REVIEW Fruit and vegetable intake and bone health in women aged 45 years and over: a systematic review M. Hamidi & B. A. Boucher & A. M. Cheung & J. Beyene & P. S. Shah Received: 26 September 2010 / Accepted: 16 November 2010 / Published online: 17 December 2010 # International Osteoporosis Foundation and National Osteoporosis Foundation 2010 Abstract Summary High fruit and vegetable intake may be associated with improved bone status among women aged ≥45 years. This is the first systematic review that specifically assessed this association and identified research gaps. The benefits of fruit and vegetables (F&V) on bone health remain unclear. Further studies are needed. Introduction F&V have several components that are beneficial to bones. Some studies report that high F&V intake is associated with improved bone status in middle aged and aged women; however, findings are inconsistent. The objective was to systematically review observational and interventional studies that investigated the effects of F&V intake on incidence of osteoporotic fractures, bone mineral density (BMD), and M. Hamidi Women’ s Health and Osteoporosis Programs, University Health Network, 200 Elizabeth Street, 7 Eaton North-228-A, Toronto, ON M5G 2C4, Canada e-mail: [email protected] A. M. Cheung (*) Women’ s Health and Osteoporosis Programs, University Health Network, 200 Elizabeth Street, 7 Eaton North-221, Toronto, ON M5G 2C4, Canada e-mail: [email protected] M. Hamidi : A. M. Cheung Institute of Medical Science, University of Toronto, Toronto, ON, Canada B. A. Boucher Prevention and Cancer Control, Cancer Care Ontario, Toronto, ON, Canada e-mail: [email protected] B. A. Boucher Department of Nutritional Sciences, University of Toronto, Toronto, ON, Canada B. A. Boucher : A. M. Cheung : J. Beyene : P. S. Shah Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada J. Beyene e-mail: [email protected] P. S. Shah e-mail: [email protected] A. M. Cheung Divisions of General Internal Medicine and Endocrinology and Metabolism, Department of Medicine, University of Toronto, Toronto, ON, Canada A. M. Cheung : J. Beyene Department of Health Policy, Management and Evaluation, University of Toronto, Toronto, ON, Canada J. Beyene Population Health Sciences, Research Institute of the Hospital for Sick Children, Toronto, ON, Canada J. Beyene Program in Population Genomics, Department of Clinical Epidemiology and Biostatistics, Faculty of Health Sciences, McMaster University, Hamilton, ON, Canada J. Beyene Department of Pathology and Molecular Medicine, Department of Medicine, McMaster University, Hamilton, ON, Canada J. Beyene : P. S. Shah Department of Paediatrics, Mount Sinai Hospital, Toronto, ON, Canada Osteoporos Int (2011) 22:1681–1693 DOI 10.1007/s00198-010-1510-0

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW
Fruit and vegetable intake and bone health in women aged45 years and over: a systematic review
M. Hamidi & B. A. Boucher & A. M. Cheung & J. Beyene &
P. S. Shah
Received: 26 September 2010 /Accepted: 16 November 2010 /Published online: 17 December 2010# International Osteoporosis Foundation and National Osteoporosis Foundation 2010
AbstractSummary High fruit and vegetable intake may be associatedwith improved bone status among women aged ≥45 years.This is the first systematic review that specifically assessedthis association and identified research gaps. The benefits offruit and vegetables (F&V) on bone health remain unclear.Further studies are needed.
Introduction F&V have several components that are beneficialto bones. Some studies report that high F&V intake isassociated with improved bone status in middle aged and agedwomen; however, findings are inconsistent. The objective wasto systematically review observational and interventionalstudies that investigated the effects of F&V intake on incidenceof osteoporotic fractures, bone mineral density (BMD), and
M. HamidiWomen’s Health and Osteoporosis Programs,University Health Network,200 Elizabeth Street, 7 Eaton North-228-A,Toronto, ON M5G 2C4, Canadae-mail: [email protected]
A. M. Cheung (*)Women’s Health and Osteoporosis Programs,University Health Network,200 Elizabeth Street, 7 Eaton North-221,Toronto, ON M5G 2C4, Canadae-mail: [email protected]
M. Hamidi :A. M. CheungInstitute of Medical Science, University of Toronto,Toronto, ON, Canada
B. A. BoucherPrevention and Cancer Control, Cancer Care Ontario,Toronto, ON, Canadae-mail: [email protected]
B. A. BoucherDepartment of Nutritional Sciences, University of Toronto,Toronto, ON, Canada
B. A. Boucher :A. M. Cheung : J. Beyene : P. S. ShahDalla Lana School of Public Health, University of Toronto,Toronto, ON, Canada
J. Beyenee-mail: [email protected]
P. S. Shahe-mail: [email protected]
A. M. CheungDivisions of General Internal Medicine and Endocrinologyand Metabolism, Department of Medicine, University of Toronto,Toronto, ON, Canada
A. M. Cheung : J. BeyeneDepartment of Health Policy, Management and Evaluation,University of Toronto,Toronto, ON, Canada
J. BeyenePopulation Health Sciences,Research Institute of the Hospital for Sick Children,Toronto, ON, Canada
J. BeyeneProgram in Population Genomics, Department of ClinicalEpidemiology and Biostatistics, Faculty of Health Sciences,McMaster University,Hamilton, ON, Canada
J. BeyeneDepartment of Pathology and Molecular Medicine,Department of Medicine, McMaster University,Hamilton, ON, Canada
J. Beyene : P. S. ShahDepartment of Paediatrics, Mount Sinai Hospital,Toronto, ON, Canada
Osteoporos Int (2011) 22:1681–1693DOI 10.1007/s00198-010-1510-0

bone turnover markers (BTM) in women aged ≥45 years and toidentify potential research gaps.Methods Electronic databases were searched, and peer-reviewed manuscripts published in English, with F&Vintake as a main dietary exposure, were included. Dataselection, extraction, and evaluation of risk of bias wereperformed independently by two reviewers.Results Eight studies were included. One cohort studyreported cross-sectional as well as longitudinal data. Therewas significant between-study heterogeneity in design,definition, and amount of F&V intake, outcomes, analyses,and reporting of results. Two studies had low, two hadmoderate, and four had high risk of bias. Among reportswith low or moderate risk of bias, two cross-sectionalanalyses reported positive associations between F&V intakeand BMD of the forearm, lumbar spine, or total hip,whereas one randomized controlled trial and two prospectivecohort analyses reported no effects. One trial reported noassociations between F&Vand BTM.Conclusions Based on limited evidence, the benefits of F&Von bone health remain unclear for women aged ≥45 years.Further studies with low risk of bias are needed.
Keywords Aging . Bone . Bone mineral density .
Bone turnover markers . Fractures . Fruit and vegetables .
Nutrition . Osteoporosis .Women
Introduction
Osteoporosis is a chronic and often asymptomatic diseasethat involves bone loss leading to fractures and significantpersonal and societal burden [1]. About 80% of thoseaffected by osteoporosis are women [2]. Due to hormonalchanges around the age of 45 years, an increased rate ofbone loss places women at higher risk for osteoporoticfractures [3]. Among women 45 years and older, osteoporosisaccounts for more days spent in hospital compared with othermajor diseases such as diabetes, heart attack, and breast cancer[4]. To prevent osteoporotic fractures, long-term drug therapyis required; however, the observed adherence to such therapyis poor due to reasons such as absence of bone losssymptoms, costs, and adverse effects [5–8]. Therefore,identifying non-pharmaceutical interventions, such as dietaryfactors that can reduce the rate of bone loss in this population,is of great interest [9, 10].
Diet is a modifiable lifestyle factor in the prevention andmanagement of osteoporosis [11–13]. Dairy products arewell established as an important food group for bone health,but less is known about other food groups [14, 15]. Severalstudies have investigated the possible beneficial effect offruit and vegetable (F&V) intake on bone health, and theresults have been conflicting. Fruit and vegetables contain
many components such as minerals (e.g., magnesium,potassium, and calcium), vitamins (e.g., vitamins C andK), antioxidants (e.g., polyphenols), and phytochemicals (e.g., phytoestrogens) that are involved in bone metabolismand can synergistically affect bone health [9, 11, 16–18].Due to their high potassium and magnesium content, dietshigh in F&V have a lower dietary acid load and maypromote a positive calcium balance [19, 20]. High acid loadis known to inhibit osteoblast function and increaseosteoclast activity resulting in reduced bone formation andincreased bone resorption [21, 22]. Fruit and vegetables arealso high in vitamin K and vitamin C which, along withmagnesium, are involved in the synthesis of bone matrix [11,17]. Additionally, phytochemicals and other antioxidantspresent in F&V could protect bone by reducing resorptiondue to high oxidative stress [9, 11, 23].
The number of studies on F&V intake and bone healthcontinues to grow with, often, contradictory results.Determining the effect of F&V intake on bone healthamong aging women is clearly an important objective withimplications for setting nutritional guidelines for theprevention and management of postmenopausal osteoporosis.Thus, the objective of this study was to perform a systematicreview of the literature to summarize the evidence on theeffect of F&V on fragility fractures, bone mineral density(BMD), or bone turnover markers (BTM) among womenaged ≥45 years and to identify potential research gaps.
Methods
Eligibility criteria
A protocol was developed prior to conducting the review.No attempt was made to publish the review protocol.Interventional (randomized or nonrandomized controlledtrials) and observational studies (cohort, case-control, orcross-sectional) that specifically reported F&V intake as amain dietary exposure among community-living women45 years and older, at baseline or at the time of interview,were included. Published peer-reviewed articles andabstracts, and book chapters reporting studies in humans,written in English, were eligible for inclusion.
We excluded studies limited to (1) individual fruits (e.g.,plums), vegetables (e.g., onions), or select F&V categoriesbased on specific nutrient content (e.g., high in vitamin C);(2) biomarkers of F&V intake (e.g., serum carotenoids, netacid excretion); (3) nutrients or food components (e.g.,potassium, magnesium, vitamin C, phytochemicals, vegetableprotein); (4) specific eating patterns such as Western,Mediterranean, and vegetarian; and (5) where the independenteffect of F&V could not be separated from that of other foodsor food groups.
1682 Osteoporos Int (2011) 22:1681–1693

We included fractures, BMD, and BTM as outcomes ofbone health. Clinically, osteoporosis manifests itself by theoccurrence of fragility fractures of the hip, vertebrae, andforearm. Fragility fractures are defined as those resultingfrom no apparent or minimal trauma, such as falls fromstanding height or less, and verified by X-ray or otherimaging reports (e.g., magnetic resonance imaging) [24].Since few studies directly link F&V intake with fractures,BMD at lumbar spine, total hip, femoral neck or forearm(radius), measured primarily by dual-energy X-ray absorp-tiometry (DXA), was chosen as an intermediate outcomesince it is often used as a surrogate for fracture risk [25, 26].Cohort studies and randomized controlled trials (RCTs) witha follow-up of at least 6 months for BMD were included as,in the absence of disease and medications, the estimatedbone remodeling cycle is 6 months, and it is unlikely thatany intervention-related BMD changes happen prior to thisperiod [27]. Bone turnover markers include serum or urinarybone resorption and/or bone formation biomarkers, such ascarboxy-terminal telopeptides of collagen cross-links (CTx;resorption markers) and bone alkaline phosphatase, procol-lagen extension peptides, or osteocalcin (formation markers).Independent of BMD, in the absence of drug therapies,increased BTM indicate detrimental effects on bone micro-architecture and fragility [28, 29].
Information sources and search strategy
We searched electronic databases to July 31, 2010: MED-LINE (from 1950), EMBASE (from 1980), CAB (from1973), PUBMED, the Cochrane Library (Issue 2, 2010),and Google Scholar (first 100 hits). Reference lists ofreviews and retrieved full-text articles were examined forother relevant publications. We also reviewed trial registries(clinicaltrials.gov/ and www.controlled-trials.com/mrct/).The search strategy included both truncated free-text andexploded MeSH terms and was modified according to eachdatabase (Appendix A).
Study selection
Titles and abstracts were screened by one reviewer (MH).Full-text articles were retrieved for further assessment if initialscreen indicated potential eligibility. All potentially relevantarticles were reviewed independently by two reviewers (MHand PSS). Discrepancies were resolved by consensus and,when necessary, arbitrated by a third independent person(BAB for nutrition and AMC for bone-health-related topics).
Data extraction and assessment of risk of bias
Data from eligible studies were extracted by two authors(MH and PSS) independently, and discrepancies were
resolved by consensus and, when necessary, in consultationwith a third reviewer (BAB). For observational studies, tworeviewers (MH and PSS) developed a tool to assess the riskof bias, incorporating guidelines from the Agency forHealthcare Research and Quality for the field of nutrition[30–32]. The tool (Appendix B) consists of seven domainsincluding sample selection, F&V assessment, outcomeassessment, confounding factors, analytical factors, selec-tive reporting, and attrition biases. The methodologicalquality of clinical trials was assessed using the CochraneCollaboration's tool for assessing risk of bias [33] slightlymodified to reflect dietary studies [31] (Appendix B).This tool also consists of seven domains. Risk of biasassessment was performed independently by thereviewers, and any disagreement was discussed andresolved. The assignment of low, moderate, or high riskdepended on the number of domains considered not to bebiased.
Synthesis of results
After detailed review of all the studies, a systematic reviewwas performed without meta-analysis because of theheterogeneity in F&V classification (e.g., inclusion ofpotatoes or pulses as vegetables), amount of intake (e.g.,various amounts reported in servings, grams, tertiles, orquintiles), methods of assessing intake [food frequencyquestionnaire (FFQ), 24-hr dietary recalls or food records(FR)], research design (e.g., study type, inclusion criteria,type of comparison group), analyses (adjusted or unadjustedfor covariates), and reporting of outcome variables (e.g.,various BMD sites, not reporting non-significant values). Theresults of the studies, as presented in the articles, aresummarized below.
Results
Study selection and characteristics
The results of the literature search and article selectionprocess are outlined in Fig. 1. Eight studies were includedfor this systematic review. Two studies were RCTs [34, 35],three were cross-sectional studies [36–38], one was aprospective cohort study [39], one a case-control study[40], and one cohort study reported cross-sectional as wellas longitudinal data [41]. The reasons for exclusion ofstudies are also outlined in Fig. 1.
The characteristics of included studies are reported inTable 1. All women were postmenopausal. Of the eightincluded studies, six were published in the past 5 years. Theintake levels and assessment of F&V intake as well asfollow-up time varied among studies. Four studies reported
Osteoporos Int (2011) 22:1681–1693 1683

outcomes for F&V combined [34–36, 41]; all othersreported fruits separate from vegetables as well as com-bined [37–40]. Only one study reported examining theeffect of subcategories of fruits or vegetables (citrus fruits,green leafy vegetables, etc.) on bone health but no datawere shown [37]. Three studies did not describe the F&Vgroup [34, 36, 41]; among those that did, one studyincluded potatoes, tubers [37], and one included pulses[38] as vegetables. Two studies did not count the vegetablesused in mixed dishes [38, 39]. One study specificallymentioned the inclusion of nuts and fruit juices as fruits[38], whereas two studies assessed nuts and seeds as non-F&V items [39, 40].
Risk of bias
Two studies had low [34, 37], two had moderate [39, 41],and four had high risk of bias [35, 36, 38, 40] (Tables 2 and3). Six studies failed to adjust for calcium and vitamin Dintake [34–37, 39, 40]. In both cohort studies, dietaryassessment was performed only at baseline [39, 41]. Allstudies with BMD measurements used DXA except forTucker et al. [41], where dual-photon absorptiometry (DPA)
was used for baseline hip (DXA was used for final visit)and single-photon absorptiometry was used for baseline andfinal radius BMD. The hip BMD measurements werecorrected for differences between DPA and DXA.
Outcomes
Fragility fractures
One study reported data on fragility fractures. In their case-control study, Xu et al. [40] reported that meeting WorldHealth Organization (WHO) recommendations for F&Vintake (described as 370 g/day) was associated with a 74%lower odds of forearm fractures in Chinese postmenopausalwomen and that, for each quintile increase in vegetableintake, the estimated risk for fractures was reduced(Table 4). Compared with the first quintile (0–104 g/day),the odds ratio and 95% confidence interval for those in thefourth quintile (254–397 g/day) of vegetable intake was 0.17(0.07–0.46) and for those in the fifth quintile (≥398 g/day), itwas 0.11 (0.04–0.35). The association with fruit intake wasnot separately reported.
Records screened (n =781)
Records identified through database searching (n =1095)
Additional records identified through other sources (n =2)
Reference list of reviews: 2 Reference list of retrieved full-text articles: 0 Trial registries: 0
Records after duplicates removed (n =781)
Records excluded (n =738)
Irrelevant content (not directly related to bone and/or F&V): 679 Not written in English: 2 Not relevant outcome data (e.g. bone stiffness): 1 Animal studies: 30 Reviews: 16 Children, youth, women aged < 45 y: 10
Full-text articles assessed for eligibility
(n =43)
Full-text articles excluded, with reasons (n = 35) Not relevant outcome data (e.g. heel BMD) : 1 The effect of F&V could not be separated from other food groups or dietary patterns (e.g. high F&V & seafood, dairy or grain products): 17 Individual fruits or vegetables (e.g. onions, plums, tomatoes) : 4 Surrogates of F&V intake (e.g. potassium, vitamin C, serum carotenoids, net acid excretion): 12
Studies included in qualitative synthesis
(n =8)
Studies included in quantitative synthesis
(meta-analysis) (n =0)
Fig. 1 Summary of study selec-tion (PRISMA 2009 FlowDiagram [60])
1684 Osteoporos Int (2011) 22:1681–1693

Bone mineral density
Three cross-sectional analyses reported positive effects ofF&V intake on BMD, whereas one cross-sectional (whereall subjects had osteopenia), two cohort studies, and oneRCT reported no effect (Table 4).
In their cross-sectional analysis of baseline data, Tuckeret al. [41] reported a positive association between a dailyincrease of one serving of F&V and BMD at the forearm(radius) but not at the femoral neck (Table 4). It isnoteworthy to mention that, unlike hip BMD, the radiusBMD was not measured using DXA. In their longitudinalanalysis, no significant association was found between
baseline F&V intake and subsequent 4-year changes inBMD at the femoral neck or radius.
Chen et al. [37] also found a positive associationbetween a daily increase of 100 g of F&V intake andBMD at the lumbar spine and total hip. The positiverelationship between F&V intake was linear for lumbarspine BMD (trend P=0.003) but not for total hip (trend P=0.108). The authors also reported that associations betweensubcategories of fruits or vegetables and BMD were lowerthan those for total fruits or total vegetables, but these datawere not shown. Prynne et al. analyzed their data using twodifferent models (Table 4) [38]. In the main model, nosignificant associations were found. Using an alternate
Table 1 Description of observational studies and randomized control trials included in the systematic review
Reference,location
Number of women,follow up time
Age, years Dietary assessmentmethod/intake referenceperiod
Intake level Relevant outcomes
Case-control study
Xu et al. 2009[40], China
209 cases 209controls, NA
50–70 110-item FFQ/previousweek before fracture(cases) or interview(controls)
Median (IQR) g/d: F&V: cases,282 (155, 384); controls, 414 (265,667); F: cases, 86 (29, 175) andcontrols, 101 (26, 215);V: cases, 154(92, 228) and controls, 288 (179, 464)
Forearm fracture
Cross-sectional studies
Tucker et al. 1999[41]a, USA
562, NA 69–97 126-item FFQ/previousyear (baseline)
Mean ± SD servings/db: F&V, 5.30±2.65 Femoral neck and forearm(radius) BMD
Prynne et al. 2006[38], UK
73, NA 60–83 7-day FR Mean, median (IQR) g/d: F&V, 440, 394(285, 546); F, 253, 232 (143, 352);V, 187, 170 (116, 352)
Lumbar spine, total hip, andfemoral neck BMD
Chen et al. 2006[37], China–HongKong
670, NA 48–63 60-item FFQ/previous12 months
Mean ± SD; median (range) g/d: F&V,470±200; 434 (117, 1,090); F, 175±102; 160 (0, 640); V, 295±150; 259(22, 894)
Lumbar spine and total hipBMD
Ebrahimof et al.2006 [36], Iran
51, NA 45–60 Two 24-hour recalls Mean ± SD g/d: F, 456±270; V, 192±115 Lumbar spine and total hipBMDBTM: serum osteocalcinand crosslaps
Prospective cohort studies
Tucker et al. 1999[41]a, USA
399, 4 years 69–97 126-item FFQ/previousyear (baseline)
Mean ± SD servings/db: F&V, 5.3±2.7 4-year change in femoralneck and forearm (radius)BMD (baseline-year 4)
Kaptoge et al. 2003[39], UK
474, 2–5 years(mean of 3 years)
65–74 7-day FR/baseline Median (fifth, 95th percentile) g/d: F&V,258 (88, 568); F, 166 (22, 408);V, 94 (27, 218)
Hip BMD at baseline and onaverage 3 years later.Mean rate of total hipBMD loss (% per annum)
Randomized controlled trials
Macdonald et al.2008 [34],Scotland-UK
Intervention, 66;placebo, 70,2 years
55–65 4-day FR/beforerandomizationand at 1 year
Difference at year 1 from baselinemean ± SD (95% CI) g/d: Intervention:F, 291±271 (223, 359); V, 39±94(15,63); placebo: F, −17±184 (−66,32);V, −18±98 (44,8)
Lumbar spine and total hipBMD at baseline and yeartwoBTM: P1NP, CTx, andfDPD/Cr
Ebrahimof et al.2009 [35], Iran
Control, 22;intervention, 23,12 weeks
50–60(women withosteopenia)
2×24-hour recalls/atbaselineand 12 weeks
Mean ± SD servings/db: intervention: F:baseline, 2.3±1.6; final, 6.4±1.9;V: baseline, 2.7±1.5; Final, 5.7±2.4;control: F: baseline, 2.6±1.8 final,3.2±2.3; V, baseline, 2.2±1.2; final, 2.0±2.3
BTM: serum osteocalcinand CTx
NA not applicable, FFQ Food Frequency Questionnaire, IQR interquartile range, g grams, d day, F&V fruits & vegetables, F fruits, V vegetables,SD standard deviation, BMD bone mineral density, BTM bone turnover markers, FR food records, CI confidnece interval, P1NP serumprocollagen type 1 amino-terminal propeptide, CTX carboxy-terminal collagen cross-links, fDPD free deoxypyridinolinea This study analyzed data cross-sectionally as well as longitudinallyb The average weight of one F&V serving is about 80 g [52, 59]
Osteoporos Int (2011) 22:1681–1693 1685

model, similar to Tucker et al. [42], they reported asignificant increase (5.6%) in lumbar spine BMD withdoubling of fruit intake (P≤0.05).
In a study of 51 women with osteopenia (low BMD),Ebrahimof et al. reported that total hip or lumbar spineBMD were not significantly different between those whoconsumed greater or less than 400 g/day of F&V, but datawere not shown [36].
Kaptoge et al. [39] reported that baseline F&V intake(both combined and separately) had no significant effect onthe annual rate of total hip BMD loss over an average of3 years.
In an RCT, Macdonald et al. [34] assessed the effect onBMD of F&V, as well as two doses of potassium citrateagainst placebo given for 2 years. They reported nosignificant differences in mean percentage change inlumbar spine or total hip BMD between the F&V andplacebo groups (Table 4).
Bone turnover markers
Two RCTs reported that adding F&V to baseline diet hadno effect on BTM (Table 4) [34, 35]. Macdonald et al.
reported no significant differences in BMT changes frombaseline (at 3, 6, 12, 18, or 24 months) between the F&Vand placebo groups [34]. Ebrahimof et al. reported that 12servings of F&V per day lowered BTM levels in theintervention group (P value not reported) but only amongthose with significantly higher mean osteocalcin (boneformation marker) and CTx (bone resorption marker) atbaseline [35].
In an earlier cross-sectional study [36], the same researchershad reported that those with F&V intakes >400 g/day hadsignificantly lower levels of osteocalcin (Table 4). Crosslaplevels were also lower, but the difference was not statisticallysignificant.
Discussion
In this systematic review of eight studies that examined theeffect of F&V on bone health, considerable between-studyheterogeneity was identified, and four of the eight studieswere considered to have high risk of bias. Considering onlythose studies with low or moderate risk of bias, littleevidence was found to support the association of F&V and
Table 2 Assessment of risk of bias for observational studies
Reference/type of study Selection Exposureassessment
Outcomeassessment
Confoundingfactors
Analytical Selectivereporting bias
Attrition Overall riskof bias
Tucker et al. 1999 [41]/Prospective cohort Yes Yes No No Yes No No Moderate
Cross-sectional Yes No No No Yes No N/A Moderate
Kaptoge et al. 2003 [39]/Prospectivecohort
Yes Yes No Yes No Yes No Moderate
Prynne et al. 2006 [38]/Cross-sectional Yes Yes No No Yes Yes N/A High
Chen et al. 2006 [37]/Cross-sectional No No No Yes No No N/A Low
Ebrahimof et al. 2006 [36]/Cross-sectional Yes No No Yes Yes Yes N/A High
Xu et al. 2009 [40]/Case–control Yes Yes No Yes No Yes N/A High
N/A not applicable for cross-sectional and case-control studies
Low if No (risk of bias) in at least five domains, Moderate if No in three or four domains, High if No in two or less domains
Table 3 Assessment of risk of bias in clinical trials
Reference Sequencegeneration
Allocationconcealment
Blinding ofoutcomeassessors
Reportingbaseline F&Vintake
Addressingincompleteoutcome data
Selectivereportingbias
Other bias Overallrisk of bias
Macdonald et al.2008 [34]
No No No No No Yes Yes: did not provide calciumand vitamin Dsupplementation
Low
Ebrahimof et al.2009 [35]
No Unclear Unclear No Yes Yes Yes: all subjects were womenwith osteopenia, adjustedconfounders unclear
High
F&V Fruit and vegetables
Low if No (risk of bias) in at least five domains, Moderate if No in three or four domains, High if No in two or less domains
1686 Osteoporos Int (2011) 22:1681–1693

Table 4 Fruits and/or vegetables intake and bone health outcomes (fractures, BMD, or BTM)
Reference Reported outcome Adjusted confounders Associationwith fruits
Associationwith vegetables
Association with F&V
FRACTURES
Case-control study
Xu et al. 2009[40]
Decreased risk offorearm fractures forquintiles of intake orintakes >370 g/d
Final model adjustments were not specified,but considered confounders were variableswith P<0.05 in univariate analysis suchas: other food groups, height, income,family history of fracture, physical activity,smoking, energy intake; cases and controlsmatched for age and urban district
Statistics not reported Yes: for each quintileincrease Trend testOR (95% CI),0.53 (0.42–0.67)
Yes: for intakes >370 g/d OR(95% CI), 0.26 (0.14–0.48)
BONE MINERAL DENSITY
Randomized controlled trials
Macdonald et al.2008 [34]
2-year mean% change inBMD (g/cm2) for300 g/d increase inF&V
Age, weight, height, social deprivation category Not analyzed separately Not analyzedseparately
No: lumbar spinea,b: F&V, −2.1±0.3%; placebo, −1.8±0.5%; totalhipa,b: F&V, −1.5±0.3%; placebo,−1.3±0.3%
Cross-sectional studies
Tucker et al. 1999[41]
Change in BMD(g/cm2) per oneserving differencein F&V intake
Age, BMI, physical activity, smoking, alcoholuse, calcium, and vitamin D supplement use,estrogen use, season of BMD measurement,energy, and other food groups intake (milk,other dairy, bread and cereal, meat, poultry and fish)
Not analyzed separately Not analyzedseparately
Yes: forearmc, 0.0049, (SE notreported), P<0.01No: Femoral neckc, 0.0024, SE notreported), P=NS
Chen et al. 2006 [37] Change in BMD(g/cm2) per100 g difference inF &/or V intake
Age, years since menopause, height, weight,physical activity, dietary energy, protein,and calcium intake
Yes: lumbar spinec,0.0194±0.0055P<0.001
No: lumbar spinec,0.058, SE=0.037,P=.117
Yes : lumbar spinec, 0.0098±0.0029P<0.001
No: Total hipc, 0.0058±0.0046 P=0.214
No: total hipc,0.0030±0.0032P=0.369
Yes: total hipc, 0.0060±0.0025P=0.024
Yes: total hipc (withoutcalcium in the model),0.0061±0.0033P=0.074
Yes: total hipc
(without calciumin the model),0.0053±0.0023P=0.025
Yes: total hipc (without calcium in themodel), 0.0076±0.0024, P=0.004
Prynne et al. 2006[38]
% Change in BMD(g/cm2) per 100%change in F &/or Vintake (g/d)
Age, energy, calcium and vitamin K1 intake,time spent in recreational activities,smoking, supplement use, age at menopauseand HRT use
No: lumbar spine:%β=3.9, SE=2.0, P=0.06
No: statistics notreported
No: statistics not reported
Alternate model height, BMI, energy intake,time spent in recreational activities, smoking,supplement use, age at menopause and HRT use
Yes (alternate model):lumbar spine, β=5.6,SE=not reported,P≤0.05
No: total hip, %β=2.2,SE=1.9, P=NS
No: femoral neck, %β=2.5, SE=1.8, P=NS
Ebrahimof et al.2006 [36]
Mean BMD (g/cm2) in agroup with >400 g/dof F&V comparedwith a group with≤400 g/d
No adjustments Not analyzed separately Not analyzedseparately
No: statistics not reported all womenhad osteopenia
Prospective cohort studies
Kaptoge et al.2003 [39]
Difference in annualmean rates of BMDloss (% per year)among tertiles ofF&/or V intake
Weight change, stair climbing, past physicalactivity levels and activities of daily livingscore
No, statistics notreported
No, statistics notreported
No: total hipa: lowest tertile, 0.53%;middle tertile, 0.40%; upper tertile,0.39%; P=0.528
Tucker et al. 1999[41]
4-year change in BMD(g/cm2) per oneserving difference inF&Vintake
Age, BMI, physical activity, smoking, alcoholuse, calcium and, vitamin D supplementuse, estrogen use, season of BMDmeasurement, energy and other food groups(milk, other dairy, bread, and cereal, meat,poultry and fish) intake,baseline BMD
Not analyzed separately Not analyzedseparately
No: forearmc, 0.000 g/cm2, (SE notreported), P=NS
No: femoral neck c, 0.0005 g/cm2,(SE not reported), P=NS
BONE TURNOVER MARKERS
Randomized controlled trials
Macdonald et al.2008 [34]
2-year change inBTM from baselinefor 300 g/d increasein F&V
Not specified/unclear Not analyzed separately Not analyzedseparately
No: P1NPd (μg/l): F&V, −2.1±17.2;placebo, −2.3 1±8.3; P=NS
CTxd (ng/l): F&V, 0.003±0.109;placebo, 0.008±0.091; P=NS
fDPD/Crd (nmol/nmol): F&V, −0.3±2.0; placebo, −0.7±1.9; P=NS
Ebrahimof et al.2009 [35]
12-week change1 inBTM from baseline
Final model adjustments were not specified,but considered
Not analyzed separately Not analyzedseparately
No: osteocalcind (μg/l): intervention,−3.1±4.5; control, −0.41±5.5; P=0.2
Osteoporos Int (2011) 22:1681–1693 1687

bone health. Fruit and/or vegetable intakes were associatedwith higher BMD in two cross-sectional analyses but not inthe two cohort studies or one RCT. The association of F&Vintake with BMD sites varied between studies. Only oneRCT examined the association between F&V and BTM andfound no association. Among studies with high risk of bias,F&V intake as well as vegetable intake alone wasassociated with reduced incidence of forearm fractures inone case-control study. One cross-sectional study found apositive association between F&V intake and BMD; onedid not. One cross-sectional study found a negativeassociation between F&V intake and BTM, and noassociations were found in one RCT.
This is the first systematic review that specificallyassessed the effect of F&V intake as a main exposure onoutcomes of bone health. Although earlier reviews havereported protective effects of F&V on bone health [11, 15,19], these findings were based on studies that assessedpotential markers of F&V intake (e.g., high intake ofpotassium, magnesium, vitamins C or K, or low net acidexcretion) or dietary patterns that, in addition to being highin F&V, are also high in other food groups (such as dairyproducts) that are beneficial for bone. We did not includestudies that used markers of F&V intake. Although F&Varehigh in magnesium and potassium, because of the generallylow consumption of F&V in Western populations, dairyproducts are the common dietary sources of these nutrients[14, 43, 44]. We also excluded studies of dietary patternssuch as Dietary Approaches to Stop Hypertension or theMediterranean diet that are high in F&V but are alsohigh in low-fat dairy and/or whole grains, poultry, fishand nuts and lower in saturated fat, red meat, sweets,sugar-containing beverages, and sodium [45–47]. Giventhat such dietary patterns include a wide range of food
groups, it is not possible to assess the independent effectof F&V on bone health. This review excluded studies thatassessed a single fruit or vegetable such as plums oronions, or select F&V based on high amounts of a singlenutrient such as vitamin C. There were several reasons forthis decision. First, it would be difficult to identify anysingle fruit, vegetable, or nutrient as superior to others,and consumption of one item in large quantities may resultin unpleasant side effects, or omission of other healthfulfoods. Second, dietary guidelines promote consuming avariety of F&V and do not identify or recommend anysingle item to achieve public health outcomes. Finally,hypotheses based on single foods or nutrients underesti-mate the synergistic effects of foods and their numerouscomponents.
Intake levels of ≥400 g/day (five servings) of F&V(excluding potatoes and other starchy tubers) have beenadvocated by the WHO and International OsteoporosisFoundation to reduce the incidence of osteoporosis [48,49]. However, given the importance of dairy products forbone health and that augmentation of one food type in thediet may lead to the reduction of another, F&V should beadvised as part of a healthy diet that also includes at leastthree servings of dairy per day [14, 50, 51].
In this review, we identified the variable impact ofF&V intake on specific indices of bone health in womenaged ≥45 years: forearm fracture; BMD of forearmradius, femoral neck, lumbar spine, and total hip; andBTM (serum osteocalcin, N-terminal propeptide of type 1collagen, CTx, and free urinary deoxypyridinoline cross-links). Differences in association between fruit and/orvegetables (as individual groups or in combination) withvarious BMD sites may be due to different F&V intake levels,types, and usage among these populations. The definitions of
Table 4 (continued)
Reference Reported outcome Adjusted confounders Associationwith fruits
Associationwith vegetables
Association with F&V
for 400 g/d increasein F&V
Crosslapsd (μg/l): intervention, −0.05±0.17; control, 0.01±0.1; P=0.3
Cross-sectional studies
Ebrahimof et al.2006 [36]
Means of BTM in agroup with >400 g/d ofF&V compared with agroup with ≤400 g/d
No adjustments Not analyzed separately Not analyzedseparately
Yes: osteocalcind (μg/l): >400 g,18±6.5; ≤400 g, 30±13.7; P<0.05
No: crosslapsd (μg/l), >400 g; 0.65±0.27; ≤400 g, 0.74±0.41; P=NS
F&V fruit & vegetables, g grams, d day, OR odds ratio, CI confidence intervals, BMD bone mineral density, SE standard error, β regressioncoefficient, P p value, NS not significant (at P=0.05), R2 R-square, SD standard deviation, HRT hormone replacement therapy, BTM bone turnovermarkers, P1NP serum procollagen type 1 amino-terminal propeptide, CTx carboxy-terminal collagen cross-links, fDPD free deoxypyridinolinea Values are estimated from published figure where exact values were unavailablebMean±SEc Regression coefficient for F&V intake±SEdMean±SD
1688 Osteoporos Int (2011) 22:1681–1693

F&V vary considerably between studies, and the reportedintake would be affected by such differences [52, 53]. Basedon recommendations from a joint WHO and Food andAgriculture Organization workshop in 2004, the vegetablesgroup includes botanical fruits (such as tomatoes, peppers,cucumbers, and eggplants), mushrooms, and seaweed andexcludes potatoes, tubers, and dry pulses [52]. Nuts can beincluded in the fruit group, although their intake levels are,in general, very low. The common approach of excludingvegetables in mixed dishes may lead to underestimation ofintake while including potatoes and tubers may lead tooverestimation, resulting in dilution bias and reduced abilityto detect associations. Some suggest that positive findings ofcross-sectional studies reflect measurements that are morerepresentative of long-term dietary patterns and accumulatedbone status while longitudinal changes in BMD are time-dependent (change from baseline) and represent the effect ofrecent diet on bone status [34, 41]. Under this assumption, itmay be that long-term (particularly premenopausal) F&Vintake is beneficial to bones and that the deleterious effectsof hormonal changes outweigh the beneficial effects of F&Vin later years.
Possible limitations of this review include the heteroge-neity of included studies and the presence of low risk ofbias in only two of eight studies. Additionally, in allobservational studies, high F&V intake may be a surrogatemeasure of multiple healthy lifestyle characteristics that arebeneficial for bones. Studies have reported that high F&Vintakes are associated with dietary supplement intake,physical activity, moderate alcohol intake, and not smoking[37, 54–56]; however, most included studies adjusted for atleast some of these confounding variables. Finally, dietarymeasurements in the two cohort studies [39, 41] were onlyperformed at baseline; therefore, changes in BMD frombaseline were not linked to dietary changes over the term ofthe studies (3–5 years).
Based on the paucity of studies identified, furtherresearch is needed to explore the effects of F&V, as themain intervention, on bone health while controlling forconsumption of other foods, nutrients, and confoundinglifestyle characteristics, and to compare the independenteffects in premenopausal and postmenopausal women.Furthermore, dietary interventions can identify theeffective amount of F&V (total, as well as subcatego-ries) for bone health and support development ofclinical and public health practice guidelines forosteoporosis prevention and management. Future cohortstudies would be strengthened by measuring dietaryintake at baseline as well as final visit, to account forchanges over time. There is a need for researchers toassess dietary intake using comparable and standardized
methods across populations. A WHO report providesuseful guidelines for the assessment of F&V intake [52].To improve the utility of future publications and outcomereporting, the CONSORT [57] and STROBE [58] state-ments should also be used. Complying with these guide-lines will result in more comparable literature, facilitatefuture systematic reviews and meta-analyses, and ulti-mately lead to the development of evidence-based dietaryrecommendations.
Based on our review, it remains unclear whether F&Vintake in postmenopausal women can prevent osteoporoticfractures, improve BMD, or slow the rate of bone loss asfew studies were found that examined this, and inadequatereporting of study characteristics, compliance, attrition,effect estimates, and confounding factors made interpreta-tion of results and assessment of potential biases difficult.Given that cross-sectional studies, although limited, suggestpositive results, there is a particular need for long-termF&V intervention trials or cohort studies to confirm thesefindings.
Acknowledgments We sincerely thank Ms. Elizabeth Uleryk forher assistance in developing and executing the search strategy aswell as Dr. Kyarash Safakish (MD) for his review of excludedcitations based on titles and abstracts to ensure all citations met theexclusion criteria.
Contributions MH was involved in project conception, develop-ment of review protocol, and study oversight and wrote the initialdraft. BAB, PSS, and AMC, respectively, were all involved in thedesign and execution of the review and made substantial revisionsto the manuscript. AMC provided advice and interpreted findingson bone health, BAB on nutrition, and PSS, JB, and AMC onconducting systematic reviews and meta-analysis. MH and PSSreviewed the selected full-text articles and determined the risk ofbias independently. BAB reviewed the selected articles andextracted data to ensure information was complete. The risk ofbias tool was designed by PSS and modified by MH for studies inthe field of nutrition and bone health. All authors commented onand approved the final manuscript. AMC has primary responsibilityfor final content.
Conflicts of interest None.
Appendix A: search strategy
MEDLINE
exp “Bone and Bones”/or bone mineral density.mp. or(bone mineral density) .ti,ab. or exp Bone Density/or boneremodeling/or bone regeneration/or bone resorption/or(Biological Markers/and “Bone and Bones”/) or exp
Osteoporos Int (2011) 22:1681–1693 1689
Osteoporosis, Postmenopausal/or exp Osteoporosis/or expFractures, Bone/or (bone adj2 turnover).ti,ab. or (bone adj2marker*).ti,ab. or (bone adj2 biomarker*).ti,ab. or (boneadj2 formation).ti,ab.
exp fruit/or exp vegetables/or (Fruit* and Vegetable*).mp.or fruit*.mp. or vegetable*.mp. or (fruit* adj2 vegetable*).ti,ab.
(clinical trial, all or clinical trial, phase I or clinical trial,phase II or clinical trial, phase III or clinical trial, phase IVor clinical trial or controlled clinical trial or meta-analysisor multicenter study or randomized controlled trial).pt. orexp Clinical Trials as Topic/or exp cross-sectionalstudies/or exp clinical trial/or exp clinical trials astopic/or exp clinical trials, phase I as topic/or exp clinicaltrials, phase II as topic/or exp clinical trials, phase III astopic/or exp clinical trials, phase IV as topic/or expcontrolled clinical trials as topic/or exp randomizedcontrolled trials as topic/or exp multicenter studies astopic/or exp intervention studies/or exp twin studies astopic/or epidemiologic studies/or exp study characteristics/orexp epidemiologic study characteristics as topic/or expepidemiologic research design/or exp case-control studies/orexp retrospective studies/or exp cohort studies/or exp longi-tudinal studies/or exp follow-up studies/or exp prospectivestudies/or observational study.mp.
EMBASE
1. exp bone/or exp bone demineralization/or exp bonemineralization/or exp bone density/or exp fracture/orexp bone fragility/or exp osteoporosis/or exp fragilityfracture/or exp bone mass/or bone metabolism/or expbone mineral/or exp bone remodeling/or exp boneregeneration/or exp bone turnover/or exp osteoporosis/or exp postmenopause osteoporosis/or exp primaryosteoporosis/or exp secondary osteoporosis/or exp boneregeneration/or exp bone remodeling/or exp bonedensity/or exp bone turnover/or exp bone/or expossification/or (bone adj2 turnover).ti,ab. or (boneadj2 marker*).ti,ab. or (bone adj2 biomarker*).ti,ab.or (bone adj2 formation).ti,ab.
2. fruit/or vegetable/or (fruit* and vegetable*).mp. orfruit*.mp. or vegetable*.mp. or (fruit* adj2 vegetable*).ti,ab.
3. exp clinical study/or exp intervention study/or explongitudinal study/or exp prospective study/or expretrospective study/or exp case control study/or exphospital based case control study/or exp populationbased case control study/or exp clinical trial/or expmulticenter study/or exp phase 1 clinical trial/or expphase 2 clinical trial/or exp phase 3 clinical trial/orexp phase 4 clinical trial/or exp controlled clinical
trial/or exp randomized controlled trial/or ct.fs. orclinical trial/or phase 1 clinical trial/or phase 2clinical trial/or phase 3 clinical trial/or phase 4clinical trial/or controlled clinical trial/or randomizedcontrolled trial/or multicenter study/or meta analysis/or (random: or (doubl: adj2 dummy) or ((Singl: ordouble: or trebl:) adj25 (blind: or mask:)) or RCT orRCTs or (control: adj25 trial:) or multicent: orplacebo: or metaanalysis: or (meta adj5 analys:) orobservational stud:).ti,ab.
4. 1 and 3 and 2
CAB
1. exp fruit/or fruits/or exp vegetables/or fruit*.mp. orvegetable*.mp. or (fruit* and vegetable*).mp. or (fruit*adj2 vegetable*).ti,ab.
2. clinical trials/or (random: or (doubl: adj2 dummy)or ((Singl: or double: or trebl:) adj25 (blind: ormask:)) or RCT or RCTs or (control: adj25 trial:) ormulticent: or placebo: or metaanalysis: or (metaadj5 analys:) or sham or effectiveness or efficacy orcompar:).ti,ab. or exp trials/or exp randomizedcontrolled trials/or exp clinical trials/or exp trials/or exp randomized controlled trials/or exp epidemi-ological surveys/or (observational study or case–control study or cohort sutdy or cross-sectionalstudy).mp.
3. osteoporosis/or osteoporosis, postmenopausal/or expbone formation/or exp bone resorption/or exp bones/or exp bone mineralization/or exp bone density/orexp bone fractures/or exp demineralization/or (boneadj2 turnover).ti,ab. or (bone adj2 marker*).ti,ab. or(bone adj2 biomarker*).ti,ab. or (bone adj2 forma-tion).ti,ab.
4. 1 and 3 and 2
PUBMED
(“Bone Density”[Mesh] OR (“Biological Markers”[Mesh] AND “Bone and Bones”[Mesh]) OR “BoneRemodeling”[Mesh] OR “Bone Resorption”[Mesh] OR“bone formation”[All Fields] OR “Bone turnover”[AllFields] OR “bone metabolism”[All Fields] OR “bone andbones”[MeSH Terms] OR “Fractures, Bone”[Mesh] OR“Osteoporosis”[Mesh] OR “Osteoporosis, Postmenopausal”[Mesh]) AND (“fruit”[MeSH Terms] OR “vegetables”[MeSHTerms] OR “fruit”[All Fields] OR “fruits”[All Fields] OR“vegetables”[All Fields] OR “vegetable”[All Fields]) AND(“Epidemiologic Methods”[Mesh] OR “Epidemiologic StudyCharacteristics as Topic”[Mesh] OR “Clinical Trials asTopic”[Mesh])
1690 Osteoporos Int (2011) 22:1681–1693
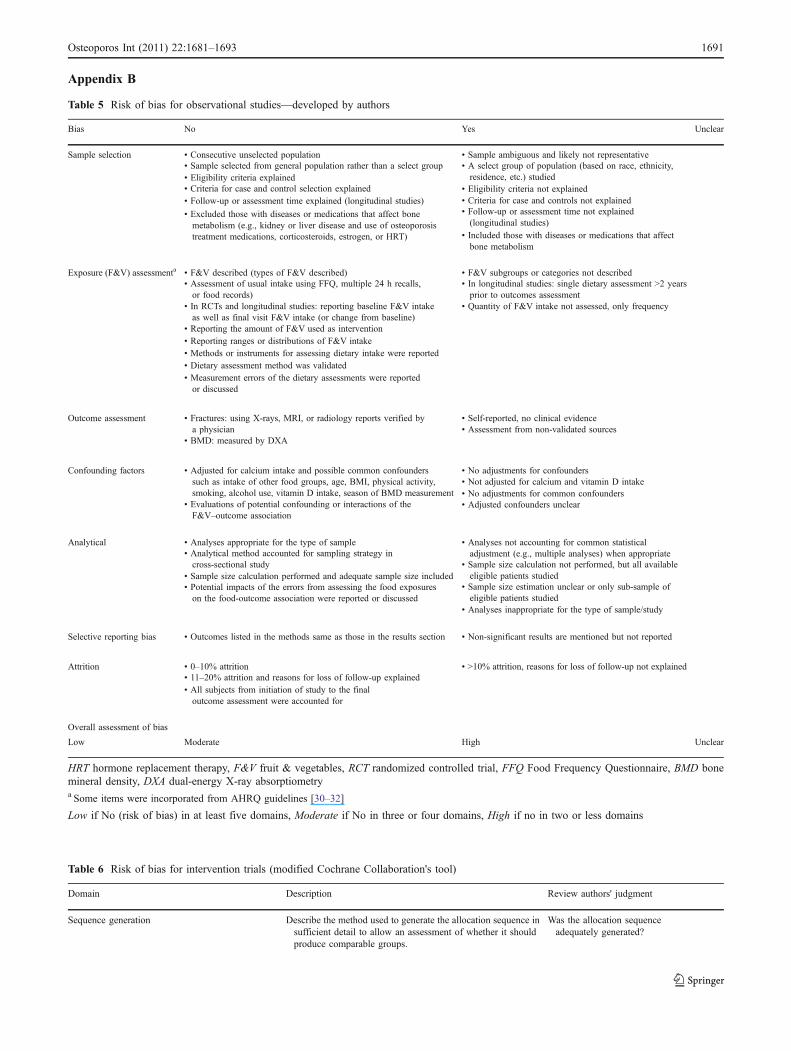
Table 5 Risk of bias for observational studies—developed by authors
Bias No Yes Unclear
Sample selection • Consecutive unselected population • Sample ambiguous and likely not representative• Sample selected from general population rather than a select group • A select group of population (based on race, ethnicity,
residence, etc.) studied• Eligibility criteria explained• Eligibility criteria not explained• Criteria for case and control selection explained• Criteria for case and controls not explained• Follow-up or assessment time explained (longitudinal studies)• Follow-up or assessment time not explained(longitudinal studies)
• Excluded those with diseases or medications that affect bonemetabolism (e.g., kidney or liver disease and use of osteoporosistreatment medications, corticosteroids, estrogen, or HRT) • Included those with diseases or medications that affect
bone metabolism
Exposure (F&V) assessmenta • F&V described (types of F&V described) • F&V subgroups or categories not described• Assessment of usual intake using FFQ, multiple 24 h recalls,or food records)
• In longitudinal studies: single dietary assessment >2 yearsprior to outcomes assessment
• In RCTs and longitudinal studies: reporting baseline F&V intakeas well as final visit F&V intake (or change from baseline)
• Quantity of F&V intake not assessed, only frequency
• Reporting the amount of F&V used as intervention• Reporting ranges or distributions of F&V intake• Methods or instruments for assessing dietary intake were reported• Dietary assessment method was validated• Measurement errors of the dietary assessments were reportedor discussed
Outcome assessment • Fractures: using X-rays, MRI, or radiology reports verified bya physician
• Self-reported, no clinical evidence
• BMD: measured by DXA• Assessment from non-validated sources
Confounding factors • Adjusted for calcium intake and possible common confounderssuch as intake of other food groups, age, BMI, physical activity,smoking, alcohol use, vitamin D intake, season of BMD measurement
• No adjustments for confounders
• Evaluations of potential confounding or interactions of theF&V–outcome association
• Not adjusted for calcium and vitamin D intake• No adjustments for common confounders• Adjusted confounders unclear
Analytical • Analyses appropriate for the type of sample • Analyses not accounting for common statisticaladjustment (e.g., multiple analyses) when appropriate• Analytical method accounted for sampling strategy in
cross-sectional study • Sample size calculation not performed, but all availableeligible patients studied• Sample size calculation performed and adequate sample size included
• Sample size estimation unclear or only sub-sample ofeligible patients studied
• Potential impacts of the errors from assessing the food exposureson the food-outcome association were reported or discussed
• Analyses inappropriate for the type of sample/study
Selective reporting bias • Outcomes listed in the methods same as those in the results section • Non-significant results are mentioned but not reported
Attrition • 0–10% attrition • >10% attrition, reasons for loss of follow-up not explained• 11–20% attrition and reasons for loss of follow-up explained• All subjects from initiation of study to the finaloutcome assessment were accounted for
Overall assessment of bias
Low Moderate High Unclear
HRT hormone replacement therapy, F&V fruit & vegetables, RCT randomized controlled trial, FFQ Food Frequency Questionnaire, BMD bonemineral density, DXA dual-energy X-ray absorptiometrya Some items were incorporated from AHRQ guidelines [30–32]
Low if No (risk of bias) in at least five domains, Moderate if No in three or four domains, High if no in two or less domains
Appendix B
Table 6 Risk of bias for intervention trials (modified Cochrane Collaboration's tool)
Domain Description Review authors' judgment
Sequence generation Describe the method used to generate the allocation sequence insufficient detail to allow an assessment of whether it shouldproduce comparable groups.
Was the allocation sequenceadequately generated?
Osteoporos Int (2011) 22:1681–1693 1691

References
1. Johnell O, Kanis JA (2004) An estimate of the worldwideprevalence, mortality and disability associated with hip fracture.Osteoporos Int 15:897–902
2. National Osteoporosis Foundation (2010) Osteoporosis prevalence:gender. National Osteoporosis Foundation. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm. Accessed on: Septem-ber 2010
3. Delaney MF (2006) Strategies for the prevention and treatment ofosteoporosis during early postmenopause. Am J Obstet Gynecol194:S12–S23
4. Kanis JA, Delmas P, Burckhardt P, Cooper C, Torgerson D (1997)Guidelines for diagnosis and management of osteoporosis. TheEuropean Foundation for Osteoporosis and Bone Disease. Osteo-poros Int 7:390–406
5. McCombs JS, Thiebaud P, Laughlin-Miley C, Shi J (2004)Compliance with drug therapies for the treatment and preventionof osteoporosis. Maturitas 48:271–287
6. Weycker D, Macarios D, Edelsberg J, Oster G (2006) Compliancewith drug therapy for postmenopausal osteoporosis. Osteoporos Int17:1645–1652
7. Imaz I, Zegarra P, Gonzalez-Enriquez J, Rubio B, Alcazar R,Amate JM (2010) Poor bisphosphonate adherence for treatment ofosteoporosis increases fracture risk: systematic review and meta-analysis. Osteoporos Int 11:1943–1951
8. Tosteson AN, Grove MR, Hammond CS, Moncur MM, Ray GT,Hebert GM, Pressman AR, Ettinger B (2003) Early discontinuationof treatment for osteoporosis. Am J Med 115:209–216
9. Trzeciakiewicz A, Habauzit V, Horcajada MN (2009) Whennutrition interacts with osteoblast function: molecular mechanismsof polyphenols. Nutr Res Rev 22:68–81
10. Mundy GR (2006) Nutritional modulators of bone remodelingduring aging. Am J Clin Nutr 83:427S–430S
11. Tucker KL (2009) Osteoporosis prevention and nutrition. CurrOsteoporos Rep 7:111–117
12. Morgan KT (2008) Nutritional determinants of bone health. J NutrElder 27:3–27
13. Cashman KD (2007) Diet, nutrition, and bone health. J Nutr137:2507S–2512S
14. Heaney RP (2009) Dairy and bone health. J Am Coll Nutr 28(Suppl 1):82S–90S
15. Kitchin B, Morgan SL (2007) Not just calcium and vitamin D:other nutritional considerations in osteoporosis. Curr RheumatolRep 9:85–92
16. Lister CE, Skinner MA, Hunter DC (2007) Fruits, vegetables andtheir phytochemicals for bone and joint health. Curr TopNutraceutical Res 5:67–82
17. Macdonald HM (2007) Influence of organic salts of potassium onbone health: possible mechanisms of action for the role of fruitand vegetables. Int Congr Ser 1297:268–281
18. Lanham-New SA (2006) Fruit and vegetables: the unexpectednatural answer to the question of osteoporosis prevention? Am JClin Nutr 83:1254–1255
19. New SA (2003) Intake of fruit and vegetables: implications forbone health. Proc Nutr Soc 62:889–899
20. Buclin T, Cosma M, Appenzeller M, Jacquet AF, DecosterdLA, Biollaz J, Burckhardt P (2001) Diet acids and alkalisinfluence calcium retention in bone. Osteoporos Int 12:493–499
21. Arnett TR (2008) Extracellular pH regulates bone cell function. JNutr 138:415S–418S
22. Brandao-Burch A, Utting JC, Orriss IR, Arnett TR (2005)Acidosis inhibits bone formation by osteoblasts in vitro bypreventing mineralization. Calcif Tissue Int 77:167–174
Table 6 (continued)
Domain Description Review authors' judgment
Allocation concealment Describe the method used to conceal the allocation sequence insufficient detail to determine whether intervention allocationscould have been foreseen in advance of, or during, enrolment
Was allocation adequatelyconcealed?
Blinding of participants, personnel and outcomeassessors Assessments should be made for eachmain outcome (or class of outcomes)
Describe all measures used, if any, to blind study participantsand personnel from knowledge of which intervention aparticipant received. Provide any information relating towhether the intended blinding was effective
Was knowledge of the allocatedintervention adequatelyprevented during the study?
Reporting baseline dietary exposure Reporting the baseline dietary intake using validated dietaryassessment tools
Were the baseline intakes ofdietary exposures reported?
Incomplete outcome data assessments should bemade for each main outcome(or class of outcomes)
Describe the completeness of outcome data for each mainoutcome, including attrition and exclusions from the analysis.State whether attrition and exclusions were reported, thenumbers in each intervention group (compared with totalrandomized participants), reasons for attrition/exclusionswhere reported, and any re-inclusions in analyses performedby the review authors
Were incomplete outcome dataadequately addressed?
Selective outcome reporting State how the possibility of selective outcome reporting wasexamined by the review authors, and what was found
Are reports of the study free ofselective outcome reporting?
Other sources of bias State any important concerns about bias not addressed in theother domains in the tool
Was the study apparently free ofother problems that could put itat a high risk of bias?
Overall assessment of bias
Low Moderate High Unclear
The Cochrane Collaboration's tool for assessing risk of bias (http://www.cochrane-handbook.org/), with the addition of “Reporting of BaselineF&V Intake” domain
Low if No (risk of bias) in at least five domains, Moderate if No in three or four domains, High if No in two or less domains
1692 Osteoporos Int (2011) 22:1681–1693

23. Hunter DC, Skinner MA, Lister CE (2008) Impact of phytochem-icals on maintaining bone and joint health. Nutrition 24:390–392
24. Brown JP, Josse RG (2002) 2002 clinical practice guidelines forthe diagnosis and management of osteoporosis in Canada. CMAJ167:S1–S34
25. Cummings SR, Bates D, Black DM (2002) Clinical use of bonedensitometry: scientific review. Rev Lat Am Enferm 288:1889–1897
26. ISCD The International Society for Clinical Densitometry (ISCD).The 2007 Official Position of ISCD: Indications for Bone MineralDensity (BMD) testing. The International Society for ClinicalDensitometry (ISCD)Website. Available at: http://www.iscd.org/visitors/positions/OfficialPositionsText.cfm. Accessed on: September 2010
27. Nikander R, Sievanen H, Heinonen A, Daly RM, Uusi-Rasi K,Kannus P (2010) Targeted exercise against osteoporosis: asystematic review and meta-analysis for optimising bone strengththroughout life. BMC Med 8:47
28. Civitelli R, Rmamento-Villareal R, Napoli N (2009) Boneturnover markers: understanding their value in clinical trials andclinical practice. Osteoporos Int 20:843–851
29. Eastell R, Hannon RA (2008) Biomarkers of bone health andosteoporosis risk. Proc Nutr Soc 67:157–162
30. Balk EM, Horsley TA, Newberry SJ, Lichtenstein AH, Yetley EA,Schachter HM, Moher D, MacLean CH, Lau J (2007) Acollaborative effort to apply the evidence-based review processto the field of nutrition: challenges, benefits, and lessons learned.Am J Clin Nutr 85:1448–1456
31. Chung M, Balk EM, Ip S, Raman G, Yu WW, Trikalinos TA,Lichtenstein AH, Yetley EA, Lau J (2009) Reporting of systematicreviews of micronutrients and health: a critical appraisal. Am JClin Nutr 89:1099–1113
32. Lichtenstein AH, Yetley EA, Lau J (2008) Application ofsystematic review methodology to the field of nutrition. J Nutr138:2297–2306
33. The Cochrane Collaboration (2009) Cochrane handbook forsystematic reviews of interventions-version 5.0.2. The CochraneCollaboration. Available at: http://www.cochrane-handbook.org/.Accessed on: September 2010
34. Macdonald HM, Black AJ, Aucott L, Duthie G, Duthie S,Sandison R, Hardcastle AC, Lanham New SA, Fraser WD, ReidDM (2008) Effect of potassium citrate supplementation orincreased fruit and vegetable intake on bone metabolism inhealthy postmenopausal women: a randomized controlled trial.Am J Clin Nutr 88:465–474
35. Ebrahimof S, Hoshiarrad A, Hossein-Nezhad A, Larijani B, KimiagarSM (2009) Effects of increasing fruit and vegetable intake on boneturnover in postmenopausal osteopenic women. Daru 17:30–37
36. Ebrahimof S, Hoshyarrad A, Hossein-Nezhad A, Zandi N,Larijani B, Kimiagar M (2006) Fruit and vegetable intake inpostmenopausal women with osteopenia. Arya J 1:183–187
37. Chen YM, Ho SC, Woo JL (2006) Greater fruit and vegetable intakeis associated with increased bone mass among postmenopausalChinese women. Br J Nutr 96:745–751
38. Prynne CJ, Mishra GD, O’Connell MA, Muniz G, Laskey MA,Yan L, Prentice A, Ginty F (2006) Fruit and vegetable intakes andbone mineral status: a cross sectional study in 5 age and sexcohorts. Am J Clin Nutr 83:1420–1428
39. Kaptoge S (2003) Effects of dietary nutrients and food groups onbone loss from the proximal femur in men and women in the 7thand 8th decades of age. Osteoporos Int 14:5–428
40. Xu L, Dibley M, D’Este C, Phillips M, Porteous J, Attia J (2009)Food groups and risk of forearm fractures in postmenopausalwomen in Chengdu, China. Climacteric 2:222–229
41. Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PW, KielDP (1999) Potassium, magnesium, and fruit and vegetable intakesare associated with greater bone mineral density in elderly menand women. Am J Clin Nutr 69:727–736
42. Tucker KL, Chen H, Hannan MT, Cupples LA, Wilson PW,Felson D, Kiel DP (2002) Bone mineral density and dietarypatterns in older adults: the Framingham Osteoporosis Study. AmJ Clin Nutr 76:245–252
43. Tucker KL (2003) Dietary intake and bone status with aging. CurrPharm Des 9:2687–2704
44. Weaver CM (2009) Should dairy be recommended as part of ahealthy vegetarian diet? Point. Am J Clin Nutr 89:1634S–1637S
45. Lin PH, Aickin M, Champagne C, Craddick S, Sacks FM,McCarron P, Most-Windhauser MM, Rukenbrod F, Haworth L(2003) Food group sources of nutrients in the dietary patterns ofthe DASH-Sodium Trial. J Am Diet Assoc 103:488–496
46. Kontogianni MD, Melistas L, Yannakoulia M, Malagaris I,Panagiotakos DB, Yiannakouris N (2009) Association betweendietary patterns and indices of bone mass in a sample ofMediterranean women. Nutrition 25:165–171
47. Mendoza Ladron De Guevara N, Santalla A, Moron F, AstorquinaTM, Gonzalez A, Quereda F, Criado MSL, Vazquez F, Borrego RS,Ruiz A (2008) Epidemiological characteristics of a population ofpostmenopausal women with osteopenia and osteoporosis: impor-tance of the Mediterranean diet. Prog Obstet Ginecol 51:265–270
48. World Health Organization (2003) Diet, nutrition and theprevention of chronic diseases-recommendations for preventingosteoporosis-disease-specific recommendations. World HealthOrganization. Available at: http://www.fao.org/DOCREP/005/AC911E/ac911e07.htm#bm07.7. Accessed on: September 2010
49. International Osteoporosis Foundation (2009) Facts and statisticsabout osteoporosis and its impact-nutrition. International OsteoporosisFoundation. Available at: http://www.iofbonehealth.org/facts-and-statistics.html#factsheet-category-21. Accessed on: September 2010
50. Fulgoni VL III, Huth PJ, DiRienzo DB, Miller GD (2004) Determina-tion of the optimal number of dairy servings to ensure a low prevalenceof inadequate calcium intake inAmericans. J AmColl Nutr 23:651–659
51. Nicklas TA, O’Neil CE, Fulgoni VL III (2009) The role of dairyin meeting the recommendations for shortfall nutrients in theAmerican diet. J Am Coll Nutr 28(Suppl 1):73S–81S
52. Agudo A (2004) Measuring intake of fruit and vegetables. WorldHealth Organization (WHO). Available at: http://www.who.int/dietphysicalactivity/fruit/en/. Accessed on: September 2010
53. Pomerleau J, Lock K, McKee M, Altmann DR (2004) The challengeof measuring global fruit and vegetable intake. J Nutr 134:1175–1180
54. Reedy J, Haines PS, Campbell MK (2005) Differences in fruit andvegetable intake among categories of dietary supplement users. JAm Diet Assoc 105:1749–1756
55. Trudeau E, Kristal AR, Li S, Patterson RE (1998) Demographic andpsychosocial predictors of fruit and vegetable intakes differ: implica-tions for dietary interventions. J Am Diet Assoc 98:1412–1417
56. Hung HC, Joshipura KJ, Jiang R, Hu FB, Hunter D, Smith-Warner SA, Colditz GA, Rosner B, Spiegelman D, Willett WC(2004) Fruit and vegetable intake and risk of major chronicdisease. J Natl Cancer Inst 96:1577–1584
57. Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, ElbourneD, Gotzsche PC, Lang T (2001) The revised CONSORT statementfor reporting randomized trials: explanation and elaboration. AnnIntern Med 134:663–694
58. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC,Vandenbroucke JP (2007) The Strengthening the Reporting ofObservational Studies in Epidemiology (STROBE) statement:guidelines for reporting observational studies. Lancet 370:1453–1457
59. He FJ, Nowson CA, MacGregor GA (2006) Fruit and vegetableconsumption and stroke: meta-analysis of cohort studies. Lancet367:320–326
60. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group(2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151:264–269
Osteoporos Int (2011) 22:1681–1693 1693
Related Documents











