J Am Acad Audiol 10 : 80-103 (1999) Glasgow Hearing Aid Benefit Profile : Derivation and Validation of a Client-centered Outcome Measure for Hearing Aid Services Stuart Gatehouse* Abstract The Glasgow Hearing Aid Benefit Profile (GHABP) has been derived, optimized, and veri- fied as an instrument suitable for application in the context of the evaluation of the efficacy and effectiveness of rehabilitative services for hearing-impaired adults . The profile produces scales of preintervention disability, handicap, reported hearing aid use, reported benefit, sat- isfaction, and residual disability, obtained over a combination of prespecified listening circumstances and those nominated by individual hearing-impaired listeners . A validity cri- terion for the GHABP and other contenders for use in the evaluation of such services is proposed and justified . The outcome scales from the GHABP are demonstrated to exhibit the power to discriminate between hearing aid fittings, and the instrument is proposed as a suitable candidate for a routine service monitoring indicator as part of a program of quality assurance and standards . Key Words : Benefit, disability, handicap, hearing aid Abbreviations : GHABP = Glasgow Hearing Aid Benefit Profile, HDABI = Hearing Disability and Aid Benefit Interview, SII = Speech Intelligibility Index T he management of adults with hearing impairment aims to alleviate the dis- abilities and handicaps that occur as a consequence . Often, an important component of that management is the provision of personal amplification via a hearing aid or hearing aids . Hearing aid services may be configured in a variety of ways but always contain elements associated with the technical performance of the prosthesis and the extent to which the device helps the listener overcome the deficits and dis- advantages experienced in everyday life . For either groups of listeners or for individuals there are a variety of options open to clinicians in both the technical and rehabilitative domains. In the context of optimizing services, demon- strating to bodies or individuals responsible for funding services and to hearing-impaired lis- teners, there is a growing requirement to pro- *MRC Institute of Hearing Research (Scottish Section), Glasgow, Scotland Reprint requests : Stuart Gatehouse, MRC Institute of Hering Research (Scottish Section), Royal Infirmary, Queen Elizabeth Building, Alexandra Parade, Glasgow G31 2ER, Scotland vide measures of outcome that are appropriate and sensitive to the various options for inter- vention . Other contributions to this volume address a number of issues concerning the dimensions and measures that might be appro- priate, but it is almost universally accepted that one of the classes of measure that is required has to reside in the assessment of the extent to which the intervention process has reduced the disabilities and handicaps experienced by hear- ing-impaired listeners and has been successful in reducing them to levels experienced by their peers in the unaffected population . Performance measures cannot adequately characterize disability and handicap ; therefore, such instruments have to reside in the self- report domain . This has led to the development of a variety of questionnaire and inventory pro- cedures for the characterization of disability and handicap and its subsequent change fol- lowing intervention (e .g., see Tannahill, 1979 ; Ventry and Weinstein, 1982 ; Weinstein and Ven- try, 1983 ; Weinstein et al, 1986 ; Lichtenstein et al, 1988 ; Newman and Weinstein, 1988 ; Brooks, 1990 ; Cox and Gilmore, Schow and Gatehouse, 1990 ; Mulrow et al, 1990 ; Cox et al, 1991 ; Dil- lon et al 1991, 1997 ; Gatehouse, 1993 ; Cox and 80

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

J Am Acad Audiol 10 : 80-103 (1999)
Glasgow Hearing Aid Benefit Profile : Derivation and Validation of a Client-centered Outcome Measure for Hearing Aid Services Stuart Gatehouse*
Abstract
The Glasgow Hearing Aid Benefit Profile (GHABP) has been derived, optimized, and veri-fied as an instrument suitable for application in the context of the evaluation of the efficacy and effectiveness of rehabilitative services for hearing-impaired adults . The profile produces scales of preintervention disability, handicap, reported hearing aid use, reported benefit, sat-isfaction, and residual disability, obtained over a combination of prespecified listening circumstances and those nominated by individual hearing-impaired listeners . A validity cri-terion for the GHABP and other contenders for use in the evaluation of such services is proposed and justified. The outcome scales from the GHABP are demonstrated to exhibit the power to discriminate between hearing aid fittings, and the instrument is proposed as a suitable candidate for a routine service monitoring indicator as part of a program of quality assurance and standards.
Key Words: Benefit, disability, handicap, hearing aid
Abbreviations : GHABP = Glasgow Hearing Aid Benefit Profile, HDABI = Hearing Disability and Aid Benefit Interview, SII = Speech Intelligibility Index
T
he management of adults with hearing impairment aims to alleviate the dis-abilities and handicaps that occur as a
consequence. Often, an important component of that management is the provision of personal amplification via a hearing aid or hearing aids . Hearing aid services may be configured in a variety of ways but always contain elements associated with the technical performance of the prosthesis and the extent to which the device helps the listener overcome the deficits and dis-advantages experienced in everyday life . For either groups of listeners or for individuals there are a variety of options open to clinicians in both the technical and rehabilitative domains. In the context of optimizing services, demon-strating to bodies or individuals responsible for funding services and to hearing-impaired lis-teners, there is a growing requirement to pro-
*MRC Institute of Hearing Research (Scottish Section), Glasgow, Scotland
Reprint requests : Stuart Gatehouse, MRC Institute of Hering Research (Scottish Section), Royal Infirmary, Queen Elizabeth Building, Alexandra Parade, Glasgow G31 2ER, Scotland
vide measures of outcome that are appropriate and sensitive to the various options for inter-vention. Other contributions to this volume address a number of issues concerning the dimensions and measures that might be appro-priate, but it is almost universally accepted that one of the classes of measure that is required has to reside in the assessment of the extent to which the intervention process has reduced the disabilities and handicaps experienced by hear-ing-impaired listeners and has been successful in reducing them to levels experienced by their peers in the unaffected population .
Performance measures cannot adequately characterize disability and handicap ; therefore, such instruments have to reside in the self-report domain . This has led to the development of a variety of questionnaire and inventory pro-cedures for the characterization of disability and handicap and its subsequent change fol-lowing intervention (e.g., see Tannahill, 1979 ; Ventry and Weinstein, 1982 ; Weinstein and Ven-try, 1983 ; Weinstein et al, 1986; Lichtenstein et al, 1988 ; Newman and Weinstein, 1988 ; Brooks, 1990 ; Cox and Gilmore, Schow and Gatehouse, 1990 ; Mulrow et al, 1990 ; Cox et al, 1991; Dil-lon et al 1991, 1997 ; Gatehouse, 1993 ; Cox and
80

Glasgow Hearing Aid Benefit Profile/Gatehouse
Rivera, 1992 ; Cox and Alexander, 1995 ; Cox, 1997) . This list is by no means comprehensive and a search of the literature would make it considerably lengthier. Instruments in the lit-erature suggested as outcome measures follow-ing hearing aid fitting can vary to a large degree in length (Schow and Gatehouse, 1990) and in their internal structure .
This article reports some aspects of research commissioned by the Department of Health in London, England whose primary aim was to identify, generate, optimize, and calibrate a series of condition-specific and generic outcome measures in both the performance and self-report domains suitable for application in the context of the United Kingdom National Health Service (UKNHS) and anchored against more intensive and extensive measures that might be used in field trial and research settings . The overall research program is described in Gate-house (1997) . The present article focuses on the development of a self-report measure of hearing aid benefit . The measure combines and recon-ciles the requirements of sufficient brevity for potential application in routine clinical settings with the psychometric properties that are nec-essary for such an instrument to distinguish between the levels, types, and delivery of hear-ing aids and hearing aid services . Although the target context of the instrument is based around the NHS in the UK, the underlying principles regarding the dimensions and properties of appropriate outcome scales are applicable to other health care contexts . The arguments and data presented in this article are intended to be independent of the particular mode of service delivery, although the rationale for the devel-opment of the measure is phrased in the UK con-text . Where UK practice imposes limitations on the extent to which the findings might be gen-eralized, this is identified in the text .
BACKGROUND
n recent years, research into the prevalence and characteristics of hearing impairment,
disability, and handicap in the adult population and the extent to which current facilities within the UK NHS are taken up (Davis, 1995) has con-firmed the continuing high prevalence of disor-ders and low penetration of services . Thus, there will be a continuing need and pressure for the development of services to alleviate the dis-abilities and handicaps that accompany adults as they acquire (predominantly) sensorineural
hearing loss with advancing age . A number of fundamental issues arise :
1. To what extent are current hearing aids and associated services effective in the reduc-tion of hearing disability and handicap?
2 . To what extent are improvements in hear-ing aid services either possible or desirable, either in terms of the technology that is provided or the rehabilitation support that is available?
3. To what extent can hearing aid services be made more accessible and attractive to the two-thirds of realistic candidates who cur-rently make no use of their availability?
Questions such as these are part of the international audiologic agenda but have always encountered the difficulty that either in the research domain or in the domain of routine service monitoring there is an absence of rele-vant information. The information is lacking primarily with regard to outcome. In the absence of scales to evaluate current services and inter-ventions, it is not possible to make rational pol-icy decisions concerning the directions in which services might be developed in the future . Before such scales can be developed, there are a num-ber of scientific issues to be addressed concern-ing "what is an appropriate scale and what its properties should be." Unlike many areas of medical intervention, the auditory system has a relatively well-developed taxonomy of pathol-ogy leading to impairment-impairments hav-ing a consequent disability in terms of the individual's reduction in effectiveness on gen-erally useful tasks and eventual auditory hand-icaps in terms of the emotional, social, and psychological disadvantages. As such, audio-logic services are well placed to move beyond the traditional descriptions of structure and process for service organization .
When considering the uses to which mea-sures of outcome may be put, it is possible to identify at least three classes of eventual user or objective. It is now well established that the purchasing and provision of health care is best accompanied by measures of the standards of the services purchased and provided . The purchasers of services wish to assure themselves of the standard and quality of the services they secure from provider institutions, while the (hospital or clinic) providers themselves wish to be able to demonstrate the effectiveness of their services and internally to optimize their effectiveness and cost effectiveness. Thus, there is an increas-
81

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
ing requirement for outcomes appropriate for ser-vice monitoring purposes . The requirements of such an outcome are relatively clear. If data on services are to be gathered comprehensively, they have to be readily available and hence have to be gathered in clinical circumstances where time is limited. The collection of data not cen-tral to the patient's management is likely to be unwelcome and unproductive . Thus, the out-comes for such a purpose have to be simple and quick to acquire and must have a high degree of relevance and clinical face validity.
Although the work reported in this article takes place in the context of a requirement for outcomes in both self-report and performance domains and is linked to research and evalua-tion efforts as well as routine clinical practice (Gatehouse, 1997), the concentration here is on a clinically viable instrument for measuring the perceived benefits of hearing aid provision. The article is constructed around two linked studies. The first is used to verify the concepts to be incorporated in an eventual instrument, while the second optimizes and verifies a particular questionnaire for eventual clinical application .
STUDY 1: INVESTIGATION OF CONCEPTS IN AND COMPONENTS
OF BENEFIT
T he plan of the research called for collection of data from samples of individuals attend- ing hearing aid clinics to investigate the extent to which the services were successful in allevi-ating the disabilities and handicaps associated with hearing impairment, with a view to cali-brating, optimizing, and documenting the per-formance of self-report measures . It should be noted and emphasized at the outset that the research is not intended as a survey of current practice and effectiveness in practice but rather as a vehicle for the optimization of the outcome measures themselves . Two centers chosen for data collection were the Audiology Unit at the Withington Hospital in Manchester, England and the Audiology Department at the Royal Infirmary in Glasgow, Scotland . These sites were chosen because of the associated research expertise (Dr. Denzil Brooks in Manchester and the Scottish Section of the MRC Institute of Hearing Research in Glasgow) and the rela-tively high patient throughput in the clinical departments. During the course of managing patients, the clinics were free to adopt whatever methods they chose for the prescription, selec-
Clinic Visit : Assessment
Glasgow Manchester Combined n=1113 n=1003 n=2116
Clinic Visit : Fitting
Glasgow n = 1078
Glasgow n = 740
Manchester n=915
Combined n = 1993
Clinic Visit : Review
Manchester Combined n = 723 ( n = 1463
12 weeks
Research Visit : Self-report Questionnaire
Glasgow n = 596
Manchester Combined n = 347 n = 943
Glasgow Manchester Combined n=342 n=314 n=656
Figure 1 Structure of the research and numbers of patients at the various stages, separately for the Glas-gow and Manchester sites.
tion, and adjustment of hearing aids and clini-cal decisions regarding additional management .
Data Collection
For each of the host clinics, all individuals for whom provision of personal amplification was the management decision were entered into the research protocol, providing that they had not worn a hearing aid at any time during the 12 months prior to attendance at the clinic . Fig-
82

Glasgow Hearing Aid Benefit Profile/Gatehouse
ure 1 illustrates the flow of patients through the research protocol . Individuals attended the clinic on at least three separate occasions for (1) ini-tial assessment of their status and the decision as to whether management via a hearing aid was appropriate-the clinic assessment visit ; (2) a visit to the clinic at which the hearing aid was fitted and initially adjusted-the clinic fitting visit ; and (3) at least one follow-up visit to ensure the adequacy of the hearing aid provision and to institute any changes that may be required-the clinic review visit . Following discharge from the clinic, patients were invited to attend for spe-cific research visits, either at the Regional Audi-ology Unit at Withington Hospital or at the Scottish Section of the MRC Institute of Hear-ing Research . At these research visits, compre-hensive measures of outcome in the self-report and the performance domains were adminis-tered . These visits are referred to as the self-report research visit and the performance test research visit, respectively. Figure 1 shows the numbers of subjects separately for Glasgow and Manchester at each stage of the research . It can be seen that the attrition between the manage-ment decision to fit a hearing aid and the actual fitting of the hearing aid is relatively modest, while around three-quarters of the subjects were available for study at the follow-up stage in the clinic . Invitation to participate specifically in the research resulted in increased attrition rates, and it will be of subsequent importance to demonstrate the extent to which the eventual research samples are representative of the orig-inal clinical populations . In total, 943 individu-als attended at Manchester and Glasgow for the self-report research visit at which outcome measures in the self-report domain were obtained . It is on this subsample that the analy-ses in this article are based . The overall report (Gatehouse, 1997) contains a comprehensive description of and protocols for the data at the self-report research visit for the current analy-sis . That visit itself contained other condition-specific measures of disability, handicap, and benefit in addition to generic measures of health-related quality of life .
Audiometric Measures
Pure-tone thresholds for air conduction and bone conduction were assessed at the clinic assessment visit using established procedures and protocols recommended by the British Soci-ety of Audiology for practice in the UK (British Society ofAudiology, 1985, 1986, 1989) . In addi-
tion, thresholds for uncomfortable listening for pure-tone sinusoidal signals were assessed using a similar protocol (British Society of Audiology, 1987) .
Hearing Aid Fitting
Hearing aid fitting was performed accord-ing to the normal procedures and protocols in place at the host clinics . These procedures were not monitored explicitly during the research as part of the original agreement with the host clinics . The research did, however, document practice with regard to the major classifications of hearing aid, earmold type, and fitting . At the self-report research visit, real-ear insertion gain measures were derived from the hearing aid for three input signals with spectral characteristics similar to that of a standard long-term speech spectrum at three presentation levels of 55, 65, and 75 dB SPL.
Hearing Disability and Aid Benefit Interview
In constructing the Hearing Disability and Aid Benefit Interview (HDABI), it was decided to attempt to retain the potentially indepen-dent components of benefit that had been iden-tified [Brooks (1990) and that Oja and Schow 19841 and our own data had shown to be differ-entially informative (Gatehouse, 1994) . The HDABI contains 14 common listening circum-stances or communication situations that, from previous pilot data, were likely to occur in the lifestyles of the patients attending the host clin-ics . For each of these 14 listening circumstances, each listener was asked seven questions, the first of which attempted to ascertain whether the listening circumstances occurred in the listener's experienced lifestyle and, if so, the frequency of occurrence . This first aspect attempts to over-come one of the fundamental disadvantages in traditional self-report measures of disability and benefit : the questionnaires all consist of a fixed list of listening situations for which the patient is required to rate some aspect of dis-
ability, handicap, or benefit . For any particular listener, many of these situations may be irrel-
evant because they simply are not experienced. Even if they are experienced, they may be expe-rienced only infrequently, or they may not be situations in which the client considers com-munication function to be very important. Even if communication is important, the listener may already experience little difficulty in any given
83

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
situation, so measurement of hearing aid ben-efit in that situation may be irrelevant . This then leads to the motivation for the inclusion of the first dimension of the HDABI: that of occur-rence of the situation itself. Note that if the sit-uation does not occur in the subject's lifestyle, all of the subsequent six dimensions are omit-ted from further consideration . (For the format and structure of the responses in the HDABI, refer to Appendix A.)
The second dimension addressed is that of preintervention hearing difficulty (disability). For each of the circumstances that occur in the sub-ject's experience, they are asked to rate the degree of hearing difficulty that they have in that particular situation, using five alternatives rang-ing from "no difficulty" to "cannot manage at all." Third, for situations that occur in the listener's experience (dimension 1) and also lead to a nonzero degree of hearing difficulty (dimension 2), listeners are asked to rate the degree of annoyance or upset (hearing handicap) of the hearing impairment and disability (i .e ., the impact on the hearing-impaired listener).
Having assessed the three dimensions of occurrence, disability, and handicap prior to intervention, the aid benefit interview then turns to four aspects of benefit and postinter-vention state. The first of these concerns hear-ing aid use . For each listening circumstance that exists in the subject's experience and prior to intervention led to a nonzero hearing difficulty, the subject is asked to report the degree of hear-ing aid use, using five alternatives ranging from "never" to "all of the time." Note that these responses differ fundamentally from the reported hearing aid use as used in most other benefit questionnaires (e.g., Brooks, 1990). There, the subject is asked to report on the absolute hours of use that they choose to wear the hearing aid. In the current aid benefit interview, for each of the relevant listening circumstances, the subject is asked to indicate the proportion of the time that they choose to use their hearing aid for those listening circumstances that prior to inter-vention exist and lead to hearing difficulty. Such a process concentrates information regarding hearing aid use on those situations that exist in a listener's auditory ecology, are important, and lead to a material difficulty.
Following the assessment of hearing aid use, the listener is asked a question concerning the benefit that is delivered by the wearing of the hearing aid for each specific listening cir-cumstance. The listener is asked "how much does your hearing aid help you" for each lis-
tening circumstance and is given six response alternatives ranging from "hearing aid makes things worse" through to "I can hear perfectly normally with the hearing aid for this situation." Note that this is a benefit, change, or a differ-ence question that accesses the extent to which things are better now following the intervention than they were prior to the intervention. In the analysis of the HDABI, the number of times that the subject used response alternative number 1 (hearing aid makes it worse) and response alternative number 2 (hearing aid no use at all) were relatively small, and it was inappro-priate to distinguish between the two response alternatives . Therefore, for the purposes of analysis they were amalgamated and the even-tual response scale restricted to five applicable alternatives . Following the assessment of ben-efit (extent to which hearing in this situation has been helped), subjects then report on the degree of residual disability (following intervention, how much difficulty do they have left for a par-ticular listening circumstance). Thus, the aid benefit interview assesses postintervention residual disability in addition to postinterven-tion benefit. Finally, for each of the situations that prior to intervention occurred and led to a hearing difficulty, listeners are asked to rate their degree of satisfaction with their hearing aid on a 5-point scale ranging from "not satis-fied at all" to "delighted with the hearing aid for this situation."
This process is repeated for each of the 14 communication circumstances that contribute to the HDABI. It has been argued elsewhere (Dil-lon et al, 1991, 1997 ; Gatehouse, 1994) that unless a self-report questionnaire contains an inordinately large number of prespecified lis-tening circumstances (and thereby carries the danger of a large number of potentially irrele-vant circumstances), it is unlikely to access all of those listening circumstances for a specific individual for which it is important for the lis-tener to be able to communicate effectively. Therefore, the HDABI contains the opportunity for the subject to specify a further four listening circumstances, for each of which the seven pre-viously described dimensions are accessed . This is done using instructions as follows: "We have dealt with a number of listening circumstances for which in our experience it is important for people to be able to hear and communicate effec-tively. However, we realize that not all of these will necessarily apply to you, and may not cover the situations that are important to you. What we would like you to do is to specify up to four
84

Glasgow Hearing Aid Benefit Profile/Gatehouse
further listening situations for which it is impor-tant for you as an individual to be able to hear and communicate as well as possible." Follow-ing the specification of the listening circum-stances, the same seven dimensions are accessed .
The questionnaire now consists of (poten-tially) 18 listening circumstances (listed in Table 1) for each of which there are the seven dimen-sional answers. From the data, a total of seven summary indices are derived, each of which is configured to vary between 0 and 100 on an arbitrary scale. The first of these is labelled auditory exposure and aggregates the responses to the 14 prespecified listening circumstances and the (up to four) subject-specified listening circumstances. Thus, an eventual score of 0 would correspond to none of the listening cir-cumstances ever occurring, and an eventual score of 100 would correspond to each of the lis-tening circumstances occurring for over 4 hours every day.
A second summary index labelled initial disability is derived from the subset of the 14 pre-specified listening circumstances that occur in the listener's experience and the (up to four) subject-specified listening circumstances . Thus, the number of listening circumstances that con-tribute to the disability scale will be a function of the particular listening experience and envi-ronment of each individual . For each individual, the responses are scaled and aggregated so that the resultant disability scale could vary between 0 and 100, with 0 corresponding to "no diffi-
Table 1 Listening Situations Used in the Hearing Disability and Aid Benefit Interview
Listening to the television on your own Listening to the television with other family or friends when the volume is adjusted to suit other people
Having a conversation on the telephone Listening at the cinema or bingo Understanding speech in a pub club or meeting Carrying on a conversation in a busy street or shop Listening to music Following a lecture or service in church Understanding speech in a car or bus Understanding children's voices Having a conversation with one other person when there
is no background noise Having a conversation with several people in a group Understanding speech on the radio Understanding what is said at work Listener-specified situation 1 Listener-specified situation 2 Listener-specified situation 3 Listener-specified situation 4
culty" in any of the listening circumstances that happen to exist in that listener's experience, and a score of 100 corresponding to "cannot manage at all" in all of the listening circum-stances within that listener's experience . Thus, the reported difficulty scale is normalized accord-ing to the number of occurring circumstances . In a similar manner, the summary scale hear-ing handicap is derived from those listening cir-cumstances that occur and for which a nonzero hearing difficulty was reported by the listener. The hearing handicap is the overall impact upon the subject of the hearing impairment from which they suffer and the hearing disability that they experience .
Fourth, for each of the circumstances that existed prior to intervention and for which a nonzero hearing difficulty was reported, the overall level of proportional hearing aid use is derived, once again on a scale of 0 to 100, nor-malized for the particular individual . Here a score of 0 corresponds to never using the hear-ing aid in any of the listening circumstances that prior to intervention caused difficulty, a score of 50 using the hearing aid about half of the time, and a score of 100 using a hearing aid all of the time .
For this same set of listening circumstances, the benefit measure is scaled between 0 and 100 . Note that the response alternatives are now restricted to "hearing aid no use at all," "hearing aid is some but not much help," "hear-ing aid is quite helpful," "hearing aid is a great help," and "hear perfectly normally with hear-ing aid in this situation ." This structure attempts to provide a potential upper bound on the reported benefit scale so that an eventual score of 100 will correspond to the listeners' percep-tions that they can now function perfectly nor-mally with their hearing aid in each and every one of the listening circumstances that prior to intervention led to a hearing difficulty, and that a score of 0 corresponds to the hearing aid deliv-ering no benefit for each of those listening circumstances .
The scale of residual disability contains the same response alternatives as the preinterven-tion disability and for each individual listener again ranges potentially between 0 and 100. The objective of a residual disability (as opposed to a benefit) scale will be of potential application in attempting to address the issue of overall effectiveness of services in their primary aim of returning the auditory abilities of impaired indi-viduals to those enjoyed by their nonimpaired peers in the population .
85

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
It is one of the contentions of this research that both the directly accessed benefit scale and a derived benefit scale (formed by differencing the residual disability and the initial disability scales) have their applications . It is suggested that the benefit scale will be maximally sensi-tive for the comparison of different interven-tions because the difference between the two specific scales will have variance contributions from both components and will suffer from end-scale effects. However, at this stage this remains a contention to be empirically investigated .
Finally, an overall scale of satisfaction rang-ing from 0 to 100 is derived, with 0 correspond-ing to reports of no satisfaction at all for each of the listening circumstances that prior to inter-vention led to hearing difficulty, and a score of 100 corresponding to a report of delight with the hearing aid for each of those same situations . After completion of the HDABI, listeners were asked to rank the order of importance for each listening circumstance in their everyday lifestyle. Unlike the specific scale of "importance" in Gate-house (1994), the ranking of importance of each communication circumstance in this data is not explicitly scored or analyzed . Rather, it is used in a subsequent derivation and assessment of a shortened benefit instrument appropriate for clinical rather than research use . Thus, the seven indices from the HDABI are derived from a mixture of prespecified and subject-specified listening circumstances associated with com-munication function.
Hearing Aid Technical Data
At each of the clinic visits and the research visits at which the hearing aid is worn, the per-formance of the hearing aid is assessed using a clinical probe tube system to assess the real-ear insertion gain of the amplification device (i .e ., the extent to which on a frequency-by-frequency basis the hearing aid amplifies sound arriving at the tympanic membrane when the hearing aid is worn by the listener, compared to the unaided acoustic situation) . (For a review see Mueller et al, 1992.) There is a widespread literature (e.g., Berger, 1990, 1991 ; Rankovic, 1991) on the use of a measure of audibility, referred to as the Articulation Index (ANSI, 1969), or a subse-quent development, the Speech Intelligibility Index (SII) (ANSI, 1993), in the assessment and selection of amplification devices. The SII pro-vides a single measure of the extent to which a speech spectrum is available to the auditory system for further processing . As such, it is a
measure of the audibility of speech rather than the intelligibility of speech . Thus, an SII of zero corresponds to a situation whereby all of the speech spectrum of interest is below threshold and hence unavailable to the auditory system, and an SII of unity corresponds to a situation whereby all of the speech spectrum is available to the auditory system for processing. The pro-cedures and calculations incorporated in ANSI (1993) were implemented and yielded SII values for input signals of 55, 65, and 75 dB SPL prior to intervention (unaided) and corresponding values following intervention (aided). The dif-ference between the unaided and aided SII val-ues is a measure of the technical benefit conferred by the hearing aid (i .e ., the extent to which a speech spectrum has been made more audible by the hearing aid than it was prior to the fitting of the device). Note that each of the real-ear insertion gain values is gathered at a volume control setting that the subject chooses to wear for the hearing aid and, to that extent, the procedure will not be contaminated by arti-ficially high SII values . Thus, the procedure does truly provide a technical measure of the extent to which speech signals have been made audible but not uncomfortably loud as experi-enced by the hearing-impaired listener. Through-out this article, the SII data for a 65 dB SPL input signal is used.
Description of the Sample
Figure 1 shows the attrition of the subject sample as they progressed in both Glasgow and Manchester from the clinic assessment visit through to the self-report research visit . Although respectable numbers are still available, these are substantially less than those who entered at the clinical assessment visit. There-fore, it is required to demonstrate that the even-tual sample is representative of those who entered the initial stages of the research . Tables 2 and 3 contain a descriptive summary of the audiometric profiles separately for the Glasgow and Manchester clinics of the subjects at the dif-ferent stages of the research design. Inspection of Tables 2 and 3 and formal statistical com-parisons show that there are no systematic dif-ferences in overall audiometric characteristics between the Glasgow and Manchester clinics and that the attrition from the clinic assess-ment visit through to the performance test research visit has not resulted in any material biases in the audiometric profile. Thus, the sam-ple upon which the data are collected can be
86

Glasgow Hearing Aid Benefit Profile/Gatehouse
Table 2 Summary of the Hearing Levels for the 2116 Subjects Seen
at the Clinic Assessment Visit
Manchester Glasgow
Mean SD Mean SD Gender Male
Left ear AC (dB HL) Female 250 Hz 41 .4 20.6 43 .3 21 .8 Household occupational group 500 Hz 41 .6 21 .1 42 .3 21 .9 Manual 1000 Hz 43.0 22 .2 43 .5 21 .9 Nonmanual 2000 Hz 48.9 21 .7 50 .3 20 .9 Tinnitus 4000 Hz 62.5 21 .9 64 .3 21 .4 None 8000 Hz 73.8 27 .5 75 .5 27 .7 Mild
Right ear AC (dB HL) Moderate 250 Hz 43.4 21 .8 41 .4 20.5 Severe 500 Hz 42.3 21 .9 41 .6 21 .1 Monaural fitting 1000 Hz 43.5 21 .9 43 .0 22.2 Binaural fitting 2000 Hz 50.3 20 .9 48.9 21 .7 Mold type 4000 Hz 64.3 21 .4 62 .5 21 .9 Shell 8000 Hz 75 .5 27 .7 73 .8 27 .5 Skeleton
Open Other
regarded as representative of the clinical target population .
Table 4 contains demographic and bio-graphical characteristics of the two clinic sam-ples . In Glasgow, there is a preponderance of
females over males, which is roughly reversed in Manchester, and significant differences in the proportion of manual as opposed to non-manual occupations between the two clinics . These differences in occupational characteristics reflect the catchment populations covered by
the two host clinics . There are other differences
Table 3 Summary of Hearing Levels for the 943 Subjects Seen at
the Self-Report Research Visit
Manchester Glasgow
Table 4 Clinical Summary Data for the 943 Subjects Seen at the Self-Report Research Visit
Vent None Comfort Acoustic
Horn Acoustic filter
Manchester M.)
Glasgow (/o)
53 .3 46 .4 46.7 53 .6
41 .8 62 .1 58.2 37 .9
69.4 66.4 21 .8 19 .1 7 .8 11 .1 1 .0 3 .4
95.6 91 .3 4.4 8.7
25.3 89.9 62.9 9.0 10 .4 0.4
1 .4 0 .8
57.6 93 .1 12 .1 5 .2 69 .7 1 .7 4.4 15 .4 8.7 0 .4
in practice at the two clinics, which become apparent from Table 4.
Table 5 provides a more comprehensive dis-tribution of the audiometric and age character-istics of the eventual samples (for Manchester and Glasgow combined) when the air-conduction frequencies are averaged across the frequen-cies of 500, 1000, 2000, and 4000 Hz. It can be seen that the median hearing levels for the bet-ter, poorer, and fitted ears show that first-time attendees are predominantly those with mod-erate hearing impairment . The 90th percentile for the four-frequency average in the fitted ear
Mean SD Mean SD
Left ear AC (dB HL) Table 5 Distribution of the 943 Subjects 250 Hz 42 .6 20 .4 42 .9 21 .4 at the Self-Report Research Visit 500 Hz 40 .1 20 .9 42 .8 21 .9 1000 Hz 44 .2 27 .3 44 .1 27 .1 2000 Hz 50 .2 21 .7 51 .8 21 .7 Percentiles
4000 Hz 62 .1 21 .9 66.2 21 .8 10th 25th Median 75th 90th 8000 Hz 77 .2 21 .2 78.4 26 .2
Right ear AC (dB HL) Better ear AC dB HL 25.0 32 .5 41 .3 50.0 57 .5
250 Hz 42.0 21 .8 40 .9 20 .4 (0 .5-4 kHz) 500 Hz 43.6 21 .8 41 .8 21 .6 Poorer ear AC dB HL 36.3 44 .8 52 .5 65 .0 81 .3
1000 Hz 44 .1 20 .9 43.4 22 .7 (0 .5-4 kHz) 2000 Hz 51 .2 21 .0 49.6 20 .9 Fitted ear AC dB HL 32.5 40 .0 47.5 57.5 68 .8 4000 Hz 65 .1 22 .1 64 .1 20 .9 (0 .5-4 kHz) 8000 Hz 77.2 26 .7 74 .7 25 .3 Age (yr) 48.0 60 .0 69.0 77.0 82 .0
87

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
is approximately 69 dB and, therefore, only some 10 percent of the eventual sample can be regarded as having severe hearing impairment . Table 5 provides the context within which the various outcomes that will be discussed in sub-sequent applications have to be appreciated and interpreted.
Performance of Outcome Measures
Development of a Criterion
This article now aims to identify the extent to which the outcomes from the HDABI can be used as a measure with which to judge the effec-tiveness via intervention of adult hearing aid fit-tings and services. The realization of such an aim is a nontrivial task. The validation of any out-come measure depends critically on a criterion or set of criteria against which its performance can be judged . The literature on hearing aid outcomes (e.g ., see Newman and Weinstein, 1988; Dillon et al, 1997) adopts a variety of cri-teria because of the absence of any recognized "gold standard" against which to assess indi-vidual candidates . This absence of a gold stan-dard leads to some potential problems and a philosophy for dealing with them is required . (For a general consideration of the validation process, see Streiner and Norman [1989].) Con-ventional approaches to validity (Newman and Weinstein, 1988 ; Dillon et al, 1997) will address the concepts such as content and construct valid-ity, aspects of scale reliability, and aspects of test-retest reliability. These, coupled with the high face validity of the items and a simple demonstration of a reduction in disability/hand-icap following intervention, have almost always been taken as sufficient evidence of the suit-ability of the scale as a measure of outcome . However, it is argued here that such an approach is fundamentally incomplete because it pays no attention to a consideration of the purposes for which the outcome measure is required . Although this has already been discussed briefly, as it forms the crux of these analytical sections, it will be investigated in a little more detail here .
Hearing aid fittings and services within any context can conceivably be restricted, amended, or developed by changes either in the amplification technology that is employed or by the manner and context within which it is used as part of the rehabilitation process for hearing-impaired listeners . Thus, a fundamental requirement of any appropriate outcome mea-
sure is that the scale should exhibit sufficient discriminatory power to be able to distinguish between different modes of service orientation and different technical properties or parameters of the amplification devices that are used . It has to be acknowledged that such a criterion pre-supposes a prior knowledge of what might be considered superior and inferior forms of tech-nical device and/or service organization if they are to be used as part of the validation process itself. This element of circularity does carry its own dangers, but if approached with caution it can be used to differentiate between different outcome scales .
In developing this context, it is suggested that there are two assumptions or axioms that can be put forward. These are:
Across very large numbers of subjects, hear-ing disability and handicap should, on aver-age, increase monotonically with increasing levels of hearing impairment. Increased perceptions of improved outcome on the part of hearing-impaired listeners should be systematically related to increasing improvements in the audibility of the speech signal induced by the hearing aid.
These axioms require some justification . They do not attempt to undermine in any way the realization that individuals of similar hear-ing impairment will experience different degrees and types of hearing disability and handicap (Stephens and Hetu, 1991). Such a perception is well founded in both theory and practice . However, what the first axiom does suggest is that if one has data on a very large number of individuals who have hearing levels, say, in the 60 to 65 dB HL range, then they should experi-ence greater degrees of hearing disability and handicap to a similar number of subjects in a group of individuals (who will be identical in as many respects as is conceivably possible) with average hearing levels in, say, the 50 to 55 dB HL range. That is, once the individual factors that lead to hearing disability and handicap have been accounted for by the availability of large datasets, the more impaired are a group of individuals, then the greater the consequent disability and handicap .
It is suspected that most readers will find such a contention unobjectionable. However, the second axiom, although based upon the same general principle, has in the past received less widespread approval . The axiom relies on the argument that as the amount of a signal (that
88

Glasgow Hearing Aid Benefit Profile/Gatehouse
the subject wishes to hear) that was previously partially or totally unavailable to the listener is then made available by the amplification device increases, then the greater will be the perceived benefit . Thus, if two groups of individuals with similar audiometric and other characteristics are fitted with hearing aids, then the group for whom the improvements in the audibility of speech are materially greater will derive more perceived benefit and improved outcome than the
group of individuals for whom the improvements in the audibility of speech are inferior (assum-ing other aspects of the signal-such as distor-tion characteristics-remain comparable) . Note that this should not be taken as a materialistic formula for the prescription of the maximum gain possible (although some prescription regimes do attempt such an argument) but rather an assessment of the outcome . Such an axiom crucially relies on the assessment of the audibility of speech in ways that are relevant to the everyday use of hearing aids by hearing-impaired listeners . Thus, the measure of outcome has to take place in the context of the gain set-tings that the hearing-impaired listeners' habit-ually use and have access to, and also in the context of speech signals to which the hearing-impaired listener is routinely exposed . Thus, in this context it is argued that one set of the val-idation criteria against which an outcome mea-sure can be sensibly assessed is that after control for subject-related variables and aspects of the initial impairment, there should be a systematic relationship between the degree of benefit per-ceived by the hearing-impaired listener and the improvements in audibility introduced by the hearing aid .
In this context, the SII is used as one of the validating criteria . Note that it is necessary to institute a statistical control for the initial impairment level to ensure that any residual cor-relation with hearing level is removed and arte-facts associated with greater degrees of impairment having greater degrees of initial disability and hence the opportunity to report greater degrees of benefit are removed from the analysis . Few examples exist in the literature of such an approach and are only made possible in this research by the availability of large num-
bers of subjects to achieve the statistical lever-age required . Table 6 contains data showing the distribution of SII scores for an input signal of 65 dB SPL (normal conversational speech) for the unaided and the aided conditions as collected from the 943 subjects at the self-report research visit . The table also contains the derived bene-
Table 6 Distribution of the Speech Intelligibility Index for an Input
Signal of 65 d13 SPL
Speech Index
Intelligibility Unaided (%)
Aided (%)
Improvement (%)
< .05 101 12 .0 1 .5 19 .2 05-.15 [ .10] 10 .8 2 .2 29 .1 15-.25 [ .20] 12 .0 3 .4 25 .7 25-.35 [.301 14 .3 9.1 17 .1 35-.45 [ .40] 14 .7 11 .2 6 .3 45-.55 [ .50] 13 .1 17 .1 2 .2 55-.65 [.601 8.8 19 .3 0.5 65-.75 [ .701 9 .1 21 .6 - 75-.85 [80] 2.3 10 .3 - 85-.95 [ .90] 1 .0 3.8 - > .95 [1 .0] 1 .9 0 .4 -
fit (improvement) in the SII by differencing the
aided and unaided values . Table 6 contains the background data for the range of SII values that can be used as part of the validation process. Comparison of the unaided and aided columns confirms that amplification improves the SII across the subject pool, with a greater propor-tion of listeners enjoying increased access to the speech spectrum . The improvement column in Table 6 demonstrates that the majority of listeners experience improvement in speech audibility in the range of .05 to .25 . In addition to the range values for the SII in Table 6, the table contains for each range a value in square brackets that represents the "bin center" for a particular range of SII data . Thus, a bin center represented as [ .101 is equivalent to a range of values from .05 through to . 15 . (As a shortform representation of the value ranges, the numbers in square brackets will be employed hereafter.) It is perhaps noteworthy from Table 6 that sig-nificant numbers of listeners enjoy improve-ments in SII values that are less than .05 using the current technology in the host clinics and the available methods of adjustment, at least for a 65 dB SPL input level .
Table 7 shows the distribution of SII improvements for five ranges of impairment level in the fitted ear and confirms the require-ment to control for the impairment level in the
fitted ear as progressive increases in the impair-ment level are associated with progressively greater degrees of improvement in the SII until the data plateau at the more severe impair-ments . Thus, when individuals with mild losses are fitted with current technology, the combi-nation of the mild nature of the hearing loss and
89

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
Table 7 Distribution of Improvements in Speech Intelligibility Index for Bands of
Impairment Level in the Fitted Ear
Outcomes from Hearing Disability and Aid Benefit Interview
Improvement in Speech Intelligibility Index (%) Fitted Ear AC
(0.5-4 kHz) [0] [10] [20] (.30] [40] [.50]
<35 dB 40.4 29.8 13 .5 12 .9 3 .4 - 35-45 dB 16.4 36.0 30 .2 13 .2 3 .2 1 .0 45-55 d B 9 .7 25.4 29 .8 23.8 8 .9 2 .0 55-65 dB 3 .4 19 .5 37 .3 21 .2 13 .6 5 .1 >65 dB 7 .4 18 .8 23 .2 24.6 15 .2 8 .7
the restricted frequency characteristic of the hearing aids results in only modest improve-ments in speech audibility, while at the more severe end of the hearing-impaired spectrum, the very severity of the hearing impairment itself limits the improvements in audibility that can be delivered to hearing-impaired listeners. It is worth noting in passing that had a rigid pre-scription and aid selection regime been in place in the Manchester and Glasgow clinics, then Table 7 would have condensed the range of improvement in speech audibility for each impairment range . The improvements would have been more tightly coupled to impairment . Thus, the clinical variability found in these NHS clinics actively facilitates the research by decou-pling the improvements in audibility from the initial impairment level. The residual correla-tion between impairment level and improve-ment in audibility requires control hereafter, however. It should also be noted that the assump-tions underlying the SII are not fulfilled by amplification regimes such as fast-acting wide dynamic range compression in more than one channel. Had the UK NHS based its practice on such devices rather than the almost universal application of postaural linear devices, then this criterion would have required modification .
A precursor to the current HDABI (described in Gatehouse, 1994) has demonstrated the abil-ity to provide scientific insights into the struc-ture and determinants of hearing disability and handicap and the benefit delivered by the pro-vision of amplification. However, the motiva-tion for that research was a desire to gain a better understanding of disabilities and handi-caps and the ways in which these might be alle-viated (or, perhaps more importantly, not be successfully approached) using current service models . Potential candidates for benefit mea-sures include the reported aid use, reported benefit, satisfaction, and the derived benefit scale (from the difference between initial dis-ability and residual disability scales). Data from the 943 listeners are shown in Table 8. Each of the scales has an available range from 0 to 100. For example, the median score of 70.2 on the reported aid use scale corresponds to 50 percent of the subjects using their hearing aid for greater than 70 percent of the time when they find themselves in listening circumstances that prior to intervention existed in their listening expe-rience and led to a nonzero hearing difficulty. By the same token, almost 25 percent of subjects only use their hearing aid in half of such simi-lar circumstances. The median score for reported benefit is close to 50 percent, which corresponds to listeners reporting the hearing aid as, on average, being "quite helpful" for the listening circumstances that exist in their lifestyle and led to nonzero hearing difficulty prior to interven-tion. Note that the values for the derived bene-fit scale (derived, that is, by taking the difference between the initial disability scale and the resid-ual disability scale) has a median value in the range of 20 to 25 percent, which corresponds closely to only one category shift in the state dis-ability scale.
The next step is to apply the audibility cri-terion developed in the previous section to the
Table 8 Distribution of Scores from the Hearing Disability and Aid Benefit Interview
Initial Reported Reported Residual Derived Disability Handicap Aid Use Benefit Satisfaction Disability Benefit
25th percentile 24.7 11 .1 49.7 38.2 46 .1 14 .1 9 .6 50th percentile 42.3 24.6 70.2 51 .6 60.4 20 .9 24 .6 75th percentile 59.9 51 .0 86.9 65.2 72.9 32 .6 40 .1

Glasgow Hearing Aid Benefit Profile/Gatehouse
outcome scales from the HDABI. As previously mentioned, control for the impairment level in the fitted ear is necessary because of the asso-ciation between that impairment and the improvement in the SII (as illustrated in Table 7) . To achieve that control, the impairment level is categorized in 5-dB bands and used as the independent variable in a one-way analysis of variance (ANOVA) . A subsequent ANOVA then uses the predicted score on the outcome variable from the first analysis as the dependent variable and the improvement in the SII as the inde-pendent variable, categorized in bands of width 0.1 . Following that analysis, a series of post hoc tests is conducted between each combination of the categories for improvement in SII using Tukey's Honestly Significant Difference Test . This procedure is robust, conservative, and applicable to each of the outcome measures, independent of the form of the relationship between the improvement in audibility and the outcome measure (or indeed the form of the con-trol for impairment level) . Thus, nonlinear as well as linear relationships can be accommo-dated in ways that are not available for linear modeling techniques . The comparison between each pair of cells for improvement in SII yields information regarding the ability of the out-come measure to discriminate between those cells and includes (a) the mean difference between the cells, (b) the standard error of that difference, (c) the significance level associated with that difference, and (d) the lower and upper bounds of the 95 percent confidence interval for that difference . In addition, each overall analy-sis yields (a) the mean square, (b) the residual, (c) the F value and associated degrees of freedom, (d) the accompanying significance level, and (e) the percentage of the variance accounted for via the overall goodness of fit of the model . This wealth of statistical detail is in danger of over-whelming the reader and could compromise the perception of the central message arising from the analyses . Therefore, a qualitative presen-tation of the quantitative statistical procedures has been adopted .
Table 9 contains such a summary for the reported use scale of the HDABI and cross-tab-ulates the improvements in SII. Each cell of the cross-tabulation contains a diagrammatic rep-resentation of the extent to which the post hoc comparisons achieve statistical significance . Thus, for Table 9, the reported use scale can dif-ferentiate between SII improvements centered on [0] and those of [2] at p < .05 and between SII improvements of [0] and those at [.3], [4],
Table 9 Cells That Can be Statistically Distinguished on a Multiple Comparison Analysis for the Reported Use Scale from the Disability and Hearing Aid Benefit
Interview after Control for Impairment Level in the Fitted Ear
Imp
101
roveme
[1]
nt in Spe
[21
ech Intel
[31
ligibility Index
[41 [5
[0] n/a Ill n/a [2] n/a [ .3] n/a [.4] n/a [ .5] n/
*p < .05, -p < .01
and [.5] at p < .01 . The format of Table 9 allows a ready appreciation of the discriminatory power of an individual outcome measure by identifi-cation of "nonempty" cells and the symbol asso-ciated with a particular level of statistical significance . The form and presentation of these analyses are referred to as "multiple compari-son analysis ." Table 9 demonstrates clearly the discriminatory power of the reported use scale from the HDABI. Tables 10, 11, and 12 contain the qualitative summaries from similar analy-ses using the reported benefit, satisfaction, and derived benefit scales from the HDABI as the dependent variable .
The reported benefit scale also shows high discriminatory capability, which is not a surro-gate artefact associated with impairment level. While the satisfaction scale has poorer dis-criminatory power, it does still achieve levels of
Table 10 Cells That Can be Statistically Distinguished on a Multiple Comparison Analysis for the Reported Benefit Scale from the Hearing Disability and Aid Benefit Interview after Control for Impairment Level in the Fitted Ear
Imp
l01
roveme
Ill
nt in Spe
[2]
ech Intel
[3]
ligibility Index
G4] [-5
[01 n/a 1.11 n/a [ .2] n/a [3] n/a [.4] n/a [ .5] n/
*p< .05, "p< .01
1
a
1
a
91
Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
Table ll Cells That Can be Statistically Distinguished on a Multiple Comparison
Analysis for the Satisfaction Scale from the Hearing Disability and Aid Benefit Interview after Control for Impairment Level in the Fitted Ear
Imp
[01
roveme
G 1]
nt in Spe
[2]
ech Intel
L31
ligibility Index
[4] [5
[0] n/a 1.11 n/a [2] n/a [ .3] n/a [ .4] n/a [ .5] n/
*p< .05, "p< .01
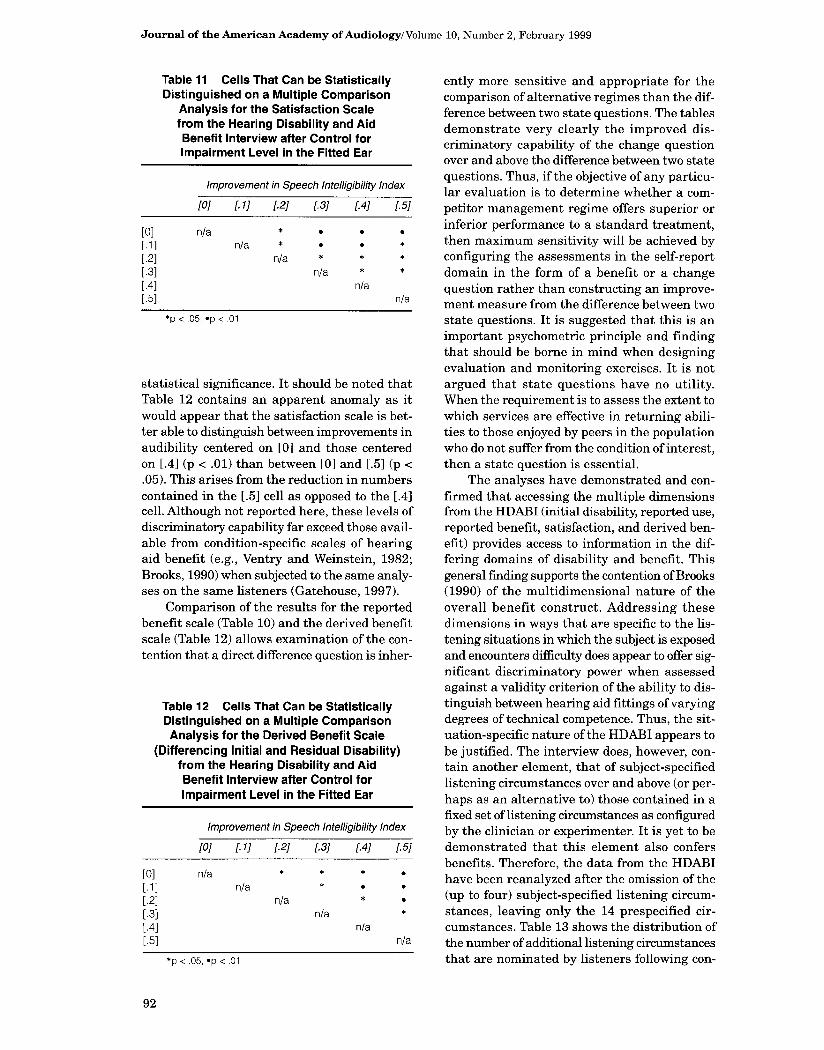
statistical significance. It should be noted that Table 12 contains an apparent anomaly as it would appear that the satisfaction scale is bet-ter able to distinguish between improvements in audibility centered on [0] and those centered on [.4] (p < .01) than between [0] and [ .5] (p < .05) . This arises from the reduction in numbers contained in the [.5] cell as opposed to the [.4] cell. Although not reported here, these levels of discriminatory capability far exceed those avail-able from condition-specific scales of hearing aid benefit (e.g ., Ventry and Weinstein, 1982 ; Brooks, 1990) when subjected to the same analy-ses on the same listeners (Gatehouse, 1997).
Comparison of the results for the reported benefit scale (Table 10) and the derived benefit scale (Table 12) allows examination of the con-tention that a direct difference question is inher-
Table 12 Cells That Can be Statistically Distinguished on a Multiple Comparison Analysis for the Derived Benefit Scale
(Differencing Initial and Residual Disability) from the Hearing Disability and Aid Benefit Interview after Control for Impairment Level in the Fitted Ear
Improveme
[0] [ 1 ]
nt in Spe
[2]
ech Intel
[31
ligibility index
[41 [5
[0] n/a Ill n/a [2] n/a [ .3] n/a [ .4] n/a [ .5] n/
*p< .05, "p< .01
92
]
a
1
a
ently more sensitive and appropriate for the comparison of alternative regimes than the dif-ference between two state questions. The tables demonstrate very clearly the improved dis-criminatory capability of the change question over and above the difference between two state questions. Thus, if the objective of any particu-lar evaluation is to determine whether a com-petitor management regime offers superior or inferior performance to a standard treatment, then maximum sensitivity will be achieved by configuring the assessments in the self-report domain in the form of a benefit or a change question rather than constructing an improve-ment measure from the difference between two state questions. It is suggested that this is an important psychometric principle and finding that should be borne in mind when designing evaluation and monitoring exercises. It is not argued that state questions have no utility. When the requirement is to assess the extent to which services are effective in returning abili-ties to those enjoyed by peers in the population who do not suffer from the condition of interest, then a state question is essential.
The analyses have demonstrated and con-firmed that accessing the multiple dimensions from the HDABI (initial disability, reported use, reported benefit, satisfaction, and derived ben-efit) provides access to information in the dif-fering domains of disability and benefit . This general finding supports the contention of Brooks (1990) of the multidimensional nature of the overall benefit construct . Addressing these dimensions in ways that are specific to the lis-tening situations in which the subject is exposed and encounters difficulty does appear to offer sig-nificant discriminatory power when assessed against a validity criterion of the ability to dis-tinguish between hearing aid fittings of varying degrees of technical competence . Thus, the sit-uation-specific nature of the HDABI appears to be justified . The interview does, however, con-tain another element, that of subject-specified listening circumstances over and above (or per-haps as an alternative to) those contained in a fixed set of listening circumstances as configured by the clinician or experimenter. It is yet to be demonstrated that this element also confers benefits . Therefore, the data from the HDABI have been reanalyzed after the omission of the (up to four) subject-specified listening circum-stances, leaving only the 14 prespecified cir-cumstances . Table 13 shows the distribution of the number of additional listening circumstances that are nominated by listeners following con-

Glasgow Hearing Aid Benefit Profile/Gatehouse
Table 13 Distribution (%) of the Number of Subject-specified Listening Circumstances in the Hearing Disability and Aid Benefit Interview
0 4 .6 1 10 .0 2 25 .1 3 37.4 4 21 .9
sideration of the fixed 14 communication envi-ronments . It has to be remembered that the data in Table 13 are of necessity only appropri-ate in the context of the 14 prespecified cir-cumstances.
Table 14 contains the results of a multiple-comparison analysis analogous to that presented in Table 10 for the reported benefit scale of the HDABI, but here using only data from the 14 prespecified listening circumstances . Compari-son of Tables 10 and 14 shows that the inclusion of the four subject-specified listening circum-stances does improve the ability of the benefit scale to achieve the test of criterion ability in terms of the ability to discriminate between hearing aid prescriptions of varying degrees of technical competence .
STUDY 2: DEVELOPMENT OF AN OUTCOME MEASURE
FOR CLINICAL USE
n developing a shortened outcome instru-ment in the self-report domain, a number of
pragmatic criteria are applied, which, it is argued, will have to be fulfilled if the instrument is to find acceptance in routine clinical prac-
Table 14 Cells That Can be Statistically Distinguished on a Multiple Comparison
Analysis for the Reported Benefit Scale from the Hearing Disability and Aid Benefit
Interview after Control for Impairment Level in the Fitted Ear with the Four Subject-specified
Listening Situations Omitted
Imp
f0]
roveme
[11
nt in Spe
G2]
ech Intel
[3]
ligibility Index
G4] G5
[0] n/a [.1] n/a [2] n/a [3] n/a [ .4] n/a [5] n/
*p< .05, "p< 01
]
a
tice . The first of these criteria concerns face validity and clinical utility. The components of a clinical instrument have to be able to be rep-resented to both hearing-impaired listeners and provider professionals as being a useful part of the assessment, management, and rehabilitation of hearing-impaired listeners and not an exter-nally imposed bureaucratic exercise for moni-toring or audit purposes . It will be extremely helpful if any routine instrument can be repre-sented as a formalization of good clinical prac-tice rather than an additional element to be imposed upon a service system already under pressure by resource restrictions . A second cri-terion is that the instrument has to be short, take little time to apply, and not be overly complex . In adapting this to a pragmatic criterion, we have imposed the restriction that any self-report ques-tionnaire should be able to be printed on a sin-gle sheet (e.g ., double sided) of A4 paper for inclusion in routine case records .
Inspection, then, of the original HDABI has led to a number of pragmatic decisions. The first of these concerns the auditory exposure or occurrence dimension. While it has been argued and demonstrated that only accessing listening circumstances that occur in the hearing-impaired listener's experience and lead to hearing diffi-culty does provide discriminatory powers for the eventual scales, little use has been made of the exposure dimension of itself in an outcome sense. Note that this is not necessarily true in the domain of scientific investigation (see, for example, Gatehouse, 1994), where a combination of difficulty and exposure has been shown to be predictive of the eventual handicap and restric-tion of health-related quality of life experienced by the listener. Thus, the pragmatic decision has been taken to exclude the exposure dimen-sion while retaining the element of determining the existence or otherwise of particular cir-cumstances within a subject's lifestyle. Initial for-matting considerations suggested that a single sheet ofA4 paper could contain six columns rep-resenting the dimensions of initial disability, handicap, reported use, reported benefit, resid-ual disability, and satisfaction with four pre-specified communication circumstances on one face of the A4 sheet and a further four listening circumstances to be specified by the user on the reverse . It has therefore been decided to spec-ify that a potential instrument should consist of four prespecified listening circumstances and up to four circumstances that can be specified by the individual hearing-impaired listener. The task is then to determine which 4 of the 14 pre-
93

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
specified listening circumstances in the HDABI are appropriate candidates to be included in the shortened instrument . Table 15 details the occurrence of the 14 listening circumstances in the HDABI in the listening experience of the 943 subjects who completed the self-report research visit and also the proportion of subjects for whom each listening circumstance occurred and sub-sequently led to a nonzero hearing difficulty. One method of proceeding would be to select the four listening circumstances that had either the maximum frequency of occurrence or the maximum occurrence of hearing difficulty. This, however, would be subject to the potential arte-fact of selecting listening circumstances that across large groups of subjects covaried and thus duplicated the information and hence had less than optional combined discriminatory power.
Amore statistical approach is adopted. The requirement is to select the four predetermined listening circumstances that have the maxi-mum statistical ability to distinguish between different degrees of technical competence of the hearing aid fitting after control for the impair-ment level in the fitted ear (a procedure analo-gous to that adopted in Study 1 as the validity criterion) . In Study 1, a multiple-comparison analysis was used to determine the extent to which the reported benefit scale from the HDABI was able to distinguish between cells associ-ated with varying degrees of improved audibil-ity of speech (e.g ., see Table 9) . A similar procedure is adopted here . There are 24,024 combinations of sets of four questions selected from the 14 predetermined items in the HDABI.
Each of these 24,024 combinations is subjected to a similar multiple-comparison analysis and the number of cells in the matrix of improve-ments in speech audibility that achieve statis-tical significance at the p < .05 level was determined . The combination of four items that leads to a maximum on this dependent variable and maximized the range of improvements in speech audibility over which those significant dif-ferences occurred is identified . This is a com-putationally tedious although conceptually simple procedure and identifies as the four lis-tening circumstances having the maximum abil-ity to distinguish between degrees of technical competence of hearing aid fitting (in terms of improvements in speech audibility) the situations shown in Table 16 .
This procedure, then, identifies the four prespecified listening circumstances that it is appropriate to incorporate into a shortened ver-sion of the HDABI. The details of Study 1 describe how, at the end of the HDABI, listen-ers were asked to rank order the importance of the 14 prespecified listening circumstances and those (up to four) communication circumstances nominated by the listeners themselves in terms of their importance to the individual of the abil-ity to communicate adequately. This ranking is now used to select on a putative predictive basis the four communication circumstances that would have been nominated by the impaired listener had they only been offered the four pre-determined listening circumstances in Table 16 . Note that this is a form of "what-if analysis" and makes the assumption that the rank ordering of the listening circumstances and the response to
Table 15 Occurrence and Associated Difficulty of the 14 Prespecified Communication Circumstances
Listening Situation Occurrence (%) Occurrence and
Experience Difficulty (~)
Listening to the television on your own 60.2 48 .4 Listening to the television with other family or friends 63.7 57.6 Having a conversation on the telephone 86.4 28.6 Listening at the cinema or bingo 18 .6 4.7 Understanding speech in a pub, club, or meeting 67 .1 56 .5 Carrying on a conversation in a busy street or shop 85 .7 55.3 Listening to music 74 .5 31 .6 Following a lecture or service in church 48.4 34.7 Understanding speech in a car or bus 86.3 52 .8 Understanding children's voices 50.9 30 .9 Having a conversation with one other person 95.0 67 .1 Having a conversation with several people 85.7 80 .1 Understanding speech on the radio 68.9 41 .6 Understanding what is said at work 23.0 14.6

Glasgow Hearing Aid Benefit Profile/Gatehouse
Table 16 Four Prespecified Communication Circumstances that Lead to a Maximum Discriminatory Power for Improvements
in Speech Audibility Listening to the television with other family and friends
when the volume is adjusted to suit other people Having a conversation with one other person when there
is no background noise Carrying on a conversation in a busy street or shop Having a conversation with several people in a group
the multidimensional questions about the lis-tening circumstance that were derived as part of the comprehensive HDABI are applicable to the hypothetical situation of only having four pre-determined listening circumstances. The extent to which this assumption can be justified will be addressed subsequently.
The analytical procedure now derives indices of initial disability, handicap, reported hearing aid use, benefit, residual disability, satisfaction, and derived benefit (the difference between ini-tial disability and residual disability) for the eight items (four prespecified and four "quasi subject specified") that make up the hypotheti-cal shortform instrument . The reported benefit scale is then subjected to the same multiple-comparison analysis as performed in Study 1 and also underlies the selection of the four circum-stances in Table 16 . Table 17 contains the results of that multiple-comparison analysis and should be viewed in association with Table 9 . Inspection of the new tables shows that although there is a minor loss of discriminatory power in the reduction of 14 predetermined and (up to four) subject-specified listening circumstances to four
Table 17 Cells That Can be Statistically Distinguished on a Multiple Comparison Analysis for the Reported Benefit Scale
of the Derived Glasgow Hearing Aid Benefit Profile after Control for
Impairment Level in the Fitted Ear
Imp
l01
roveme
[11
nt in Spe
[21
ech Intel
[31
ligibility Index
[41 [5
[0] n/a 1 .11 n/a [ .2] n/a [3] n/a [.4] n/a [5] n/
*p < 05, "p < 01
1
a
prespecified and four quasi-subject-specified lis-tening circumstances, this loss of discriminatory power is minor and still materially exceeds the discriminatory power enjoyed by competitor items such as the Hearing Handicap Inventory for the Elderly and the Manchester Hearing Aid Benefit Questionnaire (Gatehouse, 1997) . The structure outlined above leads to the generation of an instrument that will hereafter be referred to as the Glasgow Hearing Aid Benefit Profile (GHABP) .
Verification of the GHABP
Although the multiple-comparison analy-sis conducted above is instructive, it does make the assumption that the data gathered in the context of the comprehensive HDABI are rep-resentative of what would have been gathered if the short-form instrument itself had been employed . This is not a self-evident assumption and requires empirical verification. Therefore, a further data sample was taken of 293 indi-viduals who were new hearing aid users and had attended for management at the Audiology Clinic at Glasgow Royal Infirmary following the ces-sation of the data collection for the main research phase . Inspection of the biographical and audi-ologic characteristics of these 293 subjects showed that the referral pattern had not changed between the main research phase and this sub-sequent verification of the GHABR The form of the GHABP using this verification is shown in Appendices B and C . Appendix B contains the prespecified listening circumstances while Appendix C (on the reverse of a single A4 sheet) contains the four opportunities for listener-spec-ified situations . The opportunity is taken in this instance to embed the data collection in the rou-tine clinical service environment rather than the specialist context of the self-report research visit in Study 1 . The first two dimensions (ini-tial disability and handicap) are completed by audiologic staff at the clinic prior to hearing aid fitting while the subsequent dimensions are accessed at the subsequent review. It should be emphasized that the GHABP is currently com-pleted by interview rather than self-completion by the hearing-impaired listener. The proce-dures for the GHABP follow the logic and scor-ing of the HDABI in their entirety as described in Study 1 . The GHABP contains sections that are lightly shaded . These are completed by the audiologist prior to fitting the hearing aid at the clinic visit where the decision to manage by amplification is taken . The shaded sections allow
95

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
the audiologist to ascertain the occurrence of the listening situation ("does this situation happen in your life?"), and, if so, then the degree of dif-ficulty experienced in the listening circumstance and the extent to which any difficulty leads to an auditory handicap .
Table 18 contains the distribution of initial disability from the HDABI, split into two sub-sets . The first of these contains the full data that contributed to the analyses in Study 1, while the second contains the subset of four prespecified and four quasi-subject-specified listening cir-cumstances . In addition, Table 18 contains the distribution of scale scores for initial disability from the additional clinic sample at Glasgow Royal Infirmary to whom the GHABP has been applied. Table 18 also shows the distributions of data for the other five scales from the GHABP covering handicap, reported aid use, reported benefit, satisfaction, and derived benefit (the difference between residual disability and ini-tial disability) . Inspection of Table 18 and for-mal statistical tests demonstrate that there are no material differences either between the abbre-viated data subsets from the HDABI and the cor-responding full dataset or between either of these sets and the data from the GHABR
The data from the 293 listeners for whom GHABP data are available are now subjected to the same test of criterion validity described for Study 1 using a series of multiple-comparison analyses to determine the ability of the GHABP outcome scales to differentiate between hearing aid fittings leading to differing improvements in audibility (after appropriate control for impair-ment level) . Tables 19, 20, 21, and 22 contain the qualitative summaries of these analyses for the scales of reported aid, use, reported benefit, sat-isfaction, and derived benefit, respectively, from the GHABP. They may be compared with the analogous summaries from the more intensive (and research rather than clinic-based) data from the HDABT in Tables 9, 10, 11, and 12 respectively. The tables show that the GHABP clinical measure with four listener-specified cir-cumstances in addition to the optimum set of four prespecified circumstances maintains a high degree of discriminatory power. As such, it passes the test of criterion validity. Table 23 contains descriptive information regarding the extent to which hearing-impaired listeners make use of the subject-specified elements of the GHABP and the distribution of those listening environments . All listeners make use of at least one "open-ended" element, 89.8 percent at least two, and 80.2 percent at least three, and 65.9 percent
Table 18 Distribution of the Scales from the Hearing Disability and Aid Benefit Interview and the Glasgow Hearing Aid Benefit Profile
Initial Disability
ercentile
Disability and Hearing Aid Benefit Interview
Full Data Subset (14 + 4) (4+4)
Glasgow Hearing Aid Benefit
Profile
25th 24.7 22.9 20.7 50th 42 .3 43 .6 44.0 75th 59 .9 58 .4 60.7
Handicap
25th 11 .1 14 .6 12 .7 50th 24 .6 26 .4 25.8 75th 51 .0 57 .2 53.6
Reported Aid Use
25th 49 .7 50 .4 47 .9 50th 70 .2 68 .9 70 .4 75th 86.9 84 .4 86 .1
Reported Benefit
25th 38.2 40 .7 37 .4 50th 51 .6 53.8 52.9 75th 65.2 66.4 68 .2
Satisfaction
25th 46 .1 44 .8 47.0 50th 60.4 56 .4 57 .9 75th 72.9 70.4 73 .1
Derived Benefit
25th 9.6 11 .2 10 .9 50th 24 .6 23 .9 25.8 75th 40 .1 41 .7 42 .3
specified four circumstances in addition to the four prespecified circumstances .
Validity Aspects of the GHABP
The derivation and verification of the GHABP has been described in some detail, pri-marily in terms of criterion validity and respon-siveness to change. These are, however, only a subset of issues concerned with validity (Streiner and Norman, 1989) and, while they now repre-sent an increasingly dominant position in the hierarchy of requirements for health scales, they should not preclude other components . Three issues that deserve consideration are the factor structure of the scales from the GHABP,
96

Glasgow Hearing Aid Benefit Profile/Gatehouse
Table 19 Cells That Can be Statistically Distinguished on a Multiple Comparison
Analysis for the Reported Aid Use Scale of the Glasgow Hearing Aid Benefit Profile after
Control for Impairment Level in the Fitted Ear
Table 21 Cells That Can be Statistically Distinguished on a Multiple Comparison Analysis for the Satisfaction Scale of the Glasgow Hearing Aid Benefit Profile after
Control for Impairment Level in the Fitted Ear
Imp
[01
roveme
[11
nt in Spe
[21
ech Intel
[3]
ligibility I
[4]
ndex
[51
Imp
[01
roveme
[11
nt in Spe
[2]
ech Intel
[31
ligibility Index
[41 [5
[0] n/a [0] n/a Ill n/a Ill n/a [.2] n/a [2] n/a [3] n/a * [ .3] n/a [.4] n/a [ .4] n/a [5] n/a [5] n/
*p< 05, "p< 01
the internal reliability of the scales, and the test-retest reliability of the scales .
To date, the opportunity to derive factors from the GHABP has not been taken, and this decision requires to be justified . The GHABP yields six dimensions covering initial disabil-ity, handicap, hearing aid use, hearing aid ben-efit, residual disability, and satisfaction . Note that these dimensions are not analogous to the subscales in, for example, the (Abbreviated) Pro-file of Hearing Aid Benefit (Cox and Gilmore, 1990 ; Cox and Rivera, 1992 ; Cox and Alexander, 1995 ; Cox, 1997), as each dimension accesses an identical set of listening circumstances . The sets of items related to each of these dimen-sions can be submitted to a factor analysis to determine its scale structure, and each such analysis yields a factor structure (usually of two factors) . The factor structures are interpretable but are not identical across the six dimensions . This might initially appear to be a troublesome
*p< .05, "p< .01
finding but on consideration is almost inevitable. There is every reason to suppose that sets of lis-tening situations that cluster to form one factor in the disability domain will not necessarily cluster in the handicap domain . This is a nat-ural consequence of a degree of dissociation between disability and handicap . There are cer-tain circumstances where listeners will experi-ence high degrees of difficulty but that will not impact to any great degree because of the minor importance to the listener of the situation . Con-versely, other circumstances may lead to only slight or moderate difficulty but can and do have large impact on the listeners because of their central role in everyday life . In a similar manner, there are degrees of dissociation between the factor structures in the dimensions of hearing aid use and hearing aid benefit . Indeed, were the two dimensions to have such similar structure and properties, there would be limited additional leverage in accessing them
Table 20 Cells That Can be Statistically Distinguished on a Multiple Comparison
Analysis for the Handicap Scale of the Glasgow Hearing Aid Benefit Profile after Control for
Impairment Level in the Fitted Ear
Imp
[01
roveme
[11
nt in Spe
[2]
ech Intel
[31
ligibility index
[41 [5
[0] n/a
Ill n/a [2] n/a [.31 n/a [ .4] n/a [5] n/
*p< .05, "p< .01
Table 22 Cells That Can be Statistically Distinguished on a Multiple Comparison
Analysis for the Derived Benefit Scale of the Glasgow Hearing Aid Benefit Profile after
Control for Impairment Level in the Fitted Ear
1
Imp
[01
roveme
[11
nt in Spe
[2]
ech Intel
[31
ligibility Index
[41 [5
[0] n/a 1 .11 n/a [2] n/a [.3] n/a [ .4] n/a [ .5] n/
]
a
'p< .05, "p< .01
]
a
a
97
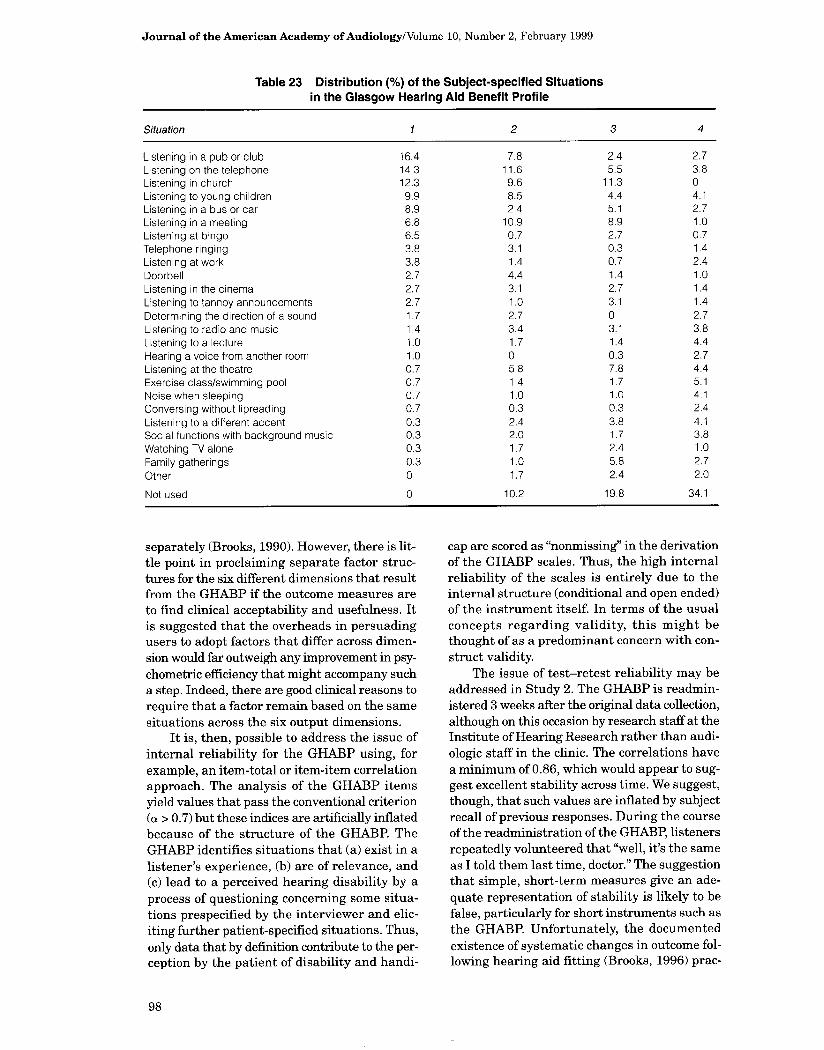
Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
Table 23 Distribution (%) of the Subject-specified Situations in the Glasgow Hearing Aid Benefit Profile
Situation 1 2 3 4
Listening in a pub or club 16.4 7 .8 2 .4 2 .7 Listening on the telephone 14.3 11 .6 5.5 3 .8 Listening in church 12.3 9 .6 11 .3 0 Listening to young children 9.9 8 .5 4 .4 4 .1 Listening in a bus or car 8.9 2 .4 5 .1 2 .7 Listening in a meeting 6.8 10 .9 8 .9 1 .0 Listening at bingo 6.5 0 .7 2 .7 0 .7 Telephone ringing 3 .8 3 .1 0 .3 1 .4 Listening at work 3 .8 1 .4 0 .7 2 .4 Doorbell 2 .7 4 .4 1 .4 1 .0 Listening in the cinema 2 .7 3 .1 2 .7 1 .4 Listening to tannoy announcements 2 .7 1 .0 3 .1 1 .4 Determining the direction of a sound 1 .7 2 .7 0 2.7 Listening to radio and music 1 .4 3.4 3 .1 3 .8 Listening to a lecture 1 .0 1 .7 1 .4 4 .4 Hearing a voice from another room 1 .0 0 0.3 2 .7 Listening at the theatre 0.7 5.8 7.8 4 .4 Exercise class/swimming pool 0 .7 1 .4 1 .7 5.1 Noise when sleeping 0.7 1 .0 1 .0 4 .1 Conversing without lipreading 0.7 0 .3 0 .3 2 .4 Listening to a different accent 0.3 2 .4 3 .8 4 .1 Social functions with background music 0.3 2 .0 1 .7 3.8 Watching TV alone 0.3 1 .7 2 .4 1 .0 Family gatherings 0.3 1 .0 5 .8 2 .7 Other 0 1 .7 2 .4 2 .0
Not used 0 10 .2 19 .8 34 .1
separately (Brooks, 1990). However, there is lit-tle point in proclaiming separate factor struc-tures for the six different dimensions that result from the GHABP if the outcome measures are to find clinical acceptability and usefulness . It is suggested that the overheads in persuading users to adopt factors that differ across dimen-sion would far outweigh any improvement in psy-chometric efficiency that might accompany such a step . Indeed, there are good clinical reasons to require that a factor remain based on the same situations across the six output dimensions .
It is, then, possible to address the issue of internal reliability for the GHABP using, for example, an item-total or item-item correlation approach. The analysis of the GHABP items yield values that pass the conventional criterion (a > 0.7) but these indices are artificially inflated because of the structure of the GHABR The GHABP identifies situations that (a) exist in a listener's experience, (b) are of relevance, and (c) lead to a perceived hearing disability by a process of questioning concerning some situa-tions prespecified by the interviewer and elic-iting further patient-specified situations . Thus, only data that by definition contribute to the per-ception by the patient of disability and handi-
cap are scored as "nonmissing" in the derivation of the GHABP scales . Thus, the high internal reliability of the scales is entirely due to the internal structure (conditional and open ended) of the instrument itself. In terms of the usual concepts regarding validity, this might be thought of as a predominant concern with con-struct validity.
The issue of test-retest reliability may be addressed in Study 2. The GHABP is readmin-istered 3 weeks after the original data collection, although on this occasion by research staff at the Institute of Hearing Research rather than audi-ologic staff in the clinic . The correlations have a minimum of 0 .86, which would appear to sug-gest excellent stability across time . We suggest, though, that such values are inflated by subject recall of previous responses. During the course of the readministration of the GHABP, listeners repeatedly volunteered that "well, it's the same as I told them last time, doctor ." The suggestion that simple, short-term measures give an ade-quate representation of stability is likely to be false, particularly for short instruments such as the GHABP. Unfortunately, the documented existence of systematic changes in outcome fol-lowing hearing aid fitting (Brooks, 1996) prac-
98

Glasgow Hearing Aid Benefit Profile/Gatehouse
tically precludes the assessment of stability across longer time frames .
DISCUSSION
T he GHABP has been derived as a candi-date outcome measure for application in routine service context for the assessment of
aspects of disability, handicap, and hearing aid benefit . Previous research has identified the importance of disability and handicap dimen-sions in the consequences of hearing impair-ment and also the relevance of access to dimensions associated with hearing aid use, hearing aid benefit, residual disability, and sat-isfaction when assessing the effectiveness and cost effectiveness of interventions . The GHABP aims to reconcile the need to access multidi-mensional information with the limitations of clinical practice regarding the length and com-plexity of instruments by a combination of infor-mation on listening environments that occur in
everyday practice across large numbers of lis-teners and those that may be specific to indi-
vidual patient's listening requirements . Each of the dimensions in the GHABP is specific to each relevant listening situation occurring and leading to difficulty and hence results in an effi-cient concentration of resources relevant to the needs of individual hearing-impaired listeners .
The derivation, optimization, and valida-tion of the GHABP within this article suggests that the instrument is a sensible candidate for this role, and it may be argued that the GHABP is a valuable clinical tool in the way that it pro-vides a formalization of good audiologic practice in the rehabilitation domain . Although the GHABP has been derived in the context of the
UK NHS and the cultural environments of clin-ics in Manchester and Glasgow, it is suggested that the principles that underpin the structure
of the GHABP are likely to apply independent of the particular mode of hearing health care deliv-ery ; hence, an instrument with structure simi-lar to the GHABP could find application in other environments . It should be stressed that the GHABP data presented in this article have all been gathered in an interview context and not in
an environment where the questionnaire is self-completed by hearing-impaired listeners . In the UK context, the median age of first-time fitting of a hearing aid is around 70 years, and the dif-ferentiation between the various dimensions of the GHABP is not necessarily obvious to hear-
ing-impaired clients . In any event, it is argued that any coherent process of provision of ampli-fication to alleviate disabilities and handicaps has to take place in the context of a rational assess-ment of those disabilities and handicaps by the individual clinical practitioner, and that a rou-
tine review of the success of intervention and an ascertainment of the need for further remedial action will also have to take place by clinical practitioners . There is a need to identify the extent to which the intervention is used by the hearing-impaired client and helps the hearing-impaired client to overcome their difficulties, and the extent to which the hearing-impaired client has residual problems that might require further intervention and derives satisfaction from the intervention . Thus, the requirement for an interview format need not be regarded as a fundamental drawback as it provides a struc-ture for processes that occur in any event .
The data presented in this article, although anchored in clinical practice in audiology cen-ters in Manchester and Glasgow, have been gath-ered in a context that is oriented toward research, and further work will be required to ascertain the extent to which practitioners in routine service contexts make use of the dimensions and capa-bilities of the GHABP and the extent to which the statistical and psychometric properties docu-mented in this article are maintained in the dif-fering service contexts . Although the report to the Department of Health in London, England (Gate-house, 1997), which describes the overall con-text of the derivation of the GHABP, does contain elements that describe the extent to which the GHABP is able to differentiate between different hearing aids (postaural versus in-the-ear, mon-aural versus binaural fittings, etc. (e .g ., see Gatehouse et al, 1997) and different types of rehabilitation regime (e.g ., the availability of pre-fitting counselling [Brooks and Johnson, 19811), it is only when outcome measures such as the GHABP are used in clinical trials and evaluation exercises that the true discriminatory power can be fully documented . The dissemination of the GHABP and its underpinning principles will be facilitated by its incorporation into routine pro-tocols, the availability of reference data in a vari-ety of cultural and service delivery contexts, and the availability of appropriate tools for the pre-sentation and scoring of the instrument . Experi-ence will determine the extent to which the intention to produce measures appropriate for quality assurance programs with appropriate clinical relevance has been successful .
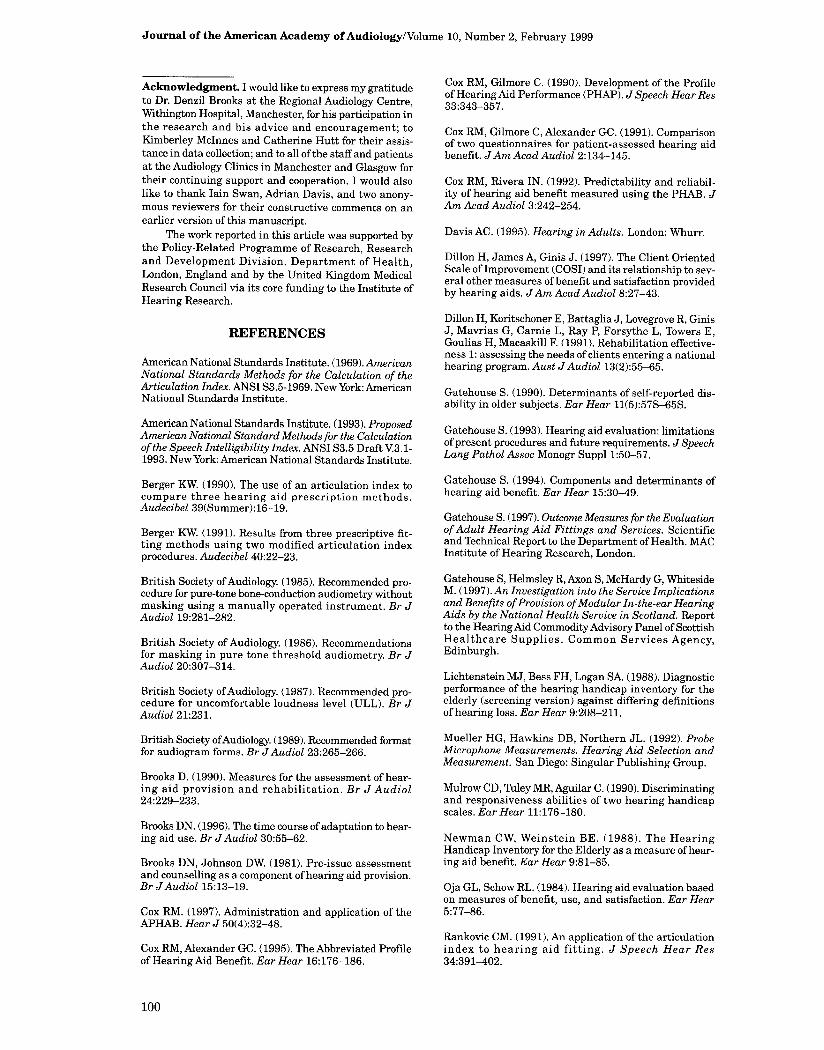
Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
Acknowledgment. I would like to express my gratitude to Dr. Denzil Brooks at the Regional Audiology Centre, Withington Hospital, Manchester, for his participation in the research and his advice and encouragement; to Kimberley McInnes and Catherine Hutt for their assis-tance in data collection; and to all of the staff and patients at the Audiology Clinics in Manchester and Glasgow for their continuing support and cooperation. I would also like to thank Iain Swan, Adrian Davis, and two anony-mous reviewers for their constructive comments on an earlier version of this manuscript .
The work reported in this article was supported by the Policy-Related Programme of Research, Research and Development Division, Department of Health, London, England and by the United Kingdom Medical Research Council via its core funding to the Institute of Hearing Research .
Cox RM, Gilmore C . (1990) . Development of the Profile of Hearing Aid Performance (PHAP) . J Speech Hear Res 33 :343-357 .
Cox RM, Gilmore C, Alexander GC . (1991). Comparison of two questionnaires for patient-assessed hearing aid benefit. J Am Acad Audiol 2:134-145 .
Cox RM, Rivera IN . (1992). Predictability and reliabil-ity of hearing aid benefit measured using the PHAB . J Am Acad Audiol 3:242-254 .
Davis AC . (1995). Hearing in Adults . London: Whurr.
Dillon H, James A, Ginis J. (1997) . The Client Oriented Scale of Improvement (COSI) and its relationship to sev-eral other measures of benefit and satisfaction provided by hearing aids . J Am Acad Audiol 8:27-43 .
REFERENCES
American National Standards Institute. (1969) . American National Standards Methods for the Calculation of the Articulation Index. ANSI S3.5-1969. New York : American National Standards Institute.
American National Standards Institute . (1993). Proposed American National Standard Methods for the Calculation of the Speech Intelligibility Index. ANSI S3.5 Draft V3 . 1-1993 . New York: American National Standards Institute .
Berger KW. (1990) . The use of an articulation index to compare three hearing aid prescription methods . Audecibel 39(Summer):16-19 .
Berger KW. (1991) . Results from three prescriptive fit-ting methods using two modified articulation index procedures. Audecibel 40:22-23 .
British Society of Audiology. (1985) . Recommended pro-cedure for pure-tone bone-conduction audiometry without masking using a manually operated instrument . Br J Audiol 19:281-282 .
British Society of Audiology. (1986) . Recommendations for masking in pure tone threshold audiometry. Br J Audiol 20:307-314 .
British Society of Audiology. (1987) . Recommended pro-cedure for uncomfortable loudness level (ULL) . Br J Audiol 21:231 .
British Society ofAudiology. (1989) . Recommended format for audiogram forms. Br JAudiol 23:265-266.
Brooks D . (1990) . Measures for the assessment of hear-ing aid provision and rehabilitation . Br J Audiol 24:229-233 .
Brooks DN . (1996). The time course of adaptation to hear-ing aid use . Br JAudiol 30:55-62 .
Brooks DN, Johnson DW (1981) . Pre-issue assessment and counselling as a component of hearing aid provision. Br JAudiol 15:13-19 .
Cox RM. (1997) . Administration and application of the APHAB. Hear J 50(4):32-48.
Cox RM, Alexander GC . (1995) . The Abbreviated Profile of Hearing Aid Benefit . Ear Hear 16:176-186 .
Dillon H, Koritschoner E, Battaglia J, Lovegrove R, Ginis J, Mavrias G, Carnie L, Ray P, Forsythe L, Towers E, Goulias H, Macaskill F. (1991) . Rehabilitation effective-ness 1 : assessing the needs of clients entering a national hearing program. Aust JAudiol 13(2):55-65 .
Gatehouse S. (1990). Determinants of self-reported dis-ability in older subjects. Ear Hear 11(5):57S-65S .
Gatehouse S . (1993). Hearing aid evaluation : limitations of present procedures and future requirements . J Speech Lang Pathol Assoc Monogr Suppl 1:50-57 .
Gatehouse S. (1994) . Components and determinants of hearing aid benefit. Ear Hear 15:30-49 .
Gatehouse S . (1997) . Outcome Measures for the Evaluation of Adult Hearing Aid Fittings and Services. Scientific and Technical Report to the Department of Health . MAC Institute of Hearing Research, London .
Gatehouse S, Helmsley R, Axon S, McHardy G, Whiteside M. (1997) . An Investigation into the Service Implications and Benefits of Provision of Modular In-the-ear Hearing Aids by the National Health Service in Scotland. Report to the Hearing Aid CommodityAdvisory Panel of Scottish Healthcare Supplies . Common Services Agency, Edinburgh.
Lichtenstein MJ, Bess FH, Logan SA. (1988) . Diagnostic performance of the hearing handicap inventory for the elderly (screening version) against differing definitions of hearing loss . Ear Hear 9:208-211 .
Mueller HG, Hawkins DB, Northern JL. (1992) . Probe Microphone Measurements . Hearing Aid Selection and Measurement. San Diego: Singular Publishing Group.
Mulrow CD, Tuley MR, Aguilar C . (1990) . Discriminating and responsiveness abilities of two hearing handicap scales . Ear Hear 11:176-180.
Newman CW, Weinstein BE . (1988) . The Hearing Handicap Inventory for the Elderly as a measure of hear-ing aid benefit . Ear Hear 9:81-85 .
Oja GL, Schow RL . (1984) . Hearing aid evaluation based on measures of benefit, use, and satisfaction . Ear Hear 5:77-86.
Rankovic CM. (1991) . An application of the articulation index to hearing aid fitting . J Speech Hear Res 34:391-402 .
100

Glasgow Hearing Aid Benefit Profile/Gatehouse
Schow RL, Gatehouse S. (1990). Fundamental issues in self-assessment of hearing. Ear Hear 11(5[Suppl]):6s-15s.
Ventry IM, Weinstein BE . (1982). The Hearing Handicap Inventory for the Elderly: a new tool . Ear Hear 3:128-134 .
Stephens D, Hetu R . (1991) . Impairment, disability and handicap in audiology : towards a consensus . Audiology 30:185-200 .
Streiner DL, Norman GR. (1989) . Health Measurement Scales: APractical Guide to Their Development and Use. Oxford : Oxford University Press.
Tannahill JC . (1979) . The hearing handicap scale as a speech measure of hearing aid benefit. J Speech Hear Disord 44:9-99.
Weinstein BE, Spitzer JB, Ventry IM . (1986). Test-retest Reliability of the Hearing Handicap Inventory for the Elderly. Ear Hear 7:295-299.
Weinstein BE, Ventry IM . (1983) . Audiometric correlates of the hearing handicap inventory for the elderly. J Speech Hear Disord 48:379-384 .
APPENDIX A
Response Format for the Hearing Disability and Aid Benefit Interview
How often does Without your Without your In this situation In this situation In this situation For this situa- this happen? hearing aid how hearing aid how what proportion how much does with your hear- tion how satis-
much difficulty much did any of the time do your hearing aid ina aid how fied are you did you have in difficulty worry, you wear your help you? much difficulty with your hear- this situation? annoy or upset hearing aid? do you have? ing aid?
you in this situ- ation?
0-Never 0-N/A 0 _N/A 0 _N/A 0-N/A 0 _N/A O N/A 1-Less than once a 1 No difficulty 1-Not at all 1Never/Not at all 1 -Hearing aid 1 No difficulty 1 -Not satisfied at all
week 2 -Only slight 2-Only a little 2 -About a quarter makes it worse 2 -Only slight 2 -Some satisfaction 2One to three days difficulty 3 -Moderate amount of the time 2 -Hearing aid no difficulty but not much
each week 3-Moderate 4 Quite a lot 3 About half the use at all 3-Moderate 3-Reasonably 3 Four to six days difficulty 5 -Very much time 3-Hearing is some difficulty satisfied
each week c_Great difficulty indeed 4-About three but not much 4 -Great difficulty 4 -Very satisfied 4 -Every day- 5 -Cannot manage quarters of the help 5 -Cannot manage 5 -Delighted with
under 4 hours at all time 4 -Hearing aid is at all hearing aid for 5 Over 4 hours 5 All the time quite helpful this situation
every day 5 -Hearing aid is a great help
6 -Hear perfectly normally with hearing aid in this situation

Journal of the American Academy of Audiology/Volume 10, Number 2, February 1999
APPENDIX B Prespecified Element of the Glasgow Hearing Aid Benefit Profile
GLASGOW HEARING AID BENEFIT PROFILE
Date of Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date of Review
How much difficulty do you have in this situation?
Q _N/A I -No difficulty 2 Only slight difficulty 3Moderate difficulty 4 __Great difficulty
Hospital Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Name . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Address . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
happen in your life? 1 Yes
How much does In this situation, In this situation, how In this sltuationl For this situation, any difficulty in what proportion much does your with your hearing how satisfied are this situation of the time do hearing aid help aid, how much you with your worry, annoy or you wear your you? dMfculty do you hearing aid? upset you? hearing aid? now have? O -NIA 0-N/A Q __N/A 0_N/A O -NIA 1-Not al all 1 Never/Not at all 1 -Hearing aid no use at all 1-No difficulty 1 _Not satisfied at all 2 _Only a little 2 About'/. of the time 2 __Hearing aid is some help 2 _Only slight difficulty 2_A Me satisfied 3__A moderate amount 3 About % of the time 3 Hearing aid is quite helpful 3Moderate difficulty 3 _Reasonably satisfied 4 Quite a lot 4 -About % of the time 4Hearing aid is a great help 4 _Great difficulty 4 Very satisfied

Glasgow Hearing Aid Benefit Profile/Gatehouse
APPENDIX C Subject-specified Element of the Glasgow Hearing Aid Benefit Profile
We have dealt with some of the situations that in our experience can lead to difficulty with hear-
ing. What we would now like you to do is to nominate up to four new situations in which it is impor-
tant for you as an individual to be able to hear as well as possible .
How much oR mu does nn t~uation, n t is situation, how difficulty do you any difficulty in what proportion much does your have in this this situation of the time do hearing aid help situation? worry, annoy or you wear your you?
upset you? hearing aid? O WA 0 N/A O WA O -N/A 1-No difficulty 1 Not at all 1 Never/Not at all 1-Hearing aid no use at all
2 -Only slight difficulty 2 -Only a little 2 About % of the time Z _Hearing aid is some help 3 Moderate difficulty 3--A moderate amount 3About % of the time 3Hearing aid is quite helpful 4 Great difficulty 4 __Quite a lot 4 About /4 of the time 4 _Hearing aid is a great help 5 -Cannot manage at all 5-Very much indeed 5-All the lime 5 Headng is perfect with aid
How much How much does "i's situation, In this situation, how difficulty do you any difficulty in what proportion much does your have in this this situation of the time do hearing aid help situation? worry, annoy or you wear your you?
upset you? hearing aid? 0 N/A 0 N/A O -N/A O -N/A 1 No difficulty 1 -Not at all 1-Never/Not at all 1 -Hearing aid no use at all 2 -Only slight difficulty 2 Only a little 2 -About % of the time 2-Hearing aid is some help 3 _Moderate difficulty 3-,4 moderate amount 3 About % of the time 3Hearing aid is quite helpful 4 Great difficulty 4 Quite a lot 4 About''/. of the time 4 -Hearing aid is a great help
5 -Cannot manage at all 5 -Very much indeed 5 -All the lime 5 Hearing is perfect with aid
How much difficulty do you have in this situation?
Flow much does any difficulty in this situation worry, annoy or upset you?
In this situation, what proportion of the time do you wear your hearing aid?
In this situation, how much does your hearing aid help you?
0-N/A O -N/A O -NIA O N/A
1-No difficulty 1 Not at all 1-Never/Not at all 1 -Hearing aid no use at all 2 Only slight difficulty 2 Only a little 2About ' of the time 2 -Hearing aid is some help 3 Moderate difficulty 3 A moderate amount 3 __About % of the time 3 Headng aid is quite helpful
4Great difficulty 4 -Quite a lot 4 About'/. of the time 4Hearing aid is a great help
5-Cannot manage at all 5 -Very much indeed 5 All the time 5 Headng is perfect with aid
How much How How m In this situation, In this situation, how difficulty do you any difficulty in what proportion much does your have in this this situation of the time do hearing aid help situation? worry, annoy or you wear your you?
upset you? hearing aid? 0 N/A 0_11A 0-N/A O -NIA
1 No difficulty 1 Not at all 1 Never/Not at all 1-Hearing aid no use al all 2 Only slight difficulty -2 Only a tittle 2About'/. of the time 2 -Hearing aid is some help
3 Moderate difficulty 3A moderate amount 3About %: of the time 3 Headng aid is quite helpful
4 Great difficulty 4-Q uite a lot 4About '/. of the time 4 Headng aid is a great help 5 -Cannot manage at ali 5 Very much indeed 5 -All the time 5 Hearing is perfect with aid
in this situation, with your hearing aid, how much difficulty do you now have? O -N/A 1-NO difficulty 2 _Only slight difficulty 3Moderate difficulty 4Great difficulty 5 _Cannot manage at all
in this situation, with your hearing aid, how much difficulty do you now have? O -N/A 1 -No difficulty 2 -Only slight difficulty 3 -Moderate difficulty 4Great difficulty 5 _Cannot manage at all
In this situation, with your hearing aid, how much difficulty do you now have? O -N/A 1-NO difficulty 2 -Only slight difficulty 3 -Moderate difficulty 4 -Great difficulty 5 -Cannot manage at all
In this situation, with your hearing aid, how much difficulty do you now have? O -NIA 1-No difficulty 2Only slight difficulty 3 _Moderate difficulty 4 Great difficulty 5 Cannot manage at all
this situation, how satisfied are you with your hearing aid?
O -N/A 1 Not satisfied at all 2__A little satisfied 3 _Reasonably satisfied 4 -Very satisfied 5 -Delighted with aid
or t is situation, how satisfied are you with your hearing aid?
D -NIA 1-Not satisfied al all 2_A little satisfied 3 __Reasonably satisfied 4 -Very satisfied 5 _Delighted with aid
Ror this situation, how satisfied are you with your hearing aid?
O -N/A 1 -Not satisfied at all 2 A little satisfied 3 _Reasonably satisfied 4-Very satisfied 5 -Delighted with aid
or this situation, how satisfied are you with your hearing aid?
D -N/A I -Not satisfied at all 2-A little satisfied 3 _Reasonably satisfied 4 -Very satisfied 5 ,_Delighted with aid
Related Documents











