9 4 6 Brief clinical and laboratory observations The Journal of Pediatrics June 1982 obstruction has also been hypothesized for some examples of human hydronephrosis, including familial unilateral hydronephrosis. 8 The short-ear mouse is also instructive because the hydronephrosis occurs in association with a generalized developmental disturbance of the skeleton (hypertelorism, broad nasal root, hypoplastic ribs, hypo- plastic pelvis, polydactyly), ear cartilage (scapha), and external genitalia not unlike those in the Schinzel-Giedion syndrome. Overall, the evidence may be interpreted as indicating the Schinzel-Giedion syndrome to be a single gene, autoso- mal recessive disorder. Although consanguinity has yet to be reported, sibs and both sexes have been affected in the absence of known chromosomal defects, teratogenic influ- ences, or parental abnormalities. Despite a diagnostic facies and many recognizable radiologic abnormalities, most of the findings listed in the Table, except hydroneph- rosis, are nonspecific and common to a great many genetic syndromes. Syndrome identification will be greatly facili- tated if the Schinzel-Giedion syndrome is "indexed" as a cause of congenital hydronephrosis, much as Meckel syndrome 9 can be easily identified because of its almost universal inclusion in the differential diagnosis of congeni- tal polycystic kidneys. The presence of hydronephrosis, which appears to be highly penetrant, also facilitates prenatal detection of an affected fetus, although there would be some uncertainty about the presence or degree of hydronephrosis in the second trimester. Prenatal detection of congenital cystic renal malformations, including hydronephrosis, has been successful in a number of set- tings, and continues to improve technically. 1~ REFERENCES 1. Schinzel A, and Giedion A: A syndrome of severe midface retraction, multiple skull anomalies, clubfeet, and cardiac and renal malformations in sibs, Am J Med Genct 1:361, 1978. 2. Donnai D, and Harris R: A further case of a new syndrome including midface retraction, hypertrichosis, and skeletal anomalies, J Med Genet 16:483, 1979. 3. Schinzel A: Personal communication, 1979. 4. Smith DW: Recognizable patterns of human malformation, ed 2, Philadelphia, 1976, WB Saunders Company, p 494. 5. Elejalde BR: Genetic and diagnostic considerations in three families with abnormalities of facial expression and congeni- tal urinary obstruction: "The Ochoa syndrome," Am J Med Genet 3:97, 1979. 6. Johnston JH, Evans JP, Glassberg KI, and Shapiro SR: Pelvic hydronephrosis in children: a review of 219 personal cases, J Urol 117:97, 1977. 7. Wallace ME, and Spickett SG: Hydronephrosis in mouse, rat, and man, J Med Genet 4:73, 1967. 8. Raffle RB: Familial hydronephrosis, Br Mcd J 1:580, 1955. 9. Opitz JM, and Howe J J: The Meckel syndrome, Birth Defects 5:167, 1969. 10. Lawson TL, Foley WD, Berland MD, and Clark KE: Ultra- sonic evaluation of fetal kidneys, Radiology 138:153, 1981. Glutaric acidemia type II." Clinical biochemical, and morphologic considerations Stephen 1. Goodman, M.D.,* Dan O. Stene, B.Sc., Edward R.B. McCabe, M.D., Ph.D, Michael D. Norenherg, M.D., Robert H. Shikes, M.D., David A. Stumpf, M.D., Ph.D., and Glenn K. Blackburn, M.D., Denver, Colo., and Somerset, Ky. From the Departments of Pediatrics, Neurology, and Pathology, University of Colorado Health Sciences Center School of Medicine and the Children's Clinic. Supported in part by a grant (RR-69) from the General Clinical Research Centers Program of the Division of Research Services, National Institutes of Health, by Maternal and Child Health Special Project 252, by National Institutes of Health grants HD-08315 and HD-02024. by a Clinical Research Grant from the Muscular Dystrophy Association, and by the Medical Research Service of the Veterans Administration. *Reprint address."Department of Pediatrics. Box C-233, University of Colorado Health Sciences Center, 4200 East Ninth Ave., Denver, CO 80262. GLUTAR1C ACIDEMIA TYPE 1! is an inborn error of metabolism characterized by the accumulation and excre- tion of metabolites of the substrates of several acyl-CoA dehydrogenases, including those specific for glutaryl-CoA, isovaleryl-CoA, and butyryl-CoA. In its acute form the condition presents with severe hypoglycemia, metabolic Abbreviations used PAS: periodic acid-Schiff FAD: flavin adenine dinucleotide DCPIP: 2,6-dichiorophenol indophenol ETF: electron transfer flavoprotein 0022-3476/82/060946+05500.50/0 1982 The C. V. Mosby Co.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9 4 6 B r i e f clinical and laboratory observations The Journal o f Pediatrics June 1982
obstruction has also been hypothesized for some examples
of human hydronephrosis, including familial unilateral
hydronephrosis. 8 The short-ear mouse is also instructive
because the hydronephrosis occurs in association with a
generalized developmental disturbance of the skeleton
(hypertelorism, broad nasal root, hypoplastic ribs, hypo-
plastic pelvis, polydactyly), ear cartilage (scapha), and
external genitalia not unlike those in the Schinzel-Giedion
syndrome.
Overall, the evidence may be interpreted as indicating
the Schinzel-Giedion syndrome to be a single gene, autoso-
mal recessive disorder. Although consanguinity has yet to
be reported, sibs and both sexes have been affected in the
absence of known chromosomal defects, teratogenic influ-
ences, or parental abnormalities. Despite a diagnostic
facies and many recognizable radiologic abnormalities,
most of the findings listed in the Table, except hydroneph-
rosis, are nonspecific and common to a great many genetic
syndromes. Syndrome identification will be greatly facili-
tated if the Schinzel-Giedion syndrome is "indexed" as a
cause of congenital hydronephrosis, much as Meckel
syndrome 9 can be easily identified because of its almost
universal inclusion in the differential diagnosis of congeni-
tal polycystic kidneys. The presence of hydronephrosis,
which appears to be highly penetrant, also facilitates
prenatal detection of an affected fetus, although there
would be some uncertainty about the presence or degree of
hydronephrosis in the second trimester. Prenatal detection
of congenital cystic renal malformations, including
hydronephrosis, has been successful in a number of set-
tings, and continues to improve technically. 1~
R E F E R E N C E S
1. Schinzel A, and Giedion A: A syndrome of severe midface retraction, multiple skull anomalies, clubfeet, and cardiac and renal malformations in sibs, Am J Med Genct 1:361, 1978.
2. Donnai D, and Harris R: A further case of a new syndrome including midface retraction, hypertrichosis, and skeletal anomalies, J Med Genet 16:483, 1979.
3. Schinzel A: Personal communication, 1979. 4. Smith DW: Recognizable patterns of human malformation,
ed 2, Philadelphia, 1976, WB Saunders Company, p 494. 5. Elejalde BR: Genetic and diagnostic considerations in three
families with abnormalities of facial expression and congeni- tal urinary obstruction: "The Ochoa syndrome," Am J Med Genet 3:97, 1979.
6. Johnston JH, Evans JP, Glassberg KI, and Shapiro SR: Pelvic hydronephrosis in children: a review of 219 personal cases, J Urol 117:97, 1977.
7. Wallace ME, and Spickett SG: Hydronephrosis in mouse, rat, and man, J Med Genet 4:73, 1967.
8. Raffle RB: Familial hydronephrosis, Br Mcd J 1:580, 1955. 9. Opitz JM, and Howe J J: The Meckel syndrome, Birth Defects
5:167, 1969. 10. Lawson TL, Foley WD, Berland MD, and Clark KE: Ultra-
sonic evaluation of fetal kidneys, Radiology 138:153, 1981.
Glutaric acidemia type II." Clinical biochemical, and morphologic considerations
Stephen 1. Goodman, M.D.,* Dan O. Stene, B.Sc., Edward R.B. McCabe, M.D., Ph.D, Michael D. Norenherg, M.D., Robert H. Shikes, M.D., David A. Stumpf, M.D., Ph.D., and
Glenn K. Blackburn, M.D., Denver, Colo., and Somerset, Ky.
From the Departments o f Pediatrics, Neurology, and Pathology, University of Colorado Health Sciences Center School o f Medicine and the Children's Clinic.
Supported in part by a grant (RR-69) from the General Clinical Research Centers Program o f the Division o f Research Services, National Institutes o f Health, by Maternal and Child Health Special Project 252, by National Institutes o f Health grants HD-08315 and HD-02024. by a Clinical Research Grant from the Muscular Dystrophy Association, and by the Medical Research Service o f the Veterans Administration.
*Reprint address." Department of Pediatrics. Box C-233, University of Colorado Health Sciences Center, 4200 East Ninth Ave., Denver, CO 80262.
GLUTAR1C ACIDEMIA TYPE 1! is an inborn error of
metabolism characterized by the accumulation and excre-
tion of metabolites of the substrates of several acyl-CoA
dehydrogenases, including those specific for glutaryl-CoA,
isovaleryl-CoA, and butyryl-CoA. In its acute form the
condition presents with severe hypoglycemia, metabolic
Abbreviations used PAS: periodic acid-Schiff FAD: flavin adenine dinucleotide DCPIP: 2,6-dichiorophenol indophenol ETF: electron transfer flavoprotein
0022-3476/82/060946+05500.50/0 �9 1982 The C. V. Mosby Co.

Volume 100 Brief clinical and laboratory observations 9 4 7 Number 6
acidosis, and dea th in early infancy? 4 The purpose of this
paper is to present the clinical, biochemical, and pathologic
features of a female infant with the disorder.
CASE REPORT.
The patient was the fourth child of unrelated parents whose first child, a girl, is well at 10 years. Their second child, also a girl, became hypotonie, tachypneic, and hypoglycemic at one day of age and died 19 days later, after a course of vomiting, intermittent acidosis, recurrent hypoglycemia, and liver dysfunction with hepatomegaly, direct hyperbilirubinemia, and elevated serum transaminase values. Postmortem examination showed severe fatty changes in the liver, cloudy swelling in the proximal convoluted tubules, and hemorrhage in the right lateral cerebral ventricle. The third child, a boy, became ill with the same symptoms at one day of age and died two days later, autopsy showing diffuse microvesicular changes in the liver, a massive intraventricular hemorrhage, and occasional large cells with PAS-positive vacuoles in the white matter of the brain.
The subject of this report was the youngest female sibling, the term product of a normal gestation and delivery. She showed little interest in her feedings for the first few days and at 72 hours became limp, vomited, and had a seizure. Laboratory investiga- tions showed hypoglycem!a (24 mg/dl), compensated metabolic acidosis, and moderate hyperammonemia (190 gg/dl).Organic acids in the urine (Fig. I, top) suggested a diagnosis of glutaric acidemia type 11, and protein intake was restricted to approxi- mately 1 gm/kg/day. On admission to the University of Colorado Health Sciences Center at I 1 days of age, physical examination showed only tachypnea and slightly diminished tone and respon- siveness. Laboratory values included: Hgb 14.2 gm/dl, WBC 4,000/ram 3 with normal differential, platelet count 155 X 103/ mm 3, Na concentration 138 mEq/L, K 5.0 mEq/L, CI 110 mEq/L, Ca 4.7 mEq/L, total CO2 19.8 mEq/L, glucose 94 mg/dl (with iv fluids), total protein 4.6 gm/dl, albumin 2.9 gm/dl, SGOT 46 IU/L (normal < 74), and SGPT 99 IU/L (normal < 25). A computed tomographie scan showed diffuse encephalo- malacia, especially in the vermis, temporal lobes and caudate, and the electroencephalogram was normal.
Treatment with bicarbonate by mouth and a diet low in protein and fat was not successful. Protein intake greater than 0.8 to 1.0 gm/kg/day resulted in acidosis and projectile vomiting, and she died in her seventh week of life, apparently of a cardiomyopathy, after developing edema, cardiomegaly, bradyeardia, and then ventricular tachycardia. Autopsy was performed within one hour of death.
M E T H O D S
Serum and urine samples were stored at - 2 0 ~ prior to
analysis. Amino acids were measured on a Beckman model
121M amino acid analyzer using l i thium ci trate buffers.
Organic acids in urine were examined by gas chromatog-
raphy as described previously, 5 and peaks were identified
on a Hewlet t -Packard model 5992A G C / M S . D and L
stereoisomers of 2-hydroxyglutaric acid were separated by
Solvent
C
[
i J I
C-24
Solvent D F Front
C-24
Fig. 1. GC tracing (OV-22) of urine organic acids at diagnosis (top) and at (bottom) 11 days of age. A = Lactic, B = 3- hydroxyisovaleric, C = malonic (internal standard = 0.33 mg/mg creatinine), D = ethylmalonic, E = 5-hydroxyhexanoic (?), F = glutaric, G = 7-hydroxyoctanoic, H = adipic, I = 2-hydroxy- glutaric, J = suberic, K = citric, L = sebacic, and M = duodeca- nedioic.
capillary gas chromatography of O-acetylated di-(-)-2-
butyl esters as described by Duran et al, 6 but on a 25 m
fused silica column of SE-54, internal d iameter 0.2 mm.
The concentrat ion of glutar ic acid in brain was measured
by gas chromatography, using malonic acid as an internal
s tandard. Fibrobasts were grown in minimal essential
medium (Eagle) containing Earle salts, nonessential amino
acids, antibiotics, and fetal bovine serum (15%).
Tissues for light and electron microscopy were processed
in routine fashion. Liver mi tochondr ia were isolated imme-
diately after autopsy, and half of the brain and much
of the liver were not fixed but were instead frozen at - 2 0 o c .
Activity of g lutaryl -CoA dehydrogenase in liver mito-
chondria and fibroblasts was measured with and without
FAD, as described previously2.7; in some fibroblast studies,
2,6-dichlorophenol indophenol (10-3M) was used as an

9 4 8 Brief clinical and laboratory observations The Journal of Pediatrics June 1982
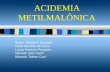
Fig. 2. A, Photomicrograph of caudate nucleus, showing numer- ous swollen astroglial nuclei (arrows) having the appearance of Alzheimer type II cells. B, Photomicrograph of thalamus from the same section, showing normal appearing astroglial nuclei; (Hema- toxylin and eosin; X300).
electron acceptor instead of methylene blue. Oxidation of D-2-hydroxyglutarate by cytochrome c in submitochondri- al particles from cultured fibroblasts was measured in the manner previously described for the oxidation of succi- nateS; the substrate concentration in these assays was 10 • 10-~M.
R E S U L T S
Large increases in glutaric, ethylmalonic, adipic, suber- ic, sebacic, and duodecanedioic acids were observed at the time of diagnosis but, on admission to University of Colorado Health Sciences Center eight days later, the C6, Cs, C10, and C~2 dicarboxylie acids had largely disappeared and 2-hydroxyglutaric acid had become prominent (Fig. 1). The latter pattern persisted with only minor variations in lactic, isobutyrylglycine, and glutaric excretion until about two days prior to death, when it reverted to the one that had been present at diagnosis. In all three urine
specimens examined by capillary gas chromatography, more than 95% of the excreted 2-hydroxyglutarate was the D-isomer.
Serum amino acid values were normal at the time of diagnosis. Reduced concentrations of branched-chain ami- no acids were first noted at 3 weeks of age, and persisted until death. There were no other consistent abnormalities of serum or urine amino acids; in particular, sarcosine was not detected in any of the five serum and 12 urine samples examined by ion-exchange chromatography.
The principal findings on autopsy were marked diffuse fatty infiltration of the myocardium, prominent fatty metamorphosis of the liver, mild fatty infiltration of the renal tubular epithelium, and striking Alzheimer type II changes that were present in the caudate nucleus and not in the adjacent thalamus (Fig. 2). The concentration of glutaric acid in the frontal cortex was 0.52 ~mole/gm wet weight (normal = not detected).
Glutaryl-CoA dehydrogenase activity in liver mitochon- dria (72.8 nmol C02/hour/mg protein) and fibroblasts (2.60 nmol CO2/hour/mg protein) was normal, even (in fibroblasts) when DCPIP was used as a terminal electron acceptor (0.0051 pmol COJhour /mg protein; con- trols = 0.0004 and 0.0037). Mitochondrial and fibroblast activity decreased by only 54 and 23%, respectively, when FAD was not present in the incubation medium.
There was no apparent difference in the ability of mitochondria from normal and mutant fibroblasts to oxidize D-2-hydroxyglutaric acid.
D I S C U S S I O N
All previous infants with glutaric acidemia type II have been male and, although several had female siblings who died with what might have been the same condition, the present case is the first in which a girl is clearly affected. Inheritance of the disorder in this family is thus most likely as an autosomal recessive trait, although X-linked inheri- tance with clinical disease in a female mosaic is not excluded.
The primary defect in the disorder remains unclear. The nature of the organic aciduria indicates simultaneous deficiency of several acyl-CoA dehydrogenases, at least three of which, i.e., glutaryl-CoA dehydrogenase, isovale- ryl-CoA dehydrogenase, and butyryl-CoA dehydrogenase, have normal activity in vitro in cultured fibroblasts. 2'4'9 The present report extends this observation, glutaryl-CoA dehydrogenase activity also being normal in liver mito- chondria.
The discrepancy between the apparent in vivo enzyme deficiency and the normat activity in vitro might be explained by defects (1) in the biosynthesis of the common coenzyme, flavin adenine dinucleotide, (2) in the move-

Volume 1 O0 Brief clinical and laboratory observations 9 4 9 Number 6
ment of acyl-CoA esters between the cytoplasm, mitochon- dria, and peroxisomes, or (3) in the transfer of electrons from the acyl-CoA dehydrogenases into or through the electron transport chain. Normal tissue activity of glutar- yl-CoA dehydrogenase without added FAD, noted previ- ously 2 and confirmed in the present case, is strong evidence against a block in FAD biosynthesis.
Our initial finding of sarcosinemia in this condition, 2 which has been confirmed in several additional patients 3. 4 but which was not found in this patient, is more consistent with a defect in electron transport since, beginning with the electron transfer flavoprotein, electrons from sarcosine dehydrogenase and acyl-CoA dehydrogenases traverse a common path to the electron transport chain, t~ The normal
fibroblast activity of glutaryl-CoA dehydrogenase using DCPIP, which accepts electrons from ETF but not directly from holodehydrogenases," suggests that the defect is not in ETF itself, and confirms previous observations made by Rhead et al 9 on another patient. Not excluded by these
findings, however, is a defect in ETF dehydrogenase, an iron-sulfur flavoprotein intermediate between ETF and coenzyme Q.12
Increased excretion of 2-hydroxyglutaric acid has been observed in all previous patients with glutaric acidemia type I1,1-4 but has received little comment. The present results show that the accumulated 2-hydroxyglutaric in this patient is predominantly the D-isomer, a compound that is normally oxidized to 2-ketoglutaric by a mitochon- drial D-2-hydroxyglutarate dehydrogenase. 13 Deficiency of this enzyme has been suggested as the cause of isolated D-2-hydroxyglutaric aciduria in man. 14 Preliminary results in this laboratory show that mitochondrial oxida- tion of D-2-hydroxyglutarate is independent of rotenone and sensitive to antimycin, suggesting electron entry into the respiratory chain at coenzyme Q, like those from the other substrates accumulated in this disorder. We were unable, however, to demonstrate a defect in this system in fibroblast mitochondria from the patient, suggesting either that the defect in the disorder is not in fact in electron transport or that, at least in relation to o-2-hydroxyglu- taric metabolism, it is not expressed in these cells.
The postmortem findings in the heart, liver, and kidneys
in this patient are similar to those reported previously TM
and were indistinguishable from those of Reye syndrome by both light and electron microscopy, suggesting that urine organic acids be examined in all infants with features of this syndrome. Not typical of Reye syndrome and extremely unusual, however, were the glial changes that were observed only in the caudate nucleus. The brain glutaric acid concentration in this patient was similar to that found in glutaric acidemia caused by glutaryl-CoA dehydrogenase deficiency, 7, ~5 in which degeneration and
fibrous gliosis of the caudate and putamen is typical. The Alzheimer type II changes in the patient may represent early signs of similar degeneration, ~6 perhaps indicating a particular sensitivity of glial cells in this region to glutarate toxicity.
Dietary treatment was not effective in this case; death probably occurred as a result of protein malnutrition superimposed on a background of mitochondrial disease. If the defect in the condition is indeed one of electron transport, and if pathogenesis is related to toxicity of accumulated acid(s), e.g., glutaric or ethylmalonic, treatment with methylene blue might be suggested as a possible way to oxidize the reduced holodehydrogenases and to permit further oxidation of the enzyme sub-
strates.
We thank Dr. Robert Summitt for his assistance with many facets of these studies, and Ms. Harriet McKelvey for expert technical assistance.
REFERENCES
1. Przyrembel H, Wendel U, Becker K, Bremer HL, Bruinvis L, Ketting D, and Wadman SK: Glutaric aciduria type I1: Report on a previously undescribed metabolic disorder, Clin Chim Acta 66:227, 1976.
2. Goodman SI, McCabe ERB, Fennessey PV, and Mace JW: Multiple acyI-CoA dehydrogenase deficiency (glutaric acidu- ria type II) with transient hypersarcosinemia and sarcosinu- ria; possible inherited deficiency of an electron transfer flavoprotein, Pediatr Res 14:12, 1980.
3. Sweetman L, Nyhan WL, Trauner DA, Merritt TA, and Singh M: Glutaric aciduria type II, J PEDIATR 96:1020, 1980.
4. Gregersen N, K~ilvraa S, Rasmussen K, Christensen E, Brandt N J, Ebbesen F, and Hansen FH: Biochemical studies on a patient with defects in the metabolism of acyl-CoA and sarcosine; another possible case of glutaric aciduria type 11, J Inherited Metab Dis 3:67, 1980.
5. Goodman SI, and Markey SP: Diagnosis of organic acidemias by gas chromatography-mass spectrometry, New York, 1981, Alan R. Liss, Inc., p 105.
6. Duran M, Kamerling JP, Bakker HD, van Gennip AH, and Wadman SK: L-2-Hydroxyglutaric aciduria: an inborn error of metabolism? J Inherited Metab Dis 3:109, 1980.
7. Goodman SI, Norenberg MD, Shikes RH, Breslich D J, and Moe PG: Glutaric aciduria: Biochemical and morphologic considerations, J PEDIATR 90:746, 1977.
8. Stumpf DA, and Parks JK: Human mitochondrial electron transport chain: Assay of succinate:cytochrome c redactase in leukocytes, platelets and cultured fibroblasts, Biochem Me~ 25:234, 1981.
9. Rhead W, Mantagos S, and Tanaka K: Glutaric aciduria type !1: In vitro studies on substrate oxidation, acyl-CoA dehydro- genases, and electron-transferring flavoprotein in cultured skin fibroblasts, Pediatr Res 14:1339, 1980.
10. Hoskins DD: The electron-transferring flavoprotein as a common intermediate in the mitochondrial oxidation of buty- ryl coenzyme A and sarcosine, J Biol Chem 241:4472, 1966.

9 5 0 Brief clinical and laboratory observations The Journal of Pediatric~s June 1982
I I. Hall CL, and Kamin H: The purification and some properties of electron transfer flavoprotein and general fatty acyl coen- zyme A dehydrogenase from pig liver mitochondria, J Biol Chem 250:3476, 1975.
12. Ruzicka F J, and Beinert H: A new iron-sulfur flavoprotein of the respiratory chain: A component of the fatty acid /3 oxidation pathway, J Biol Chem 252:8440, 1977.
13. Tubbs PK, and Greville GD: The oxidation of D-a-hydroxy- acids in animal tissues, Biochem J 81:104, 1961.
14. Chalmers RA, Lawson AM, Watts RWE, Tavill AS, Kamerl-
ing JP Hey E, and Ogilvie D: D-2-Hydroxyglutaric aciduria: Case report and biochemical studies, J Inherited Metab Dis 3:11, 1980.
15. Leibel RL, Shih VE, Goodman SI, Bauman ML, McCabc ERB, Zwerdling RG, Bergman I, and Costello C: Glutaric acidemia: A metabolic disorder causing progressive choreoa thetosis, Neurology 30:1163, 1980.
16. Norenberg MD: The astrocyte in liver disease, in Advanccs ir~ cellular neurobiology, vol 2, New York, 1981, Academic Press, Inc., p 303.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具
Related Documents