Gov ver rni ing g B Bo ody y A Assu ura anc ce Fr ram me ew wor rk Re efr res sh 20 015/1 16 6 G Go ove erning g B Bod dy me eet ting g F F F 7 7 M May y 2015 Au uth hor r(s) ) Y Su Yo ue L orks Lai shi ng re , S an Sen d H nior Hum r As mb sso ber ocia Co ate om e: R mmi Ris ssi k a ion and ning d G g S Gov Sup vern ppo nan ort nce e Sp pon nso or Tim m F Fur rne ess, D Dire ecto or o of B Bus siness P Planning g an nd Pa artn ner rships s Is yo our r re epo ort fo or A App pro ova al / / Co onsid der ration n / No otin ng Th his repor rt is s fo or c conside era atio on wit th a a v view w to o a any y ne ece ess sary y a and d ap ppr rop pria ate ch halleng ge Au udit R Req quire eme ent t CC 5. ca Fr Pr ar (T ar by CG 5 apa ram rinc rran This re b y th G O O abil mew cip nge s pa bei he G Obje Org ity wor pal em ape ng Go ect gan re rk) Ri en er ma ove tiv nis qu isk ts t pro ana rna e: ati ire k: In to ovid age anc ona me nad sup des ed, ce al d ents deq ppo s a , an Su dev s s qua ort ass nd ub C vel set ate No ura tha Co op ou e ad ola anc at t mm me ut in dhe n P ce t the mitt ent n th ere Prin tha ey a tee t to he enc nci at r are e an en 6 d ce t ple risk e di nd nsu dom to C es a ks f sc Au ure ma CC and fac uss udit CC ins CG d e ing sed t an CG s (A Co e.g. g de d, a nd G m Ann ons . pr eliv app Int mee nex stitu rote ver pro teg ets x C utio ect ry o opri grat org C N on t ag of t iate ted gan HS an gai he ely d G nis S E d o nst or ac Gov sati Eng oth t co rga ctio vern on glan er onf nis one nan al nd go flic sati ed a nce he CC ve cts o ion and e C ealt CG rna of n’s d/o Com th a As anc inte obj or c mm and ssu ce ere jec cha mitte d ura ests ctiv alle ee) nce s. ves nge ). e ed Eq Ha Is If ad qua ave it no dve alit e y att ot, w erse ty you tac wh ely im u ca che hy n y im pa arr ed? no mpa act ried ? N t? act as d o No Th on sse out here n an ess t an e is ny sme n E s n of ent Equ o e the t ual evid e 9 lity den 9 pr y Im nce rote mpa e to ect act o s ted t A sug d ch Ass ge har ses st t ract ssm tha ter men at t risti nt he ics Ye As es ssu urance e F Frame ewo ork k w will PP Ho Go PE ow ood Ac w do d r ctiv oes isk vity s y k m y you an ur p ag pap em per men r s nt w sup will ppo po ort osit inv tive vol ely lvin im ng mpa g pa act atie on ent Pa ts, atie ca ent are t an ers nd an Pu nd ubli the c E e p Eng pub gag blic gem c? me ent act tivi ity 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Govverrniingg BBoodyy AAssuuraancce Frrammeewworrk Reefrressh 20015/1166
GGooveerningg BBoddy meeettingg FFF77 MMayy 2015
Auuthhorr(s)) Y Su Yo
ue L orks
Lai shi
ng re
, S an
Sen d H
nior Hum
r As mb
sso ber
ocia Co
ate om
e: R mmi
Ris ssi
k a ion
and ning
d G g S
Gov Sup
vern ppo
nan ort
ncee
Spponnsoor Timm FFurrneess, DDireectoor oof BBussiness PPlanningg annd Paartnnerrshipss Is yoourr reepoort foor AAppproovaal // Coonsidderrationn / Nootinng
Thhis reporrt iss foor cconsideeraatioon witth aa vvieww too aanyy neeceesssaryy aandd appprroppriaate chhallengge
Auudit RReqquireemeentt
CC 5. ca Fr
Pr ar (T ar by
CG 5
apa ram
rinc rran This re b y th
G O O
abil mew
cip nge s pa bei he G
Obje Org ity
wor
pal em ape ng Go
ect gan re
rk)
Ri en er ma
ove
tiv nis qu
isk ts t pro ana rna
e: ati ire
k: In to ovid age anc
ona me
nad sup des ed, ce
al d ents
deq ppo s a , an Su
dev s s
qua ort
ass nd
ub C
vel set
ate No ura tha
Co
op ou
e ad ola anc at t mm
me ut in
dhe n P
ce t the mitt
ent n th
ere Prin tha
ey a tee
t to he
enc nci at r are e an
en 6 d
ce t ple
risk e di nd
nsu dom
to C es a ks f sc Au
ure ma
CC and fac uss udit
CC ins
CG d e ing sed t an
CG s (A
Co e.g. g de d, a nd
G m Ann
ons . pr eliv app Int
mee nex
stitu rote ver pro teg
ets x C
utio ect ry o opri grat
org C N
on t ag of t iate ted
gan HS
an gai he ely d G
nis S E
d o nst or ac
Gov
sati Eng
oth t co
rga ctio vern
on glan
er onf nis
one nan
al nd
go flic sati ed a nce
he CC
ve cts o ion and e C
ealt CG
rna of
n’s d/o
Com
th a As
anc inte obj
or c mm
and ssu
ce ere jec
cha mitte
d ura
ests ctiv alle ee)
nce
s. ves nge ).
e
ed
Eq
Ha
Is
If ad
qua
ave
it
no dve
alit
e y
att
ot, w erse
ty
you
tac
wh ely
im
u ca
che
hy n y im
pa
arr
ed?
no mpa
act
ried
? N
t? act
as
d o
No
Th on
sse
out
here n an
ess
t an
e is ny
sme
n E
s n of
ent
Equ
o e the
t
ual
evid e 9
lity
den 9 pr
y Im
nce rote
mpa
e to ect
act
o s ted
t A
sug d ch
Ass
ge har
ses
st t ract
ssm
tha ter
men
at t risti
nt
he ics
Ye
As
es
ssuurancee FFrameewoorkk wwill
PP Ho Go
PE ow ood
Ac w do
d r
ctiv oes isk
vity s y
k m
y you an
ur p ag
pap em
per men
r s nt w
sup will
ppo po ort osit
inv tive
vol ely
lvin im
ng mpa
g pa act
atie on
ent Pa
ts, atie
ca ent
are t an
ers nd
an Pu
nd ubli
the c E
e p Eng
pub gag
blic gem
c? meent acttiviity
1

Recommendations
The Governing Body is asked to:
1. Note the work undertaken to refresh the Governing Body Assurance Framework for 2015/16
2. Consider the refreshed framework and assure itself that the CCG’s corporate objectives and risks to their achievement are accurately reflected and are being effectively managed by accountable officers.
3. Identify any additional controls and mitigating actions that need to be in place to address identified risks and the methods by which it would wish to receive assurance of the effectiveness of these controls.
4. Review and comment on the scores set out within the attached Assurance Framework
2

jr
r
r
r
r
r
Govverrniingg BBoodyy AAssuuraancce Frrammeewworrk Reefrressh 20015/1166
GGooveerningg BBoddy meeettingg
77 MMayy 2015
1 Baackkgrrouundd
Exxeccuttivee DDireectoorss mmet onn MMonndaay 99 MMarrch too reevieew thee QQ4 poosittionn wwithh reegaard to thhe GGooveerning Boodyy AAsssuraancce Frrammewwork (GBAAF) annd disscuusss thhe higgh levvel rissks faacinng deliveeryy off the oorggannisaatioon’ss oobjeectivees ffor 200155/166. Aftter muuchh cconnsidderatioon it waas aagrreeed tthaat aa nuummbeer oof riskks sshoouldd nnoww bbe cclossedd bbut thaat ttheere weeree clearly a nuumbberr off risskss wwhicch neeeddedd too bee reefreshhedd, nnott onnlyy too taake acccoounnt oof uupddateed naatioonaal pprioorittiess, bbut also to reefleect thee cconntinueed ddevvelopmeent annd maatuurityy oof the CCGG oover thhe preevious 112 mmoonthhs..
Directoors aggreed a prooceesss oof reeviieww aand chhallenngee off controols and rriskk sccorress and mmet aggainn oon 88 AAprril too aagree the ffinaal AAsssuraancce Frrammewworrk pprioor tto preeseentatioon to Governning BBody. Meembeers arre aaskkedd tto cconnsider tthe Frammewoork annd offferr any addditional ccommments. TThee ddraft rrefressheed fraameewworkk iss aattaachhedd aat AApppendix 1, toogeetheer wwith tthe suummaary shheeet foor Quuartter 3 2014/155 foor mmeembberrs tto sseee wwhaat the prroppossedd chhanngees aaree.
2 Reecoommeenddattion
Thhe Gooveernningg BBoddy is aaskkedd too:
• Noote thee wworrk uundderrtakkenn too reefrresh the Gooveernningg BBoddy AAssuranncee Frammeewoork forr 200155/16
• Coonssideer thee reefreshhedd fframmeewoorkk annd asssuure itsselff thhatt thhe CCCGG’s coorpooraate objecctivves annd rissks to theirr acchieeveemmennt aare acccuurattelyy reefleecttedd annd aree bbeing efffecttiveely managed byy acccoounntablee officcerss.
• Ideenttify anny aaddditional contrrolss annd mitiggating acctioonss thhat neeedd too be in pplacce to addreesss iddenntiffiedd rriskks and thee mmethoodss bby whhichh it wwouuldd wwishh tto recceive assurranncee off thhe eeffeecttiveeneesss off thhese cconntrools..
• Reevieew and coommmeentt oon thee sscoores ssett oout withiin thee aattaachhedd AAsssurance Fraammewworrk
Paapeer preepaareed bby Suue Laingg, SSennioor AAsssocciatte: Rissk annd GGoovernaancce, Yoorkkshiree & Hummbeer CCommmmisssiooninng Suuppporrt
OOn bbehhalff off Tim Fuurness, DDirrecctorr off Buusiness Plaanninng aandd PParrtneershipps
April 200155
3


Introduction GBAF REFRESH 2015/16 (DRAFT) Appendix 1 The Board Assurance Framework aims to identify the principal or strategic risks to the delivery of the CCG’s strategic objectives. It sets out the controls that are in place to manage the risks and the assurances that show if the controls are having the desired impact. It identifies the gaps in control and hence the key mitigating actions required to reduce the risks towards the target or appetite risk score. It also identifies any gaps in assurance and what actions can be taken to increase assurance to the CCG.
The table below sets out the strategic objectives lists the various principal risks that relate to them and highlights where gaps in control or assurance have been identified. Further details can be found on the supporting pages for each of the Principal Risks.
Strategic Objective Principal Risk identified Risk Owner Risk Initial Score
Risk current Score
Risk Target or Appetite
Score
Are there GAPS in control?
Are there GAPS in
assurance?
1. To improve patient experience and access to care
1.1 Insufficient communication and engagement with patients and the public on CCG priorities and service developments, leading to loss of confidence in CCG decisions (Domain 2) TF 9 9 6 No no
1.2 System wide or specific provider capacity problems emerge to prevent delivery of NHS Constitution and/or NHS E required pledges (Domain 3) RG 15 15 9 No No
2. To improve the quality and equality of healthcare in Sheffield
2.1 Providers delivering poor quality care and not meeting quality targets (Domain 4) KC 9 9 6 No No
2.2 CCG unable to influence equality of access to healthcare because insufficient or ineffective mechanisms to change
TF 9 9 6 yes yes
3. To work with Sheffield City Council to continue to reduce health inequalities in Sheffield
3.1 CCG is unable to undertake the actions, and deliver the outcomes from them, that are set out in the HWB's plan for reducing health inequalities, eg due to financial constraints (Domain 3)
TF 9 6 3 yes yes
4. To ensure there is a sustainable, affordable healthcare system in Sheffield.
4.1 Financial Plan with insufficient ability to reflect changes to meet demands (Domain 3) JN 16 16 6 No No
4.2 Risk management and other governance arrangements put in place by CCG and SCC to manage c£270m Better Care Fund to budget prove inadequate JN 12 12 6 No No
4.3 Budgetary constraints faced by NHS England in particular re specialised services and primary care contracts adversely impact on CCG's ability to implement our plan (domain 3) JN 9 9 6 No No
4.4 Inability to secure partnerships with our main providers that help us to deliver our commissioning plans, including QIPP (Domain 3) TF 9 9 6 Yes Yes 4.5 Contractual and financial constraints facing local practices resulting in an inability of some practices to deliver existing non‐core work and/or wxpand service provision as envisaged in commissioning plans(Domain 3) KCl 12 12 6 Yes Yes
1

5. Organisational development to ensure
CCG meets organisational health
and capability requirements set out in the 6 domains (Annex C
NHS England CCG Assurance Framework)
5.1 Unable to secure timely and effective commissioning support to enable us to adequately respond and secure delivery to existing and new emerging requirements. (Domain 3) RG 12 12 6 No No 5.2 Inability to secure active participation particularly from Member Practices for delivering CCG priorities(Domain 1, 3,5) ZK 12 12 6 No No
5.3 Inadequate adherence to principles of good governance and legal framework leading to breach of regulations and consequent reputational or financial damage (Domain 4)
TF 4 4 4 No No
The Risk Ratings used in the Assurance Framework are based on the following risk stratification table:
Risk Matriz
Likelihood ‐1
Rare
‐2
Unlikely
‐3
Possible
‐4
Likely
‐5 Almost certain
Conseq
uence
Negligible ‐1
1 2 3 4 5 1 to 3 Low
Minor ‐2
2 4 6 8 10 4 to 9 Medium 10 to 14 High
Moderate ‐3
3 6 9 12 15 15 to 19 Very High (Serious) 20 to 25 Critical
Major ‐4
4 8 12 16 20
Extreme ‐5
5 10 15 20 25
2
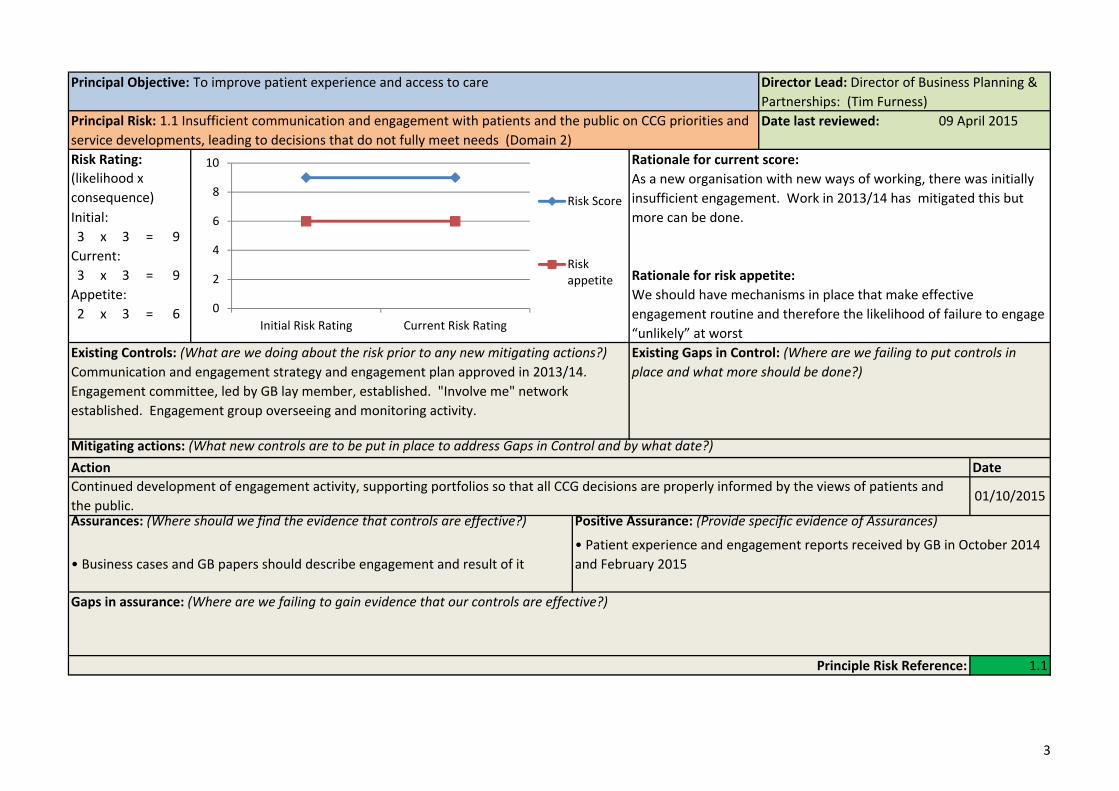
Principal Objective: To improve patient experience and access to care Director Lead: Director of Business Planning & Partnerships: (Tim Furness)
Principal Risk: 1.1 Insufficient communication and engagement with patients and the public on CCG priorities and service developments, leading to decisions that do not fully meet needs (Domain 2)
Date last reviewed: 09 April 2015
Risk Rating:
Initial: 3 x 3 = 9 Current: 3 x 3 = 9 Appetite: 2 x 3 = 6
(likelihood x consequence)
0
2
4
6
8
10
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
As a new organisation with new ways of working, there was initially insufficient engagement. Work in 2013/14 has mitigated this but more can be done.
We should have mechanisms in place that make effective engagement routine and therefore the likelihood of failure to engage “unlikely” at worst
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) Communication and engagement strategy and engagement plan approved in 2013/14. Engagement committee, led by GB lay member, established. "Involve me" network established. Engagement group overseeing and monitoring activity.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?)
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Continued development of engagement activity, supporting portfolios so that all CCG decisions are properly informed by the views of patients and the public.
01/10/2015
Assurances: (Where should we find the evidence that controls are effective?)
• Business cases and GB papers should describe engagement and result of it
Positive Assurance: (Provide specific evidence of Assurances)
• Patient experience and engagement reports received by GB in October 2014 and February 2015
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?)
Principle Risk Reference: 1.1
3
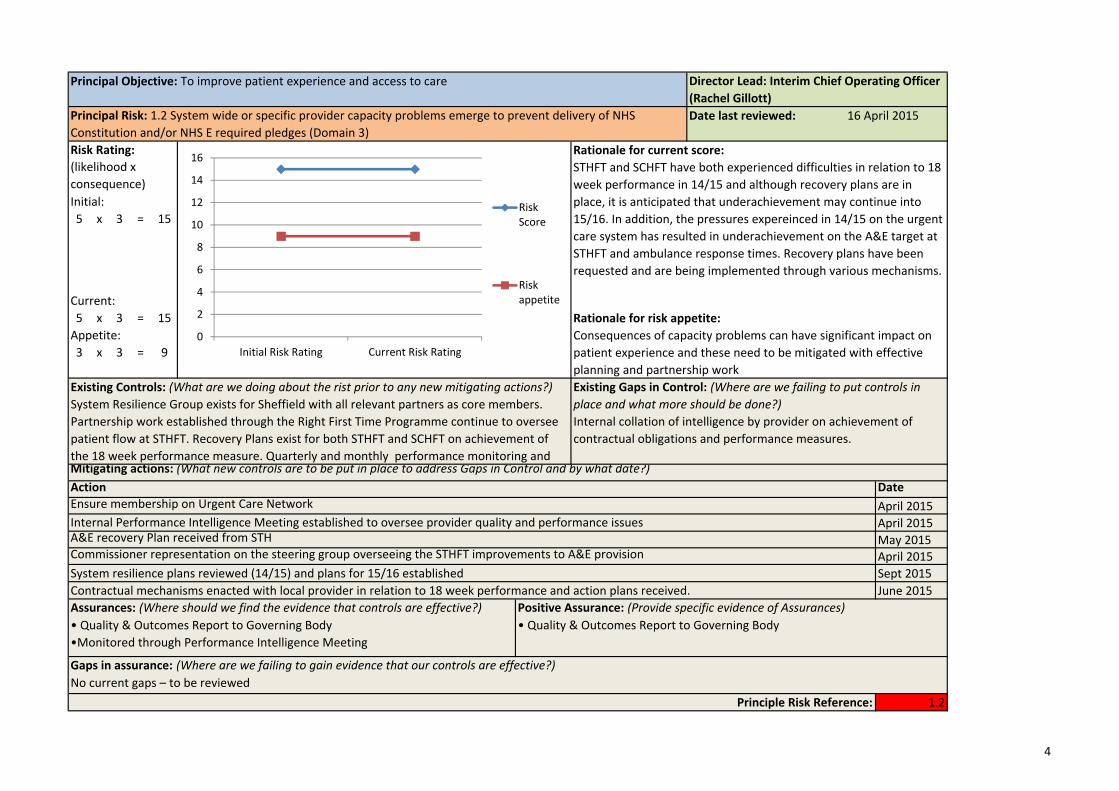
Principal Objective: To improve patient experience and access to care Director Lead: Interim Chief Operating Officer (Rachel Gillott)
Principal Risk: 1.2 System wide or specific provider capacity problems emerge to prevent delivery of NHS Constitution and/or NHS E required pledges (Domain 3)
Date last reviewed: 16 April 2015
Risk Rating:
Initial: 5 x 3 = 15
Current: 5 x 3 = 15 Appetite: 3 x 3 = 9
(likelihood x consequence)
0
2
4
6
8
10
12
14
16
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
STHFT and SCHFT have both experienced difficulties in relation to 18 week performance in 14/15 and although recovery plans are in place, it is anticipated that underachievement may continue into 15/16. In addition, the pressures expereinced in 14/15 on the urgent care system has resulted in underachievement on the A&E target at STHFT and ambulance response times. Recovery plans have been requested and are being implemented through various mechanisms.
Consequences of capacity problems can have significant impact on patient experience and these need to be mitigated with effective planning and partnership work
Existing Controls: (What are we doing about the rist prior to any new mitigating actions?) System Resilience Group exists for Sheffield with all relevant partners as core members. Partnership work established through the Right First Time Programme continue to oversee patient flow at STHFT. Recovery Plans exist for both STHFT and SCHFT on achievement of the 18 week performance measure. Quarterly and monthly performance monitoring and
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) Internal collation of intelligence by provider on achievement of contractual obligations and performance measures.
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Ensure membership on Urgent Care Network April 2015 Internal Performance Intelligence Meeting established to oversee provider quality and performance issues April 2015 A&E recovery Plan received from STH May 2015 Commissioner representation on the steering group overseeing the STHFT improvements to A&E provision April 2015 System resilience plans reviewed (14/15) and plans for 15/16 established Sept 2015 Contractual mechanisms enacted with local provider in relation to 18 week performance and action plans received. June 2015 Assurances: (Where should we find the evidence that controls are effective?) • Quality & Outcomes Report to Governing Body •Monitored through Performance Intelligence Meeting
Positive Assurance: (Provide specific evidence of Assurances) • Quality & Outcomes Report to Governing Body
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) No current gaps – to be reviewed
Principle Risk Reference: 1.2
4

Principal Objective: To improve the quality and equality of healthcare in Sheffield Director Lead: Chief Nurse: (Kevin Clifford)
Principal Risk: 2.1 Providers delivering poor quality care and not meeting quality targets (Domain 4) Date last reviewed: 09 April 2015
Risk Rating: 10 Rationale for current score: (likelihood x The impact of the Francis (2) has been reviewed by Sheffield
Initial: 3 x 3 = 9
consequence)
6
8 Risk Score
providers and the CCG requires assurance that the culture of services that we commission continues to be focused on the safety and wellbeing of patient/service users.
Current: 4 3 x 3 = 9 Risk Rationale for risk appetite: Appetite: 2 appetite To ensure that the consequence is moderate and although there will 2 x 3 = 6
0 Initial Risk Rating Current Risk Rating
always be risks to patient safety and poor quality care, that the impact on patient outcomes and experience is as low as possible.
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) National and Local Policy/ regulatory standards; CQC regulations, SI, Infection Control, Safeguarding procedures, NICE/Quality Standards, Patient Surveys, Quality standards in Contracts, Contract Quality Review Groups
The CCG commissioning for quality strategy has now been adopted by Governing Body in April and sets out our controls and action for Quality improvement.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?)
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action: Delivery of the Commissioning for Quality Strategy Date
Apr‐15
Assurances: (Where should we find the evidence that controls are effective?) Positive Assurance: (Provide specific evidence of Assurances)
• CQC inspections of providers and provider action plans, provider data and annual • Quality Assurance Committee Minutes, Serious Incident reports, reports SI investigation reports, Serious Case Reviews, Clinical Audit reports, Safeguarding reports, Monthly Governing Body Infection control,Patient Infection Control reports, Internal audit benchmarking data, provider Governance Experience /Complaints reports, data on quality targets, exception reports to Meetings, site visits, CCG Commissioning Groups, CCG quality dashboards. Governing Body Quarterly
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) No
Principle Risk Reference: 2.1
5

Principal Objective: To improve the quality and equality of healthcare in Sheffield Director Lead: Tim Furness: Director of Business Planning and Partnerships
Principal Risk: 2.2 CCG unable to influence equality of access to healthcare because insufficient or ineffective mechanisms to change
Date last reviewed: 10 April 2015
Risk Rating:
Initial: 3 x 3 = 9 Current: 3 x 3 = 9 Appetite: 2 x 3 = 6
(likelihood x consequence)
0
2
4
6
8
10
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
There are contractual obligations in place and providers have obligations under the Equality Act. However, data to assess equality of access to services is poor and no specific contractual processes have been put in place yet to measure and if necessary remedy shortcomings.
The consequence of the risk cannot be mitigated, but we should be able to improve data and then establish processes for measuring and remedying problems.
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?)
Equality of access is discussed with providers through the equality engagement group
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) Little contractual discussion. Insufficient data to understand how people with protected characteristics access services
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Develop the collection of equality data across all commissioned services 31/10/2015 Collect patient experience information on barriers to access or inequalities 31/12/2015 Highlight equality of access in contracting intentions, to ensure discussion in 2016/17 negotiations 31/12/2015
Assurances: (Where should we find the evidence that controls are effective?) Equality reporting to GB and published in website
Positive Assurance: (Provide specific evidence of Assurances)
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?)
controls are not yet in place to provide assurance on
Principle Risk Reference: 2.2
6

Principal Objective: To work with Sheffield City Council to continue to reduce health inequalities in Sheffield Director Lead: Director of Business Planning & Partnerships: (Tim Furness)
Principal Risk: 3.1 CCG is unable to undertake the actions, and deliver the outcomes from them, that are set out in the HWB's plan for reducing health inequalities, eg due to financial constraints (Domain 3)
Date last reviewed: 13 April 2015
Risk Rating:
Initial: 3 x 3 = 9 Current: 2 x 3 = 6 Appetite: 1 x 3 = 3
(likelihood x consequence)
0
2
4
6
8
10
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite: We should not commit to actions we cannot deliver, especially within the HWB partnership, and therefore need to take steps to ensure we can deliver.
The HWB has developed a plan to reduce health inequalities (which the CCG is party to). Given the scale of the challenge, it is possible that the actions for the CCG will prove difficult to achieve.
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) HWB Plan considered and agreed by GB CCG specific plan agreed by GB January 2015 and part of overall commissioning plan, and will be reported on alongside other commissioning projects
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) Health Inequalities Action Plan not within scope of the PMO
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Include health inequalities actions within PMO scope, ensuring effective project managmeent and reporting 30/06/2015
Assurances: (Where should we find the evidence that controls are effective?)
Delivery reports on the plan to CET as part of programme approach CCG performance reports
Positive Assurance: (Provide specific evidence of Assurances)
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) We do not yet have positive assurance as reporting on these actions has not yet started.
Principle Risk Reference: 3.1
7
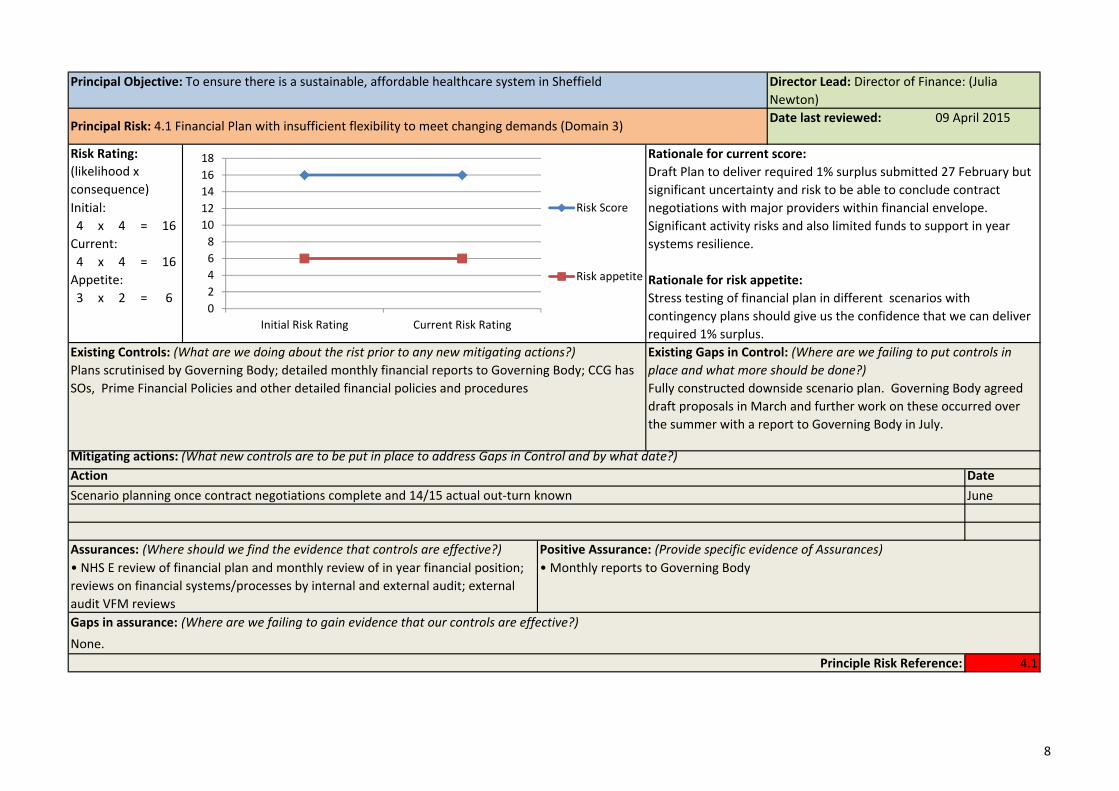
Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield Director Lead: Director of Finance: (Julia Newton)
Principal Risk: 4.1 Financial Plan with insufficient flexibility to meet changing demands (Domain 3) Date last reviewed: 09 April 2015
Risk Rating:
Initial: 4 x 4 = 16 Current: 4 x 4 = 16 Appetite: 3 x 2 = 6
(likelihood x consequence)
0 2 4 6 8 10 12 14 16 18
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
Draft Plan to deliver required 1% surplus submitted 27 February but significant uncertainty and risk to be able to conclude contract negotiations with major providers within financial envelope. Significant activity risks and also limited funds to support in year systems resilience.
Stress testing of financial plan in different scenarios with contingency plans should give us the confidence that we can deliver required 1% surplus.
Existing Controls: (What are we doing about the rist prior to any new mitigating actions?) Plans scrutinised by Governing Body; detailed monthly financial reports to Governing Body; CCG has SOs, Prime Financial Policies and other detailed financial policies and procedures
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) Fully constructed downside scenario plan. Governing Body agreed draft proposals in March and further work on these occurred over the summer with a report to Governing Body in July.
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Scenario planning once contract negotiations complete and 14/15 actual out‐turn known June
Assurances: (Where should we find the evidence that controls are effective?) • NHS E review of financial plan and monthly review of in year financial position; reviews on financial systems/processes by internal and external audit; external audit VFM reviews
Positive Assurance: (Provide specific evidence of Assurances) • Monthly reports to Governing Body
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) None.
Principle Risk Reference: 4.1
8

Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield Director Lead: Director of Finance: (Julia Newton)
Principal Risk: 4.2 Risk management and other governance arrangements put in place by CCG and SCC to manage c£270m Better Care Fund to budget prove inadequate
Date last reviewed: 09 April 2015
Risk Rating:
Initial: 3 x 4 = 12
Current: 3 x 4 = 12 Appetite: 2 x 3 = 6
(likelihood x consequence)
0
2
4
6
8
10
12
14
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite: CCG needs to get to a position that can press ahead with service redesign with confidence. Assessed as risk score of 6
SCC and CCG have ambitious integrated commissioning programme, but major changes (and savings) will take time to implement. Agreed budgets for 15/16 including £9.3m of NR funding and contingency reserves to allow delivery against budget, but shadow monitoring in 14/15 showed the BCF contained 3 major areas of overspend including social care and hospital emergency admissions.
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) Section 75 agreement will be in place from 1 April with risk management arrangements and monthly meeting of a joint Executive Mgt Group. Montly budget monitoring to this group + Governing Body to allow escalation and resolution of issues.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?)
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Completion of longer term financial planning and scenario planning by both partners on back of Deloitte report From June
Assurances: (Where should we find the evidence that controls are effective?) HWBB minutes; Minutes of Executive Mgt meetings. Continuation of Governance & Finance working group if required
Positive Assurance: (Provide specific evidence of Assurances) • Updates monthly to Executive Mgt Group and Governing Body.
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) N/A
Principle Risk Reference: 4.2
9

Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield Director Lead: Director of Finance: (Julia Newton)
Principal Risk: 4.3 Budgetary constraints faced by NHS England in particular re specialised services and primary care contracts adversely impact on CCG's ability to implement our plan (domain 3)
Date last reviewed: 09 April 2015
Risk Rating:
Initial: 3 x 3 = 9
Current: 3 x 3 = 9 Appetite: 2 x 3 = 6
(likelihood x consequence)
0
1
2
3
4
5
6
7
8
9
10
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
At the start of 15/16 we know which specialised services will transfer in year but not the budgets. So a financial risk, but not large due to specific services. Risk is much more for 16/17 when CCGs may have placed based budgets including much greater element of specialised and need to start to plan for impact ‐ ie likely cost pressures. We are only level 1 primary care co‐commissioning but concerns about sustainability of primary care with changes to core contract funding. We do not have reserves to meet costs in lieu of NHSE, without increasing QIPP which is already challenging to deliver
CCG needs to have a position where we are confident that we can work in partnership with NHS E on these areas to develop local health economy and services appropriately.
Existing Controls: (What are we doing about the rist prior to any new mitigating actions?) Joint contracting processes with NHS England. Joint strategy document on primary care. Submission of Primary Care co‐commissioning proposals on 20 June to NHS E and more active joint working. Establishment of Specialised Commissioning Oversight Group from September 2014.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) None
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Assurances: (Where should we find the evidence that controls are effective?) • NHS E led reviews
Positive Assurance: (Provide specific evidence of Assurances) • Monthly finance reports to Governing Body
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) None.
Principle Risk Reference: 4.3
10
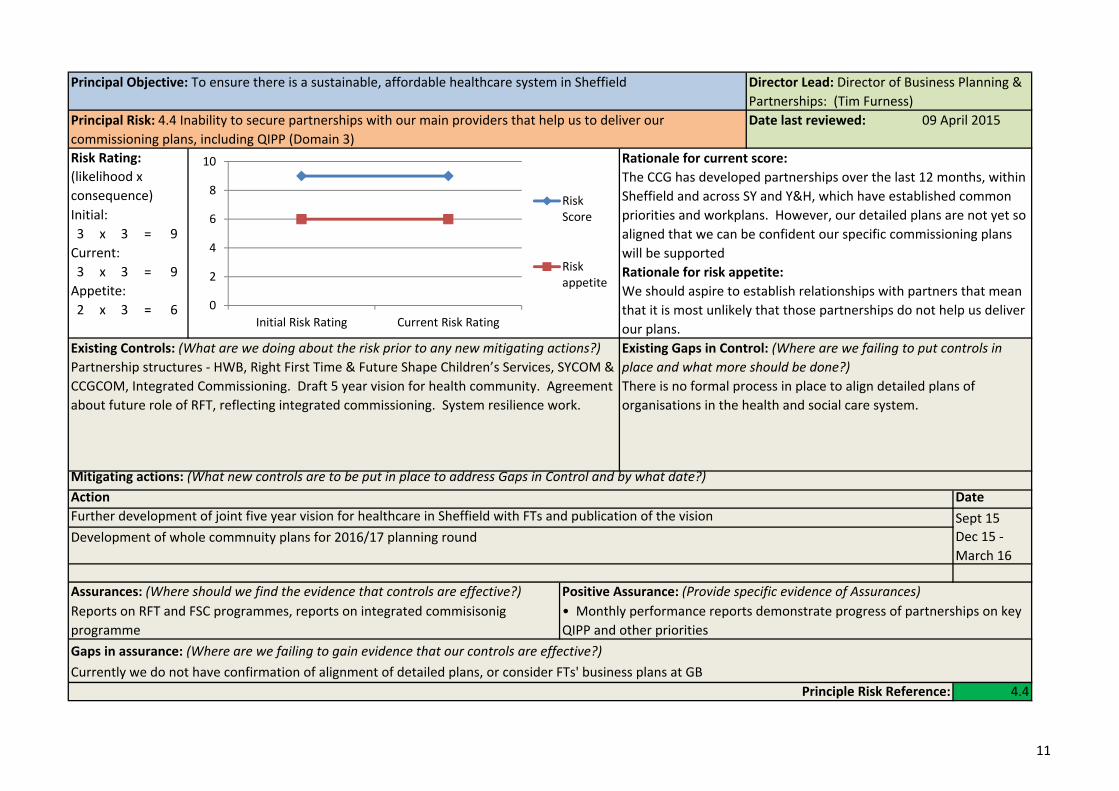
Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield Director Lead: Director of Business Planning & Partnerships: (Tim Furness)
Principal Risk: 4.4 Inability to secure partnerships with our main providers that help us to deliver our commissioning plans, including QIPP (Domain 3)
Date last reviewed: 09 April 2015
Risk Rating:
Initial: 3 x 3 = 9 Current: 3 x 3 = 9 Appetite: 2 x 3 = 6
(likelihood x consequence)
0
2
4
6
8
10
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
The CCG has developed partnerships over the last 12 months, within Sheffield and across SY and Y&H, which have established common priorities and workplans. However, our detailed plans are not yet so aligned that we can be confident our specific commissioning plans will be supported
We should aspire to establish relationships with partners that mean that it is most unlikely that those partnerships do not help us deliver our plans.
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) Partnership structures ‐ HWB, Right First Time & Future Shape Children’s Services, SYCOM & CCGCOM, Integrated Commissioning. Draft 5 year vision for health community. Agreement about future role of RFT, reflecting integrated commissioning. System resilience work.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) There is no formal process in place to align detailed plans of organisations in the health and social care system.
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Further development of joint five year vision for healthcare in Sheffield with FTs and publication of the vision Sept 15
Dec 15 ‐March 16
Development of whole commnuity plans for 2016/17 planning round
Assurances: (Where should we find the evidence that controls are effective?) Reports on RFT and FSC programmes, reports on integrated commisisonig programme
Positive Assurance: (Provide specific evidence of Assurances) • Monthly performance reports demonstrate progress of partnerships on key QIPP and other priorities
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) Currently we do not have confirmation of alignment of detailed plans, or consider FTs' business plans at GB
Principle Risk Reference: 4.4
11

Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield Director Lead: Katrina Cleary
Principal Risk: 4.5 Contractual and financial constraints facing local practices resulting in an inability of some practices to deliver existing non‐core work and/or expand service provision as envisaged in commissioning plans(Domain 3)
Date last reviewed: 09 April 2015
Risk Rating:
Initial: 3 x 4 = 12 Current: 3 x 4 = 12 Appetite: 3 x 2 = 6
(likelihood x consequence)
0
2
4
6
8
10
12
14
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
Currently the contractual changes being considered by NHSE have not come into effect. However practices are becoming more aware of the potential impact this might have and are voicing concerns about ability to take on more service delivery if resource is lost.
Delivering more services in community setting is a stated aim of the CCG and General Practice is a key facet of this. The CCG would aspire to see more services delivered by these providers in a way that does not detrimentally impact on the wider system.
Existing Controls: (What are we doing about the rist prior to any new mitigating actions?) Currently control is affected by joint discussions with NHSE in an attempt to influence their contractual decisions. Joint practice visits take place where an immediate and significant risk is identified. In 2014/15 the SY&B CCGs plan to submit an expression of intrest to NHSE to secure formal delegated responsiblities for key aspect of general practice contracts. NHSE, following publication of recent guidance on GMS/PMS finances are now
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) The key gap is currenlty the responsibility for how general practice contracts are managed and altered with NHSE, with minimal input sought from the local CCG
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Assurances: (Where should we find the evidence that controls are effective?) Positive Assurance: (Provide specific evidence of Assurances)
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?)
Principle Risk Reference: 4.5
12

Principal Objective: To ensure there is a sustainable, affordable healthcare system in Sheffield. Director Lead: Director of Business Planning and Partnerships (Tim Furness)
Principal Risk: 4.6 Provider development required to deliver new models of care and achieve CCG stated outcomes does not happen
Date last reviewed: 10 April 2015
Risk Rating:
Initial: 3 x 4 = 12 Current: 3 x 4 = 12 Appetite: 1 x 4 = 4
(likelihood x consequence)
0
2
4
6
8
10
12
14
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
Although work has started, through development of the "vanguard" new models of care bid, much work is needed, across all organisations, to agree how care should be delivered in future.
If we are to achieve our aims, we must work with providers to ensure they are able to deliver the type of support and care that people will need
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) Development of the vanguard bid Work with partners to develop 5 year vision
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) We do not yet have a clear and agreed view of the new models of care and therefore do not yet have a development plan to achieve the necessary changes
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Work with partners to develop the 5 year vision Sept 15 Ensure consideration of provider development is part of that work Sept 15
Work with providers to agree new models of care and plan to establish those 31/12/2015
Assurances: (Where should we find the evidence that controls are effective?) Positive Assurance: (Provide specific evidence of Assurances)
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) Because this work is at an early stage we have no reporting mechanism in place yet.
Principle Risk Reference: 4.6
13
Principal Objective: Organisational development to ensure CCG meets organisational health and capability requirements set out in the 6 domains (Annex C NHS England CCG Assurance Framework)
Director Lead: Interim Chief Operating Officer: (Rachel Gillott)
Principal Risk: 5.1 Unable to secure timely and effective commissioning support to enable us to adequately respond and secure delivery to existing and new emerging requirements. (Domain 3)
Date last reviewed: 17 April 2015
Risk Rating:
Initial: 3 x 4 = 12
Current: 3 x 4 = 12 Appetite: 3 x 2 = 6
(likelihood x consequence)
0
2
4
6
8
10
12
14
Initial Risk Rating Current Risk Rating
Risk Score
Risk appetite
Rationale for current score:
Rationale for risk appetite:
Current Commissioning Support Arrangements are under review and going through significant change. The commissioning landscape continues to evolve, including integrated commissioning with the LA and the CCG has adopted ambitious commissioning plans to support service transformation. New and emerging initiatives will also need to be responded to as they develop.
Effective commissioning capacity is essential for effective working of CCG .
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) Review of current externally sourced commissioning support arrangements are being reviewed and working with commissioning partners across South Yorkshire & Bassetlaw as well as Yorkshire and Humber to ensure sustainable model of commissioning support. PMO arrangements in place to approve project mandates for internal programme priorities. Specific capacity sourced for current priorties.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?)
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Proposal for new future commissioning support arrangements to be presented to Governing Body May 2015 Implement new arrangements and secure transition from current to future model of provision May onwards Development of a capacity and resourcing approach for internal approvals of commissioning priorities July 2015
Assurances: (Where should we find the evidence that controls are effective?)
CET Approvals Group and Programme Management Delivery Group via Governing Body papers
Governing Body Paper/Minutes Positive Assurance: (Provide specific evidence of Assurances) Minutes of CET & CET Approvals Group via Governing Body papers
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) Currently working with NHSE to identify alternative commissioning support arrangements.
Principle Risk Reference: 5.1
14
Principal Objective: Organisational development to ensure CCG meets organisational health and capability requirements set out in the 6 domains (Annex C NHS England CCG Assurance Framework)
Director Lead: Medical Director (Zak McMurray)
Principal Risk: 5.2 Inability to secure active participation particularly from Member Practices for delivering CCG priorities (Domain 1, 3,5)
Date last reviewed: 09 April 2015
Risk Rating: 14 Rationale for current score: (likelihood x consequence)
12 Active engagement at locality level with clear governance structure into the Clinical Executive Team.
Initial: 10 Risk Score All 88 practices have signed the constitution. Active CRG. 3 x 4 = 12 8 Comprehensive OD plan in place. Current: 6
3 x 4 = 12 4 Risk Rationale for risk appetite: Appetite: 2 appetite Service transformation requires high take up from clinicians. 2 x 3 = 6
0 Initial Risk Rating Current Risk Rating
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?)
Clinical directors now in place with executive role within CET giving clear clinical direction for the organisation. Regular engagement with practices. OD Strategy includes clinical engagement and member practice engagement at its core. CCG Structure includes GP involvement at Gov Body and its associated Committees, CET, CRG and H&WB Board.
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?)
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date
Assurances: (Where should we find the evidence that controls are effective?) • Governing Body Reports 2) OD Steering Group Minutes 3) OD Evaluation Reports to OD Steering Group 4) Response to Election Process 5) OD strategy
Positive Assurance: (Provide specific evidence of Assurances)
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) none
Principle Risk Reference: 5.2
15

Principal Objective: Organisational development to ensure CCG meets organisational health and capability requirements set out in the 6 domains (Annex C NHS England CCG Assurance Framework)
Director Lead: Director of Business Planning and Partnerships (Tim Furness)
Principal Risk: 5.3 Inadequate adherence to CCG Constitution and other governance arrangements to support Nolan Principles and e.g. protect against conflicts of interests (Domain 4)
Date last reviewed: 08 April 2015
Risk Rating: 4.5 Rationale for current score: (likelihood x 4 Robust arrangements are now in place. consequence) 3.5 Initial: 3 Risk Score
1 x 4 = 4 2.5
Current: 2
1 x 4 = 4 1.5 Rationale for risk appetite: Appetite: 1 x 4 = 4
0 0.5 1
Initial Risk Rating Current Risk Rating
Risk appetite
Authorisation is dependent on robust constitutional arrangement
Existing Controls: (What are we doing about the risk prior to any new mitigating actions?) OD strategy to strengthen governance systems and processes. Stringent policies in place to safeguard against conflict of interest. OD session Jan 14 on GB members' role. Explanatory statement now added to committee agendas and explicit discussion regarding percieved
Existing Gaps in Control: (Where are we failing to put controls in place and what more should be done?) no gaps
Mitigating actions: (What new controls are to be put in place to address Gaps in Control and by what date?) Action Date Continual review of governance arrangements, especially with regard to integrated commissioning, co‐commissioning with NHSE Assurances: (Where should we find the evidence that controls are effective?)
• Endorsement by NHS E of Constitution • Forward Planners • OD event evaluations • Governance Structure including Members Council and LEGs
Positive Assurance: (Provide specific evidence of Assurances)
Management of Conflicts of interest noted at all meetings
• Review of constitution
Gaps in assurance: (Where are we failing to gain evidence that our controls are effective?) No gaps
Principle Risk Reference: 5.3
16

Introduction Quarter 3 (Refresh) 2014/15 Appendix 2 The Board Assurance Framework aims to identify the principal or strategic risks to the delivery of the CCG’s strategic objectives. It sets out the controls that are in place to manage the risks and the assurances that show if the controls are having the desired impact. It identifies the gaps in control and hence the key mitigating actions required to reduce the risks towards the target or appetite risk score. It also identifies any gaps in assurance and what actions can be taken to increase assurance to the CCG.
The table below sets out the strategic objectives lists the various principal risks that relate to them and highlights where gaps in control or assurance have been identified. Further details can be found on the supporting pages for each of the Principal Risks.
Strategic Objective Principal Risk identified Risk Owner Risk Initial Score
Risk current Score
Risk Target or Appetite
Score
Are there GAPS in control?
Are there GAPS in
assurance?
1. To improve patient experience and access to care
1.1 Loss of public confidence in the CCG through poor communications (Domain 2) IG 12 4 4 No No
1.2 Insufficient engagement with patients and the public on CCG priorities and service developments, leading to decisions that do not fully meet needs (Domain 2) TF 9 9 6 No Yes 1.3 System wide or specific provider capacity problems emerge to prevent delivery of NHS Constitution and/or NHS E required pledges (Domain 3) IG 12 9 6 No No
2. To improve the quality and equality of healthcare in Sheffield
2.1 Providers delivering poor quality care and not meeting quality targets (Domain 4) KC 9 9 6 Yes No
3. To work with Sheffield City Council to continue to reduce health inequalities in Sheffield
3.1 CCG is unable to undertake the actions, and deliver the outcomes from them, that are set out in the HWB's plan for reducing health inequalities, eg due to financial constraints (Domain 3) TF 12 9 3 Yes Yes 3.2 Budgetary constraints faced by Sheffield City Council and CCG prevent development of effective joint governance and commissioning of integrated services from the Better Care Fund. JN 16 12 6 No No
4. To ensure there is a sustainable, affordable healthcare system in Sheffield.
4.1 Ineffective commissioning practices (Domain 3) TF 6 6 3 No Yes
4.2 Commissioned care does not reflect best practice and service changes are not devised with sufficient clinical engagement. (Domain 3) ZM 9 4 3 No No
4.3 Financial Plan with insufficient ability to reflect changes to meet demands (Domain 3) JN 12 6 6 No No
4.4 Budgetary constraints faced by NHS England in particular re specialised services and primary care contracts adversely impact on CCG's ability to implement our plan (domain 3) JN 12 9 6 No No
4.5 Inability to secure partnerships with our main providers that help us to deliver our commissioning plans, including QIPP (Domain 3) TF 9 9 3 Yes Yes 4.6 Contractual restraints facing member practices resulting in an inability of practices to deliver and expand service provision (Domain 3) KCl 12 6 4 Yes Yes
1

Strategic Objective Principal Risk identified Risk Owner
Risk Initial Score
Risk current Score
Risk Target or Appetite
Score
Are there GAPS in control?
Are there GAPS in
assurance?
5. Organisational development to ensure CCG meets organisational health and capability requirements set out in the 6 domains (Annex C NHS England CCG Assurance Framework)
5.1 CSU unable to provide timely and appropriate support (Domain 3) IG 12 9 6 No No
5.2 Inability to secure active participation particularly from Member Practices for delivering CCG priorities(Domain 1, 3,5) IG 16 8 4 No No
5.3 Ineffective succession planning for clinical engagement (Domain 1, 4) IG 9 6 6 No No 5.4 Inability to develop appropriately skilled leadership and workforce within CCG directly employed staff (Domain 6) IG 9 9 6 No No
5.5 Inadequate adherence to CCG Constitution and other governance arrangements to support Nolan Principles and e.g. protect against conflicts of interests (Domain 4) TF 12 4 4 No No
The Risk Ratings used in the Assurance Framework are based on the following risk stratification table:
Risk Matriz
Likelihood ‐1
Rare
‐2
Unlikely
‐3
Possible
‐4
Likely
‐5 Almost certain
Conseq
uence
Negligible ‐1
1 2 3 4 5 1 to 3 Low
‐2 Minor
2 4 6 8 10 4 to 9 Medium 10 to 14 High
Moderate ‐3
3 6 9 12 15 15 to 19 Very High (Serious) 20 to 25 Critical
‐4 Major
4 8 12 16 20
‐5 Extreme
5 10 15 20 25
2
Related Documents











