~)Copyright 1995by Humana Press Inc. All rights of any nature whatsoever reserved. 0163-4984/95/4802-0121 $06.00 Elevated Serum Silicon Levels in Women with Silicone Gel Breast Implants SUZANNE S. TEUBER,*'1'2 ROBERT L. SAUNDERS,1 GEORGES M. HALPERN, 1 ROBERT F. BRUCKER, 3 VICTOR CONTE, 3 BRIAN D. GOLDMAN, 3 EDWARD E. WINGER, 3 W. GRAHAM WOOD, 3 AND M. ERIC GERSHWIN 1 Division of Rheumatology, Allergy and Clinical Immunology, University of California, Davis, School of Medicine, Davis, CA 95616; 2Veterans Administration, Northern California System of Clinics, Pleasant Hill, CA; and 3Bay Area Laboratory Co-operative (BALCO), Burlingame, CA Received July 22, 1994; Revised October 23, 1994; Accepted November 20, 1994 ABSTRACT The metabolic fate of silicone gel leaked from an intact or rup- tured prosthesis is unknown. In this study, serum was blindly assayed by inductively coupled plasma atomic emission spectroscopy (ICP-AES) for elemental silicon in 72 women with silicone gel breast implants and 55 control women (mean age 48 yr, both groups). Blood was drawn and processed using silicon-free materials. The mean sili- con level in controls was 0.13 + 0.07 mg/L (range 0.06-0.35 mg/L), whereas in implant patients, the mean was significantly higher at 0.28 + 0.22 mg/L (range 0.06-0.87 rag/L) (P < 0.01, Student's t-test with correction for unequal variances). Using the mean of the control group + 2 SD as a cutoff for normal range (0.27 mg/L), 25/72 (34.7%) implant patients exceeded this value, compared with 2/55 (3.6%) con- trols. There was no significant correlation between past rupture of one or both implants, current rupture at the time of the blood draw, or the number of years with implants and silicon levels. The results suggest that serum silicon levels are elevated in many women with silicone gel breast implants. The chemical species involved and kinet- ics of this elevation remain to be determined. *Author to whom all correspondence and reprint requests should be addressed. Biological Trace Element Research 121 Vol. 48, 1995

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
~)Copyright 1995 by Humana Press Inc. All rights of any nature whatsoever reserved. 0163-4984/95/4802-0121 $06.00
Elevated Serum Silicon Levels in Women with Silicone Gel
Breast Implants SUZANNE S. TEUBER, *'1'2 ROBERT L. SAUNDERS, 1
GEORGES M. HALPERN, 1 ROBERT F. BRUCKER, 3 VICTOR CONTE, 3 BRIAN D. GOLDMAN, 3 EDWARD E. WINGER, 3
W. GRAHAM WOOD, 3 AND M. ERIC GERSHWIN 1
Division of Rheumatology, Allergy and Clinical Immunology, University of California, Davis, School of Medicine, Davis, CA 95616; 2Veterans Administration, Northern California System
of Clinics, Pleasant Hill, CA; and 3Bay Area Laboratory Co-operative (BALCO), Burlingame, CA
Received July 22, 1994; Revised October 23, 1994; Accepted November 20, 1994
ABSTRACT
The metabolic fate of silicone gel leaked from an intact or rup- tured prosthesis is unknown. In this study, serum was blindly assayed by inductively coupled plasma atomic emission spectroscopy (ICP-AES) for elemental silicon in 72 women with silicone gel breast implants and 55 control women (mean age 48 yr, both groups). Blood was drawn and processed using silicon-free materials. The mean sili- con level in controls was 0.13 + 0.07 mg /L (range 0.06-0.35 mg/L), whereas in implant patients, the mean was significantly higher at 0.28 + 0.22 mg /L (range 0.06-0.87 rag/L) (P < 0.01, Student's t-test with correction for unequal variances). Using the mean of the control group + 2 SD as a cutoff for normal range (0.27 mg/L), 25/72 (34.7%) implant patients exceeded this value, compared with 2/55 (3.6%) con- trols. There was no significant correlation between past rupture of one or both implants, current rupture at the time of the blood draw, or the number of years with implants and silicon levels. The results suggest that serum silicon levels are elevated in many women with silicone gel breast implants. The chemical species involved and kinet- ics of this elevation remain to be determined.
*Author to whom all correspondence and reprint requests should be addressed.
Biological Trace Element Research 121 Vol. 48, 1995
122 Teuber et al.
Index Entries: Serum silicon; silicone; breast implants; induc- tively coupled plasma atomic emission spectrometry.
INTRODUCTION
Biomedical applications of silicones have been numerous (1). Sili- cones are generally very well tolerated by the body, but occasional adverse reactions to the foreign material have been noted, for example, as complications of joint replacement or ventriculoperitoneal shunts (2,3). Currently, there are concerns that long-term exposure to components of silicone gel-filled breast implants may be associated with autoimmune or inflammatory diseases (4). Polydimethylsiloxane (PDMS) polymers, which form the silicone gel in breast implants, are manufactured from elemental silicon. The silicone rubber implant shell is also made of PDMS with fumed, amorphous silica added as a strengthening filler (5). It has been shown that the gel can bleed through the implant shell over time (6). In addition, there is potential for mechanical breakdown and degra- dation of the implant shell owing to hydrolysis, mechanical forces, and perhaps effects of oxidative attack from the body's inflammatory cells (7). Silicon is a major component of breast implants, accounting for 35--40% of the implant by weight (8). If implant components are degraded with time and gain access to the circulation after leakage or rupture, circulat- ing silicon might be elevated in the blood or serum of such women as soluble silicic acid, or even as hydrophobic silicone fragments in associ- ation with lipids or carried in peripheral blood cells. A recent study involving several women has shown silicon-containing material that was presumed to have migrated from their silicone gel implants to sites of connective tissue disease (9). In the current study, we examined the sera of women with and without implants, hypothesizing that the silicone gel implants would serve as an endogenous source of ongoing elevation of serum silicon levels, especially in those women who had ruptures at the time of the blood draw or a history of past rupture.
METHODS
Subjects Women with silicone gel breast implants were recruited by a press
release announcing the study. Some women were referred for the study after undergoing ultrasound or mammography locally. Control women were recruited to match the ages of the subjects. Informed consent was obtained from all volunteers. Women were excluded if they had only one implant, dual lumen or saline implants, or polyurethane coating, because it was unknown how these variables might affect serum silicon levels. Women were also excluded if their implants had been removed prior to
Biological Trace Element Research Vol. 48, 1995
Silicone Implants and Silicon Levels 123
the blood draw. Women with a history of renal disease were ineligible because of the known relationship between renal insufficiency and ele- vated blood silicon levels (10,11). The subjects were instructed to fast, dis- continue any medication (prescription or over-the-counter), and drink only bottled or municipal water (not well water, which has been reported to contain higher levels of silicon [12]) for 12 h before the serum samples were collected.
Ordinary disposable syringes or vacutainer tubes are contaminated with silicon and cannot be used to obtain serum samples (13). The sam- ples were collected using silicon-free polypropylene syringes (10 mL Neutral Luer-Monovette, Sarstedt, Inc., Newton, NC) and 21-gage x 1 in. Precision Glide needles (Becton Dickinson, Franklin Lakes, NJ). After allowing 1 h for clotting, the samples were centrifuged at 2500 rpm for 10 min, and the serum was removed with disposable polyethylene pipets and stored in 8-mL polypropylene tubes (Sarstedt, Inc.) at 4~ If the serum sample was of an adequate amount, an additional aliquot was frozen for creatinine determination. Samples for silicon analysis were labeled with an accession number and sent by overnight express mail on ice to the laboratory for blinded assay.
Equipment Serum samples were analyzed using an inductively coupled plasma
atomic emission spectrometer (ICP-AES) (Applied Research Laboratories, Dearborn, MI; Model 34000 simultaneous ICP) equipped with a C-3 type concentric nebulizer (Precision Glassblowing, Englewood, CO). The sam- ples were introduced to the argon plasma by using a peristaltic pump (Gilson Medical Electronics, Inc., Middleton, WI; Model Minipuls 2) and autosampler (Gilson Model SC-15B). The serum samples and calibration standards were weighed in 12-mL polypropylene centrifuge tubes (Sar- stedt, Inc.).
Reagents Doubly deionized water, used for the preparation of all solutions,
was prepared by passing reverse osmosis purified water (Premier, Phoenix, AZ; Model ROTFC 4SV) successivly through combination organic mixed-bed and ultrapure mixed-bed exchange cartridges (Barn- stead/Thermolyne, Dubuque, IA).
A silicon stock standard solution (1.0 mg/L) was prepared by dilut- ing a commercial 1000 mg/L certified standard silicon solution (Lot 982DB, SPEX Industries, Inc., Edison, NJ) with 10 mL/L HNO3 (Redis- tilled Nitric Acid, GFS Chemicals, Inc., Columbus, OH). The silicon solu- tion was dispensed using an Eppendorf 1000-p,L pipeter and blue pipet tip (Brinkman, Model 4700). The nitric acid was dispensed using a Nal- gene 10-mL polypropylene graduated cylinder (Nalge Company,
Biological Trace Element Research Vol. 48, 1995
124 Teuber et al.
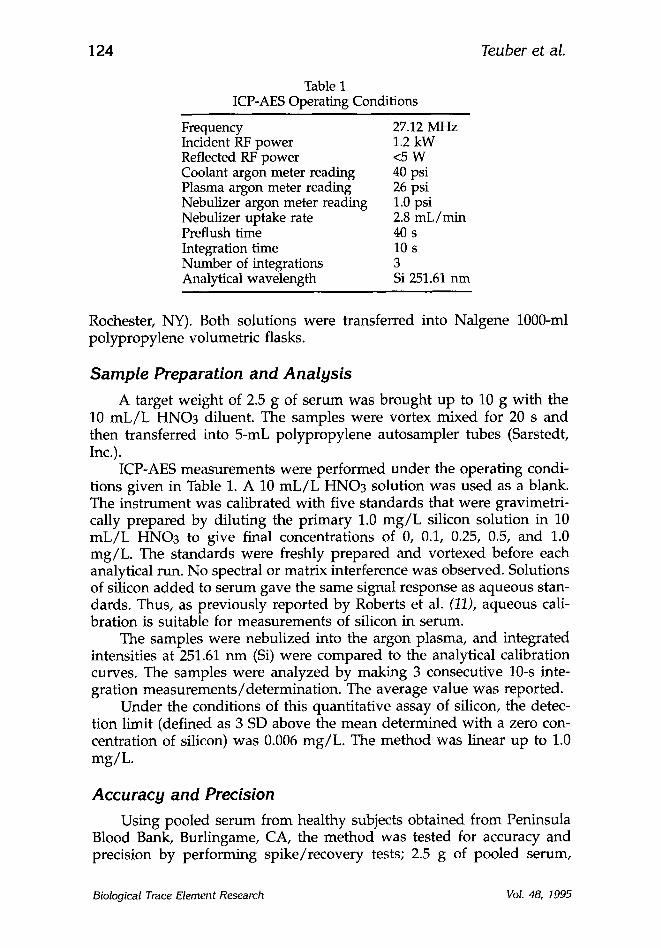
Table 1 ICP-AES Operating Conditions
Frequency 27.12 MHz Incident RF power 1.2 kW Reflected RF power <5 W Coolant argon meter reading 40 psi Plasma argon meter reading 26 psi Nebulizer argon meter reading 1.0 psi Nebulizer uptake rate 2.8 mL/min Preflush time 40 s Integration time 10 s Number of integrations 3 Analytical wavelength Si 251.61 nm
Rochester, NY). Both solutions were transferred into Nalgene 1000-ml polypropylene volumetric flasks.
Sample Preparation and Analysis A target weight of 2.5 g of serum was brought up to 10 g with the
10 mL/L HNO3 diluent. The samples were vortex mixed for 20 s and then transferred into 5-mL polypropylene autosampler tubes (Sarstedt, Inc.).
ICP-AES measurements were performed under the operating condi- tions given in Table 1. A 10 mL/L HNO3 solution was used as a blank. The instrument was calibrated with five standards that were gravimetri- cally prepared by diluting the primary 1.0 mg/L silicon solution in 10 mL/L HNO3 to give final concentrations of 0, 0.1, 0.25, 0.5, and 1.0 mg/L. The standards were freshly prepared and vortexed before each analytical run. No spectral or matrix interference was observed. Solutions of silicon added to serum gave the same signal response as aqueous stan- dards. Thus, as previously reported by Roberts et al. (11), aqueous cali- bration is suitable for measurements of silicon in serum.
The samples were nebulized into the argon plasma, and integrated intensities at 251.61 nm (Si) were compared to the analytical calibration curves. The samples were analyzed by making 3 consecutive 10-s inte- gration measurements/determination. The average value was reported.
Under the conditions of this quantitative assay of silicon, the detec- tion limit (defined as 3 SD above the mean determined with a zero con- centration of silicon) was 0.006 mg/L. The method was linear up to 1.0 mg/L.
Accuracy and Precision Using pooled serum from healthy subjects obtained from Peninsula
Blood Bank, Burlingame, CA, the method was tested for accuracy and precision by performing spike/recovery tests; 2.5 g of pooled serum,
Biological Trace Element Research Vol. 48, 1995
Silicone Implants and Silicon Levels
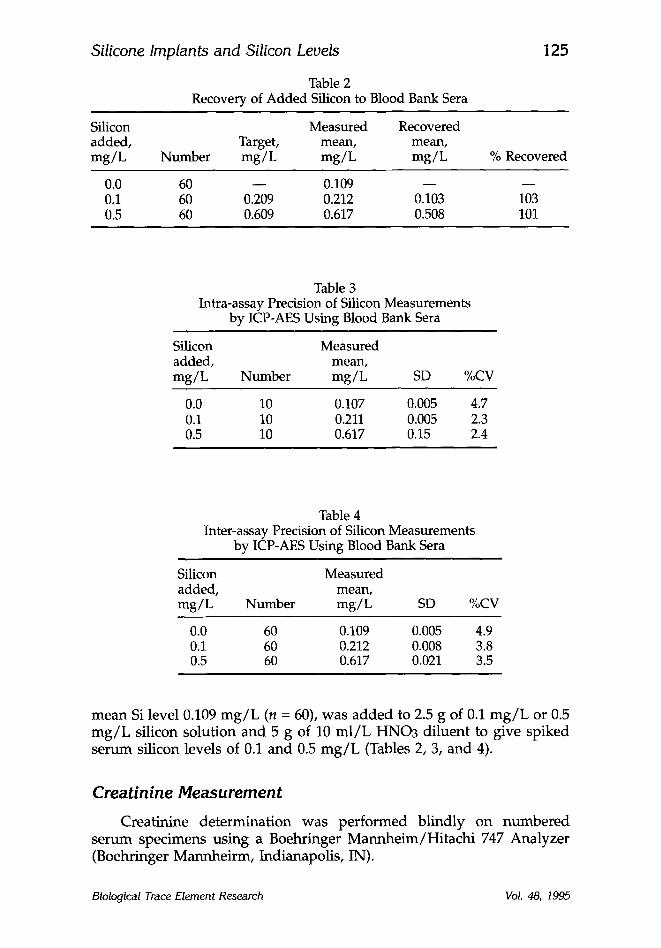
Table 2 Recovery of Added Silicon to Blood Bank Sera
125
Silicon Measured Recovered added, Target, mean, mean, mg /L Number mg/L mg /L mg /L % Recovered
0.0 60 - - 0.109 - - 0.1 60 0.209 0.212 0.103 0.5 60 0.609 0.617 0.508
103 101
Table 3 Intra-assay Precision of Silicon Measurements
by ICP-AES Using Blood Bank Sera
Silicon added, mg /L
Measured mean,
Number mg/L SD %CV
0.0 10 0.107 0.005 4.7 0.1 10 0.211 0.005 2.3 0.5 10 0.617 0.15 2.4
Table 4 Inter-assay Precision of Silicon Measurements
by ICP-AES Using Blood Bank Sera
Silicon Measured added, mean, mg /L Number mg/L SD %CV
0.0 60 0.109 0.005 4.9 0.1 60 0.212 0.008 3.8 0.5 60 0.617 0.021 3.5
m e a n Si level 0.109 m g / L (n = 60), was added to 2.5 g of 0.1 m g / L or 0.5 m g / L silicon solut ion and 5 g of 10 m l / L HNO3 di luent to give spiked se rum silicon levels of 0.1 and 0.5 m g / L (Tables 2, 3, and 4).
Creatinine Measurement
Creatinine de te rmina t ion was pe r fo rmed bl indly on n u m b e r e d se rum specimens us ing a Boehringer M a n n h e i m / H i t a c h i 747 Analyzer (Boehringer Mannhei rm, Indianapolis, IN).
Biological Trace Element Research Vol. 48, 1995
126 Teuber et al.
Statist ics
Student's t-test was used for comparison of paired groups. Stu- dent's t-test with Cochran's corrections for unequal variances was used to compare groups of values with unequal variances. Pearson's simple correlations were performed. The results are presented as mean + SD. P < 0.05 was considered significant.
RESULTS
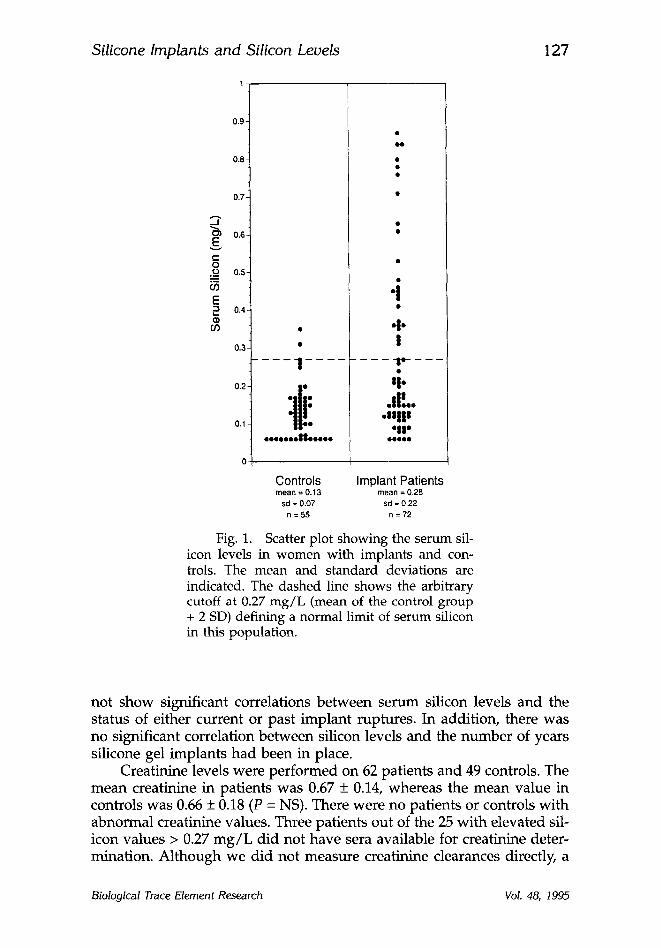
One hundred and ten women with a history of breast implants vol- unteered for the study. Thirty-eight women were excluded from analysis for the following reasons: 5 had polyurethane implants, 12 had dual lumen implants, 12 had only one implant, and 9 had undergone explan- tation prior to the blood draw. Of the remaining 72 women, the average age was 48.1 + 9.6 yr. Implants had been in place for a mean of 13.8 + 5.8 yr with a range of 1-27 yr. The 55 control women had a mean age of 47.7 + 10.7 yr (P = NS). The mean silicon level in women with implants was 0.28 + 0.22 mg/L with a range of 0.06-0.87 mg/L. The mean level in the control women was significantly less at 0.13 +_ 0.07 mg/L with a range of 0.06-0.35 mg/L (P < 0.01, t-test with correction for unequal variances). Figure 1 shows the distribution of silicon values for the two groups. The mean silicon level of the control group + 2 SD, 0.27 mg/L, can be used to designate a normal range for serum silicon in this population. Using this value as a cutoff, 25/72 (34.7%) of the implant patients exceeded this value, whereas only 2/55 (3.6%) of the controls were elevated.
Our original hypothesis had included the supposition that women with current implant ruptures at the time of the blood draw, and possi- bly those with past rupture, would have higher serum silicon levels than the rest of the implant patients. Eleven patients were available as a sub- group with current ruptures to test this hypothesis, and eight were found to have had past ruptures. Another woman was excluded from analysis because she had history of a past rupture as well as a current rupture. Four of the 11 patients with current rupture had surgery shortly after the blood draw, which confirmed rupture, in some cases, intracapsular and, in others, with extension beyond the implant connective tissue capsule. Seven patients have not had surgery yet, but are included in the group with current rupture based on MRI results in four and mammography with ultrasound in three. The mean silicon value for these women with current rupture was 0.24 + 0.15 mg/L, with a value of 0.27 + 0.22 mg/L in the 52 other implant patients without any known history of rupture (P = NS). The eight patients with a history of past rupture and subse- quent replacement of implants had a mean silicon level of 0.35 + 0.25 (P = NS). In some cases, there was documentation of silicone left on the chest wall; in others, past surgery included full capsulectomies and removal of all visible silicone gel. Pearson simple correlations also did
Biological Trace Element Research Vol. 48, 1995
Silicone Implants and Silicon Levels
1
127
0.9
0.8-
0.?-
._I
0.6-
~=
o .o_ 0.s- m
b5 E ~ 0.4,
if)
0.3.
0.2
0.1L
o-
- - - I . . . . . . .
:lli 0000000880 .00 .
o o
.i oJo I
- - l g l - - - - _ _ - -
,i. .d!..
.Ulll " I r
OQQeO
Controls Implant Patients mean = 0.13 mean = 0,28
sd = 0.07 sd = 0,22
n = 5 5 n = 7 2
Fig. 1. Scatter plot showing the serum sil- icon levels in women with implants and con- trois. The mean and standard deviations are indicated. The dashed line shows the arbitrary cutoff at 0.27 mg/L (mean of the control group + 2 SD) defining a normal limit of serum silicon in this population.
not show significant correlations be tween se rum silicon levels and the status of either current or past implant ruptures. In addit ion, there was no significant correlation be tween silicon levels and the n u m b e r of years silicone gel implants had been in place.
Creatinine levels were per formed on 62 patients and 49 controls. The mean creatinine in patients was 0.67 + 0.14, whereas the mean value in controls was 0.66 + 0.18 (P = NS). There were no patients or controls wi th abnormal creatinine values. Three patients out of the 25 wi th elevated sil- icon values > 0.27 m g / L d id not have sera available for creatinine deter- mination. Al though we d id not measure creatinine clearances directly, a
Biological Trace Element Research Vol. 48, 1995
128 Teuber et al.
previous study did not show significant elevations of serum silicon until renal insufficiency was marked with creatinine clearance < 40 mL/min (11) and another study showed good correlations between elevation of blood creatinine and silicon level (10).
DISCUSSION
Unfortunately, current technology precludes accurate quantitative measurements of silicone in biological fluids and tissues. However, all organosilicon compounds (including silicone) contain the element silicon, which can be measured accurately. ICP-AES appears to be a sensitive and precise means of measuring serum silicon levels. The mean level of sili- con in healthy individuals reported here, 0.13 mg/L, is similar to the mean values found in other studies: 0.11 mg/L by ICP-AES on whole blood from Angers, France (10), 0.14 mg/L by direct current plasma- atomic emission spectrometry (DCP-AES) on serum from Liverpool, Eng- land (11), and 0.15 and 0.17 mg/L on plasma by furnace atomic absorption spectrometry from Chapel Hill, NC (12,13). This is a proce- dure that will enable investigators to gather further analytical data on serum silicon levels in health and disease. There are no confirmed adverse health effects caused from accumulation of silicon from silicon dioxide in the dialysis bath water or drinking water in hemodiatysis patients (with serum levels up to 4.6 mg/L [12]). In fact, some have hypothesized that the high levels of silicon in blood may help protect hemodialysis patients from aluminum toxicity (14). However, another group reported that high levels of silicon, comparable to levels found in patients with renal failure, inhibit the activity of the antioxidant enzyme superoxide dismutase, which they propose could result in excess oxygen free radical production and deleterious complications, such as inflamma- tory conditions and cellular damage (15).
Silicone gel implant patients represent a completely different group, however, since the presumed source of the elevations of serum silicon-- as compared to hemodialysis patients--is a complex chemical polymer whose intermediate metabolic degradation products may have unknown and perhaps even deleterious effects. The fact that elevations are detected is significant, because for years, it had been believed that silicones were biologically inert and would not break down in the body. However, evi- dence has accumulated that silicones can induce significant local inflam- matory reactions (16) and migrate from the site of implantation. Garrido et al., in a series of publications (17-19), have shown both in animal mod- els and in women with silicone gel implants that silicone can clearly migrate from the site of implantation in an enclosed silicone rubber bag to distant sites, such as liver, and that the chemical species detected by nuclear magnetic resonance spectroscopy are not present in the original implant material, thus substantiating metabolic degradation in vivo.
Biological Trace Element Research VoL 48, 1995
Silicone Implants and Silicon Levels 129
It is interesting that women who had confirmed current ruptures of one or both implants did not necessarily have an elevated serum silicon level. Perhaps local inflammation is an important determinant of whether or not serum elevations are seen. One could hypothesize that those women with more inflammation around the silicone would have more degradation and thus a higher probability of detecting extra silicon in the serum. Conversely, those with more inflammation may have more depo- sition of collagenous scar tissue, in effect "walling off" the gel material from further interaction with the body. Several women who underwent surgery after their blood was drawn were found to have intact implants and yet had elevated silicon levels. We presume that this is reflective of the gel bleed that can occur from all implants (6). The current study was not designed to correlate elevations in silicon with symptoms, although this type of study appears worth doing, since perhaps those women with elevations reflect those women with a higher degree of inflammation around the implants or systemically. In addition, the chemical species present in the sera and the kinetics of the significant elevations seen, especially in a larger series of women with ruptures, are worth further evaluation.
ACKNOWLEDGMENTS
The help and contributions provided by James Valente and Marie Walsh are gratefully acknowledged.
REFERENCES
1. B. Arkles and P. Redinger, in Biocompatible Polymers, Metals, and Composites, M. Szycher, ed., Technomic Publishing, Lancaster, PA, pp. 749-768 (1983).
2. A. J. Christie, K. A. Weinberger, and M. Dietrich, JAMA 237, 1463-1464 (1977).
3. R. M. Goldblum, R. P. Pelley, A. A. O'Donnell, D. Pyron, and J. P. Heggers, Lancet 340, 510-513 (1992).
4. S. H. Yoshida, C. C. Chang, S. S. Teuber, and M. E. Gershwin, Reg. Toxicol. Pharmacol. 17, 3-18 (1993).
5. R. R. LeVier, M. C. Harrison, R. R. Cook, and T. H. Lane, Plast. Reconstr. Surg. 92, 163-167 (1993).
6. D. E. Barker, M. I. Retsky, and S. Schultz, Plast. Reconstr. Surg. 61, 836-841 (1978).
7. S. H. Yoshida, S. S. Teuber, J. B. German, and M. E. Gershwin, Fd Chem. Toxic. 32, 1089-1100 (1994).
8. J. L. Thomsen, L. Christensen, M. Nielsen, B. Brandt, V. B. Breiting, S. Felby, and E. Nielsen Plast. Reconstr. Surg. 85, 38-41 (1990).
9. R. M. Silver, E. E. Sahn, J. A. Allen, S. Sahn, W. Greene, J. C. Maize and P. D. Garen, Arch. Dermatol. 129, 63-68 (1993).
10. Y. Mauras, R Riberi, F. Cartier, and P. Allain, Biomedicine 33, 228-230 (1980). 11. N. B. Roberts and P. Williams, Clin. Chem. 36, 1460-1465 (1990).
Biological Trace Element Research Vol. 48, 1995
130 Teuber et al.
12. H. J. Gitelman, F. R. Alderman and S. J. Perry, Am. J. Kidney Dis. 19, 140-143 (1992).
13. H. J. Gitelman and E R. Alderman, J. Anal. Atomic Spectrom. 5, 687-689 (1990).
14. J. W. Dobbie and M. J. B. Smith, in Silicon Biochem., Ciba Foundation Sympo- sium 121, Wiley, New York, NY, pp 194-213 (1986).
15. R. Shainkin-Kestenbaum, A. J. Adler, and G. M. Berlyne, J. Trace Element Electrolytes Health Dis. 4, 97-99 (1990).
16. G. J. Picha and J. A. Goldstein Plast. Reconstr. Surg. 87, 490-496 (1991). 17. L. Garrido, B. Pfleiderer, B. C. Jenkins, C. A. Hulka, and D. B. Kopans, Mag.
Resonance Med. 31, 328-330 (1994). 18. Garrido, L., Pfleiderer, B., Papisov, M., and Ackerman, J. L., Ma. Reson. Med.
29, 839-843 (1993). 19. B. Pfleiderer, J. L. Ackerman, and L. Garrido, Man. Resort. Med. 30, 534-543
(1993).
Biological Trace Element Research Vol. 48, 1995
Related Documents











