Report EUR 26357 EN 2013 Author: Ramon Sabes-Figuera Editor: Fabienne Abadie Country Reports European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Report EUR 26357 EN
20 13
Author: Ramon Sabes-Figuera
Editor: Fabienne Abadie
Country Reports
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)

European Commission Joint Research Centre Institute for Prospective Technological Studies Contact information Address: Edificio Expo. c/ Inca Garcilaso, 3. E-41092 Seville (Spain) E-mail: [email protected] Tel.: +34 954488318 Fax: +34 954488300 http://ipts.jrc.ec.europa.eu http://www.jrc.ec.europa.eu This publication is a Scientific and Policy Report by the Joint Research Centre of the European Commission. Legal Notice Neither the European Commission nor any person acting on behalf of the Commission is responsible for the use which might be made of this publication. Europe Direct is a service to help you find answers to your questions about the European Union Freephone number (*): 00 800 6 7 8 9 10 11 (*) Certain mobile telephone operators do not allow access to 00 800 numbers or these calls may be billed.
A great deal of additional information on the European Union is available on the Internet.
It can be accessed through the Europa server http://europa.eu/.
JRC85927
EUR 26357 EN
ISBN 978-92-79-34778-8 (pdf)
ISSN 1831-9424 (online)
doi:10.2791/55973
Luxembourg: Publications Office of the European Union, 2013
© European Union, 2013
Reproduction is authorised provided the source is acknowledged.
Printed in Spain

1
Preface
A widespread uptake of eHealth technologies is likely to benefit European Healthcare systems both in terms of quality of care and financial sustainability and European society at large. This is why eHealth has been on the European Commission policy agenda for more than a decade. The objectives of the latest eHealth action plan developed in 2012 are in line with those of the Europe 2020 Strategy and the Digital Agenda for Europe.
This report, based on the analysis of the data from the "European Hospital Survey: Benchmarking deployment of e-Health services (2012–2013)" project, presents policy relevant results and findings for each of the 28 EU Member States as well as Iceland and Norway.
The results highlighted here are based on the analysis of the survey descriptive results as well as two composite indicators on eHealth deployment and eHealth availability and use that were developed based on the survey's data.


3
Table of Contents
Preface ................................................................................................................................................................. 1
Country Report Austria .................................................................................................................................. 9
1. Background .................................................................................................................................................................................. 11
2. Sample analysis ........................................................................................................................................................................ 11
3. Descriptive statistics and indicators .............................................................................................................................. 12
4. Composite indicators .............................................................................................................................................................. 16
Country Report Belgium .............................................................................................................................. 18
1. Background .................................................................................................................................................................................. 19
2. Sample analysis ........................................................................................................................................................................ 19
3. Descriptive statistics and indicators .............................................................................................................................. 20
4. Composite indicators .............................................................................................................................................................. 23
Country Report Bulgaria ............................................................................................................................. 25
1. Background .................................................................................................................................................................................. 27
2. Sample analysis ........................................................................................................................................................................ 27
3. Descriptive statistics and indicators .............................................................................................................................. 28
4. Composite indicators .............................................................................................................................................................. 31
Country Report Croatia ............................................................................................................................... 35
1. Background .................................................................................................................................................................................. 37
2. Sample analysis ........................................................................................................................................................................ 37
3. Descriptive statistics and indicators .............................................................................................................................. 38
4. Composite indicators .............................................................................................................................................................. 41
Country Report Cyprus ................................................................................................................................ 43
1. Background .................................................................................................................................................................................. 44
2. Sample analysis ........................................................................................................................................................................ 44
3. Descriptive statistics and indicators .............................................................................................................................. 45
4. Composite indicators .............................................................................................................................................................. 49
Country Report Czech Republic ................................................................................................................ 51
1. Background .................................................................................................................................................................................. 52
2. Sample analysis ........................................................................................................................................................................ 52
3. Descriptive statistics and indicators .............................................................................................................................. 53
4. Composite indicators .............................................................................................................................................................. 56
Country Report Denmark ............................................................................................................................ 58
1. Background .................................................................................................................................................................................. 59
2. Sample analysis ........................................................................................................................................................................ 59

4
3. Descriptive statistics and indicators .............................................................................................................................. 60
4. Composite indicators .............................................................................................................................................................. 63
Country Report Estonia ............................................................................................................................... 65
1. Background .................................................................................................................................................................................. 66
2. Sample analysis ........................................................................................................................................................................ 66
3. Descriptive statistics and indicators .............................................................................................................................. 67
4. Composite indicators .............................................................................................................................................................. 70
Country Report Finland ............................................................................................................................... 72
1. Background .................................................................................................................................................................................. 73
2. Sample analysis ........................................................................................................................................................................ 73
3. Descriptive statistics and indicators .............................................................................................................................. 74
4. Composite indicators .............................................................................................................................................................. 77
Country Report France ................................................................................................................................ 79
1. Background .................................................................................................................................................................................. 80
2. Sample analysis ........................................................................................................................................................................ 80
3. Descriptive statistics and indicators .............................................................................................................................. 81
4. Composite indicators .............................................................................................................................................................. 84
Country Report Germany ............................................................................................................................ 87
1. Background .................................................................................................................................................................................. 88
2. Sample analysis ........................................................................................................................................................................ 88
3. Descriptive statistics and indicators .............................................................................................................................. 89
4. Composite indicators .............................................................................................................................................................. 92
Country Report Greece ................................................................................................................................ 95
1. Background .................................................................................................................................................................................. 96
2. Sample analysis ........................................................................................................................................................................ 96
3. Descriptive statistics and indicators .............................................................................................................................. 97
4. Composite indicators ........................................................................................................................................................... 100
Country Report Hungary ........................................................................................................................... 103
1. Background ............................................................................................................................................................................... 104
2. Sample analysis ..................................................................................................................................................................... 104
3. Descriptive statistics and indicators ........................................................................................................................... 105
4. Composite indicators ........................................................................................................................................................... 108
Country Report Iceland ............................................................................................................................. 111
1. Background ............................................................................................................................................................................... 112
2. Sample analysis ..................................................................................................................................................................... 112
3. Descriptive statistics and indicators ........................................................................................................................... 113

5
4. Composite indicators ........................................................................................................................................................... 116
Country Report Ireland .............................................................................................................................. 118
1. Background ............................................................................................................................................................................... 119
2. Sample analysis ..................................................................................................................................................................... 119
3. Descriptive statistics and indicators ........................................................................................................................... 120
4. Composite indicators ........................................................................................................................................................... 123
Country Report Italy ................................................................................................................................... 126
1. Background ............................................................................................................................................................................... 127
2. Sample analysis ..................................................................................................................................................................... 127
3. Descriptive statistics and indicators ........................................................................................................................... 128
4. Composite indicators ........................................................................................................................................................... 131
Country Report Latvia ............................................................................................................................... 134
1. Background ............................................................................................................................................................................... 135
2. Sample analysis ..................................................................................................................................................................... 135
3. Descriptive statistics and indicators ........................................................................................................................... 136
4. Composite indicators ........................................................................................................................................................... 139
Country Report Lithuania ......................................................................................................................... 142
1. Background ............................................................................................................................................................................... 143
2. Sample analysis ..................................................................................................................................................................... 143
3. Descriptive statistics and indicators ........................................................................................................................... 144
4. Composite indicators ........................................................................................................................................................... 147
Country Report Luxembourg ................................................................................................................... 149
1. Background ............................................................................................................................................................................... 150
2. Sample analysis ..................................................................................................................................................................... 150
3. Descriptive statistics and indicators ........................................................................................................................... 151
4. Composite indicators ........................................................................................................................................................... 153
Country Report Malta ................................................................................................................................ 155
1. Background ............................................................................................................................................................................... 156
2. Sample analysis ..................................................................................................................................................................... 156
3. Descriptive statistics and indicators ........................................................................................................................... 157
4. Composite indicators ........................................................................................................................................................... 159
Country Report The Netherlands ........................................................................................................... 161
1. Background ............................................................................................................................................................................... 162
2. Sample analysis ..................................................................................................................................................................... 162
3. Descriptive statistics and indicators ........................................................................................................................... 163
4. Composite indicators ........................................................................................................................................................... 166

6
Country Report Norway ............................................................................................................................. 169
1. Background ............................................................................................................................................................................... 170
2. Sample analysis ..................................................................................................................................................................... 170
3. Descriptive statistics and indicators ........................................................................................................................... 171
4. Composite indicators ........................................................................................................................................................... 174
Country Report Poland .............................................................................................................................. 177
1. Background ............................................................................................................................................................................... 178
2. Sample analysis ..................................................................................................................................................................... 178
3. Descriptive statistics and indicators ........................................................................................................................... 179
4. Composite indicators ........................................................................................................................................................... 182
Country Report Portugal ........................................................................................................................... 185
1. Background ............................................................................................................................................................................... 186
2. Sample analysis ..................................................................................................................................................................... 186
3. Descriptive statistics and indicators ........................................................................................................................... 187
4. Composite indicators ........................................................................................................................................................... 190
Country Report Romania .......................................................................................................................... 193
1. Background ............................................................................................................................................................................... 194
2. Sample analysis ..................................................................................................................................................................... 194
3. Descriptive statistics and indicators ........................................................................................................................... 195
4. Composite indicators ........................................................................................................................................................... 198
Country Report Slovakia ........................................................................................................................... 201
1. Background ............................................................................................................................................................................... 202
2. Sample analysis ..................................................................................................................................................................... 202
3. Descriptive statistics and indicators ........................................................................................................................... 203
4. Composite indicators ........................................................................................................................................................... 206
Country Report Slovenia ........................................................................................................................... 209
1. Background ............................................................................................................................................................................... 210
2. Sample analysis ..................................................................................................................................................................... 210
3. Descriptive statistics and indicators ........................................................................................................................... 211
4. Composite indicators ........................................................................................................................................................... 213
Country Report Spain ................................................................................................................................. 216
1. Background ............................................................................................................................................................................... 217
2. Sample analysis ..................................................................................................................................................................... 217
3. Descriptive statistics and indicators ........................................................................................................................... 218
4. Composite indicators ........................................................................................................................................................... 221

7
Country Report Sweden ............................................................................................................................ 224
1. Background ............................................................................................................................................................................... 225
2. Sample analysis ..................................................................................................................................................................... 225
3. Descriptive statistics and indicators ........................................................................................................................... 226
4. Composite indicators ........................................................................................................................................................... 229
Country Report United Kingdom ............................................................................................................ 232
1. Background ............................................................................................................................................................................... 233
2. Sample analysis ..................................................................................................................................................................... 233
3. Descriptive statistics and indicators ........................................................................................................................... 234
4. Composite indicators ........................................................................................................................................................... 237


9
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Austria


11
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals1, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners2.
This document reports the results of this project for Austria. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Austria are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
242 hospitals were identified in Austria. Within this rough universe 201 (83%) completed the screener part of the questionnaire and 132 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (7% vs. 21%) and there were more hospitals of private, profit and non-profit, ownership (52% vs. 36%). Out of the Austrian universe, 43 acute hospitals (33%) completed the survey.
Table 1: Austrian sample breakdown by size of acute care hospitals
Austria N= Fewer than
101 beds
Between 101 and
250 beds
Between 251 and
750 beds
More than 750
beds
Don’t know/
No answer
2012 Census 132 9 60 46 14 3
7% 45% 35% 11% 2%
2012 sample 43 2 21 16 4 -
5% 49% 37% 9% -
2010 sample 15 1 9 5 - -
7% 60% 33% - -
1 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
2 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

12
Table 2: Austrian sample breakdown by ownership type
Austria N= Public Private Private not for
profit
Don't know/
No answer
Census 132 55 25 35 17
42% 19% 27% 13%
2012 43 20 7 14 2
47% 16% 33% 5%
2010 15 10 2 3 -
67% 13% 20% -
The final sample of hospitals included in the survey has a similar structure to the one of the Austrian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with more private and larger hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate. The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring. Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

13
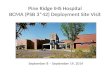
Figure 1: Austrian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 3 – eHealth indicators Austria
eHealth indicators - Austria Valid N %
hospitals
2012 difference
Austria vs.EU27+3
Austria evolution,
2012 vs. 20103
Infrastructure
Externally connected 43 91% 14% -3%
Broadband > 50Mbps 40 35% -1% -32%
Single and unified wireless 43 60% 20% -13%
Single EPR shared by all departments 41 73% 16% 0%
Applications
PACS usage 43 100% 29% 20%
ePrescribing 43 16% -30% 3%
Integrated system for eReferral 43 42% 4% 15%
Tele-monitoring 43 7% -3% 7%
Integration Exchange of clinical care information with external providers
43 88% 33% 22%
Exchange of laboratory results with external providers
41 83% 32% 16%
Exchange of radiology reports with external providers
43 91% 36% 31%
Security Clear and structured rules on access to clinical data
43 88% 3% -5%
EAS for disaster recovery in less than 24 hours
43 58% 10% -35%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
3 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Austria 2010 (n=15) Austria 2012 (n=43)

14
Position of the Austrian eHealth profile within EU27+3
Austria noticeably scores better than the average EU27+3 in four main areas: “Exchange of radiology reports with external providers”, “Exchange of laboratory results with external providers”, “Exchange of clinical care information with external providers” and “PACS usage”. In each of these areas, Austrian results exceed EU average by a 32% to 36%. In most other areas, Austria's results corresponds more or less to the European average, with the exception of “ePrescribing”- where the country´s results appear to be significantly lower (-30%), suggesting room for improvement.
Changes in the Austrian eHealth profile
Since 2010, Austria appears to have improved in many of the areas where its results are higher than European averages; “Exchange of radiology reports with external providers”, “Exchange of laboratory results with external providers”, “Exchange of clinical care information with external providers” and “PACS usage”. However, this is not a general trend, as three values recorded in 2010 were higher than the corresponding 2012 values: “EAS for disaster recovery in less than 24 hours”, “Broadband > 50Mbps” and “Single and unified wireless”. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 2: Austrian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Taking ownership type into account we observe that “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data” all reach high scores across acute hospitals regardless of ownership type. Additionally, “PACS usage” appears to be universal among Austrian acute hospitals, with 100% deployment across all ownership categories.

15
Results differ markedly for two other areas, “Broadband > 50Mbps” and “Single EPR shared by all departments”. For these, broad variations can be observed depending on the ownership category. 56% of Public hospitals enjoyed broadband access above the 50Mbps threshold, while only 1 out the 7 Private hospitals gave a similar statement. Similarly, 16 out of the 19 Public acute hospitals had a “Single EPR shared by all departments”, contrasting with 3 out of 6 for Private hospitals and 10 out of 14 for Private not for profit institutions.
Figure 3: Austrian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Taking the size of the hospitals into account, again we find that in most areas, there does not seem to be any difference among Austrian acute hospitals across most of the examined categories.
The only significant differences can be seen in the area of “Broadband > 50Mbps” where small and medium size hospitals (two categories which have between 101 and 750 beds) have a markedly lower broadband penetration, with only 5 out of 20 and 3 out of 11 hospitals respectively having high broadband penetration vs. 5 out of 8 hospitals for the very large hospitals (over 750 beds).

16
4. Composite indicators
The following section reports the results for Austria on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Austria´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Austria's eHealth Deployment indicator is based on data from 43 hospitals, while the Availability and Use indicator was built from the information provided by 35 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Austria eHealth Composite Indicators

17
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 15 hospitals) for Austria was 0.49, while the 2012 value was 0.56, which shows an increase of 7% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Austria and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a group of six hospitals with deployment above 0.5 but Effective use below 0.3. Only 3 hospitals were below EU+3 average for both composite indicators.
Figure 5: Austria's hospitals values of eHealth Composite Indicators

18
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Belgium

19
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals4, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners5.
This document reports the results of this project for Belgium. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Belgium are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
436 hospitals were identified in Belgium. Within this rough universe 243 (56%) completed the screener part of the questionnaire and 120 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (3% vs. 21%) and there were more hospitals of private, profit and non-profit, ownership (56% vs. 36%). Out of the Belgian universe, 50 acute hospitals (42%) completed the survey.
Table 4: Belgian sample breakdown by size of acute care hospitals
Belgium N= Fewer than
101 beds
Between 101 and
250 beds
Between 251 and
750 beds
More than 750
beds
Don’t know/
No answer
Census 120
3 25 49 25 18
3% 21% 41% 21% 15%
2012 50 1 10 23 10 6
2% 20% 46% 20% 12%
2010 23 - 7 11 5 -
- 30% 48% 22% -
4 his criteria was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
5 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

20
Table 5: Belgian sample breakdown by ownership type
Belgium N= Public Private Private not for
profit
Don't know/
No answer
Census 120
47 25 36 12
39% 21% 30% 10%
2012 50 23 13 13 1
46% 26% 26% 2%
2010 23 8 - 14 1
35% - 61% 4%
The final sample of hospitals included in the survey has a similar structure to the one of the Belgian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has more than doubled, with more public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate. The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.
Figure 4: Belgian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.

21
Table 6: eHealth indicators Belgium
eHealth indicators - Belgium Valid N %
hospitals
2012 difference
Belgium vs.EU27+3
Belgium evolution,
2012 vs. 20106
Infrastructure
Externally connected 50 92% 16% -4%
Broadband > 50Mbps 45 53% 18% 10%
Single and unified wireless 49 69% 29% 4%
Single EPR shared by all departments 49 73% 16% -5%
Applications
PACS usage 50 90% 19% -6%
ePrescribing 47 49% 2% 10%
Integrated system for eReferral 47 60% 22% -10%
Tele-monitoring 49 10% 0% 6%
Integration Exchange of clinical care information with external providers
49 92% 37% 1%
Exchange of laboratory results with external providers
49 92% 41% 1%
Exchange of radiology reports with external providers
50 76% 21% -11%
Security Clear and structured rules on access to clinical data
50 94% 9% 3%
EAS for disaster recovery in less than 24 hours
49 47% -1% -27%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
Position of the Belgian eHealth profile within EU27+3
Belgium scores better than the European average most notably in the following areas: “Externally connected”, “Broadband > 50Mbps”, “Single and unified wireless”, “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers”. In particular “Exchange of clinical care information with external providers” and “Exchange of laboratory results with external providers” enjoy a substantial lead over the European average, with these areas having a 37% and 41% lead. However, with respect to “EAS for disaster recovery in less than 24 hours”, “Tele-monitoring” and “ePrescribing”, Belgium either slightly lags behind the average or is very close to the average.
Changes in the Belgian eHealth profile
In the intervening period between this study and the last, it appears that Belgium’s eHealth profile has remained largely unchanged. With the exception of “EAS for disaster recovery in less than 24 hours”, which recorded a decrease relative to the 2010 results, most other values occupy a similar range. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
6 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

22
Figure 5: Belgian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Looking at the ownership types of Belgian hospitals, we can see a generally close range for the majority of the indicators. For “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”, that the variation in percentage penetration is 10% or less in all three indicators. “Exchange of clinical care information with external providers” has the largest variation of these three categories with a 10% variation between Public hospitals (95%) and Private hospitals (85%). Differences are more pronounced for “Single EPR shared by all departments”, with differences of 27 percentage points can be seen depending on the ownership type.
Figure 6: Belgian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.

23
When we take hospital scale into consideration we can see more differentiation across multiple areas. With the exception of “Clear and structured rules on access to clinical data”, all other areas show a large disparity between eHealth profile values. “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage” and “Exchange of clinical care information with external providers” all display relevant variations. However, it does not appear that scale is by itself a determinant of penetration in this context. For example, while the largest acute hospitals (over 750 beds) have 100% usage of “PACS usage” and “Exchange of clinical care information with external providers” and 69% of “Broadband > 50Mbps”, when we examine “Single EPR shared by all departments” the largest hospitals actually lag behind the smaller ones.
4. Composite indicators
The following section reports the results for Belgium on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Belgium´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Belgium's eHealth Deployment indicator is based on data from 48 hospitals, while the Availability and Use indicator was built from the information provided by 43 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.

24
Figure 4: Belgium eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. . In 2010, this indicator (based on data from 23 hospitals) for Belgium was 0.51, while the 2012 value was 0.55, which shows an increase of 4% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Belgium and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a group of 4 hospitals with deployment above 0.5 but Effective use below 0.3. Only 5 hospitals were below EU+3 average for both composite indicators.
Figure 5: Belgium's hospitals values of eHealth Composite Indicators

25
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Bulgaria


27
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals7, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners8
This document reports the results of this project for Bulgaria. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Bulgaria are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
388 hospitals were identified in Bulgaria. Within this rough universe 207 (53%) completed the screener part of the questionnaire and 109 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (34% vs. 21%) and there were more hospitals of public ownership (74% vs. 64%). Out of the Bulgarian universe, 62 acute hospitals (57%) completed the survey.
Table 7: Bulgarian sample breakdown by size of acute care hospitals
Bulgaria N= Fewer than 101 beds
Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No answer
Census 109
35 32 30 6 6
32% 29% 28% 6% 6%
2012 62 22 17 18 3 2
35% 27% 29% 5% 3%
2010 15 5 3 4 3 -
33% 20% 27% 20% -
7 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
8 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

28
Table 8: Bulgarian sample breakdown by ownership type
Bulgaria N= Public Private Private not for
profit Don't know/ No answer
Census 109
73 24 1 11
67% 22% 1% 10%
2012 62 43 14 - 5
69% 23% - 8%
2010 15 11 3 1 -
73% 20% 7% -
The final sample of hospitals included in the survey has a similar structure to the one of the Bulgarian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has quadrupled, with a lower proportion of very large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

29
Figure 7: Bulgarian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 9: eHealth indicators Bulgaria
eHealth indicators - Bulgaria Valid N %
hospitals
2012 difference
Bulgaria vs.EU27+3
Bulgaria evolution,
2012 vs. 20109
Infrastructure
Externally connected 62 60% -17% -14%
Broadband > 50Mbps 52 46% 11% 4%
Single and unified wireless 58 17% -23% -3%
Single EPR shared by all departments 61 39% -18% -7%
Applications
PACS usage 59 51% -20% 11%
ePrescribing 39 33% -13% 33%
Integrated system for eReferral 39 44% 6% 17%
Tele-monitoring 49 0% -10% -7%
Integration Exchange of clinical care information with external providers
57 44% -11% 44%
Exchange of laboratory results with external providers
57 25% -27% 25%
Exchange of radiology reports with external providers
56 20% -35% 20%
Security Clear and structured rules on access to clinical data
62 92% 7% -1%
EAS for disaster recovery in less than 24 hours
60 45% -3% -19%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
9 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

30
Position of the Bulgarian eHealth profile within EU27+3
Bulgaria noticeably scores worse than the average EU27+3 in in many areas; “Exchange of radiology reports with external providers”, “Exchange of laboratory results with external providers” and “PACS usage” are the areas with largest discrepancies. However, other areas fared better, with “Clear and structured rules on access to clinical data”, “Broadband > 50Mbps” and “Integrated system for eReferral” all very close to the European average.
Changes in the Bulgarian eHealth profile
While Bulgaria scores worse than the European average, it has shown some significant advances within a two-year period. These advances are most noteworthy in the areas of “Exchange of radiology reports with external providers” (+20%), “Exchange of clinical care information with external providers” (+44%) and also “ePrescribing” (+33%). Two areas appear to have suffered contraction: “EAS for disaster recovery in less than 24 hours” and “Externally connected” Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 8: Bulgarian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Areas as “Broadband > 50Mbps”, “Exchange of clinical care information with external providers” and “PACS usage”) show important differences. between Public and Private hospitals. Looking across ownership types, Private hospitals appear to be generally better endowed with respect to eHealth facilities, with the exception of “Broadband > 50Mbps”, where Private hospitals lag behind Public hospitals

31
Figure 9: Bulgarian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
The clearest differences in eHealth profile become apparent when Bulgarian hospitals are differentiated by size. In every single category, hospitals with more than 750 beds outperform or equal hospitals of a smaller size segment. However, when looking at the other hospital size categories, the relationship between scales is less pronounced. For example, hospitals of between 251 and 750 beds score better than smaller hospitals in most categories, but they have low scores in the “Exchange of clinical care information with external providers” category. Below this level, the relationship between scale and take-up is not clear, as hospitals with between 101 and 250 beds score higher than hospitals with fewer than 101 beds in only two categories
4. Composite indicators
The following section reports the results for Bulgaria on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4

32
categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Bulgaria´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Bulgaria's eHealth Deployment indicator is based on data from 51 hospitals, while the Availability and Use indicator was built from the information provided by 59 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Bulgaria eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 11 hospitals) for Bulgaria was 0.22, while the 2012 value was 0.32, which shows an increase of 11% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Bulgaria and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a large group of hospitals with almost no effective use at various levels of deployment. Only 2 hospitals were above EU+3 average for both composite indicators.

33
Figure 5: Bulgaria's hospitals values of eHealth Composite Indicators


35
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Croatia


37
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals10, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners11
This document reports the results of this project for Croatia. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Croatia are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
75 hospitals were identified in Croatia. Within this rough universe 32 (43%) completed the screener part of the questionnaire and 22 qualified as acute care hospitals. There were no hospitals with less than 100 beds among these hospitals, while the proportion of this type of hospitals among the universe of acute Hospitals at EU27+3 level was 21%. All the Croatian hospitals that qualified as acute were of public ownership (64% at EU27+3 level). Out of the Croatian universe, 11 acute hospitals (57%) completed the survey.
Table 10: Croatian sample breakdown by size of acute care hospitals
Croatia N= Fewer than 101 beds
Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No answer
Census 22
- 4 9 6 3
- 18% 41% 27% 14%
2012 11 - 2 6 2 1
- 18% 55% 18% 9%
2010 4 - 2 2 - -
- 50% 50% - -
10 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
11 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

38
Table 11: Croatian sample breakdown by ownership type
Croatia N= Public Private Private not for
profit Don't know/ No answer
Census 22
20 - - 2
91% - - 9%
2012 11 11 - - -
100% - - -
2010 4 4 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Croatian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with a lower proportion of very small hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate. The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

39
Figure 10: Croatian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 12 – eHealth indicators Croatia
eHealth indicators - Croatia Valid N %
hospitals
2012 difference
Croatia vs.EU27+3
Croatia evolution,
2012 vs. 201012
Infrastructure
Externally connected 11 100% 24% 0%
Broadband > 50Mbps 11 27% -8% -73%
Single and unified wireless 11 18% -22% 18%
Single EPR shared by all departments 11 82% 25% 32%
Applications
PACS usage 11 91% 20% 41%
ePrescribing 11 27% -19% 27%
Integrated system for eReferral 11 64% 26% -11%
Tele-monitoring 10 20% 10% 20%
Integration Exchange of clinical care information with external providers
11 73% 17% 23%
Exchange of laboratory results with external providers
11 82% 31% 82%
Exchange of radiology reports with external providers
10 50% -5% 25%
Security Clear and structured rules on access to clinical data
11 100% 15% 0%
EAS for disaster recovery in less than 24 hours
11 64% 16% -11%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here.
12 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Croatia 2010 (n=4) Croatia 2012 (n=11)

40
Position of the Croatian eHealth profile within EU27+3
Croatia remains close to the European average regarding the development of its eHealth profile, with variability across the range of examined indicators. Areas where Croatia performs better than the average EU27+3 include: “Externally connected”, “Single EPR shared by all departments”, “PACS usage”, “Integrated system for eReferral”, “Tele-monitoring”, “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers”, “Clear and structured rules on access to clinical data” and “EAS for disaster recovery in less than 24 hours”. Compared the EU27+3 average, areas with lower scores included “Broadband > 50Mbps”, “Single and unified wireless”, and “ePrescribing”.
Changes in the Croatian eHealth profile
Interestingly, the development of Croatia’s eHealth profile has been strong between 2010 and 2012. Croatia demonstrated a healthy growth in eHealth endowment across the acute hospital sector. Five areas in particular recorded high growth: “Single EPR shared by all departments”, “PACS usage”, “ePrescribing”, “Exchange of clinical care information with external providers” and “Exchange of laboratory results with external providers”. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size of the hospitals.
Figure 2: Croatian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
When taking the size of hospitals into account, we can see very good penetration of “Clear and structured rules on access to clinical data” across all size segments. Otherwise the results do not show any strong patterns.

41
4. Composite indicators
The following section reports the results for Croatia on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Croatia´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Croatia's eHealth Deployment indicator is based on data from 8 hospitals, while the Availability and Use indicator was built from the information provided by 7 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 3: Croatia eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Croatia EU27+3

42
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 4 hospitals) for Croatia was 0.36, while the 2012 value was 0.38, which shows an increase of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Croatia and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that Only 1 hospital is below EU+3 average for both composite indicators.
Figure 4. Croatia's hospitals values of eHealth Composite Indicators

43
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Cyprus

44
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals13, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners14
This document reports the results of this project for Cyprus. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Cyprus are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
70 hospitals were identified in Cyprus. Within this rough universe 54 (77%) completed the screener part of the questionnaire and 22 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was considerably higher compared to the universe of acute Hospitals at EU27+3 level (89% vs. 21%) and there were less hospitals of public ownership (10% vs. 64%). Out of the Cypriot universe, 13 acute hospitals (59%) completed the survey.
Table 13: Cypriot sample breakdown by size of acute care hospitals
Cyprus N= Fewer than 101 beds
Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No answer
Census 22
17 2 - - 3
77% 9% - - 14%
2012 13 9 2 - - 2
69% 15% - - 15%
2010 8 5 - 1 - 2
62% - 12% - 25%
13 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
14 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

45
Table 14: Cypriot sample breakdown by ownership type
Cyprus N= Public Private Private not for
profit Don't know/ No answer
Census 22 2 19 - 1
9% 86% - 5%
2012 13 1 12 - -
8% 92% - -
2010 8 4 4 - -
50% 50% - -
The final sample of hospitals included in the survey has a similar structure to the one of the Cypriot universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has increased, with a larger proportion of private hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

46
Figure 11: Cypriot acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 15 – eHealth indicators Cyprus
eHealth indicators - Cyprus Valid N %
hospitals
2012 difference
Cyprus vs.EU27+3
Cyprus evolution,
2012 vs. 201015
Infrastructure
Externally connected 11 36% -40% -39%
Broadband > 50Mbps 10 10% -26% 10%
Single and unified wireless 12 58% 18% 58%
Single EPR shared by all departments 9 56% -1% -19%
Applications
PACS usage 12 42% -29% 13%
ePrescribing 10 10% -37% -28%
Integrated system for eReferral 10 40% 2% -10%
Tele-monitoring 9 0% -10% 0%
Integration Exchange of clinical care information with external providers
10 30% -25% 13%
Exchange of laboratory results with external providers
11 55% 3% 21%
Exchange of radiology reports with external providers
11 64% 9% 47%
Security Clear and structured rules on access to clinical data
11 73% -13% -27%
EAS for disaster recovery in less than 24 hours
11 45% -3% -30%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
15 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

47
Position of the Cypriot eHealth profile within EU27+3
Cyprus remains below the European average in many areas. Of the 13 indicators under review, Cyprus was behind in 9 of these. The largest gaps were recorded in “Externally connected”, “Broadband >50Mbps”, “PACS usage”, and “ePrescribing”.
Changes in the Cypriot eHealth profile
Cyprus’s aggregate eHealth score has changed little between 2010 and 2012. However, the distribution of the individual values comprising the aggregate profile appears to have changed significantly. Of the 13 indicators considered, six have recorded positive growth, six have recorded negative growth, while one value remained unchanged. The most important growth areas were “Single and unified wireless” and “Exchange of radiology reports with external providers”, while contracting areas included “Externally connected” and “EAS for disaster recovery in less than 24 hours”. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 12: Cypriot acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Values for one Public and eight to eleven Private acute hospitals have been recorded for Cyprus. The sole Public hospital and 7 out of 10 Private hospitals declared having “Clear and structured rules on access to clinical data”, whereas half of the private hospitals have a “Single EPR shared by all departments” and 2 out of 9 “Exchange of clinical care information with external providers”. While the sole Public hospital declared having access to all services except for “PACS usage”, this last service was available in almost half of Private hospitals.

48
Figure 13: Cypriot acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
As Cyprus is one of the smallest European states, it is not surprising that no values were returned for the size segments of ‘Between 251 and 750 beds’ and ‘More than 750 beds’. Therefore our analysis is confined to the smaller categories, namely ‘fewer than 101 beds’ and ‘between 101 and 250 beds’. Within this grouping, the larger hospitals tend to lead in all five categories. In addition, the disparity between Cyprus’s larger and smaller hospitals is striking, with “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data” registering relevant differences.

49
4. Composite indicators
The following section reports the results for Cyprus on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Cyprus´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Cyprus's eHealth Deployment indicator is based on data from 7 hospitals, while the Availability and Use indicator was built from the information provided by 9 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Cyprus eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Cyprus EU27+3

50
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 4 hospitals) for Cyprus was 0.34, while the 2012 value was 0.43, which shows an increase of 9% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Cyprus and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there are 2 hospitals with low levels of deployment and no effective use that lower Cyprus average values of the indicators.
Figure 5. Cyprus's hospitals values of eHealth Composite Indicators

51
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Czech Republic

52
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals16, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners17.
This document reports the results of this project for Czech Republic. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Czech Republic are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
470 hospitals were identified in Czech Republic. Within this rough universe 269 (57%) completed the screener part of the questionnaire and 142 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (9% vs. 21%) and there were similar proportion hospitals of public ownership (68% and 64%). Out of the Czech universe, 40 acute hospitals (28%) completed the survey.
Table 16: Czech sample breakdown by size of acute care hospitals
Czech Republic N= Fewer than 101 beds
Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No answer
Census 142
10 45 44 16 27
7% 32% 31% 11% 19%
2012 40 3 12 11 6 8
8% 30% 28% 15% 20%
2010 15 1 4 3 6 1
7% 27% 20% 40% 7%
16 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
17 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

53
Table 17: Czech sample breakdown by ownership type
Czech Republic N= Public Private Private not for
profit Don't know/ No answer
Census 142
89 37 5 11
63% 26% 4% 8%
2012 40 25 11 2 2
62% 28% 5% 5%
2010 15 10 3 1 1
67% 20% 7% 7%
The final sample of hospitals included in the survey has a similar structure to the one of the Czech universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with a lower proportion of very large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.
Figure 14: Czech acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.

54
Table 18 – eHealth indicators Czech Republic
eHealth indicators - Czech Republic Valid N %
hospitals
2012 difference
Czech Republic
vs.EU27+3
Czech Republic
evolution, 2012 vs.
201018
Infrastructure
Externally connected 39 56% -20% -17%
Broadband > 50Mbps 37 41% 5% 7%
Single and unified wireless 39 26% -14% 12%
Single EPR shared by all departments 38 82% 25% -5%
Applications
PACS usage 40 95% 24% 22%
ePrescribing 36 50% 3% 37%
Integrated system for eReferral 36 39% 1% 19%
Tele-monitoring 39 3% -8% 3%
Integration Exchange of clinical care information with external providers
36 61% 6% 47%
Exchange of laboratory results with external providers
38 84% 33% 27%
Exchange of radiology reports with external providers
40 85% 30% -1%
Security Clear and structured rules on access to clinical data
40 95% 10% 8%
EAS for disaster recovery in less than 24 hours
39 72% 24% 15%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
Position of the Czech eHealth profile within EU27+3
The Czech Republic scores better than the average EU27+3 score in eHealth profile indicators, in particular in the areas of “Single EPR shared by all departments”, “PACS usage”, “Exchange of laboratory results with external providers”, “Exchange of radiology reports with external providers” and “EAS for disaster recovery in less than 24 hours”. Areas in which the country has worse scores than the average were “Externally connected”, “Single and unified wireless” and “Tele-monitoring”..
Changes in the Czech eHealth profile
The Czech eHealth profile has expanded considerably since 2010. Areas which have seen the most gain include “ePrescribing” (+37%), “Exchange of clinical care information with external providers” (+47%) and “Exchange of laboratory results with external providers” (+27%). Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
18 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

55
Figure 15: Czech acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Some patterns can be seen with respect to ownership of acute hospitals and performance within eHealth. Although the Private not for profit hospitals category (only 2 hospitals) had the maximum score in three of the five categories (“Single EPR shared by all departments”, “PACS usage” and “Clear and structured rules on access to clinical data”), they did not have “Broadband > 50Mbps” and were the lowest performer in “Exchange of clinical care information with external providers”. When comparing the Public and Private hospital segments a 47 percentage point difference was observed for “Broadband > 50Mbps”.
Figure 16: Czech acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.

56
They were not relevant differences between hospitals according to their size in their scores. Only in the category “Exchange of clinical care information with external providers”, large hospitals perform worse than hospitals in other categories.
4. Composite indicators
The following section reports the results for Czech Republic on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Czech Republic´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Czech Republic's eHealth Deployment indicator is based on data from 39 hospitals, while the Availability and Use indicator was built from the information provided by 34 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Czech Republic eHealth Composite Indicators

57
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 14 hospitals) for Czech Republic was 0.36, while the 2012 value was 0.36, which shows no variation over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Czech Republic and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a significant group of hospitals (9) with almost no effective use at various levels of deployment while the rest of Czech hospitals have use scores higher than the EU27+3 average.
Figure 5: Czech Republic's hospitals values of eHealth Composite Indicators

58
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Denmark

59
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals19, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners20.
This document reports the results of this project for Denmark. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Denmark are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
270 hospitals were identified in Denmark. Within this rough universe 126 (47%) completed the screener part of the questionnaire and 54 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (40% vs. 21%) and there were more hospitals of public ownership (76% vs. 64%). Out of the Danish universe, 16 acute hospitals (30%) completed the survey.
Table 19: Danish sample breakdown by size of acute care hospitals
Denmark N= Fewer than 101 beds
Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No answer
Census 54
17 3 14 8 12
31% 6% 26% 15% 22%
2012 16 5 - 5 3 3
31% - 31% 19% 19%
2010 8 - 1 4 3 -
- 12% 50% 38% -
19 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
20 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

60
Table 20: Danish sample breakdown by ownership type
Denmark N= Public Private Private not for
profit Don't know/ No answer
Census 54
38 11 1 4
70% 20% 2% 7%
2012 16 11 4 1 -
69% 25% 6% -
2010 8 8 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Danish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has doubled, with higher proportion of small and private hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

61
Figure 17: Danish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 21: eHealth indicators Denmark
eHealth indicators - Denmark Valid N %
hospitals
2012 difference
Denmark vs.EU27+3
Denmark evolution,
2012 vs. 201021
Infrastructure
Externally connected 16 81% 5% -19%
Broadband > 50Mbps 8 88% 52% -12%
Single and unified wireless 15 80% 40% -20%
Single EPR shared by all departments 15 87% 30% -13%
Applications
PACS usage 16 94% 23% -6%
ePrescribing 16 94% 47% -6%
Integrated system for eReferral 16 94% 56% -6%
Tele-monitoring 16 19% 9% -19%
Integration Exchange of clinical care information with external providers
15 100% 49% 13%
Exchange of laboratory results with external providers
15 80% 32% -20%
Exchange of radiology reports with external providers
14 93% -9% -3%
Security Clear and structured rules on access to clinical data
16 100% 15% 0%
EAS for disaster recovery in less than 24 hours
14 79% 30% 4%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
21 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferral
Tele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external
providers
Exchange of radiology reports with external
providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Denmark 2010 (n=8) Denmark 2012 (n=16)

62
Position of the Danish eHealth profile within EU27+3
Denmark noticeably scores better than the average EU27+3 in all areas but Exchange of radiology reports with external providers”. “The performances for “Integrated system for eReferral” and “Broadband > 50Mbps” were particularly outstanding, registering respectively 56% and 52% higher than EU27+3 scores.
. However, other areas fared better, with “Clear and structured rules on access to clinical data”, “Broadband > 50Mbps” and “Integrated system for eReferral” all very close to the European average.
Changes in the Danish eHealth profile
The lower average scores recorded by Denmark’s eHealth indicators between 2010 and 2012 can be partly explained by the doubling of the sample and its increased representativeness. Indeed, all but two eHealth indicators (“Exchange of clinical care information with external providers” and “EAS for disaster recovery in less than 24 hours”) dropped over the period under review. However, this evolution has to be seen in the context of the already high 2010 scores for all indicators. Nevertheless, these results should be taken with caution as mentioned. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 18: Danish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Danish eHealth indicators generally scored high across all ownership categories. While “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data” were the most widely implemented indicators across all hospital types, “Broadband > 50Mbps” was not implemented at all by the sole Private hospital interviewed. All the other indicators registered high implementation rates in both Private and Public hospitals.

63
Figure 19: Danish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In terms of hospital size, there were almost no differences in the scores between categories.
4. Composite indicators
The following section reports the results for Denmark on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Denmark´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals.

64
Denmark's eHealth Deployment indicator is based on data from 13 hospitals, while the Availability and Use indicator was built from the information provided by 10 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Denmark eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 8 hospitals) for Denmark was 0.64, while the 2012 value was 0.66, which shows an increase of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Denmark and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that for most of the hospitals there is a clear relationship between levels of deployment and of effective use. Only 1 hospital was below EU27+3 average for one of the composite indicators.
Figure 5: Denmark's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Denmark EU27+3

65
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Estonia

66
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals22, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners23.
This document reports the results of this project for Estonia. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Estonia are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
136 hospitals were identified in Estonia. Within this rough universe 90 (66%) completed the screener part of the questionnaire and 25 qualified as acute care hospitals. The proportion of hospitals of between 100 and 250 beds was higher compared to the universe of acute Hospitals at EU27+3 level (43% vs. 31%) and there were more hospitals of public ownership (88% vs. 64%). Out of the Estonian universe, 12 acute hospitals (48%) completed the survey.
Table 22: Estonian sample breakdown by size of acute care hospitals
Estonia N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 25
4 10 5 4 2
16% 40% 20% 16% 8%
2012 12 1 5 4 2 -
8% 42% 33% 17% -
2010 3 - 1 - 2 -
- 33% - 67% -
22 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
23 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

67
Table 23: Estonian sample breakdown by ownership type
Estonia N= Public Private Private not for
profit Don't know/ No answer
Census 25
21 1 2 1
84% 4% 8% 4%
2012 12 11 - 1 -
92% - 8% -
2010 3 3 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Estonian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has quadrupled, with a lower proportion of very large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI)with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

68
Figure 20: Estonian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 24: eHealth indicators Estonia
eHealth indicators - Estonia Valid N %
hospitals
2012 difference
Estonia vs.EU27+3
Estonia evolution,
2012 vs. 201024
Infrastructure
Externally connected 12 100% 24% 33%
Broadband > 50Mbps 11 73% 37% 39%
Single and unified wireless 12 33% -7% 0%
Single EPR shared by all departments 12 100% 43% 33%
Applications
PACS usage 12 100% 29% 0%
ePrescribing 12 100% 53% 0%
Integrated system for eReferral 12 83% 46% 17%
Tele-monitoring 12 17% 6% 17%
Integration Exchange of clinical care information with external providers
12 92% 36% -8%
Exchange of laboratory results with external providers
12 92% 40% 42%
Exchange of radiology reports with external providers
12 100% 45% 33%
Security Clear and structured rules on access to clinical data
12 92% 6% -8%
EAS for disaster recovery in less than 24 hours
12 50% 2% -17%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
24 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

69
Position of the Estonian eHealth profile within EU27+3
Estonia scores better than the EU27+3 average by at least 40% in five of the 13 eHealth indicators under review. These five areas are “Single EPR shared by all departments”, “ePrescribing”, “Integrated system for eReferral”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers”. Only one Estonian indicator was below the European average: “Single and unified wireless”
Changes in the Estonian eHealth profile
Estonia has grown from an already strong performance in 2010 to an even stronger eHealth position in 2012. “Externally connected”, “Broadband > 50Mbps”, “Single EPR shared by all departments”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers” have increased by between 33% and 42% over the period Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 21: Estonian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
As all of the hospitals but one belong to the public ownership category, this level of analysis and differences found is not very relevant.
70%
100%
100%
91%
91%
100%
100%
100%
100%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Public (n=10-11) Private not for profit (n=1)

70
Figure 22: Estonian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Two of the five indicators (“Single EPR shared by all departments” and “PACS usage”) were fully implemented across all categories and for the other indicators there is no clear pattern according to the size of the hospital.
4. Composite indicators
The following section reports the results for Estonia on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.

71
The following graph displays the average values of these indicators in Estonia´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Estonia's eHealth Deployment indicator is based on data from 12 hospitals, while the Availability and Use indicator was built from the information provided by 7 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Estonia eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (however based on data from only 1 hospital ) for Estonia was 0.43, while the 2012 value was 0.63, which shows an increase of 20% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Estonia and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that all Estonian hospitals were above EU27+3 average for both composite indicators
Figure 5: Estonia's hospitals values of eHealth Composite Indicators

72
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Finland

73
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals25, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners26.
This document reports the results of this project for Finland. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Finland are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
620 hospitals were identified in Finland. Within this rough universe 486 (78%) completed the screener part of the questionnaire and 46 qualified as acute care hospitals. The proportion of hospitals of between 100 and 250 beds was higher compared to the universe of acute Hospitals at EU27+3 level (50% vs. 31%)and there were more hospitals of public ownership (89% vs. 64%). Out of the Finnish universe, 26 acute hospitals (57%) completed the survey.
Table 25: Finnish sample breakdown by size of acute care hospitals
Finland N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 46
10 18 6 2 10
22% 39% 13% 4% 22%
2012 26 4 12 4 1 5
15% 46% 15% 4% 19%
2010 15 3 7 5 - -
20% 47% 33% - -
25 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
26 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

74
Table 26: Finnish sample breakdown by ownership type
Finland N= Public Private Private not for
profit Don't know/ No answer
Census 46
39 5 - 2
85% 11% - 4%
2012 26 24 2 - -
92% 8% - -
2010 15 15 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Finnish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost doubled, with a slightly lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

75
Figure 23: Finnish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 27 – eHealth indicators Finland
eHealth indicators - Finland Valid N %
hospitals
2012 difference
Finland vs.EU27+3
Finland evolution,
2012 vs. 201027
Infrastructure
Externally connected 26 85% 8% -15%
Broadband > 50Mbps 24 92% 56% -2%
Single and unified wireless 26 65% 25% -15%
Single EPR shared by all departments 25 80% 23% -7%
Applications
PACS usage 26 96% 25% -4%
ePrescribing 26 81% 34% 74%
Integrated system for eReferral 26 85% 47% -9%
Tele-monitoring 26 19% 9% -4%
Integration Exchange of clinical care information with external providers
26 81% 25% -12%
Exchange of laboratory results with external providers
26 77% 26% -23%
Exchange of radiology reports with external providers
26 85% 29% -9%
Security Clear and structured rules on access to clinical data
26 100% 15% 0%
EAS for disaster recovery in less than 24 hours
26 50% 2% 10%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
27 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

76
Position of the Finnish eHealth profile within EU27+3
Finland’s eHealth profile in the European context can be currently considered to be excellent. It displays high value positive difference in every single one of the 13 values examined – essentially having higher scores than the EU average in all areas. The two highest performing areas, “Broadband > 50Mbps” and “Integrated system for eReferral” score 56% and 47% respectively.
Changes in the Finnish eHealth profile
Less positive for Finland is the decrease in eHealth values in the overall period between 2010 and 2012: it has in fact recorded negative growth in 11 of 13 areas. Mostly the negative growth has been less than -15%; however the sharp increase in the area of “ePrescribing” (74% growth) and to a lesser extent “EAS for disaster recovery in less than 24 hours” (10% growth) have been enough to offset the losses in other categories. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 24: Finnish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
The two Finnish Private hospitals included score better than their Public counterparts in four of the five areas under examination; “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage” and “Clear and structured rules on access to clinical data”.

77
Figure 25: Finnish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
A scale advantage might be relevant when examining Finnish acute hospitals in terms of size. Hospitals which have in excess of 750 beds have perfect scores in four of five categories evaluated however hospitals between 101 and 250 beds have them only in a single category.
4. Composite indicators
The following section reports the results for Finland on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Finland´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Finland's eHealth Deployment indicator is based on data from 26 hospitals, while the Availability

78
and Use indicator was built from the information provided by 25 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Finland eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 12 hospitals) for Finland was 0.60, while the 2012 value was 0.62, which shows an increase of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Finland and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows only one hospital with low level of effective use while the others have scores in deployment and effective use considerable higher than the EU27+3 average
Figure 5: Finland's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Finland EU27+3
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Finland EU27+3

79
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report France

80
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals28, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners29.
This document reports the results of this project for France. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for France are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
7649 hospitals were identified in France. Within this rough universe 2461 (32%) completed the screener part of the questionnaire and 997 qualified as acute care hospitals. The size and ownership characteristics of these hospitals was very similar to the ones of the universe of acute Hospitals at EU27+3 level. Out of the French universe, 319 acute hospitals (32%) completed the survey.
Table 28: French sample breakdown by size of acute care hospitals
France N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 997
140 225 322 145 165
14% 23% 32% 15% 17%
2012 319 63 90 108 33 25
20% 28% 34% 10% 8%
2010 150 46 59 41 4 -
31% 39% 27% 3% -
28 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
29 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

81
Table 29: French sample breakdown by ownership type
France N= Public Private Private not for
profit Don't know/ No answer
Census 997
718 143 72 64
72% 14% 7% 6%
2012 319 241 44 32 2
76% 14% 10% 1%
2010 150 76 18 53 3
51% 12% 35% 2%
The final sample of hospitals included in the survey has a similar structure to the one of the French universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has more than doubled, with a large proportion of very large hospitals and of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI)with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

82
Figure 26: French acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 30: eHealth indicators France
eHealth indicators - France Valid N %
hospitals
2012 difference
France vs.EU27+3
France evolution,
2012 vs. 201030
Infrastructure
Externally connected 315 73% -3% -10%
Broadband > 50Mbps 299 14% -21% -29%
Single and unified wireless 316 67% 27% 19%
Single EPR shared by all departments 311 65% 8% -10%
Applications
PACS usage 314 46% -25% 21%
ePrescribing 310 41% -6% -20%
Integrated system for eReferral 310 29% -8% 6%
Tele-monitoring 312 13% 3% 5%
Integration Exchange of clinical care information with external providers
311 60% 4% 20%
Exchange of laboratory results with external providers
310 56% 5% 22%
Exchange of radiology reports with external providers
315 57% 1% 34%
Security Clear and structured rules on access to clinical data
310 81% -4% -8%
EAS for disaster recovery in less than 24 hours
313 43% -5% 5%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
30 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

83
Position of the French eHealth profile within EU27+3
France is slightly behind the European average of eHealth implementation. Despite this, there are no large outliers, with only two areas “Broadband > 50Mbps” and “PACS usage” registering differences in excess of -20%.. In the area of “Single and unified wireless” France scores significantly better than the European average, 27%t of difference.
Changes in the French eHealth profile
While France has generally increased its eHealth profile since 2010, the increase has not been very significant. This growth has come predominantly from four areas, “PACS usage”, “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers”, which all posted growth values in excess of 20%. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 27: French acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Ownership type does not appear to very important to the development of eHealth in French acute hospitals. For example, while Public and Private not for profit hospital categories lead in three of five categories each (, the lead values tend not to vary widely. For example, no hospital type leads its counterparts by more than 19% in any eHealth area.

84
Figure 28: French acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In contrast to ownership type (see above), when scale considerations are taken into account, we can see that a very definite advantage is enjoyed by French acute hospitals which have more than 750 beds. This category of hospital leads in all five areas examined, and additionally leads by significant margins in three of these categories (14% in “Broadband > 50Mbps”, 24% in “PACS usage” and 32% in “Exchange of clinical care information with external providers”). Even more significantly, the link between increased scale and greater eHealth capabilities is evident in all the categories, with smaller hospital segments recording progressively lower capabilities in each category under review.
4. Composite indicators
The following section reports the results for France on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information

85
Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in France´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. France's eHealth Deployment indicator is based on data from 312 hospitals, while the Availability and Use indicator was built from the information provided by 269 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: France eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 139 hospitals) for France was 0.37, while the 2012 value was 0.41, which shows an increase of 4% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for France and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that, as expected given that French average scores are very similar to the EU27+3 average, there are a similar number of hospitals with better scores (36%) than the EU27+3 average than with worse ones (30%).
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
France EU27+3

86
Figure 5: France's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals France EU27+3

87
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Germany

88
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals31, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners32.
This document reports the results of this project for Germany. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Germany are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
3847 hospitals were identified in Germany. Within this rough universe 2534 (61%) completed the screener part of the questionnaire and 1295 qualified as acute care hospitals The size and ownership characteristics of these hospitals was very similar to the ones of the universe of acute Hospitals at EU27+3 level. Out of the German universe, 201 acute hospitals (16%) completed the survey.
Table 31: German sample breakdown by size of acute care hospitals
Germany N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 1295
193 411 486 117 88
15% 32% 38% 9% 7%
2012 201 43 68 71 16 3
21% 34% 35% 8% 1%
2010 150 36 58 45 11 -
24% 39% 30% 7% -
31 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
32 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

89
Table 32: German sample breakdown by ownership type
Germany N= Public Private Private not for
profit Don't know/ No answer
Census 1295
387 357 373 178
30% 28% 29% 14%
2012 201 70 59 56 16
35% 29% 28% 8%
2010 150 90 33 26 1
60% 22% 17% 1%
The final sample of hospitals included in the survey has a similar structure to the one of the German universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has increased a 34%, with a lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

90
Figure 29: German acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 33: eHealth indicators Germany
eHealth indicators - Germany Valid N %
hospitals
2012 difference
Germany vs.EU27+3
Germany evolution,
2012 vs. 201033
Infrastructure
Externally connected 200 85% 8% -2%
Broadband > 50Mbps 183 31% -5% -10%
Single and unified wireless 196 27% -13% 4%
Single EPR shared by all departments 191 63% 6% 1%
Applications
PACS usage 201 77% 6% 13%
ePrescribing 194 9% -37% 3%
Integrated system for eReferral 194 23% -15% 13%
Tele-monitoring 193 4% -7% 2%
Integration Exchange of clinical care information with external providers
192 54% -2% 22%
Exchange of laboratory results with external providers
192 37% -14% 11%
Exchange of radiology reports with external providers
196 61% 6% 23%
Security Clear and structured rules on access to clinical data
195 91% 6% -5%
EAS for disaster recovery in less than 24 hours
194 55% 7% -6%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
33 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Germany 2010 (n=150) Germany 2012 (n=201)

91
Position of the German eHealth profile within EU27+3
Germany does not reach the European average in terms of eHealth adoption. The most notable lag occurs in the area of “ePrescribing” which is 37% behind the European average. In all other areas, the differences, both positive and negative, are less relevant. .
Changes in the German eHealth profile
Other than for “Exchange of clinical care information with external providers” and “Exchange of radiology reports with external providers” (which gained 22% and 23% respectively over the period under review), all gains have been marginal and lower than 15% in each category. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 30: German acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Public hospitals in Germany lead in two of the five areas investigated, namely “Broadband > 50Mbps” and “PACS usage”. Private acute hospitals, by contrast, underperform in all five areas, most notably in “Single EPR shared by all departments” where Private hospitals have only 47% penetration, a full 28 percentage points behind the lead value of 75%. Private not for profit acute hospitals lead in three areas, “Single EPR shared by all departments”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”.
32%
64%
86%
42%
91%
28%
47%
63%
53%
84%
24%
75%
75%
61%
98%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Public (n=65-70) Private (n=53-59) Private not for profit (n=50-56)

92
Figure 31: German acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In Germany, scale advantages can be observed across all eHealth indicators under review. In all five areas, “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”, acute hospitals over 750 beds in size led. For smaller size segments, the ranking is also commensurate with scale: the larger the hospital, the better it is equipped for eHealth (although in some cases the advantage was marginal).
4. Composite indicators
The following section reports the results for Germany on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information
15%
47%
49%
31%
80%
28%
62%
72%
57%
91%
29%
68%
86%
58%
94%
59%
71%
100%
64%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=26-35) Between 101 and 250 beds (n=63-69)
Between 251 and 750 beds (n=69-74) More than 750 beds (n=21-22)

93
Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Germany´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Germany's eHealth Deployment indicator is based on data from 188 hospitals, while the Availability and Use indicator was built from the information provided by 168 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Germany eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 148 hospitals) for Germany was 0.36, while the 2012 value was 0.40, which shows an increase of 4% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Germany and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a significant large group of hospitals (27%) with almost no Effective use at various levels of deployment. In contrast, an equal proportion of hospitals (27%) are above EU27+3 average in both indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Germany EU27+3

94
Figure 5: Germany's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Germany EU27+3

95
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Greece

96
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals34, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners35.
This document reports the results of this project for Greece. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Greece are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
687 hospitals were identified in Greece. Within this rough universe 398 (58%) completed the screener part of the questionnaire and 120 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (36% vs. 21%) and there were more hospitals of public ownership (80% vs. 64%). Out of the Greek universe, 68 acute hospitals (57%) completed the survey.
Table 34: Greek sample breakdown by size of acute care hospitals
Greece N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 120
32 28 25 3 32
27% 23% 21% 3% 27%
2012 68 18 16 18 2 14
26% 24% 26% 3% 21%
2010 26 5 11 7 3 -
19% 42% 27% 12% -
34 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
35 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

97
Table 35: Greek sample breakdown by ownership type
Greece N= Public Private Private not for
profit Don't know/ No answer
Census 120
85 20 1 14
71% 17% 1% 12%
2012 68 59 8 1 -
87% 12% 1% -
2010 26 24 1 1 -
92% 4% 4% -
The final sample of hospitals included in the survey has a similar structure to the one of the Greek universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with a lower proportion of very large (more than 750 beds) and intermediate (Between 101 and 250 beds) hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

98
Figure 32: Greek acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 36 – eHealth indicators Greece
eHealth indicators - Greece Valid N %
hospitals
2012 difference
Greece vs.EU27+3
Greece evolution,
2012 vs. 201036
Infrastructure
Externally connected 67 70% -6% -11%
Broadband > 50Mbps 61 11% -24% -8%
Single and unified wireless 68 12% -28% 8%
Single EPR shared by all departments 63 52% -5% -1%
Applications
PACS usage 65 32% -39% 9%
ePrescribing 68 94% 47% 44%
Integrated system for eReferral 68 71% 33% 40%
Tele-monitoring 62 2% -9% -3%
Integration Exchange of clinical care information with external providers
64 19% -37% 10%
Exchange of laboratory results with external providers
66 20% -32% 11%
Exchange of radiology reports with external providers
63 17% -38% 9%
Security Clear and structured rules on access to clinical data
61 67% -18% -9%
EAS for disaster recovery in less than 24 hours
64 34% -14% 14%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
36 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

99
Position of the Greek eHealth profile within EU27+3
Greece is behind the European average in terms of eHealth development. The areas which contribute the most to this lag are “PACS usage” (-39%), “Exchange of clinical care information with external providers” (-37%), “Exchange of laboratory results with external providers”, (-32%) and “Exchange of radiology reports with external providers” (-38%). Greece, however, exceeds the European average in “ePrescribing” (47%) and “Integrated system for eReferral” (33%).
Changes in the Greek eHealth profile
Despite lagging behind the European average, Greece has in fact made significant progress over its previous eHealth profile as evaluated in 2010. The country improvements are mainly due to the two areas in which it exceeds the average, “ePrescribing” and “Integrated system for eReferral. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 33: Greek acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Greece’s Public acute hospitals underperform in all areas examined and consistently rank equal to or behind the average values for all indicators. Private hospitals fare much better, exceeding the average value in all areas, sometimes by a wide margin, for example in “PACS usage”.
11%
50%
27%
14%
65%
14%
62%
75%
57%
75%
0
100%
0
0
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Public (n=52-56) Private (n=7-8) Private not for profit (n=1)

100
Figure 34: Greek acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Considering the scale of acute hospitals in Greece, the only hospital with more than 750 beds has good scores in the categories where data is available. However, the lack of representativeness prevents from any generalization. The results for the others categories do not show a clear relationship between size and performance in the indicators evaluated..
4. Composite indicators
The following section reports the results for Greece on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the
21%
50%
12%
7%
62%
6%
53%
35%
33%
56%
4%
50%
32%
12%
76%
100%
0
100%
0
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=14-17)Between 101 and 250 beds (n=16-19)Between 251 and 750 beds (n=21-26)

101
Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Greece´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Greece's eHealth Deployment indicator is based on data from 63 hospitals, while the Availability and Use indicator was built from the information provided by 59 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Greece eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 24 hospitals) for Greece was 0.25, while the 2012 value was 0.27, which shows an increase of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Greece and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a group of hospitals with no effective use at various (low) levels of deployment. Only 5 hospitals were above EU27+3 average for both composite indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Greece EU27+3

102
Figure 5: Greece's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Greece EU27+3

103
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Hungary

104
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals37, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners38.
This document reports the results of this project for Hungary. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Hungary are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
492 hospitals were identified in Hungary. Within this rough universe 279 (57%) completed the screener part of the questionnaire and 102 qualified as acute care hospitals. The proportion of hospitals with more than 750 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (25% vs. 12%) and there were more hospitals of public ownership (92% vs. 64%). Out of the Hungarian universe, 43 acute hospitals (42%) completed the survey.
Table 37: Hungarian sample breakdown by size of acute care hospitals
Hungary N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 102
15 20 34 23 10
15% 20% 33% 23% 10%
2012 43 6 7 17 8 5
14% 16% 40% 19% 12%
2010 10 - 2 7 1 -
- 20% 70% 10% -
37 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
38 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

105
Table 38: Hungarian sample breakdown by ownership type
Hungary N= Public Private Private not for
profit Don't know/ No answer
Census 102
90 7 1 4
88% 7% 1% 4%
2012 43 40 1 1 1
93% 2% 2% 2%
2010 10 9 - - 1
90% - - 10%
The final sample of hospitals included in the survey has a similar structure to the one of the Hungarian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has quadrupled, with a lower proportion of large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

106
Figure 35: Hungarian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 39 – eHealth indicators Hungary
eHealth indicators - Hungary Valid N %
hospitals
2012 difference
Hungary vs.EU27+3
Hungary evolution,
2012 vs. 201039
Infrastructure
Externally connected 43 63% -14% -27%
Broadband > 50Mbps 43 23% -12% 3%
Single and unified wireless 43 5% -35% -15%
Single EPR shared by all departments 43 86% 29% -4%
Applications
PACS usage 43 81% 11% 21%
ePrescribing 42 98% 51% 98%
Integrated system for eReferral 42 57% 19% 7%
Tele-monitoring 43 0% -10% -20%
Integration Exchange of clinical care information with external providers
43 40% -16% -16%
Exchange of laboratory results with external providers
42 62% 11% -5%
Exchange of radiology reports with external providers
43 40% -16% 0%
Security Clear and structured rules on access to clinical data
43 91% 5% 11%
EAS for disaster recovery in less than 24 hours
42 45% -3% -35%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
39 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Hungary 2010 (n=10) Hungary 2012 (n=43)

107
Position of the Hungarian eHealth profile within EU27+3
Hungary lies close to the European average in terms of its eHealth indicators. The areas with scores significantly higher than the European average were “Single EPR shared by all departments” (29%), “ePrescribing” (51%) and “Integrated system for eReferral” (19%). Leads in all other areas are relatively marginal
Changes in the Hungarian eHealth profile
The whole Hungary’s eHealth profile has not risen significantly since 2010. However growth has been uneven over the period under review with, of the 13 areas, 7 registering negative growth. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 36: Hungarian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
There were not enough hospitals belonging to the private (for profit and not for profit) category to allow the analysis by ownership to draw any relevant message.
25%
85%
80%
42%
90%
0
100%
100%
0
100%
0
100%
100%
0
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Public (n=40) Private (n=1) Private not for profit (n=1)

108
Figure 37: Hungarian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Scale does not appear have a clear influence on the results of eHealth progress in Hungarian acute hospitals. In two areas, “Single EPR shared by all departments” and “Clear and structured rules on access to clinical data”, although larger hospitals tend to have higher scores, this lead is not dramatic and overall values are closely grouped
4. Composite indicators
The following section reports the results for Hungary on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which
29%
86%
71%
14%
86%
0
80%
60%
20%
80%
21%
84%
79%
53%
95%
33%
89%
100%
56%
89%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=7)Between 101 and 250 beds (n=5)Between 251 and 750 beds (n=19)

109
all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Hungary´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Hungary's eHealth Deployment indicator is based on data from 41 hospitals, while the Availability and Use indicator was built from the information provided by 42 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Hungary eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 9 hospitals) for Hungary was 0.36, while the 2012 value was 0.33, which shows a negative growth of 3% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Hungary and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that, besides two hospitals with no effective use, hospitals with highest levels of deployment have as well higher levels of availability and of use.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Hungary EU27+3

110
Figure 5: Hungary's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Hungary EU27+3

111
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Iceland

112
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals40, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners41.
This document reports the results of this project for Iceland. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Iceland are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
14 hospitals were identified in Iceland. Within this rough universe 11 (79%) completed the screener part of the questionnaire and 10 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (78% vs. 21%) and all the hospitals were of public ownership compared with a 64% among the universe of acute Hospitals at EU27+3 level. Out of the Icelandic universe, 9 acute hospitals (90%) completed the survey.
Table 40: Icelandic sample breakdown by size of acute care hospitals
Iceland N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 10
7 1 1 - 1
70% 10% 10% - 10%
2012 9 7 1 1 - -
78% 11% 11% - -
2010 3 2 1 - - -
67% 33% - - -
40 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
41 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

113
Table 41: Icelandic sample breakdown by ownership type
Iceland N= Public Private Private not for
profit Don't know/ No answer
Census 10
9 - - 1
90% - - 10%
2012 9 9 - - -
100% - - -
2010 3 3 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Icelandic universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has tripled.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

114
Figure 38: Icelandic acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 42 – eHealth indicators Iceland
eHealth indicators - Iceland Valid N %
hospitals
2012 difference
Iceland vs.EU27+3
Iceland evolution,
2012 vs. 201042
Infrastructure
Externally connected 9 89% 13% -11%
Broadband > 50Mbps 8 50% 14% 50%
Single and unified wireless 9 22% -18% -11%
Single EPR shared by all departments 9 33% -24% -67%
Applications
PACS usage 9 100% 29% 33%
ePrescribing 9 67% 20% -33%
Integrated system for eReferral 9 78% 40% 11%
Tele-monitoring 8 13% 2% 13%
Integration Exchange of clinical care information with external providers
9 89% 34% 56%
Exchange of laboratory results with external providers
9 78% 27% 44%
Exchange of radiology reports with external providers
9 67% 12% 0%
Security Clear and structured rules on access to clinical data
9 78% -8% -22%
EAS for disaster recovery in less than 24 hours
7 86% 38% 52%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
42 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Iceland 2010 (n=3) Iceland 2012 (n=9)

115
Position of the Icelandic eHealth profile within EU27+3
Iceland noticeably scores better than the average EU27+3 as regards eHealth. The lead values are also well distributed, with an outperformance of around 12% to 27% for most indicators. The most successful Icelandic areas of eHealth appear to be “Integrated system for eReferral” (40%), “Exchange of clinical care information with external providers” (34%) and “EAS for disaster recovery in less than 24 hours” (38%). Additionally, only three indicators out of 13 posted a negative value: “Single and unified wireless”, “Single EPR shared by all departments” and “Clear and structured rules on access to clinical data” scoring -18%, -24% and -8% respectively.
Changes in the Icelandic eHealth profile
Iceland’s eHealth profile has grown significantly since 2010. The highest gains were posted in the areas of “Broadband > 50Mbps”, “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers” and “EAS for disaster recovery in less than 24 hours”, which all grew in excess of 50%. However, “Single EPR shared by all departments” dropped by 67% in the same period. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size of the hospitals.
Figure 2: Icelandic acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
There were not enough hospitals belonging to the size categories of between 101 and 250 beds and between 251 and 750 beds to allow the analysis by size to draw any relevant message.
33%
43%
100%
86%
86%
100%
0%
100%
100%
100%
100%
0%
100%
100%
0%
0% 20% 40% 60% 80% 100%
Broadband >50Mbps
Single EPR sharedby all departments
PACS usage
Echange of CCI withext. providers
Clear data accessrules
Fewer than 101 beds (n=6-7)
Between 101 and 250 beds (n=1)
Between 251 and 750 beds (n=1)

116
4. Composite indicators
The following section reports the results for Iceland on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Iceland´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Iceland's eHealth Deployment indicator is based on data from 8 hospitals, while the Availability and Use indicator was built from the information provided by 7 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 3: Iceland eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Iceland EU27+3

117
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 3 hospitals) for Iceland was 0.45, while the 2012 value was 0.55, which shows an increase of 10% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Iceland and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a clear positive relationship among Icelandic hospitals between level of deployment and of availability and use. Only 1 hospital was below EU27+3 average for both composite indicators.
Figure 4: Iceland's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Iceland EU27+3

118
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Ireland

119
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals43, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners44.
This document reports the results of this project for Ireland. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Ireland are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
492 hospitals were identified in Ireland. Within this rough universe 358 (73%) completed the screener part of the questionnaire and 42 qualified as acute care hospitals. The proportion of hospitals with less than 250 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (66% vs. 52%). Out of the Irish universe, 23 acute hospitals (55%) completed the survey.
Table 43: Irish sample breakdown by size of acute care hospitals
Ireland N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 42
6 20 13 - 3
14% 48% 31% - 7%
2012 23 5 11 7 - -
22% 48% 30% - -
2010 8 - 1 4 3 -
- 12% 50% 38% -
43 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
44 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

120
Table 44: Irish sample breakdown by ownership type
Ireland N= Public Private Private not for
profit Don't know/ No answer
Census 42
27 9 3 3
64% 21% 7% 7%
2012 23 16 6 1 -
70% 26% 4% -
2010 8 8 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Irish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with a significantly higher proportion of hospitals with less than 250 beds and non public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

121
Figure 39: Irish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 45 – eHealth indicators Ireland
eHealth indicators - Ireland Valid N %
hospitals
2012 difference
Ireland vs.EU27+3
Ireland evolution,
2012 vs. 201045
Infrastructure
Externally connected 23 74% -2% -14%
Broadband > 50Mbps 21 57% 22% -43%
Single and unified wireless 23 39% -1% -11%
Single EPR shared by all departments 23 30% -27% -7%
Applications
PACS usage 23 83% 12% 8%
ePrescribing 23 9% -38% 9%
Integrated system for eReferral 23 30% -7% -7%
Tele-monitoring 21 0% -10% -25%
Integration Exchange of clinical care information with external providers
23 78% 23% -9%
Exchange of laboratory results with external providers
23 70% 18% -18%
Exchange of radiology reports with external providers
23 65% 10% -10%
Security Clear and structured rules on access to clinical data
21 90% 5% -10%
EAS for disaster recovery in less than 24 hours
23 39% -9% -11%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
45 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Ireland 2010 (n=8) Ireland 2012 (n=23)

122
Position of the Irish eHealth profile within EU27+3
In 2012 Ireland was largely in line with the European average with respect to eHealth indicators. In 6 of them, Ireland scores higher than the average EU27+3 and worse in 7. Those with the highest negative differences are “eprescribing” (38%) and “Single EPR shared by all departments” (27%). The category “Exchange of clinical care information with external providers” is where positive differences are higher (23%).
Changes in the Irish eHealth profile
Ireland has made negative progress since 2010 as regards its eHealth profile. The largest drops occurred in the areas of “Broadband > 50Mbps” and “Tele-monitoring”, which registered drops of -43% and -25% respectively. Ireland has fallen in 11 of the 13 categories since 2010. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 40: Irish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Areas as “PACS usage” and “Single EPR shared by all departments” show important differences between Public and Private hospitals. However, it is not clear what type of hospitals performs better (as there is only one hospital belonging to the category not for profit, this category has not been considered)
53%
12%
88%
81%
93%
60%
67%
67%
67%
80%
100%
100%
100%
100%
100%
0% 50% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Exchange of clinical care informationwith external providers
Clear and structured rules on accessto clinical data
Public (n=15-16) Private (n=5-6) Private not for profit (n=1)

123
Figure 41: Irish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In terms of hospital size, Ireland returned no values for establishments with over 750 beds. The values reported tend to be roughly evenly grouped, although the medium-sized and larger hospital segments (between 101 and 250 beds, and from 251 beds to 750 beds) tend to lead in four of the five areas: “Broadband > 50Mbps”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”.
4. Composite indicators
The following section reports the results for Ireland on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that,
0
33%
33%
0
100%
70%
45%
91%
91%
91%
57%
0
88%
88%
86%
0 0.5 1
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Exchange of clinical care informationwith external providers
Clear and structured rules on access toclinical data
Fewer than 101 beds (n=2-3)Between 101 and 250 beds (n=10-11)Between 251 and 750 beds (n=7-8)

124
for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Ireland´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Ireland's eHealth Deployment indicator is based on data from 22 hospitals, while the Availability and Use indicator was built from the information provided by 19 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Ireland eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 7 hospitals) for Ireland was 0.65, while the 2012 value was 0.47, which shows a negative growth of 18% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Ireland and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows the low level of effective use, independently of the level of deployment, among all but 2 hospitals. These 2 hospitals were the only ones above EU27+3 average for both composite indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Ireland EU27+3

125
Figure 5: Ireland's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Ireland EU27+3

126
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Italy

127
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals46, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners47.
This document reports the results of this project for Italy. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Italy are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
2517 hospitals were identified in Italy. Within this rough universe 1063 (42%) completed the screener part of the questionnaire and 497 qualified as acute care hospitals. The proportion of public hospitals among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (75% vs 64%). Out of the Italian universe, 196 acute hospitals (39%) completed the survey.
Table 46: Italian sample breakdown by size of acute care hospitals
Italy N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 497
87 96 143 55 116
18% 19% 29% 11% 23%
2012 196 39 37 67 21 32
20% 19% 34% 11% 16%
2010 90 29 26 21 10 4
32% 29% 23% 11% 4%
46 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
47 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

128
Table 47: Italian sample breakdown by ownership type
Italy N= Public Private Private not for
profit Don't know/ No answer
Census 497
342 106 11 38
69% 21% 2% 8%
2012 196 136 51 9 -
69% 26% 5% -
2010 90 47 29 14 -
52% 32% 16% -
The final sample of hospitals included in the survey has a similar structure to the one of the Italian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has more than doubled, with a lower proportion of small and private hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

129
Figure 42: Italian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 48 – eHealth indicators Italy
eHealth indicators - Italy Valid N %
hospitals
2012 difference Italy
vs.EU27+3
Italy evolution, 2012
vs. 201048
Infrastructure
Externally connected 196 86% 9% 1%
Broadband > 50Mbps 187 39% 3% 6%
Single and unified wireless 194 36% -4% 12%
Single EPR shared by all departments 191 30% -27% -6%
Applications
PACS usage 196 86% 15% 11%
ePrescribing 188 53% 6% 34%
Integrated system for eReferral 188 37% -1% 9%
Tele-monitoring 191 18% 8% 1%
Integration Exchange of clinical care information with external providers
192 56% 1% 15%
Exchange of laboratory results with external providers
193 54% 3% 14%
Exchange of radiology reports with external providers
190 58% 3% 19%
Security Clear and structured rules on access to clinical data
190 86% 1% -2%
EAS for disaster recovery in less than 24 hours
192 47% -1% 1%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
48 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Italy 2010 (n=90) Italy 2012 (n=196)

130
Position of the Italian eHealth profile within EU27+3
Italy closely resembles the European average in eHealth. Of 13 areas considered, only one, “Single EPR shared by all departments”, showed a significant difference with the EU27+3 average (-27%). All other areas track the European average very closely, with only marginal discrepancies.
Changes in the Italian eHealth profile
Italy’s eHealth profile has progressed well from its 2010 position. In addition to this, the distribution has been relatively even, with only one of 13 areas posting a growth level in excess of 10%, being “ePrescribing” with a growth of 34%. All other growth areas were marginal, and of all areas examined, only two areas displayed negative growth, which was also marginal. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 43: Italian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Public acute hospitals in Italy appear to enjoy the best penetration of eHealth capabilities, leading in four of five areas. The distribution of eHealth capabilities also appears to be roughly similar across Private and Private not for profit acute hospitals, with Private hospitals slightly behind in terms of percentage penetration (taking last place in three areas of five: “Single EPR shared by all departments”, “PACS usage” and “Exchange of clinical care information with external providers”).
48%
31%
90%
66%
87%
19%
26%
75%
31%
86%
11%
33%
89%
44%
78%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Public (n=130-136) Private (n=46-51) Private not for profit (n=9)

131
Figure 44: Italian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
There appears to be a certain scale effect in Italian hospitals in relation to eHealth endowments, however it is not as clearly pronounced as in other European countries. For example, hospitals with fewer than 101 beds have worse results in all five areas considered, however at the larger end of the spectrum hospitals over 750 beds only lead in two of five categories (“Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”), as do hospitals with between 251 and 750 beds (“Broadband > 50Mbps” and “Single EPR shared by all departments”).
4. Composite indicators
The following section reports the results for Italy on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4
21%
21%
54%
38%
79%
33%
33%
98%
52%
86%
50%
36%
97%
58%
87%
43%
27%
89%
70%
88%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=33-35)
Between 101 and 250 beds (n=39-42)
Between 251 and 750 beds (n=58-61)
More than 750 beds (n=42-45)

132
categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Italy´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Italy's eHealth Deployment indicator is based on data from 189 hospitals, while the Availability and Use indicator was built from the information provided by 182 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Italy eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 84 hospitals) for Italy was 0.38, while the 2012 value was 0.45, which shows an increase of 7% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Italy and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a positive relationship among Italian hospitals between level of deployment and of availability and use. Nevertheless, there are also hospitals with low levels of deployment and relatively high levels of use and vice versa.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Italy EU27+3

133
Figure 5: Italy's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Italy EU27+3

134
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Latvia

135
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals49, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners50.
This document reports the results of this project for Latvia. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Latvia are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
138 hospitals were identified in Latvia. Within this rough universe 95 (69%) completed the screener part of the questionnaire and 32 qualified as acute care hospitals. The proportion of very large hospitals w among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (4% vs. 12%) and there were more hospitals of public ownership (88% vs. 64%). Out of the Latvian universe, 19 acute hospitals (59%) completed the survey.
Table 49: Latvian sample breakdown by size of acute care hospitals
Latvia N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 32
8 10 8 1 5
25% 31% 25% 3% 16%
2012 19 5 9 3 1 1
26% 47% 16% 5% 5%
2010 3 - 2 1 - -
- 67% 33% - -
49 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
50 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

136
Table 50: Latvian sample breakdown by ownership type
Latvia N= Public Private Private not for
profit Don't know/ No answer
Census 32
23 3 - 6
72% 9% - 19%
2012 19 16 1 - 2
84% 5% - 11%
2010 3 3 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Latvian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has increased considerably, with a lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

137
Figure 45: Latvian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 51 – eHealth indicators Latvia
eHealth indicators - Latvia Valid N %
hospitals
2012 difference
Latvia vs.EU27+3
Latvia evolution, 2012
vs. 201051
Infrastructure
Externally connected 19 84% 8% 18%
Broadband > 50Mbps 18 33% -2% 0%
Single and unified wireless 19 26% -14% 26%
Single EPR shared by all departments 16 75% 18% 8%
Applications
PACS usage 18 78% 7% 11%
ePrescribing 13 8% -39% 8%
Integrated system for eReferral 13 46% 8% 13%
Tele-monitoring 14 0% -10% 0%
Integration Exchange of clinical care information with external providers
13 62% 6% 28%
Exchange of laboratory results with external providers
13 38% -13% 5%
Exchange of radiology reports with external providers
14 100% 45% 67%
Security Clear and structured rules on access to clinical data
18 78% -8% -22%
EAS for disaster recovery in less than 24 hours
16 69% 21% 35%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
51 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Latvia 2010 (n=3) Latvia 2012 (n=19)

138
Position of the Latvian eHealth profile within EU27+3
Latvia experienced an uneven development, with results for the indicators “Exchange of radiology reports with external providers” and “EAS for disaster recovery in less than 24 hours” been higher than the EU27+3 mean by 45% and 21% respectively, while “ePrescribing” was 29% below the European average.
Changes in the Latvian eHealth profile
Latvia has made progress in its development of eHealth in acute hospitals. “Exchange of radiology reports with external providers” and “EAS for disaster recovery in less than 24 hours” accounted for the largest areas of growth at 67% and 35% respectively. Of the 13 areas examined, only one experienced negative growth and two recorded no variation in relation to the 2010 results. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 46: Latvian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
As the category of Private not for profit returned no values for Latvia and there was only one hospital in the Private category, it is not possible to analyse indicators results by hospital’s ownership.
33%
77%
80%
55%
73%
0
100%
100%
0
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Public (n=11-15) Private (n=1)

139
Figure 47: Latvian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In Latvia, acute hospitals of between 101 and 250 beds in size appear to have the highest penetration of eHealth capabilities, with four of five categories being led (or jointly led) by this segment. In two of these areas (“Single EPR shared by all departments” and “PACS usage”) hospitals with between 101 and 250 beds posted 100% values. Similarly, the largest hospitals with more than 750 beds also recorded full implementation in two areas (“Single EPR shared by all departments” and “Exchange of clinical care information with external providers”), but large hospitals have underperformed elsewhere, often by a wide margin. Nevertheless, these results should be taken with caution given the low number of hospitals in each category.
4. Composite indicators
The following section reports the results for Latvia on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator.
0
33%
75%
0
75%
50%
100%
100%
33%
83%
0
67%
67%
100%
67%
50%
100%
50%
100%
50%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=1-4)Between 101 and 250 beds (n=5-6)Between 251 and 750 beds (n=2-3)

140
Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Latvia´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Latvia's eHealth Deployment indicator is based on data from 9 hospitals, while the Availability and Use indicator was built from the information provided by 15 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Latvia eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 2 hospitals) for Latvia was 0.22, while the 2012 value was 0.32, which shows an increase of 10% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Latvia and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that only 1 hospital was above EU27+3 average for both composite indicators and another hospital had a high score in the use indicator despite its low score in the deployment indicator..
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Latvia EU27+3

141
Figure 5: Latvia's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Latvia EU27+3

142
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Lithuania

143
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals52, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners53.
This document reports the results of this project for Lithuania. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Lithuania are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
219 hospitals were identified in Lithuania. Within this rough universe 119 (54%) completed the screener part of the questionnaire and 63 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (30% vs. 21%) and there were more hospitals of public ownership (98% vs. 64%). Out of the Lithuanian universe, 32 acute hospitals (51%) completed the survey.
Table 52: Lithuanian sample breakdown by size of acute care hospitals
Lithuania N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 63
18 17 11 10 7
29% 27% 17% 16% 11%
2012 32 10 12 5 5 -
31% 38% 16% 16% -
2010 10 - 3 4 3 -
- 30% 40% 30% -
52 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
53 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

144
Table 53: Lithuanian sample breakdown by ownership type
Lithuania N= Public Private Private not for
profit Don't know/ No answer
Census 63
57 1 - 5
90% 2% - 8%
2012 32 32 - - -
100% - - -
2010 10 10 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Lithuanian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has tripled, with a lower proportion of very large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

145
Figure 48: Lithuanian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 54 – eHealth indicators Lithuania
eHealth indicators - Lithuania Valid N %
hospitals
2012 difference
Lithuania vs.EU27+3
Lithuania evolution,
2012 vs. 201054
Infrastructure
Externally connected 32 66% -11% -14%
Broadband > 50Mbps 31 45% 10% 15%
Single and unified wireless 32 13% -28% 13%
Single EPR shared by all departments 30 23% -34% 3%
Applications
PACS usage 32 69% -2% 9%
ePrescribing 27 15% -32% 15%
Integrated system for eReferral 27 33% -4% -7%
Tele-monitoring 23 0% -10% 0%
Integration Exchange of clinical care information with external providers
30 20% -35% 0%
Exchange of laboratory results with external providers
30 7% -45% -13%
Exchange of radiology reports with external providers
30 30% -25% 10%
Security Clear and structured rules on access to clinical data
30 63% -22% -27%
EAS for disaster recovery in less than 24 hours
31 19% -29% -41%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
54 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Lithuania 2010 (n=10) Lithuania 2012 (n=32)

146
Position of the Lithuanian eHealth profile within EU27+3
Lithuania is behind the European average in terms of eHealth, with lower values than the EU27+3 average in 12 of the 13 examined categories.. The two areas with the biggest differences were “Exchange of clinical care information with external providers” and “Exchange of laboratory results with external providers”, with -35% and -45% respectively.
Changes in the Lithuanian eHealth profile
Lithuania has seen a marginal decrease in its overall eHealth profile since 2010. The main contractions were observed in “Clear and structured rules on access to clinical data” and “EAS for disaster recovery in less than 24 hours”, which dropped by 27% and 41% respectively. In all other areas, the decline amounted to less than 15%, with some areas (“Tele-monitoring” and “Exchange of clinical care information with external providers”) recording no variation over the two-year period. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size of the hospitals (No comparison by ownership type can be carried out for Lithuania since only public hospitals returned data for the survey).
Figure 2: Lithuanian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Lithuanian hospitals with more than 750 beds score better than all other segments in all categories under review.. By contrast, acute hospitals with fewer than 101 beds have the lowest scores in three of the five categories.
12%
12%
33%
0
75%
46%
15%
77%
23%
62%
50%
33%
75%
25%
50%
100%
60%
100%
50%
75%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=8-9)Between 101 and 250 beds (n=13)Between 251 and 750 beds (n=3-4)

147
4. Composite indicators
The following section reports the results for Lithuania on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Lithuania´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Lithuania's eHealth Deployment indicator is based on data from 30 hospitals, while the Availability and Use indicator was built from the information provided by 32 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 3: Lithuania eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Lithuania EU27+3

148
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 10 hospitals) for Lithuania was 0.23, while the 2012 value was 0.30, which shows an increase of 7% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Lithuania and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a large group of hospitals with almost no Effective use at various levels of deployment. No hospital was above EU27+3 average for both composite indicators.
Figure 4: Lithuania's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Lithuania EU27+3

149
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Luxembourg

150
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals55, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners56.
This document reports the results of this project for Luxembourg. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Luxembourg are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
7 hospitals were identified in Luxembourg. Within this rough universe 7 (100%) completed the screener part of the questionnaire and all of them qualified as acute care hospitals. The proportion of hospitals with between 250-750 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (71% vs. 36%). Out of the Luxembourgish universe, 3 acute hospitals (43%) completed the survey.
Table 55: Luxembourgish sample breakdown by size of acute care hospitals
Luxembourg N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 7
2 - 5 - -
29% - 71% - -
2012 3 - - 3 - -
- - 100% - -
2010 3 1 - 2 - -
33% - 67% - -
55 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
56 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

151
Table 56: Luxembourgish sample breakdown by ownership type
Luxembourg N= Public Private Private not for
profit Don't know/ No answer
Census 7
4 - 3 -
57% - 43% -
2012 3 1 - 2 -
33% - 67% -
2010 3 2 1 - -
67% 33% - -
Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has remained the same, with a lower proportion of public hospitals than in 2010 and with no small hospitals.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours:

152
Figure 49: Luxembourgish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 57 – eHealth indicators Luxembourg
eHealth indicators - Luxembourg Valid N %
hospitals
2012 difference
Luxembourg
vs.EU27+3
Luxembourg evolution,
2012 vs. 201057
Infrastructure
Externally connected 3 100% 24% 0%
Broadband > 50Mbps 3 100% 64% 33%
Single and unified wireless 3 100% 60% 33%
Single EPR shared by all departments 3 33% -24% -67%
Applications
PACS usage 3 100% 29% 0%
ePrescribing 3 67% 20% 0%
Integrated system for eReferral 3 33% -4% 33%
Tele-monitoring 3 0% -10% 0%
Integration Exchange of clinical care information with external providers
2 50% -5% -17%
Exchange of laboratory results with external providers
3 67% 15% 0%
Exchange of radiology reports with external providers
3 100% 45% 33%
Security Clear and structured rules on access to clinical data
3 67% -19% -33%
EAS for disaster recovery in less than 24 hours
3 100% 52% 33%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
57 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Luxembourg 2010 (n=3) Luxembourg 2012 (n=3)

153
Position of the Luxembourgish eHealth profile within EU27+3
Luxembourg has an excellent eHealth profile compared to the European average. Values for “Broadband > 50Mbps” and “Single and unified wireless” were particularly strong, with significant leads over the EU27+3 average.
Changes in the Luxembourgish eHealth profile
Luxembourg’s overall eHealth profile has not changed considerably since 2010. “Single EPR shared by all departments” accounted for the most dramatic change, with a drop of 67% in relation to the 2010 position, while “Broadband >50Mbps”, “Single and unified wireless”, “Integrated system for eReferral”, “Exchange of radiology reports with external providers” and “EAS for disaster recovery in less than 24 hours” all posted gains of 33%. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Low number of hospitals included in the sample prevents from analyzing differences in the results by hospital characteristics as size and ownership.
4. Composite indicators
The following section reports the results for Luxembourg on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Luxembourg´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Luxembourg's eHealth Deployment indicator is based on data from 3 hospitals, while the Availability and Use indicator was built from the information provided by 3 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 2: Luxembourg eHealth Composite Indicators

154
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 3 hospitals) for Luxembourg was 0.45, while the 2012 value was 0.57, which shows an increase of 12% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Luxembourg and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that all hospitals (3) were above EU27+3 average for both composite indicators.
Figure 3: Luxembourg's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Luxembourg EU27+3
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Luxembourg EU27+3

155
European Hospital Survey: Benchmarking
deployment of e-Health services (2012–2013)
Country Report Malta

156
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals58, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners59.
This document reports the results of this project for Malta. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Malta are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
10 hospitals were identified in Malta. Within this rough universe 8 (80%) completed the screener part of the questionnaire and 3 qualified as acute care hospitals. Out of the Maltese universe, 2 acute hospitals (67%) completed the survey.
Table 58: Maltese sample breakdown by size of acute care hospitals
Malta N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 3
1 1 - 1 -
33% 33% - 33% -
2012 2 - 1 - 1 -
- 50% - 50% -
2010 3 2 - - 1 -
67% - - 33% -
58 This criteria was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
59 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

157
Table 59: Maltese sample breakdown by ownership type
Malta N= Public Private Private not for
profit Don't know/ No answer
Census 3
2 1 - -
67% 33% - -
2012 2 2 - - -
100% - - -
2010 3 2 1 - -
67% 33% - -
Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has decreased.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours:

158
Figure 50: Maltese acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 60 – eHealth indicators Malta
eHealth indicators - Malta Valid N %
hospitals
2012 difference
Malta vs.EU27+3
Malta evolution, 2012
vs. 201060
Infrastructure
Externally connected 2 50% -26% 17%
Broadband > 50Mbps 1 0% -36% -67%
Single and unified wireless 2 0% -40% -33%
Single EPR shared by all departments 2 50% -7% 50%
Applications
PACS usage 2 100% 29% 33%
ePrescribing 2 0% -47% 0%
Integrated system for eReferral 2 0% -38% -33%
Tele-monitoring 2 0% -10% 0%
Integration Exchange of clinical care information with external providers
1 100% 45% 67%
Exchange of laboratory results with external providers
1 100% 49% 67%
Exchange of radiology reports with external providers
2 100% 45% 67%
Security Clear and structured rules on access to clinical data
na na na na
EAS for disaster recovery in less than 24 hours
na na na na
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
60 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Malta 2010 (n=3) Malta 2012 (n=2)

159
Position of the Maltese eHealth profile within EU27+3
Malta trails the European average in eHealth, with significant discrepancies in four of the 13 areas examined. However, the low number of hospitals (2) included in the Maltese sample requires that these results should be taken with caution.
Changes in the Maltese eHealth profile
Since 2010, Malta has made progress on its eHealth profile. “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers” are the areas where the increase has been bigger. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years and the sample sizes are very small.
4. Composite indicators
The following section reports the results for Malta on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Malta´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Malta's eHealth Deployment indicator is based on data from only 1 hospital, as the Availability and Use indicator. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.

160
Figure 4: Malta eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 3 hospitals) for Malta was 0.31, while the 2012 value was 0.72, which shows an increase of 41% over the two year period. As mentioned before, 2012 result is based on data form only one hospital. Therefore, the finding on increase of deployment should be taken with caution. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Malta EU27+3

161
European Hospital Survey: Benchmarking
deployment of e-Health services (2012–2013)
Country Report The Netherlands

162
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals61, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners62.
This document reports the results of this project for the Netherlands. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for the Netherlands are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
606 hospitals were identified in the Netherlands. Within this rough universe 381 (63%) completed the screener part of the questionnaire and 114 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (9% vs. 21%) and there were more hospitals of public ownership (89% vs. 64%). Out of the Dutch universe, 26 acute hospitals (23%) completed the survey.
Table 61: Dutch sample breakdown by size of acute care hospitals
Netherlands N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 114
7 10 48 15 34
6% 9% 42% 13% 30%
2012 26 5 3 14 3 1
19% 12% 54% 12% 4%
2010 29 - 3 19 4 3
- 10% 66% 14% 10%
61
This criteria was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
62 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

163
Table 62: Dutch sample breakdown by ownership type
Netherlands N= Public Private Private not for
profit Don't know/ No answer
Census 114
85 4 6 19
75% 4% 5% 17%
2012 26 20 1 5 -
77% 4% 19% -
2010 29 27 1 - 1
93% 3% - 3%
The final sample of hospitals included in the survey has a similar structure to the one of the Dutch universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has decreased, with a lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

164
Figure 51: Dutch acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 63 – eHealth indicators The Netherlands
eHealth indicators - the
Netherlands Valid N
%
hospitals
2012 difference the
Netherlands
vs.EU27+3
the Netherlands
evolution, 2012 vs.
201063
Infrastructure
Externally connected 25 68% -8% -22%
Broadband > 50Mbps 26 81% 45% 10%
Single and unified wireless 26 58% 18% 13%
Single EPR shared by all departments 26 73% 16% 8%
Applications
PACS usage 26 92% 21% -4%
ePrescribing 25 72% 25% 24%
Integrated system for eReferral 25 68% 30% -15%
Tele-monitoring 26 35% 3% 68%
Integration Exchange of clinical care information with external providers
26 88% 33% 8%
Exchange of laboratory results with external providers
26 85% 33% 3%
Exchange of radiology reports with external providers
25 76% 21% -9%
Security Clear and structured rules on access to clinical data
26 88% 3% -12%
EAS for disaster recovery in less than 24 hours
25 72% 21% 8%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
63 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Netherlands 2010 (n=29) Netherlands 2012 (n=26)

165
Position of the Dutch eHealth profile within EU27+3
The Netherlands scores better than the European average eHealth profile by a wide margin, with “Broadband > 50Mbps” 45% in excess of the European average. This good performance is distributed evenly across all sectors, with only one indicator of the 13 under review scoring below the EU27+3 average (“Externally connected” at -8%)..
Changes in the Dutch eHealth profile
The Dutch eHealth profile has not changed significantly between 2010 and 2012. The single largest gain was realised in the area of “Tele-monitoring”, which increased by 68% over the period. By contrast, “Externally connected”, “PACS usage”, “Integrated system for eReferral”, “Exchange of radiology reports with external providers” and “Clear and structured rules on access to clinical data” all posted negative growth; however, with the exception of “Externally connected” these reductions did not exceed 15%. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 52: Dutch acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
When considering capabilities based on the ownership type of the hospital in question, in the Netherlands we can observe that both Private and Private not for profit hospitals lead in all five categories: “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”. Public hospitals, by contrast, lag behind in all these categories, being the gap larger for the indicator “Single EPR shared by all departments”.
Areas as “Broadband > 50Mbps”, “Exchange of clinical care information with external providers” and “PACS usage”) show important differences. between Public and Private hospitals. Looking across ownership types, Private hospitals appear to be generally better endowed with respect to eHealth facilities, with the exception of “Broadband > 50Mbps”, where Private hospitals lag behind Public hospitals
75%
70%
95%
90%
85%
100%
0
0
100%
100%
100%
100%
100%
80%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Public (n=20) Private (n=1) Private not for profit (n=5)

166
Figure 53: Dutch acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In terms of hospital size, eHealth performance in the Netherlands remains evenly distributed, with very high penetration rates being posted across most segments for “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”. However, in most categories, no data was returned for hospitals with fewer than 101 beds.
4. Composite indicators
The following section reports the results for the Netherlands on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
67%
0
0
0
0
50%
100%
100%
100%
100%
88%
100%
100%
100%
75%
100%
100%
100%
67%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=3) Between 101 and 250 beds (n=4)

167
The following graph displays the average values of these indicators in the Netherlands´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. the Netherlands's eHealth Deployment indicator is based on data from 25 hospitals, while the Availability and Use indicator was built from the information provided by 20 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: the Netherlands eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 23 hospitals) for the Netherlands was 0.60, while the 2012 value was 0.57, which shows a negative growth of 3% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for the Netherlands and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is large variability between hospitals in their level of effective use, even at similar levels of deployment. Only 1 hospital was below EU27+3 average for both composite indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Netherlands EU27+3

168
Figure 5: the Netherlands's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Netherlands EU27+3

169
European Hospital Survey: Benchmarking
deployment of e-Health services (2012–2013)
Country Report Norway

170
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals64, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners65.
This document reports the results of this project for Norway. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Norway are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
100 hospitals were identified in Norway. Within this rough universe 75 (75%) completed the screener part of the questionnaire and 28 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (48% vs. 21%) and there were more hospitals of public ownership (81% vs. 64%). Out of the Norwegian universe, 6 acute hospitals (21%) completed the survey.
Table 64: Norwegian sample breakdown by size of acute care hospitals
Norway N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 28
12 6 4 3 3
43% 21% 14% 11% 11%
2012 6 2 2 1 1 -
33% 33% 17% 17% -
2010 7 1 2 3 1 -
14% 29% 43% 14% -
64 This criteria was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
65 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

171
Table 65: Norwegian sample breakdown by ownership type
Norway N= Public Private Private not for
profit Don't know/ No answer
Census 28
21 4 1 2
75% 14% 4% 7%
2012 6 3 3 - -
50% 50% - -
2010 7 6 - 1 -
86% - 14% -
The final sample of hospitals included in the survey has a similar structure to the one of the Norwegian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has reduced, with a lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

172
Figure 54: Norwegian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 66 – eHealth indicators Norway
eHealth indicators - Norway Valid N %
hospitals
2012 difference
Norway vs.EU27+3
Norway evolution,
2012 vs. 201066
Infrastructure
Externally connected 6 100% 24% 0%
Broadband > 50Mbps 5 80% 44% -20%
Single and unified wireless 6 17% -23% -12%
Single EPR shared by all departments 6 67% 10% -19%
Applications
PACS usage 6 67% -4% -33%
ePrescribing 5 40% -7% 26%
Integrated system for eReferral 5 80% 42% 9%
Tele-monitoring 5 20% 10% 6%
Integration Exchange of clinical care information with external providers
6 50% -5% -36%
Exchange of laboratory results with external providers
6 67% 15% -33%
Exchange of radiology reports with external providers
6 67% 12% -19%
Security Clear and structured rules on access to clinical data
6 100% 15% 0%
EAS for disaster recovery in less than 24 hours
6 83% 35% 40%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
66 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

173
Position of the Norwegian eHealth profile within EU27+3
Norway noticeably scores better than the average EU27+3 in in the areas of “Broadband > 50Mbps” and “Integrated system for eReferral”. The country is slightly behind in terms of “Single and unified wireless”, “PACS usage”, “ePrescribing” and “Exchange of clinical care information with external providers”.
Changes in the Norwegian eHealth profile
Norway’s eHealth profile has declined in relation to 2010, with nine of 13 areas posting zero growth or negative growth in 2012. This reduction was fairly evenly distributed, with the largest decreases registered in “PACS usage”, “Exchange of clinical care information with external providers” and “Exchange of laboratory results with external providers”. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 55: Norwegian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Although Private not for profit hospitals did not return any results for Norway, a clear comparison can still be made between Public and Private hospitals in terms of eHealth capabilities. Public hospitals in Norway recorded full implementation in all five areas under scrutiny and outperformed Private hospitals by a wide margin in the areas of “Broadband > 50Mbps”, “Single EPR shared by all departments” and “PACS usage”.

174
Figure 56: Norwegian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
The largest hospitals in Norway by scale (Between 251 and 750 beds and More than 750 beds) appear to enjoy a distinct advantage over the smaller categories of acute hospitals. Larger hospitals led in five of five examined areas, and in four categories enjoyed a 50 percentage point lead over their smaller counterparts. These categories were “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage” and “Exchange of clinical care information with external providers”.
4. Composite indicators
The following section reports the results for Norway on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information

175
Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Norway´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Norway's eHealth Deployment indicator is based on data from 4 hospitals, while the Availability and Use indicator was built from the information provided by 5 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Norway eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 7 hospitals) for Norway was 0.64, while the 2012 value was 0.53, which shows a negative growth of 11% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators (only 3 ), it is possible to map these individual values on a graph and compare them with the average value for Norway and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a significant difference in the score of the indicators between one hospital and the other 2 with completed data.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Norway EU27+3

176
Figure 5: Norway's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Norway EU27+3

177
European Hospital Survey: Benchmarking
deployment of e-Health services (2012–2013)
Country Report Poland

178
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals67, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners68.
This document reports the results of this project for Poland. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Poland are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
2411 hospitals were identified in Poland. Within this rough universe 1110 (46%) completed the screener part of the questionnaire and 459 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was lower compared to the universe of acute Hospitals at EU27+3 level (16% vs. 21%) and there were more hospitals of public ownership (81% vs. 64%). Out of the Polish universe, 149 acute hospitals (32%) completed the survey.
Table 67: Polish sample breakdown by size of acute care hospitals
Poland N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 459
67 157 180 26 29
15% 34% 39% 6% 6%
2012 149 18 65 54 9 3
12% 44% 36% 6% 2%
2010 99 21 34 36 3 5
21% 34% 36% 3% 5%
67 This criteria was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
68 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

179
Table 68: Polish sample breakdown by ownership type
Poland N= Public Private Private not for
profit Don't know/ No answer
Census 459
349 69 13 28
76% 15% 3% 6%
2012 149 118 22 7 2
79% 15% 5% 1%
2010 99 85 12 - 2
86% 12% - 2%
The final sample of hospitals included in the survey has a similar structure to the one of the Polish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has increased a 50%, with a lower proportion of very small hospitals (less than 100 beds) than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

180
Figure 57: Polish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 69 – eHealth indicators Poland
eHealth indicators - Poland Valid N %
hospitals
2012 difference
Poland vs.EU27+3
Poland evolution,
2012 vs. 201069
Infrastructure
Externally connected 149 56% -21% 30%
Broadband > 50Mbps 146 11% -25% -5%
Single and unified wireless 147 12% -28% 6%
Single EPR shared by all departments 144 50% -7% -4%
Applications
PACS usage 148 68% -3% 18%
ePrescribing 106 25% -22% 13%
Integrated system for eReferral 106 29% -9% 5%
Tele-monitoring 117 4% -6% -1%
Integration Exchange of clinical care information with external providers
142 25% -30% 8%
Exchange of laboratory results with external providers
146 23% -29% 14%
Exchange of radiology reports with external providers
145 35% -20% 21%
Security Clear and structured rules on access to clinical data
146 76% -9% -14%
EAS for disaster recovery in less than 24 hours
142 32% -16% -41%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
69 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.

181
Position of the Polish eHealth profile within EU27+3
Poland is universally behind the European average in eHealth, with all areas under review behind the corresponding average value. The country’s lag was evenly distributed across all 13 sectors and the difference did not exceed 30% in all sectors.
Changes in the Polish eHealth profile
Despite falling far behind the European average, Poland’s eHealth profile has improved somewhat. However, the changes have been broadly spread out across the 13 areas, with the two largest movers (“Externally connected” and “EAS for disaster recovery in less than 24 hours”) posting a 30% and a -41% difference since then. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 58: Polish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
There are no clear discrepancies in terms of eHealth capabilities in Polish acute hospitals when ownership characteristics are taken into account. Private not for profit acute hospitals score highly in two specific areas (“Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”), but either scored worse or did not return values for the other areas under review. Public hospitals, by contrast, led in only two areas (“PACS usage” and “Broadband > 50Mbps”), although this advantage was only marginal.
12%
48%
70%
25%
75%
9%
64%
59%
19%
77%
0
43%
57%
43%
86%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Public (n=112-117) Private (n=21-22) Private not for profit (n=7)

182
Figure 59: Polish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
The scale of Polish acute hospitals does appear to be a significant factor in the development of eHealth capabilities, both in terms of leadership and extent of leadership. In all five categories examined, hospitals with between 251 and 750 beds and with more than 750 beds outperformed hospitals of lesser scale. In addition, this advantage was often significant, as can be seen in “Broadband > 50Mbps”, “Single EPR shared by all departments” and “PACS usage”.
4. Composite indicators
The following section reports the results for Poland on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which
6%
28%
28%
22%
56%
2%
45%
66%
20%
70%
18%
65%
79%
32%
89%
50%
50%
88%
38%
75%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=17-18) Between 101 and 250 beds (n=60-63)
Between 251 and 750 beds (n=53-57) More than 750 beds (n=8)

183
all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Poland´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Poland's eHealth Deployment indicator is based on data from 129 hospitals, while the Availability and Use indicator was built from the information provided by 146 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Poland eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 98 hospitals) for Poland was 0.23, while the 2012 value was 0.25, which shows an increase of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Poland and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a large group of hospitals with almost no Effective use at various levels of deployment. Only 9 hospitals were above EU27+3 average for both composite indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Poland EU27+3

184
Figure 5: Poland's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Poland EU27+3

185
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Portugal

186
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals70, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners71.
This document reports the results of this project for Portugal. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Portugal are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
589 hospitals were identified in Portugal. Within this rough universe 224 (38%) completed the screener part of the questionnaire and 73 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (45% vs. 21%) and there were less hospitals of public ownership (55% vs. 64%). Out of the Portuguese universe, 41 acute hospitals (56%) completed the survey.
Table 70: Portuguese sample breakdown by size of acute care hospitals
Portugal N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 73
21 16 7 3 26
29% 22% 10% 4% 36%
2012 41 13 11 6 3 8
32% 27% 15% 7% 20%
2010 20 7 5 7 1 -
35% 25% 35% 5% -
70 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did
not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
71 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

187
Table 71: Portuguese sample breakdown by ownership type
Portugal N= Public Private Private not for
profit Don't know/ No answer
Census 73
34 20 8 11
47% 27% 11% 15%
2012 41 24 13 4 -
59% 32% 10% -
2010 20 13 2 5 -
65% 10% 25% -
The final sample of hospitals included in the survey has a similar structure to the one of the Portuguese universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has doubled, with similar characteristics than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

188
Figure 60: Portuguese acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 72 – eHealth indicators Portugal
eHealth indicators - Portugal Valid N %
hospitals
2012 difference
Portugal vs.EU27+3
Portugal evolution,
2012 vs. 201072
Infrastructure
Externally connected 40 85% 9% 5%
Broadband > 50Mbps 38 66% 30% 31%
Single and unified wireless 40 50% 10% 25%
Single EPR shared by all departments 40 63% 6% -28%
Applications
PACS usage 41 83% 12% -12%
ePrescribing 40 95% 48% 15%
Integrated system for eReferral 40 15% -23% -40%
Tele-monitoring 37 5% -5% 0%
Integration Exchange of clinical care information with external providers
39 67% 11% 17%
Exchange of laboratory results with external providers
40 48% -4% 28%
Exchange of radiology reports with external providers
39 54% -1% 19%
Security Clear and structured rules on access to clinical data
38 84% -1% 0%
EAS for disaster recovery in less than 24 hours
39 31% -17% -22%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
72 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Portugal 2010 (n=20) Portugal 2012 (n=41)

189
Position of the Portuguese eHealth profile within EU27+3
Portugal is close to the European average in its eHealth profile. However, the gains over and above the European average are not evenly distributed, with “ePrescribing” alone standing 48% above the EU27+3 average. Similarly, “Broadband > 50Mbps” was 30% above the average, with most other areas varying by less than 15%.
Changes in the Portuguese eHealth profile
The greatest gains since 2010 have been achieved in “Broadband > 50Mbps”, “Exchange of laboratory results with external providers” and “Single and unified wireless” which delivered 31%, 28% and 25% growth respectively. However, “Single EPR shared by all departments” and “Integrated system for eReferral” posted negative growth, at -28% and -40% respectively. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 61: Portuguese acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Public acute hospitals in Portugal appear to be the best endowed in terms of eHealth capabilities, with Public hospitals leading by a wide margin in three areas: “Broadband > 50Mbps”, “PACS usage” and “Exchange of clinical care information with external providers”. However, Private not for profit acute hospitals led notably in “Single EPR shared by all departments”, while Private hospitals led in “Clear and structured rules on access to clinical data”.
86%
50%
92%
87%
77%
50%
77%
77%
33%
100%
0
100%
50%
50%
67%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Public (n=22-24) Private (n=12-13) Private not for profit (n=3-4)

190
Figure 62: Portuguese acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
The distribution of eHealth capabilities appears to be relatively even in terms of hospital size. Although the largest hospital segments (Between 251 and 750 beds, as well as More than 750 beds) have leadership positions in “Broadband > 50Mbps”, “PACS usage” and “Exchange of clinical care information with external providers”, smaller hospitals lead in “Clear and structured rules on access to clinical data” as well as “Single EPR shared by all departments”. Significantly, the smallest segment (Fewer than 101 beds) underperformed in three of the five categories by a wide margin.
4. Composite indicators
The following section reports the results for Portugal on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which
40%
78%
50%
40%
89%
58%
80%
93%
57%
85%
90%
30%
100%
100%
80%
75%
50%
100%
75%
75%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Echange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=9-10) Between 101 and 250 beds (n=12-15)
Between 251 and 750 beds (n=10) More than 750 beds (n=4)

191
all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Portugal´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Portugal's eHealth Deployment indicator is based on data from 39 hospitals, while the Availability and Use indicator was built from the information provided by 34 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Portugal eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 11 hospitals) for Portugal was 0.44, while the 2012 value was 0.40, which shows a negative growth of 4% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Portugal and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is large variability between Portuguese hospitals and that it seems that there is a clear relationship between levels of deployment and levels of use.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Portugal EU27+3

192
Figure 5: Portugal's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Portugal EU27+3

193
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Romania

194
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals73, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners74.
This document reports the results of this project for Romania. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Romania are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
1042 hospitals were identified in Romania. Within this rough universe 612 (59%) completed the screener part of the questionnaire and 166 qualified as acute care hospitals. There were more hospitals of public ownership (96% vs. 64%) compared to the universe of acute Hospitals at EU27+3 level. Out of the Romanian universe, 85 acute hospitals (51%) completed the survey.
Table 73: Romanian sample breakdown by size of acute care hospitals
Romania N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 166
31 53 49 29 4
19% 32% 30% 17% 2%
2012 85 15 27 28 15 -
18% 32% 33% 18% -
2010 38 8 13 10 6 1
21% 34% 26% 16% 3%
73 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
74 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

195
Table 74: Romanian sample breakdown by ownership type
Romania N= Public Private Private not for
profit Don't know/ No answer
Census 166
157 7 - 2
95% 4% - 1%
2012 85 82 3 - -
96% 4% - -
2010 38 37 - - 1
97% - - 3%
The final sample of hospitals included in the survey has a similar structure to the one of the Romanian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has more than doubled, with similar hospital’s characteristics than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

196
Figure 63: Romanian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 75 – eHealth indicators Romania
eHealth indicators - Romania Valid N %
hospitals
2012 difference
Romania vs.EU27+3
Romania evolution,
2012 vs. 201075
Infrastructure
Externally connected 85 84% 7% 15%
Broadband > 50Mbps 74 35% 0% 9%
Single and unified wireless 85 13% -27% 2%
Single EPR shared by all departments 82 61% 4% 8%
Applications
PACS usage 83 23% -48% -14%
ePrescribing 81 88% 41% 85%
Integrated system for eReferral 81 17% -20% -10%
Tele-monitoring 64 2% -9% -1%
Integration Exchange of clinical care information with external providers
83 28% -28% 3%
Exchange of laboratory results with external providers
82 26% -26% 6%
Exchange of radiology reports with external providers
82 18% -37% 2%
Security Clear and structured rules on access to clinical data
80 78% -8% 6%
EAS for disaster recovery in less than 24 hours
81 30% -19% -19%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
75 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Romania 2010 (n=38) Romania 2012 (n=85)

197
Position of the Romanian eHealth profile within EU27+3
Romania scores worse than the average EU27+3 in eHealth. Five areas in particular are responsible for the majority of this lag: “Single and unified wireless”, “PACS usage”, “Exchange of clinical care information with external providers”, “Exchange of laboratory results with external providers” and “Exchange of radiology reports with external providers”. However, the country performs well in “ePrescribing”.
Changes in the Romanian eHealth profile
Despite its poor profile by contrast to the European average, Romania’s eHealth profile is improving. However, this growth has been uneven. The largest growth was recorded in the area of “ePrescribing” while all other areas have registered less significant changes, both positive and negative. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 64: Romanian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
When looking at the ownership type of Romanian acute hospitals, we can see the private acute hospital sector is far better performing in the areas of “Broadband > 50Mbps”, “Single EPR shared by all departments”, “PACS usage”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”. However, only 3 hospitals were of private ownership.
34%
61%
21%
26%
77%
67%
67%
67%
67%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Public (n=71-80) Private (n=3)

198
Figure 65: Romanian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In terms of hospital size, the very largest segment (More than 750 beds) registered much better performance than the smaller hospitals, with leading values in four of the five categories under review. Unusually, however, the worst performing category is not the smallest segment (Fewer than 101 beds) but the next largest segment of Between 101 and 250 beds.
4. Composite indicators
The following section reports the results for Romania on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
30%
64%
18%
27%
80%
24%
50%
12%
20%
67%
46%
54%
24%
21%
82%
35%
84%
37%
50%
83%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Exchange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=10-11) Between 101 and 250 beds (n=21-25)
Between 251 and 750 beds (n=26-29) More than 750 beds (n=17-19)

199
The following graph displays the average values of these indicators in Romania´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Romania's eHealth Deployment indicator is based on data from 82 hospitals, while the Availability and Use indicator was built from the information provided by 78 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Romania eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 11 hospitals) for Romania was 0.27, while the 2012 value was 0.34, which shows an increase of 7% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Romania and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a large group of hospitals with almost no Effective use at various levels of deployment. It also shows that almost 15% of the hospitals were above EU27+3 average for both composite indicators while 65% of them were below average for both indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Romania EU27+3

200
Figure 5: Romania's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Romania EU27+3

201
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Slovakia

202
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals76, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners77.
This document reports the results of this project for Slovakia. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Slovakia are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
391 hospitals were identified in Slovakia. Within this rough universe 187 (48%) completed the screener part of the questionnaire and 72 qualified as acute care hospitals. The size and type of ownership of these hospitals were similar than those of the universe of acute Hospitals at EU27+3 level. Out of the Slovakian universe, 33 acute hospitals (46%) completed the survey.
Table 76: Slovakian sample breakdown by size of acute care hospitals
Slovakia N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 72
11 19 30 5 7
15% 26% 42% 7% 10%
2012 33 6 10 14 3 -
18% 30% 42% 9% -
2010 12 4 4 1 2 1
33% 33% 8% 17% 8%
76 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
77 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

203
Table 77: Slovakian sample breakdown by ownership type
Slovakia N= Public Private Private not for
profit Don't know/ No answer
Census 72
43 14 9 6
60% 19% 13% 8%
2012 33 22 8 3 -
67% 24% 9% -
2010 12 3 2 6 1
25% 17% 50% 8%
The final sample of hospitals included in the survey has a similar structure to the one of the Slovakian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost tripled, with a higher proportion of public and big (more than 250 beds) hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

204
Figure 66: Slovakian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 78 – eHealth indicators Slovakia
eHealth indicators - Slovakia Valid N %
hospitals
2012 difference
Slovakia vs.EU27+3
Slovakia evolution,
2012 vs. 201078
Infrastructure
Externally connected 33 42% -34% 33%
Broadband > 50Mbps 33 36% 0% 1%
Single and unified wireless 30 20% -5% 3%
Single EPR shared by all departments 33 82% 6% 0%
Applications
PACS usage 33 79% 2% 7%
ePrescribing 27 26% -5% 4%
Integrated system for eReferral 27 19% -5% -2%
Tele-monitoring 33 0% -3% -4%
Integration Exchange of clinical care information with external providers
32 22% -8% -1%
Exchange of laboratory results with external providers
32 53% 0% 3%
Exchange of radiology reports with external providers
33 52% -1% 0%
Security Clear and structured rules on access to clinical data
33 85% 0% -4%
EAS for disaster recovery in less than 24 hours
32 59% 3% 5%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
78 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Slovakia 2010 (n=12) Slovakia 2012 (n=33)

205
Position of the Slovakian eHealth profile within EU27+3
Slovakia trails behind the European average in eHealth. Four specific areas account for most of this lag: “Externally connected”, “Single and unified wireless”, “ePrescribing” and “Exchange of clinical care information with external providers”. However, Slovakia is not universally behind the European average in all areas, with five of the 13 areas very close to or exceeding the European average.
Changes in the Slovakian eHealth profile
Although it is still behind the European average, Slovakia has improved on its 2010 eHealth profile. The major areas of increase were “Externally connected” and “PACS usage”, which had gains of 133% and 7% respectively. “EAS for disaster recovery in less than 24 hours” also improved. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 67: Slovakian acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Type of ownership does not appear to affect eHealth capabilities in any definite way in Slovakia, with both Private not for profit and Public hospitals leading in various different areas. While Private hospitals score better than public ones in four of five areas, the disparity in performance levels in three of these areas is not very high.
41%
86%
91%
23%
82%
38%
62%
50%
12%
88%
0
100%
67%
50%
100%
0% 50% 100%
Broadband > 50Mbps
Single EPR shared byall departments
PACS usage
Exchange of CCI withext. providers
Clear data accessrules
Public (n=22) Private (n=8) Private not for profit (n=2-3)

206
Figure 68: Slovakian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Scale does not appear to be a definite factor either in deciding the eHealth development of acute hospitals in Slovakia. While the largest hospitals have a clear advantage in two areas, “Broadband > 50Mbps” and “Exchange of clinical care information with external providers”, acute hospitals in the segment of Between 101 and 250 beds perform at 100% levels in two areas; “Single EPR shared by all departments” and “PACS usage”. Hospitals of all sizes perform well in the final category, “Clear and structured rules on access to clinical data”, and in this area, the maximum variation between results is not very high between the lowest and highest performers. By contrast, greater disparity in performance can be seen in “Broadband > 50Mbps”, “PACS usage” and “Exchange of clinical care information with external providers”.
4. Composite indicators
The following section reports the results for Slovakia on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the
29%
57%
43%
29%
86%
33%
100%
100%
20%
83%
36%
86%
86%
14%
93%
75%
75%
100%
50%
75%
0% 50% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI withext. providers
Clear data access rules
Fewer than 101 beds (n=7)Between 101 and 250 beds (n=5-6)Between 251 and 750 beds (n=14)

207
level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Slovakia´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Slovakia's eHealth Deployment indicator is based on data from 33 hospitals, while the Availability and Use indicator was built from the information provided by 32 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Slovakia eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 9 hospitals) for Slovakia was 0.22, while the 2012 value was 0.31, which shows an increase of 9% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Slovakia and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a group of 7 hospitals with almost no Effective use at various levels of deployment. 5 hospitals were above EU27+3 average for both composite indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Slovakia EU27+3

208
Figure 5: Slovakia's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Slovakia EU27+3

209
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Slovenia

210
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals79, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners80.
This document reports the results of this project for Slovenia. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Slovenia are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
186 hospitals were identified in Slovenia. Within this rough universe 104 (56%) completed the screener part of the questionnaire and 14 qualified as acute care hospitals. The proportion of hospitals of public ownership among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (92% vs. 64%). Out of the Slovenian universe, 6 acute hospitals (53%) completed the survey.
Table 79: Slovenian sample breakdown by size of acute care hospitals
Slovenia N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 14
2 5 2 3 2
14% 36% 14% 21% 14%
2012 6 - 3 2 1 -
- 50% 33% 17% -
2010 3 1 1 1 - -
33% 33% 33% - -
79 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
80 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

211
Table 80: Slovenian sample breakdown by ownership type
Slovenia N= Public Private Private not for
profit Don't know/ No answer
Census 14
12 1 - 1
86% 7% - 7%
2012 6 6 - - -
100% - - -
2010 3 3 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Slovenian universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has doubled, with a lower proportion of very large hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

212
Figure 69: Slovenian acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 81 – eHealth indicators Slovenia
eHealth indicators - Slovenia Valid N %
hospitals
2012 difference
Slovenia vs.EU27+3
Slovenia evolution,
2012 vs. 201081
Infrastructure Externally connected 6 83% 7% 17%
Broadband > 50Mbps 6 50% 14% 17%
Single and unified wireless 6 50% 10% 17%
Single EPR shared by all departments 6 33% -24% -33%
Applications PACS usage 6 50% -21% 17%
ePrescribing 5 0% -47% 0%
Integrated system for eReferral 5 0% -38% 0%
Tele-monitoring 6 0% -10% 0%
Integration Exchange of clinical care information with external providers
5 0% -55% -33%
Exchange of laboratory results with external providers
6 50% -1% 17%
Exchange of radiology reports with external providers
6 17% -38% -17%
Security Clear and structured rules on access to clinical data
62 92% 7% -1%
EAS for disaster recovery in less than 24 hours
60 45% -3% -19%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
81 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Slovenia 2010 (n=3) Slovenia 2012 (n=6)

213
Position of the Slovenian eHealth profile within EU27+3
Slovenia scores worse than the average EU27+3 in in many areas; with the biggest disparities evident in “ePrescribing”, “Integrated system for eReferral”, “Exchange of clinical care information with external providers” and “Exchange of radiology reports with external providers”.
Changes in the Slovenian eHealth profile
Slovenia’s eHealth profile has changed marginally since 2010. Six areas have improved slightly, while four areas have dropped in value, being “Single EPR shared by all departments” and “Exchange of clinical care information with external providers” the categories where the decrease in scores is higher. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals. However, as only public hospitals recorded values in relation to ownership type, no contrast is possible between other ownership types in Slovenia.
Figure 2: Slovenian acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
In relation to the size of hospitals , the low number of hospitals pertaining to each size category do not allow us to extract clear conclusions.
4. Composite indicators
The following section reports the results for Slovenia on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level
33%
33%
0
0
100%
50%
50%
100%
0
50%
100%
0
100%
0
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Between 101 and 250 beds (n=2-3)
Between 251 and 750 beds (n=2)

214
of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Slovenia´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Slovenia's eHealth Deployment indicator is based on data from 6 hospitals, while the Availability and Use indicator was built from the information provided as well by 6 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 3: Slovenia eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 3 hospitals) for Slovenia was 0.18, while the 2012 value was 0.28, which shows an increase of 10% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Slovenia and with the average value of
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Slovenia EU27+3

215
the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there are 3 hospitals (50% of the sample) with almost no Effective use, the three of them with similar levels of deployment. No hospital was above EU27+3 average for both composite indicators.
Figure 4: Slovenia's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Slovenia EU27+3

216
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Spain

217
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals82, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners83.
This document reports the results of this project for Spain. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Spain are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
1311 hospitals were identified in Spain. Within this rough universe 845 (64%) completed the screener part of the questionnaire and 478 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (35% vs. 21%) and there were less hospitals of public ownership (52% vs. 64%). Out of the Spanish universe, 124 acute hospitals (26%) completed the survey.
Table 82: Spanish sample breakdown by size of acute care hospitals
Spain N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 478
121 127 70 32 128
25% 27% 15% 7% 27%
2012 124 30 36 19 6 33
24% 29% 15% 5% 27%
2010 90 19 27 26 16 2
21% 30% 29% 18% 2%
82 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
83 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

218
Table 83: Spanish sample breakdown by ownership type
Spain N= Public Private Private not for
profit Don't know/ No answer
Census 478
225 157 50 46
47% 33% 10% 10%
2012 124 67 44 13 -
54% 35% 10% -
2010 90 62 16 11 1
69% 18% 12% 1%
The final sample of hospitals included in the survey has a similar structure to the one of the Spanish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has increased almost a 50%, with a lower proportion of public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

219
Figure 70: Spanish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 84: eHealth indicators Spain
eHealth indicators - Spain Valid N %
hospitals
2012 difference
Spain vs.EU27+3
Spain evolution, 2012
vs. 201084
Infrastructure Externally connected 123 89% 12% -5%
Broadband > 50Mbps 118 54% 19% 0%
Single and unified wireless 122 55% 15% 15%
Single EPR shared by all departments 121 50% -7% -28%
Applications PACS usage 123 93% 23% 10%
ePrescribing 122 68% 21% 19%
Integrated system for eReferral 122 23% -15% -24%
Tele-monitoring 123 22% 12% 7%
Integration Exchange of clinical care information with external providers
118 71% 16% -1%
Exchange of laboratory results with external providers
117 58% 7% -8%
Exchange of radiology reports with external providers
121 64% 9% 0%
Security Clear and structured rules on access to clinical data
123 94% 9% -1%
EAS for disaster recovery in less than 24 hours
122 66% 17% 5%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
84 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Spain 2010 (n=90) Spain 2012 (n=124)

220
Position of the Spanish eHealth profile within EU27+3
Spain is comfortably ahead of the European average in eHealth. For example, “PACS usage” and “ePrescribing” recorded scores of 20% or more above the European average (“PACS usage” is 23% above and “ePrescribing” is 21% above)
Changes in the Spanish eHealth profile
Despite being ahead of the EU average, Spain’s eHealth profile has contracted slightly since 2010. Seven areas registered declines from the 2010 values , the highest being “Single EPR shared by all departments” and “Integrated system for eReferral” at -27% and -24%.. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 71: Spanish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Type of ownership does not appear to influence the development of eHealth capabilities across Spanish acute hospitals. For example, in “PACS usage” and “Clear and structured rules on access to clinical data” values are quite closely grouped, with a maximum variation of 7% between the lowest and highest performer. More variation can be seen in “Broadband > 50Mbps”, “Single EPR shared by all departments” and “Exchange of clinical care information with external providers”, and in these categories the lead position is twice held by Public hospitals, and once by Private hospitals
66%
38%
96%
77%
94%
37%
65%
91%
63%
93%
54%
54%
92%
67%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Exchange of CCI with ext. providers
Clear data access rules
Public (n=62-67) Private (n=41-44) Private not for profit (n=12-13)

221
Figure 72: Spanish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Scale appears to be slightly influential in Spanish acute hospitals, but not universally so. A certain advantage appears to be conferred upon larger hospital segments in three categories, “Exchange of clinical care information with external providers”, “Clear and structured rules on access to clinical data” and “PACS usage”, with acute hospitals of More than 750 beds leading in these areas. However, this segment performs much less well in “Broadband > 50Mbps” and “Single EPR shared by all departments”, where performance is reversed and where significant gaps were noted between the highest and lowest performers.
4. Composite indicators
The following section reports the results for Spain on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the
44%
63%
91%
67%
91%
59%
52%
95%
67%
93%
73%
41%
92%
83%
96%
45%
42%
100%
92%
100%
0% 50% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=33-35) Between 101 and 250 beds (n=39-41)
Between 251 and 750 beds (n=22-24) More than 750 beds (n=11-12)

222
Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Spain´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Spain's eHealth Deployment indicator is based on data from 119 hospitals, while the Availability and Use indicator was built from the information provided by 112 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Spain eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 87 hospitals) for Spain was 0.53, while the 2012 value was 0.51, which shows a decrease of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Spain and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is a large group of hospitals (72%) were above EU27+3 average for both composite indicators. Nevertheless, there is as well a group of 10 hospitals with almost no Effective use at various levels of deployment.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Spain EU27+3

223
Figure 5: Spain's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Spain EU27+3

224
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report Sweden

225
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals85, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners86.
This document reports the results of this project for Sweden. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for Sweden are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
246 hospitals were identified in Sweden. Within this rough universe 131 (53%) completed the screener part of the questionnaire and 78 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (32% vs. 21%) and there were more hospitals of public ownership (92% vs. 64%). Out of the Swedish universe, 26 acute hospitals (33%) completed the survey.
Table 85: Swedish sample breakdown by size of acute care hospitals
Sweden N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 78
18 13 17 9 21
23% 17% 22% 12% 27%
2012 26 6 5 9 3 3
23% 19% 35% 12% 12%
2010 8 1 1 3 2 1
12% 12% 38% 25% 12%
85 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
86 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

226
Table 86: Swedish sample breakdown by ownership type
Sweden N= Public Private Private not for
profit Don't know/ No answer
Census 78
59 2 3 14
76% 3% 4% 18%
2012 26 20 - 2 4
77% - 8% 15%
2010 8 8 - - -
100% - - -
The final sample of hospitals included in the survey has a similar structure to the one of the Swedish universe of acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has more than tripled, with a lower proportion of very large and public hospitals than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

227
Figure 73: Swedish acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 87 – eHealth indicators Sweden
eHealth indicators - Sweden Valid N %
hospitals
2012 difference
Sweden vs.EU27+3
Sweden evolution,
2012 vs. 201087
Infrastructure Externally connected 26 85% 8% 10%
Broadband > 50Mbps 22 100% 64% 14%
Single and unified wireless 25 76% 36% -12%
Single EPR shared by all departments 24 79% 22% -21%
Applications PACS usage 25 88% 17% -12%
ePrescribing 26 85% 38% -15%
Integrated system for eReferral 26 69% 31% -6%
Tele-monitoring 26 8% -3% -21%
Integration Exchange of clinical care information with external providers
26 85% 29% 10%
Exchange of laboratory results with external providers
25 96% 45% 21%
Exchange of radiology reports with external providers
25 84% 29% 9%
Security Clear and structured rules on access to clinical data
26 96% 11% -4%
EAS for disaster recovery in less than 24 hours
25 72% 24% -28%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
87 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) Sweden 2010 (n=8) Sweden 2012 (n=26)

228
Position of the Swedish eHealth profile within EU27+3
Sweden is one of the strongest eHealth performers in the sample. In fact, in all 13 indicators examined, Sweden scored worse than the EU27+3 average in only one area (“Tele-monitoring”) and in this area is only marginally behind (-3% points). The areas within which Sweden is the most evolved by contrast to other countries within this study are “Broadband > 50Mbps” (64% ahead) and “Exchange of laboratory results with external providers” (64% ahead).
Changes in the Swedish eHealth profile
Despite Sweden’s strong position in eHealth, there has been some contraction of eHealth capabilities when contrasted with 2010 values. .The most notable decrease was recorded for in “EAS for disaster recovery in less than 24 hours”. In the 13 areas under review, five indicators posted modest growth, being “Exchange of laboratory results with external providers” the area where the growth was bigger. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 74: Swedish acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Only data for Public and Private not for profit hospitals were returned by our survey, and within this data we see that the latter segment of the market appears to have slightly better scores. Nevertheless, the sample size of this category, just 2 hospitals, is too small to extract definitive conclusions
100%
72%
95%
85%
95%
100%
100%
50%
100%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Public (n=17-20) Private not for profit (n=2)

229
Figure 75: Swedish acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Scale does appear to affect the eHealth capabilities of Swedish acute hospitals, with the very largest hospital segment (More than 750 beds) scoring 100% in all five indicator areas. The lowest performing hospitals, by contrast, are the two smallest segments, being Fewer than 101 beds and Between 101 and 250 beds..
4. Composite indicators
The following section reports the results for Sweden on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which
100%
71%
71%
71%
86%
100%
80%
80%
80%
100%
100%
75%
100%
100%
100%
100%
100%
100%
100%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Fewer than 101 beds (n=6-7) Between 101 and 250 beds (n=5)
Between 251 and 750 beds (n=7-9) More than 750 beds (n=3-4)

230
all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
The following graph displays the average values of these indicators in Sweden´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. Sweden's eHealth Deployment indicator is based on data from 25 hospitals, while the Availability and Use indicator was built from the information provided by 24 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: Sweden eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 7 hospitals) for Sweden was 0.64, while the 2012 value was 0.62, which shows a decrease of 2% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for Sweden and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that all Swedish hospitals but 2 were above EU27+3 average for both composite indicators. However, these two hospitals have scores lower than the European average in both indicators.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
Sweden EU27+3

231
Figure 5: Sweden's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals Sweden EU27+3

232
European Hospital Survey: Benchmarking Deployment of e-Health Services (2012–2013)
Country Report United Kingdom

233
1. Background
With the aim to benchmark the level of eHealth use in acute hospitals in all 27 EU Member States and Croatia, Iceland and Norway (EU27+3), a survey was launched to: (i) gather and analyse data on deployment, that is comparable to a 2010 similar survey; (ii) compute a composite index and use it to monitor evolution of adoption over time; and (iii) develop a new index that will monitor availability and use of eHealth.
In total 26,551 healthcare establishments in EU27+3, were contacted and screened to help define an as much homogeneous group of hospitals as possible. In total, 5424 qualified as acute care hospitals88, and of those 1717 completed the interview, 49 questions with an average duration of 43 minutes, over the period October 2012 -January 2013. The survey targeted Chief Information Officers (CIOs) and it was carried out via Computer-Aided Telephone Interviewing (CATI). The novelty of this survey is that it includes a number of questions that enable the comparison of availability and use of eHealth specific functionality; this set of questions is compatible with OECD early guidelines, as well as with the equivalent part of a similar survey among Europeans General Practitioners89.
This document reports the results of this project for United Kingdom. It starts with a brief description of the characteristics of the sample and presents a comparison with the 2010 sample. It then provides descriptive statistics and indicators. Finally, the results of the composite indicators for United Kingdom are displayed. When possible, these results are compared with the European level results, and the evolution over the period 2010-2012 is analyzed.
2. Sample analysis
889 hospitals and National Health Service (NHS) trusts were identified in United Kingdom. Within this rough universe 510 (57%) completed the screener part of the questionnaire and 102 qualified as acute care hospitals. The proportion of hospitals with less than 100 beds among these hospitals was higher compared to the universe of acute Hospitals at EU27+3 level (34% vs. 21%) and there were more hospitals of public ownership (74% vs. 64%). Out of the United Kingdom universe, 33 acute hospitals and NHS trusts (32%) completed the survey. In order to guarantee the representativeness of the healthcare system in the United Kingdom, the 2012 results of the acute hospitals within NHS trusts have been duplicated based on the number of hospitals represented by the trust. After this duplication process, the United Kingdom counts 69 hospitals in its sample.
Table 88: United Kingdom sample breakdown by size of acute care hospitals
United Kingdom N= Fewer than
101 beds Between 101 and 250 beds
Between 251 and 750 beds
More than 750 beds
Don’t know/ No
answer
Census 102
59 9 15 4 15
58% 9% 15% 4% 15%
2012 69 36 7 16 5 5
64% 9% 9% 3% 15%
2010 38 9 4 18 7 -
24% 11% 47% 18% -
88 This criterion was based on whether respondents considered that the hospital was an acute or general hospital and in case they did not, whether they reported that the hospital had an emergency department, and at least one of the following: a) routine and/or life-saving surgery operating room; and/or b) an intensive care unit.
89 Benchmarking Deployment of eHealth among General Practitioners (2013). ISBN 978-92-79-31130-7 DOI: 10.2759/24556"

234
Table 2: United Kingdom breakdown by ownership type
United Kingdom N= Public Private Private not for
profit Don't know/ No answer
Census 102
55 43 2 2
54% 42% 2% 2%
2012 69 55 13 1 -
80% 19% 1% -
2010 38 28 5 5 -
74% 13% 13% -
The final sample of hospitals included in the survey has a bigger proportion of public hospitals than the universe of United Kingdom acute hospitals. Comparing this 2012 final sample with the one of the 2010 survey, the number of hospitals has almost doubled, with a higher proportion of small hospitals (less than 100 beds) than in 2010.
3. Descriptive statistics and indicators
Using 13 eHealth indicators derived from the specific answers to the questionnaire, an eHealth profile has been constructed for each country and is represented through a spider diagram. These diagrams have scores ranging from 0 to 5, which respectively correspond to a 0% to 100% implementation rate . The 13 indicators cover the following 4 thematic areas:
Infrastructure: Externally connected, Broadband > 50Mbps and Single and unified wireless: Applications: Single Electronic Patient Records (EPR) shared by all departments, Picture Archiving and Communication System (PACS) usage, ePrescribing, Integrated system for eReferral and Tele-monitoring Integration: Exchange of clinical care information (CCI) with external providers; Exchange of laboratory results with external providers; and Exchange of radiology reports with external providers. Security: Clear and structured rules on access to clinical data and Enterprise Archive Strategy (EAS) for disaster recovery in less than 24 hours: The results for some of these indicators are also reported by groups of hospitals according to the ownership and size of the hospitals that completed the survey.

235
Figure 76: United Kingdom acute hospital eHealth profile
Note: The scoring scale from 0 to 5 points corresponds to an implementation rate from 0% to 100%.
Table 89 – eHealth indicators United Kingdom
eHealth indicators - United
Kingdom Valid N
%
hospitals
2012 difference
United Kingdom
vs.EU27+3
United Kingdom
evolution, 2012 vs.
201090
Infrastructure Externally connected 68 79% 3% -15%
Broadband > 50Mbps 37 81% 46% 13%
Single and unified wireless 67 64% 24% -2%
Single EPR shared by all departments 68 40% -17% -31%
Applications PACS usage 69 97% 26% 2%
ePrescribing 67 21% -26% -11%
Integrated system for eReferral 67 73% 35% 10%
Tele-monitoring 68 22% 12% 11%
Integration Exchange of clinical care information with external providers
67 76% 10% -23%
Exchange of laboratory results with external providers
67 73% 11% -30%
Exchange of radiology reports with external providers
68 65% 4% -2%
Security Clear and structured rules on access to clinical data
66 85% 0% -13%
EAS for disaster recovery in less than 24 hours
58 57% 9% -16%
Note: Results are based on valid answers only - bases (n) may differ from the ones reported here
90 These results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
0
1
2
3
4
5Externally connected
Broadband > 50Mbps
Single and unified wireless
Single EPR shared by all departments
PACS usage
ePrescribing
Integrated system for eReferralTele-monitoring
Exchange of clinical care information with external
providers
Exchange of laboratory results with external providers
Exchange of radiology reports with external providers
Clear and structured rules on access to clinical data
EAS for disaster recovery in less than 24 hours
EU27+3 (n=1753) United Kingdom 2010 (n=38) United Kingdom 2012 (n=69)

236
Position of the United Kingdom eHealth profile within EU27+3
The United Kingdom is above the average in terms of the adoption of eHealth capabilities. The United Kingdom’s largest scores above the average value come from “Broadband > 50Mbps”, “Single and unified wireless”, “PACS usage” and “Integrated system for eReferral”. Only the “Single EPR shared by all departments”, “ePrescribing” and “Clear and structured rules on access to clinical data” indicators scored below average.
Changes in the United Kingdom eHealth profile
Despite the United Kingdom’s healthy position in relation to the average EU27+3 results, the country’s performance has dropped in several areas, with only four areas where the 2012 results are higher than the 2010 ones.. All other nine indicators registered negative growth, with “Single EPR shared by all departments”, “Exchange of clinical care information with external providers” and “Exchange of laboratory results with external providers” being the areas where this decrease has been more significant. Nevertheless, these results should be taken with caution. Although samples are representative of the universe in each survey, they might not be fully comparable between the two years.
Out of the 13 indicators included and analysed in the eHealth profile, 5 were selected to explore variability in the results according to size and ownership of the hospitals.
Figure 77: United Kingdom acute hospitals eHealth profile by ownership
Note: Results are based on valid answers only - category bases may vary from the total reported here.
No definite trends can be observed based on ownership type among United Kingdom hospitals. Public hospitals appear to perform better, scoring highest or joint highest in three of five categories (“Broadband > 50Mbps”, “PACS usage” and “Exchange of clinical care information with external providers”) and Private hospitals perform better in “Clear and structured rules on access to clinical data” and “Single EPR shared by all departments”. Private not for profit acute hospitals only returned data for one of five categories under investigation
93%
35%
100%
81%
83%
29%
62%
85%
58%
100%
0%
0%
100%
0%
0%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by alldepartments
PACS usage
Exchange of CCI with ext.providers
Clear data access rules
Public (n=30-55) Private (n=7-13) Private not for profit (n=1)

237
Figure 78: United Kingdom acute hospitals eHealth profile by size
Note: Results are based on valid answers only - category bases may vary from the total reported here.
Scale appears to be more influential in the development of eHealth capabilities across UK hospitals, with the largest hospitals (Between 251 and 750 beds and More than 750 beds) outperforming other segments in four of five indicator areas. In addition, for three of these indicator, “Broadband > 50Mbps”, “Exchange of clinical care information with external providers” and “Clear and structured rules on access to clinical data”, the margin between the highest and lowest performers is considerable.
4. Composite indicators
The following section reports the results for United Kingdom on the composite indicators for eHealth Deployment and eHealth Availability and Use. Deployment, in this context, is understood as the existence of infrastructure (i.e. broadband connection), applications (i.e. a computerised system for eprescribing), systems (i.e.to exchange clinical information with other care providers electronically) and regulations (i.e. on security and privacy of medical data). Availability is understood as the level of implementation of eHealth functionalities across hospitals' units while use is understood as the extent to which health professionals use the eHealth functionalities that have been implemented. The composite indicators are calculated at Hospital level before obtaining average country values. These indicators have been developed by IPTS through multivariate statistical analysis and they make it possible to benchmark between countries and compare 2012 results for eHealth deployment with those from a similar survey carried out in 2010.
The indicator for eHealth Deployment was based on 45 variables from the survey that provided information on characteristics related to the deployment of eHealth in each hospital. These variables were grouped in 4 dimensions (Infrastructure, Applications, Health Information Exchange, and Security and Privacy) and each dimension was given the same weight in the final indicator. Further, the eHealth Availability and Use indicator was based on information from the survey on the level of availability and use in each hospital of 39 different eHealth functionalities pertaining to 4 categories (View/Input Information on EHR; Clinical Decision Support on EHR; Health Information Exchange; and Telehealth). For both indicators, the range of possible values is 0-1. This implies that, for instance, a hospital with positive answers in all 45 variables which were the basis for the Deployment indicator would score a value of 1 in this indicator. Correspondingly, a hospital in which all 39 of the eHealth functionalities were unavailable (or available but not being used) would obtain a score of zero in the Availability and Use indicator.
69%
41%
95%
68%
82%
50%
33%
100%
67%
67%
100%
36%
100%
82%
82%
90%
27%
100%
100%
100%
0% 20% 40% 60% 80% 100%
Broadband > 50Mbps
Single EPR shared by all departments
PACS usage
Exchange of CCI with ext. providers
Clear data access rules
Fewer than 101 beds (n=16-41) Between 101 and 250 beds (n=2-4)
Between 251 and 750 beds (n=7-11) More than 750 beds (n=10-11)

238
The following graph displays the average values of these indicators in United Kingdom´s hospitals, comparing them with the average values obtained for the whole sample of EU27+3 hospitals. United Kingdom's eHealth Deployment indicator is based on data from 67 hospitals, while the Availability and Use indicator was built from the information provided by 51 hospitals. The values for the EU27+3 indicators are obtained from samples of 1,643 hospitals (Deployment) and 1,533 hospitals (Use and Availability). These differences are the consequence of different numbers of missing values in each of the survey blocks.
Figure 4: United Kingdom eHealth Composite Indicators
For the eHealth Deployment indicator, it is also possible to analyse the evolution over the period 2010-2012. In 2010, this indicator (based on data from 37 hospitals) for United Kingdom was 0.62, while the 2012 value was 0.58, which shows a negative growth of 4% over the two year period. In comparison, the average increase in eHealth Deployment for the EU27+3 hospitals (2010 results based on data from 844 hospitals) was 3%.
Finally, for hospitals with valid data for both indicators, it is possible to map these individual values on a graph and compare them with the average value for United Kingdom and with the average value of the EU27+3 hospitals in order to show the variability of the hospitals' results. This exercise is displayed in the following graph. It shows that there is significant variability among UK hospitals and NHS trusts91. While 9 hsopitals (36% of the sample) were above EU27+3 average for both composite indicators, there were as well 6 hospitals (25%) with results below EU27+3 average for both composite indicators.
91 In this graph, results for NHS trusts have been not duplicated based on the number of hospitals represented by the trust.
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
2012 Deployment 2012 Availability & Use
UK EU27+3

239
Figure 5: United Kingdom's hospitals values of eHealth Composite Indicators
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Ava
ilab
ility
& U
se
Deployment
Hospitals UK EU27+3

240

European Commission
EUR 26357 – Joint Research Centre – Institute for Prospective Technological Studies
Title: European Hospital Survey: Benchmarking deployment of e-Health services (2012–2013) – Country Reports
Author: Ramon Sabes-Figuera
Luxembourg: Publications Office of the European Union
2013 – 239 pp. – 21.0 x 29.7 cm
EUR – Scientific and Technical Research series – ISSN 1831-9424 (online)
ISBN 978-92-79-34778-8 (pdf)
I
doi:10.2791/55973
Abstract
A widespread uptake of eHealth technologies is likely to benefit European Healthcare systems both in terms of quality of care and financial sustainability and European society at large. This is why eHealth has been on the European Commission policy agenda for more than a decade. The objectives of the latest eHealth action plan developed in 2012 are in line with those of the Europe 2020 Strategy and the Digital Agenda for Europe.
This report, based on the analysis of the data from the "European Hospital Survey: Benchmarking deployment of e-Health services (2012–2013)" project, presents policy relevant results and findings for each of the 28 EU Member States as well as Iceland and Norway.
The results highlighted here are based on the analysis of the survey descriptive results as well as two composite indicators on eHealth deployment and eHealth availability and use that were developed based on the survey's data

z
As the Commission’s in-house science service, the Joint Research Centre’s mission is to provide EU policies with independent, evidence-based scientific and technical support throughout the whole policy cycle. Working in close cooperation with policy Directorates-General, the JRC addresses key societal challenges while stimulating innovation through developing new standards, methods and tools, and sharing and transferring its know-how to the Member States and international community. Key policy areas include: environment and climate change; energy and transport; agriculture and food security; health and consumer protection; information society and digital agenda; safety and security including nuclear; all supported through a cross-cutting and multi-disciplinary approach.
LF-NA
-26
35
7-E
N-N
Related Documents