Gazing into the Crystal Ball: How will Evolving Gazing into the Crystal Ball: How will Evolving Future Therapies Change how we Position Biologics for Future Therapies Change how we Position Biologics for Use in IBD? Use in IBD? William J. Sandborn, MD William J. Sandborn, MD Professor & Chief, Division of Professor & Chief, Division of Gastroenterology Gastroenterology Director, UCSD IBD Center Director, UCSD IBD Center

Gazing into the Crystal Ball: How will Evolving Future Therapies Change how we Position Biologics for Use in IBD? William J. Sandborn, MD Professor & Chief,
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Gazing into the Crystal Ball: How will Evolving Future Therapies Gazing into the Crystal Ball: How will Evolving Future Therapies Change how we Position Biologics for Use in IBD?Change how we Position Biologics for Use in IBD?
William J. Sandborn, MDWilliam J. Sandborn, MD Professor & Chief, Division of GastroenterologyProfessor & Chief, Division of Gastroenterology Director, UCSD IBD CenterDirector, UCSD IBD Center

Therapies for IBD: the PipelineTherapies for IBD: the Pipeline
• Anti-Selective Adhesion Anti-Selective Adhesion MoleculeMoleculeAnti-integrin antibodiesAnti-integrin antibodies
Etrolizumab (anti-Etrolizumab (anti-ββ7)7)AMG 181 (anti-AMG 181 (anti- β β7)7)Anti-Anti-MAdCAM-1MAdCAM-1
• S1P1 Receptor modulator S1P1 Receptor modulator (RPC1063)(RPC1063)
• Antagonist to Janus kinase 3 Antagonist to Janus kinase 3 (JAK3)(JAK3)TofacitinibTofacitinib
• Anti-Interleukin 12/23Anti-Interleukin 12/23Ustekinumab (CNTO 1275, Ustekinumab (CNTO 1275, Stelara)Stelara)
• Anti-Interleukin-23Anti-Interleukin-23• Anti-interleukin 6Anti-interleukin 6• Anti-IP 10 antibodyAnti-IP 10 antibody• EldelumabEldelumab
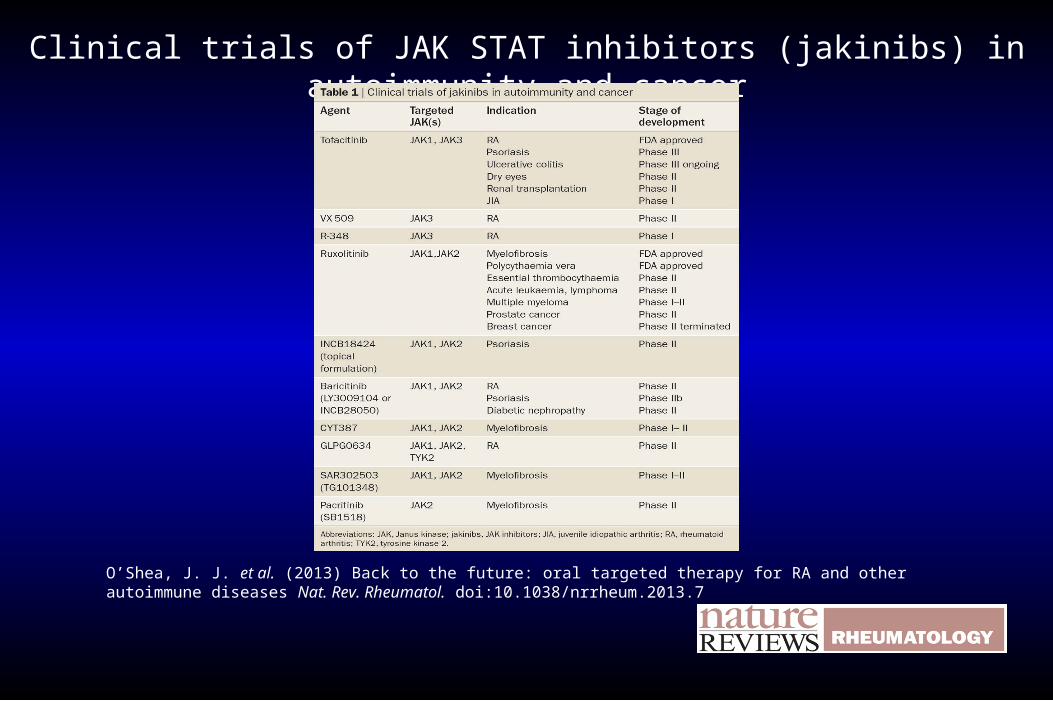
Clinical trials of JAK STAT inhibitors (jakinibs) in autoimmunity and cancer
O’Shea, J. J. et al. (2013) Back to the future: oral targeted therapy for RA and other autoimmune diseases Nat. Rev. Rheumatol. doi:10.1038/nrrheum.2013.7
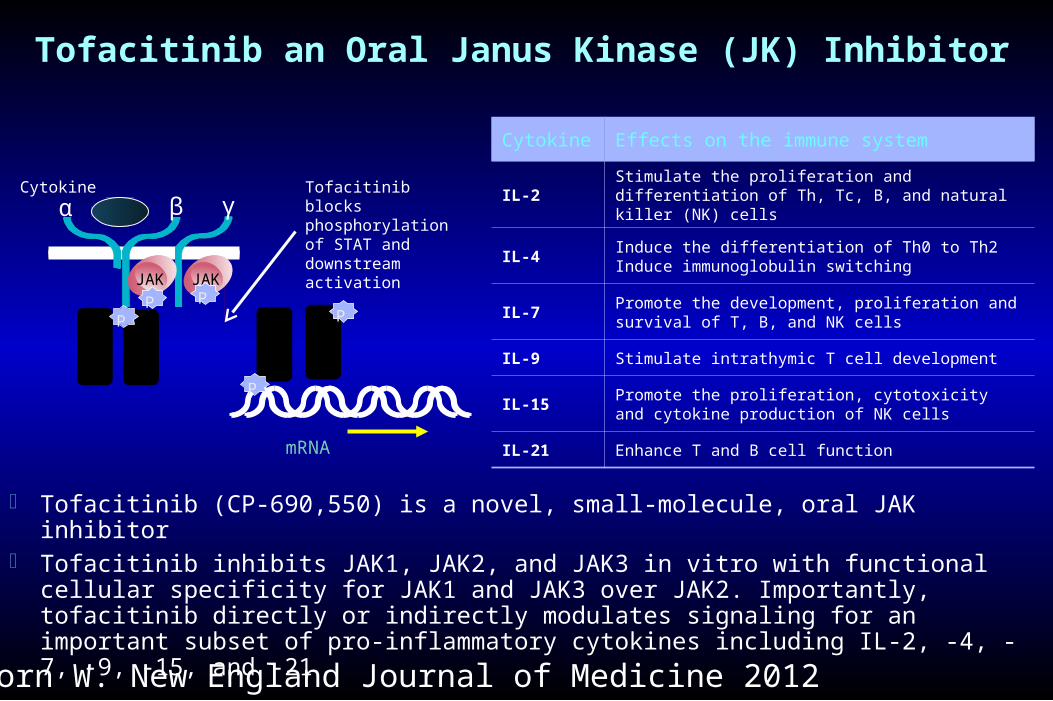
Tofacitinib an Oral Janus Kinase (JK) Inhibitor
Tofacitinib blocks phosphorylation of STAT and downstream activation
JAK
α
STAT
STAT
mRNA
JAKPP
STAT
STAT
P
P
P
β γCytokine
Cytokine Effects on the immune system
IL-2Stimulate the proliferation and differentiation of Th, Tc, B, and natural killer (NK) cells
IL-4Induce the differentiation of Th0 to Th2Induce immunoglobulin switching
IL-7Promote the development, proliferation and survival of T, B, and NK cells
IL-9 Stimulate intrathymic T cell development
IL-15Promote the proliferation, cytotoxicity and cytokine production of NK cells
IL-21 Enhance T and B cell function
Tofacitinib (CP-690,550) is a novel, small-molecule, oral JAK inhibitor Tofacitinib inhibits JAK1, JAK2, and JAK3 in vitro with functional cellular specificity for JAK1 and JAK3
over JAK2. Importantly, tofacitinib directly or indirectly modulates signaling for an important subset of pro-inflammatory cytokines including IL-2, -4, -7, -9, -15, and -21
Sandborn W. New England Journal of Medicine 2012
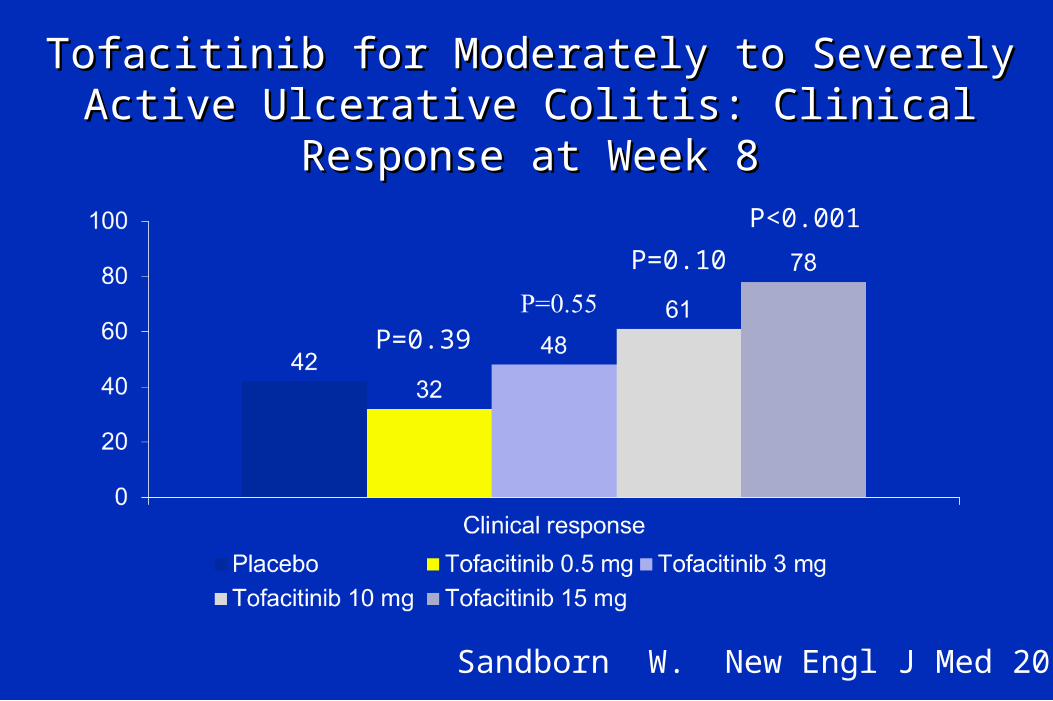
Tofacitinib for Moderately to Severely Active Tofacitinib for Moderately to Severely Active Ulcerative Colitis: Clinical Response at Week 8Ulcerative Colitis: Clinical Response at Week 8
Sandborn W. New Engl J Med 2012.
P=0.39
P=0.10
P<0.001

Tofacitinib for Moderately to Severely Active Tofacitinib for Moderately to Severely Active Ulcerative Colitis: Clinical Remission at Week 8Ulcerative Colitis: Clinical Remission at Week 8
Sandborn W. New Engl J Med 2012.
P=0.76
P<0.001 P<0.001

Tofacitinib for Moderately to Severely Active Tofacitinib for Moderately to Severely Active Ulcerative Colitis: Endoscopic ResponseUlcerative Colitis: Endoscopic Response
Sandborn W. New Engl J Med 2012.
P=0.64
P=.07P=.001

Tofacitinib for Moderately to Severely Active Crohn’s Tofacitinib for Moderately to Severely Active Crohn’s Disease: Clinical Remission at Week 4Disease: Clinical Remission at Week 4
Sandborn W. Clin Gastroenterol Hepatol 2014
P=.42
P=.54

Mean percentage change from baseline in log transformed CRP (mg/L) in those patients with baseline CRP ≥5 mg/L (B)
Sandborn W. Clin Gastroenterol Hepatol 2014

Mean percentage change from baseline in log transformed fecal calprotectin (mg/kg) in in those patients with baseline
fecal calprotectin ≥250 mg/kg (B)
Sandborn W. Clin Gastroenterol Hepatol 2014
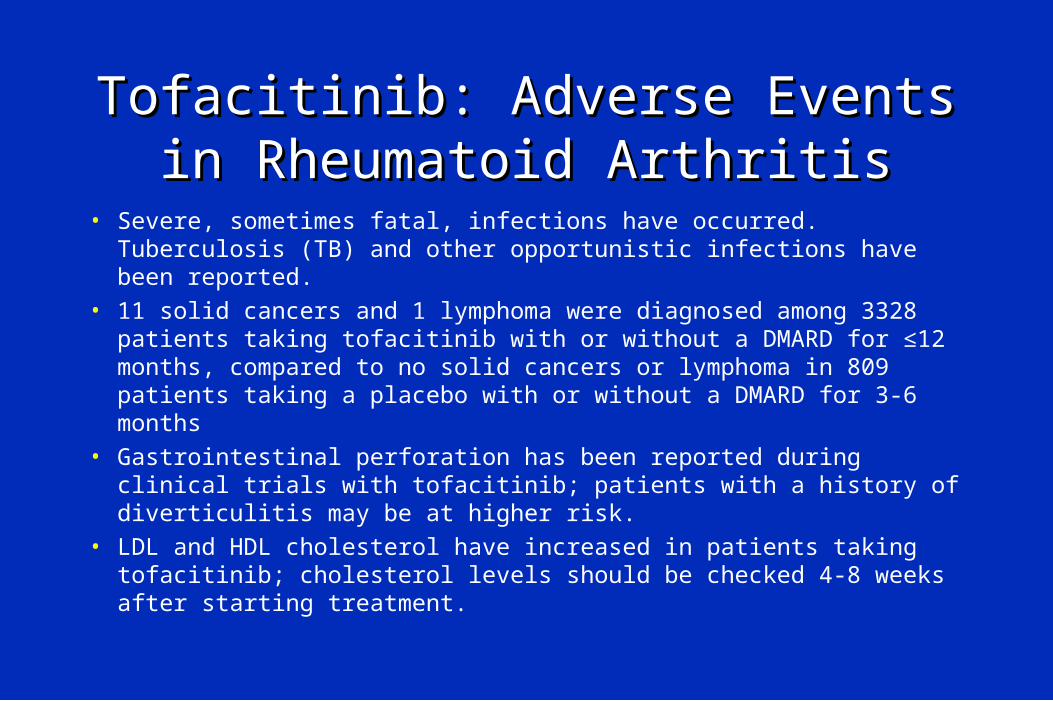
Tofacitinib: Adverse Events in Tofacitinib: Adverse Events in Rheumatoid ArthritisRheumatoid Arthritis
• Severe, sometimes fatal, infections have occurred. Tuberculosis (TB) and other opportunistic infections have been reported.
• 11 solid cancers and 1 lymphoma were diagnosed among 3328 patients taking tofacitinib with or without a DMARD for ≤12 months, compared to no solid cancers or lymphoma in 809 patients taking a placebo with or without a DMARD for 3-6 months
• Gastrointestinal perforation has been reported during clinical trials with tofacitinib; patients with a history of diverticulitis may be at higher risk.
• LDL and HDL cholesterol have increased in patients taking tofacitinib; cholesterol levels should be checked 4-8 weeks after starting treatment.

Tofacitinib: Adverse Events in Tofacitinib: Adverse Events in Rheumatoid Arthritis (Continued)Rheumatoid Arthritis (Continued)
• Elevations in liver aminotransferase levels have occurred; liver enzymes should be monitored regularly.
• Lymphocytopenia, neutropenia and low hemoglobin levels can develop in patients taking tofacitinib. Lymphocytes should be monitored at baseline and then every 3 months. Neutrophils and hemoglobin levels should be monitored at baseline, after 4-8 weeks of treatment, and then every 3 months.
• Tofacitinib is classified as category C (risk cannot be ruled out) for use during pregnancy. It is fetocidal and teratogenic in rats and rabbits.

CD4+
TCR
AntigenPresenting Cell
MHCII
Ag
StimulusTLR?
IFNg(Th1)
p40p35
Biology of Interleukins 12 and 23Biology of Interleukins 12 and 23
IL-12
IL-12R1
2
IL-23
p40p19
IL-17(Th17)IL-23R
IL-12R1
Anti-IL-12/23
Anti-IL-12/23
X
• Ustekinumab and Ustekinumab and briakinumab are fully briakinumab are fully human IgG1 monoclonal human IgG1 monoclonal antibodiesantibodies
• Bind the p40 subunit of Bind the p40 subunit of human IL-12/23human IL-12/23
• Prevent IL-12 and IL-23 Prevent IL-12 and IL-23 from binding IL-12Rb1from binding IL-12Rb1
• Normalize IL-12 and IL-Normalize IL-12 and IL-23 mediated signaling, 23 mediated signaling, cellular activation, and cellular activation, and cytokine productioncytokine production
• In development in In development in Crohn’s disease and Crohn’s disease and psoriasispsoriasis
Anti-IL-12/23Anti-IL-12/23
Ustekinumab (Stelara)Ustekinumab (Stelara)
• Approved for psoriasis and psoriatic arthritis Approved for psoriasis and psoriatic arthritis at a dose of 45 mg (90 mg for weight > 100 at a dose of 45 mg (90 mg for weight > 100 kg) at weeks 0 and 4 and then every 12 kg) at weeks 0 and 4 and then every 12 weeks weeks
• Indication is for the treatment of adults with Indication is for the treatment of adults with moderate to severe plaque psoriasis who moderate to severe plaque psoriasis who are candidates for phototherapy or systemic are candidates for phototherapy or systemic therapytherapy

Ustekinumab (anti-IL 12/23p40) for Induction of Clinical Ustekinumab (anti-IL 12/23p40) for Induction of Clinical Response in Moderate to Severe Crohn’s DiseaseResponse in Moderate to Severe Crohn’s Disease
Sandborn WJ. Gastroenterology 2008;135:1130-1141.
UstekinumabPlacebo
2 4 6 80
20
40
60
80
100
Weeks
Pat
ient
s (%
)
2 4 6 80
20
40
60
80
100
Weeks
Infli
xim
ab-E
xper
ienc
edP
atie
nts
(%)
P=.046 P=.001 P=.004 P=.022
0
0.2
0.4
0.6
0.8
1.2
1.0
IntravenousSubcutaneous Intravenous Subcutaneous
Placebo
Med
ian
CR
P (
mg/
dL)
Ustekinumab
P=.335P=.02 P=.019 P=.337
Week 8Week 0
All Patients Previously Treated with Infliximab
CRP in All Patients

Ustekinumab (Anti-IL-12/23p40) for Induction of Moderate to Severe Ustekinumab (Anti-IL-12/23p40) for Induction of Moderate to Severe Crohn’s DiseaseCrohn’s Disease
+p<0.05 vs. PBO by CMH test
+
+
+
++
+
+
Sandborn WJ. N Engl J Med 2012; 367:1519-1528
+
+
+
Clinical Response Clinical Remission

Ustekinumab (Anti-IL-12/23p40) for Maintenance of Ustekinumab (Anti-IL-12/23p40) for Maintenance of Moderate to Severe Crohn’s DiseaseModerate to Severe Crohn’s Disease
p=0.029
p<0.001
Sandborn WJ. N Engl J Med 2012; 367:1519-1528

Sandborn WJ, et al. N Engl J Med 2012;367:1519-28.
Corticosteroid-free Remission at 22 Weeks Following Corticosteroid-free Remission at 22 Weeks Following Treatment with UstekinumabTreatment with Ustekinumab

Ustekinumab: Adverse Events in Psoriasis Ustekinumab: Adverse Events in Psoriasis and Psoriatic Arthritisand Psoriatic Arthritis
• Serious infections requiring hospitalization occurred Serious infections requiring hospitalization occurred including diverticulitis, cellulitis, pneumonia, appendicitis, including diverticulitis, cellulitis, pneumonia, appendicitis, cholecystitis, sepsis, osteomyelitis, viral infections, cholecystitis, sepsis, osteomyelitis, viral infections, gastroenteritis and urinary tract infectionsgastroenteritis and urinary tract infections
• 1.7% of ustekinumab-treated patients reported malignancies 1.7% of ustekinumab-treated patients reported malignancies excluding non-melanoma skin cancers (0.60 per hundred excluding non-melanoma skin cancers (0.60 per hundred patient-years of follow-up). Non-melanoma skin cancer was patient-years of follow-up). Non-melanoma skin cancer was reported in 1.5% of ustekinumab-treated patients (0.52 per reported in 1.5% of ustekinumab-treated patients (0.52 per hundred patient-years of follow-up). Malignancies other than hundred patient-years of follow-up). Malignancies other than non-melanoma skin cancer in ustekinumab-treated patients non-melanoma skin cancer in ustekinumab-treated patients were similar in type and number to what would be expectedwere similar in type and number to what would be expected
Ustekinumab: Adverse Events in Psoriasis Ustekinumab: Adverse Events in Psoriasis and Psoriatic Arthritis (Continued)and Psoriatic Arthritis (Continued)
• Reversible Posterior Leukoencephalopathy Syndrome (RPLS). RPLS is a neurological disorder, which is not caused by demyelination or a known infectious agent. RPLS can present with headache, seizures, confusion and visual disturbances. Conditions with which it has been associated include preeclampsia, eclampsia, acute hypertension, cytotoxic agents and immunosuppressive therapy. One case of RPLS was observed in the clinical trial safety databases for psoriasis and psoriatic arthritis.

• S1P1R agonism induces receptor internalization lymphocytes lose response to S1P gradient
• Become trapped in lymph nodes causing peripheral lymphopenia
• Upon drug withdrawal receptor expression is restored and lymphocytes leave nodes reversing lymphopenia
Sphingosine 1‐Phosphate Receptor 1 Modulation Sphingosine 1‐Phosphate Receptor 1 Modulation Mechanism of ActionMechanism of Action
Courtesy Dr. Alan Olsen

RPC1063 (an S1P receptor modulator)RPC1063 (an S1P receptor modulator)
• RCT of oral RPC1063 at doses of 0.5 mg and 1 mg versus RCT of oral RPC1063 at doses of 0.5 mg and 1 mg versus placebo in 199 patients with moderate to severe UCplacebo in 199 patients with moderate to severe UC
• Remission at week 8 in 16.4% on 1 mg dose (p<0.05), 13.8% Remission at week 8 in 16.4% on 1 mg dose (p<0.05), 13.8% on 0.5 mg dose (p=NS), and 6.2% on placeboon 0.5 mg dose (p=NS), and 6.2% on placebo
• Clinical response at week 8 in 58.2% on 1 mg dose (p<0.05), Clinical response at week 8 in 58.2% on 1 mg dose (p<0.05), and 36.9% on placeboand 36.9% on placebo
• All other secondary endpoints at week 8, including change in All other secondary endpoints at week 8, including change in the Mayo score and mucosal improvement on endoscopy the Mayo score and mucosal improvement on endoscopy were also positive and statistically significant for the 1 mg were also positive and statistically significant for the 1 mg dose, trends were observed for the 0.5 mg dose group that dose, trends were observed for the 0.5 mg dose group that demonstrated dose responsedemonstrated dose response
Receptos press release October 27, 2014

ConclusionsConclusions
• Agents targeted against multiple targets Agents targeted against multiple targets including the p40 subunit of interleukin including the p40 subunit of interleukin 12/23, JAK, and S1P receptor hold great 12/23, JAK, and S1P receptor hold great promise for the futurepromise for the future
Related Documents











