Renal replacement therapy in children Dr. Lokesh R pediatrics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Renal replacement therapyin children
Dr. Lokesh R
pediatrics

RENAL REPLACEMENT
• DEFINITION
• MODALITIES
• INDICATIONS- AKI / ESRD
• PERITONEAL DIALYSIS
• HEMODIALYSIS

DEFINITION
Renal replacement therapy
is a procedure which help to clear
accumulated solutes, water or toxins from
the blood by diffusion or convection or both
across a semipermeable membrane.
Renal failure important and independent factor determines outcome in critically ill children-morbidity and mortality

MODALITIES OF RRT
• Peritoneal dialysis
• Intermittent Hemodialysis (IHD)
• Continuous renal replacement (CRRT)
• Renal transplantation – best for ESRD
– Decision of modality determined by size of pt, duration , abdominal pathology,catabolicrate, hemodynamic stability, vascular access and whether primary goal is fluid or solute removal, resources availability

Indications for Dialysis1. In Acute renal failure:
Inadequate response to conservative management
• A : Acidosis metabolic (pH < 7.2)
• E : Electrolytes -- Hyperkalemia (K >6.5 meq/L)
or rapidly rising K, 5.5-6.5 with EEC changes),
• I : Ingestion - toxins and drugs
• O : Overload of fluid – symptomatic >15-20%
• U : Uremia - pericarditis, encephalopathy, bleeding

Indications for Dialysis
2. In chronic renal failure:
GFR= <15 ml/min/1.73 m2 body surface area
Severe hypertension.
Intractable intravascular volume overload
Profound electrolyte abnormalities:
hyperkalemia or hyperphosphatemia.

Dialysis- principles 1. Diffusion
2. Convection
Dialysis = diffusion = passive movement
of solutes across a semi-permeable
membrane down concentration gradient– small molecules

Dialysis- principles
Hemfiltration = convection = solute + fluid
removal across semi-permeable membrane
down a pressure gradient (solvent drag)-hydrostatic
pressure / osmotic pressure
fluid ,small and medium-size

PERITONEAL DIALYSIS
PD catheters
• Polyurethane trocar catheter: infant, pediatric and adult sizes.
• Most commonly used PD catheter: silasticTenckhoff catheter

Hard catheter
• Hard catheter

PD solutions
Potassium:3-4 meq/lHeparin 500-1000U/L
DEXTROSE—OSMOTIC GRADIENT, HIGH DEX- HYPERGLYCEMIA,
PEROTONITIS. ALT- ICODEXTRIN

Preparation of dialysate
• Solution A: 440 ml 5% dextrose + 60 ml sodium bicarbonate
• Solution B: 500 ml normal saline
• 500 ml solution B +250 ml solution A,
• Sodium : 140 mEq/l,
• Bicarbonate: 40 mEq/l
• Dextrose : 1.5 g/dl
• IV calcium:precipitate if added to a bicarbonate containing fluid.

Insertion of the Catheter
1. Empty the bladder2. Surgically drape the abdomen.3. Anesthetize the skin and subcutaneous tissue
in the midline at 1/3rd of the distance from the umbilicus to the public symphysis.
In young infants, it may be preferable to insert the catheter in the left flank.
4. Insert a gauge 16 or 18 ‘intracath’ at the above point into the peritoneal cavity and infuse 20 to 40 ml/kg of warmed dialysateover a period of 5 to 10 minutes to distend the abdomen and facilitate catheter insertion.

5.Remove the ‘intracath’ and prepare the PD catheter. Insert the stylet into the catheter and note the black markings indicating the direction of the curve of the tip, which should face the pubic symphysis.
6. Puncture the abdominal skin with a No. 15 blade held vertically.
7. Insert the PD catheter with the styletusing a gentle ‘boring’ motion. Entry into the peritoneal cavity is indicated by a sudden decrease in resistance & gush of dialysis fluid into the catheter.

8. Attach the right-angled end of the connecting set to the catheter and run in dialysis fluid, which should flow in a continuous stream.
9. About half the dialysate is allowed to rapidly run out by gravity drainage.
10. The inflow is then started.
11. Strict asepsis must be maintained throughout the procedure.
• Optimal fill volume of dialysate for each exchange : 1100-1200 ml/m2 BSA
• 30-50 ml/kg/body weight.
• The fill volume should not exceed a maximum of 2 l.

• Acute PD can be performed either manually or by a machine.
• 3 phases,
• Fill time = 5-10 minutes
• Dwell time =30-45 minutes
• Drain time = 5-10 minutes
• Total cycle = 60 minutes.

• Dialysis is continued till
• Correction of fluid & electrolyte disturbances
• Acidosis is corrected,
• Blood urea level is reduced
• Renal function starts recovering.
Once the last exchange is over, the dialysateis drained out completely and the catheter is removed.

Monitoring • BP & HR
• Intake & output.
• Weight at least once daily
• Blood levels :Urea, creatinine, electrolytes & sugar should be measured daily or more frequently.
• Peritoneal fluid should be examined periodically to detect peritonitis

Complications
• Bleeding after catheter insertion• Perforation of gut• Abdominal pain• Leakage around catheter• Difficult drainage• Pulmonary complications• Exit site infections• Peritonitis• Metabolic problems

CHRONIC PERITONEAL DIALYSIS
• Accepted mode of treatment for patients awaiting renal transplantation.
Chronic dialysis: 2 types
• CAPD (chronic ambulatory peritoneal dialysis) performed manually
• CCPD (continuous cycling peritoneal dialysis) automated device
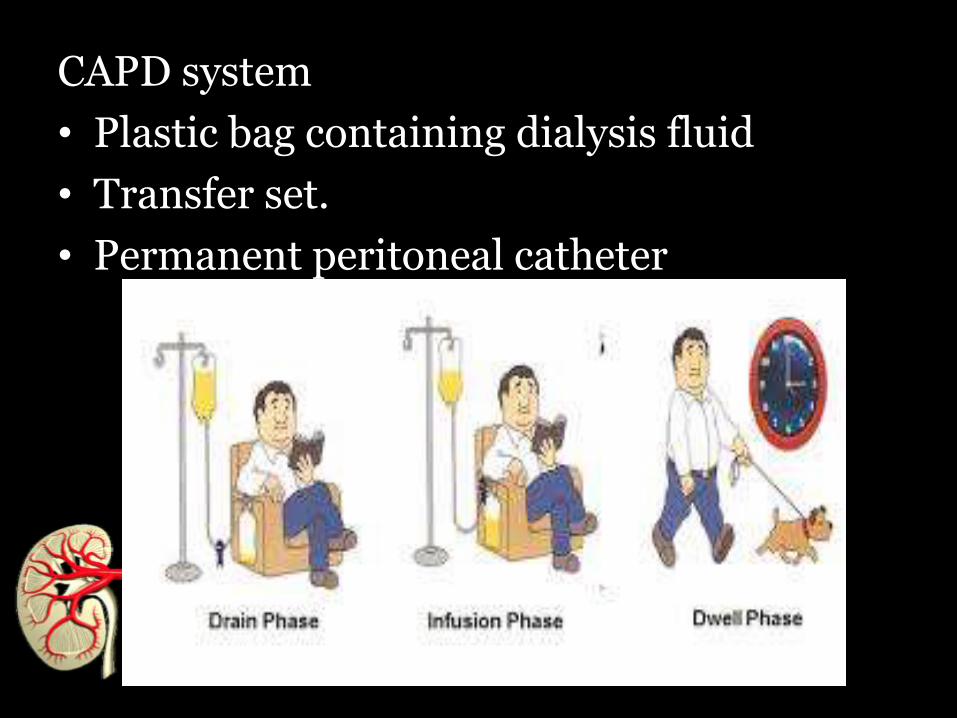
CAPD system
• Plastic bag containing dialysis fluid
• Transfer set.
• Permanent peritoneal catheter

Dialysis Prescription
• 4-6 daily exchanges are carried out while the child is awake (every 4-6 hour).
• Goal volume of 1100-1200 ml/1.73 m2/cycle.

Advantages:
• Continuous removal of solute & water.
• Avoids rapid fluid & solute shifts.
• Hypertension & anemia better controlled.
• Particularly suitable for infants & small children.
Disadvantage:
• Peritonitis
• Abdominal wall hernia,
• Hydrothorax
• Respiratory difficulty
• Protein & amino acids loss.
• Hypogammaglobulinemia
• Diabetes, obesity and hyperlipidemia

Automated Peritoneal Dialysis (APD)
• Cycler is used to help in the delivery and drainage of dialysate.
• Cycling of dialysate during the night while the child is asleep.
• Small volume of dialysate allowed to dwell during the daytime while the child carries out his/her normal activities.

Dialysis prescription• Total of about 10 hours of exchanges
during the night (6 cycles, each about 1.5 hr in duration)
Advantages
• Reduces the risk of peritonitis
• Better metabolic control
• Freedom to the child during the daytime.

INTERMITTENT HEMODIALYSIS
• Rapid ultrafiltration and solute removal
• Accurate & precise volume removal.
• Ultrafiltration & solute removal can be isolated from each other and independently controlled.

Click to add title
Basic principles of HD
• Ultrafiltration
• Solute removal
• Convective transport
• Diffusive transport
Dialyser -polysulfone
Dialyser -polysulfone

Hemodialysis
• Dialysis occurs when blood and dialysateare made to interface across an artificial semi-permeable membrane (the dialyzer) outside the body.
• The driving force behind ultrafiltration is the hydrostatic pressure gradient across the dialyzer that the HD machine generates using a pump.

In HDIn HD


Vascular Access
Short term IHD:
• Femoral , subclavian or internal jugular(IJ) veins.
Long -term IHD
• Central venous catheter
• Arteriovenous (AV) fistulae

Dialyzers and Blood Tubing
• Extracorporeal blood not exceed 10-15% of the blood volume.
• Surface area of the dialyzer =75-100% BSA of the child.

Dialysis Prescription
• Dialyzer and blood tubing.
• Duration of dialysis= 3-4 hours per session,
• Frequecy = 3/week (every other day).
• Infants & small children may require daily dialysis.

Difficulties During Dialysis1.Dialysis disequilibrium syndrome:
Manifested as seizures.
• Rapid solute removal with a resultant fall in plasma osmolality.
• First few cycles.
• Associated with very high BUN.
Prevention
• Continuous mannitol infusion at 0.5 to 1 g/kg.
• Dialysis using low blood flow rates.

2. Hypotension.
Prevention
• Rapid infusion of low volumes (50-100 ml) of normal saline or albumin
• Temporarily stopping ultrafiltration.
Disadvantages
• Hemodynamic instability due to rapid fluid shifts induced by volume removal and osmotic changes relating from rapid correction of azotemia,
• Need for systemic anticoagulation and the risk of bleeding,
• Technical challenges in using it in smaller children.

CONTINUOUS RENAL REPLACEMENT THERAPY• HD therapies done for days to weeks.
• Continuous & prolonged without interruption.
Advantages
• Less rapid osmotic shifts.
• Hemodynamic stability much better than IHD.
Modality of choice:
• Critically ill & hemodynamically unstable.
• Patients on vasoactive infusions for sepsis or cardiogenic shock.

CRRT Modalities
1. CVVH- Continuous Veno-Venous Hemofiltration1. Convection
2. CVVHD- Continuous Veno-Venous Hemodialysis1. Diffusion
3. CVVHDF- Continuous Veno-Venous Hemodiafiltration1. Diffusion and Convection
• Blood from the patient is removed from the venous circulation and returned back into the venous system

Indications for CRRT• Critically ill, hemodynamically unstable
patients
• Neonates & infants with cardiovascular or abdominal surgery, trauma with shock and multisystem failure.
• Removes inflammatory cytokines
• Rapid generation of toxic metabolites:
• Inborn error of metabolism
• Tumor lysis syndrome.

Dialysis Prescription
• Starting net ultrafiltration rate is 0-1 mg/kg body weight per hour.
• Hourly basis calculation is done of all the fluids given.
• Dialysate flow rates are much slower:2000 ml/1.73 m2 BSA/hour.

Disadvantages of CRRT
• Hypomagnesemic & hypophosphatemic.
• Continuous & prolonged anticoagulation
• Technically more challenging.

Advantages and disadvantages of various modalities of renal
replacement therapy

Nutritional Management
• 100 to 110% of RDA for calories & protein.• Daily protein intake: S albumin>3g/dl
• Infants & children < 3 years =2.5-3 g/kg,
• 3 to 12 years = 2.0-2.5 g/kg • Postpubertal children = 1-1.5 g/kg
• Vitamins and micronutrients • Other medications:
• erythropoietin,• Iron • Vitamin D

TAKE HOME MESSAGE
• In children with renal failure RRT – important and
independent determinant of outcome
• Newborn and young children – PD clear advantage over
hemodialysis
• Hard PD catheter left maximum of 72 hours
• With the availability of HD one can control ultrafiltrate
or solute removal independently, accurately
• Renal transplant is the Best RRT for ESRD

References
1. Pediatric nephrology-Avner. 5th edition.
2. Pediatric nephrology- Arvind Bagga 5th
edition
3. Nelson textbook of pediatrics- 19th edition.
4. Uptodate.com
5. Acute renal replacement therapy in pediatrics-International Journal of Nephrology

Thank you

Hemodialysis
Advantages
• Maximum solute clearance
• Best tx for severe hyper-K+
• Ready availability
• Limited anti-coagulation time
• Bedside vascular access
Disadvantages
• Hemodynamic instability
• Hypoxemia
• Rapid fluid + solute shifts
• Complex equipment
• Specialized personnel
• Difficult in small infants

Peritoneal dialysis
Advantages• Simple to set up +
perform• Easy to use in infants• Hemodynamic stability• No anti-coagulation• Bedside peritoneal
access
Disadvantages• Unreliable
ultrafiltration• Slow fluid + solute
removal• Drainage failure,
leakage• Catheter obstruction• Respiratory
compromise• Hyperglycemia• Peritonitis
CVVHAdvantages
• Easy to use in PICU
• Rapid electrolyte correction
• Excellent solute clearances
• Rapid acid/base correction
• Controllable fluid balance
• Tolerated by unstable patients
• Early use of TPN
• Bedside vascular access routine
Disadvantages
• Systemic anticoagulation *
• Citrate anticoagulation new
• Frequent filter clotting
• Hypotension in small infants
• Vascular access in infants
Related Documents





![THAILAND RENAL REPLACEMENT THERAPY YEAR 2011 · 2020. 8. 27. · THAILAND RENAL REPLACEMENT THERAPY YEAR 2011 ] Page 3 ACKNOWLEDGEMENTS The Thai Renal Replacement Therapy (TRT) committee](https://static.cupdf.com/doc/110x72/6096115f208ae70f0b464852/thailand-renal-replacement-therapy-year-2011-2020-8-27-thailand-renal-replacement.jpg)





