Endoscopic Endonasal Management of Orbital Pathologies Paolo Castelnuovo, MD a,b , Mario Turri-Zanoni, MD a,b, *, Paolo Battaglia, MD a,b , Davide Locatelli, MD b,c , Iacopo Dallan, MD b,d INTRODUCTION External approaches to the orbit are well estab- lished, including transconjunctival, transcranial, or lateral orbitotomies, depending on the localiza- tion of the lesion. Among these, orbitozygomatic craniotomy is generally used for lesions that extend intracranially and into the orbit and is used for exposure of the optic nerve and canal. 1 The transnasal endoscopic route, initially devel- oped for treating inflammatory sinuses disease, has emerged in the last decades as a minimally invasive corridor to approach adjacent anatomic areas such as ventral skull base, orbit, and orbital apex regions. 2 What is paramount for the applica- tion of endoscopic transnasal approaches to the orbit is the close anatomic relationship between the paranasal sinuses and the orbital content, sum- marized in the concept of sino-orbito-cranial inter- face. 3 In this respect, endoscopic visualization from the transnasal route has provided surgeons the possibility of reaching the medial orbital struc- tures as well as the orbital apex region without skin incision, major bony work, or brain retraction. Given these facts, endoscopic endonasal orbital and optic nerve decompressions have become accepted treatments for thyroid eye disease 4 and traumatic optic neuropathy that is unresponsive to steroids. 5 The endoscopic endonasal technique is widely used as well for ophthalmologic proce- dures such as drainage of subperiosteal abscesses and dacryocystorhinostomy. Recently, some All the authors certify that they have no conflict of interest or financial relationship with any entity mentioned in the article. No sponsors or grants are involved in the article. a Unit of Otorhinolaryngology, Department of Biotechnology and Life Sciences (DBSV), Ospedale di Circolo e Fondazione Macchi, University of Insubria, via Guicciardini 9, Varese 21100, Italy; b Head and Neck Surgery & Forensic Dissection Research Center (HNS&FDRc), DBSV, University of Insubria, via Guicciardini 9, Varese 21100, Italy; c Unit of Neurosurgery, Civic Hospital, via Papa Giovanni Paolo II, Legnano 20025, Italy; d First Otorhino- laryngologic Unit, Azienda Ospedaliero-Universitaria Pisana, via Paradisa 2, Pisa 56124, Italy * Corresponding author. Unit of Otorhinolaryngology, Azienda Ospedaliero-Universitaria Ospedale di Circolo e Fondazione Macchi, University of Insubria, Via Guicciardini 9, Varese 21100, Italy. E-mail address: [email protected] KEYWORDS Endoscopic assisted Endonasal approach Skull base Orbit Optic nerve Paranasal sinuses KEY POINTS Endoscopic endonasal techniques are able to reach the medial orbital structures as well as the orbital apex region without skin incision and brain retraction. The endoscopic endonasal management of orbital pathologic conditions may include the complete removal of the lesion or only a tissue sampling for diagnostic purposes. The lateral limit of the transnasal approach is represented by the course of the optic nerve that must not be crossed. Endonasal approaches can be used in combination with superior/inferior eyelid approaches to manage complex lesions involving the orbit, the superior/inferior orbital fissure, and the anterior/ middle skull base (multiportal surgery). Neurosurg Clin N Am - (2015) -–- http://dx.doi.org/10.1016/j.nec.2015.03.001 1042-3680/15/$ – see front matter Ó 2015 Elsevier Inc. All rights reserved. neurosurgery.theclinics.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Endoscopic EndonasalManagement of Orbital
Pathologies Paolo Castelnuovo, MDa,b, Mario Turri-Zanoni, MDa,b,*,Paolo Battaglia, MDa,b, Davide Locatelli, MDb,c,Iacopo Dallan, MDb,dKEYWORDS
� Endoscopic assisted � Endonasal approach � Skull base � Orbit � Optic nerve � Paranasal sinuses
KEY POINTS
� Endoscopic endonasal techniques are able to reach the medial orbital structures as well as theorbital apex region without skin incision and brain retraction.
� The endoscopic endonasal management of orbital pathologic conditions may include the completeremoval of the lesion or only a tissue sampling for diagnostic purposes.
� The lateral limit of the transnasal approach is represented by the course of the optic nerve that mustnot be crossed.
� Endonasal approaches can be used in combination with superior/inferior eyelid approaches tomanage complex lesions involving the orbit, the superior/inferior orbital fissure, and the anterior/middle skull base (multiportal surgery).
INTRODUCTION
External approaches to the orbit are well estab-lished, including transconjunctival, transcranial,or lateral orbitotomies, depending on the localiza-tion of the lesion. Among these, orbitozygomaticcraniotomy is generally used for lesions thatextend intracranially and into the orbit and isused for exposure of the optic nerve and canal.1
The transnasal endoscopic route, initially devel-oped for treating inflammatory sinuses disease,has emerged in the last decades as a minimallyinvasive corridor to approach adjacent anatomicareas such as ventral skull base, orbit, and orbitalapex regions.2 What is paramount for the applica-tion of endoscopic transnasal approaches to the
All the authors certify that they have no conflict of interein the article. No sponsors or grants are involved in thea Unit of Otorhinolaryngology, Department of BiotechnoFondazione Macchi, University of Insubria, via GuicciardiForensic Dissection Research Center (HNS&FDRc), DBSV, UItaly; c Unit of Neurosurgery, Civic Hospital, via Papa Giovlaryngologic Unit, Azienda Ospedaliero-Universitaria Pisa* Corresponding author. Unit of Otorhinolaryngology, Ae Fondazione Macchi, University of Insubria, Via GuicciaE-mail address: [email protected]
Neurosurg Clin N Am - (2015) -–-http://dx.doi.org/10.1016/j.nec.2015.03.0011042-3680/15/$ – see front matter � 2015 Elsevier Inc. All
orbit is the close anatomic relationship betweenthe paranasal sinuses and the orbital content, sum-marized in the concept of sino-orbito-cranial inter-face.3 In this respect, endoscopic visualizationfrom the transnasal route has provided surgeonsthe possibility of reaching the medial orbital struc-tures as well as the orbital apex region withoutskin incision, major bony work, or brain retraction.
Given these facts, endoscopic endonasal orbitaland optic nerve decompressions have becomeaccepted treatments for thyroid eye disease4 andtraumatic optic neuropathy that is unresponsiveto steroids.5 The endoscopic endonasal techniqueis widely used as well for ophthalmologic proce-dures such asdrainage of subperiosteal abscessesand dacryocystorhinostomy. Recently, some
st or financial relationship with any entity mentionedarticle.logy and Life Sciences (DBSV), Ospedale di Circolo eni 9, Varese 21100, Italy; b Head and Neck Surgery &niversity of Insubria, via Guicciardini 9, Varese 21100,anni Paolo II, Legnano 20025, Italy; d First Otorhino-na, via Paradisa 2, Pisa 56124, Italyzienda Ospedaliero-Universitaria Ospedale di Circolordini 9, Varese 21100, Italy.
rights reserved. neurosurgery.th
eclinics.com
Castelnuovo et al2
studies concerning the endoscopic endonasal bi-opsy, debulking, or even radical resection oftumors involving the orbit also have been reported,expanding the indications for such endonasalapproaches.6,7 Herein are described the anatomicprinciples, indications, technical nuances, and lim-itations of the endoscopic endonasal approachesfor the management of selected orbital pathologicconditions.
INDICATIONS AND CONTRAINDICATIONS
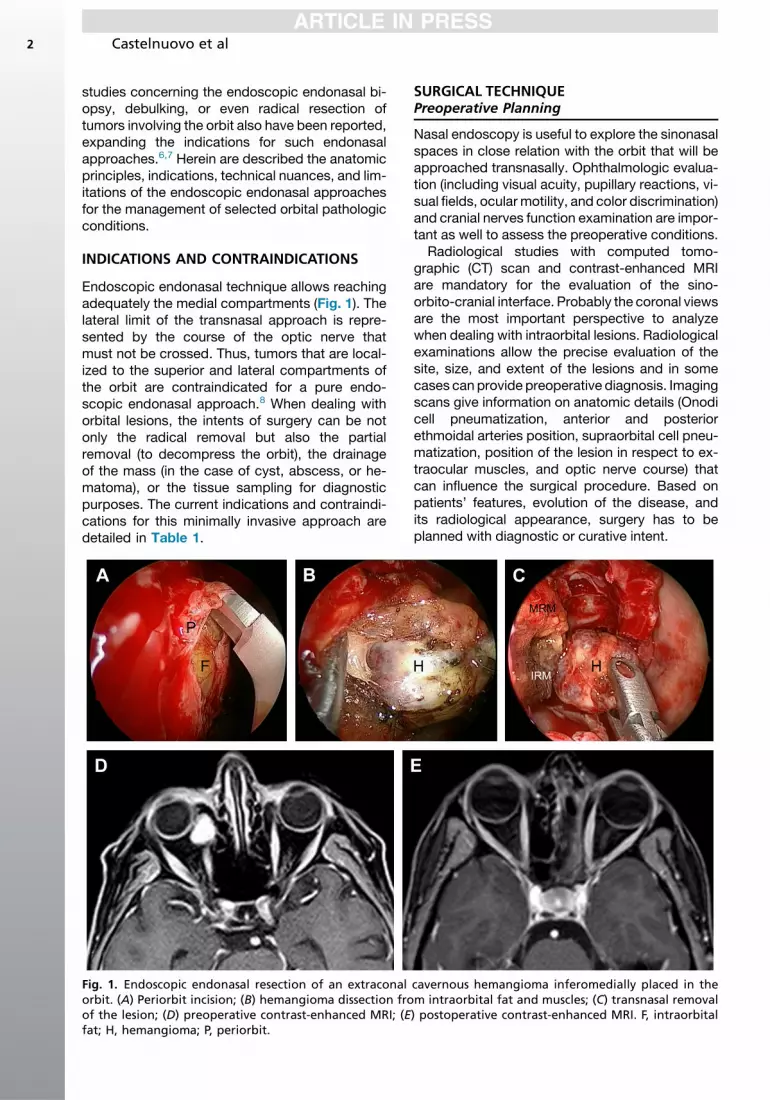
Endoscopic endonasal technique allows reachingadequately the medial compartments (Fig. 1). Thelateral limit of the transnasal approach is repre-sented by the course of the optic nerve thatmust not be crossed. Thus, tumors that are local-ized to the superior and lateral compartments ofthe orbit are contraindicated for a pure endo-scopic endonasal approach.8 When dealing withorbital lesions, the intents of surgery can be notonly the radical removal but also the partialremoval (to decompress the orbit), the drainageof the mass (in the case of cyst, abscess, or he-matoma), or the tissue sampling for diagnosticpurposes. The current indications and contraindi-cations for this minimally invasive approach aredetailed in Table 1.
Fig. 1. Endoscopic endonasal resection of an extraconalorbit. (A) Periorbit incision; (B) hemangioma dissection froof the lesion; (D) preoperative contrast-enhanced MRI; (Efat; H, hemangioma; P, periorbit.
SURGICAL TECHNIQUEPreoperative Planning
Nasal endoscopy is useful to explore the sinonasalspaces in close relation with the orbit that will beapproached transnasally. Ophthalmologic evalua-tion (including visual acuity, pupillary reactions, vi-sual fields, ocular motility, and color discrimination)and cranial nerves function examination are impor-tant as well to assess the preoperative conditions.Radiological studies with computed tomo-
graphic (CT) scan and contrast-enhanced MRIare mandatory for the evaluation of the sino-orbito-cranial interface. Probably the coronal viewsare the most important perspective to analyzewhen dealing with intraorbital lesions. Radiologicalexaminations allow the precise evaluation of thesite, size, and extent of the lesions and in somecases can provide preoperative diagnosis. Imagingscans give information on anatomic details (Onodicell pneumatization, anterior and posteriorethmoidal arteries position, supraorbital cell pneu-matization, position of the lesion in respect to ex-traocular muscles, and optic nerve course) thatcan influence the surgical procedure. Based onpatients’ features, evolution of the disease, andits radiological appearance, surgery has to beplanned with diagnostic or curative intent.
cavernous hemangioma inferomedially placed in them intraorbital fat and muscles; (C) transnasal removal) postoperative contrast-enhanced MRI. F, intraorbital
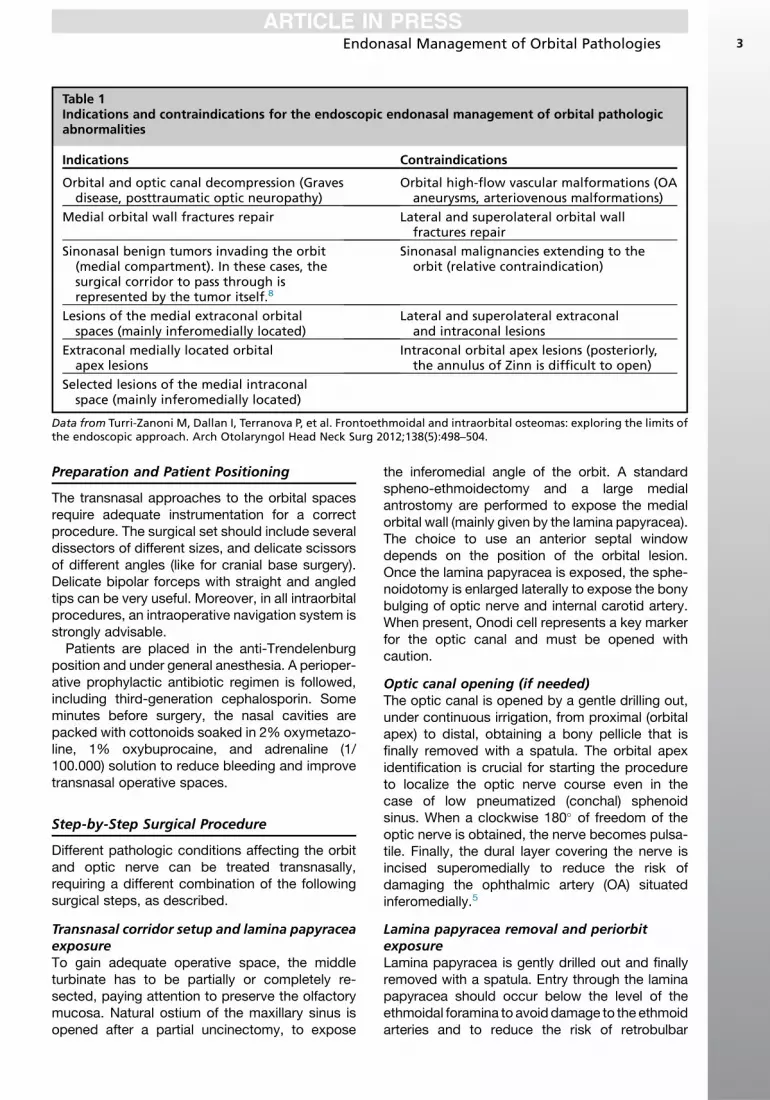
Table 1Indications and contraindications for the endoscopic endonasal management of orbital pathologicabnormalities
Indications Contraindications
Orbital and optic canal decompression (Gravesdisease, posttraumatic optic neuropathy)
Orbital high-flow vascular malformations (OAaneurysms, arteriovenous malformations)
Medial orbital wall fractures repair Lateral and superolateral orbital wallfractures repair
Sinonasal benign tumors invading the orbit(medial compartment). In these cases, thesurgical corridor to pass through isrepresented by the tumor itself.8
Sinonasal malignancies extending to theorbit (relative contraindication)
Lesions of the medial extraconal orbitalspaces (mainly inferomedially located)
Lateral and superolateral extraconaland intraconal lesions
Extraconal medially located orbitalapex lesions
Intraconal orbital apex lesions (posteriorly,the annulus of Zinn is difficult to open)
Selected lesions of the medial intraconalspace (mainly inferomedially located)
Data from Turri-Zanoni M, Dallan I, Terranova P, et al. Frontoethmoidal and intraorbital osteomas: exploring the limits ofthe endoscopic approach. Arch Otolaryngol Head Neck Surg 2012;138(5):498–504.
Endonasal Management of Orbital Pathologies 3
Preparation and Patient Positioning
The transnasal approaches to the orbital spacesrequire adequate instrumentation for a correctprocedure. The surgical set should include severaldissectors of different sizes, and delicate scissorsof different angles (like for cranial base surgery).Delicate bipolar forceps with straight and angledtips can be very useful. Moreover, in all intraorbitalprocedures, an intraoperative navigation system isstrongly advisable.
Patients are placed in the anti-Trendelenburgposition and under general anesthesia. A perioper-ative prophylactic antibiotic regimen is followed,including third-generation cephalosporin. Someminutes before surgery, the nasal cavities arepacked with cottonoids soaked in 2% oxymetazo-line, 1% oxybuprocaine, and adrenaline (1/100.000) solution to reduce bleeding and improvetransnasal operative spaces.
Step-by-Step Surgical Procedure
Different pathologic conditions affecting the orbitand optic nerve can be treated transnasally,requiring a different combination of the followingsurgical steps, as described.
Transnasal corridor setup and lamina papyraceaexposureTo gain adequate operative space, the middleturbinate has to be partially or completely re-sected, paying attention to preserve the olfactorymucosa. Natural ostium of the maxillary sinus isopened after a partial uncinectomy, to expose
the inferomedial angle of the orbit. A standardspheno-ethmoidectomy and a large medialantrostomy are performed to expose the medialorbital wall (mainly given by the lamina papyracea).The choice to use an anterior septal windowdepends on the position of the orbital lesion.Once the lamina papyracea is exposed, the sphe-noidotomy is enlarged laterally to expose the bonybulging of optic nerve and internal carotid artery.When present, Onodi cell represents a key markerfor the optic canal and must be opened withcaution.
Optic canal opening (if needed)The optic canal is opened by a gentle drilling out,under continuous irrigation, from proximal (orbitalapex) to distal, obtaining a bony pellicle that isfinally removed with a spatula. The orbital apexidentification is crucial for starting the procedureto localize the optic nerve course even in thecase of low pneumatized (conchal) sphenoidsinus. When a clockwise 180� of freedom of theoptic nerve is obtained, the nerve becomes pulsa-tile. Finally, the dural layer covering the nerve isincised superomedially to reduce the risk ofdamaging the ophthalmic artery (OA) situatedinferomedially.5
Lamina papyracea removal and periorbitexposureLamina papyracea is gently drilled out and finallyremoved with a spatula. Entry through the laminapapyracea should occur below the level of theethmoidal foramina to avoid damage to the ethmoidarteries and to reduce the risk of retrobulbar

Castelnuovo et al4
hemorrhage and vision loss. Once the lamina pap-yracea is removed, the medial aspect of the perior-bit is exposed.Generally, the superomedial angle ofthe orbit is preserved to keep the patency of thefrontal recess (Fig. 2).
Extraconal fat exposureAfter removal of the periorbit, the extraconal fat isexposed. Posteriorly, the extraconal fat is lessevident; therefore, sometimes, medial rectus mus-cle (MRM) can be found immediately below theperiorbit. At the level of the orbital apex, theannulus of Zinn is rapidly exposed below the peri-orbit and not infrequently an extraconal venouschannel is evident connecting the orbital systemwith the cavernous sinus.9
Extraconal fat removal and medial muscularwall exposureBy removing the extraconal fat, the “medialmuscular wall” comes into view. It is given mainlyby the MRM and inferior rectus muscles (IRMs)and, to a lesser part, by the superior oblique
Fig. 2. Endoscopic endonasal step-by-step surgical approremoval; (B) drilling out of the inferomedial orbital angecF, extraconal fat; FS, frontal sinus; ICA, internal carotidON, optic nerve; P, periorbit; Py, lamina papyracea; S, nasa
muscle (SOM). Between the medial and IRM, it ispossible to identify intraconal fat (Fig. 3). The ante-rior ethmoidal artery (AEA) passes between theMRM and the SOM, while the posterior ethmoidalartery usually passes above the SOM.
Approach to the intraconal spacesTo manage the medial (mostly inferomedial) intra-conal spaces, the best corridor lies between themedial and the IRMs. Sometimes, to increase thesize of this surgical window, the medial aspect ofthe orbital floor can be removed, paying attentionto preserve the infraorbital nerve, which allowsan increased mobility of the orbital structures. Inselected cases, for lesions localized posteriorly inthe orbit in a superomedial area, a surgical corridorbetween the MRM and the SOM is preferred.When this superior corridor is indicated, the AEAis generally identified, cauterized, and cut (Fig. 4).
Medial intraconal space dissectionWithin the orbit, a complex reticular system offibrous septa divides the fat into distinct lobules.
ach to the extraconal region. (A) Lamina papyraceale; (C) periorbit incision; (D) extraconal fat exposure.artery; ION, infraorbital nerve; MS, maxillary sinus;l septum; SS, sphenoid sinus.

Fig. 3. Endoscopic endonasal step-by-step surgical approach to the intraconal region. (A) Medial muscular wallexposure after removing the extraconal fat; (B) surgical corridor between MRM and SOM; (C) surgical corridorbetween medial and IRMs; (D) intraconal dissection with identification of neurovascular orbital structures.CAs, ciliary arteries; EB, eye ball; ICA, internal carotid artery; LCNs, long ciliary nerves; MRMb, branches of theMRM; ON, optic nerve.
Fig. 4. Anatomic representation of the 2 surgical cor-ridors to approach the intraconal spaces. The surgicalwindow between the MRMs and the IRMs allowapproach to the inferomedial intraconal region (espe-cially the anterior portion). The corridor between theMRM and the SOM can be used to address the poste-rior intraconal region superomedially. ACF, anteriorcranial fossa; FS, frontal sinus; MS, maxillary sinus.
Endonasal Management of Orbital Pathologies 5
These septa are well evident in the anterior orbitand bridges together extraocular muscles, thus“creating” an intraconal and extraconal space.10
Posteriorly, this division is less evident. The lateralborder of dissection is given by the optic nerve.Obviously, it is critical to avoid crossing the planeof the optic nerve. In the upper part, above an axialplane passing through the optic nerve, the OA, thenasociliary nerve (NCN), and superior ophthalmicvein (SOV) can be seen.10 In close proximity toOA, the NCN runs branching off the ethmoidalnerves (anterior and posterior) and the infratro-chlear nerve. The SOV is the largest and mostimportant vein of the orbit and usually runs closeto the OA. It usually originates by the fusionbetween the continuation of the supraorbital veinand the angular vein. On the internal aspect of theMRM, it is possible to identify the branch of the oc-ulomotor nerve and the muscular arterial branchesusually coming from the OA. As a general rule, themuscular branches are nearly all situated in the

Fig. 5. Anterior septal window illustration. This tech-nique allows approach to the anterior portion ofthe medial orbital compartment (red dotted line).
Castelnuovo et al6
intraconal side of the muscles, principally at theirposterior part. What is crucial for intraorbital lesiondissection, especially for the intraconal one, is thecareful preservation of as much neural andvascular structures as possible, even at the costof partial resection, since a given procedure willbe considered minimally invasive not only for thetype of surgical approach adopted but also mainlyfor the functional outcomes obtained.
Optic nerve exposureOnce themedial intraconal fat is removed, the intra-orbital portion of the optic nerve with its tortuouscourse becomes evident (see Fig. 3). Anteriorly,the optic nerve is closely associated with vascularnetwork, mainly given by ciliary arteries (branchesof theOA).Close to these vessels, longciliary nervesare usuallywell identifiable.10 In the posterior aspectof the orbit, posterior ciliary arteries (PCA) can beseen. They arise independently from the proximalpart of the OA: the superior PCA is always locatedsuperior to the ON. The medial PCA and the centralretinal artery (CRA) are usually the first branches ofthe OA. From an endoscopic transnasal perspec-tive, it is usually possible to identify the CRA thatusually enters the optic nerve from its inferior sur-face. Sometimes it can also reach the nerve fromits medial aspect. It should be noted that CRA isone of the smallest branches of the OA and its posi-tion is unpredictable preoperatively.10
Orbital apex exposureIn the orbital apex region, by splitting the annulusof Zinn between the MRM and IRM, the inferior di-vision of the oculomotor nerve, with its branches,becomes evident.9 Between them, the proximalpart of the orbital OA can be seen.
It is really necessary a medial orbital wallreconstruction?Contrary to what is reported by some investigators,even in the case ofwide removal of the periorbit andextensive intraorbital dissection, medial orbital wallreconstruction is not necessary.11 In the large ma-jority of cases, where only the periorbital layer isremoved, the orbital stability is warranted by the in-traorbital connective septal system. However, evenin the case of intraconal dissection with interrup-tions of the connective septa, postoperative scartissue is enough to restore the orbital continence.
Surgical Tips and Tricks
� Anterior septal window: creation of an anteriorseptal window allows a 2-nostril techniquewith a 3- to 4-hands technique and a morefavorable angle of attack. A reduced conflictbetween instruments is also provided (Fig. 5).
� Four-hands technique: it is helpful to have onesurgeon retracting the mass inferomedially,while the other surgeon uses a bimanual tech-nique to dissect tumor margins.
� Dissection: dissection along the lesion’scapsule by inserting cottonoid pledgets, tocreate space all around the lesion and to in-crease its mobilization. To note, the spacewhere cottonoids are inserted is given by theincrease in volume of the lesion itself thatgenerally has spread out the surrounding neu-rovascular structures. This surgical trick isparticularly useful for superomedially locatedlesions, approached through a superiorcorridor (between MRM and SOM).
� Medial retraction of MRM: to increase theworking window between the MRMs andIRMs, the MRM can be retracted in the direc-tion of the nasal septum.6 Usually this is doneusing a vessel loop or a stitch. This maneuverupturns the ability to dissect and work withinthe medial intraconal space, reducing at thesame time the conflicts between instruments.
� Canine fossa trephination: for introducing adissector useful to lateralize and lower theIRM. In this way, the surgical corridor lyingbetween the MRM and IRM could beaugmented.
� Extraocular muscles anterior stiffening: ante-rior stiffening of MRMs and IRMs by meansof transconjunctival looping representsanother help for transnasal orbital dissection,especially for extraconal lesions. By pullingthe stitches anteriorly, the muscles becomerigid, thus making extraconal dissectioneasier and safer.

Endonasal Management of Orbital Pathologies 7
INTRAOPERATIVE COMPLICATIONSVascular Damages
� Muscular branches, mainly of the MRM: thisvessel can be injured especially in posterioraspect of the orbit. This complication is infre-quent especially if a careful blunt perilesionaldissection is carried out.
� Central retinal artery: damage of this arteryleads to sudden blindness. Unfortunately,the position of the CRA is unpredictable.Most of the time, the artery enters the nerveon its inferior surface, but sometimes it canhave a medial entrance.
� Ciliary arteries: this network surrounds theoptic nerve and can be seen from a transnasalview. Their damage can be very serious andmay lead to severe visual impairment.
� Ophthalmic artery: given the position of theartery, direct damage of the vessel is veryrare during transnasal intraorbital procedures
Neural Damages
� Motor nerves (branches of the inferior divisionof oculomotor nerve): this lesion can lead to adysfunction of the muscles (MRMs and IRMs).These branches usually enter the muscles ontheir inner surface, in the posterior orbit.Therefore, their damage during transnasal in-traorbital procedures is not common.Notwithstanding, a careful perilesional dissec-tion is strongly advisable because it greatly re-duces the risk to damage these branches.
� Long ciliary nerves: these nerves are mainlysensory but can also contain sympathetic fi-bers for pupillary dilatation. They can be foundon the medial aspect of the optic nerve andtheir damage can lead to some disturbancesin sclera’s sensation.
� Optic nerve: a direct damage to the opticnerve is infrequent if a careful dissection isperformed, but when it occurs, it causesblindness.
Muscular Damages
The extraocular muscle with the highest risk ofdamage is the MRM. Direct trauma or even surgi-cal maneuvers by themselves can lead to a post-operative impairment of extraocular muscles withconsequent diplopia. Usually the dysfunctionsdisappear within months.
POSTOPERATIVE COMPLICATIONS
� Orbital hematoma: intraorbital blood collec-tion may occur in the case of blood vesselinjuries. To avoid increasing of intraorbital
pressure, a careful hemostasis (using warmwater irrigation, bipolar forceps, hemostaticagents) should be achieved at the end of theprocedure. Notwithstanding, given the open-ing at the level of the periorbital window, rarelya severe intraorbital hematoma develops afterthis type of procedure.
� Diplopia, especially if related to MRM impair-ment, is usually transient and should beconsidered a possible consequence of suchan approach. Persistent diplopia is a rareevent, generally related to severe injury of ex-traocular muscles or to medial displacementsof the eyeball resulting from connective tissueseptae interruptions within the orbital fat.
� Enophthalmos, resulting from orbital fat herni-ation intranasally, may occur as a late compli-cation of expanded intraconal approaches.
� Nasal obstruction and chronic rhinosinusitisare possible sequelae in the case of paranasalsinuses natural ostia blockage for scar tissueformation or for intranasal orbital fat herniation.For this reason, postoperative endoscopicevaluations and debridements are mandatoryto assess the nasal situation after surgery andto ensure patency of nasal cavity and sinuses.
POSTOPERATIVE CARE
Nasal packing, when used, is normally removedunder endoscopic visualization on the first postop-erative day. Vision and nasal endoscopy are regu-larly checked for the first few days. Duringhospitalization, CT or MRI scan is performed onlywhen complications are suspected. During theearly postoperative period, the patient is recom-mended to avoid blowing the nose for some weeksto reduce the risk of pneumo-orbit. Moreover,nasal rinsing with saline solution and sodium hya-luronate is suggested to the patient to optimize thecleaning of the nasal fossae and to accelerate thehealing process. Finally, patients should be sub-mitted to adjuvant treatments or to a regularfollow-up program, according to the biology ofthe pathologic condition treated.
OUTCOMES
The efficacy of endoscopic endonasal approachesto decompress the orbit and the optic nerve is wellknown and proved by several case seriesdescribing outcomes of endonasal procedures inthe case of Graves ophthalmopathy4 as wellas in posttraumatic optic neuropathy.5 Themanagement of intraorbital space-occupying le-sions still represents a challenge in terms of bothradical removal and biopsy for histopathological

Castelnuovo et al8
examination. Excluding single case reports, theoutcomes observed in the largest case series aresummarized in Table 2. Data emerging from thesestudies underline that the endonasal corridor has
Table 2Summary of published case series on endoscopic end
Author, YearNo. ofCases Biology of the Lesions
Lund & Rose,12
200612 12, Sph-O meningioma
Sieskiewicz et al,13
20086 2, pseudotumors
2, inflammatory lesions1, plasmocytoma1, carcinoma
McKinney et al,14
20106 Not specified
Gavriel et al,15
20103 3, intraorbital abscesse
Murchison et al,16
201112 44% benign tumors
28% malignant tumors17% inflammatorylesions
11% infectious disease
Tomazic et al,6
20116 2, cavernous hemangio
1, schwannoma1, melanoma1, lymphoma1, optic glioma
Castelnuovo et al,7
201216 6, cavernous
hemangioma2, solitary fibroustumors
2, optic nerve tumors2, metastases2, pseudotumors1, lymphoma1, intraorbital abscess
Karaki et al,17
20124 1, cavernous
hemangioma1, intraorbitalhematoma
1, inflammatory lesion1, metastasis
Netuka et al,18
20133 2, cavernous
hemangioma1, solitary fibrous tumo
Berhouma et al,19
201411 4, Sph-O meningiomas
3, optic nervemeningiomas
1, trigeminal neuroma1, pseudotumor1, ossifying fibroma
Abbreviations: c.n., cranic nerve; CSF, cerebrospinal fluid; PRorbital meningiomas.
Data from Refs.6,7,12–19
some advantages over external approaches formedial lesions. The endonasal approach mini-mizes external scarring and preserves cosmesis.On the other hand, external approaches require
onasal approach to orbital lesions
Outcomes ofSurgery Complications
s 12, debulking None
6, biopsy None
4, RR1, PR1, biopsy
Not reported
s 3, drainage None
s
Biopsy debulkingRR (numbersnot specified)
2, decreased visualacuity
1, transient diplopia1, CSF leakage
ma 2, RR1, PR3, biopsy
None
6, biopsy8, RR1, PR1, drainage
5, transient diplopia1, transient III c.n. palsy1, periorbital edema
2, biopsy1, drainage1, RR
None
r
3, RR 1, reduced eyeabduction
5, debulking4, biopsy2, RR
1, epistaxis1, pneumo-orbit
, partial resection; RR, radical resection; Sph-O, spheno-
Endonasal Management of Orbital Pathologies 9
skin incisions, osteotomies, and significantdisplacement of orbital structures, including theglobe. Given the deep, cone-shaped surgicalwindow provided by the external approach, italso has the disadvantage of suboptimal visibilitycompared with the endonasal approach. In addi-tion, external approaches to intraconal lesionsmay also require deinsertion of extraocularmuscles, with subsequent impact on extraocularmobility. For these reasons, when feasible, theendoscopic endonasal technique can be consid-ered a safe and effective surgical option tomanage the optic nerve and orbital compartments(medial side) for various posttraumatic, inflamma-tory, infective, or tumoral diseases.
FUTURE DIRECTIONS
At present, endoscopic-assisted procedures tothe orbit are mainly performed via transnasalroutes. However, alternative minimally invasiveendoscopic-assisted approaches through supe-rior and inferior eyelid incisions have beenrecently proposed to treat selected orbital patho-logic conditions placed laterally or superolaterally,outside from the orbital regions approachablefrom the transnasal route. In this way, surgeonsnowadays have available different endoscopic-assisted procedures to manage different situa-tions, for a minimally invasive comprehensiveapproach to the orbit.
Furthermore, pioneering experiences are goingto open the door to new surgical corridors for man-aging not only orbital lesions but also profounderareas. In other words, nowadays the orbit shouldbe considered not only the site of a pathologiccondition but also a potential corridor for deeperareas. Clinical experiences seem to demonstratethe feasibility and effectiveness of such “transorbi-tal” procedures. For example, anterior cranialfossa has been approached via the superior eyelidroute.20 More recently, it has been reported as apossibility to address the lateral wall of thecavernous sinus21 as well as to manage the ante-rior aspect of the temporal lobe by means of atransorbital approach.22 The possibility of usingdifferent entry windows, each one with its own ad-vantages and limits, will represent the basis for thedevelopment of the multiportal surgery concept.Obviously, this new exciting field is only in itsbeginning and requires multidisciplinary coopera-tion to increase success rates and decrease risks.
SUMMARY
Endoscopic endonasal procedures are safe andeffective to manage orbital pathologic conditions
in properly selected cases. They should be consid-ered a valid option for optic nerve or orbitalwall decompression in the case of Graves oph-thalmopathy and posttraumatic optic neuropathyas well as for addressing extraconal or intraconallesions placed medially to the optic nerve course.Future evolutions including the development ofendoscopic-assisted transorbital surgery andmul-tiportal approaches will contribute to expand theactual indications for such an approach.
REFERENCES
1. McDermott MW, Durity FA, Rootman J, et al. Com-
bined frontotemporal-orbitozygomatic approach for
tumors of the sphenoid wing and orbit. Neurosur-
gery 1990;26(1):107–16.
2. Castelnuovo P, Lepera D, Turri-Zanoni M, et al. Qual-
ity of life following endoscopic endonasal resection
of anterior skull base cancers. J Neurosurg 2013;
119(6):1401–9.
3. Dallan I, Lenzi R, de Notaris M, et al. Quantitative
study on endoscopic endonasal approach to the pos-
terior sino-orbito-cranial interface: implications and
clinical considerations. Eur Arch Otorhinolaryngol
2014;271(8):2197–203.
4. Sellari-Franceschini S, Berrettini S, Santoro A, et al.
Orbital decompression in graves’ ophthalmopathy
by medial and lateral wall removal. Otolaryngol
Head Neck Surg 2005;133(2):185–9.
5. Emanuelli E, Bignami M, Digilio E, et al. Post-trau-
matic optic neuropathy: our surgical and medical
protocol. Eur Arch Otorhinolaryngol 2014. http://dx.
doi.org/10.1007/s00405-014-3408-5.
6. Tomazic PV, Stammberger H, HabermannW, et al. In-
traoperativemedialization of medial rectusmuscle as
a new endoscopic technique for approaching intra-
conal lesions. Am J Rhinol Allergy 2011;25(5):363–7.
7. Castelnuovo P, Dallan I, Locatelli D, et al. Endo-
scopic endonasal intraorbital surgery: our experi-
ence with 16 cases. Eur Arch Otorhinolaryngol
2012;269:1929–35.
8. Turri-Zanoni M, Dallan I, Terranova P, et al. Fron-
toethmoidal and intraorbital osteomas: exploring
the limits of the endoscopic approach. Arch Otolar-
yngol Head Neck Surg 2012;138(5):498–504.
9. Dallan I, Castelnuovo P, de Notaris M, et al. Endo-
scopic endonasal anatomy of the superior orbital
fissure andorbital apex regions: critical considerations
for clinical applications. Eur Arch Otorhinolaryngol
2013;270(5):1643–9.
10. Dallan I, Seccia V, Lenzi R, et al. Transnasal
approach to the medial intraconal space: anatomic
study and clinical considerations. Minim Invasive
Neurosurg 2010;53:164–8.
11. Karligkiotis A, Appiani MC, Verillaud B, et al. How
to prevent diplopia in endoscopic transnasal
Castelnuovo et al10
resection of tumors involving the medial orbital wall.
Laryngoscope 2014;124(9):2017–20.
12. Lund VJ, Rose GE. Endoscopic transnasal
orbital decompression for visual failure due to
sphenoid wing meningioma. Eye (Lond) 2006;
20(10):1213–9.
13. Sieskiewicz A, Lyson T, Mariak Z, et al. Endoscopic
trans-nasal approach for biopsy of orbital tumours
using image-guided neuro-navigation system. Acta
Neurochir (Wien) 2008;150(5):441–5.
14. McKinney KA, Snyderman CH, Carrau RL, et al.
Seeing the light: endoscopic endonasal intraconal
orbital tumor surgery. Otolaryngol Head Neck Surg
2010;143:699–701.
15. Gavriel H, Kessler A, Eviatar E. Management
implications of diagnosing orbital abscess as
subperiosteal orbital abscess. Rhinology 2010;
48(1):90–4.
16. Murchison AP, Rosen MR, Evans JJ, et al. Endo-
scopic approach to the orbital apex and periorbital
skull base. Laryngoscope 2011;121(3):463–7.
17. KarakiM, AkiyamaK,KagawaM, et al. Indications and
limitations of endoscopic endonasal orbitotomy for
orbital lesion. J Craniofac Surg 2012;23(4):1093–6.
18. Netuka D, Masopust V, Bel�san T, et al. Endoscopic
endonasal resection of medial orbital lesions with in-
traoperative MRI. Acta Neurochir (Wien) 2013;
155(3):455–61.
19. Berhouma M, Jacquesson T, Abouaf L, et al.
Endoscopic endonasal optic nerve and orbital
apex decompression for nontraumatic optic neurop-
athy: surgical nuances and review of the literature.
Neurosurg Focus 2014;37(4):E19.
20. Andaluz N, Romano A, Reddy LV, et al. Eyelid
approach to the anterior cranial base. J Neurosurg
2008;109(2):341–6.
21. Bly RA, Ramakrishna R, Ferreira M, et al. Lateral
transorbital neuroendoscopic approach to the
lateral cavernous sinus. J Neurol Surg B Skull
Base 2014;75(1):11–7.
22. Chen HI, Bohman LE, Loevner LA, et al. Transorbital
endoscopic amygdalohippocampectomy: a feasibility
investigation. J Neurosurg 2014;120(6):1428–36.
Related Documents











