Epidemiology Research at KCI

Epidemiology Research at KCI. Epidemiology Epidemiology is the study of the distribution of diseases in the population. Epidemiologic methods are used.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Epidemiology Research at KCI
Epidemiology
Epidemiology is the study of the distribution of diseases in the population.
Epidemiologic methods are used for the identification of risk factors for disease and determination of optimal treatment approaches used in clinical practice.
In the study of communicable and chronic diseases, the work of epidemiologists involves study design, data collection and statistical analysis.
Epidemiologic Methods
Observational: Case-Control: Exposures, genes, and/or behaviors in
individuals with a particular disease (cases) are compared to individuals without the disease (controls).
Cohort: A group of individuals with and without a particular exposure are followed to compare disease outcomes.
Interventional:Clinical Trials: Individuals are randomized to receive a particular treatment within the clinic setting.
Community Trials: A community participates in a behavioral intervention, a screening intervention, etc.
Study Design
Study Design:
Population-Based: Individuals under study belong to a defined population, i.e., residents of a geographic region.
Clinic or Hospital-Based: Studies are based upon patients seen at a particular hospital or clinic.
Community-Based: Participants are volunteers in the community.
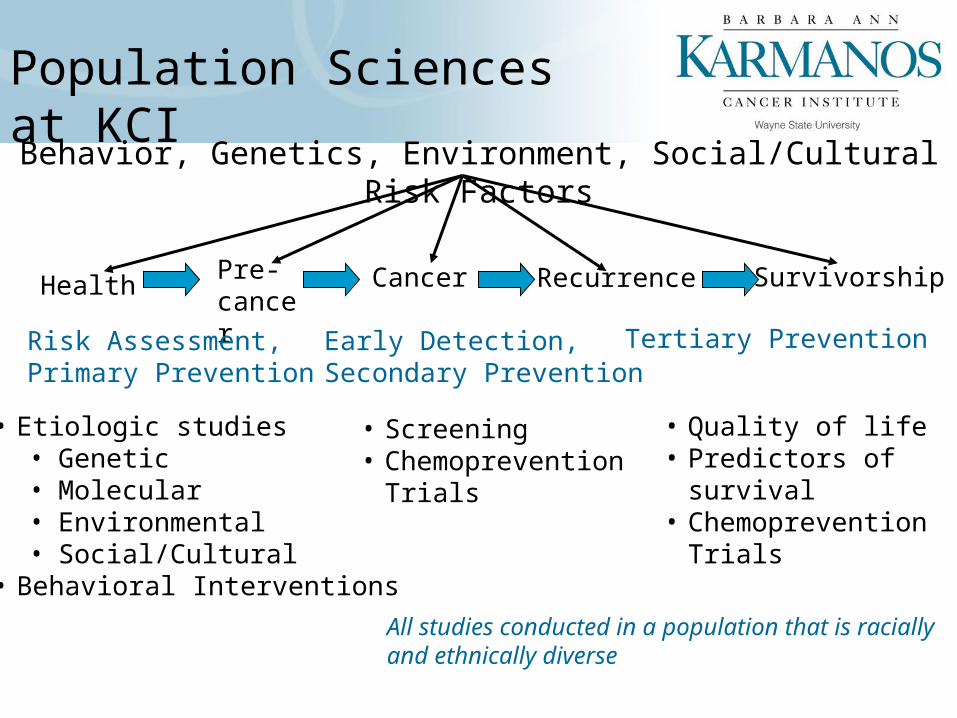
Behavior, Genetics, Environment, Social/Cultural Risk Factors
HealthPre-cancer
Cancer Recurrence
• Etiologic studies• Genetic• Molecular• Environmental• Social/Cultural
• Behavioral Interventions
• Screening• Chemoprevention
Trials
• Quality of life• Predictors of
survival• Chemoprevention
Trials
Survivorship
Risk Assessment,Primary Prevention
Early Detection,Secondary Prevention
Tertiary Prevention
Population Sciences at KCI
All studies conducted in a population that is racially and ethnically diverse
Population-Based Cancer Epidemiology
Surveillance Epidemiology and End Results (SEER) Program
• Assemble and report estimates of cancer incidence and mortality in the United States.
• Monitor annual cancer incidence trends.
• Provide continuing information on changes over timein extent of disease at diagnosis, trends in therapy, and associated changes in patient survival.
• Promote studies designed to identify factors amenable to cancer control interventions.
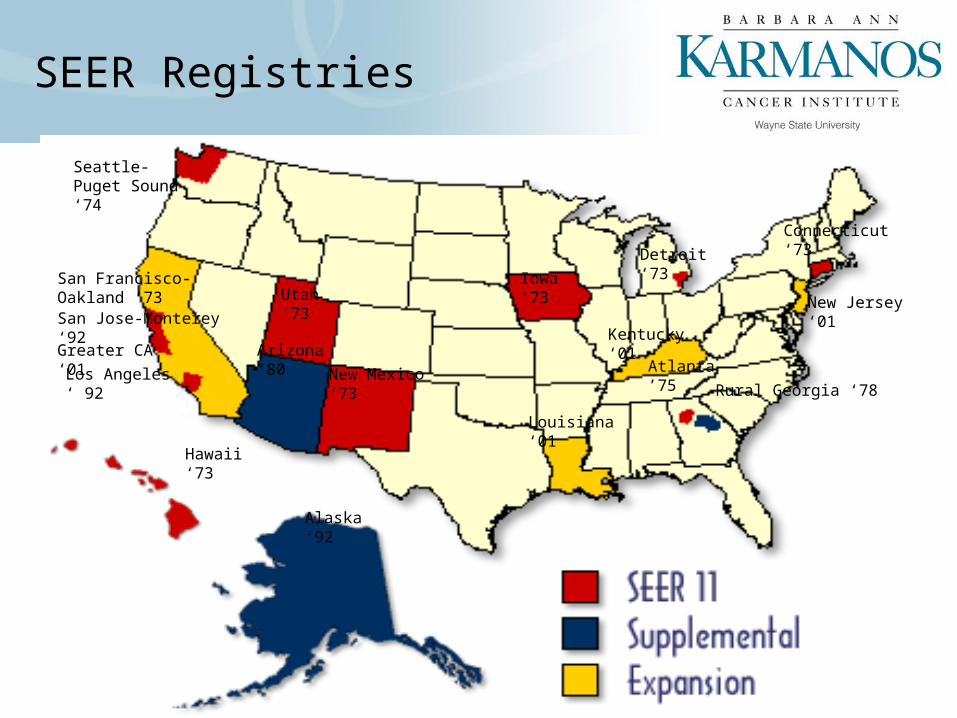
SEER Registries
Utah ‘73Iowa ‘73
Detroit ‘73
Connecticut ‘73
Seattle-Puget Sound ‘74
Atlanta ’75
New Jersey ‘01
Kentucky ‘01
Louisiana ‘01
New Mexico ‘73
Arizona ‘80
Alaska ‘92
Hawaii ‘73
San Francisco-Oakland ‘73
Los Angeles ‘ 92
Greater CA ‘01
Rural Georgia ‘78
San Jose-Monterey ‘92
Metropolitan Detroit Cancer Surveillance System (MDCSS)
• Cancer is a reportable disease in Michigan. • The Metropolitan Detroit Cancer Surveillance System
(MDCSS) is the designated arm of the Michigan Department of Community Health for collection of cancer information for the tri-county area.
• About 25,000 in situ and invasive cancers are diagnosed among residents each year.
• Our database includes information on over 700,000 cancer cases.
MDCSS
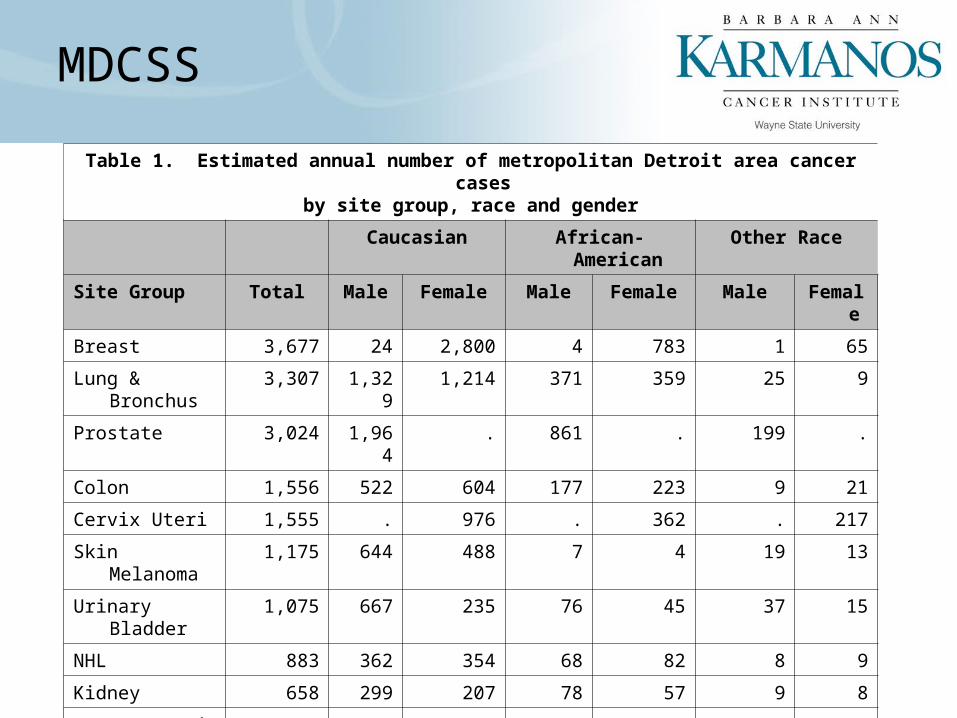
Table 1. Estimated annual number of metropolitan Detroit area cancer cases by site group, race and gender
Caucasian African-American Other Race
Site Group Total Male Female Male Female Male Female
Breast 3,677 24 2,800 4 783 1 65
Lung & Bronchus
3,307 1,329 1,214 371 359 25 9
Prostate 3,024 1,964 . 861 . 199 .
Colon 1,556 522 604 177 223 9 21
Cervix Uteri 1,555 . 976 . 362 . 217
Skin Melanoma 1,175 644 488 7 4 19 13
Urinary Bladder 1,075 667 235 76 45 37 15
NHL 883 362 354 68 82 8 9
Kidney 658 299 207 78 57 9 8
Corpus Uteri 621 . 496 . 116 . 9
Other Cancers 7,307 2,697 2,719 788 914 85 104
Total 24,838 8,508 10,093 2,430 2,945 392 470
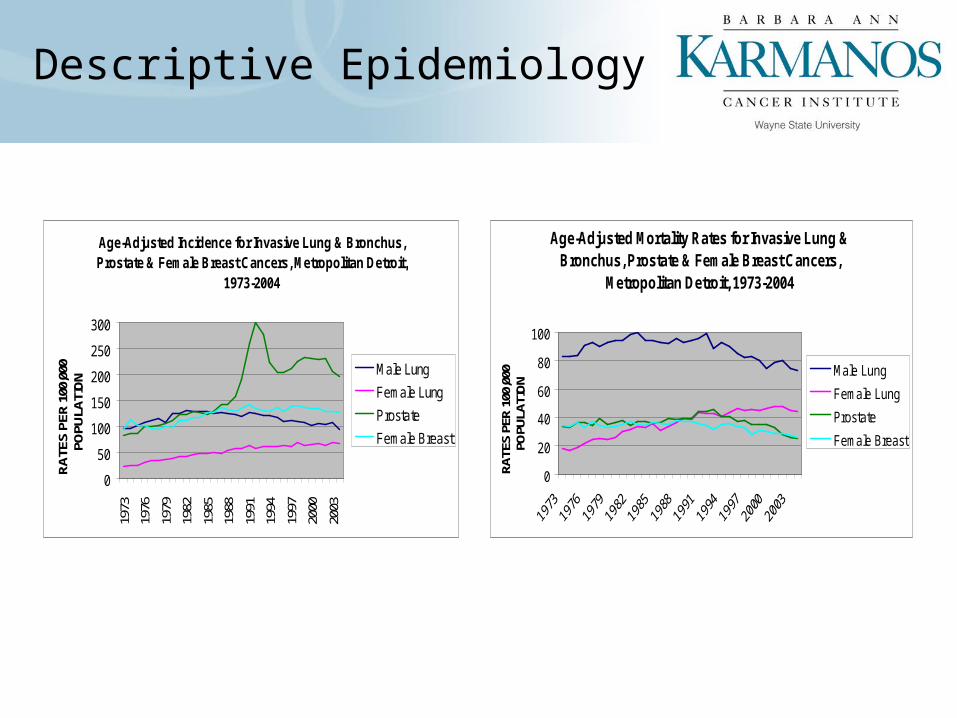
Descriptive Epidemiology
Age-Adjusted Incidence for Invasive Lung & Bronchus, Prostate & Female Breast Cancers, Metropolitan Detroit,
1973-2004
0
50
100
150
200
250
300
1973
1976
1979
1982
1985
1988
1991
1994
1997
2000
2003
RA
TES
PER
100
,000
PO
PULA
TIO
N
Male Lung
Female Lung
Prostate
Female Breast
Age-Adjusted Mortality Rates for Invasive Lung & Bronchus, Prostate & Female Breast Cancers,
Metropolitan Detroit, 1973-2004
0
20
40
60
80
100
RATE
S PE
R 10
0,00
0 PO
PULA
TIO
N
Male Lung
Female Lung
Prostate
Female Breast
Exploring Health, Ancestry and Lung Epidemiology (EXHALE)Schwartz AG; R01 CA60691
Case-Control study to identify chromosomal regions associated with risk of lung cancer among African Americans (AA)
549 AA cases from MDCSS572 AA volunteer controlsBiospecimens collected for 94% of participants
Schwartz AG, Cote ML, Wenzlaff AS, Land S, Amos CI. Racial Differences in the Association Between SNPs on 15q25.1, Smoking Behavior, and Risk of Non-small Cell Lung Cancer. J Thorac Oncol 2009
• SNPS in the CHRNA3 and CHRNA5 region contribute to lung cancer risk• While variant alleles are less frequent in African Americans, risk may be greater
than in whites and less likely to reflect an indirect effect on lung cancer risk through nicotine dependence
Luminal Lipid Exposure, Genetics & Colon Cancer RiskKato I; R01 CA93817
Genotyping for FABP2 A54, APO E2/E3 polymorphisms, which are postulated to modify intestinal lipid absorption
1205 cases from MDCSS1552 controls using random digit dialing
(RDD)
• Populations with lower intake of luminal modifiers (calcium, fiber) may have differential risks of colorectal cancer associated with dietary fatty acid intake
• These SNPs may not be useful in predicting colorectal cancer risk in populations with high fat intake
Cancer In Arab Americans: Estimating Rates & Fostering Research Schwartz K, N01 PC35154-RRSS
•Arab/Chaldean men had greater proportions of leukemia , multiple myeloma, liver, kidney, and urinary bladder cancers.
•Arab/Chaldean women hadgreater proportions of leukemia, thyroid, and brain cancers.
•Arab–American women have similar distribution ofbreast cancer histology to European–Americanwomen.
•Arab–American stage, age, and hormone receptor status at diagnosis was more similar to African–American women.
•Arab–American women have a better overall survival than even European–American women.
Epidemiology Research Core (ERC)
Established in December, 2007 due to a specific need for standardizing procedures for access to and use of the local and national SEER data
– Confidentiality of metropolitan Detroit SEER registry data
– Complexity of SEER registry data
ERC Services
1. Consultation and collaboration
study design, proposal development, interpretation of population-based local and national SEER data
2. Rapid case ascertainment for case identification
3. Control Identification
4. Oversight and support of study interviews
5. Collection and abstraction of medical records
6. Collection of biological specimens
7. Response to data requests requiring access to local and national SEER data
8. Linkage of external data sources to local SEER data
Related Documents




![(c) B. Gerstman 2007Chapter 91 Epidemiology Kept Simple Chapter 9: Types of Epidemiologic Studies [Introduction to Analytic Studies]](https://static.cupdf.com/doc/110x72/56649d6b5503460f94a4a898/c-b-gerstman-2007chapter-91-epidemiology-kept-simple-chapter-9-types-of.jpg)