Endothelial Keratoplasty Techniques Mark A. Terry, M.D. Michael D. Straiko, M.D. Neda Shamie, M.D. Endothelial Keratoplasty and DALK Course: ASCRS 2014 The speaker has a financial interest in the EK instruments which he designed. The author has had research support from Fischer Instruments The author has been a sponsored speaker for Alcon DISCLOSURE Endothelial Keratoplasty: Current technique, complications and clinical results Mark A. Terry, MD Director, Corneal Services Devers Eye Institute D Scientific Director Lions VisionGift Research Lab Portland, Oregon, U.S.A. Endothelial Keratoplasty (EK) is a form of corneal transplantation that replaces just the posterior diseased cornea, leaving the corneal surface relatively untouched. Endothelial Keratoplasty: Multiple names and acronyms PLK: Posterior Lamellar Keratoplasty (Melles) DLEK: Deep Lamellar Endothelial Keratoplasty (Terry) DSEK: Descemets Stripping Endothelial Keratoplasty (Melles) DSAEK: Descemets Stripping with Automated Endothelial Keratoplasty (Gorovoy) DMEK: Descemets Membrane Endothelial Keratoplasty (Melles) DMAEK: Descemets Membrane Automated Endothelial Keratoplasty (Price) The evolution of Endothelial Keratoplasty DLEK: Hand dissected donor placed in a hand resected bed DSAEK: Microkeratome donor placed on a smooth stripped surface DMEK: Stripped Descemet’s placed on a smooth stripped surface DMAEK: A DMEK with peripheral stroma to improve adhesion and handling

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Endothelial Keratoplasty Techniques Mark A. Terry, M.D.
Michael D. Straiko, M.D. Neda Shamie, M.D.
Endothelial Keratoplasty and DALK Course: ASCRS 2014
The speaker has a financial interest in the EK instruments which he designed.
The author has had research support from Fischer Instruments
The author has been a sponsored speaker for Alcon
DISCLOSURE
Endothelial Keratoplasty: Current technique, complications and
clinical results
Mark A. Terry, MD Director, Corneal Services
Devers Eye Institute
DD
Scientific Director Lions VisionGift Research Lab
Portland, Oregon, U.S.A.
Endothelial Keratoplasty (EK) is a form of corneal transplantation that replaces just the posterior diseased cornea, leaving the
corneal surface relatively untouched.
Endothelial Keratoplasty: Multiple names and acronyms
! PLK: Posterior Lamellar Keratoplasty (Melles) ! DLEK: Deep Lamellar Endothelial
Keratoplasty (Terry) ! DSEK: Descemets Stripping Endothelial
Keratoplasty (Melles) ! DSAEK: Descemets Stripping with Automated
Endothelial Keratoplasty (Gorovoy) ! DMEK: Descemets Membrane Endothelial
Keratoplasty (Melles) ! DMAEK: Descemets Membrane Automated
Endothelial Keratoplasty (Price)
The evolution of Endothelial Keratoplasty
DLEK: Hand dissected donor placed in a hand resected bed
DSAEK: Microkeratome donor placed on a smooth stripped surface
DMEK: Stripped Descemet’s placed on a smooth stripped surface
DMAEK: A DMEK with peripheral stroma to improve adhesion and handling

Our Current experience with over 1,800 cases of EK surgery from March 2000 to
April 2013 (Prospective IRB Study)
We developed and performed the first EK procedure in the U.S.:
! 275 cases of DLEK (9mm and 5 mm inc) ! 37 cases of DSEK ! Over 1,400 cases of DSAEK ! >90 cases DMEK
We have published over 100 peer- reviewed research papers, review articles, editorials, and book chapters on endothelial keratoplasty
DSAEK: Pre-op Diagnosis
! Reason for transplant: First 725 DSAEK cases 575 Fuchs (79%)
• 110 PBK (15%) • 5 Other endothelial failure (.7%) • 24 failed PK (3%) • 6 ABK (.8%) • 5 ICE (.7%)
! Patients with comorbidity: 210 (29%)
Visual results: 6 months Fuchs’ Dystrophy Eyes
Visual Results (eyes with no retinal disease) (n=160)
! mean BSCVA 20/31 (range 20/15-60)
! 93% with vision 20/40 or better
! 13% with vision 20/20 or better
Terry et al: EK for Fuchs Ophthalmology 2009; 116:631-9
What happens over time with Vision after DSAEK?
Same eyes at every time point , no co-morbidities: N=96
Time-Point 20/20 20/25 20/30
! 6 Months 15% 37% 69% ! 1 Year 18% 40% 78% ! 2 Years 33% 60% 83% ! 3 Years 44% 72% 91%
Li JY, Shamie N, Terry MA, et al: Ophthalmology 2012
Major Problems with DSAEK surgery in the U.S. (recent surveys)
! Dislocation Rate of Donor from Recipient Bed: 15% Wide range reported: 1% to 82%
! Primary (iatrogenic) Graft Failure Rate: 5% Wide range reported: 0% to 29% ! Pupillary block glaucoma: 0.1% to 9.5% ! Eccentric Donor trephination: 0% to 10%
Lee WB, Jacobs DS, Musch DC, Kaufman SC, Reinhart WJ, Shtein RM. Descemet's Stripping Endothelial Keratoplasty: Safety and Outcomes --A Report by the American Academy of Ophthalmology. Ophthalmology. 2009 Jul 28. [Epub ahead of print]
Current Complication Rates Devers Eye Institute
First 915 cases: same surgical technique (2 experienced surgeons and 7 novice) ! Dislocation rate: 2.8% (26 out of 915) ! Primary graft failure rate: <0.5% (4 out of 915)
! Pupillary Block rate: <0.2% (1 out of 915)
! Eccentric Trephinations: <0.1% (1 out of 915)
Take home message: DSAEK using our standard technique has a very low risk profile.
DSAEK
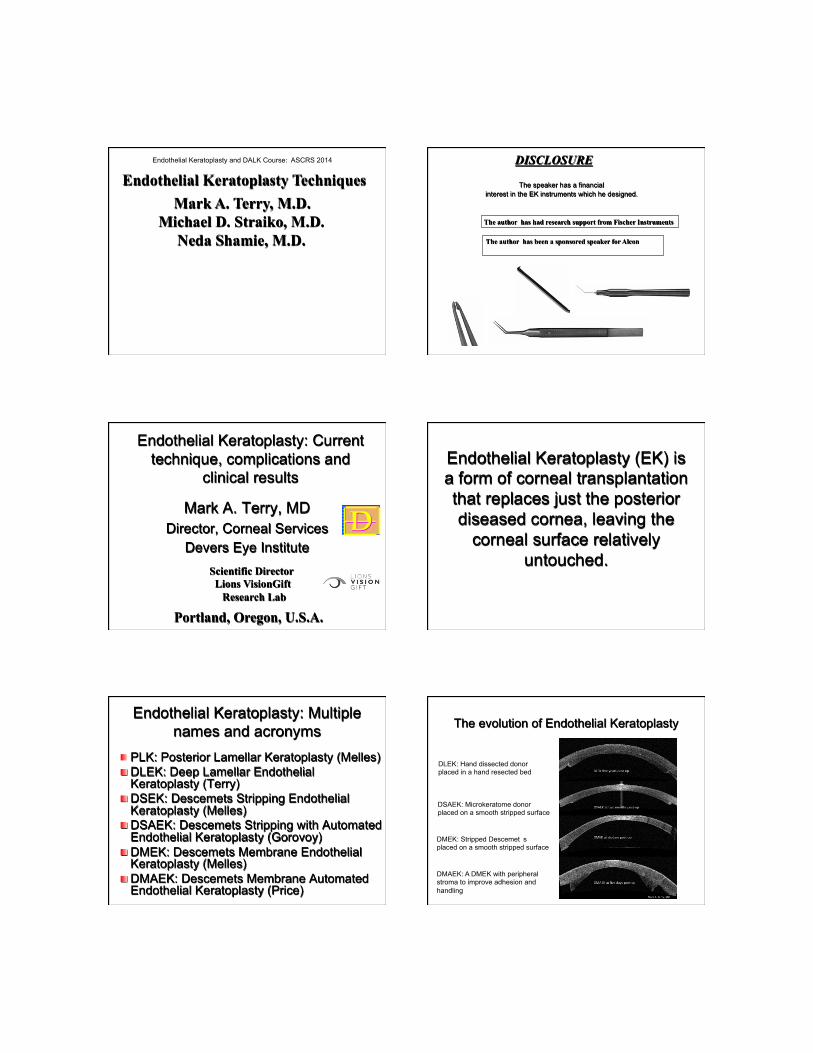
Graft Dislocation Rate by Category
2.5
5.75 5
8.1
012
3456
789
Control (n=810)
All Complex (n=105)
ACIOL (n=40)
PGS (n=62)
EK Under PK(n=20)
Dis
loca
tion
Rat
e (%
)
p = 0.259 p = 0.405 p = 0.03 CONTROL p = 0.06
5 Dislocated DSAEK Grafts in eyes with h/o Glaucoma Filtration Surgery HYPOTONY => => DISLOCATION
! pt1-trab: bleb leak noted intraop (hypotony) ! pt2-trab: IOL exchange/dislocation
day 5 ! pt3-trab: bleb leak/overfiltration by bleb with
severe hypotony ! pt4-both: no bubble in AC day 1 hypotony ! pt5-tube: severe hypotony, leaking bleb wound
Goshe JM, Terry MA, Li JY, Straiko MD, Davis-Boozer D. Graft dislocation and hypotony after DSAEK in patients with previous glaucoma surgery. Ophthalmology. 2012 Feb 29. [Epub ahead of print
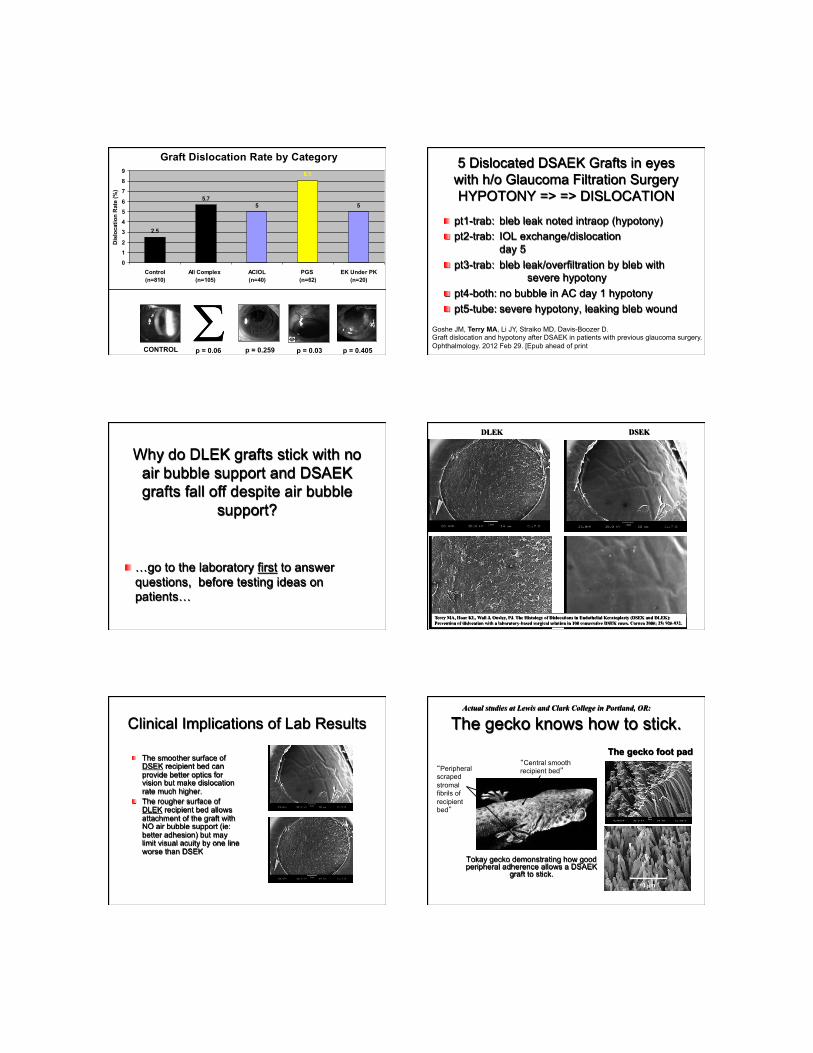
Why do DLEK grafts stick with no air bubble support and DSAEK grafts fall off despite air bubble
support?
! …go to the laboratory first to answer questions, before testing ideas on patients…
DLEK DSEK
Terry MA, Hoar KL, Wall J, Ousley, PJ. The Histology of Dislocations in Endothelial Keratoplasty (DSEK and DLEK): Prevention of dislocation with a laboratory-based surgical solution in 100 consecutive DSEK cases. Cornea 2006; 25: 926-932.
Clinical Implications of Lab Results
! The smoother surface of DSEK recipient bed can provide better optics for vision but make dislocation rate much higher.
! The rougher surface of DLEK recipient bed allows attachment of the graft with NO air bubble support (ie: better adhesion) but may limit visual acuity by one line worse than DSEK
The gecko knows how to stick.
Tokay gecko demonstrating how good peripheral adherence allows a DSAEK
graft to stick.
“Peripheral scraped stromal fibrils of recipient bed”
“Central smooth recipient bed”
The gecko foot pad
Actual studies at Lewis and Clark College in Portland, OR:

TERRY SCRAPER
Scraping the peripheral 1mm after stripping Descemet’s membrane leaves white stromal fibrils
Distal edge of Scraper is semi-sharp
Fuchs’ Dystrophy with Cataract ! First: Determine if patient needs BOTH the cataract
removed and the endothelium replaced. If very minor guttata, do phaco only and place IOL for a -1.00 myopic result…just in case.
! Second: NEVER put in a multifocal IOL in a patient with known Fuchs’ dystrophy!
! A Triple procedure (DSAEK, Phaco, IOL) is always performed in eyes that have cornea and lens disease…there is NO risk of Healon coating surfaces and preventing donor attachment. (DO NOT USE VISCOAT!)
! Make the capsulotomy 4 to 5 mm in size to keep IOL in bag during donor insertion
! If Bullae central and obscuring the view: Scrape the central 8 mm off to improve view…no dislocations associated with this maneuver.
! If edema horrible for visualization or getting keratometry, consider doing DSAEK first, and once cornea clears, do Phaco 2 months later.
Key points to avoiding complications in DSAEK surgery ! Use 5 mm scleral incision at limbus - good wound construction! ! Minimize trauma to donor at EVERY step of the surgery ! Do peripheral scraping of bed – NOT SUBTLE! ! Modulate the size of the pupil for what you need:
--dilate pupil (without NSAIDS) for cataract surgery --constrict pupil (with Miochol and stroking iris) for insertion of tissue --dilate pupil (with standard drops) at end of case to prevent block
! To remove interface fluid: sweep cornea with elevated IOP of air-leave IOP at above 40 for 2 to 3 minutes then lower to normal for 7 to 8 minutes – total 10 min wait time
! Venting incisions are NOT necessary and can cause epithelial ingrowth and infections of interface!
! Close scleral wound with vicryl sutures: prevent hypotony ! Remove ALL air from eye, then replace with only a 5 or 6 mm
air bubble…NO Need to see patient 1 hour later after surgery. ! Patient SUPINE for 1 hour then as much as possible day of
surgery – NO Pressure on Eye!
Interface Fluid Centrally: Only where the recipient bed edges were scraped are holding the graft on
Different meridians show the areas of attachment and also the access region for interface fluid
1 year s/p DSAEK - VA (without glasses!) = 20/25 - Graft interface clear -Endothelial Specular = 2580 cells/mm2
Interface fluid resolves without intervention
1 day post-DSAEK UCVA=20/200
1 weeks post-DSAEK UCVA=20/200
3 weeks post-DSAEK UCVA=20/100
2 months post-DSAEK +1.25 + 1.00 x 25 = 20/40
UCVA=20/60

Take Home Points
! Scraping can provide a physical adhesion of tissue to prevent dislocation until the endothelium “wakes up” to solidify adhesion
! If tissue is attached but interface fluid…do NOT re-bubble…WAIT…tissue will attach without intervention.
! Only re-bubble if detachment is imminent or patient is impatient for vision
! One exception to the rule…
Full Thickness Edge from Eccentric Trephination Implanted Tissue Shows “Architectural Separation”
(Which will NOT resolve with observation and risks epithelial ingrowth of donor epithelium)
Take Home Point
! Use the Microscope for Trephination of the Donor Tissue to avoid Eccentric Trephination…even if you are a “pre-presbyope” you cannot reliably discern a tolerance of ¼ mm with the naked eye! (ie: an 8.5 mm trephination in a 9.0 mm bed)
! In addition: If you do NOT use a microscope for trephination, you can get an eccentric trephination and NOT EVEN KNOW IT!
Summary of practical points regarding pre-cut tissue for DSAEK:
(Experience with COLD STORAGE OPTISOL only) ! My personal experience with it is with over 1,400
cases and it has worked as well as tissue cut on site. ! Request tissue that is at least 120 microns in
thickness…thicker is easier, no detriment to vision. ! Do NOT trust any centering marks made by Eye
Bank Technician…made with naked eye and can smudge in transit.
! Care must be taken in not getting an eccentric punch…use the microscope to punch tissue!
! Ink Marks on stromal surface KILL endothelial cells! (and are not necessary)
! If you are compelled to use ink marks, use a “dry ink” method to mark the stroma, not the pen
Terry MA: Pre-cut tissue for Descemet stripping automated endothelial keratoplasty: Complications are from technique, not tissue. Cornea 2008 (Editorial); 6:627-9 Stoeger C, Holiman, J, Davis-Boozer D, Terry, MA. The endothelial safety of using a gentian violet dry ink “S” stamp for pre-cut corneal tissue. Cornea 2012;31:801-803
What else do we know about DSAEK? Most any case of endo failure can be treated successfully with DSAEK
EK under PK for old RK EK under an old RK
EK for CHED in a 7 year old EK over a Phakic Artisan AC IOL for PBK
Anecdotal Evidence DSAEK in CHED Eyes:
Long term follow-up Pre-op: CHED in 7 y/o girl Va cc = 20/200
Post-op at 3 years: Va cc = 20/30+
No Cataract, but recipient stroma is “frosty” from structural changes of chronic edema
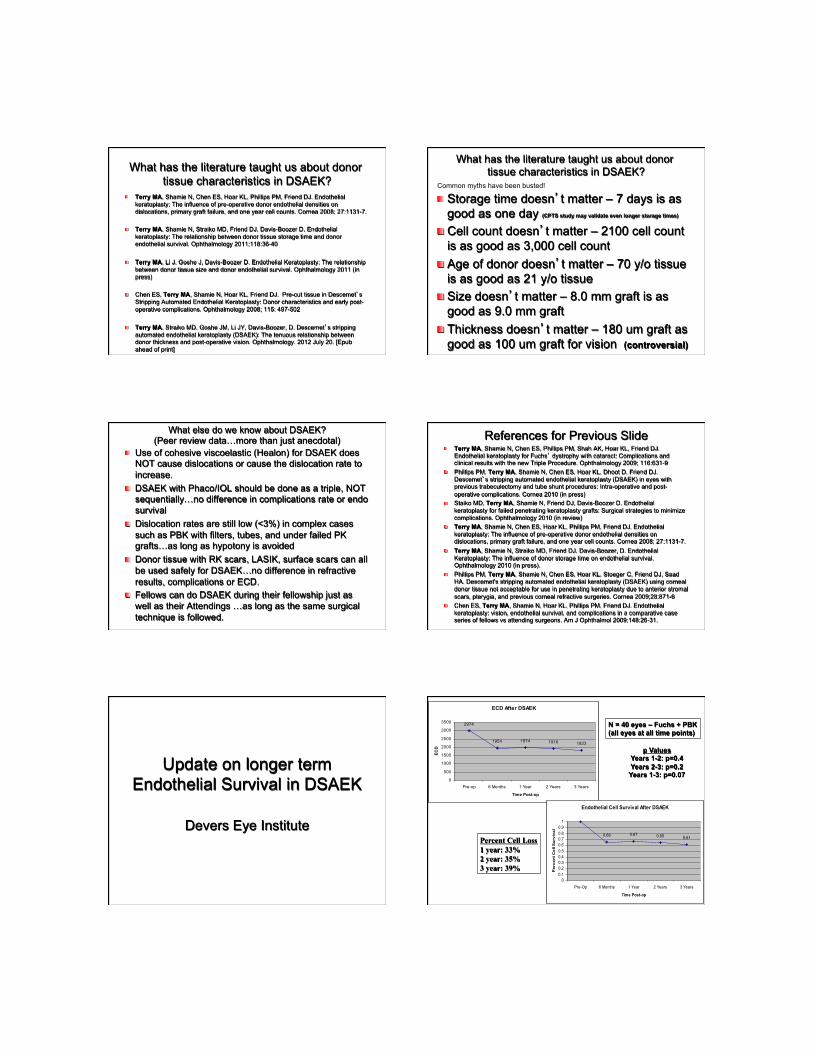
What has the literature taught us about donor tissue characteristics in DSAEK?
! Terry MA, Shamie N, Chen ES, Hoar KL, Phillips PM, Friend DJ. Endothelial keratoplasty: The influence of pre-operative donor endothelial densities on dislocations, primary graft failure, and one year cell counts. Cornea 2008; 27:1131-7.
! Terry MA, Shamie N, Straiko MD, Friend DJ, Davis-Boozer D. Endothelial keratoplasty: The relationship between donor tissue storage time and donor endothelial survival. Ophthalmology 2011;118:36-40
! Terry MA, Li J, Goshe J, Davis-Boozer D. Endothelial Keratoplasty: The relationship between donor tissue size and donor endothelial survival. Ophthalmology 2011 (in press)
! Chen ES, Terry MA, Shamie N, Hoar KL, Friend DJ. Pre-cut tissue in Descemet’s
Stripping Automated Endothelial Keratoplasty: Donor characteristics and early post-operative complications. Ophthalmology 2008; 115: 497-502
! Terry MA, Straiko MD, Goshe JM, Li JY, Davis-Boozer, D. Descemet’s stripping automated endothelial keratoplasty (DSAEK): The tenuous relationship between donor thickness and post-operative vision. Ophthalmology. 2012 July 20. [Epub ahead of print]
What has the literature taught us about donor tissue characteristics in DSAEK?
! Storage time doesn’t matter – 7 days is as good as one day (CPTS study may validate even longer storage times)
! Cell count doesn’t matter – 2100 cell count is as good as 3,000 cell count
! Age of donor doesn’t matter – 70 y/o tissue is as good as 21 y/o tissue
! Size doesn’t matter – 8.0 mm graft is as good as 9.0 mm graft
! Thickness doesn’t matter – 180 um graft as good as 100 um graft for vision (controversial)
Common myths have been busted!
What else do we know about DSAEK? (Peer review data…more than just anecdotal)
! Use of cohesive viscoelastic (Healon) for DSAEK does NOT cause dislocations or cause the dislocation rate to increase.
! DSAEK with Phaco/IOL should be done as a triple, NOT sequentially…no difference in complications rate or endo survival
! Dislocation rates are still low (<3%) in complex cases such as PBK with filters, tubes, and under failed PK grafts…as long as hypotony is avoided
! Donor tissue with RK scars, LASIK, surface scars can all be used safely for DSAEK…no difference in refractive results, complications or ECD.
! Fellows can do DSAEK during their fellowship just as well as their Attendings …as long as the same surgical technique is followed.
References for Previous Slide ! Terry MA, Shamie N, Chen ES, Phillips PM, Shah AK, Hoar KL, Friend DJ.
Endothelial keratoplasty for Fuchs’ dystrophy with cataract: Complications and clinical results with the new Triple Procedure. Ophthalmology 2009; 116:631-9
! Phillips PM, Terry MA, Shamie N, Chen ES, Hoar KL, Dhoot D, Friend DJ. Descemet’s stripping automated endothelial keratoplasty (DSAEK) in eyes with previous trabeculectomy and tube shunt procedures: Intra-operative and post-operative complications. Cornea 2010 (in press)
! Staiko MD, Terry MA, Shamie N, Friend DJ, Davis-Boozer D. Endothelial keratoplasty for failed penetrating keratoplasty grafts: Surgical strategies to minimize complications. Ophthalmology 2010 (in review)
! Terry MA, Shamie N, Chen ES, Hoar KL, Phillips PM, Friend DJ. Endothelial keratoplasty: The influence of pre-operative donor endothelial densities on dislocations, primary graft failure, and one year cell counts. Cornea 2008; 27:1131-7.
! Terry MA, Shamie N, Straiko MD, Friend DJ, Davis-Boozer, D. Endothelial Keratoplasty: The influence of donor storage time on endothelial survival. Ophthalmology 2010 (in press).
! Phillips PM, Terry MA, Shamie N, Chen ES, Hoar KL, Stoeger C, Friend DJ, Saad HA. Descemet's stripping automated endothelial keratoplasty (DSAEK) using corneal donor tissue not acceptable for use in penetrating keratoplasty due to anterior stromal scars, pterygia, and previous corneal refractive surgeries. Cornea 2009;28:871-6
! Chen ES, Terry MA, Shamie N, Hoar KL, Phillips PM, Friend DJ. Endothelial keratoplasty: vision, endothelial survival, and complications in a comparative case series of fellows vs attending surgeons. Am J Ophthalmol 2009;148:26-31.
Update on longer term Endothelial Survival in DSAEK
Devers Eye Institute
ECD After DSAEK
2974
1954 1974 1916 1823
0
500
1000
1500
2000
2500
3000
3500
Pre-op 6 Months 1 Year 2 Years 3 Years
Time Post-op
ECD
Endothelial Cell Survival After DSAEK
0.66 0.67 0.65 0.61
00.10.20.30.40.50.60.70.80.9
1
Pre-Op 6 Months 1 Year 2 Years 3 Years
Time Post-op
Per
cent
Cel
l Sur
viva
l
N = 40 eyes – Fuchs + PBK (all eyes at all time points)
p Values Years 1-2: p=0.4 Years 2-3: p=0.2 Years 1-3: p=0.07
Percent Cell Loss 1 year: 33% 2 year: 35% 3 year: 39%

5 year DSAEK data: M. Price retrospective study
Ophthalmology 2011
! N = 165 ! 89% Fuchs’ ! Forceps insertion through 5 mm incision ! Kaplan Meir Survival:
- 95% for Fuchs’, 76% for PBK ! Median Endo cell loss at 5 years:
- 53% (range=7% to 89%) (n = 90) Take Home Message: ECD after DSAEK may be better than PK long term
What about incision size for insertion of tissue?
Also: Does technique of insertion of tissue matter?
Terry MA, Saad HA, Shamie N, Chen ES, Friend DJ, Holiman JD, Stoeger C. Endothelial Keratoplasty:The influence of insertion techniques and incision size on donor endothelial survival. Cornea 2009; 28:24-31.
3mm Forceps
3mm Pull-
Through
5mm Forceps
5mm Pull-
Through
3mm Folded Pull-
Through 6
1 2
5
3mm Busin’s
Glide 4 3
Acute Endothelial Damage from Insertion: Incision size matters, method is less important
8.64
18.3917.7420.26
27.9430.4429.92
55.88
0
10
20
30
40
50
60
Average Endo. Damage
Control5mm Forceps5mm Pull-Through5mm Busin's Glide3mm Busin's Glide3mm Forceps3mm Folded Pull-Through3mm Pull-Through
5 mm
3 mm
Maneuver-Induced Endo. Damage
5mm incision size: 8% +/- 3% Damage Versus
3mm incision size: 26% +/- 13% Damage
7.71
26.41
0
10
20
30
40
50
60
Average Endo. Damage
5mm incision3mm incision
p< .001
5 mm
3 mm
Smaller incisions cause more endothelial damage: Clinical data
! Price, Gorovoy et al: Cornea 2010; 29:523-7
Incision size %loss-6 mon %loss-12 mon 3.2 mm (n=103) 40% 44% 5.0 mm (n=64) 27% 31%
p< 0.001 p< 0.001

Incision Size: 3mm v 5 mm Technique n Study
Primary Graft Failure Rate
Dislocation Rate
Endothelial Cell Loss
3 mm Incision Forceps n = 105 (Foster, Vasan, Walter Cornea 2011)
5% 28% 44% (n=52)
5 mm Incision Forceps n = 225 (Terry et al Ophthalmology 2009)
0% 2% 29%
Take Home Message REGARDLESS OF TECHNIQUE Because the wound compresses the tissue
during insertion: ! Small incision (<5mm) – Big Damage ! Larger incision (>5mm) – Small Damage
Endothelial Keratoplasty Complications
Mark A. Terry, M.D. Director, Corneal Services, Devers Eye Inst Professor, Clinical Ophthalmology, OHSU
DD
Primary Graft Failure: Attached but still edematous (upside down graft)
Pt referred to Devers after 3 prior DSAEK grafts failed
How to avoid unrecognized upside down grafts?
! Use a technique where the graft unfolds SLOWLY so you can watch for upside-down movement OR ! Place a “dry-ink” mark on peripheral
stroma to show “correct side up” (do NOT use ink pen directly on tissue)
Terry MA, Shamie N, Chen ES, Hoar KL, Friend DF. EK: A Simplified Technique. Ophthalmology 2008; 115: 1179-1186.
Stoeger C, Holiman, J, Davis-Boozer D, Terry, MA. The endothelial safety of using a gentian violet dry ink “S” stamp for pre-cut corneal tissue. Cornea 2012 (in press)
How to avoid PGF?
! Minimize endothelial trauma at every step of the procedure
! Use an insertion incision that is 5 mm or larger in length to minimize tissue compression OR ! Use an insertion device to deliver the
tissue to the AC without compression from the wound
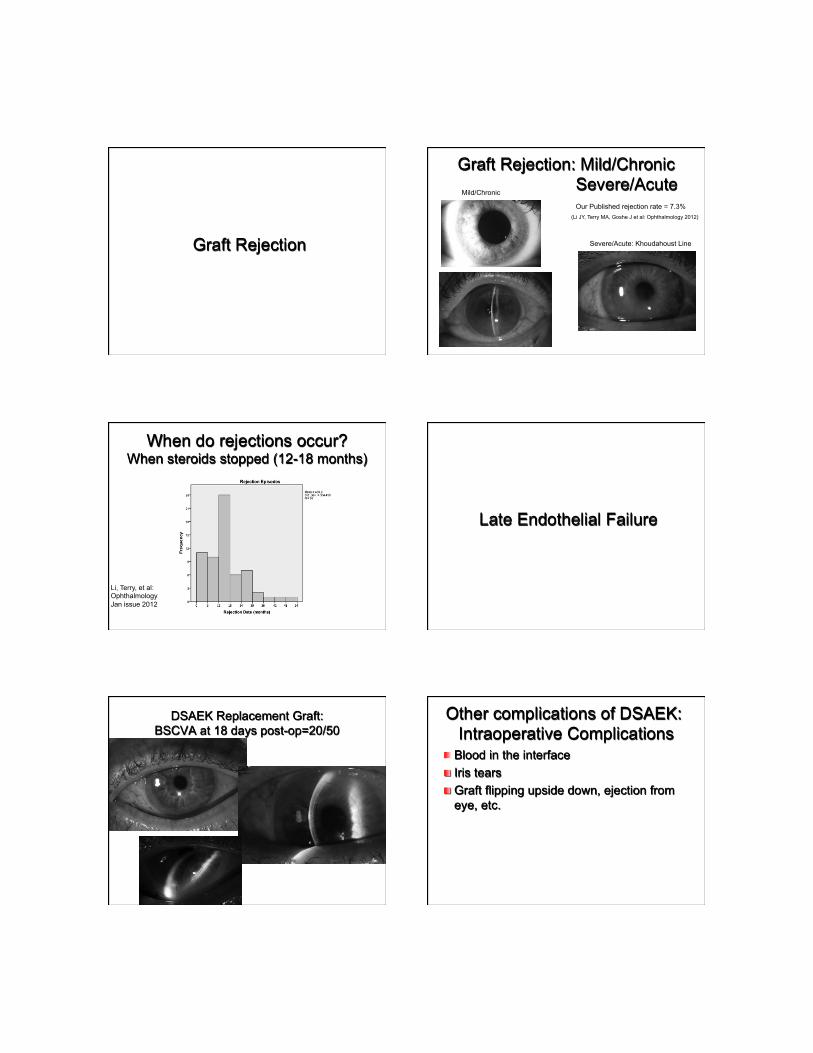
Graft Rejection
Graft Rejection: Mild/Chronic Severe/Acute Mild/Chronic
Severe/Acute: Khoudahoust Line
Our Published rejection rate = 7.3% (Li JY, Terry MA, Goshe J et al: Ophthalmology 2012)
When do rejections occur? When steroids stopped (12-18 months)
Li, Terry, et al: Ophthalmology Jan issue 2012
Late Endothelial Failure
DSAEK Replacement Graft: BSCVA at 18 days post-op=20/50
Other complications of DSAEK: Intraoperative Complications
! Blood in the interface ! Iris tears ! Graft flipping upside down, ejection from
eye, etc.
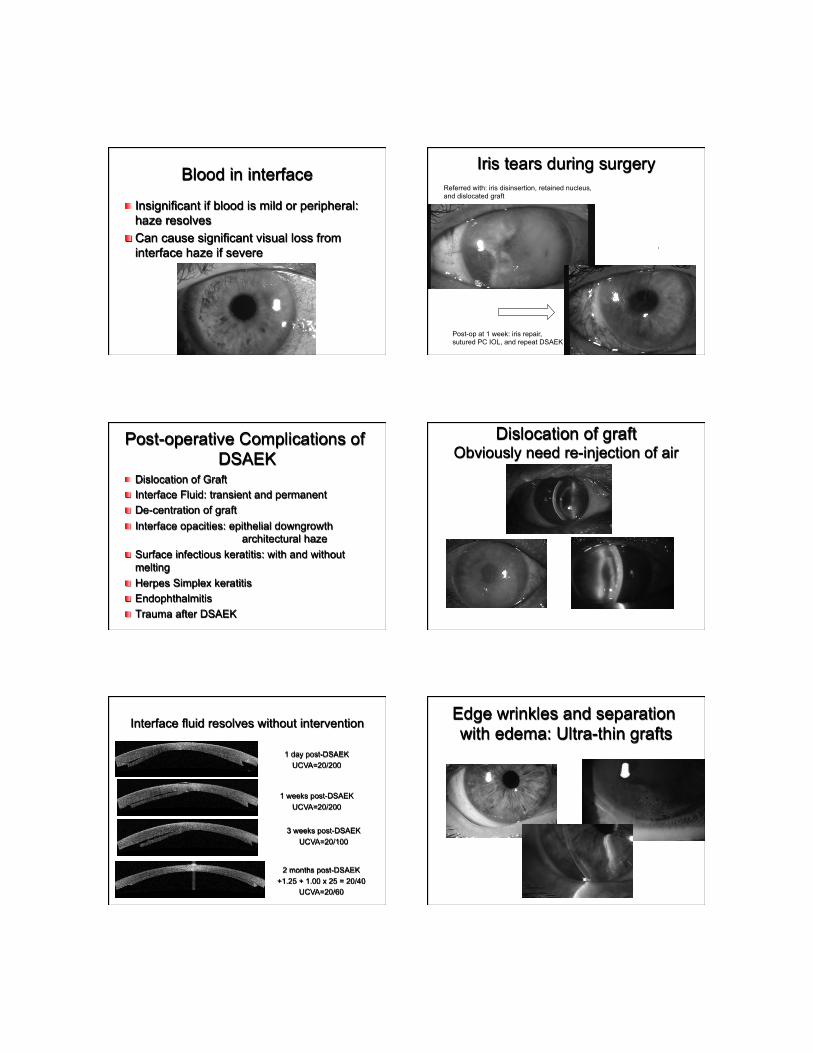
Blood in interface
! Insignificant if blood is mild or peripheral: haze resolves
! Can cause significant visual loss from interface haze if severe
Iris tears during surgery Referred with: iris disinsertion, retained nucleus, and dislocated graft
Post-op at 1 week: iris repair, sutured PC IOL, and repeat DSAEK
Post-operative Complications of DSAEK
! Dislocation of Graft ! Interface Fluid: transient and permanent ! De-centration of graft ! Interface opacities: epithelial downgrowth
architectural haze ! Surface infectious keratitis: with and without
melting ! Herpes Simplex keratitis ! Endophthalmitis ! Trauma after DSAEK
Dislocation of graft Obviously need re-injection of air
Interface fluid resolves without intervention
1 day post-DSAEK UCVA=20/200
1 weeks post-DSAEK UCVA=20/200
3 weeks post-DSAEK UCVA=20/100
2 months post-DSAEK +1.25 + 1.00 x 25 = 20/40
UCVA=20/60
Edge wrinkles and separation with edema: Ultra-thin grafts
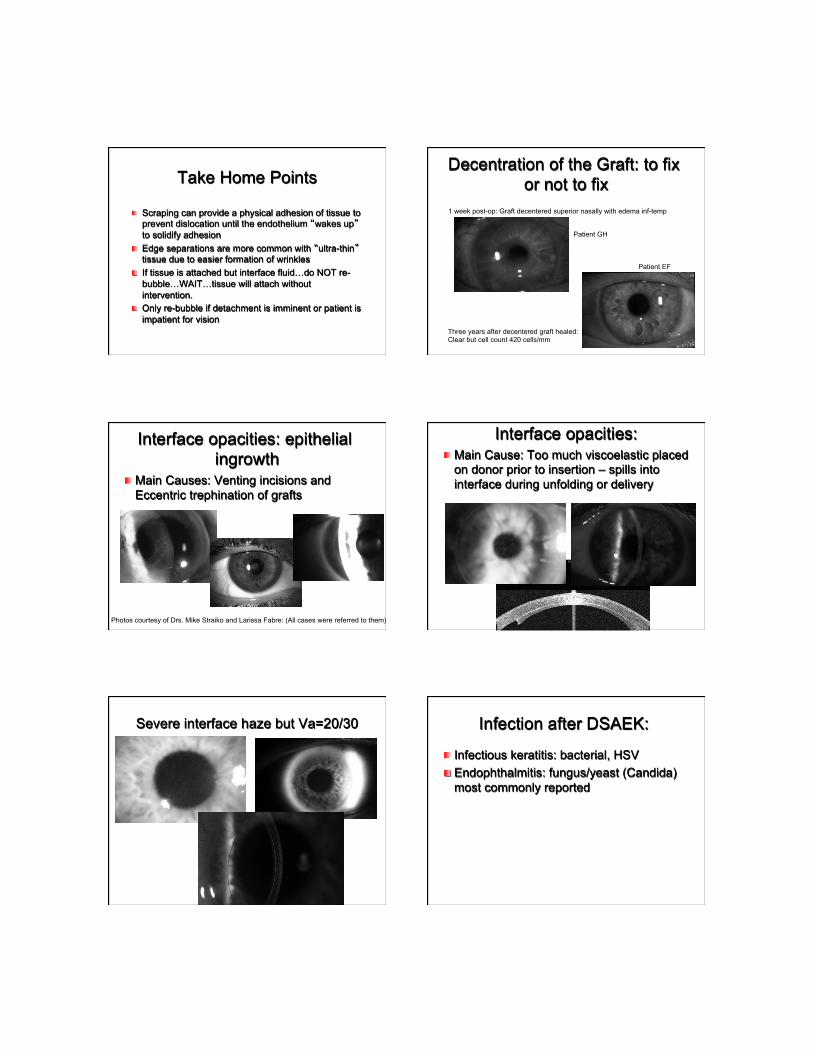
Take Home Points
! Scraping can provide a physical adhesion of tissue to prevent dislocation until the endothelium “wakes up” to solidify adhesion
! Edge separations are more common with “ultra-thin” tissue due to easier formation of wrinkles
! If tissue is attached but interface fluid…do NOT re-bubble…WAIT…tissue will attach without intervention.
! Only re-bubble if detachment is imminent or patient is impatient for vision
Decentration of the Graft: to fix or not to fix
1 week post-op: Graft decentered superior nasally with edema inf-temp
Patient GH
Patient EF
Three years after decentered graft healed: Clear but cell count 420 cells/mm
Interface opacities: epithelial ingrowth
! Main Causes: Venting incisions and Eccentric trephination of grafts
Photos courtesy of Drs. Mike Straiko and Larissa Fabre: (All cases were referred to them)
Interface opacities: ! Main Cause: Too much viscoelastic placed
on donor prior to insertion – spills into interface during unfolding or delivery
Severe interface haze but Va=20/30 Infection after DSAEK:
! Infectious keratitis: bacterial, HSV ! Endophthalmitis: fungus/yeast (Candida)
most commonly reported
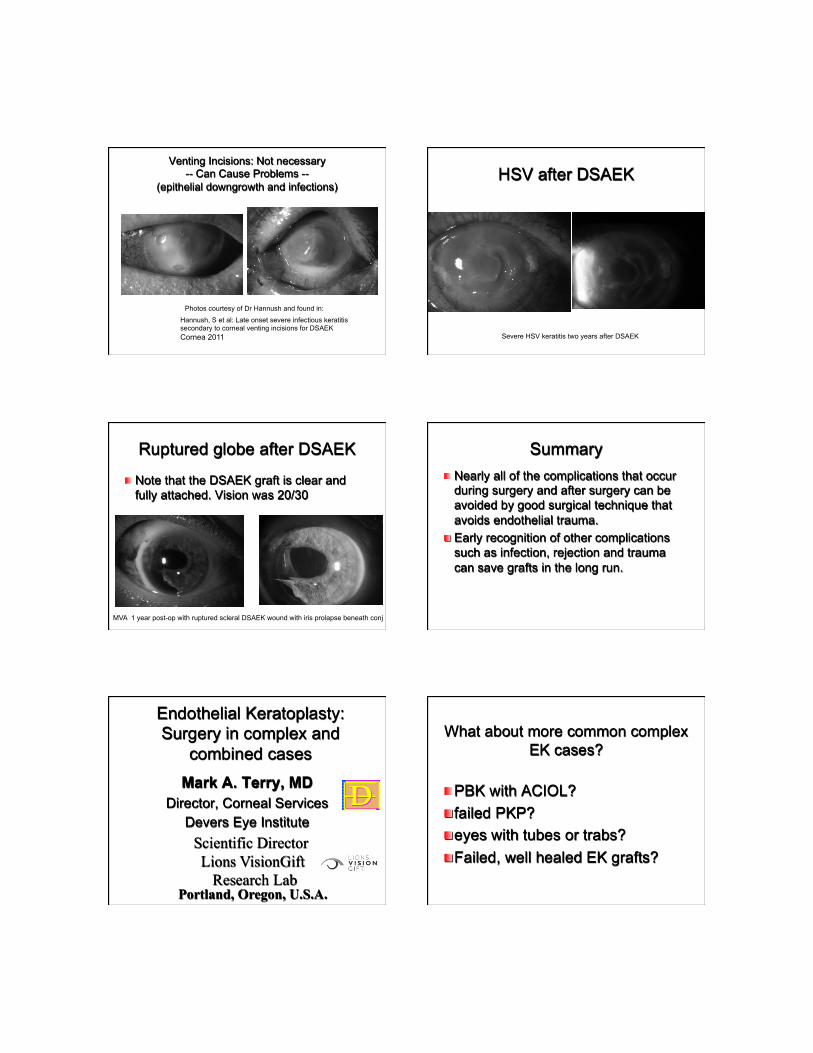
Venting Incisions: Not necessary -- Can Cause Problems --
(epithelial downgrowth and infections)
Hannush, S et al: Late onset severe infectious keratitis secondary to corneal venting incisions for DSAEK Cornea 2011
Photos courtesy of Dr Hannush and found in:
HSV after DSAEK
Severe HSV keratitis two years after DSAEK
Ruptured globe after DSAEK
! Note that the DSAEK graft is clear and fully attached. Vision was 20/30
MVA 1 year post-op with ruptured scleral DSAEK wound with iris prolapse beneath conj
Summary ! Nearly all of the complications that occur
during surgery and after surgery can be avoided by good surgical technique that avoids endothelial trauma.
! Early recognition of other complications such as infection, rejection and trauma can save grafts in the long run.
Endothelial Keratoplasty: Surgery in complex and
combined cases Mark A. Terry, MD
Director, Corneal Services Devers Eye Institute
DD
Scientific Director Lions VisionGift
Research Lab Portland, Oregon, U.S.A.
What about more common complex EK cases?
! PBK with ACIOL? ! failed PKP? ! eyes with tubes or trabs? ! Failed, well healed EK grafts?

DSAEK in Eyes with Anterior Chamber IOL
PBK with ACIOL ! 83 yo c/o gradual blurring
of vision over 2 years and onset of severe pain – closed loop ACIOL x 25
years – large sector iridectomy – vision of 20/30 until 2 years
ago ! BCVA: HM ! pachy: 935 ! bullous corneal edema,
well positioned, stable ACIOL
PBK with ACIOL: should the lens be exchanged?
! retain ACIOL if.... – stable, well positioned lens – prolonged good vision with ACIOL – delayed endothelial failure – sufficient anterior chamber depth – elderly patient – surgeon has a healthy heart
DSAEK with retained ACIOL ! preop BCVA: HM ! pachy 935 ! 1 week postop
– BCVA 20/40
! 3 months postop – BCVA 20/30
! DLEK performed, no air bubble at end of surgery
! Post-op Va = 20/25 at 5 years out ! Post-op ECD = 1626 cells/mm2 at
5 years out ! Pt seen 2012 at 10 years out: Va
same – ECD down to 600 but with clear graft
DSAEK with retained ACIOL: surgical tips
! evaluate air management early ! thorough vitrectomy critical ! Constrict pupil with Miochol and close large P.I.
for better air bubble management ! Insert graft eccentrically, protecting endothelium ! inserting folded graft puts stroma against IOL,
protecting graft endothelium ! may need to modify the unfolding, pushing IOL
posteriorly while injecting fluid or air to unfold ! ok to choose smaller graft to make unfolding
easier ! Remove most of air behind iris at end of case
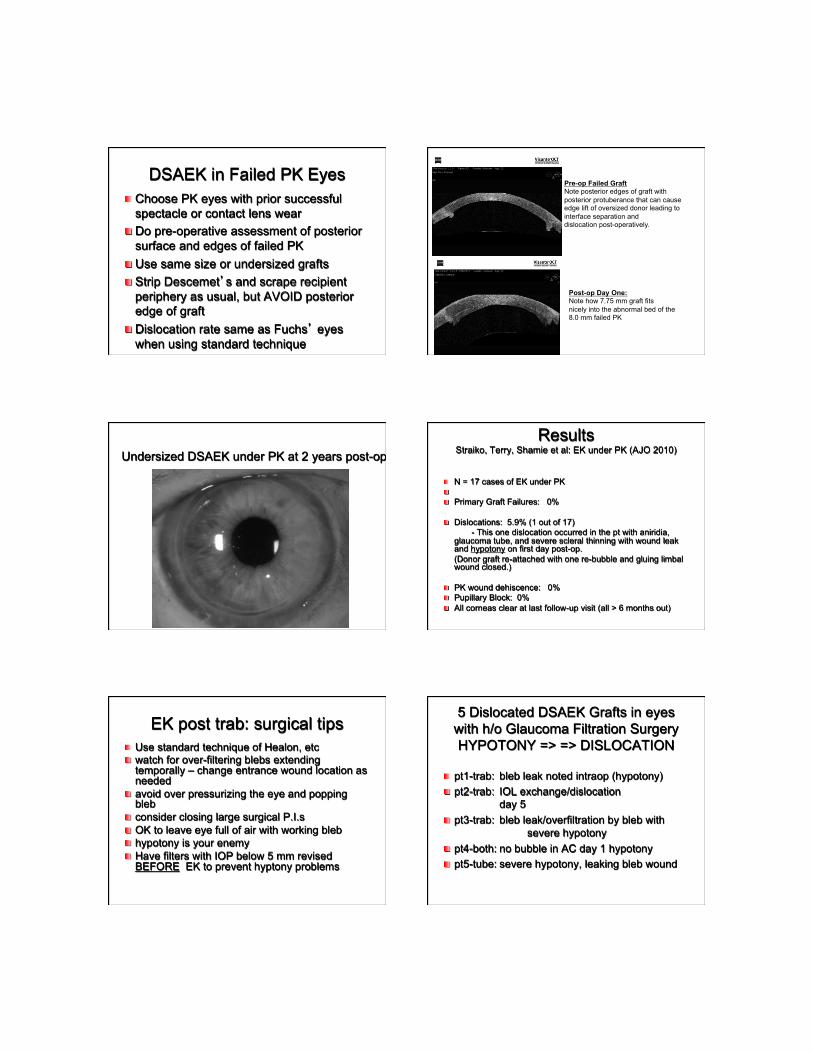
DSAEK in Failed PK Eyes ! Choose PK eyes with prior successful
spectacle or contact lens wear ! Do pre-operative assessment of posterior
surface and edges of failed PK ! Use same size or undersized grafts ! Strip Descemet’s and scrape recipient
periphery as usual, but AVOID posterior edge of graft
! Dislocation rate same as Fuchs’ eyes when using standard technique
Pre-op Failed Graft Note posterior edges of graft with posterior protuberance that can cause edge lift of oversized donor leading to interface separation and dislocation post-operatively.
Post-op Day One: Note how 7.75 mm graft fits nicely into the abnormal bed of the 8.0 mm failed PK
Undersized DSAEK under PK at 2 years post-op Results
Straiko, Terry, Shamie et al: EK under PK (AJO 2010)
! N = 17 cases of EK under PK ! ! Primary Graft Failures: 0% ! Dislocations: 5.9% (1 out of 17)
- This one dislocation occurred in the pt with aniridia, glaucoma tube, and severe scleral thinning with wound leak and hypotony on first day post-op. (Donor graft re-attached with one re-bubble and gluing limbal wound closed.)
! PK wound dehiscence: 0% ! Pupillary Block: 0% ! All corneas clear at last follow-up visit (all > 6 months out)
EK post trab: surgical tips ! Use standard technique of Healon, etc ! watch for over-filtering blebs extending
temporally – change entrance wound location as needed
! avoid over pressurizing the eye and popping bleb
! consider closing large surgical P.I.s ! OK to leave eye full of air with working bleb ! hypotony is your enemy ! Have filters with IOP below 5 mm revised
BEFORE EK to prevent hyptony problems
5 Dislocated DSAEK Grafts in eyes with h/o Glaucoma Filtration Surgery HYPOTONY => => DISLOCATION
! pt1-trab: bleb leak noted intraop (hypotony) ! pt2-trab: IOL exchange/dislocation
day 5 ! pt3-trab: bleb leak/overfiltration by bleb with
severe hypotony ! pt4-both: no bubble in AC day 1 hypotony ! pt5-tube: severe hypotony, leaking bleb wound
Repeat EK for failed DLEK or DSAEK grafts: Precautions
Standard DSAEK technique except for: ! When taking graft out,
-FIRST: cut edges of old graft with a reverse cystitome to prevent tearing recipient Descemet’s all the way to the angle
-Second: sweep interface with spatula -Third: remove graft carefully
! Re-scrape periphery of recipient bed ! For failed DLEK: make diameter of replacement DSAEK, ¼ mm smaller size
! For failed DSAEK: Make diameter of replacement DSAEK same size or larger.
Summary
! even in complex cases, surgical technique can remain mostly consistent
! respect the endothelium at every stage of the procedure
! hypotony is your enemy ! if at all possible, for corneal endothelial
disease, EK needs to be first line of surgical treatment
DSAEK: New Insertion Techniques
Mark A. Terry, M.D. Director, Corneal Services
Professor, Clinical Ophthalmology
DD
Devers Eye Institute Lions VisionGift Research Lab
Portland, Oregon, U.S.A.
What has the literature taught us about DSAEK inserters?
Insertion Devices: complications and ECD loss
! NCI: (Terry) Dislocation: 2% ECD loss: 33% ! Busin Glide: (Busin) Dislocation: 7% ECD loss: 21% - 47%
! EndoSerter: (Walter) Dislocation: 5.7% ECD loss: 28% ! EndoGlide: (Tan) Dislocation: 1.4% ECD loss: 13% - 26%
! Forceps: (Phillips) (Terry) Dislocation: 1% to 2% ECD loss: 17% to 28%
(Published Series)
Summary ! The new insertion devices currently have
only preliminary data on less than 75 eyes in each series:
Complications: ! Dislocation rates are low (1.6% to 5.7%)
and comparable to forceps insertion by experienced surgeons. (1% to 2%)
! PGF rates are low (0% to 1.6%), similar to forceps (0% to <1%) by experienced surgeons.
Summary
! ECD loss at 6 months has limited data on only a very small number of eyes (Tan=22, Terry = 47, Walter = 38)
! The ECD loss so far with inserters (13% to 28%) seems comparable to that of the Forceps (17% to 28%) and the Busin glide or Rosenwasser shovel (22%) with far larger number of eyes for analysis with these established, reusable instruments
Endothelial Cell Loss
What has the literature taught us about DSAEK inserters?
! Primary graft failure rate has been reduced in the hands of investigators
! Range of clinical Endo loss at 6-12 months between 13% (Tan EndoGlide) and 28% (EndoSerter) and not significantly different than recent large forceps series
! May be easier for some surgeons to use than forceps or other manual insertions
! Added cost of devices (about $150 per case) is main downside
Only small series available right now, and no randomized trials yet published: Therefore limited data available.
Conclusions ! The decision to use new insertion devices for DSAEK
surgery should be based on the individual surgeons satisfaction with his/her current results using his/her current technique.
! Surgeons proficient with forceps may not need to switch to insertion devices, while surgeons with high complication rates with forceps may find inserters easier and safer.
! The economic disadvantage of new insertion devices (nearly $200/case) should be weighed against the time commitment required for proficiency in established forceps and glide techniques…both of which can yield comparable results as insertion devices.
! Longer term data with higher numbers of eyes is required before the assumption of better results with inserters can be validated or disproven.
Summary of EK Techniques Talk
! The current forceps technique that we use with DSAEK surgery yields a very low dislocation rate in the hands of novice and experienced surgeons alike.
! Central Endothelial cell density (with our technique) appears to be relatively stable over the first 5 years after DSAEK, and seems better than PK, but even longer term data is needed
! DSAEK surgery should be done with 5mm or larger wounds to prevent endothelial damage – Regardless of what technique of insertion is used.
! Newer insertion devices (such as injectors) which avoid wound compression should help reduce endothelial damage and improve long term cell counts, but so far the data doesn’t show that.
! Strict adherence to an established DSAEK technique will yield a near 0% rate of PGF and a dislocation rate of less than 2% with good vision within weeks and 91% 20/30 or better (44% 20/20 or better) over time .
Deep Anterior Lamellar Keratoplasty (DALK): A Safer Technique
Mark A. Terry, MD Director, Corneal Services
Devers Eye Institute
DDScientific Director Lions Vision Gift
Research Lab
Portland, Oregon, U.S.A.
ASCRS- 2013
Disclosure
! No financial interest in this presentation ! Other non-relevant disclosures
-Bausch and Lomb Surgical -Optovue -Alcon -Fischer Surgical -Katena

Main indications for DALK ! Corneal scars with healthy endothelium ! Herpes Simplex scarring ! Herpes Zoster scarring ! Ectasia following Lasik surgery ! Ectasia following RK surgery ! Atopic Disease ! Down’s Syndrome patients ! Deeply vascularized corneas
(any corneal disease with healthy endothelium) DALK complications
! Intra-operative: perforation of Descemet’s membrane during resection of recipient stroma: Incidence between 2% and 30%
! Post-operative: All same problems with sutures and astigmatism as PK
! Post-operative: stronger resistance to rupture of wound than PK
! May be more “reactive” to relaxing incisions than PK
Tips for Avoiding Conversion to PK ! Avoid cases with prior Descemet’s
membrane breaks (Hydrops, 100% scarring, etc)
! Avoid over-inflation and bursting of Big Bubble
! After Big Bubble, keep eye extremely soft by frequent milking of the paracentesis site
! Use Healon liberally to maintain pre-Descemet’s space
! Use blunt tipped scissors (Cindy Scissors) for resection
! Try to avoid urge to resect very last fibers of peripheral posterior stroma – “The enemy of good is better”
Other Surgical Tips ! Get pachymetry map pre-operatively to determine
thinnest area for trephination depth estimation and cap resection considerations
! Mark the recipient rim with marking pen BEFORE injection Big Bubble – helps with visualization of edge for resection if stroma of rim whitens diffusely
! If not sure Big Bubble is there: Inject small amount of air into AC through paracentesis site – if Big Bubble present, air goes to peripheral area of chamber; if Big Bubble absent, air goes to central area of chamber.
! Use same size graft for keratoconus pts and moderate myopia eyes and use 0.25 mm oversize grafts for others
! Suture graft in place with preferred method, but be care to suture tighter than with standard PK
! Suture and Tuck edges of donor under recipient rim to avoid edge lift
What to do if you have a perforation ! Stop cursing immediately ! Assess the extent of the perforation:
Central? Peripheral? Extending? ! Place air bubble into AC to close defect ! Carefully complete dissection, recognizing
that only the central area needs to be near baring of Descemet’s
! Inject further air and position pt to allow coverage of perforation site by bubble
! Dilate pupil ! What if perforation is not noted until next
day? (eg: a suture needle pass perforation)…..Place full bubble and P.I.
Summary
! Lamellar corneal transplantation allows the selective replacement of only the diseased portion of the cornea, leaving the healthy corneal tissues behind.
! Lamellar techniques (EK and DALK) should be learned by every transplant surgeon wishing to offer their patients safer surgery with faster visual rehabilitation.
Related Documents











![Transplantation - OMICS Publishing Group · endothelial keratoplasty (DSAEK) has become a standard procedure for corneal transplantation in patients with endothelial dysfunction [20-23].](https://static.cupdf.com/doc/110x72/5f025baf7e708231d403e06d/transplantation-omics-publishing-group-endothelial-keratoplasty-dsaek-has-become.jpg)