For personal use. Only reproduce with permission from The Lancet Publishing Group. THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 618 Current malaria-control strategies emphasise domestic protection against adult mosquitoes with insecticides, and improved access to medical services. Malaria prevention by killing adult mosquitoes is generally favoured because moderately reducing their longevity can radically suppress community-level transmission. By comparison, controlling larvae has a less dramatic effect at any given level of coverage and is often more difficult to implement. Nevertheless, the historically most effective campaign against African vectors is the eradication of accidentally introduced Anopheles gambiae from 54 000 km 2 of largely ideal habitat in northeast Brazil in the 1930s and early 1940s. This outstanding success was achieved through an integrated programme but relied overwhelmingly upon larval control. This experience was soon repeated in Egypt and another larval control programme successfully suppressed malaria for over 20 years around a Zambian copper mine. These affordable approaches were neglected after the advent of dichlorodiphenyltrichloroethane (DDT) and global malaria- control policy shifted toward domestic adulticide methods. Larval-control methods should now be re-prioritised for research, development, and implementation as an additional way to roll back malaria. Lancet Infect Dis 2002; 2: 618–27 The rise, fall, and recovery of malaria vector control in Africa Current malaria-control strategies emphasise domestic protection against adult mosquitoes with insecticides and improved access to medical services. 1–8 Malaria prevention by killing adult mosquitoes is generally favoured because of the relative ease with which houses can be identified and mapped, as well as the exquisite sensitivity of transmission intensity to the mortality rate of adult female mosquito vectors. 5,9–14 To transmit malaria a mosquito must ingest infectious gametocyte forms of the malaria parasite from an infected person, survive long enough for these to successfully transform into infectious sporozoites, and then bite another susceptible human host. 15 For Plasmodium falciparum, the most dangerous and prevalent human malaria parasite in Africa, this process takes a minimum of 10 days and usually longer. 15 Thus, increasing the mortality rate of mosquitoes entering houses can substantially suppress malaria transmission in whole communities. 16–22 By Historical review Eradication of Anopheles gambiae from Brazil GFK is an ecological epidemiologist at the Department of Public Health and Epidemiology, Swiss Topical Institute, Basel, Switzerland, and adjunct assistant professor at the Department of Tropical Medicine, School of Public Health and Tropical Medicine, Tulane University Health Sciences Centre, New Orleans, Louisiana, USA; UF and LCG are medical entomologists at Mbita Point Research and Training Centre, International Center of Insect Physiology and Ecology, Mbita, Suba District, Nyanza Province, Kenya; IK is the Malaria and HIV/AIDS Coordinator at Rusinga Island Child and Family Programme, The Christian Children’s Fund, Rusinga Island, Suba District, Kenya; and BGJK is a medical entomologist and visiting scientist at the Laboratory of Entomology, Wageningen University Research Centre, Wageningen, Netherlands. Correspondence: Dr Gerry F Killeen, Department of Public Health and Epidemiology, Swiss Tropical Institute, Socinstrasse 57, PO Box CH-4002, Basel, Switzerland. Tel+41 (0)61 2848284; fax: +41 (0)61 2717951; email [email protected] Eradication of Anopheles gambiae from Brazil: lessons for malaria control in Africa? Gerry F Killeen, Ulrike Fillinger, Ibrahim Kiche, Louis C Gouagna, and Bart G J Knols Figure 1. The range and physical geography of habitats infested by A gambiae in Brazil. Reproduced from reference 79.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com618
Current malaria-control strategiesemphasise domestic protection againstadult mosquitoes with insecticides, and improved access to medicalservices. Malaria prevention by killingadult mosquitoes is generally favouredbecause moderately reducing theirlongevity can radically suppresscommunity-level transmission. Bycomparison, controlling larvae has a less dramatic effect at any given level of coverage and is often moredifficult to implement. Nevertheless, thehistorically most effective campaignagainst African vectors is theeradication of accidentally introducedAnopheles gambiae from 54 000 km2
of largely ideal habitat in northeastBrazil in the 1930s and early 1940s. Thisoutstanding success was achievedthrough an integrated programme butrelied overwhelmingly upon larvalcontrol. This experience was soonrepeated in Egypt and another larvalcontrol programme successfullysuppressed malaria for over 20 yearsaround a Zambian copper mine. These affordableapproaches were neglected after the advent ofdichlorodiphenyltrichloroethane (DDT) and global malaria-control policy shifted toward domestic adulticide methods.Larval-control methods should now be re-prioritised forresearch, development, and implementation as an additionalway to roll back malaria.
Lancet Infect Dis 2002; 2: 618–27
The rise, fall, and recovery of malaria vectorcontrol in AfricaCurrent malaria-control strategies emphasise domesticprotection against adult mosquitoes with insecticides andimproved access to medical services.1–8 Malaria preventionby killing adult mosquitoes is generally favoured because ofthe relative ease with which houses can be identified andmapped, as well as the exquisite sensitivity of transmissionintensity to the mortality rate of adult female mosquitovectors.5,9–14 To transmit malaria a mosquito must ingestinfectious gametocyte forms of the malaria parasite from an infected person, survive long enough for these to
successfully transform into infectious sporozoites, and thenbite another susceptible human host.15 For Plasmodiumfalciparum, the most dangerous and prevalent humanmalaria parasite in Africa, this process takes a minimum of10 days and usually longer.15 Thus, increasing the mortalityrate of mosquitoes entering houses can substantiallysuppress malaria transmission in whole communities.16–22 By
Historical review Eradication of Anopheles gambiae from Brazil
GFK is an ecological epidemiologist at the Department of PublicHealth and Epidemiology, Swiss Topical Institute, Basel,Switzerland, and adjunct assistant professor at the Department ofTropical Medicine, School of Public Health and Tropical Medicine,Tulane University Health Sciences Centre, New Orleans, Louisiana,USA; UF and LCG are medical entomologists at Mbita PointResearch and Training Centre, International Center of InsectPhysiology and Ecology, Mbita, Suba District, Nyanza Province,Kenya; IK is the Malaria and HIV/AIDS Coordinator at Rusinga IslandChild and Family Programme, The Christian Children’s Fund,Rusinga Island, Suba District, Kenya; and BGJK is a medicalentomologist and visiting scientist at the Laboratory of Entomology,Wageningen University Research Centre, Wageningen, Netherlands.
Correspondence: Dr Gerry F Killeen, Department of Public Healthand Epidemiology, Swiss Tropical Institute, Socinstrasse 57, PO Box CH-4002, Basel, Switzerland. Tel+41 (0)61 2848284; fax: +41 (0)61 2717951; email [email protected]
Eradication of Anopheles gambiae from Brazil:lessons for malaria control in Africa?
Gerry F Killeen, Ulrike Fillinger, Ibrahim Kiche, Louis C Gouagna, and Bart G J Knols
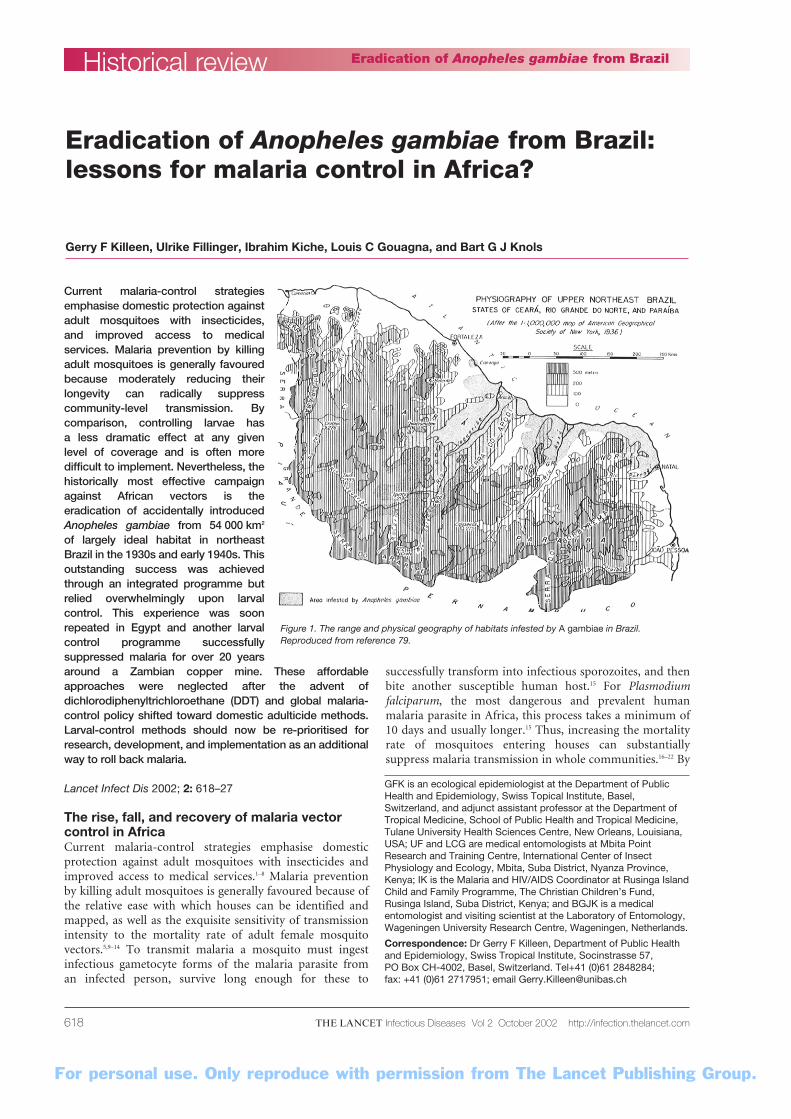
Figure 1. The range and physical geography of habitats infested by A gambiae in Brazil.Reproduced from reference 79.

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 619
comparison, controlling larvae has a less dramatic, directlylinear effect on transmission and larval habitats are oftenmore difficult to identify than houses.9–14 Although RonaldRoss himself was the first to highlight the sensitivity ofmalaria transmission to any measure that shortened the livesof adult mosquitoes,23 he was also quick to realise that thelimited mobility and focal concentration of their aquaticstages rendered them much more susceptible to attack:24
“The most vulnerable point in the history of gnats is whenthey are larvae; they can be destroyed wholesale”, he wrote.25
Up until World War II, programmes for malaria controlthrough environmental management and regular larvicidaltreatment of breeding sites were successfully developedacross Europe, Asia, and the Americas.5,9,26–28 The suppressionand even eradication of malaria from vast areas has beenattributed to determined large-scale programmes to killimmature Anopheles species vectors or reduce the amount of suitable habitat for them in proximity to vulnerablehuman populations.26–29 However, the advent ofdichlorodiphenyltrichloroethane (DDT) may have misledthe malaria-control community into the idea that malariacould be controlled and even eradicated by almostexclusively targeting adult mosquitoes with syntheticinsecticides.28,30–33 Such was the enthusiasm for indoor-residual spraying that alternatives were abandoned,neglected, and marginalised.5,9,10,28,31–33 Sadly, the earlyoptimism arising from DDT’s outstanding properties as aninsecticide were premature and the campaign to eradicatemalaria is often anecdotally credited with exterminatingmedical entomologists rather than parasites or vectors.10,28,31–33
Encouraging predictions of malaria eradication12,30 weresuccessfully achieved in southern Europe, the USSR, Taiwan,the USA, and parts of the Caribbean, Venezuela, China,Madagascar, and South Africa.3,8,9,20,21,28,31,32,34 Additionally,DDT has been credited with wholesale suppression and evencomplete disappearance of vector species such as Anophelessergenti and Anopheles funestus from sizeable areas of Egypt,South Africa, Madagascar and Mauritius.3,8,9,20,21,28,31,32,34–36
However, eradication or even substantial suppression ofmalaria transmission could not be realised in many part ofthe tropics because of shortcomings in political will andlimited resources,28,31,32 as well as fundamental biologicalobstacles such as the avoidance of excito-repellentinsecticides, inter-species differences in behaviour, and thepotential for resistance among mosquito vectors.24,32,33,37,38
Although intra-domiciliary insecticides remain powerfuland indispensable tools for malaria control,2,3,6–9,34,39–42
even these superb interventions often fall short of theefficacy levels required to eradicate malaria in tropicalsettings. 13,22,24,28,42–45 Today malaria remains robustly endemicacross most of the tropics, especially sub-Saharan Africawhere human populations, ideal climatic conditions,46,47 andexceedingly efficient vectors mediate transmission intensitiesup to 1000-fold higher than required to maintain it.44,48
It took many years for the credibility of vector-control ofmalaria in Africa to recover from the acceptance that theaims of the Global Eradication Campaign could not beachieved, even with DDT.28,31,32 Fortunately, persistentdevelopment and testing of bednets as an alternative means
for applying insecticides in houses proved successful over thepast decade42 and has restored confidence in malariaprevention through vector control in Africa. Nowadays, theefficacy of indoor spraying and bednets is clearly establishedand the number of lives that they could save if appliedubiquitously is undoubtedly huge.8,42,43,46,47
Why are bednets and clinical management notenough?Although indoor spraying and bednets can reduce exposureby at least an order of magnitude,13,16–19,22 they often havelimited clinical impact when faced with intense transmissionby African vectors.13,42 The Garki project carefully examinedthe effects of intensive domestic insecticide spraying innorthern Nigeria during the early 1970s and marked amilestone in epidemiological entomology that is bestreflected in its objectives as explained in the foreword of itspublished report: “It was essential to know what could orcould not be achieved and, as far as possible, to find out whythat was so; and it was therefore considered justified to applycontrol measures and methods of supervision that were moreexpensive than would be acceptable in a control program.”22
The Garki project revealed that indoor spraying was indeedhighly effective in reducing the ability of the vectorpopulation to transmit malaria but that this simply was notenough to destabilise transmission in the savannah ofnorthern Nigeria.22 Subsequent empirical and theoreticalstudies have confirmed that many parts of sub-SaharanAfrica will require determined integration of highly effectivevector control with vastly improved surveillance andtreatment of infected individuals.13,43–45 High levels ofabsolute coverage, in terms of the human population,24 withbednets are often difficult to achieve in practice,49–51 with costand delivery mechanism being critical determinants ofsuccess.39,40,49,52–55 Furthermore, the ability of vectors to avoidmany domestic insecticide interventions can compromisetheir effective coverage of the target vector population.24,37
The availability of healthcare services for diagnosis andtreatment is crucial to minimising the mortality riskassociated with exposure to malaria-infected mosquitoes,but can do little to limit the incidence of clinical malaria inareas of high transmission because it deals only with malariainfections after they occur and has minimal impact on theinfectiousness of the human reservoir.10,13 Large-scaleprophylaxis has played a significant role in some notablysuccessful control programmes,9,21,27,35,36,56,57 but may also havelimited impacts and even quite dangerous consequencessuch as the emergence of drug resistance58,59 or even theintensification of transmission.60–63 Even intensive infectioncontrol with active detection, drug treatment, and follow upcannot eliminate endemic malaria from most parts of sub-Saharan Africa unless rapid re-infection can be prevented byeffective vector control.10,13,44,45
Malaria transmission is much more difficult to control inAfrica than most other places because poor healthinfrastructure allows chronic P falciparum infections tosurvive undisturbed in human hosts until they aretransmitted by long-lived and anthropophilic vectors thatare the most efficient in the world.10,13,44 Untreated and drug-
Historical reviewEradication of Anopheles gambiae from Brazil

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com620
resistant malaria infections can persist in human beings formonths or years,64–68 and vectors such as Anopheles gambiaeGiles, Anopheles arabiensis Patton, and A funestus Giles thatpick up parasites are more likely than any others to surviveand pass them on to another victim. Thus, stable endemicmalaria can manifest itself in sub-Saharan Africa wherepeople are exposed to less than one mosquito bite per weekand transmission is undetectable.44 Clearly, if our ambitionsfor malaria control in Africa are to go beyond attenuatingtransmission and minimising the effects of its consequences,truly integrated control, combining all tools at our disposal,will be necessary.10,13,29,45,69 Larval control has long been anoption for malaria control,9,27,29,70 but we suggest that this is agrossly underdeveloped and underused approach,particularly in tropical Africa where it may be of muchgreater utility than generally appreciated.
Back to the future: reconsidering larval controlof African malaria vectorsGiven that the most commonly advocated malaria controltools for protecting against adult mosquitoes have clearlimitations, it is worth considering other technologies, not asalternatives but rather as possible additions to integratedprogrammes.10,13,27,29,45,69,70 Currently, the development ofsophisticated approaches to malaria control, such astransmission-blocking vaccines and genetically modifiedmosquitoes, are being vigorously advocated andpursued.33,71,72 These approaches are unlikely to bear fruit forseveral years and their likelihood of success has beenquestioned.73–77 In this context, it may be useful to reconsiderthe simple control tools that enabled the most historicallysuccessful attempts to control malaria transmission byA gambiae,78,79 before such approaches were abandoned infavour of modern synthetic adulticides.
Although other examples of successful wholesalesuppression of African malaria vectors do exist, the completeeradication of accidentally introduced A gambiae from thenortheast coast of Brazil79 and the Nile Valley of Egypt78 areparticularly notable. These are the only campaigns that haveever succeeded in completely eliminating a major Africanmalaria vector species from areas spanning hundreds ofkilometres. One can only conclude that, in both these cases,100% effective coverage was achieved because every lastmosquito was removed and no specimen of A gambiae hasbeen recorded at either site over the six subsequent decades.Both of these campaigns were executed almost exclusively byrigorous, well-managed implementation of effective larvalcontrol and constitute outstanding examples of howeffective malaria control might be achieved at district,provincial, and national scales in modern Africa.78,79
The rise and fall of A gambiae in BrazilThe most effective documented campaign against Africanmalaria vectors is undoubtedly the unprecedentederadication of accidentally introduced A gambiae fromapproximately 54 000 km2 of northeast Brazil in the face ofseemingly impossible odds and overwhelming scepticism.Wisely, the invasion of Brazil by A gambiae and subsequentevents were meticulously recorded by Soper and Wilson in
their book, succinctly entitled Anopheles gambiae in Brazil:1930 to 1940.79 Here we summarise the events that led up tothe eradication campaign and highlight the most importantfactors that contributed to the unforeseen andoverwhelming success of this endeavour.
The arrival of A gambiae sensu lato in Brazil was firstdiscovered in March 1930 when approximately 2000 larvaewere collected within a kilometre of the port of Natal wherewarships carrying mail from west Africa regularlyanchored.80 It is notable that this first observation was not anaccidental one but occurred during an entomological surveyof the Yellow Fever Programme that eliminated Aedesaegypti Linneus from most of Latin America81 and formedthe basis of the subsequent campaign that succeeded againstA gambiae. In 1930, it was not yet known that freshwater A gambiae is in fact a cryptic species complex,82 andsubsequent efforts to apply modern molecular methods tomuseum specimens have not succeeded (W Takken,Wageningen University Research Centre, Wageningen,Netherlands, personal communication), so we do not knowwhether the species in question was actually A gambiae sensustricto Giles or A arabiensis Patton. Fortunately, the state ofRio Grande do Norte, where A gambiae first established itselfin quite localised habitats such as flooded fields, provedotherwise quite inhospitable because of arid climate and welldrained soils.
The arrival of A gambiae was associated withunprecedented malaria epidemics in Natal: 28, 139, and 344 deaths in the town were attributed to malaria in 1929,1930, and 1931, respectively. A swift campaign by theBrazilian government, followed immediately, and used ParisGreen—a copper acetoarsenite—as a larvicide to eliminate A gambiae from the city but, crucially, not from thesurrounding area. The African mosquito slowly andinconspicuously spread westward to the wetter, morepopulated valleys of the Assú, Apodí, and Jaguaribe riverswhere widespread agricultural activity presented diverse andabundant opportunities for propagation (figure 1). Between1932 and 1937, this colonisation proceeded without anyserious outbreaks of malaria, allowing substantialpopulations of mosquitoes to develop before the inevitableepidemics finally arrived. A catastrophic malaria epidemic,comparable with the invasion of Mauritius by the sameinsect,36,83 hit northeast Brazil in 1938: “The human languageis far from adequate to describe the desolation which existedin the region, in which suffering, tears and mourning spreadtheir lugubrious mantle over thousands of graves. Thegeneral belief was that the Northeast would be depopulatedbecause those who did not die at once would abandon it”,reported the Gazeta de Noticias, Fortaleza of April 11, 1940.79
On August 5, 1938, the President of Brazil, GetulioVargas, decreed the immediate organisation of a newantimalaria service to tackle this emergency. The Braziliangovernment subsequently joined forces with the RockefellerFoundation and co-funded the subsequent AntimalariaService of the Northeast with a budget of about US$350 000,equivalent to US$3 200 000 in 1995. The new service, whichharnessed existing legislation and infrastructure, set up itsheadquarters in Fortaleza and immediately set about dealing
Historical review Eradication of Anopheles gambiae from Brazil

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 621
with the deluge of malaria patients, aswell as the control of the alienmosquito.
Although adult mosquitoes weretargeted by spraying of houses,automobiles, planes, and boats wereconducted, the bulk of the efforts tokill A gambiae focused upon theirlarvae: “The Malaria Service of theNortheast began its activities in 1939with no very clear cut program for theeradication of gambiae from Brazilother than to rely on Paris Green asmuch as possible, study the possibilityof using disinsectization of houses byspray insecticide, and work from theperiphery of the infested area towardthe centre”.79
Figure 2 illustrates the elegantsimplicity of the tools that enabled theeradication of malaria from Brazil:effective larvicide, abundant labour,close supervision, and adaptation to the ecology of the targetspecies. Although Green could not be applied today becauseof its established toxicity (there were almost 600 cases ofpoisoning during the Brazilian campaign, including threedeaths), it was highly effective at killing larval anopheles andcould be readily applied mixed with dust or sand, negatingthe need for oil or other bulky or expensive diluents. Thecombination of large numbers of field workers with shrewdand strictly enforced task-allocation and supervision systemsunderpinned the complete coverage achieved. Eachindividual field worker, known as a larval inspector, wasgiven a fixed area in which to identify and treat potentialbreeding sites and for which he alone was responsible. Everyinspector was allocated a reasonable area which was carefullymapped and both the inspector and the mosquitopopulation he faced were monitored regularly, using twoflags to mark where he had left the road and where he waslocated at any time. The campaign was designed to tackle Agambiae according to its ecological niche so inspectorscarried out their work on bicycles or on foot and wereequipped with clothing and hats appropriate to the hightemperatures. A gambiae prefers sunlit, generally quite smallbodies of water as larval habitats38,84–89 and these had to besearched for rigorously throughout the countryside inchallenging conditions.
The real secret behind the success of the Malaria Serviceof the Northeast was in the clearly defined and rigorousorganisation of its activities. A cartographic unit wasimmediately set up and the infested area was exhaustivelymapped and remapped using aerial photographs. Acommon laboratory and epidemiological section allowedcentralised training, surveillance, and decision-making.Although adulticide and medicinal measures were similarlyorganised, Soper and Wilson clearly emphasised theadministrative structure in relation to larval-controlactivities. The entire infested area was rationally divided intozones, defined as follows: “An antilarval zone represented
the area in which one man could apply larvicide to allpotential foci during one week”.79
The work of inspectors in their allocated zones wasclosely scrutinised and managed by a District ChiefInspector who was typically allocated only five zones forwhich they were held individually and solely responsible.The zones and districts were further aggregated andmanaged through administrative units termed posts anddivisions, both of which were headed by medical doctorswho could deal with the clinical aspects of the programme inaddition to vector control. A simple but inspired system offlags and on-site field documentation ensured that eachinspector was monitored on an almost hourly basis andcould be held unambiguously accountable for any lapses.Notably, the activities of the anti-larval and anti-adultcontrol teams were separately reported at district level sothat discrepancies could be identified, and separate adultcapture squads conducted independent evaluations of allvector-control activities by knockdown catches in houses ona monthly basis. Soper himself was a notoriously autocraticand demanding superior with an unambiguous approach topersonnel management: “Soper drove up in a car and askedHobbs to get in; Hobbs demurred, gesturing at his sweatyshirt. ‘Son,’ Soper responded, ‘we used to go out in a day likethis in Brazil and if we found a sector chief whose shirt wasnot wet we’d fire him’”.31
The vertical management methods applied in Brazil werenot particularly new and remain the mainstay of vectorcontrol in Europe, America, and Asia wherever mosquitoabatement is an everyday reality.9,27,28 However, theirapplication in this setting is especially notable because it iscommonly reasoned that such methods do not work forspecies like A gambiae because they prefer larval habitats thatare small, transient, and unpredictably scattered. We suggestthat this dogma needs to be seriously questioned because thedetermined and organised application of available resourcesin Brazil resulted in complete eradication from an area the
Historical reviewEradication of Anopheles gambiae from Brazil
Figure 2. The equipment and dailyactivities of a typical larvalinspector during the campaignthat eradicated A gambiae fromnortheast Brazil between 1939and 1940. Reproduced fromreference 79.
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com622
size of Togo: “gambiae was stopped in its career of invasion,was beaten back and finally eradicated from the knowninfested area . . . in less than two years time”.79
Indeed by mid-1940, the process of eradication fromBrazil was so well advanced that the programme voluntarilyreduced its own budget by 20% and eventually returnedsupplies worth US$175 000 (1995 US$1 600 000) to theBrazilian government. It is difficult to overstate themagnitude of these achievements or the scale of the disasteraverted: “There is no doubt that this invasion of gambiaethreatens the Americas with a catastrophe in comparisonwith which ordinary pestilence, conflagration or even warare but small and temporary calamities”, wrote Barber in1940.90
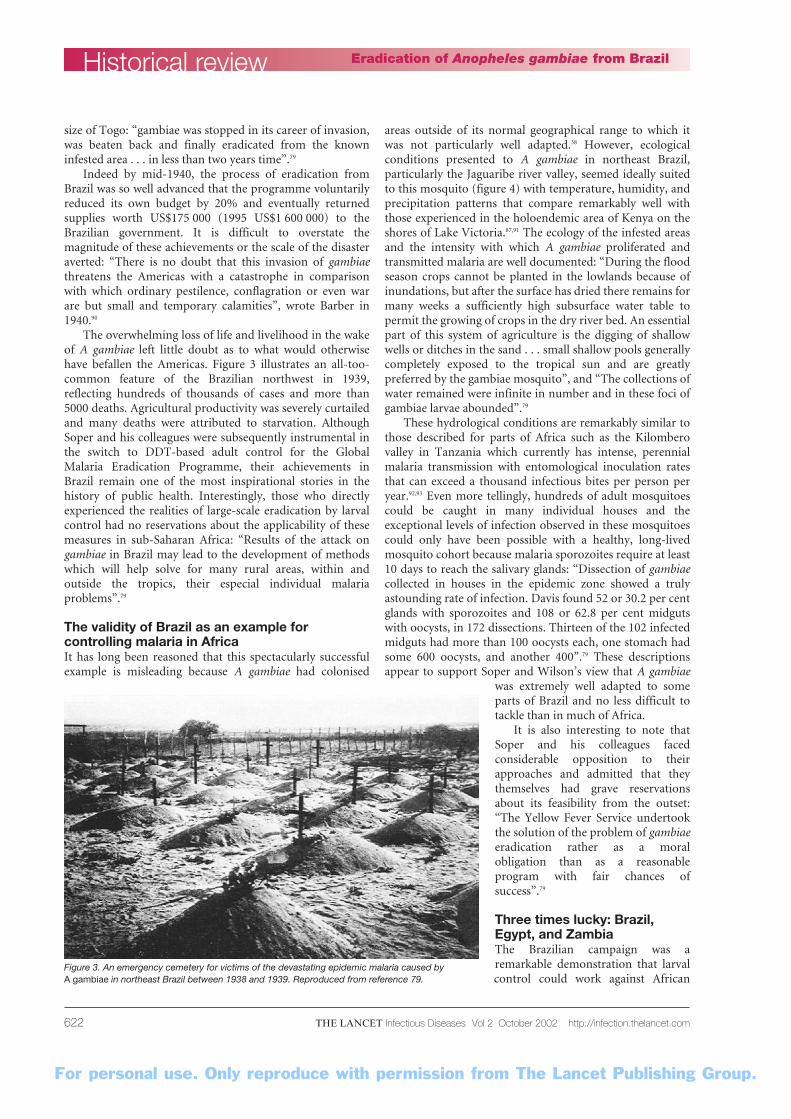
The overwhelming loss of life and livelihood in the wakeof A gambiae left little doubt as to what would otherwisehave befallen the Americas. Figure 3 illustrates an all-too-common feature of the Brazilian northwest in 1939,reflecting hundreds of thousands of cases and more than5000 deaths. Agricultural productivity was severely curtailedand many deaths were attributed to starvation. AlthoughSoper and his colleagues were subsequently instrumental inthe switch to DDT-based adult control for the GlobalMalaria Eradication Programme, their achievements inBrazil remain one of the most inspirational stories in thehistory of public health. Interestingly, those who directlyexperienced the realities of large-scale eradication by larvalcontrol had no reservations about the applicability of thesemeasures in sub-Saharan Africa: “Results of the attack ongambiae in Brazil may lead to the development of methodswhich will help solve for many rural areas, within andoutside the tropics, their especial individual malariaproblems”.79
The validity of Brazil as an example forcontrolling malaria in Africa It has long been reasoned that this spectacularly successfulexample is misleading because A gambiae had colonised
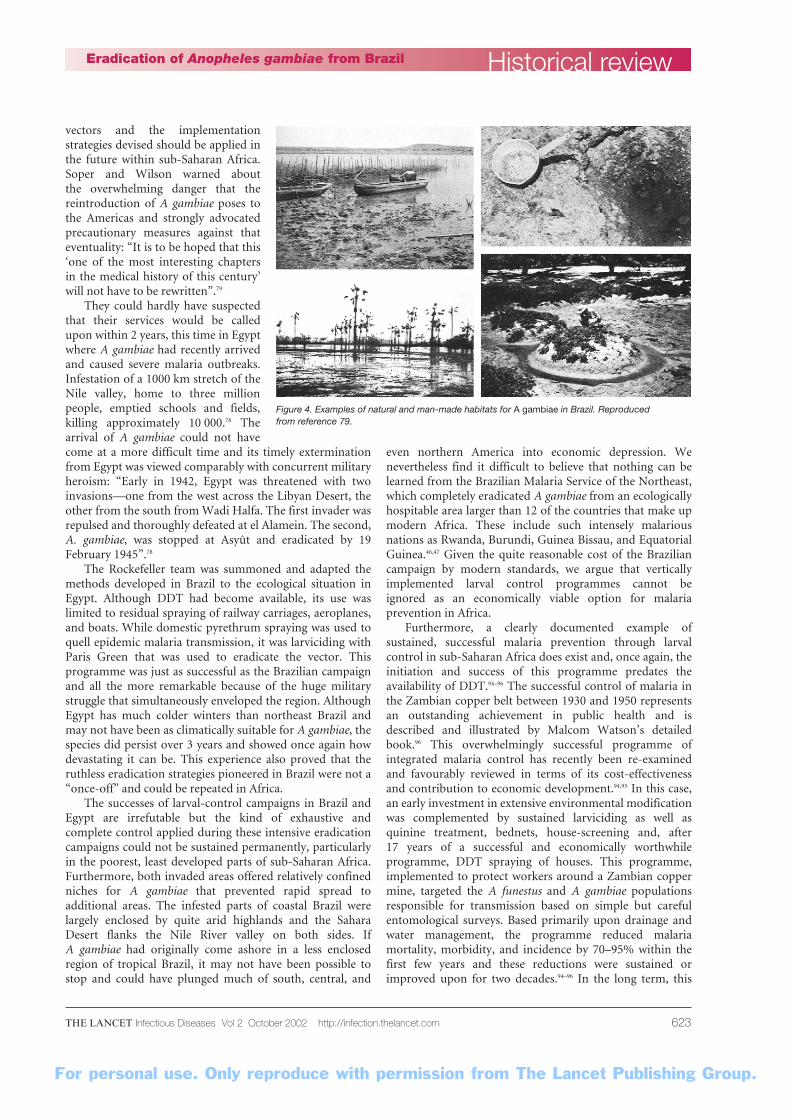
areas outside of its normal geographical range to which itwas not particularly well adapted.38 However, ecologicalconditions presented to A gambiae in northeast Brazil,particularly the Jaguaribe river valley, seemed ideally suitedto this mosquito (figure 4) with temperature, humidity, andprecipitation patterns that compare remarkably well withthose experienced in the holoendemic area of Kenya on theshores of Lake Victoria.87,91 The ecology of the infested areasand the intensity with which A gambiae proliferated andtransmitted malaria are well documented: “During the floodseason crops cannot be planted in the lowlands because ofinundations, but after the surface has dried there remains formany weeks a sufficiently high subsurface water table topermit the growing of crops in the dry river bed. An essentialpart of this system of agriculture is the digging of shallowwells or ditches in the sand . . . small shallow pools generallycompletely exposed to the tropical sun and are greatlypreferred by the gambiae mosquito”, and “The collections ofwater remained were infinite in number and in these foci ofgambiae larvae abounded”.79
These hydrological conditions are remarkably similar tothose described for parts of Africa such as the Kilomberovalley in Tanzania which currently has intense, perennialmalaria transmission with entomological inoculation ratesthat can exceed a thousand infectious bites per person peryear.92,93 Even more tellingly, hundreds of adult mosquitoescould be caught in many individual houses and theexceptional levels of infection observed in these mosquitoescould only have been possible with a healthy, long-livedmosquito cohort because malaria sporozoites require at least10 days to reach the salivary glands: “Dissection of gambiaecollected in houses in the epidemic zone showed a trulyastounding rate of infection. Davis found 52 or 30.2 per centglands with sporozoites and 108 or 62.8 per cent midgutswith oocysts, in 172 dissections. Thirteen of the 102 infectedmidguts had more than 100 oocysts each, one stomach hadsome 600 oocysts, and another 400”.79 These descriptionsappear to support Soper and Wilson’s view that A gambiae
was extremely well adapted to someparts of Brazil and no less difficult totackle than in much of Africa.
It is also interesting to note thatSoper and his colleagues facedconsiderable opposition to theirapproaches and admitted that theythemselves had grave reservationsabout its feasibility from the outset:“The Yellow Fever Service undertookthe solution of the problem of gambiaeeradication rather as a moralobligation than as a reasonableprogram with fair chances ofsuccess”.79
Three times lucky: Brazil,Egypt, and ZambiaThe Brazilian campaign was aremarkable demonstration that larvalcontrol could work against African
Historical review Eradication of Anopheles gambiae from Brazil
Figure 3. An emergency cemetery for victims of the devastating epidemic malaria caused by A gambiae in northeast Brazil between 1938 and 1939. Reproduced from reference 79.
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 623
vectors and the implementationstrategies devised should be applied inthe future within sub-Saharan Africa.Soper and Wilson warned about the overwhelming danger that thereintroduction of A gambiae poses tothe Americas and strongly advocatedprecautionary measures against thateventuality: “It is to be hoped that this‘one of the most interesting chaptersin the medical history of this century’will not have to be rewritten”.79
They could hardly have suspectedthat their services would be calledupon within 2 years, this time in Egyptwhere A gambiae had recently arrivedand caused severe malaria outbreaks.Infestation of a 1000 km stretch of theNile valley, home to three millionpeople, emptied schools and fields,killing approximately 10 000.78 Thearrival of A gambiae could not havecome at a more difficult time and its timely exterminationfrom Egypt was viewed comparably with concurrent militaryheroism: “Early in 1942, Egypt was threatened with twoinvasions—one from the west across the Libyan Desert, theother from the south from Wadi Halfa. The first invader wasrepulsed and thoroughly defeated at el Alamein. The second,A. gambiae, was stopped at Asyût and eradicated by 19February 1945”.78
The Rockefeller team was summoned and adapted themethods developed in Brazil to the ecological situation inEgypt. Although DDT had become available, its use waslimited to residual spraying of railway carriages, aeroplanes,and boats. While domestic pyrethrum spraying was used toquell epidemic malaria transmission, it was larviciding withParis Green that was used to eradicate the vector. Thisprogramme was just as successful as the Brazilian campaignand all the more remarkable because of the huge militarystruggle that simultaneously enveloped the region. AlthoughEgypt has much colder winters than northeast Brazil andmay not have been as climatically suitable for A gambiae, thespecies did persist over 3 years and showed once again howdevastating it can be. This experience also proved that theruthless eradication strategies pioneered in Brazil were not a“once-off” and could be repeated in Africa.
The successes of larval-control campaigns in Brazil andEgypt are irrefutable but the kind of exhaustive andcomplete control applied during these intensive eradicationcampaigns could not be sustained permanently, particularlyin the poorest, least developed parts of sub-Saharan Africa.Furthermore, both invaded areas offered relatively confinedniches for A gambiae that prevented rapid spread toadditional areas. The infested parts of coastal Brazil werelargely enclosed by quite arid highlands and the SaharaDesert flanks the Nile River valley on both sides. If A gambiae had originally come ashore in a less enclosedregion of tropical Brazil, it may not have been possible tostop and could have plunged much of south, central, and
even northern America into economic depression. Wenevertheless find it difficult to believe that nothing can belearned from the Brazilian Malaria Service of the Northeast,which completely eradicated A gambiae from an ecologicallyhospitable area larger than 12 of the countries that make upmodern Africa. These include such intensely malariousnations as Rwanda, Burundi, Guinea Bissau, and EquatorialGuinea.46,47 Given the quite reasonable cost of the Braziliancampaign by modern standards, we argue that verticallyimplemented larval control programmes cannot be ignored as an economically viable option for malariaprevention in Africa.
Furthermore, a clearly documented example ofsustained, successful malaria prevention through larvalcontrol in sub-Saharan Africa does exist and, once again, theinitiation and success of this programme predates theavailability of DDT.94–96 The successful control of malaria inthe Zambian copper belt between 1930 and 1950 representsan outstanding achievement in public health and isdescribed and illustrated by Malcom Watson’s detailedbook.96 This overwhelmingly successful programme ofintegrated malaria control has recently been re-examinedand favourably reviewed in terms of its cost-effectivenessand contribution to economic development.94,95 In this case,an early investment in extensive environmental modificationwas complemented by sustained larviciding as well asquinine treatment, bednets, house-screening and, after 17 years of a successful and economically worthwhileprogramme, DDT spraying of houses. This programme,implemented to protect workers around a Zambian coppermine, targeted the A funestus and A gambiae populationsresponsible for transmission based on simple but carefulentomological surveys. Based primarily upon drainage andwater management, the programme reduced malariamortality, morbidity, and incidence by 70–95% within thefirst few years and these reductions were sustained orimproved upon for two decades.94–96 In the long term, this
Historical reviewEradication of Anopheles gambiae from Brazil
Figure 4. Examples of natural and man-made habitats for A gambiae in Brazil. Reproduced from reference 79.
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com624
approach enabled the development of an industry thatgenerated the equivalent of at least $US7 billion in 1995terms, and was found to be of comparable cost-effectivenessto impregnated nets.94,95 Both the original participants in theZambian programme and contemporary researchers whohave reviewed their work have enthusiastically advocatedlarval control, through environmental management andregular larviciding, as an ideal addition to pharmacologicaland adulticide interventions.94–96 Interestingly, thisprogramme faced similar pessimism at the outset to that ofthe Brazilian campaign: “When Mr Chester Beatty and hisfellow Directors . . . began the work, not one Government inEurope believed they would succeed: the certainty of theirfailure to control disease was coupled with an equal certaintyof their waste of good money”.96
There are many other examples of how larval controlwith standard insecticides and biological control agents70 hascontributed to malaria control on the continent of Africaand its associated islands,97–101 notably Mauritius where localtransmission has been sustainably eliminated.35,36 Clearly,larval control of anopheles mosquitoes is viable in sub-Saharan Africa and needs to be reconsidered as a credibleoption for malaria control where it is most desperatelyneeded. Thus far, all reports of successful control of malariavectors in Africa have been descriptive evaluations ofoperational programmes. We therefore propose that larvalcontrol now needs to be evaluated in Africa throughrigorous and specific trials5 similar to those that bednetshave been put through.42
Adapting eradication strategies for malariacontrol in modern AfricaWe suggest that larval control, in the form of environmentalmanagement or routine larvicide application, should beintegrated with more commonly used approaches such asimproved access to screening and treatment, bednets, orindoor-spraying.10,13,27,29,69 For over a century, larval controlhas been advocated as an indispensable component ofmalaria control but it has also been appreciated that thisapproach depends upon dedicated and laborious
implementation: “Such operations carried out on a largescale will require constant care, involving a great deal oftrouble and expense; while untrustworthy agents will be verylikely to neglect their work”.25
In at least one way, the sheer poverty of the mostmalaria-endemic rural areas may actually make larvalcontrol an economically feasible option because one of themost important components of any larval-controlprogramme is abundant labour. Taking western Kenya as anexample, we estimate that the annual wage for a modernequivalent of a larval inspector from the Brazil campaignwould be less than the cost of 200 bednets and that such anindividual could probably cover an area populated by atleast the same number of people every week. To accuratelyassess the feasibility of larval control in sub-Saharan Africa,it is important to bear in mind that most endemic areas havequite moderate mosquito densities that support stabletransmission because they happen to be extremely efficientvectors.44,48 Thus, the actual quantity of productive larvalhabitat may be manageable if such habitat can be identified.Controlling aquatic stages of malaria vectors depends uponfinding where and when they occur and targeting them withappropriate intervention measures on a regular andindefinite basis.9,10,27,29,102,103 Given the extensive, diverse, andsometimes obscure nature of breeding sites chosen byAfrotropical vectors,38,84–89 this targeting represents aformidable challenge but one that has proven feasible in thepast.9,78,79,94–96 Furthermore, the highly specific adaptation of A gambiae to feeding on humans makes their larvae mucheasier to find than more generalist species because they tendto aggregate around human habitations, often in artificialwater bodies.38,86–89 Indeed, it is precisely this close associationwith human habitation which has also facilitated highlysuccessful larval-control campaigns against Ae aegypti, themajor vector of yellow fever and dengue.81,104 Thus thebehavioural traits that make A gambiae so deadly as a vectorof P falciparum also render it vulnerable to old-fashionedvector-control methods.10
Recent years have seen renewed interest in larval controlof malaria vectors across the tropics,105,106 includingAfrica.5,24,94,95,107 This timely change in attitudes hasreawakened interest in the ecology of African vectors in theirimmature aquatic stages84–87,108–110 and the evaluation ofenvironmentally acceptable larvicides against them.5,91,101,111–113
The largest remaining obstacle to the realisation of larval-control programmes in Africa is probably the developmentof rigorous and sustainable systems for administration andimplementation. Larval control does not confer personalprotection so substantial local suppression of overall malariatransmission intensity is the only acceptable criterion for itssuccess. Larval control efforts are therefore more vulnerableto shortcomings in coverage and to influxes of flying adultmosquitoes from outside of the controlled area than arebednets or indoor sprays. Effective larval control for malariaprevention necessitates consistently high levels of effectivecoverage over contiguous areas that are larger than themaximum flight range of the vector. Fortunately, Africanmalaria vectors rarely fly more than a few kilometres,114–116 sotransmission is largely a local problem, particularly in towns
Historical review Eradication of Anopheles gambiae from Brazil
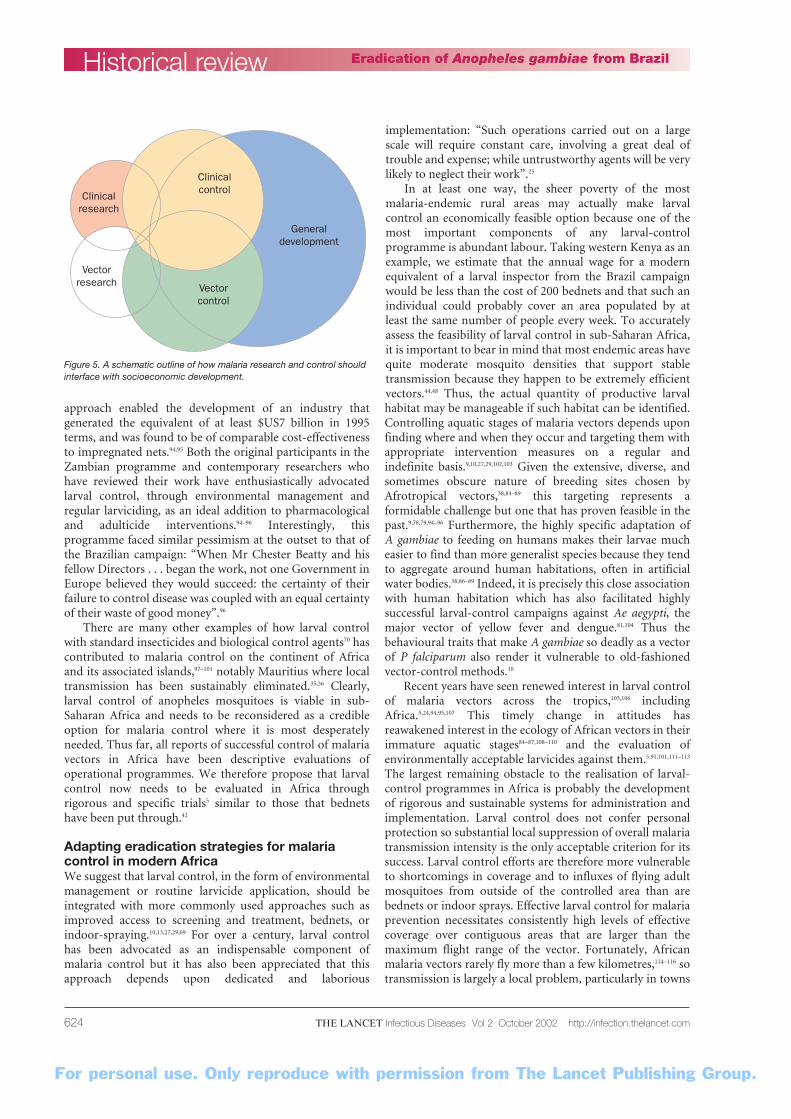
Figure 5. A schematic outline of how malaria research and control shouldinterface with socioeconomic development.
Clinicalcontrol
Generaldevelopment
Clinicalresearch
Vectorresearch Vector
control

For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 625
and cities where people are rarely bitten by vectors that have travelled more than 100 m.117–119 Larval-controlprogrammes could therefore be implemented and evaluatedon manageable spatial scales and then be adapted for largerareas. Nevertheless, larval control does require judicious andwell-organised management, so, although some notablesuccesses have been reported,26 it is generally not well suited to horizontal, community-based implementation or the primary healthcare delivery mechanisms that are being harnessed for most contemporary Roll BackMalaria activities.1,4,28,120 Clearly, the development andimplementation of larval-control programmes in Africa willrequire different strategies to those typically used fordistributing bednets or making more effective drugs,vaccines, and clinical services available. However, theauthoritarian approaches to larval control that succeededbefore World War II may not be well accepted in theincreasingly democratic setting of modern, post-colonialAfrica. Instead, a new generation of larval-controlprogrammes should be rooted in both existing and rapidlyemerging political and administrative structures of theindependent countries that make up Africa today.
The development of malaria control cannot be carriedout in isolation from other health and developmentissues.121,122 Political, economic, and health-sectordevelopment can and will proceed in Africa,123–125 so it iscrucially important that those concerned with malariacontrol participate vigorously in these activities: “Ratherthan resign ourselves to the belief that regions such as sub-Saharan Africa have an intractable legacy of naturalresource degradation, conflict, economic decline, andsocial disruption, we have to consider the cost effectivenessof sustainable interventions such as improvements ininfrastructure, the provision of safe water and wasteremoval services. Insecticides and drugs will neverpermanently roll back malaria in sub-Saharan Africa. To achieve true malaria control, we need to ensure that the most vulnerable regions are vigorously and equitablydeveloped”.122 Agricultural, economic, and otherdevelopment activities have large impacts on not only thelevel of malaria transmission but also the ability of localpeople to prevent and treat it.107,126–129 Entomological andclinical specialists often lack the skills required to set upand manage locally sustained clinical and public healthprogrammes. Conversely, there are a huge number ofpeople active in the development field, throughgovernmental, non-governmental, and community-basedorganisations with an essential role to play in thedevelopment of locally sustained malaria-controlprogrammes but who do not clearly understand theepidemiology of the disease or how best to control it. Wetherefore suggest that malaria research and control capacitycan only be developed in Africa through improvedpartnership of malaria researchers with each other and withthe broader development community (figure 5).
Nowadays, community-based organisations, non-governmental organisations and foreign aid programmesabound in many malaria-endemic African nations and thesebodies may be ideally placed to implement larval-control
programmes using existing governmental systems,resources, and infrastructure. Larval control is particularlywell suited to vertical implementation through collaborationwith those concerned with agricultural, industrial, andurban development, many of which operate throughadministrative structures very similar to those applied inBrazil and Egypt and in contemporary mosquito-controlprogrammes across Europe, America, and Asia. It isnoteworthy that the most successful of these controlprogrammes are usually operated by bodies that have nomedical function and operate as independent departmentsof local and national governments. A clear example of whylarval control of mosquitoes might be better implementedoutside the health development sector has recently beenidentified in the same region of Brazil from which A gambiaewas eradicated.130 In this instance, outbreaks of choleradistracted local health workers from domestic mosquitocontrol, leading to clearly associated dengue outbreaks.130 Wefirmly believe that larval control can work in Africa butsuggest that this is most likely to be achieved throughinfrastructure and capacity development that is primarilyfocused outside the health sector.
We propose that much can be gained by integratingmalaria vector control into national systems, using thesame principles of accountability and capacity buildingapplied elsewhere in the development sector. Improvingadministrative capacity, combined with increasing coverageof Africa with mobile phones, computers, and geographicalinformation technology10,102,103,131,132 could facilitate verticallymanaged larval-control programmes in the near future.
ConclusionThe neglect of larval control for African malaria vectors isprobably best reflected in the fact that its greatest successesare rapidly receding from living memory. Furthermore, ourunderstanding of mosquito larval ecology has scarcelyadvanced since the days of Ronald Ross, leaving most of thequestions that were raised over 50 years ago38 unanswered.The sheer scale of the global malaria burden is now beingmore lucidly revealed,125,133 and so are the limitations ofapproaches based on domestic control of malaria vectorswith insecticides.10,13,22,24,28,45,69 Our historical review of larvalcontrol of African malaria vectors indicates that theseapproaches are largely limited by practical obstacles toimplementation, even for these challenging mosquitospecies. It may therefore be time to reconsider larval control strategies and to prioritise them for more extensive development, evaluation, and implementation inmodern Africa.
Historical reviewEradication of Anopheles gambiae from Brazil
Search strategy and selection criteriaData for this review were identified through PubMed Medline,the extensive files of the authors, the suggestions of twoanonymous reviewers, and reference lists of relevant articles.The Pubmed search was conducted using the followingBoolean search statement: “malaria” and (“larvae” or “larval”or “larvicide”) and (“control” or “prevention” or “protection” or“environmental” or “source reduction”) and (“mosquito” or“vector”). Articles in English or French were selected.
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com626
AcknowledgementsWe thank Ian Sutherland and John Beier for access to an original copyof Anopheles gambiae in Brazil: 1930 to 1940, and Susan Muir andBernadette Pierre at the Rockefeller Foundation for their assistance in clarifying copyright issues relating to the reproduction of figuresfrom this book. We are grateful to two anonymous reviewers whoseconsiderable experience and helpful suggestions greatly improved the final manuscript. We thank the National Institutes of Health (grant numbers U19 AI45511 and D43 TW01142), the Christian
Children’s Fund, and Valent BioSciences Corporation for financialsupport.
Conflicts of interestUF has been supported by Valent BioSciences Corporation, acommercial manufacturer of microbial larvicides. None of our sourcesof financial support or agents thereof has had any role in the selectionor interpretation of information for this publication or in the decisionto submit this paper for publication.
Historical review Eradication of Anopheles gambiae from Brazil
References1 Greenwood B, Mutabingwa T. Malaria in 2002.
Nature 2002; 415: 670–72.2 Goodman CA, Mills AJ. The evidence base on the
cost-effectiveness of malaria control measures inAfrica. Health Policy Plan 1999; 14: 301–12.
3 Curtis CF, Lines J. Should DDT be banned byinternational treaty? Parasitol Today 2000; 16:119–21.
4 Nabarro DN, Tayler EM. The “roll back malaria”campaign. Science 1998; 280: 2067–68.
5 Walker K. A review of control methods for Africanmalaria vectors. Washington, DC: US Agency forInternational Development, 2002: Activity Report 54.
6 Guyatt HL, Kinnear J, Buruni M, Snow RW. Acomparative cost analysis of insecticide treated netsand indoor residual spraying in highland Kenya.Health Policy Plan 2002; 17: 144–53.
7 Goodman CA, Mnzava AEP, Diamini SS, Sharp BL,Mthembu DJ, Gumede JK. Comparison of the costand cost-effectiveness of insecticide-treated bednetsand residual house-spraying in KwaZulu-Natal,South Africa. Trop Med Int Health 2001; 6: 280–95.
8 Curtis CF, Mnzava AEP. Comparison of housespraying and insecticide-treated nets for malariacontrol. Bull World Health Organ 2000; 78: 1389–401.
9 Pampana E. A textbook of malaria eradication.London: Oxford University Press, 1963.
10 Carter R, Mendis KN, Roberts D. Spatial targeting ofinterventions against malaria. Bull World HealthOrgan 2000; 78: 1401–11.
11 Anderson RM, May RM. Infectious diseases ofhumans. Oxford: Oxford University Press, 1991.
12 MacDonald G. The epidemiology and control ofmalaria. London: Oxford University Press, 1957.
13 Killeen GF, McKenzie FE, Foy BD, Schieffelin C,Billingsley PF, Beier JC. The potential impacts ofintegrated malaria transmission control onentomologic inoculation rate in highly endemicareas. Am J Trop Med Hyg 2000; 62: 545–51.
14 Koella JC. On the use of mathematical models ofmalaria transmission. Acta Trop 1991; 49: 1–25.
15 Beier JC. Malaria development in mosquitoes. Annu Rev Entomol 1998; 43: 519–43.
16 Magesa SM, Wilkes TJ, Mnzava AEP, et al. Trial ofpyrethroid impregnated bednets in an area ofTanzania holoendemic for malaria. Part 2 Effects onthe malaria vector population. Acta Trop 1991; 49:97–108.
17 Robert V, Carnevale P. Influence of deltamethrintreatment of bed nets on malaria transmission in theKou valley, Burkina Faso. Bull World Health Organ1991; 69: 735–40.
18 Carnevale P, Robert V, Boudin C, et al. La luttecontre le plaudisme par des moustiquairesimpregnees de pyrethroides au Burkina Faso. Bull Soc Path Exot 1988; 81: 832–46.
19 Charlwood JD, Graves PM. The effect ofpermethrin-impregnated bednets on a population ofAnopheles farauti in coastal Papua New Guinea. Med Vet Entomol 1987; 1: 319–27.
20 Kouznetsov RL. Malaria control by application ofindoor spraying of residual insecticides in tropicalAfrica and its impact on community health. TropicalDoctor 1977; 7: 81–93.
21 Romi R, Razaiarimanga MC, Raharimanga R, et al.Impact of the malaria control campaign (1993–1998)in the highlands of Madagascar; parasitological and entomological data. Am J Trop Med Hyg 2002; 66: 2–6.
22 Molineaux L, Gramiccia G. The Garki Project.Geneva: World Health Organization, 1980.
23 Ross R. The prevention of malaria. London: Murray,1911.
24 Killeen GF, Fillinger U, Knols BGJ. Advantages oflarval control for African malaria vectors: lowmobility and behavioural responsiveness ofimmature mosquito stages allow high effectivecoverage. Malar J 2002; 1: 8.
25 Ross R, Annett HE, Austen EE, Giles GM, Fielding-Ould R. Report of the malaria expedition ofthe Liverpool School of Tropical Medicine andMedical Parasitology with supplementary reports.Liverpool: University Press of Liverpool, 1900.
26 Ault SK. Environmental management: a re-emergingvector control strategy. Am J Trop Med Hyg 1994; 50: 35–49.
27 Kitron U, Spielman A. Suppression of transmissionof malaria through source reduction: antianophelinemeasures applied in Israel, the United States, andItaly. Rev Infect Dis 1989; 11: 391–406.
28 Najera JA. Malaria control: achievements, problemsand strategies. Parassitologia 2001; 43: 1–89.
29 Kitron U. Malaria, agriculture, and development:lessons from past camapigns. Int J Health Serv 1987;17: 295–326.
30 Garrett-Jones C. Prognosis for interruption ofmalaria transmission through assessment of themosquito’s vectorial capacity. Nature 1964; 204:1173–75.
31 Gladwell M. The mosquito killer: millions of peopleowe their lives to Fred Soper. Why isn’t he a hero?The New Yorker 2001; July 2: 42–51.
32 Spielman A, D’Antonio M. Mosquito: a naturalhistory of our most persistent and deadly foe. SanFrancisco: Hyperion, 2001.
33 Spielman A, Pollack RJ, Kiswewski AE, Telford III SR. Issues in public health entomology.Vector Borne Zoonotic Dis 2001; 1: 3–19.
34 Curtis CF. Restoration of malaria control in theMadagascar highlands by DDT spraying. Am J TropMed Hyg 2002; 66: 1.
35 Ragavoodoo C. Situation du paludimse a Maurice.Santé 1995; 5: 371–75.
36 Julvez J. Historique du paludime insulaire dansl’ocean Indien (sud-Ouest). Une approche eco-epidemiologique. Santé 1995; 5: 353–57.
37 Muirhead-Thomson RC. The significance ofirritability, behaviouristic avoidance and alliedphenomena in malaria eradication. Bull WorldHealth Organ 1960; 22: 721–34.
38 Muirhead-Thomson RC. Mosquito behaviour inrelation to malaria transmission and control in thetropics. London: Edward Arnold & Co, 1951.
39 Guyatt HL, Snow RW. The cost of not treatingbednets. Trends Parasitol 2002; 18: 12–16.
40 Guyatt HL, Gotink MH, Ochola SA, Snow RW. Freebednets to pregnant women through antenatal clinicsin Kenya: a cheap, simple and equitable approach todelivery. Trop Med Int Health 2002; 7: 1–12.
41 Guyatt HL, Corlett SK, Robinson TP, Ochola SA,Snow RW. Malaria prevention in highland Kenya:indoor residual house-spraying vs. insecticide-treatedbednets. Trop Med Int Health 2002; 7: 298–303.
42 Lengeler C. Insecticide treated bednets and curtainsfor malaria control. Cochrane Library Reports 1998;3: 1–70.
43 Smith TA, Leuenberger R, Lengeler C. Childmortality and malaria transmission intensity inAfrica. Trends Parasitol 2001; 17: 145–49.
44 Beier JC, Killeen GF, Githure J. Short report:entomologic inoculation rates and Plasmodiumfalciparum malaria prevalence in Africa. Am J TropMed Hyg 1999; 61: 109–13.
45 Marsh K, Snow RW. Malaria transmission andmorbidity. Parasitologia 1999; 41: 241–46.
46 Snow RW, Craig M, Deichmann U, Marsh K.Estimating mortality, morbidity and disability due tomalaria among Africa’s non-pregnant population.Bull World Health Organ 1999; 77: 624–40.
47 Snow RW, Craig MH, Deichmann U, le Sueur D. A preliminary continental risk map for malariamortality among African children. Parasitol Today1999; 15: 99–104.
48 Hay SI, Rogers DJ, Toomer JF, Snow RW. AnnualPlasmodium falciparum entomological inoculationrates across Africa: literature survey, internet accessand review. Trans R Soc Trop Med Hyg 2000; 94: 113–27.
49 Snow RW, McCabe E, Mbogo CNM, et al. The effectof delivery mechanism on the uptake of bed net re-impregnation in Kilifi district, Kenya. Health PolicyPlan 1999; 14: 18–25.
50 Lines J. Mosquito nets and insecticides for nettreatment: a discussion of existing and potentialdistribution systems in Africa. Trop Med Int Health1996; 1: 616–32.
51 Lengeler C, Snow RW. From efficacy to effectiveness:insecticide treated bednets in Africa. Bull WorldHealth Organ 1996; 73: 325–32.
52 Winch PJ, Makemba AM, Makame VR, et al. Socialand cultural factors affecting rates of regularretreatment of mosquito nets with insecticide inBagamoyo District, Tanzania. Trop Med Int Health1997; 2: 760–70.
53 Curtis CF, Maxwell CA. Free insecticide for nets iscost effective. Trends Parasitol 2002; 18: 204–05.
54 Schellenberg JR, Abdulla S, Minja H, et al. KINET: asocial marketing programme of treated nets and nettreatment for malaria control in Tanzania, withevaluation of child health and long-term survival.Trans R Soc Trop Med Hyg 1999; 93: 225–31.
55 Armstrong Schellenberg JRM, Abdulla S, Nathan R,et al. Effect of large–scale social marketing ofinsecticide–treated nets on child survival in ruralTanzania. Lancet 2001; 357: 1241–47.
56 Alonso PL, Lindsay SW, Armstrong SchellenbergJRM, et al. A malaria control trial using insecticide-treated bed nets and targeted chemoprophylaxis in arural area of the Gambia, West Africa. 6. The impactof interventions on mortality and morbidity frommalaria. Trans R Soc Trop Med Hyg 1993; 87(suppl 2): 37–44.
57 Kaneko A, Taleo G, Kalkoa M, Yamar S,Kobayakawa T, Bjorkman A. Malaria eradication onislands. Lancet 2000; 356: 1560–64.
58 Krogstad DJ. Malaria as a re-emerging disease.Epidemiol Rev 1996; 18: 77–89.
59 Molyneux DH, Floyd K, Barnish G, Fevre EM. Trans-mission control and drug resistance in malaria: acrucial interaction. Parasitol Today 1999; 15: 238–40.
60 Buckling AG, Taylor LH, Carlton JM, Read AF.Adaptive changes in Plasmodium transmissionstrategies following chloroquine chemotherapy. Proc R Soc Lond B Biol Sci 1997; 264: 553–59.
61 Hogh B, Gamage-Mendis A, Butcher GA, et al. Thediffering impact of chloroquine andpyrimethamine/sulfadoxine upon the infectivity ofmalaria species to the mosquito vector. Am J TropMed Hyg 1998; 58: 176–82.
62 Puta C, Manyando C. Enhanced gametocyteproduction in Fansidar-treated Plasmodiumfalciparum malaria patients: implications for malariatransmission control programmes. Trop Med IntHealth 1997; 2: 227–29.
63 Lines JD, Wilkes TJ, Lyimo EO. Human malariainfectiousness measured by age-specific sporozoiterates in Anopheles gambiae in Tanzania. Parasitology1991; 102: 167–77.
64 Arez AP, Snounou G, Pinto J, et al. A clonalPlasmodium falciparum population in an isolatedoutbreak of malaria in the Republic of Cabo Verde.Parasitology 1999; 118: 347–55.
65 Zetyenga J, Rogier C, Tall A, et al. No influence of age on infection complexity and allelicdistribution in Plasmodium falciparum infections inNdiop, a Senegalese village with seasonal,mesoendemic malaria. Am J Trop Med Hyg 1998; 59: 726–35.
66 Earle WC, Perez M, Del Rio J, Arzola C.Observations on the course of naturally acquiredmalaria in Puerto Rico. PRJ Public Health Trop Med1939; 14: 391–406.
67 Bekessy A, Molineaux L, Storey J. Estimation ofincidence and recovery rates of Plasmodiumfalciparum parasitaemia from longitudinal data. Bull World Health Organ 1976; 54: 685–93.
68 Hamad AA, El-Hassan IM, El-Khalifa AA, et al.Chronic Plasmodium falciparum infections in an area
For personal use. Only reproduce with permission from The Lancet Publishing Group.
THE LANCET Infectious Diseases Vol 2 October 2002 http://infection.thelancet.com 627
of low intensity malaria transmission in the Sudan.Parasitology 1999; 120: 447–56.
69 Shiff C. Integrated approach to malaria control. Clin Microbiol Rev 2002; 15: 278–98.
70 Rozendaal JA. Vector control. Methods for use byindividuals and communities. Geneva: WHO, 1997.
71 Ito J, Ghosh A, Moreira LA, Wimmer EA, Jacobs-Lorena M. Transgenic anopheline mosquitoesimpaired in transmission of a malaria parasite.Nature 2002; 417: 452–55.
72 Richie TL, Saul A. Progress and challenges formalaria vaccines. Nature 2002; 415: 694–701.
73 Boete C, Koella JC. A theoretical approach topredicting the success of genetic manipulation ofmalaria mosquitoes in malaria control. Malar J2002; 1: 3.
74 Kiszewski AE, Spielman A. Spatially explicit modelof transposon-based genetic drive mechanisms fordisplacing fluctuating populations of anophelinevector mosquitoes. J Med Entomol 1998; 35: 584–90.
75 Saul A. Minimal efficacy requirements for malariavaccines to significantly lower transmission inepidemic or seasonal malaria. Acta Trop 1993; 52: 283–96.
76 Foy BD, Killeen GF, Magalhaes T, Beier JC.Immunological targeting of critical insect antigens.Am Entomol (in press).
77 Enserink M. Ecologists see flaws in transgenicmosquito. Science 2002; 297: 30–31.
78 Shousha AT. Species-eradication. The eradication ofAnopheles gambiae from Upper Egypt, 1942–1945.Bull World Health Organ 1948; 1: 309–53.
79 Soper FL, Wilson DB. Anopheles gambiae in Brazil: 1930 to 1940. New York: RockefellerFoundation, 1943.
80 Shannon RC. O apparecimento de uma especieAfricana de Anopheles no Brazil. Brazil-Medico 1930;44: 515–16.
81 Schliessman DJ, Calheiros LB. A review of the statusof yellow fever and Aedes aegypti eradicationprograms in the Americas. Mosquito News 1974; 34: 1–8.
82 White GB. Anopheles gambiae complex and diseasetransmission in Africa. Trans R Soc Trop Med Hyg1974; 68: 279–301.
83 Lounibos LP. Invasions by insect vectors of humandisease. Annu Rev Entomol 2002; 47: 233–66.
84 Gimnig JE, Ombok M, Otieno S, Kaufman MG,Vulule JM, Walker ED. Density-dependentdevelopment of Anopheles gambiae (Diptera:Culicidae) larvae in artificial habitats. J Med Entomol2002; 39: 162–72.
85 Gimnig JE, Ombok M, Kamau L, Hawley WA.Characteristics of larval anopheline (Diptera:Culicidae) habitats in Western Kenya. J Med Entomol2001; 38: 282–88.
86 Charlwood JD, Edoh D. Polymerase chain reactionused to describe larval habitat use by Anophelesgambiae complex (Diptera: Culicidae) in theenvirons of Ifakara, Tanzania. J Med Entomol 1996;33: 202–04.
87 Minakawa N, Mutero CM, Githure JI, Beier JC, Yan G. Spatial distribution and habitat character-ization of Anopheline mosquito larvae in WesternKenya. Am J Trop Med Hyg 1999; 61: 1010–16.
88 Gillies MT, DeMeillon B. The Anophelinae of AfricaSouth of the Sahara (Ethiopian zoogeographicalregion). Johannesburg: South African Institute forMedical Research, 1968.
89 Gillies MT, Coetzee M. A supplement to theAnophelinae of Africa south of the Sahara(Afrotropical region). Johannesburg: South AfricanMedical Research Institute, 1987.
90 Barber MA. The present status [summer 1939] ofAnopheles gambiae in Brazil. Am J Trop Med 1940;20: 249–67.
91 Fillinger U, Knols BGJ, Becker N. Efficacy andefficiency of new Bacillus thuringiensis var. Israelensisand Bacillus sphaericus formulations againstAfrotropical Anophelines in Western Kenya. TropMed Int Health (in press).
92 Smith T, Charlwood JD, Takken W, Tanner M,Spiegelhalter DJ. Mapping densities of malariavectors within a single village. Acta Trop 1995; 59: 1–18.
93 Smith T, Charlwood JD, Kihonda J, et al. Absence ofseasonal variation in malaria parasitemia in an areaof intense seasonal transmission. Acta Trop 1993; 54: 55–72.
94 Utzinger J, Tozan Y, Doumani F, Singer BH. Theeconomic payoffs of integrated malaria control inthe Zambian copperbelt between 1930 and 1950.Trop Med Int Health 2002; 7: 657–77.
95 Utzinger J, Tozan Y, Singer BH. Efficacy and costeffectiveness of environmental management formalaria control. Trop Med Int Health; 6: 677–87.
96 Watson M. African highway: The battle for health incentral Africa. London: John Murray, 1953.
97 Gopaul R. Surveillance entomologique a Maurice.Santé 1995; 5: 401–05.
98 Fletcher M, Teklehaimanot A, Yemane G. Control ofmosquito larvae in the port city of Assab by anindigenous larvivorous fish, Aphanius dispar. ActaTrop 1992; 52: 155–66.
99 Sabatinelli G, Blanchy S, Majori G, Papakay M.Impact of the use of the larvivorous fish, Poeciliareticulata in the transmission of malaria in theFederal Islamic Republic of Comoros. Ann ParasitolHum Comp 1991; 66: 84–88.
100 Louis JP, Albert JP. Malaria in the Republic ofDjibouti. Strategy for control using a biologicalantilarval campaign: indigenous larvivorous fishes(Aphanius dispar) and bacterial toxins. MédicineTropicale 1988; 48: 127–131.
101 Barbazan P, Baldet T, Darriet F, Escaffre H, Djoda DH, Hougard JM. Impact of treatments withBacillus sphaericus on Anopheles populations and thetransmission of malaria in Maroua, a large city in asavannah region of Cameroon. J Am MosquitoControl Assoc 1998; 14: 33–39.
102 Kitron U. Risk maps: transmission and burden of vector–borne diseases. Parasitol Today 2000; 16:324–25.
103 Kitron U. Landscape ecology and epidemiology ofvector-borne dieases: tools for spatial analysis. J MedEntomol 1998; 35: 435–45.
104 Kay BH, Nam VS, Tien VT, et al. Control of Aedesvectors of dengue in three provinces of Vietnam byuse of Mesoclops (Copepda) and community-basedmethods validated by entomologic, clinical, andserological surveillance. Am J Trop Med Hyg 2002;66: 40–48.
105 Yapabandara AMGM, Curtis CF. Laboratory andfield comparisons of pyriproxifen, polystyrene beadsand other larvicidal methods against malaria vectorsin Sri Lanka. Acta Trop 2002; 81: 211–23.
106 Yapabandara AMGM, Curtis CF, WickramasingheMB, Fernando WP. Control of malaria vectors with the insect growth regulator pyrproxyfen in agem-mining area in Sri Lanka. Acta Trop 2001; 80:265–76.
107 Keiser J, Utzinger J, Singer BH. The potential ofintermittent irrigation for increasing rice yields,lowering water consumption, reducing methaneemissions, and controlling malaria in African ricefields. J Am Mosquito Control Assoc (in press).
108 Mutero C, Blank H, Konradsen F, van der Hoek W.Water management for controlling the breeding ofmosquitoes in rice irrigation schemes in Kenya. Acta Trop 2000; 76: 253–63.
109 Ye-ebiyo Y, Pollack RJ, Spielman A. Enhanceddevelopment in nature of larval Anopheles arabiensismosquitoes feeding on maize pollen. Am J Trop MedHyg 2000; 63: 90–93.
110 Minakawa N, Githure JI, Beier JC, Yan G.Anopheline mosquito survival strategies during thedry period in western Kenya. J Med Entomol 2001;38: 388–92.
111 Seyoum A, Abate D. Larvicidal efficacy of Bacillusthuringiensis var. israelensis and Bacillus spaericus onAnopheles arabiensis in Ethiopia. World J MicrobiolBiotechnol 1997; 13: 21–24.
112 Karanja DM, Githeko AK, Vulule JM. Small-scalefield evaluation of the monomolecular surface film‘Arosurf MSF’ against Anopheles arabiensis Patton.Acta Trop 1994; 56: 365–69.
113 Karch S, Asidi N, Manzambi ZM, Salaun JJ.Efficacy of Bacillus sphaericus against the malariavector Anopheles gambiae and other mosquitoes inswamps and rice fields in Zaire. J Am MosquitoControl Assoc 1992; 8: 376–80.
114 Costantini C, Li SG, Della Torre A, Sagnon N,Coluzzi M, Taylor CE. Density, survival anddispersal of Anopheles gambiae complexmosquitoes in a west African Sudan savannavillage. Med Vet Entomol 1996; 10: 203–19.
115 Gillies MT. Studies on the dispersion and survivalof Anopheles gambiae in East Africa, by means ofmarking and release experiments. Bull Entomol Res1961; 52: 99–127.
116 Thomson MC, Connor SJ, Qinones ML, Jawara M,Todd J, Greenwood BM. Movement of Anophelesgambiae s.l. vectors between villages in TheGambia. Med Vet Entomol 1995; 9: 413–19.
117 Manga L, Fondjo E, Carnevale P, Robert V.Importance of low dispersion of Anopheles gambiae(Diptera: Culicidae) on malaria transmission inhilly towns in South Cameroon. J Med Entomol1993; 30: 936–38.
118 Trape JF, Lefebvre-Zante E, Legros F, et al. Vectordensity gradients and the epidemiology of urbanmalaria in Dakar, Senegal. Am J Trop Med Hyg1992; 47: 181–89.
119 Thompson R, Begtrup K, Cuamba N, et al. TheMatola malaria project: a temporal and spatialstudy of malaria transmission and disease in asuburban area of Maputo, Mozambique. Am J TropMed Hyg 1997; 57: 550–59.
120 Lines J, Harpham T, Leake C, Schofield C. Trends,priorities and policy directions in the control ofvector-borne diseases in urban environments.Health Policy Plan 1994; 9: 113–29.
121 Nicoll A. Current issues in tropical paediatricinfectious disease: Integrated management of childhood illness in resource-poor countries: an initiative from the World Health Organization.Trans R Soc Trop Med Hyg 2000; 94: 9–11.
122 Lerer LB. Cost-effectiveness of malaria control insub-Saharan Africa. Lancet 1999; 354: 1123–24.
123 Feacham RGA. The World Bank’s contribution totropical medicine: diagnosis and prognosis. Am J Trop Med Hyg 1998; 59: 19–23.
124 Sachs JD. Growth in Africa: it can be done. The Economist 1996; June 29: 23–25.
125 Sachs J, Malaney P. The economic and socialburden of malaria. Nature 2002; 415: 680–85.
126 Ijumba JN, Mosha FW, Lindsay SW. Malariatransmission risk variations derived from differentagricultural practices in an irrigated area ofnorthern Tanzania. Med Vet Entomol 2002; 16:28–38.
127 Ijumba J, Lindsay S. Impact of irrigation onmalaria in Africa: paddies paradox. Med VetEntomol 2001; 15: 1–11.
128 Service MW. Agricultural development andarthropod-borne diseases: a review. Revista deSaude Publica (Sao Paulo) 1991; 25: 165–78.
129 Service MW. Problems of vector-borne diseases and irrigation projects. Insect Sci Applic 1984; 5: 227–31.
130 Pontes RJ, Freeman J, Oliveira-Lima JW, Hodgson JC, Spielman A. Vector densities thatpotentiate dengue outbreaks in a Brazilian city. Am J Trop Med Hyg 2000; 62: 378–83.
131 Utzinger J, Tanner M, Singer BH. The internet: avaluable tool for Roll Back Malaria. Trends Parasitol2001; 17: 159–61.
132 Rogers DJ, Randolph SE, Snow RW, Hay SI.Satellite imagery in the study and forecast ofmalaria. Nature 2002; 415: 710–15.
133 Breman JG, Egan A, Keutsch GT. The intolerableburden of malaria: a new look at the numbers. Am JTrop Med Hyg 2001; 64 (suppl 1): iv–vii.
Historical reviewEradication of Anopheles gambiae from Brazil
Related Documents











