Aiz J Cli,z Nuir l995;6l: 1037-42. Printed in USA. © 1995 American Society for Clinical Nutrition I037 Feeding premature newborn infants palmitic acid in amounts and stereoisomeric position similar to that of human milk: effects on fat and mineral balance13 Virgilio P Carnielli, Iiigrid HT Luijendijk, Johannes B van Boerlage, Herman J Degenhart, and Pieter JJ Sauer ABSTRACT The effect of the structure of human milk triglycerides on intestinal fat absorption remains controversial. Twelve infants were each fed, for 1 wk in a crossover design, two formulas that differed only in triglyceride configuration. The “a” formula contained triglycerides similar to those in human milk (26% palmitic acid, esterified predominantly to the sn-2 position) whereas in the “a” formula, which contained triglycerides similar to those in formulas currently marketed, palmitate was mainly at the sn-l,3 positions. Fatty acid, fat, and mineral balances were measured at the end of each 1-wk period. Myristic, palmitic, and stearic acids were absorbed better from the 3 formula, but total fat excretion was not reduced. During the feeding of /3 formula fecal calcium excre- tion was lower, urinary calcium higher, and urinary phosphate lower. A formula containing triglycerides similar to those in human milk has significant effects on fatty acid intestinal absorption and improves mineral balance in comparison with a conventional formula. Am J Clin Nutr 1995;61:l037-42. KEY WORDS Formula study, synthesized triglycerides, triglyceride structure, infant formula, palmitic acid, fatty acids, fat absorption, premature infants, calcium absorption, mineral balance Introduction Fat is the major source of energy in human milk (1) and in most infant formulas. Whereas in human adults fat absorption is almost complete, newborns and especially premature neo- nates exhibit impaired absorption during the first weeks of life (2-5). This is believed to be caused mainly by low intraduo- denal concentrations of pancreatic lipase (6, 7) and bile salts (8-10). In addition, the absorption of fat from infant formulas is reported to be lower than from human milk (4, 1 1-13). This difference has been explained by the presence of lipases in human milk (14, 15) and by the unique stereoisomeric structure of human milk triglycerides (1, 16) that favor their digestion and absorption. In human milk triglycerides, palmitic acid accounts for 20-25% of total milk fatty acids and it is esterified mainly to the center sn-2 position of the triglyceride glycerol (f3 position) (1, 16). In contrast, in cow milk fat or in vegetable oils, it is predominantly esterified to the sn-i and sn-3 positions (a positions) (16). Because the acyl chain at the Goudoever, Eric J Sulkers, Anneke A 13 position is relatively resistant to the lipolytic action of pancreatic lipase, the fatty acids (FAs) in the 3 position remain intact as monoglycerides during digestion and absorption. Therefore, in the presence of sufficient pancreatic lipase activ- ity, free FAs and 2-monoacylglycerol are the final products of triglyceride digestion ( i 7). 2-Monoglyceride is well-absorbed because it readily forms mixed micellae with bile acids and cannot form insoluble soaps with divalent cations such as calcium and magnesium. Saturated fatty acids, which are not well-absorbed as free FAs, are probably better absorbed as monoglyceride. The absorption of palmitic acid, therefore, could be greater from fat when it is esterified at the sn-2 position than when it is esterified predominantly at the sn-1,3 positions. This could also be advantageous in high-calcium- containing diets (eg, infant formulas) by avoiding calcium soap formation and improving intestinal absorption of calcium. Al- though early studies by Tomarelli et al (18) in rats and by Filer et al (19) in term newborn infants indicated better absorption of palmitic acid when esterified to the sn-2 position of the diet fat, more recent studies in premature infants have failed to dem- onstrate similar benefits (20, 21). Differences in the fatty acid composition of the formulas, apart from their palmitic acid content, and differences in the patient populations may explain the lack of effect. We studied whether palmitic acid in the f3 position of dietary triglycerides and in amounts similar to those found in breast milk improves fat, FAs, and calcium absorption in preterm infants. We did this using synthetic triglycerides that differed only in the isomeric position of palmitic acid. Patients and methods Formulas, subjects, and clinical design The two infant formulas used in this study had a similar composition and fatty acid profile, but different isomeric po- I From the Department of Pediatrics, Sophia Children’s Hospital and University Hospital/Erasmus University Rotterdam, Rotterdam, Nether- lands. 2 Supported by grants from Nutricia, Zoetermeer, Netherlands. 3 Reprints not available. Address correspondence to VP Carnielli, Sophia Children’s Hospital, Room Sp 3456, Dr Molewaterplein 60, 3015 GJ, Rotterdam, Netherlands. Received December 22, 1993. Accepted for publication October 31, 1994. by guest on October 11, 2015 ajcn.nutrition.org Downloaded from

Feeding Premature Newborn Infants
Dec 06, 2015
Feeding premature newborn infants
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ai�z J Cli,z Nuir l995;6l: 1037-42. Printed in USA. © 1995 American Society for Clinical Nutrition I037
Feeding premature newborn infants palmitic acid inamounts and stereoisomeric position similar to that ofhuman milk: effects on fat and mineral balance13
Virgilio P Carnielli, Iiigrid HT Luijendijk, Johannes B van
Boerlage, Herman J Degenhart, and Pieter JJ Sauer
ABSTRACT The effect of the structure of human milk
triglycerides on intestinal fat absorption remains controversial.
Twelve infants were each fed, for 1 wk in a crossover design,two formulas that differed only in triglyceride configuration.
The “a” formula contained triglycerides similar to those in
human milk (26% palmitic acid, esterified predominantly to the
sn-2 position) whereas in the “a” formula, which contained
triglycerides similar to those in formulas currently marketed,
palmitate was mainly at the sn-l,3 positions. Fatty acid, fat, and
mineral balances were measured at the end of each 1-wk
period. Myristic, palmitic, and stearic acids were absorbed
better from the 3 formula, but total fat excretion was not
reduced. During the feeding of /3 formula fecal calcium excre-
tion was lower, urinary calcium higher, and urinary phosphatelower. A formula containing triglycerides similar to those in
human milk has significant effects on fatty acid intestinal
absorption and improves mineral balance in comparison with a
conventional formula. Am J Clin Nutr 1995;61:l037-42.
KEY WORDS Formula study, synthesized triglycerides,
triglyceride structure, infant formula, palmitic acid, fatty acids,
fat absorption, premature infants, calcium absorption, mineral
balance
Introduction
Fat is the major source of energy in human milk (1) and inmost infant formulas. Whereas in human adults fat absorption
is almost complete, newborns and especially premature neo-
nates exhibit impaired absorption during the first weeks of life
(2-5). This is believed to be caused mainly by low intraduo-
denal concentrations of pancreatic lipase (6, 7) and bile salts
(8-10). In addition, the absorption of fat from infant formulas
is reported to be lower than from human milk (4, 1 1-13). This
difference has been explained by the presence of lipases in
human milk (14, 15) and by the unique stereoisomeric structure
of human milk triglycerides (1, 16) that favor their digestion
and absorption. In human milk triglycerides, palmitic acidaccounts for 20-25% of total milk fatty acids and it is
esterified mainly to the center sn-2 position of the triglyceride
glycerol (f3 position) (1, 16). In contrast, in cow milk fat or in
vegetable oils, it is predominantly esterified to the sn-i and
sn-3 positions (a positions) (16). Because the acyl chain at the
Goudoever, Eric J Sulkers, Anneke A
13 position is relatively resistant to the lipolytic action ofpancreatic lipase, the fatty acids (FAs) in the �3 position remain
intact as monoglycerides during digestion and absorption.
Therefore, in the presence of sufficient pancreatic lipase activ-
ity, free FAs and 2-monoacylglycerol are the final products of
triglyceride digestion ( i 7). 2-Monoglyceride is well-absorbed
because it readily forms mixed micellae with bile acids and
cannot form insoluble soaps with divalent cations such as
calcium and magnesium. Saturated fatty acids, which are not
well-absorbed as free FAs, are probably better absorbed asmonoglyceride. The absorption of palmitic acid, therefore,
could be greater from fat when it is esterified at the sn-2
position than when it is esterified predominantly at the sn-1,3
positions. This could also be advantageous in high-calcium-
containing diets (eg, infant formulas) by avoiding calcium soap
formation and improving intestinal absorption of calcium. Al-
though early studies by Tomarelli et al (18) in rats and by Filer
et al (19) in term newborn infants indicated better absorption of
palmitic acid when esterified to the sn-2 position of the diet fat,
more recent studies in premature infants have failed to dem-
onstrate similar benefits (20, 21). Differences in the fatty acid
composition of the formulas, apart from their palmitic acid
content, and differences in the patient populations may explain
the lack of effect. We studied whether palmitic acid in the f3position of dietary triglycerides and in amounts similar to those
found in breast milk improves fat, FAs, and calcium absorption
in preterm infants. We did this using synthetic triglycerides that
differed only in the isomeric position of palmitic acid.
Patients and methods
Formulas, subjects, and clinical design
The two infant formulas used in this study had a similar
composition and fatty acid profile, but different isomeric po-
I From the Department of Pediatrics, Sophia Children’s Hospital and
University Hospital/Erasmus University Rotterdam, Rotterdam, Nether-
lands.
2 Supported by grants from Nutricia, Zoetermeer, Netherlands.
3 Reprints not available. Address correspondence to VP Carnielli,
Sophia Children’s Hospital, Room Sp 3456, Dr Molewaterplein 60, 3015
GJ, Rotterdam, Netherlands.
Received December 22, 1993.
Accepted for publication October 31, 1994.
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from

1038 CARNIELLI El AL
sition of the FM in triacylgiycerols (Table 1). The f3formula
contained triglycerides similar to those in human milk: 26%(wt:wt) of FM as palmitic acid, which is predominantly ester-
ified to the sn-2 (�3) position. The a formula contained similar
amounts of palmitic acid but it was mainly esterified to thesn-1,3 (a) positions. Part of the fat in the �3 formula consistedof synthetic triglycerides known as Betapol. This is produced
by interesterifying a tripalmitin-rich palm fraction with a mix-
ture of other oils by using the sn-1,3 specific lipase from
Rhizomucor miehei (code SP-392; Novo Industries, Copenha-
gen) (22).Twelve preterm infants born after a gestation ranging be-
tween 28 and 32 wk were randomly assigned to be fed the a or
13formula for 1 wk at a postnatal age of 38 ± 7 d. The infantswere then crossed over to receive the other formula for the
subsequent week. Half of the infants were first fed the aformula and then the f3 formula whereas the other half received
the formula in the reverse order. All infants were free ofmanifest disease, were not receiving any medication, and hadgrown normally before the study. The investigators wereblinded to the type of formula given to the infants. The anthro-pometric characteristics of the patients at birth and at the end of
the 7-d feeding periods are reported in Table 2.The study was conducted according to the guidelines of the
Ethical Committee of the Erasmus University, Rotterdam,
Netherlands, which agree with the principles expressed in theDeclaration of Helsinki.
Balance studies
Intakes of the formulas were determined by weighing the
bottles or by recording the volume with syringes in the case oftube feeding. Conversion from volume into grams was done by
TABLE 1
Composition of formula fed to preterm infants’
a Formula 13Formula
Protein (%) 2.01 1.99
Fat (%) 4.08 4.16
Calcium (%) 0.102 0.099
Phosphate (%) 0.045 0.046
Magnesium (%) 0.0065 0.0067
Fatty acids (% of total fatty acids by wt)
6:0-10:0 4.5 (ND) 4.0 (ND)
12:0 12.1 (17.2) 10.6 (16.2)
14:0 5.4 (3.3) 4.9 (3.9)
16:0 25.7 (9.8) 25.4 (58.0)
18:0 2.6 (1.1) 3.7 (2.4)
20:0 0.22 (ND) 0.26 (ND)
22:0 0.11 (ND) 0.12 (ND)
24:0 0.03 (ND) 0.05 (ND)
16:lco7 0.17 (ND) 0.21 (ND)
18:1w9 34.8 (41.8) 34.8 (13.2)
20:1 0.20 (ND) 0.32 (ND)
22:1 0.03 (ND) 0.08 (ND)
24:1 0.02 (ND) 0.03 (ND)
18:2w6 12.1 (22.1) 12.6 (5.1)
18:3w3 2.0 (0.3) 2.7 (0.5)
‘ Value in parentheses is the fatty acid composition (wt:wt) of the sn-2position. Both ready-to-feed formulas are devoid of arachidonic (20:4w6)
and docosahexaenoic acid (22:6o3). ND, not determined.
TABLE 2
Clinical characteristics of preterm infants at birth and at the end of the
two 1-wk diet periods’
.
At birtha Formula
.
period
(3 Formula.
period
Weight (kg) 1.4 ± 0.2 2.1 ± 0.3 2.1 ± 0.3
Gestational age (wk) 29.9 ± 1.4 - -
Head circumference 27.8 ± 1.2 31.8 ± 1.1 31.6 ± 1.6
Length(cm) - 44±2 44±2
Postnatal age (d) - 38 ± 7 38 ± 6
Fat mass (%) - 8.6 ± 3.5 8.2 ± 3.1
1 � � SD; n = 12. During the first week of the study six infants were fed
the a formula and six infants were fed the f3 formula. During the second
week the formulas were reversed. There were no significant differences.
multiplying the volume by the density value of 1035 g/L,
which was identical for both formulas.Balance studies with separate collections of urine (24 h) and
feces (72 h) were performed during the last 3 d of each feeding
period. Fecal collections were carried out bracketed by carmine
red. Fifty milligrams of carmine red were dissolved in 3 mL
distilled water and given either via the nasogastric tube or in
the mouth just before the 1200 feed on days 4 and 7 of eachdiet. Intestinal transit time was assumed to be equal to the timeelapsing from the administration of the carmine red and theproduction of the first red stool; it was measured twice in each
balance period (at the beginning and at the end of the 72 h) and
the two determinations averaged. Feces were collected includ-
ing the first red stool and excluding the last red stool ‘3 d later
for each collection period. Plastic sheets were placed inside thediapers for collection. Corrections were made for accidental
losses of feces into the diapers (double weighing of the diaper)
and for the feces sticking to the buttocks of the infants (double
weighing of the cleaning swabs). The total amount of feces
collected during the 3-d balance period was weighed and
homogenized and a small sample of the homogenate was
freeze-dried. Fat excretion was determined by using a modifi-
cation of the method of Jeejeebhoy et al (23), with twice asmuch hydrochloric acid added. Calcium and magnesium were
measured with an atomic-absorption spectrophotometer (model2380; Perkin-Elmer, Norwalk, CT) after acid digestion [3 h at
300 #{176}Cin 5 mL of a concentrated mixture of HNO3 andconcentrated H2S04 (2:1, by vol)]. The total urine volume was
measured and urinary calcium and magnesium were also mea-
sured by atomic-absorption spectrophotometry. Phosphate was
measured by a colorimetric method (24). In all cases, matrix
effects were eliminated by means of the standard addition
method (25).Excretions were calculated by multiplying the volume of
feces (or urine) produced by the concentration of the com-
pounds of interest. Intestinal absorption was calculated bydividing the apparent amount absorbed (intake - excretion) bythe intake, and then multiplying by 100.
Determination of FAs in the formulas and in the feces
The individual FA content of the formulas and of the feces
was determined by gas chromatography (GC), and analyses
were done in triplicate. Fresh fecal samples of 5-10 mg each
were transesterified by HCI methanol after the addition of
nonanoic (C9), heptadecanoic (C17), and tricosanoic (C23)
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from

Results
Because of the crossover design the clinical characteristics of
�3-PALMITATE IN PRETERM INFANTS 1039
acids as internal standards. The separation and identification of
FA methyl esters was performed by GC (model 5890 II;
Hewlett Packard, Amstelveen, Netherlands) equipped with a
fused-silica column (Supelcowax 10, 60 m X 0.25 mm internal
diameter, 0.25-sm film thickness; Supelco, Leusden, Nether-
lands), a flame-ionization detector (280 #{176}C),and a split-split-
less injector used in splitless mode (280 #{176}C).The GC was
operated at 60 #{176}Cinitially for 5 mm, then the oven temperature
was raised 20 #{176}C/minto 205 #{176}Cand held at this temperature for
15 mm. The temperature was then increased again 0.2 #{176}C/min
to 222 #{176}C.Helium was used as a carrier gas (2 mL/min) andpeak areas were calculated with HP-Chem station software
(Hewlett Packard) using nonanoic, heptadecanoic, and trico-
sanoic acids as internal standards. Fatty acids were identifiedby comparing the retention times with known standards (NuChek Prep, Elysian, MN). All reagents were analytical grade.
Statistical analysis
Data are presented as group mean ± SE unless otherwise
stated. Comparison of means was made by Student’s t test for
paired data after analysis of variance (ANOVA) showed no
significant period effect for all the studied variables. Correla-
tions between the data were by simple linear regression. All
calculations were performed with the statistical package SYS-TAT, version 5.2 (SYSTAT, mc, Evanston, IL).
the patients at the time of each study were almost identical
(Table 2). The intake of the formulas was similar between the
a and 13 periods: 154 ± 4 and 158 ± 5 mL . kg � . d ‘,
respectively. Fecal output, although somewhat higher in the
infants when fed the a formula (6.1 ± 0.8 and 4.3 ± 0.6g � kg ‘ . d� � for a and f3 formulas, respectively), was not
significantly different by treatment. Neither water (66 ± 2 and
60 ± 2%) nor fat (1.5 ± 0.2 and 1.3 ± 0.3 g � kg_i . d1)
accounted for this difference in stool weight. No differences
were found in urine production, 87 ± 2 and 91 ± 5
mL . kg ‘ . d � in infants fed the a and f3 formulas, respec-
tively. Mean intestinal transit time was also not significantly
different between diet periods: 29 ± 4 and 30 ± 5 h, respec-
tively, for the a and /3 formula.The fecal concentrations of the major FAs are reported in
Table 3. When fed the a formula, the infants had significantlyhigher concentrations of myristic (14:0), palmitic (16:0), and
stearic (18:0) acids and significantly lower concentrations of
oleic (18:1w9) and linoleic (18:2co6) acids in their feces than
when fed the 13 formula. Linolenic acid (18:3w3) in feces was
not significantly different between the two groups. Fat and FA
balance data are reported in Table 4. The intestinal absorptionof myristic, palmitic, and stearic acids was significantly better
when infants received the �3 formula than when they were fed
the a formula. Intestinal absorption of oleic and of linoleic
acids was not significantly different between the a and /3
periods. Total fat excretion was on average 0.2 g � kg � . d
lower and fat absorption 5% higher with the /3 formula than
with the a formula, but these differences were not statistically
significant (Table 4).
TABLE 3
Concentrations of selected fatty acids in feces of infants fed the a
formula for 1 wk and the /3 formula for 1 wk’
Fatty acid a Formula /3 Formula
12:0
(mg/g wet feces) 6.8 ± 0.6 5.1 ± 0.7
(% of fecal fat) 2.7 ± 0.1 1.9 ± 0.22
14:0
(mg/g wet feces) 11.8 ± 1.0 7.7 ± 0.8�
(% of fecal fat) 4.7 ± 0.2 2.8 ± 0.22
16:0
(mg/g wet feces) 140.4 ± 10.0 106.0 ± 9.8�
(% of fecal fat) 56.3 ± 1.6 38.6 ± 1.62
18:0
(mg/g wet feces) 28.7 ± 2.1 22.4 ± 1.7�
(% of fecal fat) 1 1.5 ± 0.4 8.5 ± 042
18:1w9
(mg/g wet feces) 36.3 ± 4.6 82.3 ± 9.12
(% of fecal fat) 14.3 ± 1.4 29.8 ± 1.72
18:2w6
(mg/g wet feces) 9.6 ± 2.3 25.5 ± 5.22
(% of fecal fat) 3.7 ± 1.0 8.8 ± 1.0�
18:3w3
(mg/g wet feces) 0.9 ± 0.1 1.5 ± 0.3
(% of fecal fat) 0.4 ± 0.06 0.5 ± 0.06
‘i±SE;n= 12.2-5 Significantly different from a formula: 2 p < 0.001, � P = 0.004,
4 P = 0.002, � P = 0.01.
During the /3 formula period, fecal excretion of calcium wassignificantly lower, 58.8 ± 7.8 and 82.0 ± 9.9 mg . kg’ . d1
(P < 0.05), whereas urinary calcium excretion was higher, 4.0
± 0.7 and 2.3 ± 0.5 mg . kg’ . d’ (P < 0.05), than during
the a formula period (Table 4). The intestinal absorption ofphosphorus was not different between periods; however, the
urinary excretion of phosphorus was significantly lower during
the /3 than the a periods (11.4 ± 1.9 and 16.7 ± 2.3
mg . kgt . d’, respectively, P < 0.02). On the /3 formula the
infants retained significantly more phosphorus than when fed
the a formula (58.1 ± 3.3 and 49.2 ± 2.7 mg . kgt . d’,respectively, P < 0.03). Urinary phosphorus losses were
inversely and significantly correlated with calcium absorption(r -0.43, P = <0.05).
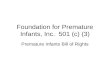
Magnesium data were not different during the two dietperiods (Table 4). Palmitic acid was the major fecal fatty acidin the majority of the infants. We found significant correlationsbetween fecal calcium excretion and the excretions of fat and
of the major fatty acids. Palmitic acid showed the highestcorrelation coefficient, followed by oleic acid and linoleic acid(Figure 1).
The fecal calcium content was significantly correlated withmyristic (r 0.42, P = 0.04), palmitic (r = 0.46, P = 0.039),and stearic (r = 0.42, P = 0.025) acids, ie, the major saturated
fatty acids, but not with the mono- or the polyunsaturated fattyacids. No correlation was observed between the fecal concen-trations of fat or of individual fatty acids and phosphorus or
magnesium.
Discussion
The results of this study support the importance of thestructure of dietary triglyceride on intestinal FA absorption and
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from

0 20 40 60 80 100 120 140 160 180
1040 CARNIELLI El AL
TABLE 4
Fat, fatty acid (FA), and mineral balances of infants fed the a formula
for 1 wk and the /3 formula for 1 wk’
a Formula 13 Formula
Fat
Intake (g . kg� . d�) 6.3 ± 0.6 6.6 ± 0.7
Fecal excretion (gkg1 .d_i) 1.5 ± 0.2 1.3 ± 0.2
Intestinal absorption (%) 76 ± 3 81 ± 4
FA intestinal absorption (%)12:0 95±1 97±1
14:0 80±3 90±22
16:0 51±6 73±42
18:0 9±12 61±52
18:1w9 88±3 82±4
18:2w6 91±3 84±5
18:3w3 95±1 96±1
Calcium
Intake (mg . kg � . d i) 162.1 ± 5.1 162.2 ± 4.9
Fecal excretion (mg . kg’ . d’) 82.0 ± 9.9 58.8 ± 7.8�
Intestinal absorption (%) 49.2 ± 5.9 63.7 ± 5.1
Urinary excretion (mg . kg � . d i) 2.3 ± 0.5 4.0 ± 073
Retention (mg . . d i) 77.9 ± 10.5 99.5 ± 8.2
(%) 47.7 ± 5.9 61.3 ± 5.0
Phosphorus
Intake (mg . kg � . d i) 71.9 ± 2.2 75.3 ± 2.3
Fecal excretion (mg . kg � . d i) 6.0 ± 1.2 5.8 ± 1.0
Intestinal absorption (%) 91.9 ± 1.5 92.2 ± 1.5
Urinary excretion (mg�kg’ .di) 16.7 ± 2.3 11.4 ± 1.9�’
Retention (mg . kg_i . d_i) 49.2 ± 2.7 58.1 ± 3#{149}35
(%) 69.0 ± 4.0 77.0 ± 3.8
Magnesium
Intake (mg . kg � . d i) 10.4 ± 0.3 1 1.0 ± 0.3
Fecal excretion (mg . kg � . d 1) 6.1 ± 0.7 5.6 ± 0.7
Intestinal absorption (%) 40.8 ± 7.0 48.6 ± 6.4
Urinary excretion (mg . kg_i . d_i) 1.4 ± 0.3 2.8 ± 0.8
Retention (mg.kg_i .d_i) 2.9 ± 0.9 2.6 ± 0.9
(%) 27.5 ± 8.5 23.2 ± 8.8
‘.f ± SE; n = 12.2-5 Significantly different from a formula: 2 p < 0.01, -� � < 0.05,
4 P < 0.02, � P < 0.03.
on mineral metabolism. The perception that the positionaldistribution of the FM in human milk and in formula triglyc-eride is important during the processes of digestion and ab-sorption is not new (26) and this problem has attracted the
interest of researchers for many years (18-21). No conclusive
data had been obtained to date. Our study was novel becausewe used synthetic triglycerides, and were thus able to produceinfant formulas with profiles identical to those of major FM,differing only in the isomeric position of FM in the triacyl-glycerols. Formulas, as opposed to human milk, do not containlipolytic enzymes, which improve fat absorption; therefore, theonly difference between the study periods was the structure ofthe dietary triglycerides. A different study including a humanmilk-fed group would not have been as informative as thepresent study because of the uncontrolled effects of the lipo-lytic enzymes and variable mineral content. Furthermore thecrossover design is well suited for the study of prematureinfants known to have a large variability in intestinal fat ab-
sorption (20). Thus we could study the two formulas in thesame infant and during two periods of comparable gastrointes-tinal function. A drawback of our study was its inability
Calcium Excretion (mg #{149}kg� #{149}d1)
FIGURE 1. Correlations between the excretion of calcium and of 16:0,
18:1, and 18:2.o6. All regressions are statistically significant. FA, fatty
acid.
to provide information on the effect of the dietary triglycerideon growth of the infants, because of its relative short study
periods.When fed the a formula the infants had in their feces
significantly higher concentrations of myristic, palmitic, andstearic acids, and significantly lower concentrations of oleic
and linoleic acids than when fed the /3 formula. A similarpattern of fecal FA concentrations was described by Verkade et
al (21), who compared the fecal FAs of a group of prematureinfants fed a lard-modified formula containing 88% of itspalmitic acid in the sn-2 position (and only 14% of oleic) with
a group fed a formula that had only 16% of palmitate but 40%
of the oleic acid in the same position. These authors foundhigher concentrations of oleic acid and lower concentrations ofmyristic and palmitic acids in the feces of the infants fed thelard-modified formula. In the above-mentioned study impor-
tant differences in the FA profiles of the formulas (ie, medium-chain triglycerides were present in the control formula but notin the lard-modified formula) prevented the authors from draw-
ing firm conclusions on the effects of the sn-2 palmitic acid.Nevertheless, the fecal concentrations of palmitic and oleicacids showed a pattern similar to our results.
If we had measured only the fecal concentrations of the FM
(qualitative data) we would have probably discussed the ad-vantage of the sn-2 position and the negative effect of esteri-
fication to the sn-1,3 positions. However, because the fecaloutput was higher (although not significantly) during the aformula period than during the /3 formula period, the FAbalance data show better intestinal absorption of myristic,
palmitic, and stearic acids during the /3 formula period, but nosignificant differences for oleic and linoleic acids. The latterFM were significantly more abundant in the feces of infantsfed the /3 formula than of those fed the a formula. The largevariability introduced when excretions are calculated (fecal
concentrations are multiplied by the more variable fecal output)may have contributed to the lack of statistical difference. Wecannot explain the larger (although not significant) fecal outputduring the a formula period. Other factors than those measuredby us (FM, fat, water, and minerals) may account for the
difference. The balance data indicate that the improvement inabsorption of the saturated FAs outweighed the slightly re-
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from

/3-PALMITATE IN PRETERM INFANTS 1041
duced absorption of the other FAs. We speculate that the
advantage of the /3 position could be even greater in term
infants. Lipid digestion and absorption are reported to be better
in term infants than in preterm infants, because of a larger
contribution of pancreatic lipase (6, 7) and more abundant bile
salts. The latter are extremely important for monoglyceride
absorption (8-10).
The relationship between fecal calcium and fecal fat or fecalFA has long been explored (27). Increasing calcium intakes in
children (28) and in neonates (12) increases the excretion of fat
and of saturated FAs. In our study, the intake of calcium was
similar from both formulas so we can only speculate that
during the a formula a larger amount of free intraluminal
palmitate may have trapped the calcium, perhaps via formation
of calcium soaps (26). The observation of lower fecal calcium
in the infants fed the /3 formula is supported by the concomitant
observations of higher calcium and lower phosphorus in the
urine. During the /3 formula period the mean calcium retentionincreased by 22 mg . kg � . d �. Note that this was achieved
with a formula containing 26% of FAs as palmitic acid (unlike
most of the infant formulas on the market), with most at the
sn-2 position, as is found in human milk. Improvements in
calcium balance have also been reported in infants fed formula
in which a large part of the fat blend was replaced by medium-
chain triglycerides (29, 30). Alternatively, increased retention
of �“22 mg Ca . kg � . d � could be achieved by an increaseddietary intake of =40-50 mg Ca . kg � . d’ (31). An increase
in the calcium content in the formula, however, could increase
the precipitation of calcium in the formula (32, 33), or have
detrimental effects on fat and FA absorption (12). Note that
during the j3 formula period the infants had a mean calcium
retention of 100 mg . kg ‘ . d ‘, and this value is “70% of
the calculated intrauterine retention (34).
In conclusion, we demonstrated that the isomeric position ofFM in dietary triglycerides has significant effects on the in-testinal metabolism of the FM. The use of the /3 formula,
which contained triglycerides with a structure similar to those
in human milk (26% of FAs as palmitic acid, which is pre-
dominantly esterified to the /3 position), was associated with an
improvement in the absorption of myristic, palmitic, and stearic
acids and of mineral balance. We emphasize that the structure
of human milk triglycerides offers advantages even in the
absence of the lipolytic enzymes of human milk. U
We gratefully acknowledge the help of Daniella Roofthooft in contrib-
uting to the recruitment of the patients during the initial part of the study.
References
1. Jensen RG. Lipids in human milk-composition and fat-soluble vita-
mins. In: Lebenthal E, ed. Textbook of gastroenterology and nutrition
in infancy. 2nd ed. New York: Raven Press, 1989:157-208.
2. Atkinson SA, Bryan MH, Anderson GH. Human milk feeding in
premature infants: protein, fat, and carbohydrate balances in the first
two weeks of life. I Pediatr 1981;99:617-24.
3. Brooke 00, Wood C, Barley I. Energy balance, nitrogen balance, and
growth in preterm infants fed expressed breast milk, a premature infant
formula, and two low-solute adapted formulae. Arch Dis Child 1982;
57:898-904.
4. Jarvenpaa AL. Feeding the low-birth-weight infant IV. Fat absorption
as a function of diet and duodenal bile acids. Pediatrics 1983;72:
684-9.
5. Watkins JB. Lipid digestion and absorption. Pediatrics 1985;
75(suppl):151-6.
6. Zoppi G, Andreotti G, Njai DM, Gaburro D. Exocrine pancreas func-
tion in premature and full term neonates. Pediatr Res 1972;6:880-6.
7. Fredrikzon B, Olivecrona T. Decrease of lipase and esterase activities
in intestinal contents of newborn infants during test meals. Pediatr Res
1978;12:631-4.
8. Brueton Mi, Berger HM, Brown GA, Ablitt L, Iyngkaran N, Wharton
BA. Duodenal bile acid conjugation and dietary sulphur amino acids in
the newborn. Gut 1978;19:95-8.
9. Murphy GM, Singer E. Bile acid metabolism in infants and children.
Gut 1974;15:151-63.
10. Watkins JB, Szczepanic P, Gould JB, Klein P, Lester R. Bile salt
metabolism in human premature infant. Gastroenterology 1975;69:
706-13.
11. Alemi B, Hamosh M, Scanlon JW, Salzman-Mann C, Hamosh P. Fat
digestion in very-low-birth-weight infants: effect of administration of
human milk to low-birth-weight formula. Pediatrics 1981;68:484-9.
12. Chappell JE, Clandinin MT. Kearney-Volpe C, Reichman B, Swyer
PW. Fatty acid balance studies in premature infants fed human milk or
formula: effect of calcium supplementation. I Pediatr 1986;108:439-
47.
13. Signer E, Murphy GM, Edkins 5, Anderson CM. Role of bile salts in
fat malabsorption of premature infants. Arch Dis Child 1974;49:174-
80.
14. Hamosh M. Enzymes in human milk: their role in nutrient digestion,
gastrointestinal function, and nutrient delivery to the newborn infant.
In: Lebenthal E, ed. Textbook of gastroenterology and nutrition in
infancy. 2nd ed. New York: Raven Press, 1989:121-34.
15. Bernback 5, Blackberg L, Hernell 0. The complete digestion of human
milk triacylglycerol in vitro requires gastric lipase, pancreatic co-
lipase-dependent lipase, and bile salt-stimulated lipase. I Clin Invest
1990;85:1221-6.
16. Breckenridge WC. Stereospecific analysis oftriacylglycerols. In: Kuk-
sis A, ed, Handbook of lipid research 1-fatty acids and glycerides.
New York: Plenum Press, 1978:197-232.
17. Thomson AB, Keelan M, Garg ML, Clandinin MT. Intestinal aspects
of lipid absorption: in review. Can J Physiol Pharmacol 1989;67:179-
91.
18. Tomarelli RM, Meyer BJ, Weaber JR, Bernhart FW. Effect of posi-
tional distribution on the absorption of the fatty acids of human milk
and infant formulas. I Nutr 1968;95:583-90.
19. Filer U Jr, Mattson FH, Fomon SJ. Triglyceride configuration and fat
absorption in the human infant. I Nutr 1969;99:293-8.
20. Verkade W, van Asselt WA, Vonk RI, et al. Fat absorption in
premature infants: the effect of lard and antibiotics. Eur J Pediatr
1989; 149: 126-9.
21. Verkade HJ, Hoving EB, Muskiet FM, et al. Fat absorption in neo-
nates: comparison of long-chain-fatty acid and triglyceride composi-
tions of formula, feces and blood. Am I Clin Nutr 1991;53:643-51.
22. Quinlan P, Moore S. Modification of triglycerides by lipases: process
technology and its application to the production of nutritionally im-
proved fats. Inform 1993;4:580-5.
23. Jeejeebhoy KN, Ahmad 5, Kozak G. Determination of fecal fat con-
taming both medium and long chain triglycerides and fatty acids. Clin
Biochem 1970;3:157-63.
24. Bartels PC, Roijers AFM. A kinetic study on the influence of the
parameters in the determination of inorganic phosphate by the molyb-
denum blue reaction. Clin Chim Acta 1975;61:135-44.
25. Willard HH, Merritt LL Jr, Dean JA. Instrumentation methods of
analysis. 4th ed. Princeton, NJ: D Van Nostrand Company, Inc, 1965:
342-4.
26. Small DM. The effects of glyceride structure on absorption and me-
tabolism. Annu Rev Nutr 1991;11:413-34.
27. Hanna FM, Navarrete DA, Hsu FA. Calcium-fatty acid absorption in
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from

1042 CARNIELLI El AL
term infants fed human milk and prepared formulas simulating human
milk. Pediatrics 1970;45:216-24.
28. Lutwak L, Laster L, Giltelman HI, Fox M, Whedon D. Effect of
dietary calcium and phosphorus on calcium phosphorus, nitrogen and
fat metabolism in children. Am I Clin Nutr 1964;14:76-82.
29. Tantibhedhyangkul P, Hashim SA. Medium-chain triglyceride feeding
in premature infants: effects on calcium and magnesium absorption.
Pediatrics 1978;61 :537-45.
30. Sulkers El, Lafeber HN, Degenhart Hi, Lindemans I, Sauer P11.
Comparison of two preterm formulas with or without addition of
medium chain triglycerides (MCTs). II: Effects on mineral balance. I
Pediatr Gastroenterol Nutr 1992;15:42-7.
31. Bronner F, Salle BL, Putet G, Rigo I, Senterre J. Net calcium absorp-
tion in premature infants: results of 103 metabolic balance studies. Am
I Clin Nutr 1992;56:1037-44.
32. Bhatia I, Fomon SI. Formulas for premature infants: fate of the
calcium and phosphorus. Pediatrics 1983;72:37-40.
33. Bhatia I. Formula fixed. Pediatrics 1985;75:800-1.
34. Ziegler EE, O’Donnell AM, Nelson SE, Fomon SI. Body composition
of the reference fetus. Growth 1976;40:329-41.
by guest on October 11, 2015
ajcn.nutrition.orgD
ownloaded from
Related Documents