End Stage Renal Disease and End Stage Renal Disease and Renal Replacement Therapies Renal Replacement Therapies Alexander J. Alexander J. Ansara Ansara , Pharm. D. , Pharm. D. St. Louis College of Pharmacy St. Louis College of Pharmacy and St. Luke’s Hospital and St. Luke’s Hospital Therapeutics 1 Therapeutics 1 Fall 2003 Fall 2003 Reading Materials Reading Materials Required Required – Dipiro Dipiro Chapter 47, pp. 867 Chapter 47, pp. 867- 887 887 – Ifudu Ifudu O. Care of Patients Undergoing O. Care of Patients Undergoing Hemodialysis Hemodialysis . N . N Engl Engl J Med 1998; 339: 1054 J Med 1998; 339: 1054- 1062. 1062. Supplemental Supplemental – Pastan Pastan S, Bailey J. Dialysis Therapy. S, Bailey J. Dialysis Therapy. N N Engl Engl J Med 1998; J Med 1998; 338:1428-1437.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
End Stage Renal Disease and End Stage Renal Disease and Renal Replacement TherapiesRenal Replacement Therapies
Alexander J. Alexander J. AnsaraAnsara, Pharm. D., Pharm. D.St. Louis College of Pharmacy St. Louis College of Pharmacy
and St. Luke’s Hospitaland St. Luke’s HospitalTherapeutics 1 Therapeutics 1
Fall 2003Fall 2003
Reading MaterialsReading Materials
RequiredRequired–– DipiroDipiro Chapter 47, pp. 867Chapter 47, pp. 867--887887–– Ifudu Ifudu O. Care of Patients Undergoing O. Care of Patients Undergoing
HemodialysisHemodialysis. N . N Engl Engl J Med 1998; 339: 1054J Med 1998; 339: 1054--1062.1062.
SupplementalSupplemental–– PastanPastan S, Bailey J. Dialysis Therapy. S, Bailey J. Dialysis Therapy.
N N Engl Engl J Med 1998; J Med 1998; 338:1428-1437.

2
EpidemiologyEpidemiologyOverall incidence ESRD: 240/million ptsOverall incidence ESRD: 240/million pts–– 180/million180/million caucasiancaucasian patientspatients–– 758/million758/million african americanafrican american patientspatients
US population with ESRD:US population with ESRD:–– > 200,000 pts on any dialysis> 200,000 pts on any dialysis–– ≈≈ 20,000 pts on peritoneal dialysis20,000 pts on peritoneal dialysis–– > 70,000 pts with functioning transplants> 70,000 pts with functioning transplants
PrevalencePrevalence–– Increasing at 7Increasing at 7--9% per year9% per year–– Estimated 600,000 dialysis patients by 2010Estimated 600,000 dialysis patients by 2010–– # transplants # transplants remainining remainining stablestable
Increasing PrevalenceIncreasing Prevalence

3
Mortality and Life ExpectancyMortality and Life Expectancy
Importance of PreventionImportance of Prevention
PreventionPrevention–– Cardiac deaths #1 causeCardiac deaths #1 cause–– Peritonitis #2 causePeritonitis #2 cause–– Limited availability of transplantsLimited availability of transplants–– CostCostCostCost–– Avg Avg cost/pt/yr cost/pt/yr ≈≈ $45,000$45,000–– US expenditure/yr: US expenditure/yr: ≈≈ $15 billion$15 billion–– Estimated cost by 2010: Estimated cost by 2010: ≈≈ $28 billion$28 billion

4
Treating ESRDTreating ESRDPreventionPreventionTreat concurrent Treat concurrent diseasesdiseases–– HTNHTN–– DiabetesDiabetes
DialysisDialysis–– HemodialysisHemodialysis (HD)(HD)–– Peritoneal Dialysis Peritoneal Dialysis
(PD)(PD)Renal transplantationRenal transplantation
Renal Replacement Therapy:Renal Replacement Therapy:Replacing Kidney Functions Replacing Kidney Functions
HH220 balance0 balanceElectrolyte balanceElectrolyte balanceAcid/Base balanceAcid/Base balance
Waste Removal (urea, Waste Removal (urea, creatininecreatinine))Filter, reabsorb, secrete substancesFilter, reabsorb, secrete substances–– Plasma proteins, HPlasma proteins, H220, blood cells, amino 0, blood cells, amino
acids, glucose, urea, mineral saltsacids, glucose, urea, mineral saltsEndocrine functionsEndocrine functions–– Vitamin D activationVitamin D activation
–– Erythropoietin productionErythropoietin production

5
The Vowels of Renal The Vowels of Renal Replacement TherapyReplacement Therapy
BUN accumulationBUN accumulationUUremiaremia
PostPost--op fluid gain, op fluid gain, excessive IV fluidsexcessive IV fluids
Fluid Fluid OOverloadverload
SalicylatesSalicylates, Li++, , Li++, MethMeth--anolanol, Ethylene Glycol, Ethylene Glycol
IIntoxicationntoxication
HyperkalemiaHyperkalemia//magnesemiamagnesemia
EElectrolyte Disturbancelectrolyte Disturbance
Metabolic acidosisMetabolic acidosisAAcid Base Abnormalitycid Base Abnormality
SETTINGSETTINGINDICATIONINDICATION
Principles of Principles of HemodialysisHemodialysisHemodialysisHemodialysis:: The removal of nitrogenous The removal of nitrogenous wastes, wastes, uremic uremic toxins, and water from the blood toxins, and water from the blood via diffusion and convectionvia diffusion and convection
Diffusion:Diffusion: The process of solute transfer from The process of solute transfer from high concentration to low concentration until high concentration to low concentration until equillibriumequillibrium
Convection (“Convection (“ultrafiltrationultrafiltration”):”): Primary means of Primary means of removal of excess body Hremoval of excess body H220, maximized by:0, maximized by:–– ↑↑ hydrostatic pressure hydrostatic pressure –– ↑↑ permeability of membranepermeability of membrane

6
Factors Affecting Diffusion RateFactors Affecting Diffusion Rate
Concentration gradientConcentration gradientBlood flow rateBlood flow rate
Dialysis flow rateDialysis flow rateDialysis filter compositionDialysis filter composition
Solute characteristicsSolute characteristics
Principles of Principles of HemodialysisHemodialysisHemodialysisHemodialysis:: The removal of nitrogenous The removal of nitrogenous wastes, wastes, uremic uremic toxins, and water from the blood toxins, and water from the blood via diffusion and convectionvia diffusion and convection
Diffusion:Diffusion: The process of solute transfer from The process of solute transfer from high concentration to low concentration until high concentration to low concentration until equillibriumequillibrium
Convection (“Convection (“ultrafiltrationultrafiltration”):”): Primary means of Primary means of removal of excess body Hremoval of excess body H220, maximized by:0, maximized by:–– ↑↑ hydrostatic pressure hydrostatic pressure –– ↑↑ permeability of membranepermeability of membrane

7
ConvectionConvection
Low volume filtration:Low volume filtration:–– No significant clearance of toxins or drugsNo significant clearance of toxins or drugs–– Performed to maintain fluid balancePerformed to maintain fluid balance–– UltrafiltrationUltrafiltration rate (UFR) < 200rate (UFR) < 200--400 400 mLmL/hr/hrLarge volume filtration:Large volume filtration:–– Significant clearance of urea and drugsSignificant clearance of urea and drugs–– Must replace fluid loss to avoid major Must replace fluid loss to avoid major
electrolyte disturbanceselectrolyte disturbances–– UFR 1UFR 1--2 L/hr2 L/hr
Vascular AccessVascular Access
Permanent access to bloodstream necessaryPermanent access to bloodstream necessary
Native Native arteriovenous arteriovenous (AV) fistula(AV) fistula
Synthetic AV vascular graftsSynthetic AV vascular grafts

8
Native AV FistulaNative AV Fistula
Fistula between cephalic vein and radial Fistula between cephalic vein and radial arteryartery2 months to “mature” before use2 months to “mature” before useLow rate of complicationsLow rate of complicationsLongest survival (of access)Longest survival (of access)Used less frequentlyUsed less frequently
Native AV FistulaNative AV Fistula

9
Native AV FistulaNative AV Fistula
Fistula between cephalic vein and radial Fistula between cephalic vein and radial arteryartery2 months to “mature” before use2 months to “mature” before useLow rate of complicationsLow rate of complicationsLongest survival (of access)Longest survival (of access)Used less frequentlyUsed less frequently
Synthetic AV Vascular GraftsSynthetic AV Vascular Grafts
Synthetic graft between brachial artery Synthetic graft between brachial artery and and basilic basilic veinveinMade of Made of polytetrafluoroethylene polytetrafluoroethylene (PTFE), (PTFE), requires 2requires 2--3 weeks to 3 weeks to endothelializeendothelializeHigher rates of infection and thrombosisHigher rates of infection and thrombosisShorter device survivalShorter device survivalMost commonly usedMost commonly used

10
Synthetic AV Vascular GraftsSynthetic AV Vascular Grafts
Synthetic AV Vascular GraftsSynthetic AV Vascular Grafts
Synthetic graft between brachial artery Synthetic graft between brachial artery and and basilic basilic veinveinMade of Made of polytetrafluoroethylene polytetrafluoroethylene (PTFE), (PTFE), requires 2requires 2--3 weeks to 3 weeks to endothelializeendothelializeHigher rates of infection and thrombosisHigher rates of infection and thrombosisShorter device survivalShorter device survivalMost commonly usedMost commonly used
FistulaFistula

11
Choosing a Route of AccessChoosing a Route of Access
Immediacy of need for dialysisImmediacy of need for dialysis–– Acute dialysis, may use central line; used for Acute dialysis, may use central line; used for
months as bridge for permanent accessmonths as bridge for permanent accessAdequacy of vascular accessAdequacy of vascular accessComplicationsComplications–– InfectionInfection–– ThrombosisThrombosis–– StenosisStenosis
2020--40% of hospitalizations40% of hospitalizations
HemodialysisHemodialysis
Blood pumped to Blood pumped to dialyzerdialyzerBlood and electrolyte solution (Blood and electrolyte solution (dialysatedialysate):):–– Seperated Seperated by semiby semi--permeable membranepermeable membrane–– Pumped in countercurrent directionsPumped in countercurrent directions–– Solutes exchanged until Solutes exchanged until equilibruimequilibruimProtein bound drugs not removedProtein bound drugs not removedLow permeability membrane (low to Low permeability membrane (low to medium flux)medium flux)
HDHD

12
Goals of DialysisGoals of Dialysis
–– Achieve desired dry weightAchieve desired dry weight
–– Adequate removal of waste productsAdequate removal of waste products
–– Prevent Prevent sequelae sequelae of electrolyte disturbancesof electrolyte disturbances
–– Reduce morbidity and mortalityReduce morbidity and mortality

13
The The Hemodialysis Hemodialysis “Rx”“Rx”
Dialyzer Dialyzer manufacturer and sizemanufacturer and sizeAmount of weight/fluid to removeAmount of weight/fluid to removeDurationDurationFrequencyFrequencyBlood flow rate: 200Blood flow rate: 200--350mL/min350mL/minDialysateDialysate–– CompositionComposition–– Flow rate: Flow rate: ≈≈ 500 500 mLmL/min/min
Hemodialysate Hemodialysate CompositionComposition
00--0.2 0.2 0.20.2Glucose (g/Glucose (g/dLdL))2525--40 40 3535BicarbonateBicarbonate8787--120 105120 105ChlorideChloride00--0.75 0.250.75 0.25MagnesiumMagnesium00--2.0 2.0 1.251.25CalciumCalcium00--4.0 2.04.0 2.0PotassiumPotassium
135135--155 140 155 140 SodiumSodium
HemodialysateHemodialysateRange TypicalRange Typical
Component Component ((mmolmmol/L)/L)

14
The The Hemodialysis Hemodialysis “Rx”“Rx”
Dialyzer Dialyzer manufacturer and sizemanufacturer and sizeAmount of weight/fluid to removeAmount of weight/fluid to removeDurationDurationFrequencyFrequencyBlood flow rate: 200Blood flow rate: 200--350mL/min350mL/minDialysateDialysate–– CompositionComposition–– Flow rate: Flow rate: ≈≈ 500 500 mLmL/min/min
Hemodialysis Hemodialysis Flow RatesFlow Rates
< 3 hrs< 3 hrs< 3 hrs< 3 hrs44--5 hrs5 hrsRequired TimeRequired Time
> 220 > 220 > 220 > 220 < 200< 200Urea clearance Urea clearance rate (rate (mLmL/min)/min)
500500--1000 1000 700700--1000 1000 400400--500 500 Dialysate Dialysate flow flow rate (rate (mLmL/min)/min)
400400--500 500 300300--600 600 200200--350 350 Blood flow rate Blood flow rate ((mLmL/min)/min)
High flux High flux dialysisdialysis
RapidRapid--high high efficiencyefficiency
ConventionalConventional

15
“Dosing” Dialysis“Dosing” Dialysis
Individualized per patientIndividualized per patientSurvival improves with higher dosesSurvival improves with higher doses
Expressed as:Expressed as:–– UreaUrea--reduction ratio (URR) reduction ratio (URR)
or or –– Kt/Kt/VVureaurea
Urea Reduction RatioUrea Reduction Ratio
Not 100% accurateNot 100% accurate–– Does not account for convective removal of Does not account for convective removal of
ureaurea–– Urea demonstrates twoUrea demonstrates two--compartment compartment
behavior (redistributes after dialysis)behavior (redistributes after dialysis)
URR = URR = (pre(pre--dialysis BUN) dialysis BUN) –– (post(post--dialysis BUN)dialysis BUN)prepre--dialysis BUNdialysis BUN

16
Kt/Kt/VVureaurea
Unitless Unitless parameterparameterMeasures fraction of total body water cleared of Measures fraction of total body water cleared of urea during a dialysis sessionurea during a dialysis session
Kt/Kt/VVurea urea = = (urea clearance)(time)(urea clearance)(time)urea distribution volumeurea distribution volume
K=K= dialyzerdialyzer clearance of urea (L/h)clearance of urea (L/h)t = duration of dialysis (h)t = duration of dialysis (h)V= urea volume of distribution (calculated)V= urea volume of distribution (calculated)
Goal Kt/Goal Kt/VVureaurea ValuesValues
HD (nonHD (non--diabetic) = 1.2diabetic) = 1.2HD (diabetic) = 1.4 HD (diabetic) = 1.4 –– 1.51.5HighHigh--flux dialysis (HFD) = 1.5flux dialysis (HFD) = 1.5CAPD = 1.7/weekCAPD = 1.7/weekNIPD and APD = 2.2/weekNIPD and APD = 2.2/weekAcute renal failure = much higherAcute renal failure = much higher

17
Complications of Complications of HemodialysisHemodialysisFewer with highFewer with high--flux dialysisflux dialysisLess hypotension with bicarbonate in Less hypotension with bicarbonate in dialysatedialysate
ItchingItchingHypotensionHypotensionCrampsCrampsNausea/vomitingNausea/vomitingHeadacheHeadacheDisequillibriumDisequillibrium syndromesyndromeDialyzerDialyzer reactionsreactions–– Anaphylactic (Type A)Anaphylactic (Type A)–– Nonspecific (Type B)Nonspecific (Type B)
Complications of Complications of HemodialysisHemodialysis
Idiopathic, Idiopathic, vasodilation vasodilation 2/2 2/2 acetate, caffeine withdrawalacetate, caffeine withdrawal
55HeadacheHeadache
Hypotension, disequilibrium Hypotension, disequilibrium syndromesyndrome
55--1515Nausea/Nausea/VomitingVomiting
Hypotension, dehydration, low Hypotension, dehydration, low NaNa++ in in dialysatedialysate, idiopathic, idiopathic
22--5050CrampsCramps
Excessive UF, low target wt, Excessive UF, low target wt, vasodilation vasodilation 2/2 acetate, meds or 2/2 acetate, meds or food, bleedingfood, bleeding
1515--5050HypotensionHypotension
Uremic Uremic toxins, dry skin, toxins, dry skin, ↑↑Ca/POCa/PO44product, allergyproduct, allergy
5050--9090ItchingItching
Etiology/Risk FactorsEtiology/Risk FactorsIncidence Incidence (%)(%)
ComplicationComplication

18
Dialyzer Dialyzer ReactionsReactions
AnaphylacticAnaphylactic–– Type AType A–– Response to ethylene oxide or heparinResponse to ethylene oxide or heparin–– Worse with pts on Worse with pts on ACEIsACEIsNonspecific Nonspecific –– Type BType B–– More common, less severeMore common, less severe–– Chest pain, back pain within minutes of dialysisChest pain, back pain within minutes of dialysis–– Lowest incidence with synthetic highLowest incidence with synthetic high--fluxflux
membrancesmembrances
Disequilibrium SyndromeDisequilibrium SyndromeDefinition:Definition: A central nervous system disorder A central nervous system disorder characterized by characterized by neurologic neurologic symptoms caused symptoms caused by cerebral edemaby cerebral edemaSxSx:: Nausea, vomiting, headache, seizures, Nausea, vomiting, headache, seizures, obtundationobtundation, coma; EEG changes, coma; EEG changesRisk Factors:Risk Factors: new dialysis patients, age (old or new dialysis patients, age (old or young), preyoung), pre--existing neurological disorders, existing neurological disorders, metabolic acidosismetabolic acidosisTreatment:Treatment: prevention, use of UF, reducing prevention, use of UF, reducing URR, maintaining NaURR, maintaining Na++ and glucose levels inand glucose levels indialysatedialysate
19
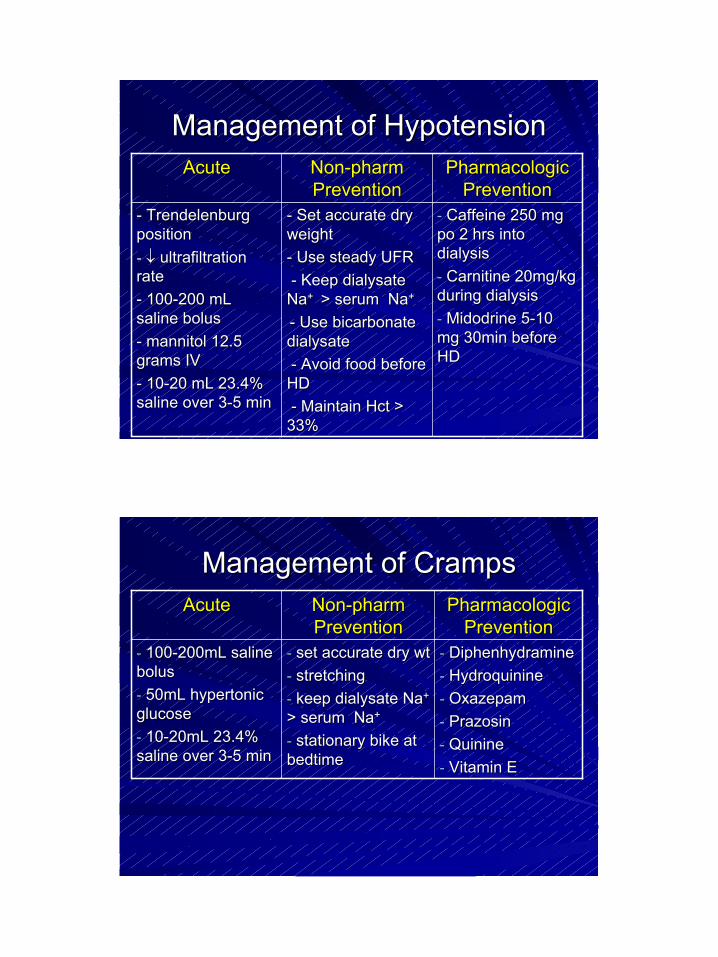
Management of HypotensionManagement of Hypotension
-- Caffeine 250 mg Caffeine 250 mg po po 2 hrs into 2 hrs into dialysisdialysis-- Carnitine Carnitine 20mg/kg 20mg/kg during dialysisduring dialysis-- Midodrine Midodrine 55--10 10 mg 30min before mg 30min before HDHD
-- Set accurate dry Set accurate dry weightweight-- Use steady UFRUse steady UFR-- Keep Keep dialysatedialysate
NaNa+ + > serum Na> serum Na++
-- Use bicarbonateUse bicarbonatedialysatedialysate-- Avoid food before Avoid food before
HDHD-- Maintain Maintain HctHct > >
33%33%
-- TrendelenburgTrendelenburgpositionposition-- ↓↓ ultrafiltrationultrafiltrationraterate-- 100100--200200 mLmLsaline bolussaline bolus-- mannitolmannitol 12.5 12.5 grams IVgrams IV-- 1010--2020 mLmL 23.4% 23.4% saline over 3saline over 3--5 min5 min
Pharmacologic Pharmacologic PreventionPrevention
NonNon--pharm pharm PreventionPrevention
AcuteAcute
Management of CrampsManagement of Cramps
-- DiphenhydramineDiphenhydramine-- HydroquinineHydroquinine-- OxazepamOxazepam-- PrazosinPrazosin-- QuinineQuinine-- Vitamin EVitamin E
-- set accurate dry wtset accurate dry wt-- stretchingstretching-- kkeep eep dialysatedialysate NaNa+ +
> serum Na> serum Na++
-- stationary bike at stationary bike at bedtimebedtime
-- 100100--200mL saline 200mL saline bolusbolus-- 50mL hypertonic 50mL hypertonic glucoseglucose-- 1010--20mL 23.4% 20mL 23.4% saline over 3saline over 3--5 min 5 min
Pharmacologic Pharmacologic PreventionPrevention
NonNon--pharm pharm PreventionPrevention
AcuteAcute

20
Management of ItchingManagement of Itching
-- Topical emollients or Topical emollients or capsaicin BIDcapsaicin BID-- hydroxyzinehydroxyzine-- cyproheptadinecyproheptadine-- loratidineloratidine//fexofenadinefexofenadine-- cholestyraminecholestyramine-- activated charcoalactivated charcoal
-- deliver adequate Kt/deliver adequate Kt/VVureaurea
-- use biocompatible use biocompatible dialyzersdialyzers-- diet phosphate compliancediet phosphate compliance-- maintain maintain Hct Hct > 33%> 33%-- uv uv B light treatmentB light treatment-- acupunctureacupuncture
Pharmacologic Pharmacologic Prevention*Prevention*
NonNon--pharm pharm PreventionPrevention
*Poor response to antihistamines suggests histamine not predominant mediator
Peritoneal DialysisPeritoneal DialysisThree components of dialysis:Three components of dialysis:1)1) DialysateDialysate filled compartment filled compartment 2) Blood filled compartment 2) Blood filled compartment 3) Semi3) Semi--permeable membrane permeable membrane
No way to regulate blood flow, No way to regulate blood flow, so PD less efficient than HDso PD less efficient than HDLarger molecules permitted to Larger molecules permitted to pass in PD compared to HDpass in PD compared to HDSolute profiles level out, similar Solute profiles level out, similar to endogenous renal functionto endogenous renal function

21
The Peritoneal ProcedureThe Peritoneal Procedure
Dialysate Dialysate flows into peritoneal cavity by flows into peritoneal cavity by gravity over 15 minutesgravity over 15 minutesToxins from blood cross peritoneal Toxins from blood cross peritoneal membrane and enter membrane and enter dialysatedialysateDialysate Dialysate removed and exchanged for new removed and exchanged for new dialysate dialysate solutionsolutionThirty minutes for entire processThirty minutes for entire process
Peritoneal DialysisPeritoneal Dialysis
Types of PDTypes of PDContinuous Ambulatory (CAPD)Continuous Ambulatory (CAPD)–– 3 exchanges during waking hours3 exchanges during waking hours
Automated or Alternative (APD)Automated or Alternative (APD)–– Nocturnal Intermittent (NIPD)Nocturnal Intermittent (NIPD)
No exchange during day, 6No exchange during day, 6--8 at night via cycling machine8 at night via cycling machine
–– Nocturnal Tidal (NTPD)Nocturnal Tidal (NTPD)No exchange during day, 6No exchange during day, 6--8 at night each hour with a 8 at night each hour with a constant volume of constant volume of ≈≈ 1,500 1,500 mLmL in peritoneal cavityin peritoneal cavity
–– Continuous Cyclic (CCPD)Continuous Cyclic (CCPD)Dialysate Dialysate instilled in AM, dwells during day, removed prior to instilled in AM, dwells during day, removed prior to bedbed

22
The Peritoneal “Rx”The Peritoneal “Rx”
Dose altered by Dose altered by ↑↑ osmotic gradient across osmotic gradient across peritoneum peritoneum ↑↑ ultrafiltration ultrafiltration and diffusionand diffusion–– 1) # of bag exchanges per day1) # of bag exchanges per day–– 2) volume of each exchange2) volume of each exchange–– 3) strength of dextrose in 3) strength of dextrose in dialysatedialysateRecommended Kt/Recommended Kt/VVureaurea = 1.7/week= 1.7/week–– Must determine total volume drainedMust determine total volume drained–– Multiply x 7 for weekly Kt/V valueMultiply x 7 for weekly Kt/V value
Kt/V in PDKt/V in PDKt = D/P x volume drained (L/day)Kt = D/P x volume drained (L/day)
Divide by V to give Kt/V per dayDivide by V to give Kt/V per dayMultiple x 7 for weekly dose of Kt/VMultiple x 7 for weekly dose of Kt/VPatients on PD have some Kt/V contributed by Patients on PD have some Kt/V contributed by residual renal function…residual renal function…Initially… Initially…
Kt/Kt/VVtotaltotal = Kt/V= Kt/VPD PD + Kt/+ Kt/VVrenalrenal
As renal As renal fxnfxn declines and reach zero…declines and reach zero…Kt/Kt/VVtotaltotal = Kt/V= Kt/VPDPD

23
Complications of PDComplications of PD
MechanicalMechanical
MedicalMedical
InfectiousInfectious
Mechanical Complications of PDMechanical Complications of PD
Kinking of catheterKinking of catheterInflow/outflow obstructionInflow/outflow obstruction
Catheter motion Catheter motion tissue aggravationtissue aggravationPain from catheter tipPain from catheter tip
Rapid Rapid dialysate dialysate flow flow inflow paininflow pain
24
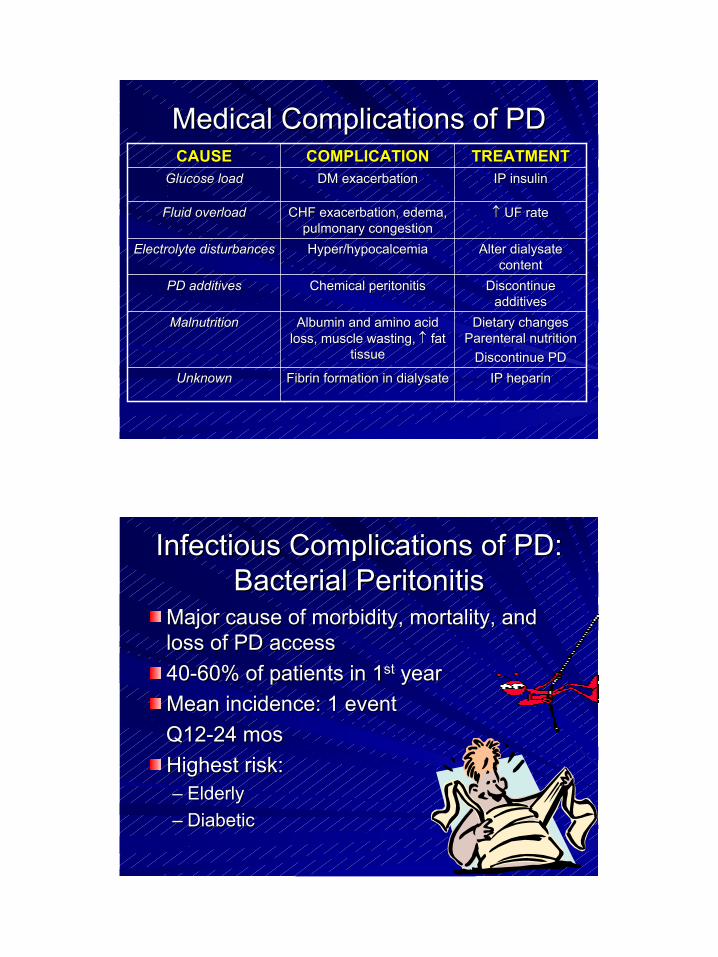
Medical Complications of PDMedical Complications of PD
IP heparinIP heparinFibrin formation in Fibrin formation in dialysatedialysateUnknownUnknown
Dietary changes Dietary changes Parenteral Parenteral nutrition nutrition
Discontinue PDDiscontinue PD
Albumin and amino acid Albumin and amino acid loss, muscle wasting, loss, muscle wasting, ↑↑ fat fat
tissuetissue
MalnutritionMalnutrition
Discontinue Discontinue additivesadditives
Chemical peritonitisChemical peritonitisPD additivesPD additives
Alter Alter dialysate dialysate contentcontent
Hyper/Hyper/hypocalcemiahypocalcemiaElectrolyte disturbancesElectrolyte disturbances
↑↑ UF rateUF rateCHF exacerbation, edema, CHF exacerbation, edema, pulmonary congestionpulmonary congestion
Fluid overloadFluid overload
IP insulinIP insulinDM exacerbationDM exacerbationGlucose loadGlucose loadTREATMENTTREATMENTCOMPLICATIONCOMPLICATIONCAUSECAUSE
Infectious Complications of PD:Infectious Complications of PD:Bacterial PeritonitisBacterial Peritonitis
Major cause of morbidity, mortality, and Major cause of morbidity, mortality, and loss of PD accessloss of PD access4040--60% of patients in 160% of patients in 1stst yearyearMean incidence: 1 event Mean incidence: 1 event Q12Q12--24 24 mosmosHighest risk:Highest risk:–– ElderlyElderly–– DiabeticDiabetic

25
Signs and Symptoms of Signs and Symptoms of PeritonitisPeritonitis
1818ChillsChills
2525Nausea/VomitingNausea/Vomiting
3838FeverFever
7676Abdominal Abdominal tendernesstenderness
9898Cloudy effluentCloudy effluent
Incidence (%)Incidence (%)Sign/Sign/SxSx
Diagnosing PeritonitisDiagnosing PeritonitisCloudy Cloudy dialysatedialysate
Signs and symptomsSigns and symptoms
Culture Culture dialysatedialysate–– WBC > 100/mmWBC > 100/mm33
–– > 50% > 50% neutrophilsneutrophils
Gram’s stainGram’s stain

26
Microbiological EtiologyMicrobiological Etiology
55--2020FungiFungi1010--1515Mixed infectionsMixed infections22--33ProteusProteus22--33KlebsiellaKlebsiella22--33AcinetobacterAcinetobacter22--33EnterobacterEnterobacter55--88Pseudomonas Pseudomonas aeruginosaaeruginosa
55--1212Escherichia coliEscherichia coli33--55EnterococciEnterococci
1010--1515StreptococciStreptococci1010--2020Staphylococcus Staphylococcus aureusaureus3030--4545Staphylococcus Staphylococcus epidermidisepidermidis
% of Episodes% of EpisodesOrganismOrganism
Treatment of PeritonitisTreatment of Peritonitis
Empiric antibiotic therapyEmpiric antibiotic therapy
Gram positive cultureGram positive culture
Gram negative cultureGram negative culture

27
Empiric Antibiotics for PeritonitisEmpiric Antibiotics for Peritonitis

28
29
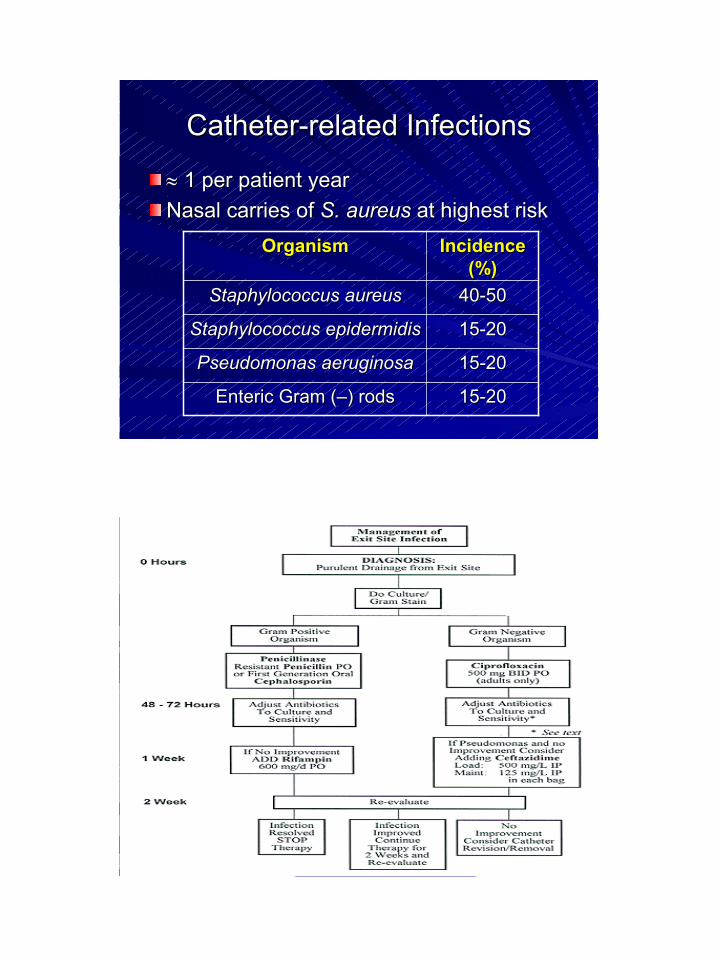
CatheterCatheter--related Infectionsrelated Infections
≈≈ 1 per patient year1 per patient yearNasal carries of Nasal carries of S. S. aureusaureus at highest riskat highest risk
1515--2020Enteric Gram (Enteric Gram (––) rods) rods
1515--2020Pseudomonas Pseudomonas aeruginosaaeruginosa
1515--2020StaphylococcusStaphylococcus epidermidisepidermidis
4040--5050Staphylococcus Staphylococcus aureusaureus
Incidence Incidence (%)(%)
OrganismOrganism

30
Advantages and Disadvantages Advantages and Disadvantages of of HemodialysisHemodialysis
AdvantagesAdvantages–– High solute clearanceHigh solute clearance–– Clear adequacy Clear adequacy
paramtersparamters–– Low failure ratesLow failure rates–– Better correction of Better correction of
hemostasishemostasis–– Close monitoring of Close monitoring of
patientpatient
DisadvantagesDisadvantages–– Multiple visits/weekMultiple visits/week–– Long adjustment for Long adjustment for
complicationscomplications–– Complement activating Complement activating
membranesmembranes–– Vascular access Vascular access
infectionsinfections–– Faster decline of Faster decline of
residual renal residual renal fxn fxn than than PDPD
Advantages and Disadvantages Advantages and Disadvantages of Peritoneal Dialysisof Peritoneal Dialysis
AdvantagesAdvantages–– Patient can do alonePatient can do alone–– No electricity or HNo electricity or H22OO–– PortablePortable–– No anticoagulant No anticoagulant
neededneeded–– Minimal CV stressMinimal CV stress–– No blood lossNo blood loss–– IP drug deliveryIP drug delivery–– Clearance of larger Clearance of larger
solutessolutes
DisadvantagesDisadvantages–– High risk of peritonitisHigh risk of peritonitis–– Patient selfPatient self--imageimage–– Transport of materialsTransport of materials–– High protein lossesHigh protein losses–– Lower urea clearance Lower urea clearance
than HDthan HD–– Patient burnoutPatient burnout–– Excessive glucose Excessive glucose
absorption absorption obesityobesity–– Mechanical problemsMechanical problems

31
The Pharmacist’s RoleThe Pharmacist’s Role
Knowing pharmacokinetic alterationsKnowing pharmacokinetic alterationsAdjustment of doses in renal failureAdjustment of doses in renal failureProper use of expensive drugsProper use of expensive drugs–– AntibioticsAntibiotics–– EpogenEpogen–– IV iron productsIV iron productsReplacement of dialyzed drugsReplacement of dialyzed drugs–– AntibioticsAntibiotics–– WaterWater--soluble vitamins (“soluble vitamins (“NephrocapsNephrocaps”)”)
Factors Increasing Drug RemovalFactors Increasing Drug Removal
↓↓ protein bindingprotein binding
↑↑ hydrophilicityhydrophilicity
↑↑ concentration concentration gradient (high gradient (high
steady state level)steady state level)
countercurrent countercurrent flowflow
membrane bindingmembrane binding
↓↓ VVDD↑↑ dialysis flow ratedialysis flow ratechargecharge
chargecharge↑↑ durationduration↑↑ surface areasurface area
↓↓ molecular wtmolecular wt↑↑ blood flow rateblood flow rate↑↑ pore sizepore size
DrugDrug--specificspecificDialysisDialysis--specificspecificDialyzerDialyzer--specificspecific

32
Protein BindingProtein Binding
Only unbound drugs eliminated by RRTOnly unbound drugs eliminated by RRTAbility of drug to be filtered determined by Ability of drug to be filtered determined by sieving coefficient (SC), or “nonsieving coefficient (SC), or “non--bound bound fraction”fraction”SC determined by:SC determined by:–– % protein binding% protein binding–– membrane charge (i.e. binding to membrane)membrane charge (i.e. binding to membrane)–– porosity of membraneporosity of membrane
Sieving CoefficientSieving Coefficient
SC = SC = CCufuf/C/CPP
SC = sieving coefficientSC = sieving coefficientCCufuf = conc. of drug in = conc. of drug in ultrafiltrate ultrafiltrate (waste)(waste)
CCPP = conc. of drug in plasma (blood)= conc. of drug in plasma (blood)
If SC = 1, drug freely filteredIf SC = 1, drug freely filteredIf SC = 0, drug not filtered (highly protein bound)If SC = 0, drug not filtered (highly protein bound)

33
Drug DosingDrug Dosing
Drugs with renal clearance > 30% of total Drugs with renal clearance > 30% of total body clearance require replacementbody clearance require replacementLoading doses:Loading doses:–– No adjustments necessaryNo adjustments necessary–– Depends on target blood levelDepends on target blood level
LD (mg) = desired CLD (mg) = desired CPP (mg/L) x (mg/L) x VVd d (L)(L)LD = loading doseLD = loading dose
CCPP = plasma concentration= plasma concentrationVVd d = volume of distribution= volume of distribution
Drug DosingDrug Dosing
Example: Example: Vanco Vanco loading doseloading dosePt wt = 65kg Pt wt = 65kg VVdd = 0.7 L/kg C= 0.7 L/kg CPP = 35mg/L= 35mg/L
LD (mg) = desired CLD (mg) = desired CPP (mg/L) x(mg/L) x VVdd (L)(L)
Vanco Vanco dose = 35 mg/L x (65kg x 0.7 L/kg)dose = 35 mg/L x (65kg x 0.7 L/kg)= 35 mg/L x 45.5 L= 35 mg/L x 45.5 L
= 1592.5 mg = 1592.5 mg = = ≈≈ 1500mg1500mg

34
Drug DosingDrug Dosing
Maintenance DosingMaintenance Dosing–– Maintain therapeutic levelsMaintain therapeutic levels–– Use therapeutic drug monitoring (TDM) if Use therapeutic drug monitoring (TDM) if
possible (i.e. possible (i.e. vancovanco/gent drug levels)/gent drug levels)–– Creatinine Creatinine clearance methodclearance method
Estimates rate of drug removalEstimates rate of drug removalDoes not account for residual renal clearance Does not account for residual renal clearance (unless (unless anuricanuric) or non) or non--renal clearancerenal clearance
Creatinine Creatinine Clearance MethodClearance Method
CrCl CrCl = SC x UFR= SC x UFR
SC = sieving coefficientSC = sieving coefficientUFR = UFR = ultrafiltration ultrafiltration rate rate (rate of waste into bag)(rate of waste into bag)

35
Creatinine Creatinine Clearance MethodClearance MethodExample: Example: CrCl CrCl method for renal clearancemethod for renal clearance
Patient on CVVH with an UFR of 1.8 L/hrPatient on CVVH with an UFR of 1.8 L/hr
SC = 1.0 UFR = 1.8 L/hrSC = 1.0 UFR = 1.8 L/hrCrClCrCl = SC x UFR= SC x UFR
CrCl CrCl = 1.0 x 1.8 L/hr = 1.0 x 1.8 L/hr = 1,800 = 1,800 mLmL/hr/hr= 30 = 30 mLmL/min/min
Questions?Questions?
Related Documents











