Etiologies of Rash and Fever Illnesses in Campinas, Brazil José Cássio de Moraes, Cristiana M. Toscano, Eliana N. C. de Barros, Brigina Kemp, Fabio Lievano, Steven Jacobson, Ana Maria S. Afonso, Peter M. Strebel, K. Lisa Cairns, the VigiFex Group Downloaded from https://academic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Etiologies of Rash and Fever Illnesses in Campinas,
Brazil
José Cássio de Moraes, Cristiana M. Toscano, Eliana N. C. de Barros, Brigina
Kemp, Fabio Lievano, Steven Jacobson, Ana Maria S. Afonso, Peter M. Strebel,
K. Lisa Cairns, the VigiFex Group
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
S U P P L E M E N T A R T I C L E
Etiologies of Rash and Fever Illnesses inCampinas, Brazil
Jose Cassio de Moraes,1 Cristiana M. Toscano,3,5,a Eliana N. C. de Barros,4,a Brigina Kemp,4 Fabio Lievano,5,a
Steven Jacobson,6 Ana Maria S. Afonso,2 Peter M. Strebel,5,a K. Lisa Cairns,5,a and the VigiFex Group1Santa Casa de Sao Paulo Medical Sciences University, and 2Instituto Adolfo Lutz-Sao Paulo, Sao Paulo, 3Pan American Health Organization, Brasilia,and 4Municipal Health Department, Campinas, Brazil; 5National Center for Immunizations and Respiratory Diseases, Centers for Disease Control andPrevention, Atlanta, Georgia; and 6National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, Maryland
Background. Few population-based studies of infectious etiologies of fever-rash illnesses have been conducted.
This study reports on enhanced febrile-rash illness surveillance in Campinas, Brazil, a setting of low measles and
rubella virus transmission.
Methods. Cases of febrile-rash illnesses in individuals aged ,40 years that occurred during the period 1 May
2003–30 May 2004 were reported. Blood samples were collected for laboratory diagnostic confirmation, which
included testing for adenovirus, dengue virus, Epstein-Barr virus (EBV), enterovirus, human herpes virus 6
(HHV6), measles virus, parvovirus-B19, Rickettsia rickettsii, rubella virus, and group A streptococci (GAS)
infections. Notification rates were compared with the prestudy period.
Results. A total of 1248 cases were notified, of which 519 (42%) had laboratory diagnosis. Of these, HHV-6
(312 cases), EBV (66 cases), parvovirus (30 cases), rubella virus (30 cases), and GAS (30 cases) were the most
frequent causes of infection. Only 10 rubella cases met the rubella clinical case definition currently in use.
Notification rates were higher during the study than in the prestudy period (181 vs 52.3 cases per 100,000
population aged ,40 years).
Conclusions. Stimulating a passive surveillance system enhanced its sensitivity and resulted in additional
rubella cases detected. In settings with rubella elimination goals, rubella testing may be considered for all cases of
febrile-rash illness, regardless of suspected clinical diagnosis.
Relatively few comprehensive population-based studies of
the etiology of fever-rash illnesses have been conducted,
and most of these are from the northern hemisphere
[1–6]. Such studies are important to better understand
the age and geographic distribution and the incidence of
these etiologies. In the context of the Americas’ measles
and rubella elimination goals, this information can also
inform a minimum suspected measles and rubella re-
porting rate, which aims to ensure surveillance sensitive
enough to detect circulating measles and rubella virus.
In 1994, the Region of the Americas set the goal of
measles elimination (‘‘elimination’’ is defined as the ab-
sence of endemic measles cases in a defined geographical
area for a period of at least 12 months, in the presence of
a well-perfoming surveillance system) by 2000. This goal
was achieved in November 2002. Since then, all reported
measles cases have been linked to importation from
measles-endemic countries [7]. In Brazil, 2 confirmed
measles cases were reported in 2003 [8] and 0 cases were
reported in 2004 [9]. During 2001–2002, Brazil con-
ducted vaccination campaigns targeting all women of
childbearing age (the target age group varied by state,
with 12 years the lowest and 49 years the upper age limit)
Potential conflicts of interest: F. L. is currently working as Senior Director,Clinical Risk Management and Safety Surveillance, Merck & Co., Inc. All otherauthors: no conflicts.Presented in part: 4th Expo Epi (Brazilian exhibit of experiences on
epidemiology) Conference, Brasilia, Brazil, 2004.aPresent affiliations: Merck & Co, Inc., Whitehouse Station, New Jersey (F. L.);
Federal University of Goias, Goiania, Brazil (C. M. T.); World Health Organization,Beijing, China (K. L. C.); World Health Organization, Geneva, Switzerland (P. M. S.);and National Coordination for Respiratory and Vaccine Preventable DiseasesSurveillance, Brazilian Ministry of Health, Brazil (E. N. C. d. B.).Correspondence: Cristiana M. Toscano, MD, PhD, Av. T-05, 715. Apto. 301. Setor
Bueno - Goiania, GO - Brazil 74230-045 ([email protected]).
The Journal of Infectious Diseases 2011;204:S627–S636� The Author 2011. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected] (print)/1537-6613 (online)/2011/204S2-0010$14.00DOI: 10.1093/infdis/jir490
Rash and Fever Syndromic Surveillance d JID 2011:204 (Suppl 2) d S627
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

for accelerated rubella control and congenital rubella syn-
drome (CRS) prevention. Five hundred sixty-three cases of
rubella were reported nationwide in 2003 [8] and 401 were re-
ported in 2004 [10]. In September 2003, the Americas endorsed
the rubella and CRS elimination goal by 2010 [11]
To monitor progress toward measles and rubella elimination,
the Pan American Health Organization (PAHO) recommends
that all countries in the region have integrated measles and rubella
surveillance. In Brazil, all cases of fever and rash meeting clinical
case definitions for measles (defined as fever and maculopapular
rash accompanied by $1 of the 3 following symptoms, cough,
coryza, or conjunctivitis, in any individual, regardless of age or
vaccination status) or rubella (defined as fever and maculopapular
rash accompanied by retroauricular, occipital, or cervical
lymphadenopathy in any individual, regardless of age and vacci-
nation status) should be notified and confirmed or discarded by
laboratory testing [12, 13]. The use of specific indicators to eval-
uate the quality of surveillance has been proposed. The World
Health Organization (WHO) has suggested an annual rate of
reported suspected measles or rubella cases of $2 cases per
100,000 population as an indicator of the sensitivity of the sur-
veillance system. PAHO has recently endorsed this indicator as
a criterion for documentation and verification of measles, rubella,
and CRS elimination in the American region [14].
To better understand the etiologies, distribution, and back-
ground rates of fever-rash illnesses in a community setting with
low rates of measles and rubella virus transmission and to assess
the usefulness and feasibility of a minimum suspected measles or
rubella reporting rate as an indicator of measles-rubella sur-
veillance sensitivity, we conducted enhanced passive surveillance
for fever-rash illnesses in individuals aged ,40 years during the
period from 1 May 2003 through 30 May 2004 in Campinas, Sao
Paulo State, Brazil.
METHODS
Study SettingCampinas, a city of �1 million inhabitants located 120 kilo-
meters northwest of Sao Paulo, Brazil, was selected as a study site
due to its well-functioning disease surveillance system, low rates
of measles and rubella virus transmission, and proximity to
a reference laboratory capable of testing for numerous infectious
agents. Public health care, provided by the National Health
System (NHS; Sistema Unico de Saude), is used exclusively by
�70% of the population; the remaining 30%, although eligible
for NHS services, receive most health care through the private
sector. In the public sector, Campinas has 78 clinics, 3 urgent
care centers, and 1 hospital. In the private sector, there are 5000
practitioners employed mainly by 4 major Health Maintenance
Organizations [15] and 21 hospitals. In addition, there are
2 university hospitals. Before this study, measles, rubella,
and dengue surveillance existed, in accordance with national
guidelines. Reporting came almost exclusively from public
health providers. Surveillance quality was considered good, as
demonstrated by standard performance indicators [16].
Study ImplementationThe study was conducted from 1 May 2003 through 30 May 2004.
Before initiating the study, meetings were held with surveillance
workers and both private and public primary health care pro-
viders in Campinas. An international seminar was convened when
the study was launched, and folders, posters, and CDs were dis-
tributed to health care professionals from both public and private
settings invited to participate. A website through which fever-rash
illnesses could be electronically reported was developed.
Information about the study was made available to the pop-
ulation via the media. Throughout the study, meetings were held
with health care providers from private and university settings
whenever they reported fewer than expected cases. Prior to the
end of the study, a surveillance bulletin was distributed to all
reporting sites, and a seminar targeting surveillance professionals
was held to present the study’s findings.
Implementation of the study was done through the existing
surveillance structure. To provide the additional workforce nec-
essary, the municipal surveillance team was supplemented by
12 staff (1 manager, 8 nurse assistants, 2 laboratory technicians,
and 1 driver). One person oversaw rash and fever surveillance in
each of the 5 health districts of the city. Data were reported
directly to the municipal level responsible for managing the sur-
veillance system.
Data CollectionA standard case reporting form was used to collect demographic,
clinical, and risk factor information for all nonvesicular febrile-
rash illnesses in individuals aged ,40 years. To facilitate private
sector participation, a simplified notification form was developed
for their use. Fever was defined as axillary temperature .37.8�Cand rash as recent presence of generalized red lesions on the skin.
Completed forms were sent daily to the district surveillance
team who identified missing information or specimens and
sought collection of this information through home visits.
Surveillance was passive but was supplemented by weekly or
biweekly active case finding in 3 selected emergency departments
and 3 urgent care clinics that had historically underreported
measles and rubella cases.
Specimen Collection and ProcessingThe specimen collection and testing protocol assumed that some
patients would receive a presumptive clinical diagnosis at the
time of presentation for care, and this diagnosis was factored
into the algorithm. At the time of initial presentation to the
health care provider, 3–5 mL of blood was drawn for laboratory
testing, unless rubella, dengue, or Rocky Mountain spotted fever
(RMSF; ie, Rickettsia rickettsii infection) was the presumptive
S628 d JID 2011:204 (Suppl 2) d de Moraes et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
clinical diagnosis. If the latter occurred, the first specimen was
drawn, respectively, on the fifth, sixth, or seventh day after rash
onset. Oropharyngeal swabs were collected up to 5 days after
rash onset from all patients with cough and coryza and trans-
ported in viral transport media vials for enterovirus and ade-
novirus testing. Persons with suspected group A streptococci
(GAS) infection had oropharyngeal swabs transported in acti-
vated carbon media. A second convalescent-phase blood sample
was collected from all reported cases 3–4 weeks after rash onset,
when any missing clinical and epidemiologic data were also
collected during home visits.
Whole-blood and oropharyngeal samples were refrigerated
at 4�C and sent every other day to 1 of the 2 municipal refer-
ence laboratories in Campinas, where blood samples were
centrifuged. Samples were shipped 3–5 times weekly from these
reference laboratories to the Instituto Adolfo Lutz Laboratory in
Sao Paulo, where oropharyngeal swabs were centrifuged and
blood and oropharyngeal samples were further processed and
tested.
Laboratory ProceduresSerum specimens were tested in the laboratory for serological
evidence of the following etiologies of febrile-rash illnesses: ad-
enoviruses, dengue virus, Epstein Barr virus (EBV), enteroviruses
(coxsackieviruses B1–B6; echoviruses 4, 6, 9, 11, and 30; entero-
viruses 70 and 71; and polioviruses 1–3), human herpes virus 6
(HHV6), measles virus, parvovirus B19, R. rickettsii, and rubella
virus. Oropharyngeal swabs were tested for GAS bacterial culture
or for enteroviruses and adenoviruses viral culture.
Testing for adenovirus, enterovirus, and RMSF could only be
performed when both acute- and convalescent-phase serum
specimens were available. Testing for GAS was only performed
when an oropharyngeal swab was available (in addition to serum
samples).
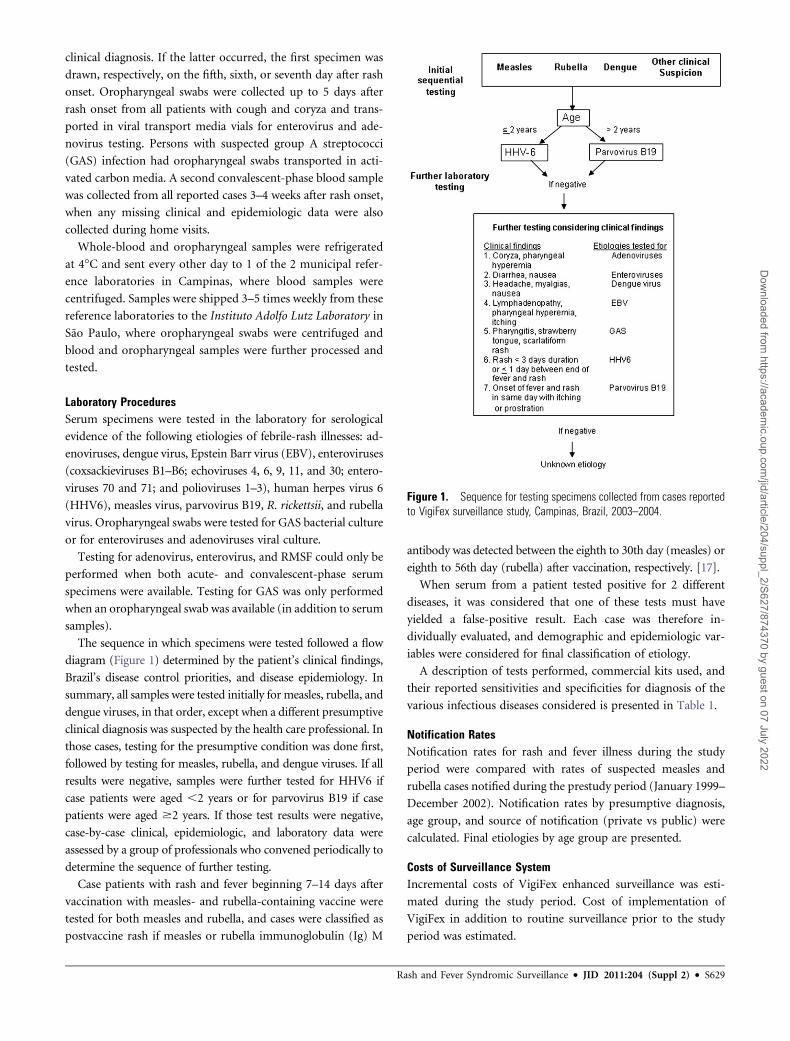
The sequence in which specimens were tested followed a flow
diagram (Figure 1) determined by the patient’s clinical findings,
Brazil’s disease control priorities, and disease epidemiology. In
summary, all samples were tested initially for measles, rubella, and
dengue viruses, in that order, except when a different presumptive
clinical diagnosis was suspected by the health care professional. In
those cases, testing for the presumptive condition was done first,
followed by testing for measles, rubella, and dengue viruses. If all
results were negative, samples were further tested for HHV6 if
case patients were aged ,2 years or for parvovirus B19 if case
patients were aged $2 years. If those test results were negative,
case-by-case clinical, epidemiologic, and laboratory data were
assessed by a group of professionals who convened periodically to
determine the sequence of further testing.
Case patients with rash and fever beginning 7–14 days after
vaccination with measles- and rubella-containing vaccine were
tested for both measles and rubella, and cases were classified as
postvaccine rash if measles or rubella immunoglobulin (Ig) M
antibody was detected between the eighth to 30th day (measles) or
eighth to 56th day (rubella) after vaccination, respectively. [17].
When serum from a patient tested positive for 2 different
diseases, it was considered that one of these tests must have
yielded a false-positive result. Each case was therefore in-
dividually evaluated, and demographic and epidemiologic var-
iables were considered for final classification of etiology.
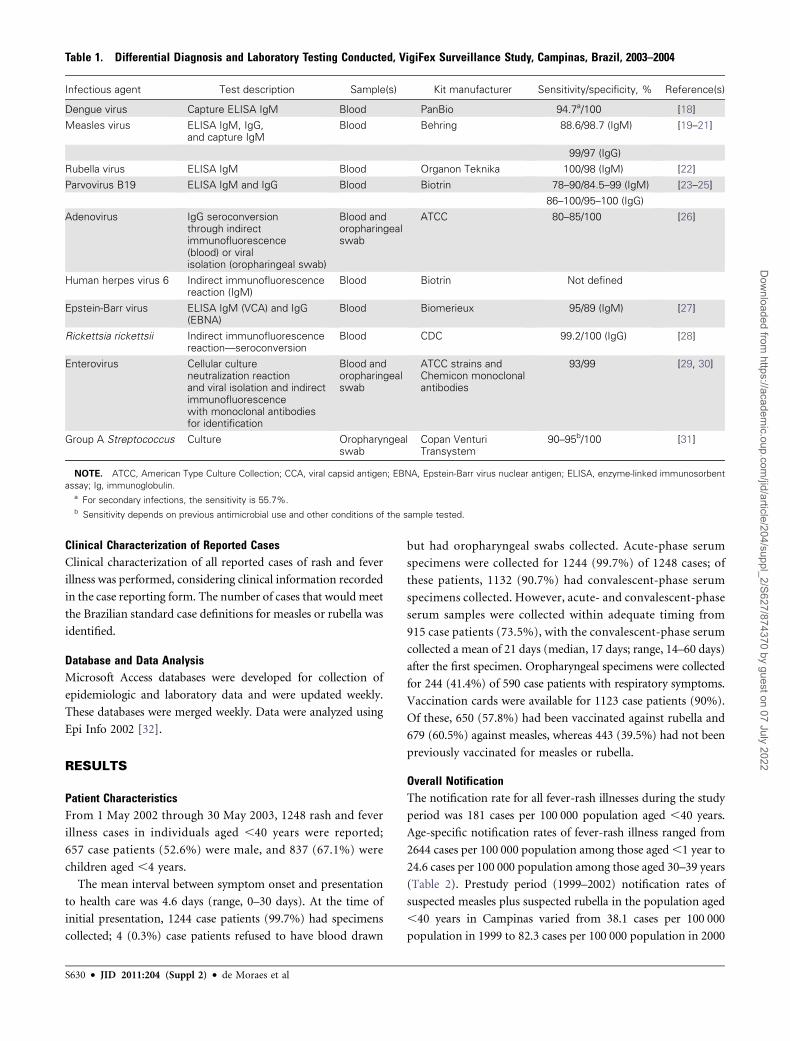
A description of tests performed, commercial kits used, and
their reported sensitivities and specificities for diagnosis of the
various infectious diseases considered is presented in Table 1.
Notification RatesNotification rates for rash and fever illness during the study
period were compared with rates of suspected measles and
rubella cases notified during the prestudy period (January 1999–
December 2002). Notification rates by presumptive diagnosis,
age group, and source of notification (private vs public) were
calculated. Final etiologies by age group are presented.
Costs of Surveillance SystemIncremental costs of VigiFex enhanced surveillance was esti-
mated during the study period. Cost of implementation of
VigiFex in addition to routine surveillance prior to the study
period was estimated.
Figure 1. Sequence for testing specimens collected from cases reportedto VigiFex surveillance study, Campinas, Brazil, 2003–2004.
Rash and Fever Syndromic Surveillance d JID 2011:204 (Suppl 2) d S629
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
Clinical Characterization of Reported CasesClinical characterization of all reported cases of rash and fever
illness was performed, considering clinical information recorded
in the case reporting form. The number of cases that would meet
the Brazilian standard case definitions for measles or rubella was
identified.
Database and Data AnalysisMicrosoft Access databases were developed for collection of
epidemiologic and laboratory data and were updated weekly.
These databases were merged weekly. Data were analyzed using
Epi Info 2002 [32].
RESULTS
Patient CharacteristicsFrom 1 May 2002 through 30 May 2003, 1248 rash and fever
illness cases in individuals aged ,40 years were reported;
657 case patients (52.6%) were male, and 837 (67.1%) were
children aged ,4 years.
The mean interval between symptom onset and presentation
to health care was 4.6 days (range, 0–30 days). At the time of
initial presentation, 1244 case patients (99.7%) had specimens
collected; 4 (0.3%) case patients refused to have blood drawn
but had oropharyngeal swabs collected. Acute-phase serum
specimens were collected for 1244 (99.7%) of 1248 cases; of
these patients, 1132 (90.7%) had convalescent-phase serum
specimens collected. However, acute- and convalescent-phase
serum samples were collected within adequate timing from
915 case patients (73.5%), with the convalescent-phase serum
collected a mean of 21 days (median, 17 days; range, 14–60 days)
after the first specimen. Oropharyngeal specimens were collected
for 244 (41.4%) of 590 case patients with respiratory symptoms.
Vaccination cards were available for 1123 case patients (90%).
Of these, 650 (57.8%) had been vaccinated against rubella and
679 (60.5%) against measles, whereas 443 (39.5%) had not been
previously vaccinated for measles or rubella.
Overall NotificationThe notification rate for all fever-rash illnesses during the study
period was 181 cases per 100 000 population aged ,40 years.
Age-specific notification rates of fever-rash illness ranged from
2644 cases per 100 000 population among those aged ,1 year to
24.6 cases per 100 000 population among those aged 30–39 years
(Table 2). Prestudy period (1999–2002) notification rates of
suspected measles plus suspected rubella in the population aged
,40 years in Campinas varied from 38.1 cases per 100 000
population in 1999 to 82.3 cases per 100 000 population in 2000
Table 1. Differential Diagnosis and Laboratory Testing Conducted, VigiFex Surveillance Study, Campinas, Brazil, 2003–2004
Infectious agent Test description Sample(s) Kit manufacturer Sensitivity/specificity, % Reference(s)
Dengue virus Capture ELISA IgM Blood PanBio 94.7a/100 [18]
Measles virus ELISA IgM, IgG,and capture IgM
Blood Behring 88.6/98.7 (IgM) [19–21]
99/97 (IgG)
Rubella virus ELISA IgM Blood Organon Teknika 100/98 (IgM) [22]
Parvovirus B19 ELISA IgM and IgG Blood Biotrin 78–90/84.5–99 (IgM) [23–25]
86–100/95–100 (IgG)
Adenovirus IgG seroconversionthrough indirectimmunofluorescence(blood) or viralisolation (oropharingeal swab)
Blood andoropharingealswab
ATCC 80–85/100 [26]
Human herpes virus 6 Indirect immunofluorescencereaction (IgM)
Blood Biotrin Not defined
Epstein-Barr virus ELISA IgM (VCA) and IgG(EBNA)
Blood Biomerieux 95/89 (IgM) [27]
Rickettsia rickettsii Indirect immunofluorescencereaction—seroconversion
Blood CDC 99.2/100 (IgG) [28]
Enterovirus Cellular cultureneutralization reactionand viral isolation and indirectimmunofluorescencewith monoclonal antibodiesfor identification
Blood andoropharingealswab
ATCC strains andChemicon monoclonalantibodies
93/99 [29, 30]
Group A Streptococcus Culture Oropharyngealswab
Copan VenturiTransystem
90–95b/100 [31]
NOTE. ATCC, American Type Culture Collection; CCA, viral capsid antigen; EBNA, Epstein-Barr virus nuclear antigen; ELISA, enzyme-linked immunosorbent
assay; Ig, immunoglobulin.a For secondary infections, the sensitivity is 55.7%.b Sensitivity depends on previous antimicrobial use and other conditions of the sample tested.
S630 d JID 2011:204 (Suppl 2) d de Moraes et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

(Figure 2), with a mean rate in the period of 52.3 cases per
100 000 population aged ,40 years.
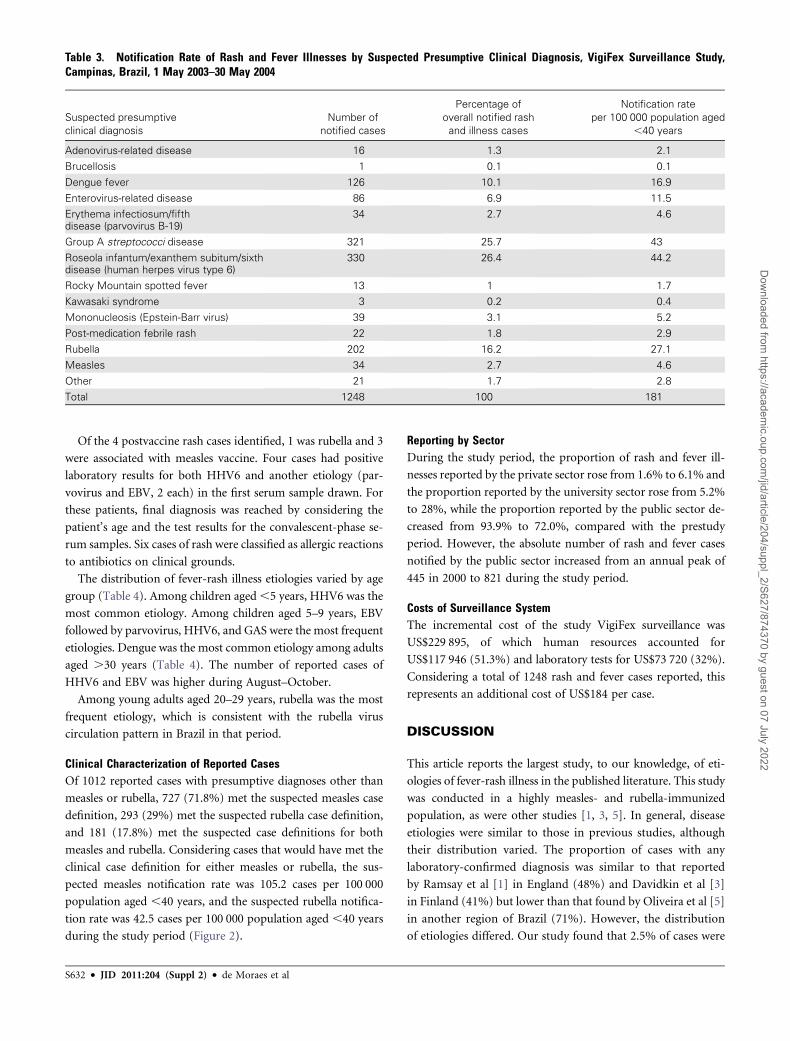
Notification by Initial Presumptive Clinical DiagnosisNotification rates of rash and fever illnesses by presumptive
clinical diagnosis are presented in Table 3. Presumptive clinical
diagnoses before laboratory testing with the highest notification
rates were HHV6 (44.2 cases per 100 000 population aged ,40
years), GAS (43.0 cases per 100 000 population aged,40 years),
rubella (27.1 cases per 100 000 population aged ,40 years), and
dengue (16.9 cases per 100 000 population aged ,40 years). The
notification rate for suspected measles or rubella was 31.6 cases
per 100 000 population aged ,40 years (Table 3 and Figure 2).
Etiology of Rash and Fever IllnessOverall, 519 (41.7%) of 1132 rash-fever cases had an etiologic
diagnosis determined by laboratory, with the highest proportions
with a laboratory-confirmed diagnosis among children aged ,1
year (59.0%) and among persons aged 30–39 years (53.7%)
(Table 2). Children aged ,10 years accounted for 455 (87.7%) of
cases with an identified etiology (Table 2). The most common
laboratory-determined etiologies were HHV6 (312 cases), EBV
(66 cases), parvovirus (30 cases), rubella virus (30 cases), GAS (30
cases), and dengue virus (22 cases) (Table 4).
No cases of measles were confirmed, supporting Brazil’s
achievement of measles elimination. Two hundred two rash
and fever cases were reported as suspected rubella, of which 8
were laboratory-confirmed. An additional 22 rubella cases
were detected through laboratory testing, for a total of 30
cases. Two of these 22 additional cases actually met Brazil’s
clinical case definition for rubella and thus should have been
reported as suspected rubella. These 2 cases were diagnosed as
dengue infection. The majority (n 5 18) of diagnosed rubella
cases (n 5 30) occurred in children aged ,4 years (60.3%).
Table 2. Notification Rate of Rash and Fever Illnesses and Laboratory-Confirmed Diagnosis by Age Group, VigiFex Surveillance Study,Campinas, Brazil, 2003–2004
Age group,
years Population
Number of
notified cases (n)
Notification
rate per 100 000 population
Number (%) of notified
cases with laboratory-confirmed
diagnosis
,1 14 937 395 2644.44 233 (59.0)
1–4 63 028 442 701.28 167 (37.8)
5–9 78 381 213 271.75 55 (25.8)
10–14 85 266 51 59.81 10 (19.6)
15–19 93 913 32 34.07 11 (34.4)
20–29 187 414 74 39.48 21 (28.4)
30–39 166 453 41 24.63 22 (53.7)
Total 689 392 1248 181 519 (41.7)
NOTE. Diagnosis was considered preliminary for cases with positive human herpes virus 6 test results.
Figure 2. Annual notification rates of confirmed rubella/measles cases, all rash and fever illness, and other etiologies meeting the rubella or measles casedefinition in Campinas, Brazil, per 100 000 population aged ,40 years, 1999–2004.
Rash and Fever Syndromic Surveillance d JID 2011:204 (Suppl 2) d S631
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
Of the 4 postvaccine rash cases identified, 1 was rubella and 3
were associated with measles vaccine. Four cases had positive
laboratory results for both HHV6 and another etiology (par-
vovirus and EBV, 2 each) in the first serum sample drawn. For
these patients, final diagnosis was reached by considering the
patient’s age and the test results for the convalescent-phase se-
rum samples. Six cases of rash were classified as allergic reactions
to antibiotics on clinical grounds.
The distribution of fever-rash illness etiologies varied by age
group (Table 4). Among children aged ,5 years, HHV6 was the
most common etiology. Among children aged 5–9 years, EBV
followed by parvovirus, HHV6, and GAS were the most frequent
etiologies. Dengue was the most common etiology among adults
aged .30 years (Table 4). The number of reported cases of
HHV6 and EBV was higher during August–October.
Among young adults aged 20–29 years, rubella was the most
frequent etiology, which is consistent with the rubella virus
circulation pattern in Brazil in that period.
Clinical Characterization of Reported CasesOf 1012 reported cases with presumptive diagnoses other than
measles or rubella, 727 (71.8%) met the suspected measles case
definition, 293 (29%) met the suspected rubella case definition,
and 181 (17.8%) met the suspected case definitions for both
measles and rubella. Considering cases that would have met the
clinical case definition for either measles or rubella, the sus-
pected measles notification rate was 105.2 cases per 100 000
population aged ,40 years, and the suspected rubella notifica-
tion rate was 42.5 cases per 100 000 population aged ,40 years
during the study period (Figure 2).
Reporting by SectorDuring the study period, the proportion of rash and fever ill-
nesses reported by the private sector rose from 1.6% to 6.1% and
the proportion reported by the university sector rose from 5.2%
to 28%, while the proportion reported by the public sector de-
creased from 93.9% to 72.0%, compared with the prestudy
period. However, the absolute number of rash and fever cases
notified by the public sector increased from an annual peak of
445 in 2000 to 821 during the study period.
Costs of Surveillance SystemThe incremental cost of the study VigiFex surveillance was
US$229 895, of which human resources accounted for
US$117 946 (51.3%) and laboratory tests for US$73 720 (32%).
Considering a total of 1248 rash and fever cases reported, this
represents an additional cost of US$184 per case.
DISCUSSION
This article reports the largest study, to our knowledge, of eti-
ologies of fever-rash illness in the published literature. This study
was conducted in a highly measles- and rubella-immunized
population, as were other studies [1, 3, 5]. In general, disease
etiologies were similar to those in previous studies, although
their distribution varied. The proportion of cases with any
laboratory-confirmed diagnosis was similar to that reported
by Ramsay et al [1] in England (48%) and Davidkin et al [3]
in Finland (41%) but lower than that found by Oliveira et al [5]
in another region of Brazil (71%). However, the distribution
of etiologies differed. Our study found that 2.5% of cases were
Table 3. Notification Rate of Rash and Fever Illnesses by Suspected Presumptive Clinical Diagnosis, VigiFex Surveillance Study,Campinas, Brazil, 1 May 2003–30 May 2004
Suspected presumptive
clinical diagnosis
Number of
notified cases
Percentage of
overall notified rash
and illness cases
Notification rate
per 100 000 population aged
,40 years
Adenovirus-related disease 16 1.3 2.1
Brucellosis 1 0.1 0.1
Dengue fever 126 10.1 16.9
Enterovirus-related disease 86 6.9 11.5
Erythema infectiosum/fifthdisease (parvovirus B-19)
34 2.7 4.6
Group A streptococci disease 321 25.7 43
Roseola infantum/exanthem subitum/sixthdisease (human herpes virus type 6)
330 26.4 44.2
Rocky Mountain spotted fever 13 1 1.7
Kawasaki syndrome 3 0.2 0.4
Mononucleosis (Epstein-Barr virus) 39 3.1 5.2
Post-medication febrile rash 22 1.8 2.9
Rubella 202 16.2 27.1
Measles 34 2.7 4.6
Other 21 1.7 2.8
Total 1248 100 181
S632 d JID 2011:204 (Suppl 2) d de Moraes et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
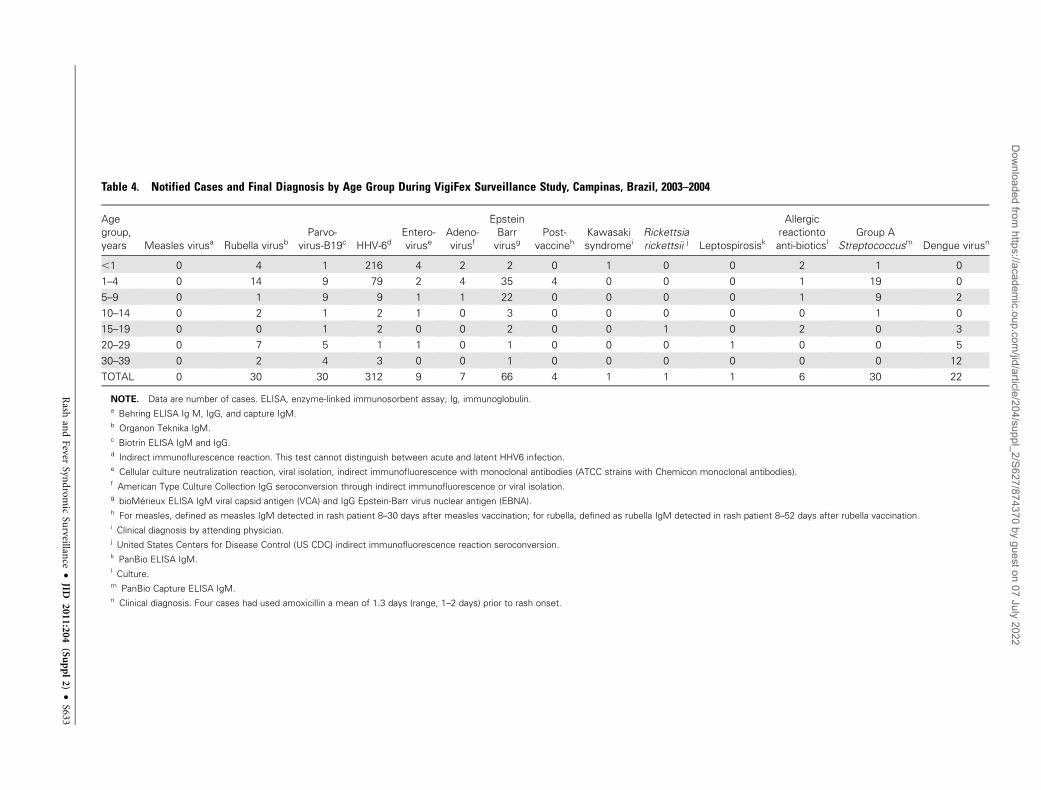
Table 4. Notified Cases and Final Diagnosis by Age Group During VigiFex Surveillance Study, Campinas, Brazil, 2003–2004
Age
group,
years Measles virusa Rubella virusbParvo-
virus-B19c HHV-6dEntero-
viruseAdeno-
virusf
Epstein
Barr
virusgPost-
vaccinehKawasaki
syndromeiRickettsia
rickettsii j Leptospirosisk
Allergic
reactionto
anti-bioticslGroup A
Streptococcusm Dengue virusn
,1 0 4 1 216 4 2 2 0 1 0 0 2 1 0
1–4 0 14 9 79 2 4 35 4 0 0 0 1 19 0
5–9 0 1 9 9 1 1 22 0 0 0 0 1 9 2
10–14 0 2 1 2 1 0 3 0 0 0 0 0 1 0
15–19 0 0 1 2 0 0 2 0 0 1 0 2 0 3
20–29 0 7 5 1 1 0 1 0 0 0 1 0 0 5
30–39 0 2 4 3 0 0 1 0 0 0 0 0 0 12
TOTAL 0 30 30 312 9 7 66 4 1 1 1 6 30 22
NOTE. Data are number of cases. ELISA, enzyme-linked immunosorbent assay; Ig, immunoglobulin.a Behring ELISA Ig M, IgG, and capture IgM.b Organon Teknika IgM.c Biotrin ELISA IgM and IgG.d Indirect immunoflurescence reaction. This test cannot distinguish between acute and latent HHV6 infection.e Cellular culture neutralization reaction, viral isolation, indirect immunofluorescence with monoclonal antibodies (ATCC strains with Chemicon monoclonal antibodies).f American Type Culture Collection IgG seroconversion through indirect immunofluorescence or viral isolation.g bioMerieux ELISA IgM viral capsid antigen (VCA) and IgG Epstein-Barr virus nuclear antigen (EBNA).h For measles, defined as measles IgM detected in rash patient 8–30 days after measles vaccination; for rubella, defined as rubella IgM detected in rash patient 8–52 days after rubella vaccination.i Clinical diagnosis by attending physician.j United States Centers for Disease Control (US CDC) indirect immunofluorescence reaction seroconversion.k PanBio ELISA IgM.l Culture.m PanBio Capture ELISA IgM.n Clinical diagnosis. Four cases had used amoxicillin a mean of 1.3 days (range, 1–2 days) prior to rash onset.
Rash
and
Fever
Synd
rom
icSu
rveillance
dJID
2011:204(Suppl2)
dS633
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

attributable to parvovirus B19, compared with 9%–19% in
other studies, whereas 25% of our cases were attributed to
HHV-6 in contrast to the 2%–12% reported elsewhere [1, 3–5].
Nonetheless, the age distributions of both HHV-6 and parvo-
virus cases were similar to those previously described [1, 3].
Our findings may reflect regional and temporal variations in
febrile-rash illnesses; however, they may also be influenced by
testing limitations. We diagnosed HHV6 using IgM indirect
immunofluorescence. However, HHV-6 is a ubiquitous in-
fection that may be acute or latent, and establishing a link be-
tween HHV-6 and acute rash and fever illness remains
a challenge because there is no gold-standard diagnostic test that
can distinguish between latent infection and active viral repli-
cation [33, 34]. Viral isolation is the only test that can reliably
distinguish between these 2 states; however, it lacks sensitivity
and is not practical on a population basis [35].
We identified 3 school-based clusters of GAS. Treatment of
GAS can prevent rheumatic heart disease, a documented cause
of economic burden in Brazil [36].
Almost three-quarters of the rubella cases detected through
laboratory testing were not suspected on clinical grounds, in most
part because they did not meet the case definition. Of 30 patients
with confirmed rubella, 20 did not present with lymphadenopa-
thy, which is included in the rubella case definition. These data
demonstrate that clinical case definition for rubella in place in
Brazil [12, 13] and recommended by WHO [37] may lack
sensitivity for settings with rubella and CRS elimination goals.
To our knowledge, this is also the only study designed to
assess the value and feasibility of a recommended minimum
reporting rate for suspected measles and rubella as a surveillance
indicator in settings of measles and rubella elimination. Our
study found a notification rate for all febrile-rash illness of
181 cases per 100 000 population aged ,40 years.
The overall notification rate of suspected measles (4.6) or
rubella (27.1) cases by presumptive clinical diagnosis was 31.6
cases per 100 000 population aged ,40 years. Notification rates
of suspected measles and rubella cases that would meet the
standardized clinical case definitions were 105.2 and 42.5 cases
per 100 000 population aged ,40 years, respectively. All of the
aforementioned reporting rates far exceeded the proposed in-
dicator of $2 suspected measles or rubella cases cases per
100 000 population adequately investigated to monitor surveil-
lance sensitivity [14]. Although the feasibility of meeting this
benchmark has been questioned in diverse settings, our findings
demonstrate that implementing enhanced surveillance was fea-
sible at a reasonable additional cost in a setting with a well-
structured surveillance system of a developing country with an
intermediate per-capita income level.
In fact, our data raise the question of whether a reporting rate
of 2 cases per 100 000 population is sensitive enough to detect
virus circulation in regions where measles elimination has been
achieved and where rubella and CRS elimination is in progress,
such as the Americas. Additional assessments that consider
surveillance data from other countries will be needed to assess
whether this benchmark is adequate.
This study highlights the importance of incorporating the
private sector into surveillance activities. The expansion of no-
tification to all rash and fever illnesses and outreach efforts to
private health care facilities during VigiFex resulted in a marked
increase in notifications, particularly from private and university
facilities. However, the proportion of total notifications coming
from them remained low, and their participation throughout
the study was difficult to maintain.
More than 30% of the incremental costs associated with en-
hanced surveillance implemented in this study were related to
expenses for necessary laboratory tests. Approximately 20% of
all laboratory costs were used to purchase diagnostic material for
enterovirus and HHV-6. It may not be feasible to recommend
routine testing for all fever-rash cases as broadly as was done in
this study because of the high costs and difficulties associated
with this method.
This study had several limitations. Because it was confined to
a 13-month period, the average contribution of specific diseases
with multiyear epidemic cycles, such as dengue, to rash-fever ill-
ness in Campinas may have been either over- or underestimated.
Furthermore, some persons with cases of fever-rash illness
undoubtedly remained at home; because this study was facility
based, these cases would have gone undetected. As previously
mentioned, the proportion of fever and rash that could truly be
attributed to HHV-6 is questionable due to the limitations of the
HHV-6 testing available.
CONCLUSIONS AND RECOMMENDATIONS
Variations in measles and rubella case definitions and the stage
of control will likely influence measles and rubella detection
rates through surveillance. Because the current clinical case
definition for rubella lacks sensitivity, rubella testing may be
considered for all cases of febrile-rash illness, regardless of sus-
pected clinical diagnosis, in settings with rubella elimination
goals. Because enhanced surveillance allowed the identification
of disease clusters that would otherwise remain undetected,
making outbreak-associated GAS a notifiable disease in the
country should be considered.
Reaching the currently recommended febrile-rash illness no-
tification rate is achievable and affordable. Additional evaluation
will be needed after data are made available from countries using
this indicator in the context of measles elimination.
Finally, our findings suggest that stimulating a well-functioning
surveillance system through enhanced rash and fever surveillance
would allow reporting of potential measles cases and additional
rubella cases that may have gone unnoticed considering current
clinical surveillance case definitions and regular rubella and
measles surveillance.
S634 d JID 2011:204 (Suppl 2) d de Moraes et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

Funding
This work was supported by the US Centers for Disease Control and
Prevention and the Pan American Health Organization. Laboratory and
surveillance personnel were funded by the municipal and state health de-
partment. The Campinas Medicine and Surgery Society, State University
of Campinas (UNICAMP), and PUC-Campinas University provided funds
for the communication strategies and the symposium.
Acknowledgments
The authors have submitted this manuscript on behalf of the VigiFex
Group, whose participants are listed below:
Claudia Bento Safi, Fabiana Medeiros Lopes de Oliveira, Genoefa
Aparecida Casagrande, Maria Alice Sato, Maria Cristina Siqueira M. Prini,
Mariza Natalina dos Santos, Neuza Teles de Lima Martins, Thais Fernanda
Degan, Municipal Health Department, Campinas; Marcia Regina Pacola,
Regional Direction for Surveillance, DIR XII Campinas Sao Paulo State
Health Department; Telma Regina Marques Pinto Carvalhanas, Neuma
Terezinha Rossetto Hidalgo, Flavia Helena Ciccone—Centers for Surveil-
lance, Sao Paulo State Health Department; Fernando R. de Barros, Tereza
Cristina Segatto—National Coordination for Respiratory Diseases Sur-
veillance, Brazilian Ministry of Health; Vania Martins Fontes Del Guercio,
Patrıcia Poletini—Regional Instituto Adolfo Lutz, Campinas; Luiza T. M.
Souza, Andrea Stangarlin, Suely Pires Curti, Cristina Adelaide Figueiredo,
Marcia Theobaldo, Maria Isabel de Oliveira, Ivani Bisordi Ferreira, Maria
Akiko Ishida, Terezinha Maria de Paiva, Maria do Carmo Sampaio Tavares
Timenetsky, Rita de Cassia Carmona Compagnoli, Denise Hage Russo,
Adriana Luchs, Aurea Silveira da Cruz, Silvia Colombo, Maria Cristina de
Cunto Brandileone, Instituto Adolfo Lutz, Sao Paulo.
This study was carried out in accordance with the Declaration of Hel-
sinki as revised in 2000, and approved by the Ethics Committee of the
Instituto Adolfo Lutz-Sao Paulo. Study participants were not required to
provide informed consent as this study was considered by the Ethics
Committee to be part of routine surveillance activities.
References
1. Ramsay M, Reacher M, O’Flynn C, et al. Causes of morbilliform rash in
a highly immunised English population. Arch Dis Child 2002; 87:202–6.
2. Shirley JA, Revill S, Cohen BJ, Buckley MM. Serological study of
rubella-like illnesses. J Med Virol 1987; 21:369–79.
3. Davidkin I, Valle M, Peltola H, et al. Etiology of measles- and rubella-
like illnesses in measles, mumps, and rubella-vaccinated children.
J Infect Dis 1998; 178:1567–70.
4. Papania M, Bromberg K, Grabowsky M, Bellini W, Stewart J, Erdman D.
Differential diagnosis of febrile rash illness in children, Brooklyn, 1994
[abstract K748]. In: Program and abstracts of the 36th Interscience
Conference on Antimicrobial Agents and Chemotherapy. Washington,
DC: American Society for Microbiology, 1996.
5. Oliveira SA, Siqueira MM, Camacho LA, et al. The aetiology of mac-
ulopapular rash diseases in Niteroi, State of Rio de Janeiro, Brazil: im-
plications for measles surveillance. Epidemiol Infect 2001; 127:509–16.
6. Nordin JD, Harpaz R, Harper P, Rush W. Syndromic surveillance for
measleslike illnesses in a managed care setting. J Infect Dis 2004;
189(Suppl 1):S222–S226.
7. de Quadros CA, Izurieta H, Venczel L, Carrasco P. Measles eradication in
the Americas: progress to date. J Infect Dis 2004; 189(Suppl 1):S227–S235.
8. Pan American Health Organization. Vaccines and Immunizations—
Morbidity Tables. Washington, DC: PAHO, 2006.
9. Pan American Health Organization. Immunization in the Americas—
Summary 2005. Washington, DC: PAHO, 2005.
10. Ministerio da Saude, Brasil. Casos confirmados de rubeola. Brasil e
Grandes Regioes, 1997–2006. Brasılia: Ministerio da Saude, 2007.
11. Pan American Health Organization (PAHO). Sustaining Immunization
Programs—Elimination of rubella and congenital rubella syndrome
(CRS). In: 44th Directing Council CD44/11. Washington, DC: PAHO,
2003.
12. BRASIL.Fundacxao Nacional de Saude. Guia de Vigilancia
Epidemiologica. II, 5th ed. Brasilia: FUNASA, 2002.
13. BRASIL.Ministerio da Saude. Secretaria de Vigilancia em Saude.
Manual de Vigilancia para a Erradicacxao do Sarampo, Controle da
Rubeola e Eliminacxao da Sındrome da Rubeola Congenita (SRC), 3rd
ed. Brasilia: Secretaria de Vigilancia em Saude, 2003.
14. Pan American Health Organization (PAHO). Plan of action for the
documentation and verification of measles, rubella, and congenital rubella
syndrome elimination in the Region of the Americas. Washington, DC:
PAHO, 2009.
15. Kemp B, Toscano C, Barros ENC, Barros FR, Moraes JC. Incorporacxao do
setor privado de saude no sistema de vigilancia epidemiologica de febre e
exantema em Campinas /SP: Licxoes aprendidas. In: Anais do 11� CON-
GRESSO MUNDIAL DE SAUDE PUBLICA E 8� CONGRESSO BRASI-
LEIRO DE SAUDE COLETIVA. Rio de Janeiro, Brazil: ABRASCO, 2006.
16. Barros ENC. Praticas em Vigilancia Epidemiologica: Maneiras de Ver e
Fazer. [Dissertacxao de Mestrado]. Campinas (SP): Universidade Es-
tadual de Campinas, 2004.
17. Pan American Health Organization. Classification of suspect measles/
rubella cases as ‘‘vaccine-related’’: compliance with PAHO recom-
mendations. In: Immunization Newsletter. Vol 28. Washington, DC:
Pan American Health Organization, 2006:5.
18. Innis BL, Nisalak A, Nimmannitya S, et al. An enzyme-linked im-
munosorbent assay to characterize dengue infections where dengue
and Japanese encephalitis co-circulate. Am J Trop Med Hyg 1989; 40:
418–27.
19. Ratnam S, Tipples G, Head C, Fauvel M, Fearon M, Ward BJ. Per-
formance of indirect immunoglobulin M (IgM) serology tests and IgM
capture assays for laboratory diagnosis of measles. J Clin Microbiol
2000; 38:99–104.
20. Tipples GA, Hamkar R, Mohktari-Azad T, et al. Assessment of im-
munoglobulin M enzyme immunoassays for diagnosis of measles. J
Clin Microbiol 2003; 41:4790–2.
21. Hesketh L, Charlett A, Farrington P, Miller E, Forsey T, Morgan-
Capner P. An evaluation of nine commercial EIA kits for the detection
of measles specific IgG. J Virol Methods 1997; 66:51–9.
22. Revello MG, Percivalle E, Zavattoni M, Gerna G. Rubella IgM antibody
determination: comparison of two indirect and two capture com-
mercial enzyme immunoassays. Microbiologica 1987; 10:393–401.
23. Bruu AL, Nordbo SA. Evaluation of five commercial tests for detection
of immunoglobulin M antibodies to human parvovirus B19. J Clin
Microbiol 1995; 33:1363–5.
24. Doyle S, Kerr S, O’Keeffe G, O’Carroll D, Daly P, Kilty C. Detection
of parvovirus B19 IgM by antibody capture enzyme immunoassay:
receiver operating characteristic analysis. J Virol Methods 2000; 90:
143–52.
25. Wildig J, Michon P, Siba P, et al. Parvovirus B19 infection contributes
to severe anemia in young children in Papua New Guinea. J Infect Dis
2006; 194:146–53.
26. Takimoto S, Grandien M, Ishida MA, et al. Comparison of enzyme-
linked immunosorbent assay, indirect immunofluorescence assay, and
virus isolation for detection of respiratory viruses in nasopharyngeal
secretions. J Clin Microbiol 1991; 29:470–4.
27. Bruu AL, Hjetland R, Holter E, et al. Evaluation of 12 commercial tests
for detection of Epstein-Barr virus-specific and heterophile antibodies.
Clin Diagn Lab Immunol 2000; 7:451–6.
28. Philip RN, Casper EA, MacCormack JN, et al. A comparison of sero-
logic methods for diagnosis of Rocky Mountain spotted fever. Am
J Epidemiol 1977; 105:56–67.
29. Bastis D, Simonet S, Patterson MA, Neill S. Identification of enter-
oviruses by indirect immunofluorescence using monoclonal anti-
bodies. Clin Diagn Virol 1995; 3:83–93.
30. Rigonan AS, Mann L, Chonmaitree T. Use of monoclonal antibodies
to identify serotypes of enterovirus isolates. J Clin Microbiol 1998; 36:
1877–81.
Rash and Fever Syndromic Surveillance d JID 2011:204 (Suppl 2) d S635
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022

31. Facklam RR, Washington JA II. Streptococcus and related catalase-
negative Gram positive cocci. In Balows A, Hausler WJ Jr, Hermann
KL, Isenberg HD, Shadomy HJ eds. Washington, DC: American Society
for Microbiology, 1991:238–57.
32. Dean AD, Dean JA, Burton JH, Dicker RC. Epi Info, version 6.04:
a word processing, database, and statistics program for epidemiology
on microcomputers. [version 6.04]. Atlanta, GA: Centers for Disease
Control and Prevention, 1998.
33. Caserta MT, McDermott MP, Dewhurst S, et al. Human herpesvirus
6 (HHV6) DNA persistence and reactivation in healthy children.
J Pediatr 2004; 145:478–84.
34. Carrigan DR, Knox KK. Human herpesvirus 6: diagnosis of active
infection. Am Clin Lab 2000; 19:12.
35. Bland RM, Mackie PL, Shorts T, Pate S, Paton JY. The rapid di-
agnosis and clinical features of human herpesvirus 6. J Infect 1998;
36:161–5.
36. Terreri MT, Ferraz MB, Goldenberg J, Len C, Hilario MO. Resource
utilization and cost of rheumatic fever. J Rheumatol 2001; 28:1394–7.
37. World Health Organization (WHO)/Department of Vaccines and Bi-
ologicals/Vaccine Assessment and Monitoring Team. Guidelines for
surveillance of congenital rubella syndrome and rubella. WHO/V&B/
99.22. Geneva, Switzerland: WHO, 1999.
S636 d JID 2011:204 (Suppl 2) d de Moraes et al
Dow
nloaded from https://academ
ic.oup.com/jid/article/204/suppl_2/S627/874370 by guest on 07 July 2022
Related Documents











