Endoscopic endonasal transsphenoidal surgery: surgical results of 228 pituitary adenomas treated in a pituitary center Jackson A. Gondim Michele Schops Joa ˜o Paulo C. de Almeida Lucas Alverne F. de Albuquerque Erika Gomes Ta ˆnia Ferraz Francisca Andre ´a C. Barroso Ó Springer Science+Business Media, LLC 2009 Abstract Pituitary tumors are challenging tumors in the sellar region. Surgical approaches to the pituitary have undergone numerous refinements over the last 100 years. The introduction of the endoscope have revolutionized pituitary surgery. The aim of this study is to report the results of a consecutive series of patients undergoing pituitary surgery using a pure endoscopic endonasal approach and to evaluate the efficacy and safety of this procedure. We reviewed the data of 228 consecutive patients who underwent endonasal transsphenoidal ade- noma removal over an 10-year period. Pre- and post- operative hormonal status (at least 3 months after surgery) were analyzed and compared with clinical parameters presented by the patients. Tumor removal rate, endocri- nological outcomes, and complications were retrospec- tively assessed in 228 patients with pituitary adenomas who underwent 251 procedures between December 1998 and December 2007. There were 93 nonfunctioning ade- nomas, 58 growth hormone-secreting, 41 prolactin- secreting, 28 adrenocorticotropin hormone secreting, 7 FSH-LH secreting and 1 thyroid-stimulating hormone- secreting adenomas. Gross total removal was achieved in 79.3% of the cases after a median follow-up of 61.5 months. The remission results for patients with non- functioning adenomas was 83% and for functioning ade- nomas were 76.3% (70.6% for GH hormone-secreting, 85.3% for prolactin hormone-secreting, 71.4% for ACTH hormone-secreting, 85.7% for FSH-LH hormone-secreting and 100% for TSH hormone-secreting), with no recurrence at the time of the last follow-up. Post-operative compli- cations were present in 35 (13.9%) cases. The most fre- quent complications were temporary and permanent diabetes insipidus (six and two cases, respectively), syn- drome of inappropriate antidiuretic hormone secretion (two cases) and CSF leaks (eight cases). There was no death related to the procedure in this series. The endoscopic endonasal approach for resection of pituitary adenomas, provides acceptable results representing a safe alternative procedure to the microscopic approach. This less invasive method, associated with a small number of complications, provides excellent tumor removal rates and represents an important tool for the achievement of good results in the pituitary surgery, mainly for the complete removal of large adenomas. Keywords Endoscopic surgery Á Endonasal Á Transsphenoidal surgery Á Pituitary adenoma Introduction The transsphenoidal approach for pituitary gland was first successfully described by Schloffer, when he reported the first transsphenoidal removal of a pituitary tumor in 1906 J. A. Gondim (&) Á J. P. C. de Almeida Á L. A. F. de Albuquerque Department of Neurosurgery, General Hospital of Fortaleza, Fortaleza, Brazil e-mail: [email protected]; [email protected] M. Schops Á J. P. C. de Almeida Á L. A. F. de Albuquerque School of Medicine, Federal University of Ceara, Fortaleza, Brazil E. Gomes Department of Ear, Nose and Throat Surgery, General Hospital of Fortaleza, Fortaleza, Brazil T. Ferraz Á F. A. C. Barroso Department of Endocrinology, General Hospital of Fortaleza, Fortaleza, Brazil 123 Pituitary DOI 10.1007/s11102-009-0195-x

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Endoscopic endonasal transsphenoidal surgery: surgical resultsof 228 pituitary adenomas treated in a pituitary center
Jackson A. Gondim Æ Michele Schops ÆJoao Paulo C. de Almeida Æ Lucas Alverne F. de Albuquerque ÆErika Gomes Æ Tania Ferraz Æ Francisca Andrea C. Barroso
� Springer Science+Business Media, LLC 2009
Abstract Pituitary tumors are challenging tumors in the
sellar region. Surgical approaches to the pituitary have
undergone numerous refinements over the last 100 years.
The introduction of the endoscope have revolutionized
pituitary surgery. The aim of this study is to report the
results of a consecutive series of patients undergoing
pituitary surgery using a pure endoscopic endonasal
approach and to evaluate the efficacy and safety of this
procedure. We reviewed the data of 228 consecutive
patients who underwent endonasal transsphenoidal ade-
noma removal over an 10-year period. Pre- and post-
operative hormonal status (at least 3 months after surgery)
were analyzed and compared with clinical parameters
presented by the patients. Tumor removal rate, endocri-
nological outcomes, and complications were retrospec-
tively assessed in 228 patients with pituitary adenomas
who underwent 251 procedures between December 1998
and December 2007. There were 93 nonfunctioning ade-
nomas, 58 growth hormone-secreting, 41 prolactin-
secreting, 28 adrenocorticotropin hormone secreting, 7
FSH-LH secreting and 1 thyroid-stimulating hormone-
secreting adenomas. Gross total removal was achieved in
79.3% of the cases after a median follow-up of
61.5 months. The remission results for patients with non-
functioning adenomas was 83% and for functioning ade-
nomas were 76.3% (70.6% for GH hormone-secreting,
85.3% for prolactin hormone-secreting, 71.4% for ACTH
hormone-secreting, 85.7% for FSH-LH hormone-secreting
and 100% for TSH hormone-secreting), with no recurrence
at the time of the last follow-up. Post-operative compli-
cations were present in 35 (13.9%) cases. The most fre-
quent complications were temporary and permanent
diabetes insipidus (six and two cases, respectively), syn-
drome of inappropriate antidiuretic hormone secretion (two
cases) and CSF leaks (eight cases). There was no death
related to the procedure in this series. The endoscopic
endonasal approach for resection of pituitary adenomas,
provides acceptable results representing a safe alternative
procedure to the microscopic approach. This less invasive
method, associated with a small number of complications,
provides excellent tumor removal rates and represents
an important tool for the achievement of good results in the
pituitary surgery, mainly for the complete removal of large
adenomas.
Keywords Endoscopic surgery � Endonasal �Transsphenoidal surgery � Pituitary adenoma
Introduction
The transsphenoidal approach for pituitary gland was first
successfully described by Schloffer, when he reported the
first transsphenoidal removal of a pituitary tumor in 1906
J. A. Gondim (&) � J. P. C. de Almeida �L. A. F. de Albuquerque
Department of Neurosurgery, General Hospital of Fortaleza,
Fortaleza, Brazil
e-mail: [email protected]; [email protected]
M. Schops � J. P. C. de Almeida � L. A. F. de Albuquerque
School of Medicine, Federal University of Ceara,
Fortaleza, Brazil
E. Gomes
Department of Ear, Nose and Throat Surgery, General Hospital
of Fortaleza, Fortaleza, Brazil
T. Ferraz � F. A. C. Barroso
Department of Endocrinology, General Hospital of Fortaleza,
Fortaleza, Brazil
123
Pituitary
DOI 10.1007/s11102-009-0195-x

[1]. Hirsch in 1910 described a direct endonasal trans-
sphenoidal approach, a procedure that involved resection of
the middle turbinate and part of the nasal septum. Such
operation was performed in five different steps at intervals
lasting days to 2 weeks [2]. In the same year, Halstead
described the sublabial gingival via [3]. Cushing in 1912
modified the sublabial transsphenoidal approach to the
sella turcica, making it essentially as it is used nowadays
[4–6]. Since then the approach, either via sublabial or via
septal has gain importance in surgical treatment for pitui-
tary adenomas [4].
In the 1950s and 1960s, Guiot, developed introperative
fluoroscopy for trassphenoidal surgery, and Hardy, that
combined fluoroscopy with microsurgical techniques,
importantly contributed to the development of the pituitary
surgery, reducing the risk of brain injure and improving the
rate of tumor resection and favorable outcome [7–10].
In 1970, Messerklinger [11] developed the endoscopic
technique. After it, the endoscope started to be used in skull
base surgery and in sellar and parasellar region [12, 13]. In
1992, Jankowski et al. [14] introduced the endoscope in the
pituitary surgery, describing the use of the endonasal
transsphenoidal endoscopic technique for removal of three
pituitary adenomas.
The transsphenoidal endoscopic guided pituitary surgery
was standardized in actual clinical practice by Carrau and
Jho [15, 16] and Cappabianca et al. [17]. The development
of neuroendoscopy and the popularization of transsphe-
noidal endoscopic guided pituitary surgery have been
associated with better tumor resection results. Although
presenting better illumination and visualization of the
lesions, no report has definitively proved the superiority of
endoscopy over microsurgery in pituitary surgery, so far.
We performed our first purely endoscopic resection of a
pituitary adenoma in 1998. Now, we report our 10 years
experience series of 228 patients treated with endoscopic
endonasal transsphenoidal surgery for pituitary adenomas.
We also compare our results with other endoscopy
and microscopy pituitary surgery series reported in the
literature.
Methods
Study design
Between May 1998 and December 2007, a total of 309
patients underwent endoscopic transsphenoidal procedures
for skull base lesions at the Neuroendocrinological
Department of General Hospital of Fortaleza, Brazil. This
retrospective study comprises the evaluation of 228 cons-
ecutives patients who underwent 251 pure endoscopic en-
donasal treatment of pituitary adenomas. Any other lesion
was excluded from the study. The authors reviewed the
patients’ files in order to collect clinical and surgical data
for the study.
All patients underwent neurologic, ophthalmologic and
endocrinologic examinations. The patient follow up varied
from 8 months to 11 years.
Endocrinological assessment
All the endocrinological investigation was performed at
our hospital. Multiple measurements of plasma GH, insu-
lin-like growth factor-I (IGF-I), GH level after oral glucose
tolerance test (OGTT), prolactin, adrenocorticotrophic
hormone (ACTH), cortisol, 24-h urinary free cortisol
(when Cushing’s disease was suspected), thyreoid-stimu-
lating hormone (TSH), free thyroxine, luteinizing hormone
(LH) and follicle stimulating hormone (FSH), testosterone,
and estradiol levels were studied. All tumors were sub-
mitted to immunohistochemical analysis of the tissue
removed.
Neuroradiology
All patients underwent tumor evaluation by magnetic res-
onance imaging (MRI), with and without administration of
intravenous contrast agent. We utilized a 1.5 Tesla MRI
with T1 and T2-weighted spin echo before and after gad-
olinium-base contrast medium. Tumor size was classified
according to maximum tumor diameter in two categories:
microadenoma (\10 mm), and macroadenomas (C10 mm).
A facial computed tomographic scan was used in all
patients to evaluate the paranasal sinuses (septal anatomy,
sphenoidal, and maxillofacial format) for surgical planning.
Follow-up MRI studies were obtained at 3 months and
every 6 months thereafter.
Surgical technique
All patients were treated by the same medical team, using
identical procedures. Under general anesthesia, the patient
is placed in the supine position on the operative table with
the back elevated 30�, the head tilted back 20�, and toward
the left shoulder 25�. The neurosurgeon is positioned on the
right side of the patient and the ear, nose and throat (ENT)
surgeon on the left side. Usually, the left nostril is used, but
the choice is based on nasal anatomy. Routinely a bilateral
approach affords significant improvement in exposure and
confort for the surgeon. A 30�, and less frequently 45 or
70�, rigid endoscope (180/4 mm) is used. The endoscope is
navigated into the nasal cavity. The floor of the sella is
located *1 cm above the inferior margin of the middle
turbinate. The space between the middle turbinate and the
nasal septum is gently widened, and a large opening is
Pituitary
123

made in the posterior internasal septum. Normally we do
not resect the middle turbinate by are gently lateralized but
preserved to promote normal post-operative middle meatus
physiology. The anterior wall of the sphenoidal sinus is
open. Inside the sphenoidal sinus, the sella is then local-
ized, the anterior wall of the sella and the dura mater are
largely opened with a highspeed drill or Kerrison rongeur.
Visualization of the sellar region is initially performed with
a 0� endoscope. Following tumor resection, both 0 and
angled (30, 45 and 70�) endoscopes are placed into the
surgical cavity to explore for any residual tumor. Intraop-
erative image guidance is used in adenomas with a retro
sellar component or adenomas presenting close contact to
the third ventricle. For the reconstruction of the sellar
region, we used a combination of fascia lata, abdominal fat,
mucoperiosteum, fibrin sealants and a vascularized nasal
septal mucosa flap as a final layer over the onlay graft,
followed by Foley catheter as a buttress that is removed in
48 h [18].
Tumor control
The aim of treatment was to remove the tumor in its totality
without causing hypopituitarism. The criteria for disease
control were tumor total removal in nonfunctioning ade-
nomas and hormonal control in functioning adenomas
(prolactinomas, GH-secreting adenomas, ACTH-secreting
adenomas, TSH-secreting adenomas and FSH/LH-secret-
ing adenomas).
The success of the tumor removal is based on both MRI
findings with contrast obtained 3 months after surgery and
the surgeon’s intraoperative vision. The tumor is consid-
ered to be totally removed when the surgeon’s vision and
MRI image examination documents no residual tumor. The
resection is considered subtotal when more than 80% of the
lesion has been removed and partial resection when less
than 80% has been removed.
The criteria for acromegaly control used were the cur-
rent internationally accepted criteria for biochemical
‘‘cure’’ of the disease [19]: the nadir GH level after oral
glucose should be less than 1 lg/l, and the IGF-1 should be
age and sex-matcher. The criteria for Cushing’s disease
control used were an early morning cortisol level mea-
surement (\100 nmol/l requiring substitutive therapy)
obtained in the first 48 h after surgery along with sup-
pression to the low-dose dexamethasone (1 mg) overnight
test and normalization of the 24-h urinary free cortisol
(both at 4 and 6 week follow-up). Prolactinomas were
considered under control when serum prolactin after
surgery was \20 ng/ml. In FSH/LH cases, normalization
of serum FSH and LH levels was required for hor-
monal control. Endocrinologically ‘‘cured’’ TSH-secreting
adenoma patients were those presenting normal levels of
T3, free T4 and TSH after surgery.
Statistical analysis
All data are expressed as mean ± standard deviation (SD).
Statistical software, SPSS 16.0 (SPSS Inc., Chicago, IL)
was used for statistical analysis, with P \ 0.05 considered
statistical significant.
Results
General analysis (see Table 1)
From 1998 to December 2007, 228 patients were admitted
in our center for surgical treatment of pituitary adenomas.
Males and females represented 44.7% (102 patients) and
55.3% (126 patients) of these, respectively. The mean age
of the studied population was 42.51 ± 15.25 years old
(range 13–79 years).
According to the size of the lesion, 190 (83.8%) tumors
were classified as macroadenomas (mean size of the
lesions: 24.68 ± 14.57 mm). Cystic components were
present in 48 cases (21.1%) and destruction of the sella
floor was detected in 93 patients (40.8%). Functioning
adenomas represented most of the lesions (135 cases,
59.3%). The most common hormone-secreting lesions were
GH secreting pituitary adenomas (58 adenomas, 25.4%),
followed by prolactinomas (41 adenomas, 17.9%). Disease
control was achieved in 33 (86.8%) cases of microadeno-
mas and 142 (74.7%) of macroadenomas.
Headache and visual complaints were present in 154
(67.5%) and 75 (32.9%) patients, respectively.
Table 1 General characteristics and analysis of 228 pituitary
adenomas
Adenomas characteristics N %
Total of patients 228 100
Nonfunctioning adenomas 93 40.7
Hormone-secreting adenomas 135 59.3
GH secreting adenomas 58 25.4
Prolactinoma 41 17.9
ACTH secreting adenomas 28 12.2
FSH/LH secreting adenomas 7 3
TSH secreting adenoma 1 0.4
Microadenomas 38 16.6
Macroadenomas 190 83.8
[10 mm 97 42.5
Localized perfuration of the sella floor 26 11.5
Diffuse perforation of the sella floor 67 29.4
Cystic component 48 21.1
Pituitary
123

Subgroup analysis
Nonfunctioning adenomas (see Table 2)
Nonfunctioning adenomas were the most common single
subgroup of pituitary adenomas operated in this series
(93 cases, 40.8%). All the tumors were macroadenomas;
the mean size of the lesions in this group was
30.4 ± 15.1 mm. These lesions presented cystic compo-
nents in 24 cases (25.8%). Visual complaints secondary to
optic chiasm compression were referred by 50 patients
(53.8%). In 70 cases (75.2%), gross total resection was
possible and no residual tumor or tumor regrowth was
observed during the follow up. In 23 patients complete
resection was not achieved during the first procedure: 13
had subtotal resection ([80%) and 10 partial resection
(\80%). In the subgroup of partial resection a second
endoscopic surgery was performed in all patients and total/
subtotal removal of the residual lesions was obtained in
eight cases (four subtotal resections and four total resec-
tions); the two remain patients were referred to radiother-
apy for treatment of important cavernous sinus invasion.
The 13 cases with subtotal resection are under clinical
observation and have not presented any symptoms during
the follow up.
Growth hormone-secreting adenomas (see Table 3)
Acromegaly was the most common hormone-secreting
pituitary adenoma subgroup in our series (58 cases,
25.4%). The micro- and macroadenomas corresponded to
11 (18.9%) and 47 (81%) cases, respectively. Cystic
lesions were observed only in six cases (10.3%). Hormonal
control was achieved in 9 microadenomas (81.8%) and 32
macroadenomas (68%) (total hormonal control rate: 41
patients, 70.7%).
Seventeen patients did not achieve hormonal control:
four macrodenomas were submitted to a second endoscopic
procedure and obtained disease control; and 13 patients
have been using somatostin analogues post-operatively.
Three cases (1.3% of all adenomas and 5.17% of acro-
megaly) of GH-prolactin co-secreting adenomas were
present in this group: hormonal control after surgery was
obtained in two of these and one patient was submitted to
medical treatment based on cabergoline and somatostatin
analogue once complete endocrinological control was not
achieved after the endoscopic resection.
Prolactinomas (see Table 4)
Endoscopic resection of prolactinomas was performed in
selected cases: cystic chiasmatic compressive lesions, no
hormonal control with use of medical therapy, important
medical therapy side effects or refusal to clinical treatment.
Macroadenomas were present in 34 patients (82.9%). About
15 cases (36.6%) presented as predominantly cystic ade-
nomas. We achieved an overall hormonal control in 35
patients (85.3%). All the microprolactinomas (seven
patients) presented hormonal control after surgery and 28
macroprolactinomas were controlled after resection
(82.3%). The six patients who did not achieve hormonal
control after endoscopic resection were submitted to clini-
cal therapy based on cabergoline. Recurrence was observed
in three cases of macroprolactinomas during the follow up.
Such cases were successfully submitted to cabergoline
based treatment, with no side effects observed. No patient
was submitted to radiotherapy for adjuvant treatment.
ACTH-secreting hormone (see Table 5)
Twenty-eight cases (12.2%) of Cushing Disease were
treated by endoscopic resection in our series. Most of those
Table 2 Nonfunctioning adenomas characteristics
Nonfunctioning adenomas 93
Mean size 30.4 ± 15.1 mm
Microadenomas 0
Macroadenomas 93 (100%)
Total resection 70 (75.2%)
Subtotal resection ([80%) 13 (13.9%)
Partial resection (\80%) 10 (10.7%)
Table 3 Growth hormone secreting adenomas characteristics
GH secreting adenomas 58
Mean size 20.8 ± 10.02 mm
Microadenomas 11 (18.9%)
Hormonal control 9 (81.8%)
Macroadenomas 47 (81.1%)
Hormonal control 32(68%)
Second surgery 4
Cure after the second procedure 4
Table 4 Prolactinomas characteristics
Prolactinomas 41
Mean size 20.2 ± 10.8 mm
Microadenomas 7 (17.1%)
Hormonal control 7 (100%)
Macroadenomas 34 (82.9%)
Hormonal control 28 (82.3%)
Pituitary
123
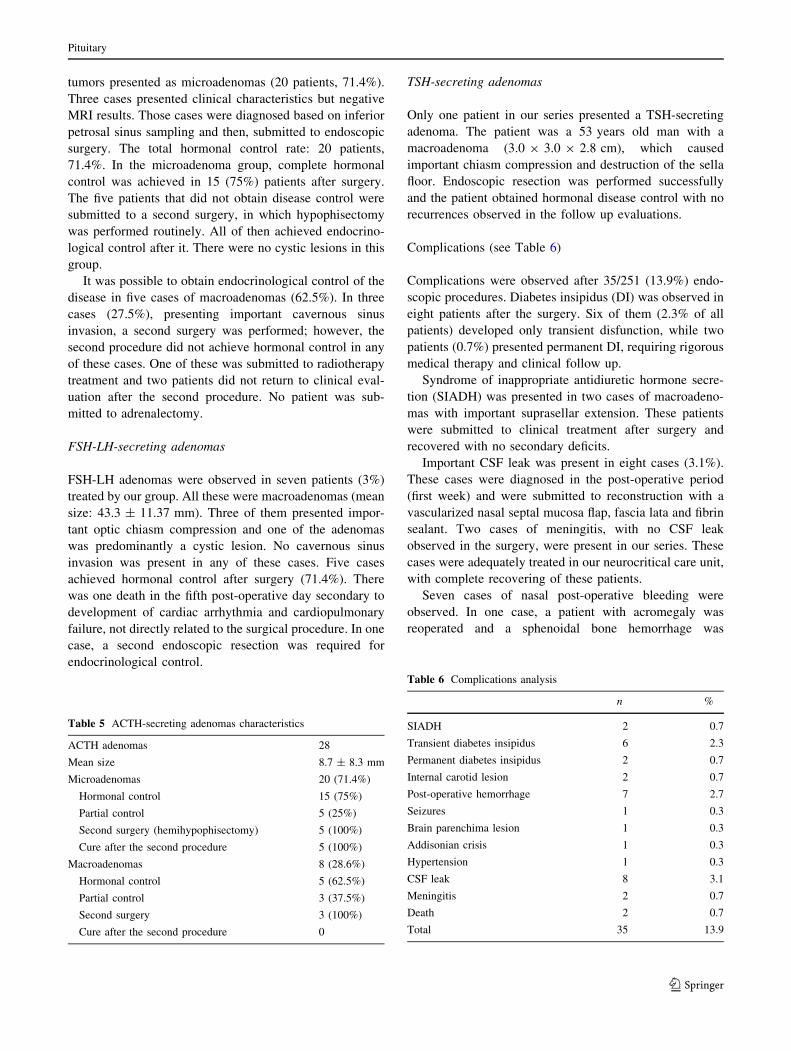
tumors presented as microadenomas (20 patients, 71.4%).
Three cases presented clinical characteristics but negative
MRI results. Those cases were diagnosed based on inferior
petrosal sinus sampling and then, submitted to endoscopic
surgery. The total hormonal control rate: 20 patients,
71.4%. In the microadenoma group, complete hormonal
control was achieved in 15 (75%) patients after surgery.
The five patients that did not obtain disease control were
submitted to a second surgery, in which hypophisectomy
was performed routinely. All of then achieved endocrino-
logical control after it. There were no cystic lesions in this
group.
It was possible to obtain endocrinological control of the
disease in five cases of macroadenomas (62.5%). In three
cases (27.5%), presenting important cavernous sinus
invasion, a second surgery was performed; however, the
second procedure did not achieve hormonal control in any
of these cases. One of these was submitted to radiotherapy
treatment and two patients did not return to clinical eval-
uation after the second procedure. No patient was sub-
mitted to adrenalectomy.
FSH-LH-secreting adenomas
FSH-LH adenomas were observed in seven patients (3%)
treated by our group. All these were macroadenomas (mean
size: 43.3 ± 11.37 mm). Three of them presented impor-
tant optic chiasm compression and one of the adenomas
was predominantly a cystic lesion. No cavernous sinus
invasion was present in any of these cases. Five cases
achieved hormonal control after surgery (71.4%). There
was one death in the fifth post-operative day secondary to
development of cardiac arrhythmia and cardiopulmonary
failure, not directly related to the surgical procedure. In one
case, a second endoscopic resection was required for
endocrinological control.
TSH-secreting adenomas
Only one patient in our series presented a TSH-secreting
adenoma. The patient was a 53 years old man with a
macroadenoma (3.0 9 3.0 9 2.8 cm), which caused
important chiasm compression and destruction of the sella
floor. Endoscopic resection was performed successfully
and the patient obtained hormonal disease control with no
recurrences observed in the follow up evaluations.
Complications (see Table 6)
Complications were observed after 35/251 (13.9%) endo-
scopic procedures. Diabetes insipidus (DI) was observed in
eight patients after the surgery. Six of them (2.3% of all
patients) developed only transient disfunction, while two
patients (0.7%) presented permanent DI, requiring rigorous
medical therapy and clinical follow up.
Syndrome of inappropriate antidiuretic hormone secre-
tion (SIADH) was presented in two cases of macroadeno-
mas with important suprasellar extension. These patients
were submitted to clinical treatment after surgery and
recovered with no secondary deficits.
Important CSF leak was present in eight cases (3.1%).
These cases were diagnosed in the post-operative period
(first week) and were submitted to reconstruction with a
vascularized nasal septal mucosa flap, fascia lata and fibrin
sealant. Two cases of meningitis, with no CSF leak
observed in the surgery, were present in our series. These
cases were adequately treated in our neurocritical care unit,
with complete recovering of these patients.
Seven cases of nasal post-operative bleeding were
observed. In one case, a patient with acromegaly was
reoperated and a sphenoidal bone hemorrhage was
Table 5 ACTH-secreting adenomas characteristics
ACTH adenomas 28
Mean size 8.7 ± 8.3 mm
Microadenomas 20 (71.4%)
Hormonal control 15 (75%)
Partial control 5 (25%)
Second surgery (hemihypophisectomy) 5 (100%)
Cure after the second procedure 5 (100%)
Macroadenomas 8 (28.6%)
Hormonal control 5 (62.5%)
Partial control 3 (37.5%)
Second surgery 3 (100%)
Cure after the second procedure 0
Table 6 Complications analysis
n %
SIADH 2 0.7
Transient diabetes insipidus 6 2.3
Permanent diabetes insipidus 2 0.7
Internal carotid lesion 2 0.7
Post-operative hemorrhage 7 2.7
Seizures 1 0.3
Brain parenchima lesion 1 0.3
Addisonian crisis 1 0.3
Hypertension 1 0.3
CSF leak 8 3.1
Meningitis 2 0.7
Death 2 0.7
Total 35 13.9
Pituitary
123

observed and then controlled. The other six cases presented
no important clinical manifestations.
Lesion of the internal carotid artery occurred in two
patients. Both happened during a reoperation for resection
of a lateral extension of macroadenomas with important
cavernous sinus invasion. In both cases, obstruction of the
vessel was performed by the interventional radiology team
of our center. One of the patients presented mild left
hemiparesis at the last follow up evaluation; the other one
did not return to the follow up evaluation.
Fatal outcome was present in two cases after surgery
(0.7%). One patient died at the fifth post-operative day
secondary to cardiac arrhythmia and cardiopulmonary
failure; in the second case, the patient developed pneu-
monia after surgery and died at the 20th post-operative
day. No death was directly related to the endoscopic
surgery.
Discussion
The development of the endonasal endoscopic approach to
the resection of pituitary adenomas has been one of the
most remarkable advances for the treatment of these
tumors in the last decades. Since 1997, after the initial
reports of large series of endoscopic pituitary surgery by
Jho and Carrau [15, 16] and Cappabianca et al. [17], the
technique has been disseminated worldwide and represents,
nowadays, the main surgical approach for sellar lesions in
different neurosurgical centers.
The endoscopic transsphenoidal approach can be per-
formed as a ‘‘pure’’ technique, with the endoscope as the
sole visualizing tool along the whole procedure, as pre-
sented in our series; or as an ‘‘endoscope-assisted’’ pro-
cedure, where the endoscope is used in association with the
microscope [16, 17, 20–23].
A panoramic vision inside the surgical area, a superior
close up of the anatomy and an improved working angle
represent some of the advantages brought by the use of the
endoscope to the pituitary surgery [24]. Nevertheless, less
nasal cavity injuries, without the use of nasal speculum or
fluoroscopy and patients fast recovering also are benefits
reported in the literature [21, 25, 26]. Comparing it to the
sub-labial incision, there is an important reduction in
morbidity, mainly related to the reduction of upper lip and
nasal complications [25, 27].
The results of the pure endoscopic pituitary surgery for
tumor resection and hormonal control of pituitary adeno-
mas have been extensively compared to the results
obtained by microsurgery [24, 28, 29]. However, no con-
clusive evidence of different results has been demonstrated
[24, 28, 29]. Until the moment, no large randomized study
has compared the results of these techniques.
In our series, most of the tumors were macroadenomas
(81%). The size of the lesions treated in our center (mean
tumor size, 24.6 ± 15.1 mm) is larger than the size of the
adenomas treated by other groups [28, 30]. We attribute the
occurrence of larger lesions in our study to the long dis-
tance between the reference center and the small towns in
the country and the important delay between development
of symptoms and admission in our neurosurgical depart-
ment. We believe this explain why our total resection
results (76.7%) are slightly inferior to the results presented
by Dehdashti et al. [24], that report levels of overall gross
total resection of 88%. Jain et al. [30] analyzed the relation
between the size of pituitary adenomas and outcome in a
series of 20 patients treated by the endonasal endoscopic
approach. They observed that tumor volume of less than
5 ml (P \ 0.05) and no parasellar or suprasellar extension
are favorable variables for total removal. Tabaee et al. [28]
submitted 57 patients to purely endoscopic pituitary sur-
gery obtaining gross tumor removal in 89% and hormonal
control in 90% of the cases. He observed that the only
significant predictor of the extent of tumor removal was
maximum tumor size. Larger tumors were associated with
visual dysfunctions (P = 0.02), longer procedures (P =
0.03) and duration of hospital stay (P = 0.0005) [28].
Nonfunctioning adenomas
The endoscopic surgical control of nonfunctioning adeno-
mas, based on gross total resection analysis, varies from 62
to 93% [21, 24, 26, 28, 29, 31, 32]. The large difference
between the results reported is partially secondary to the
learning curve required to master the procedure and to the
development of new endoscopic instruments. Therefore,
more access to tumors with extensions to the suprasellar
and parasellar regions is possible nowadays, what reduces
the percentage of subtotal resections.
The main limitation for gross total removal of non-
functioning adenomas was the presence of cavernous sinus
invasion. Twelve of the 23 patients (52.2%) who did not
experience total tumor resection after the first endoscopic
procedure in our series presented cavernous sinus invasion.
Two of them were referred to radiotherapy once presented
important nerve compression signs; the other ten patients
have been asymptomatic since surgery and are under
clinical follow up.
Although the nonfunctioning adenomas studied in this
series presented larger mean size (30.4 ± 15.1 mm) than
those presented by other groups [28, 30], we obtained
75.2% (70 cases) of disease control after the first endo-
scopic procedure, similarly to recent published reports
[29]. We attribute the difference between our results and
those presented by the endoscopic series of Dehdashti et al.
[24] (88% of gross total removal) and the results obtained
Pituitary
123

by the weighted average value of microscopic series cal-
culated in that paper (82% of gross total removal) to the
large size of the lesions presented in our study. Tumor size
has been demonstrated to be closely related to the extent of
resection obtained by the endoscopic pituitary surgery.
According to Tabaee et al. [28] there is a three folder
decrease in complete tumor removal for every 1 cm
increase in tumor size (P = 0.047).
Functioning adenomas
Acromegaly
Hormonal control results after the endoscopic resection of
GH-secreting adenomas varies from 65 to 85% in the lit-
erature [24, 28, 29, 31–33], presenting superior results
when compared to microsurgery series (52–85%) [24, 34–
36]. We obtained 70.1% of hormonal control after the first
endoscopic procedure and a level of 77.5% of control when
patients submitted to a second endoscopic procedure were
also analyzed. Previously, analyzing only intrasellar GH-
secreting tumors, our group reported a level of 84.84% of
disease control secondary to the endoscopic surgery [37].
Therefore, we believe that the suprasellar and parasellar
extension of the tumor represent the main cause of the
difference between these results.
Prolactinomas
Our disease control results (85%) are similar to the previ-
ously presented by other endoscopic series (64–100%) [24,
26, 28, 29, 31–33]. Gross total resection of prolactinomas
was not performed in six cases (15%) who presented
important parasellar extension. All cases in which hor-
monal control was not achieved after surgery were sub-
mitted to pharmacological therapy based on cabergoline/
bromocriptine. The superiority of endoscopic surgery for
hormonal control of prolactinomas has not been conclu-
sively demonstrated. In the literature, a wide range of
different results are presented for tumors operated by the
microsurgery technique (54–86%) [24, 32, 38–40]. A ran-
domized study comparing the results of the endoscopic
endonasal technique versus the sublabial microsurgical
approach demonstrated similar results in terms of prolac-
tinoma resection and hormonal control [26]. However,
endoscopic surgery was associated with fewer complica-
tions, shorter hospital stay and operative time [26].
ACTH-secreting tumors
In our 10 years of endoscopic experience, 28 cases of
Cushing Disease have been treated. After the first surgery,
20 patients (71.4%) achieved hormonal control. If the
results obtained after a second endoscopic procedure are
considered, 25 patients (89.2%) obtained disease control.
The results of hormonal control for ACTH-secreting ade-
nomas operated by endoscopic and microsurgery technique
varies from 67.8 to 86% [24, 28, 29, 31, 32] and from 70 to
86% [24, 41, 42], respectively. The largest series of
Cushing’s disease operated via the endoscopic technique
has been reported by Netea-Maier et al. [43]. In that study
the authors report remission of hypercortisolism in 77% of
the patients after the first pituitary operation and in 83% of
the patients after the first and the second pituitary operation
taken together. Similarly, to that group, we try to perform
the tumor resection preserving as much as possible the
normal parenchyma of the gland. In cases of patients pre-
senting negative MRI studies, hemihypophysectomy was
performed according to the results of the inferior petrosal
sinus sampling. Hypophysectomy was only performed in
cases of relapsing microadenomas in which the tumor was
not identified intraoperatively.
FSH-LH-secreting adenomas
We treated seven patients with FSH-LH-secreting adeno-
mas, and achieved hormonal control after the first procedure
in 71.4%. Considering the second procedure, the hormonal
control was 85.7%. All cases were macroadenomas.
TSH-secreting adenomas
Because of the rarity of such adenoma, our experience in
TSH-secreting adenomas is limited to just on case. Although
treated with success, we can not take any conclusion.
Complication analysis
As in other endoscopic series, the nasal complications are
reduced, mainly because the endoscopic approach skips the
nasal phase and the surgery really begins in the sphenoidal
ostium. Nasal complications in our series were resumed to
seven patients (2.7%) who presented epistaxis after surgery.
Such complication has been reported to occur in 0.7–1.7% of
the patients treated by this technique [24, 29, 31, 44, 45].
Permanent DI was observed in 0.7%, an inferior rate
than that observed in the literature (1.0–3.42%) [24, 29, 31,
44, 45]. Transient DI and SIADH were observed in 2.3 and
0.7% of the patients, respectively. All patients presented
good outcome after intensive care management.
CSF leak is one of the most important complications of
pituitary surgery. It was present in 3.1% of the patients in
our 150 first cases of this series. In the last 78 cases we
have no CSF leak. The variation of endoscopic surgery
series is: 1.2–6% [24, 29, 31, 44, 45], and the microsurgery
Pituitary
123

series reports: 0.9–3% [7, 46, 47]. The absence of CSF leak
in the last 78 cases is do to a vascularized nasal septal
mucosa flap as a final layer over the onlay graft, followed
by Foley catheter as a buttress that is removed in 48 h [18].
No case of CSF leak was associated with the development
of meningitis. Two cases of meningitis were observed
(0.7%), comparable to results previously published (0.4–
1.2%) [24, 29, 31, 44, 45].
Lesions of the internal carotid artery is reported in the
literature in 0–0.68% of patients treated by the endoscopic
approach. In our series we observed two cases (0.7%). The
two cases were reoperation and happened at the beginning of
the series when we did not use neuronavigation. After this, all
reoperations are done with this method [24, 29, 31, 44, 45].
Other frequent complications mentioned in literature [24,
29, 31, 44, 45], as sinusistis, mucocele, septum perforation,
ischemia, hematoma, vision deterioration, ophtalmoplegia
and intracerebral hemorrhage, were not observed in our series.
In this series, a total of 35 patients (13.9%) developed
complications, a result comparable to the literature data:
10–26.3% [24, 29, 31, 44, 45]. Our mortality rate was 0.7%
and in the literature it varies from 0 to 0.68% [24, 29, 31,
44, 45]. The microscopic endonasal approach present 37.6–
47% of complications and 0–0.6% of mortality; and the
microscopic transnasal approach presents 8.2–11% of
complication and 0.3–0.9% of mortality [7, 46, 47]. We
present a mortality rate slightly higher than other series.
However, none of the deaths was directly secondary to the
surgical procedure.
Endoscopy limitations
The endoscopic approach presents some particular limita-
tions, such as a narrow channel to the sella, necessity of
special instrumentation, different kind of view what
requires different skills, and some experience of the sur-
geon with the use of the endoscope [48]. Another potential
disadvantage is related to the difficult management of
bleeding complications during the procedure.
The loss of the three-dimensional vision in the endo-
scopic surgery has been advocated as one of the most
important disadvantages of the technique As Cappabianca
et al. [49] we do not consider the endoscopic bidimensional
vision lacking in depth of field. It is undeniable that there is
a remarkable difference when compared to the microscopic
view, but we believe the surgeon can perfectly overcome it
based on the knowledge of anatomic landmarks and with
movements of the endoscope.
Limitations of the study
Our study presents some limitations: it is a retrospective
experience, the data are largely descriptive and it is a
non-randomized, single institutional study design. There
was no direct comparison between the traditional micro-
scopic and endoscopic procedures. We have no data to
demonstrate that endoscopy provides a measurable differ-
ence in outcome as compared to the microsurgical trans-
sphenoidal technique, and therefore, it is not possible to
definitively prove the superiority of endoscopic visualiza-
tion. Another limitation is the short follow up period of
some patients in our series, considering that recurrence of
functioning adenoma may occur after many years.
Conclusion
Nowadays there is a tendency in favor of minimally
invasive technique as the pure endoscopic approach,
because of faster recovery of patient and less complication
and hospitalization time. An important aspect is the expe-
rience of the surgeon with the method. Use of the endo-
scope for sellar lesions is safe and effective, and it is clear
that the endoscope provides important intraoperative data
that are not obtainable with the tunnel vision of the
microscope. Gross total resection of large lesions may be
adequately achieved by the technique, without higher rates
of complications.
Although presenting important advantages, endoscopy
has not been proved to be superior to microsurgery. We
believe larger, randomized, studies are required for analy-
sis of the definitive role of endoscopy in the treatment of
pituitary adenomas.
References
1. Schloffer H (1906) Zur frage der Operationen an der Hypophyse.
Beitr Klin Chir 50:767–817
2. Hirsch O (1910) Endonasal method of removal of hypophyseal
tumors. With a report of two successful cases. JAMA 55:772–774
3. Halstead AE (1910) Remarks on the operative treatment of
tumors of the hypophysis. With the report of two cases operated
on by an oro-nasal method. Surg Gynecol Obstet 10:494–502
4. Rosegay H (1981) Cushing’s legacy to transsphenoidal surgery.
J Neurosurg 54:448–454
5. Cushing H (1912) The Pituitary Body and Its Disorders: Clinical
States Produced by Disorders of the Hypophysis Cerebri. JB
Lippincott, Philadelphia, pp 296–305
6. Cushing H (1914) The Weir Mitchell Lecture. Surgical experi-
ences with pituitary disorders. JAMA 63:1515–1525
7. Zada G, Kelly DF, Cohan P, Wang C, Swerdloff R (2003) En-
donasal transsphenoidal approach for pituitary adenomas and
other sellar lesions: an assessment of efficacy, safety, and patient
impressions. J Neurosurg 98:350–358
8. Liu JK, Das K, Weiss MH, Laws ER Jr, Couldwell WT (2001)
The history and evolution of transsphenoidal surgery. J Neuro-
surg 95:1083–1096
9. Hardy J (1969) Transsphenoidal microsurgery of the normal and
pathological pituitary. Clin Neurosurg 16:185–217
Pituitary
123
10. Guiot G (1973) Transsphenoidal approach in surgical treatment
of pituitary adenomas. General principles and indications in
nonfunctioning adenomas. In: Kolher PO, Ross GT (eds) Diag-
nosis and treatment of pituitary tumors, vol 303. Excepta Medica
Congress Series, Amsterdam, pp 159–178
11. Messerklinger W (1970) Endoscopy of the nose. Monatsschr
Ohrenheilkd Laryngorhinol 104:451–456
12. Kennedy DW, Cohn ES, Papel ID, Holliday MJ (1984) Trans-
sphenoidal approach to the sella the Johns Hopkins experience.
Laryngoscope 94:1066–1074. doi:10.1288/00005537-198408000-
00015
13. Draf W (1991) Endonasal micro-endoscopic frontal sinus surgery
the Fulda concept. Operative Tech Otolaryngol Head Neck Surg
2:234–240
14. Jankovsky R, Auque J, Simon CMJC, Hepner H, Wayoff M
(1992) Endoscopic pituitary surgery. Laryngoscope 102:198–202
15. Jho H, Carrau R (1996) Endoscopy assisted transsphenoidal
surgery for pituitary adenoma. Acta Neurochir (Wien) 138:1416–
1425. doi:10.1007/BF01411120
16. Jho H, Carrau R (1997) Endoscopic endonasal transsphenoidal
surgery: experience with fifty patients. J Neurosurg 87:44–51
17. Cappabianca P, Alfieri A, de Divitiis E (1998) Endoscopic en-
donasal transsphenoidal approach to the sella: towards functional
endoscopic pituitary surgery (FEPS). Minim Invasive Neurosurg
41:66–73. doi:10.1055/s-2008-1052019
18. Hadad G, Bassagasteguy L, Carrau RL, Mataza JC, Kassam A,
Snyderman CH et al (2006) A novel reconstructive technique
following endoscopic expanded endonasal approaches: vascular
pedicle nasoseptal flap. Laryngoscope 116:1881–1885. doi:
10.1097/01.mlg.0000234933.37779.e4
19. Melmed S, Casanueva F, Cavagnini F, Chanson P, Frohman LA,
Gaillard R, Ghigo E, Ho K, Jaquet P, Kleinberg D, Lamberts S,
Laws E, Lombardi G, Sheppard MC, Thorner M, Vance ML,
Wass JA, Giustina A (2005) Consensus statement: medical
management of acromegaly. Eur J Endocrinol 153:737–740. doi:
10.1530/eje.1.02036
20. Jho HD, Carrau RL, Ko Y, Daly MA (1997) Endoscopic pituitary
surgery: an early experience. Surg Neurol 7:213–223. doi:
10.1016/S0090-3019(96)00452-1
21. Cappabianca P, Cavallo LM, de Divitiis E (2004) Endoscopic
endonasal transsphenoidal surgery. Neurosurgery 55:933–940.
doi:10.1227/01.NEU.0000137330.02549.0D
22. Perneczky A, Fries G (1998) Endoscope-assisted brain surgery:
part 1—evolution, basic concept, and current technique. Neu-
rosurgery 42:219–224. doi:10.1097/00006123-199802000-00001
23. Fries G, Perneczky A (1998) Endoscope-assisted brain surgery:
part 2—analysis of 380 procedures. Neurosurgery 42:226–231;
discussion 231–232. doi:10.1097/00006123-199802000-00008
24. Dehdashti AR, Ganna A, Karabatsou K, Gentili F (2008) Pure
endoscopic endonasal approach for pituitary adenomas: early
surgical results in 200 patients and comparison with previous
microsurgical series. Neurosurgery 62:1006–1017. doi:10.1227/
01.neu.0000325862.83961.12
25. Koren I, Hadar T, Rappaport ZH, Yaniv E (1999) Endoscopic
transnasal transsphenoidal microsurgery versus the sublabial
approach for the treatment of pituitary tumors: endonasal com-
plications. Laryngoscope 109:1838–1840
26. Cho D-Y, Liau W-R (2002) Comparison of endonasal endoscopic
surgery and sublabial microsurgery for prolactinomas. Surg
Neurol 58:371–376. doi:10.1016/S0090-3019(02)00892-3
27. Sheehan MT, Atkinson JLD, Kasperbauer JL, Erickson BJ,
Nippoldt TB (1999) Preliminary comparison of the endoscopic
transnasal versus the sublabial transseptal approach for clinically
nonfunctioning pituitary macroadenomas. Mayo Clin Proc
74:661–670. doi:10.4065/74.7.661
28. Tabaee A, Anand VK, Barron Y, Hiltzik DH, Brown SM, Kacker
A, Mazumdar M, Schwartz TH (2008) Predictors of short-term
outcomes following endoscopic pituitary surgery. Clin Neurol
Neurosurg 2:119–122
29. Frank G, Pasquini E, Farneti G, Mazzatenta D, Sciarretta V,
Grasso V, Faustini Fustini M (2006) The endoscopic versus the
traditional approach in pituitary surgery. Neuroendocrinology
83:240–248. doi:10.1159/000095534
30. Jain AK, Gupta AK, Pathak A, Bhansali A, Bapuraj JR (2008)
Endonasal transsphenoidal pituitary surgery: is tumor volume a
key factor in determining outcome? Am J Otolaryngol 29(1):48–
50. doi:10.1016/j.amjoto.2007.01.006
31. Jho HD (2001) Endoscopic transsphenoidal surgery. J Neuroon-
col 54:187–195. doi:10.1023/A:1012969719503
32. Kabil MS, Eby JB, Shahinian HK (2005) Fully endoscopic endo-
nasal versus transseptal transsphenoidal pituitary surgery. Minim
Invasive Neurosurg 48:348–354. doi:10.1055/s-2005-915635
33. Shen CC, Wang YC, Hua WS, Chang CS, Sun MH (2000)
Endoscopic endonasal transsphenoidal surgery for pituitary
tumors. Chin Med J Taipei 63:301–310
34. Davis DH, Laws ER Jr, Ilstrup DM, Speed JK, Caruso M, Shaw
EG, Abboud CF, Scheithauer BW, Root LM, Schleck C (1993)
Results of surgical treatment for growth hormone-secreting
pituitary adenomas. J Neurosurg 79:70–75
35. Freda PU, Wardlaw SL, Post KD (1998) Long-term endocrino-
logical follow-up evaluation in 115 patients who underwent
transsphenoidal surgery for acromegaly. J Neurosurg 89:353–358
36. Sheaves R, Jenkins P, Blackburn P, Huneidi AH, Afshar F,
Medbak S, Grossman AB, Besser GM, Wass JA (1996) Outcome
of transsphenoidal surgery for acromegaly using strict criteria for
surgical cure. Clin Endocrinol (Oxf) 45:407–413. doi:10.1046/
j.1365-2265.1996.8370847.x
37. Gondim JA, Ferraz T, Mota I, Studart D, Almeida JP, Gomes E,
Schops M (2009) Outcome of surgical intrasellar growth hor-
mone tumor performed by a pituitary specialist surgeon in a
developing country. Surg Neurol 72:15–29; discussion 19
38. Charpentier G, de Plunkett T, Jedynak P, Peillon F, Le Gentil P,
Racadot J, Visot A, Derome P (1985) Surgical treatment of
prolactinomas. Short- and long-term results, prognostic factors.
Horm Res 22:222–227. doi:10.1159/000180098
39. Derome P (1985) Surgical treatment of prolactinomas. Short and
long-term results, prognostic factors. Horm Res 22:222–227. doi:
10.1159/000180098
40. Scanlon MF, Peters JR, Thomas JP, Richards SH, Morton WH,
Howell S et al (1985) Management of selected patients with
hyperprolactinaemia by partial hypophysectomy. Br Med J (Clin
Res Ed) 291:1547–1550
41. Fahlbusch R, Buchfelder M, Muller OA (1986) Transsphenoidal
surgery for Cushing’s disease. J R Soc Med 79:262–269
42. Hammer GD, Tyrrell JB, Lamborn KR, Applebury CB, Hanne-
gan ET, Bell S, Rahl R, Lu A, Wilson CB (2004) Transsphenoidal
microsurgery for Cushing’s disease: initial outcome and long-
term results. J Clin Endocrinol Metab 89:6348–6357. doi:
10.1210/jc.2003-032180
43. Netea-Maier RT, van Lindert EJ, den Heijer M, van der Eerden
A, Pieters GF, Sweep CG, Grotenhuis JA, Hermus AR (2006)
Transsphenoidal pituitary surgery via the endoscopic technique:
results in 35 consecutive patients with Cushing’s disease. Eur J
Endocrinol 154:675–684. doi:10.1530/eje.1.02133
44. Cappabianca P, Cavallo LM, Colao A, de Divitiis E (2006)
Surgical complications associated with the endoscopic endonasal
transsphenoidal approach for pituitary adenomas. J Neurosurg
97:293–298
45. de Divitiis E, Cappabianca P, Cavallo M (2003) Endoscopic
endonasal transsphenoidal approach to the sellar region. In: de
Pituitary
123
Divitiis E, Cappabianca P (eds) Endoscopic Endonasal Trans-
sphenoidal Surgery. Springer, Wien, pp 91–130
46. Ciric I, Ragin A, Baumgartner C, Pierce DB (1997) Complica-
tions of transsphenoidal surgery: results of a national survey,
review of the literature and personal experience. Neurosurgery
40:225–237. doi:10.1097/00006123-199702000-00001
47. Semple PL, Laws ER Jr (1999) Complications in a contemporary
series of patients who underwent transsphenoidal surgery for
Cushing’s disease. J Neurosurg 91:175–179
48. Gondim J, Schops M, Tella OI Jr (2003) Transnasal endoscopic
surgery of the sellar region: study of the first 100 cases. Arq
Neuropsiquiatr 61:836–841. doi:10.1590/S0004-282X20030005
00024
49. Cappabianca P, Divitiis E (2004) Endoscopy and transsphenoidal
surgery. Neurosurgery 54:1043–1050. doi:10.1227/01.NEU.000
0119325.14116.9C
Pituitary
123
Related Documents











