Gene Therapy (1999) 6, 683–688 1999 Stockton Press All rights reserved 0969-7128/99 $12.00 http://www.stockton-press.co.uk/gt BRIEF COMMUNICATION Gene delivery to the myocardium by intrapericardial injection Y Fromes 1 , A Salmon 1 , X Wang 1 , H Collin 1 , A Rouche 1 , A Hage `ge 2 , K Schwartz 1 and MY Fiszman 1 1 INSERM U153 – Institut de Myologie, Paris; and 2 Laboratoire de recherche en imagerie, Faculte ´ de Me ´decine Necker-Enfants Malades, Universite ´ Paris V, Paris, France Several studies have demonstrated the feasibility of gene cardium. Transgene expression is predominant in the left transfer into the heart muscle. However, all the available ventricle and the interventricular septum but limited in the data also indicate that the extent of transfection remains right ventricle. In vivo echocardiographic measurements of limited. As an alternative method to intravascular adminis- the left ventricular diameters at end diastolic and end sys- tration, we have developed a novel strategy which uses tolic times show no difference between virus- and sham- the pericardial sac. When a replication-deficient adenovirus injected animals, thus indicating a good clinical tolerance containing the cDNA encoding a bacterial b-galactosidase to this strategy of virus delivery. The same protocol has is injected into the pericardial sac of adult Wistar rats the been used with the same efficiency in mice, which leads staining is exclusively restricted to the pericardial cell lay- us to propose injection into the pericardial sac as an effec- ers. However, injecting a mixture of collagenase and hyalu- tive and harmless method for gene transfer into the heart ronidase together with the virus, leads to a large diffusion muscle. of the transgene activity, reaching up to 40% of the myo- Keywords: gene transfer; gene therapy; pericardium; adenovirus; myocardium Gene therapy is a potential new strategy for cardiovascu- lar diseases which concerns single gene disease as well as more complex multigene pathologies affecting either the heart muscle or its vasculature. One of the major issues raised by this strategy is the development of efficient and safe gene transfer techniques. So far, a number of publications have demonstrated the potential of direct injection of genes into the myocar- dium. 1–7 This may seem an attractive approach as it avo- ids complicated and expensive ex vivo manipulations fol- lowed by in vivo cell or organ grafting. However, direct injection into the myocardium results in gene expression over a limited region due to the lack of diffusion of the vector and, furthermore, it also results in local tissue damage which makes it a rather inappropriate thera- peutic approach. 4,8,9 Intravascular gene delivery has raised higher hopes since the myocardium has a high density of capillaries. 10,11 Indeed, as opposed to single shot injection, it has been proved that coronary infusion allows some diffusion of reporter genes to the myocar- dium. However, at the present state of our knowledge, the efficiency of this strategy appears to be still limited by various factors such as a low permeability of the capil- laries to large molecules or particles due to their continu- ous non-fenestrated endothelium, or to the need for high perfusion pressure or because of a limited time contact Correspondence: Y Fromes, INSERM U153 – Institut de Myologie, Ba ˆti- ment Babinski – Ho ˆpital Pitie ´-Salpe ´trie `re, 47 boulevard de l’Ho ˆpital, 75651 Paris Cedex 15, France Received 12 August 1998; accepted 4 November 1998 of the vector with the target cell. 12 Moreover, Wright et al 13 pointed out that intracoronary infusion of cationic liposomes can result in multiple microinfarction. In view of these difficulties, we have developed an alternative approach for myocardial gene transfer which is based on local delivery of the therapeutic gene into the pericardium. The pericardial envelope of the heart may be used to overcome some of the restrictions inherent in other trans- fer methods. First, access to the pericardium can be obtained through rather simple procedures. Second, since the pericardium has a closed cavity, this may be used to maintain a prolonged contact time with the genetic vec- tors. The drawback of this approach is that the pericardial envelope appears to be rather tight, however, we will show that diffusion across this membrane can be increased by various pharmacological agents. Using this simple procedure, we show that significant territories of the myocardium can be transduced by adenoviral vectors. Adult male Wistar rats were injected with a DE1- recombinant adenoviral vector containing a CMV-driven bacterial b-galactosidase gene without a nuclear localiz- ation signal. 14 We used adenovirus since it has proven to be a rather reliable vector for gene transfer into the heart muscle due to its ability to infect nondividing cells, an absolute requirement for terminally differentiated cardiac myocytes. 9 Intra-pericardial injections were performed through a small incision of the abdominal wall below the xyphoid appendix, with a trans-diaphragmatic approach. Delivery of adenoviral vectors into the pericardium can be performed safely under visual control. Seven days

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Gene Therapy (1999) 6, 683–688 1999 Stockton Press All rights reserved 0969-7128/99 $12.00
http://www.stockton-press.co.uk/gt
BRIEF COMMUNICATION
Gene delivery to the myocardium by intrapericardialinjection
Y Fromes1, A Salmon1, X Wang1, H Collin1, A Rouche1, A Hagege2, K Schwartz1 and MY Fiszman1
1INSERM U153 – Institut de Myologie, Paris; and 2Laboratoire de recherche en imagerie, Faculte de Medecine Necker-EnfantsMalades, Universite Paris V, Paris, France
Several studies have demonstrated the feasibility of gene cardium. Transgene expression is predominant in the lefttransfer into the heart muscle. However, all the available ventricle and the interventricular septum but limited in thedata also indicate that the extent of transfection remains right ventricle. In vivo echocardiographic measurements oflimited. As an alternative method to intravascular adminis- the left ventricular diameters at end diastolic and end sys-tration, we have developed a novel strategy which uses tolic times show no difference between virus- and sham-the pericardial sac. When a replication-deficient adenovirus injected animals, thus indicating a good clinical tolerancecontaining the cDNA encoding a bacterial b-galactosidase to this strategy of virus delivery. The same protocol hasis injected into the pericardial sac of adult Wistar rats the been used with the same efficiency in mice, which leadsstaining is exclusively restricted to the pericardial cell lay- us to propose injection into the pericardial sac as an effec-ers. However, injecting a mixture of collagenase and hyalu- tive and harmless method for gene transfer into the heartronidase together with the virus, leads to a large diffusion muscle.of the transgene activity, reaching up to 40% of the myo-
Keywords: gene transfer; gene therapy; pericardium; adenovirus; myocardium
Gene therapy is a potential new strategy for cardiovascu-lar diseases which concerns single gene disease as wellas more complex multigene pathologies affecting eitherthe heart muscle or its vasculature. One of the majorissues raised by this strategy is the development ofefficient and safe gene transfer techniques.
So far, a number of publications have demonstrated thepotential of direct injection of genes into the myocar-dium.1–7 This may seem an attractive approach as it avo-ids complicated and expensive ex vivo manipulations fol-lowed by in vivo cell or organ grafting. However, directinjection into the myocardium results in gene expressionover a limited region due to the lack of diffusion of thevector and, furthermore, it also results in local tissuedamage which makes it a rather inappropriate thera-peutic approach.4,8,9 Intravascular gene delivery hasraised higher hopes since the myocardium has a highdensity of capillaries.10,11 Indeed, as opposed to singleshot injection, it has been proved that coronary infusionallows some diffusion of reporter genes to the myocar-dium. However, at the present state of our knowledge,the efficiency of this strategy appears to be still limitedby various factors such as a low permeability of the capil-laries to large molecules or particles due to their continu-ous non-fenestrated endothelium, or to the need for highperfusion pressure or because of a limited time contact
Correspondence: Y Fromes, INSERM U153 – Institut de Myologie, Bati-ment Babinski – Hopital Pitie-Salpetriere, 47 boulevard de l’Hopital,75651 Paris Cedex 15, FranceReceived 12 August 1998; accepted 4 November 1998
of the vector with the target cell.12 Moreover, Wright etal13 pointed out that intracoronary infusion of cationicliposomes can result in multiple microinfarction.
In view of these difficulties, we have developed analternative approach for myocardial gene transfer whichis based on local delivery of the therapeutic gene intothe pericardium.
The pericardial envelope of the heart may be used toovercome some of the restrictions inherent in other trans-fer methods. First, access to the pericardium can beobtained through rather simple procedures. Second, sincethe pericardium has a closed cavity, this may be used tomaintain a prolonged contact time with the genetic vec-tors. The drawback of this approach is that the pericardialenvelope appears to be rather tight, however, we willshow that diffusion across this membrane can beincreased by various pharmacological agents. Using thissimple procedure, we show that significant territoriesof the myocardium can be transduced by adenoviralvectors.
Adult male Wistar rats were injected with a DE1-recombinant adenoviral vector containing a CMV-drivenbacterial b-galactosidase gene without a nuclear localiz-ation signal.14 We used adenovirus since it has proven tobe a rather reliable vector for gene transfer into the heartmuscle due to its ability to infect nondividing cells, anabsolute requirement for terminally differentiated cardiacmyocytes.9 Intra-pericardial injections were performedthrough a small incision of the abdominal wall below thexyphoid appendix, with a trans-diaphragmatic approach.Delivery of adenoviral vectors into the pericardium canbe performed safely under visual control. Seven days

Gene delivery to the myocardium by intrapericardial injectionY Fromes et al
684 after the injection, the animals were killed and theirhearts as well as other organs (lungs, diaphragm, liver,kidney, spleen) were harvested. Serial frozen sectionswere performed and assayed for b-galactosidase activity.X-gal (5-bromo-4-chloro-3-indolyl-b-d-galactoside) stain-ing was observed almost exclusively in the pericardialcell layers (Figure 1). Only rarely were myocardial cellsfound to be transduced by the adenovirus (Figure 1b). Nosignificant staining was found either in the lungs or thediaphragm (data not shown). The same observation wasalso true for organs at the abdominal level, such as theliver, spleen or kidneys. Hence, the pericardium appearsto be transduced by adenoviral vectors, but it also provesto be a tight envelope around the heart which allows nosignificant transduction of the myocardium. A similarobservation was made by another group.15 Such data arenot so surprising since pericardial cells form a layer of
a
b
Figure 1 Intrapericardial administration of E1-deficient adenovirus containing a CMV-driven b-galactosidase gene. Wistar rats were injected locallywith 4 × 109 p.f.u. of recombinant adenovirus. The enzyme activitity was revealed by incubation of cryosections in X-gal. (a) Low magnification (×40)shows transfection of the visceral pericardial cells. (b) Higher magnification (×100) reveals that the adenovirus did not transduce cardiac myocytes.
tightly joined cells limiting diffusion across this anatom-ical barrier. Moreover, the connective tissue layers foundin the cardiac muscle most probably diminish the spreadand overall infectivity of vectors.16–18 Various strategieshave been described to circumvent this problem. Lamp-ing et al15 showed that pre-treatment with tetracycline didincrease ventricular myocyte transfection, possiblythrough the induction of an inflammatory process whichcould have increased a vector uptake at the level of theepicardium. Interestingly, Aoki et al19 have reported myo-cardial transfection after injection within the pericardiumof a hemagglutinating virus of Japan (HVJ)–liposomecomplex. However, their data only showed transfectionin a limited area of the myocardium which extendedthrough few surface layers. Transfected cells includedcardiac myocytes and fibroblasts beneath the pericar-dium and some myocytes in the middle of the myocar-

Gene delivery to the myocardium by intrapericardial injectionY Fromes et al
685
a b
c
Figure 2 Intrapericardial vector delivery in the presence of proteolytic enzymes improves gene transfer. Serial cryosections demonstrate the extent ofX-gal staining of the myocardium. (a) A typical transverse section shows that most transduced myocytes are found in the left ventricle (inferior walland part of the lateral wall) and the interventricular septum. The right ventricle is only partly transfected. (b) A longitudinal section confirms thetransfected area extending from the basis to the apex. (c) Microscopic analysis demonstrates that X-gal staining concerns essentially cardiac myocytes,even though staining is not homogeneous (magnification ×100).
dium around the vasa vasorum.19 However, such treat-ment still remains inefficient.
We used a different strategy and reasoned that a loos-ening of the pericardial barrier might allow the virus tospread into the myocardium. To achieve this, we testedthe possibility of interfering with some of the moleculeswhich constitute this barrier. Among the various compo-nents of the extracellular matrix which composes the car-diac interstitium, molecules of collagen type I and typeIII are important. Thus, as a first step, we tested whetherincreasing concentrations of collagenase could improvediffusion of the recombinant adenovirus following injec-tion in the pericardium. High doses of collagenase (over2 mg) appeared to be lethal after a few days and weestablished that the maximal tolerable dose had to be lessthan 2 mg for an adult rat. However, under these con-ditions, transfection of cardiac myocytes remained poorand still limited to the immediate layer underlying thepericardium (data not shown).
Another major component of the extracellular matrixis hyaluronic acid and so we tested the effect of injectingincreasing concentrations of hyaluronidase ranging from1 to 700 units. Even at the highest doses, this enzymewas totally inefficient in facilitating gene transfer to themyocardium across the pericardial barrier (data notshown).
However, when both enzymes were used in conjunc-tion, a different picture emerged. As shown in Figure 2,optimized concentrations of collagenase (1 mg) and hya-luronidase (500 U), when injected together with therecombinant adenovirus, allow the virus to diffuse in themyocardium. In particular, a longitudinal section of theheart (Figure 2(b)) clearly indicates that b-galactosidaseexpression is distributed from the base down to the apex.There is, however, a restriction in the distribution of theexpressed gene since transfection mostly concerned theanterior wall of the left ventricle, the interventricular sep-tum, part of the lateral wall of the left ventricle and part
Gene delivery to the myocardium by intrapericardial injectionY Fromes et al
686 of the right ventricle (Figure 2a). Figure 2c clearly indi-cates that the cardiac myocytes express the reporter gene.It is also noteworthy that no inflammatory reaction couldbe found in the transfected area at the time of death.
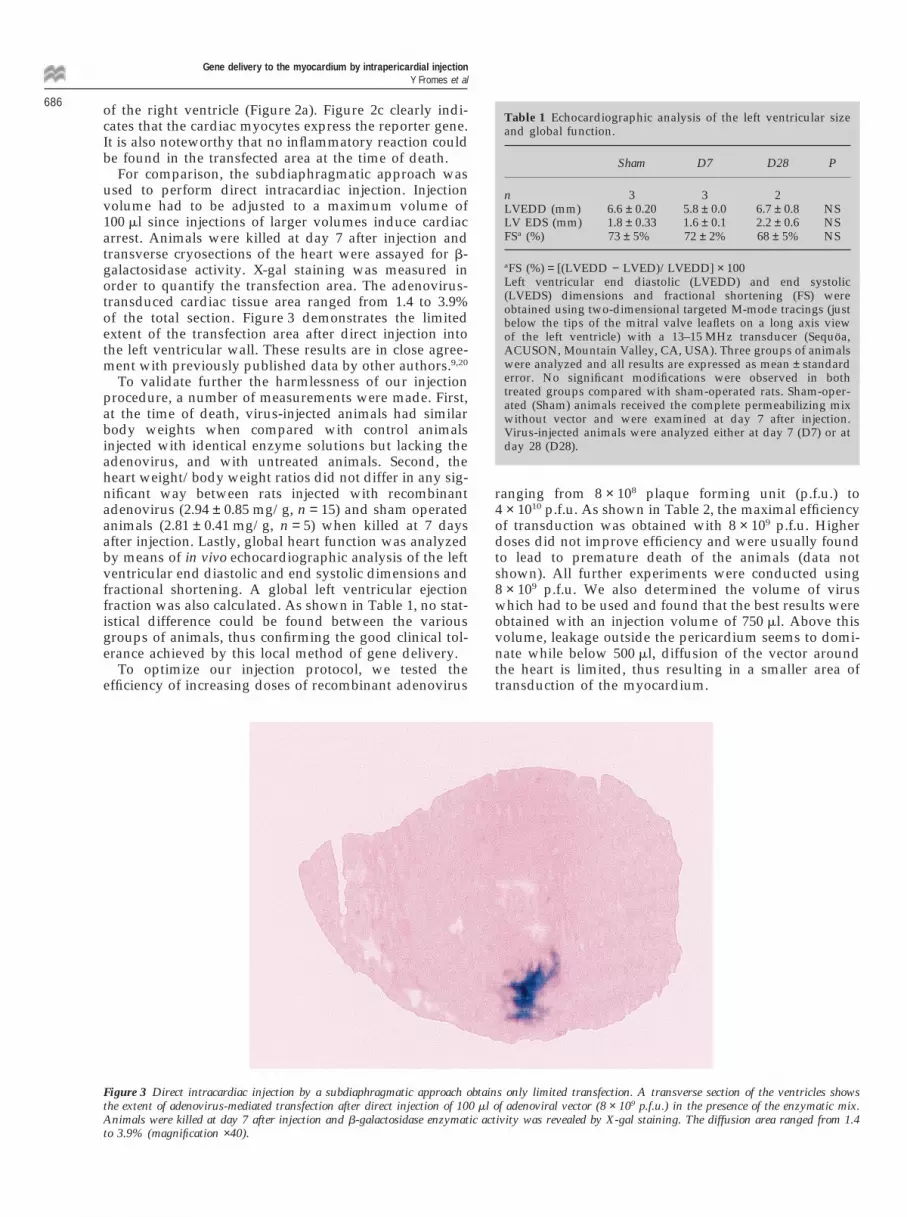
For comparison, the subdiaphragmatic approach wasused to perform direct intracardiac injection. Injectionvolume had to be adjusted to a maximum volume of100 ml since injections of larger volumes induce cardiacarrest. Animals were killed at day 7 after injection andtransverse cryosections of the heart were assayed for b-galactosidase activity. X-gal staining was measured inorder to quantify the transfection area. The adenovirus-transduced cardiac tissue area ranged from 1.4 to 3.9%of the total section. Figure 3 demonstrates the limitedextent of the transfection area after direct injection intothe left ventricular wall. These results are in close agree-ment with previously published data by other authors.9,20
To validate further the harmlessness of our injectionprocedure, a number of measurements were made. First,at the time of death, virus-injected animals had similarbody weights when compared with control animalsinjected with identical enzyme solutions but lacking theadenovirus, and with untreated animals. Second, theheart weight/body weight ratios did not differ in any sig-nificant way between rats injected with recombinantadenovirus (2.94 ± 0.85 mg/g, n = 15) and sham operatedanimals (2.81 ± 0.41 mg/g, n = 5) when killed at 7 daysafter injection. Lastly, global heart function was analyzedby means of in vivo echocardiographic analysis of the leftventricular end diastolic and end systolic dimensions andfractional shortening. A global left ventricular ejectionfraction was also calculated. As shown in Table 1, no stat-istical difference could be found between the variousgroups of animals, thus confirming the good clinical tol-erance achieved by this local method of gene delivery.
To optimize our injection protocol, we tested theefficiency of increasing doses of recombinant adenovirus
Figure 3 Direct intracardiac injection by a subdiaphragmatic approach obtains only limited transfection. A transverse section of the ventricles showsthe extent of adenovirus-mediated transfection after direct injection of 100 ml of adenoviral vector (8 × 109 p.f.u.) in the presence of the enzymatic mix.Animals were killed at day 7 after injection and b-galactosidase enzymatic activity was revealed by X-gal staining. The diffusion area ranged from 1.4to 3.9% (magnification ×40).
Table 1 Echocardiographic analysis of the left ventricular sizeand global function.
Sham D7 D28 P
n 3 3 2LVEDD (mm) 6.6 ± 0.20 5.8 ± 0.0 6.7 ± 0.8 NSLV EDS (mm) 1.8 ± 0.33 1.6 ± 0.1 2.2 ± 0.6 NSFSa (%) 73 ± 5% 72 ± 2% 68 ± 5% NS
aFS (%) = [(LVEDD − LVED)/LVEDD] × 100Left ventricular end diastolic (LVEDD) and end systolic(LVEDS) dimensions and fractional shortening (FS) wereobtained using two-dimensional targeted M-mode tracings (justbelow the tips of the mitral valve leaflets on a long axis viewof the left ventricle) with a 13–15 MHz transducer (Sequoa,ACUSON, Mountain Valley, CA, USA). Three groups of animalswere analyzed and all results are expressed as mean ± standarderror. No significant modifications were observed in bothtreated groups compared with sham-operated rats. Sham-oper-ated (Sham) animals received the complete permeabilizing mixwithout vector and were examined at day 7 after injection.Virus-injected animals were analyzed either at day 7 (D7) or atday 28 (D28).
ranging from 8 × 108 plaque forming unit (p.f.u.) to4 × 1010 p.f.u. As shown in Table 2, the maximal efficiencyof transduction was obtained with 8 × 109 p.f.u. Higherdoses did not improve efficiency and were usually foundto lead to premature death of the animals (data notshown). All further experiments were conducted using8 × 109 p.f.u. We also determined the volume of viruswhich had to be used and found that the best results wereobtained with an injection volume of 750 ml. Above thisvolume, leakage outside the pericardium seems to domi-nate while below 500 ml, diffusion of the vector aroundthe heart is limited, thus resulting in a smaller area oftransduction of the myocardium.

Gene delivery to the myocardium by intrapericardial injectionY Fromes et al
687Table 2 Dose-dependent effect of gene transfer into the rat heart
n Transfected area % P
Control 4 0.00 ± 0.008.0 × 108 6 4.18 ± 2.28 0.00832.6 × 109 4 8.99 ± 3.73 NS4.0 × 109 4 17.18 ± 1.80 0.02098.0 × 109 8 41.10 ± 6.62 0.0066
The influence of the total viral load was estimated by measuringthe X-gal-stained area on transverse sections. Animals werekilled at 6.5 days after injection. This planimetric methods whichintegrates adjacent areas may underestimate sparsely trans-fected myocardial cells, but is almost operator independent onsuccessive sections. Results are expressed as mean ± standarderror and were compared pairwise by statistical tools.
b
a
Figure 4 Intrapericardial injections may be achieved in mice. C57BL/6 mice were injected locally with 4 × 108 p.f.u. of recombinant adenovirus. (a)Serial cryosections of mouse heart demonstrate gene transfer into the heart. (b) A detailed view shows the staining pattern of galactosidase activity afteradenovirus-induced transfection. X-gal staining is found in epicardial layers on the cross-section of the mouse heart. Larger areas of transfection canbe seen on the interventricular septum and anterior wall of the left ventricle.
A time-course analysis of transgene expression showsthat, already at day 1, a significant expression of thetransgene can be detected which increases until day 7when 40.8 ± 7.3% (n = 8) of the myocardium is transfectedby the adenovirus (Table 3). Thereafter, transgeneexpression progressively declined due to a significantinflammatory reaction which was found around all areasexpressing the transgene (data not shown). This time-course correlates well with previous results reported on
Table 3 Time course of transgene expression in the rat heart
n Transfected area % P
Control 4 0.00 ± 0.00D1 4 16.37 ± 13.70 0.0472D7 8 40.81 ± 9.08 0.0108D14 4 22.54 ± 7.83 0.0174D21 4 6.35 ± 1.12 0.0209D28 4 0.57 ± 0.21 0.0209D42 4 0.40 ± 0.56 NS
Gene expression in the myocardium was followed from day 1to day 42 after injection. X-gal-stained areas were expressed asa percentage of the total transverse section area. Results areexpressed as mean ± standard error. The evolution of this valuewas analyzed pairwise by statistical tools.
direct injection of adenoviral vectors into the myocar-dium, where transgene expression strongly increasedduring the first 7 days and then progressively declinedat 14 and 21 days.4 We did not try to immunosuppressour animals since our goal was not to look for long-termgene expression, but to establish the conditions whichwould allow an optimal viral transduction of the myocar-dium. It is well known that first generation adenoviralvectors induce an immune response that is a major cause

Gene delivery to the myocardium by intrapericardial injectionY Fromes et al
688 of transient gene expression in immunocompetent ani-mals and avoidance of an immune response may extendexpression of genes introduced into the myocardium.21,22
Tissues other than the myocardium were routinelyassayed for b-galactosidase activity. As anticipated, lung,liver, spleen and kidneys were always positive; however,the diaphragm muscle never showed evidence of trans-duction by the adenovirus, indicating that our transdi-aphramatic injection did not induce any transfection ofthe diaphragm.
Our strategy is not limited to the rat, and Figure 4shows that a comparable result can be obtained withC57BL/6 mice. The distribution of expression is similarto that found in the rat, especially with regard to theregions of the myocardium which are excluded such asthe left ventricle (compare Figure 2 and Figure 4).
In conclusion, our results demonstrate that intra-peri-cardial injection of recombinant adenovirus vectors in thepresence of proteolytic enzymes leads to an efficient andsafe strategy to deliver a transgene to the heart. No dam-age to the global heart function could be detected by ech-ocardiographic measurements nor could we find any sig-nificant structural alterations of the myocardium at thisearly stage. As anticipated, we subsequently observed aninflammatory reaction due to the immunogenic potentialof both the adenovirus vector and the reporter gene. Forfuture development of this strategy it is obvious thatother vectors will need to be used which will include bet-ter tailored defective adenovirus or less immunogenicviruses such as the adeno-associated virus23,24 or evennaked DNA. Moreover, the fact that other noncardiactissues were also efficiently transduced emphasizes theneed for another level of control. This will be achievedby placing the therapeutic gene under the control of acardiac-specific promoter. Finally, the fact that we couldtranspose our method to another animal model andobtain similar results prompts us to suggest that thisapproach will be useful for future gene therapy inheart disease.
AcknowledgementsWe thank the Vector Core of the University Hospital ofNantes supported by the Association Francaise contre lesMyopathies (AFM) for providing the AdCMVlacZ vector.
References1 Lin H et al. Expression of recombinant genes in myocardium in
vivo after direct injection of DNA. Circulation 1990; 82: 2217–2221.
2 Stratford-Perricaudet LD, Makeh I, Perricaudet M, Briand P.Widespread long-term gene transfer to mouse skeletal musclesand heart. J Clin Invest 1992; 90: 626–630.
3 Von Harsdorf R et al. Gene injection into canine myocardium
as a useful model for studying gene expression in the heart oflarge mammals. Circ Res 1993; 72: 688–695.
4 French B, Mazur W, Geske R, Bolli R. Direct in vivo gene transferinto porcine myocardium using replication-deficient adenoviralvectors. Circulation 1994; 90: 2414–2424.
5 Lee J et al. Cardiac gene transfer by intracoronary infusion ofadenovirus vector-mediated reporter gene in the transplantedmouse heart. J Thorac Cardiovasc Surg 1996; 111: 246–252.
6 Coffin RS et al. Gene therapy to the heart in vivo and to cardiacmyocytes and vascular smooth muscle cells in vitro using herpesvirus vectors. Gene Therapy 1996; 3: 560–566.
7 Kypson AP et al. Ex vivo adenovirus-mediated gene transfer tothe adult rat heart. J Thorac Cardiovasc Surg 1998; 115: 623–630.
8 Magovern CJ et al. Direct in vivo gene transfer to canine myocar-dium using a replication-deficient adenovirus vector. Ann ThoracSurg 1996; 62: 425–434.
9 Guzman R et al. Efficient gene transfer into the myocardium bydirect injection of adenovirus vectors. Circ Res 1993; 73: 1202–1207.
10 Barr E et al. Efficient catheter-mediated gene transfer into theheart using replication-defective adenovirus. Gene Therapy 1994;1: 51–58.
11 Budker V et al. The efficient expression of intravascularly deliv-ered DNA in rat muscle. Gene Therapy 1998; 5: 272–276.
12 Donahue JK et al. Ultrarapid, highly efficient viral gene transferto the heart. Proc Natl Acad Sci USA 1997; 94: 4664–4668.
13 Wright M et al. b-Galactosidase staining following intracoronaryinfusion of cationic liposomes in the in vivo rabbit heart is pro-duced by microinfarction rather than effective gene transfer: acautionary tale. Gene Therapy 1998; 5: 301–308.
14 Davidson BL et al. A model system for in vivo gene transfer intothe central nervous system using an adenoviral vector. Nat Genet1993; 3: 219–223.
15 Lamping K et al. Intrapericardial administration of adenovirusfor gene transfer. Am J Physiol 1997; 272: H310-H317.
16 Lim CS et al. Direct in vivo gene transfer into the coronary andperipheral vasculatures of the intact dog. Circulation 1991; 83:2007–2011.
17 Muhlhauser J et al. Safety and efficacy of in vivo gene transferinto the porcine heart with replication-deficient, recombinantadenovirus vectors. Gene Therapy 1996; 3: 145–153.
18 Rothmann T et al. Heart muscle-specific gene expression usingreplication defective recombinant adenovirus. Gene Therapy1996; 3: 919–926.
19 Aoki M et al. Efficient in vivo gene transfer into the heart in therat myocardial infarction model using the HVJ(haemagglutinating virus of Japan)-liposome method. J Mol CellCardiol 1997; 29: 949–959.
20 Kass-Eisler A et al. Quantitative determination of adenovirus-mediated gene delivery to rat cardiac myocytes in vitro and invivo. Proc Natl Acad Sci USA 1993; 90: 11498–11502.
21 Gilgenkrantz H et al. Transient expression of genes transferredin vivo into heart using first-generation adenoviral vectors: roleof the immune response. Hum Gene Ther 1995; 6: 1265–1274.
22 Quinones M et al. Avoidance of immune response prolongsexpression of genes delivered to the adult rat myocardium byreplication-defective adenovirus. Circulation 1996; 94: 1394–1401.
23 Lynch CM et al. Adeno-associated virus vectors for vasculargene delivery. Circ Res 1997; 80: 497–505.
24 Fisher KJ et al. Recombinant adeno-associated virus for muscledirected gene therapy. Nature Med 1997; 3: 306–312.
Related Documents











