of retina (or region 1 if
no region 2 involvement) with RH.
(M) Morphology
Morphology describes the depth of retinal involvement:
i. Intraretinal hemorrhages only (within the retinal layers,excluding sub–inner limiting membrane [ILM]).
ii. Extraretinal involvement, for example, preretinal, sub-ILM, subretinal, or vitreous hemorrhage.
The determination of the traumatic hemorrhagic reti-nopathy (THR) grade is made according to Table 1. Agrade 3 hemorrhagic retinopathy can involve either region1, 2, or both, along with retinal folds or retinoschisis.Grade 2 is any hemorrhagic retinopathy extending to re-gion 2, without the presence of retinal folds or retinoschi-sis. Grade 1, logically, is any hemorrhagic retinopathylimited to region 1.
The second tier of our grading system describes thenumber and proportion of involved retina. Subdivision Ais given where 10 or fewer distinct hemorrhages are pre-sent. Where more than 10 hemorrhages are present butless than half the retina (or region 1 in grade 1) is involvedwith hemorrhage, a subdivision B is given. Where morethan half the retina (or region 1 in grade 1) is involved inhemorrhage, a subdivision C is given.
The third tier of the THR grade describes the depth ofretinal involvement. Involvement of only the intraretinallayers is given a subdivision of i; extraretinal involvement,such as subretinal, preretinal, or vitreous hemorrhage isgiven a subdivision of ii.
The nomenclature is written as grade (1, 2, or 3; A, B, orC; i or ii) and is accompanied by a short description of ex-traretinal involvement and other lesions, that is, preretinal,subretinal, or vitreous hemorrhage, papilledema, macularretinoschisis or fold, and so forth. An algorithm simplifyingthe THRG is provided in Figure 5.
Clinical Evaluation of Traumatic HemorrhagicRetinopathy Grading System
Multicenter ethics approval was obtained from the Chil-dren’s Hospital at Westmead Ethics Committee. All pro-cedures were carried out in accordance with the tenets of
Journal of AAPOS

FIG 2. Grade 1 traumatic hemorrhagic retinopathy. A, Grade 1Ai (openarrow shows intraretinal peripapillary nerve fiber layer hemorrhage).B, Grade 1Bii (intraretinal, preretinal). C, Grade 1Cii (intraretinal, pre-retinal). The solid arrow demonstrates deep intraretinal hemorrhageand open arrow shows large preretinal hemorrhage.
FIG 3. Grade 2 traumatic hemorrhagic retinopathy. A, Grade 2AI. B,Grade 2Bii (intraretinal, preretinal). C, grade 2Cii (intraretinal, prereti-nal, subretinal).
Volume 18 Number 6 / December 2014 Bhardwaj et al 525
the Declaration of Helsinki. The grading system was eval-uated by two independent graders: a pediatric ophthalmol-ogist and a general ophthalmologist. The graders wereprovided with the algorithm (Figure 5) to familiarizethem with the determination of THR grades. The graderswere then shown RetCam photographs of 38 eyes of 19 pa-tients from our study cohort of infants with retinal hemor-rhages associated with head injuries, both accidental andabusive. The photographs were taken as part of a prospec-
Journal of AAPOS
tive, consecutive, comparative case series at the two tertiarypediatric hospitals in Sydney, NSW, Australia.
Five standard photographs of each eye were shown—posterior pole, superior, inferior, nasal and temporalretina. These photographs had regions 1 and 2
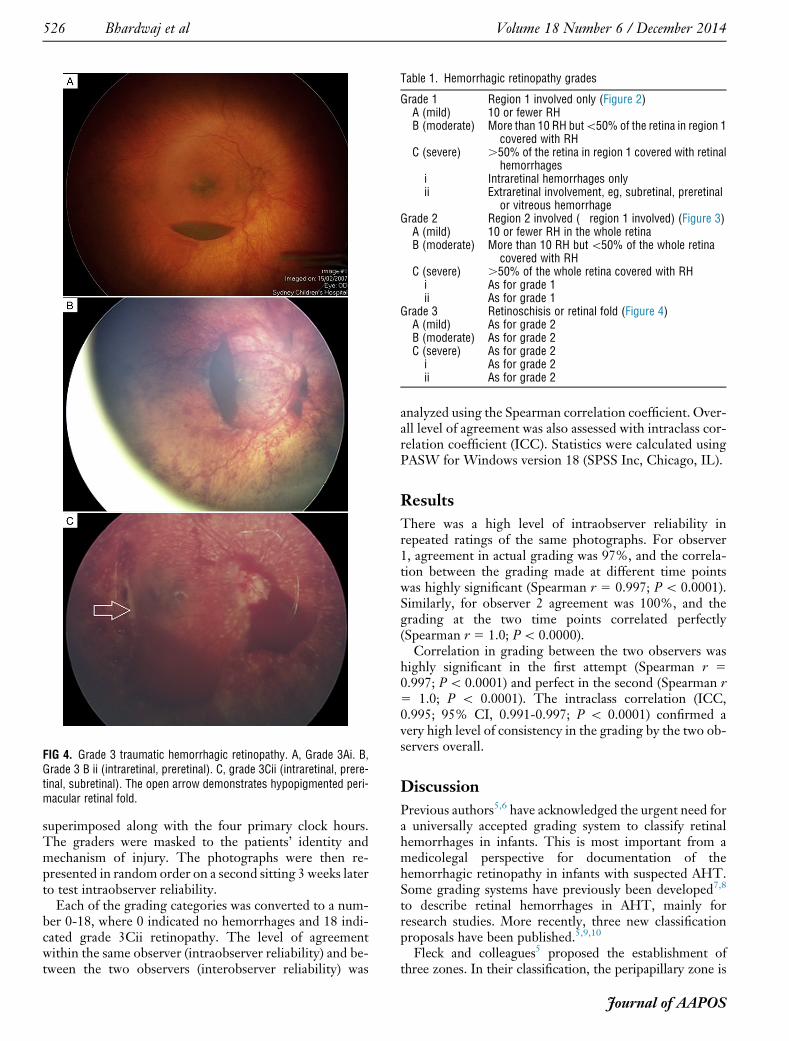
FIG 4. Grade 3 traumatic hemorrhagic retinopathy. A, Grade 3Ai. B,Grade 3 B ii (intraretinal, preretinal). C, grade 3Cii (intraretinal, prere-tinal, subretinal). The open arrow demonstrates hypopigmented peri-macular retinal fold.
Table 1. Hemorrhagic retinopathy grades
Grade 1 Region 1 involved only (Figure 2)A (mild) 10 or fewer RHB (moderate) More than 10 RH but\50% of the retina in region 1
covered with RHC (severe) .50% of the retina in region 1 covered with retinal
hemorrhagesi Intraretinal hemorrhages onlyii Extraretinal involvement, eg, subretinal, preretinal
or vitreous hemorrhageGrade 2 Region 2 involved (�region 1 involved) (Figure 3)A (mild) 10 or fewer RH in the whole retinaB (moderate) More than 10 RH but\50% of the whole retina
covered with RHC (severe) .50% of the whole retina covered with RHi As for grade 1ii As for grade 1
Grade 3 Retinoschisis or retinal fold (Figure 4)A (mild) As for grade 2B (moderate) As for grade 2C (severe) As for grade 2i As for grade 2ii As for grade 2
526 Bhardwaj et al Volume 18 Number 6 / December 2014
superimposed along with the four primary clock hours.The graders were masked to the patients’ identity andmechanism of injury. The photographs were then re-presented in random order on a second sitting 3 weeks laterto test intraobserver reliability.
Each of the grading categories was converted to a num-ber 0-18, where 0 indicated no hemorrhages and 18 indi-cated grade 3Cii retinopathy. The level of agreementwithin the same observer (intraobserver reliability) and be-tween the two observers (interobserver reliability) was
analyzed using the Spearman correlation coefficient. Over-all level of agreement was also assessed with intraclass cor-relation coefficient (ICC). Statistics were calculated usingPASW for Windows version 18 (SPSS Inc, Chicago, IL).
Results
There was a high level of intraobserver reliability inrepeated ratings of the same photographs. For observer1, agreement in actual grading was 97%, and the correla-tion between the grading made at different time pointswas highly significant (Spearman r 5 0.997; P\ 0.0001).Similarly, for observer 2 agreement was 100%, and thegrading at the two time points correlated perfectly(Spearman r 5 1.0; P\ 0.0000).
Correlation in grading between the two observers washighly significant in the first attempt (Spearman r 50.997; P\ 0.0001) and perfect in the second (Spearman r5 1.0; P \ 0.0001). The intraclass correlation (ICC,0.995; 95% CI, 0.991-0.997; P \ 0.0001) confirmed avery high level of consistency in the grading by the two ob-servers overall.
Discussion
Previous authors5,6 have acknowledged the urgent need fora universally accepted grading system to classify retinalhemorrhages in infants. This is most important from amedicolegal perspective for documentation of thehemorrhagic retinopathy in infants with suspected AHT.Some grading systems have previously been developed7,8
to describe retinal hemorrhages in AHT, mainly forresearch studies. More recently, three new classificationproposals have been published.5,9,10
Fleck and colleagues5 proposed the establishment ofthree zones. In their classification, the peripapillary zone is
Journal of AAPOS

GRADE 3 <10 RH Grade 3A Intraretinal only Grade 3Ai
Other layers involved Grade 3Aii >10 RH Grade 3B Intraretinal only Grade 3Bi
Other layers involved Grade 3Bii >50% retina Grade 3C Intraretinal only Grade 3Ci
Other layers involved Grade 3Cii
GRADE 2 <10 RH Grade 2A Intraretinal only Grade 2Ai
Other layers involved Grade 2Aii >10 RH Grade 2B Intraretinal only Grade 2Bi
Other layers involved Grade 2Bii >50% retina Grade 2C Intraretinal only Grade 2Ci
Other layers involved Grade 2Cii
GRADE 1 <10 RH Grade 1A Intraretinal only Grade 1Ai
Other layers involved Grade 1Aii >10 RH Grade 1B Intraretinal only Grade 1Bi
Other layers involved Grade 1Bii >50% Region 1 Grade 1C Intraretinal only Grade 1Ci
Other layers involved Grade 1Cii
GRADE 0
Y
Y
N
Retinoschisis or folds present?
No retinoschisis or folds BUT region 2
involved
No retinoschisis or folds AND only
region 1 involved
No RH
Y
Y
N
N
FIG 5. Algorithm for determination of traumatic hemorrhagic retinopathy grade.
Volume 18 Number 6 / December 2014 Bhardwaj et al 527
3 disk diameters, centered on the disk. The posterior polezone is a circle with a radius of 4 disk diameters, with thecenter of the circle on a line bisecting the retinal arcadesand the optic disk, and with the nasal edge of the zonetangential to the peripapillary zone. The peripheral zone isclassified as the region outside the peripapillary zone.Tandon and colleagues9 also devised an RH description
tool, defining the peripapillary area (zone A) as 1 disk diam-eter around thedisk.Theposterior pole (zoneB) is defined asa circle centered at the fovea which was tangential to thenasal edge of zone A. The midperiphery (zone C) is the re-gion outside zoneB up until the ampullae of the vortex veins.The peripheral retina (zone D) is classified as the area ante-rior to the vortex ampullae. The actual details of the tool todescribe the findings are not included in the article.We feel that these previously proposed classification of
zones5,9 is overly complex, especially because theirdesignation is arbitrary. It may be difficult to apply thesezones in practice for a clinician examining a child andmay only be useful when examining RetCamphotographs. Furthermore, the delineation betweenmidperiphery and periphery in the proposal by Tandonand colleagues9 may be difficult in practice due to poor vis-ibility of the vortex ampullae in many eyes.Ngand colleagues10 calculated the interobserver and intra-
observer reliability of a proforma used to record RH. Theyproposed only two zones, based on the ICROP zones andcombined zone 2 and 3 as a peripheral zone. Although these
Journal of AAPOS
previous studies5,9,10 describe different ways of dividing theretina to classify findings, none of the studies actuallydefine a clinically useful classification system to describe thefindings. They appear to be focused more on calculatinginterobserver reliability between clinicians at assessing theretina rather than a grading system for describing RH.
Although it seems convenient to use the preexistingzones designed for ROP in defining the areas of retinalinvolvement in AHT, there is no clinical or scientific justi-fication to do so. Retinal pathology in AHT is usuallycentered at the macula. The fovea is also the anatomicalcenter of the retina, meaning that two zones centered atthe fovea are concentric and the peripheral region is uni-form in width. Although the fovea can sometimes beobscured by hemorrhage, it can usually be approximatedwith reasonable certainty. The fovea was thus chosen asthe center of region 1 in our grading system, similar tothe descriptions by Fleck and colleagues5 and Tandonand colleagues.9
We believe that our system, classifying region 1 as a cir-cle centered at the fovea, with a radius twice the disk–foveadistance, allows the clinician to rapidly assess the extent ofretinal involvement.We also preferred the terminology re-gion to zone to avoid any confusion with ICROP zones.
In terms of delineating among grades 1, 2, and 3 in oursystem, our priority was to create a memorable and logicalsequence. Grade 3 was chosen as the highest grade becauseretinal folds and retinoschisis are currently the most

528 Bhardwaj et al Volume 18 Number 6 / December 2014
specific retinal lesions associated with AHT. In terms ofthe distinction between subdivisions A and B, we felt thatcounting more than 10 retinal hemorrhages could becomearduous and inaccurate on a practical level. This is espe-cially so in an awake child with whom there may a limitedopportunity for examination. Also the delineation betweenB and C can be made with a quick glance by determiningwhether the fundus appears mostly red (hemorrhage) ormostly normal.
There are some limitations to this novel THR gradingsystem. As mentioned, obscuration of the fovea maymake accurate delineation of the regions difficult. Thismay be compounded if the disk is also obscured. This israre, however, and the regions can usually be well approx-imated without difficulty. Second, certain grades may bequite unlikely to occur clinically, such as grade 1C (i andii), because it is unusual for hemorrhages to be confluentto the point of occupying more than 50% of region 1 andnot having any region 2 involvement. Also, it is uncommonto find retinal folds or schisis when the hemorrhagic reti-nopathy is limited to region 1. We do not believe this is atrue weakness, because we considered it important to beable to assign a grade to any pattern of hemorrhage, regard-less of how unlikely.
Various factors affect the assessment of the traumatichemorrhagic retinopathy grade. First, a dilated examina-tion is mandatory because much of region 2 is not visiblethrough a constricted pupil. The timing of the examinationfollowing the injury must be documented. If examination isdelayed, the grade is likely to be an underestimation due torapid resolution of intraretinal hemorrhages. Dense vitre-ous hemorrhage may preclude accurate grading.
In consultation with numerous pediatric ophthalmolo-gists at the Royal Australian and New Zealand College ofOphthalmologists (RANZCO) annual congress (Adelaide,November 2010), simplicity and practicality were empha-sized as being important factors in the clinical acceptanceof a grading system.We have developed a simple, clinicallyrelevant, and reliable grading system that takes intoaccount the extent, morphology, and severity of RH.These
factors are not only important in a grading scale but alsorelevant in the diagnosis and outcome of patients withAHT. Further studies may shed light on whether there isa correlation between the THR grade and neurologicalprognosis.
Literature Search
PubMed was searched (1970 to present) using thefollowing terms: grading system AND retinal hemorrhage.The same terms were also searched in MEDLINE(1950-present), EMBASE (1947-present), and Evidence-Based Medicine Reviews simultaneously via OVID. Arti-cles cited in the reference lists of other articles were alsosearched.
References
1. Committee for the Classification of Retinopathy of Prematurity. Aninternational classification of retinopathy of prematurity. Arch Oph-thalmol 1984;102:1130-34.
2. ICROPCommittee for Classification of Late Stages ROPAn interna-tional classification of retinopathy of prematurity, II: the classificationof retinal detachment. Arch Ophthalmol 1987;105:906-12.
3. An International Committee for the Classification of Retinopathy ofPrematurity. The international classification of retinopathy of prema-turity revisited. Arch Ophthalmol 2005;123:991-9.
4. Murphree AL. Intraocular retinoblastoma: the case for a new groupclassification. Ophthalmol Clin North Am 2005;18:41-53.
5. Fleck BW, Tandon A, Jones PA, Mulvihill AO, Minns RA. An inter-rater reliability study of a new “zonal” classification for reporting thelocation of retinal haemorrhages in childhood for clinical, legal andresearch purposes. Br J Ophthalmol 2010;94:886-90.
6. Taylor DSI. Educational paper—retinal haemorrhages in abusivehead trauma in children. Eur J Pediatr 2011;1-3.
7. Vinchon M, Defoort-Dhellemmes S, Desurmont M, Dhellemmes P.Accidental and nonaccidental head injuries in infants: a prospectivestudy. J Neurosurg 2005;102:380-84.
8. Wilkinson WS, Han DP, Rappley MD, Owings CL. Retinal hemor-rhage predicts neurologic injury in the shaken baby syndrome. ArchOphthalmol 1989;107:1472-4.
9. Tandon A, Susan M, Yu A, et al. Retinal haemorrhage descriptiontool. Br J Ophthalmol 2011;95:1719-22.
10. Ng W, Watts P, Lawson Z, Kemp A, Maguire S. Development andvalidation of a standardized tool for reporting retinal findings inabusive head trauma. Am J Ophthalmol 2012;154:333-9.
Journal of AAPOS
Related Documents





![Web viewaneurysm.[21,22] Preretinal or subhyaloid hemorrhages – large, smooth bordered and on the retinal surface – occur in up to 25% of patients.[23]](https://static.cupdf.com/doc/110x72/5a6fbd577f8b9ac0538b5bb8/capcuuamateurfileswordpresscom-nbspdoc-fileweb.jpg)





